Introduction
Overview
The term “epidermal nevus syndromes” defines a group of conditions characterized by the association of epidermal nevi with systemic manifestations. The two syndromes associated with neurologic expression due to CNS involvement that correspond to neurocutaneous syndromes are discussed in this review: keratinocytic nevus syndrome and sebaceous nevus syndrome. There are four distinctive phenotypes derived from the two principal syndromes: (1) Proteus syndrome; (2) sebaceous nevus, aplasia cutis congenita, limbal dermoid, and pigmented (melanocytic) nevus (SCALP) syndrome; (3) congenital lipomatous overgrowth, vascular malformations, epidermal (keratinocytic) nevi, scoliosis/skeletal and spinal anomalies (CLOVES) syndrome; and (4) Heide’s syndrome.
Other types of epidermal nevus syndromes that do not affect, or only rarely affect, the nervous system are not discussed in this article. They include Becker nevus syndrome, an epidermal nevus with hypertrichosis and “smooth muscle hamartoma” associated with shoulder, arm, and breast hypoplasia; inflammatory linear verrucous epidermal nevus (ILVEN) syndrome; and congenital hemidysplasia with ichthyosiform nevus and limb defect (CHILD) syndrome.
The area of distribution of the sebaceous or keratinocytic nevus is determined by the region of the neural crest involved.
Genetic somatic mutations occurring as mosaicism have been demonstrated in several subtypes; the most recent include postzygotic RAS mutations in both linear keratinocytic nevus syndrome and linear sebaceous nevus syndrome, the neurologic phenotypes. Another important mutation is the AKT1 gene in the Proteus syndrome subtype. The pathogenesis of skin lesions and many systemic anomalies in both phenotypes is explained by defective neural crest. The two most frequent phenotypes of epidermal nevus syndromes, linear keratinocytic nevus syndrome, and linear sebaceous nevus syndrome, are associated with neurologic manifestations, mainly epilepsy and intellectual disability. The most important cerebral anomaly that causes the neurologic picture is hemimegalencephaly, which is sometimes not recognized. The distinctive triad of facial keratinocytic or sebaceous nevus, hemifacial hyperplasia with lipomatosis, and ipsilateral hemimegalencephaly defines “Heide’s syndrome” (eponymous of the first patient reported with this entity), which is justified historically and medically. Frequently, one of the components of this syndrome is overlooked. Early recognition of Heide’s syndrome can help physicians plan a multidisciplinary approach to investigation, management, and prognosis. On the other hand, the term “linear sebaceous nevus syndrome” is a well-defined entity and has been recognized since the 19th century. It is inappropriate to rename it for a more recent author as an eponym, such as “Schimmelpenning syndrome,” due to the numerous previous and later contributions of so many authors over more than a century.
The discovery of activating HRAS and KRAS mutations in both keratinocytic and sebaceous nevi and their resulting phenotypes confirms the concept that they are a spectrum of the same syndrome (61; 66; 95; 164), confirming the early interpretation by Solomon and colleagues that epidermal nevus syndrome is an inclusive term for congenital disorders characterized by epidermal nevi as the common denominator and is associated with neurologic and other systemic involvement (160).
Key points
| |
• Epidermal nevus syndromes are an inclusive term for congenital disorders characterized by epidermal nevi as the common denominator and associated with neurologic and other systemic involvement. |
| |
• The pathogenesis of the skin lesions and many systemic anomalies in epidermal nevus syndromes is explained by a defect in neural crest. |
| |
• The two most frequent phenotypes, linear sebaceous nevus syndrome and keratinocytic nevus syndrome, are neurologic phenotypes. The most frequent manifestations are epilepsy and intellectual disability. These two main neurologic phenotypes are subdivided into several forms. The principal cerebral pathology is hemimegalencephaly. |
| |
• Genetic somatic mosaic mutations in HRAS and KRAS genes cause both keratinocytic nevus syndrome and linear sebaceous nevus syndrome. |
| |
• Proteus syndrome, a phenotype of keratinocytic nevus syndrome, is caused by somatic mutations in the AKT1 gene. |
| |
• There are four distinctive phenotypes derived from the two principal syndromes: (1) Proteus syndrome; (2) sebaceous nevus, aplasia cutis congenita, limbal dermoid, and pigmented (melanocytic) nevus (SCALP) syndrome; (3) congenital lipomatous overgrowth, vascular malformations, epidermal (keratinocytic) nevi, scoliosis/skeletal and spinal anomalies (CLOVES) syndrome; and (4) Heide’s syndrome. |
Historical note and terminology
In comparison with other neurocutaneous syndromes recognized in the 19th century with cutaneous lesions described before the neurologic findings, tuberous sclerosis in particular, the clinical neurologic picture of sebaceous nevus syndrome was described simultaneously with the skin lesions. One example is the case of a girl with ocular lesions, facial sebaceous nevus, and epilepsy as reported by Gerhardt in 1871 (58). In both conditions, the definite histopathological delineation of the cutaneous lesions and neuropathological features were defined later. The initial reports by distinguished 19th century dermatologists described in detail the clinical and histopathological characteristics of the two more frequent varieties of epidermal nevi associated with neurologic involvement: keratinocytic nevi by Von Baerensprung in 1863 (172) and sebaceous nevi by Jadassohn in 1895 (78). Other systemic involvement in sebaceous nevus syndrome, in particular ocular anomalies, was also described in the 19th century by Gerhardt in 1871 and Bogel in 1886 (58; 19). Before the detailed clinical and histopathological description of sebaceous nevus by Jadassohn, the distinction between keratinocytic nevus and sebaceous had not been established.
In the detailed clinicopathological description of sebaceous nevus made by Jadassohn (78), he cited Gerhardt’s contribution. Despite the early descriptions by Jadassohn in 1895 and others in the 19th century, as well as reports in the early 1920s and 1930s, the subtype of linear sebaceous nevus syndrome was recognized and considered a new neurocutaneous syndrome only after the early 1960s with the report of Feuerstein and Mims in 1962 and early 1970s (49; 105; 72; 167; 91). Those early reports were followed by numerous case reports and reviews of sebaceous nevi in the face, scalp, neck, trunk, and extremities. In several instances, patients presented neurologic, ocular, or other systemic features (159). Jadassohn himself recorded involvement of the CNS in some of the articles he reviewed and cited Gerhardt’s case (78; 182). Particularly after Robinson, many authors have used the term “nevus sebaceous of Jadassohn,” which is justified because he was the first to describe this lesion (135).
The first detailed report of a patient with a keratinocytic nevus syndrome with the typical neurologic picture of epilepsy and intellectual impairment was the case of a girl who had left hemifacial hyperplasia, left verrucous keratinocytic nevus in of the face, neck, and arm, associated with ipsilateral hemimegalencephaly, confirmed by autopsy (62). By disgrace, Heide, the little girl who was the subject of this report, was a victim of “active euthanasia” in 1943 (138). Two years after that report, Schimmelpenning described a 17-year-old female with a sebaceous nevus located in the left side of the scalp, a nevus vasculosus on the left side of the neck (more likely part of the nevus and not hemangioma), ocular anomalies, and epilepsy under the title “Clinical contribution to symptomatology of phakomatosis” (151). Although he did not include Jadassohn’s reference in his report, Schimmelpenning did recognize Jadassohn’s contribution in the text, saying: “Jadassohn was probably the first to recognize nevus sebaceous and differentiate it from adenoma Pringle.” It was the report by Feuerstein and Mims of two children with a linear sebaceous nevus in the midline of the face (confirmed by skin biopsy) associated with epilepsy and cognitive deficit under the explicit title “Linear nevus sebaceous with convulsions and mental retardation” that drew attention from the medical community towards this “new” neurocutaneous syndrome (49). Soon after, the recognition of this constellation resulted in numerous reports under the designation “linear sebaceous nervus syndrome” and sometimes “Feuerstein-Mims syndrome” or “Schimmelpenning-Feuerstein-Mims syndrome” appeared, adding ocular, cardiovascular, renal, and musculoskeletal anomalies. Solomon and colleagues reported 12 patients with epidermal nevi associated with a variety of systemic anomalies and further reviewed the syndrome. They coined the term "epidermal nevus syndrome," the rubric that remains widely accepted and encompasses the different phenotypes (160; 159; 55; 51). In their review of 60 patients, Solomon and Esterly further defined a variety of clinical presentations (159).
Happle stated that Feuerstein and Mims “rediscovered” in English the condition described by Schimmelpenning in 1957 in German, ignoring the early contributions of Gerhardt, Bogel, and Jadassohn, which were also in German, and he asserted that this syndrome should bear Schimmelpenning’s name (70). The eponym Schimmelpenning syndrome is not appropriate because Jadassohn was the first to define the histopathology and clinical features of sebaceous nevi in 1895; other authors, beginning in the 20th century, also contributed to defining the “linear sebaceous nevus syndrome” (54). Also, it is noteworthy that the two unrelated children reported by Feuerstein and Mims in 1962 represent the typical presentation of sebaceous nevi located in the midline of the face or mildly lateralized, extending from the forehead as a continuous line to the tip of the nose and corresponding to the distribution of the prosencephalic neural crest (51). The sebaceous nevi of the patient described by Schimmelpenning was located on the left side of the scalp, face, eye, and neck and arose mainly from the mesencephalic neural crest. Even though both lesions correspond to sebaceous nevi, it is important to distinguish them because the different distribution suggests a difference in neural crest origin. It is correct to continue using the descriptive term suggested by Feuerstein-Mims to the condition they described in 1962, including cases with other locations of the sebaceous nevus, retaining the term “linear sebaceous nervus syndrome” (coined by Lansky and colleagues) to denote the association with neurologic and other systemic anomalies described by many authors (91). When referring to either form (midfacial or lateral scalp) or other localization of sebaceous nevi, associated with systemic findings, the term “linear sebaceous nevus syndrome” should be appropriately applied.
Other authors have expressed that it is not justified to designate either Schimmelpenning or Feuerstein and Mims to the syndrome (Feuerstein and Mims did not try to give their name to the syndrome) because the large number of contributors to the description of these disorders over more than a century precludes the use of new author eponyms (167; 182).
In Jadassohn’s original description, he considered sebaceous nevi as “organoid” due to the involvement of several skin adnexa; therefore, several authors have used the term "organoid nevi” and “organoid nevus syndrome" (108; 13; 153). Jadassohn made seminal contributions to dermatology besides the first definition and correct classification of the sebaceous nevus (177).
Epidermal nevi correspond to a distinct group of congenital hamartomatous malformations of the skin; there are several types and several syndromes. They are classified based on histopathological criteria according to their predominant component (159; 123; 137; 136; 162; 171). Only two types, keratinocytic and sebaceous nevi, are associated with CNS involvement and neurologic manifestations (49, 55; 49, 51). When these nevi are associated with neurologic and systemic involvement, keratinocytic or sebaceous nevus syndromes result, and two main phenotypes are delineated: linear nevus sebaceous syndrome and keratinocytic nevus syndrome. Phakomatosis pigmentokeratotica is the coexistence of nevus sebaceous with melanocytic nevi (71; 74). In a few cases of phakomatosis pigmentokeratotica, intellectual deficit can be present but cerebral anomalies were not demonstrated (165; 57).
The incidence of epidermal nevi is approximately 1 in 1000 live births without gender predominance (159). In a study, epidermal nevi were seen in 1 of 85 pediatric dermatologic patients, and epidermal nevus syndromes showed a relative frequency of 1 in 1080 of these patients (171).
Sebaceous nevus can often be diagnosed at birth (58; 111; 97). Although the nonspecific term “epidermal nevus syndrome” is often used interchangeably with “keratinocytic nevus syndrome” and “linear nevus sebaceous syndrome,” the last two terms should be applied more specifically to avoid ambiguity. Linear nevus sebaceous syndrome should be restricted to those cases with sebaceous nevi; an example is the typical nevus in the midline of the forehead as a yellowish to orange or tan plaque-like nevus known as nevus sebaceous of Jadassohn.
Nevus of Jadassohn in a 5-year-old boy
(A) Face of a 5-year-old boy with a typical nevus of Jadassohn in the frontal region, dorsum of the nose and neck on the left side. A continuous line extends from the forehead onto the nose. He has epilepsy and mild intellectual d...
Blaschko described the linear pattern of epidermal nevi and other dermatoses, now known as “Blaschko lines,” and other authors have confirmed the pattern (18; 69; 162; 171). Blaschko lines are traditionally thought to be pathways of embryonic and fetal skin cell development and migration (18; 110). Subsequent reconsideration of their embryology suggests that the lines of Blaschko more likely correspond to neural crest migrations to and within the dermis (147). It is important to distinguish that in epidermal nevus syndrome, there are two main neurologic phenotypes with prominent involvement of the central nervous system: the linear sebaceous nevus syndrome and keratinocytic nevus syndrome; both have characteristic clinical subtypes.
-
Epidermal nevus syndrome in a 10-year-old boy
Face of a 10-year-old boy with a lightly pigmented epidermal nevus and a lipomatous mass on the right side of the face; he has right hemimegalencephaly and intellectual disability with left hemiparesis and left-sided epilepsia ...
-
Linear sebaceous nevus syndrome in a 16-year-old boy
(A) 16-year-old boy with several epidermal nevi, left complex choristoma, profound intellectual disability, and severe refractory epilepsy that caused the right frontal injury observed in the picture. (B) A large sebaceous nevus o...
There are four subtypes of the two main neurologic phenotypes originally described in the last century or earlier. The acronym SCALP, which stands for sebaceous nevus, central nervous system malformations, aplasia cutis congenita, limbal dermoid, and pigmented nevus (melanocytic nevus), was introduced for this particular clinical presentation (90; 75; 29). Patients identified under another acronym, CLOVES syndrome, were initially mistakenly identified as having Proteus syndrome (145). CLOVES stands for congenital lipomatous overgrowth, vascular malformations, and epidermal nevi, later expanded to CLOVES syndrome to include the association with scoliosis and skeletal and spinal anomalies (05). CLOVES syndrome can be associated with hemimegalencephaly but only infrequently is recognized (63).
Proteus syndrome is a complex hamartomatous disorder characterized by disproportionate, asymmetrical overgrowth of any tissue of the body, particularly the skeleton, cerebriform connective tissue nevi, epidermal nevi, vascular malformations, and dysregulated adipose tissue with multiple systemic complications (32; 33; 16). Proteus syndrome is a distinctive and severe neurologic phenotype of keratinocytic nevus syndrome (55; 51). Hemimegalencephaly is the most common cause of neurologic manifestations (134; 33; 55; 51).
Heide’s syndrome is characterized by congenital hemifacial hyperplasia with lipomatosis, epidermal or sebaceous nevus, and hemimegalencephaly.
Clinical manifestations
Presentation and course
Since the early detailed description of a variety of epidermal nevi and the associated systemic anomalies, the clinical picture has been delineated. There are numerous case reports and series of patients in the literature. These contributions have led to the definition of two distinct neurologic phenotypes: keratinocytic nevus syndrome and sebaceous nevus syndrome.
Cutaneous and subcutaneous lesions. Epidermal nevi may be present at birth in particular sebaceous nevi (106) or may develop later in infancy; some usually increase around the time of puberty. During childhood, sebaceous nevi become progressively darker, thicker, and extend in size, but stabilize on reaching adolescence (170). The two most frequent epidermal nevi are sebaceous nevus and keratinocytic nevus (also referred to as epidermal nevus or verrucous nevus); both correspond to neurologic phenotypes (51). The age-dependent progression of sebaceous nevus is related to hormonal factors (129; 176). Three different stages were described in a nevus sebaceous life history (108). First, in infancy and childhood, the nevus usually is flat and hairless with underdevelopment of sebaceous glands and hair. A second phase at puberty is marked by massive development of sebaceous glands and papillomatous epidermal hyperplasia. The third stage is characterized by benign or malignant neoplasms that originate in the nevi. Linear sebaceous nevi are found in 10% of patients on the face and scalp (159). In a careful literature review of 37 cases, sebaceous nevi were found in the face in 83%, scalp and cheek in 54%, forehead and neck in 43%, extremities in 48%, and trunk in 32% (182). An unusual cerebriform aspect suggestive of sebaceous nevus can be observed in the scalp (10). The plaques of the nevus are free of hair and verrucous components, and the color ranges from yellow-orange in white children to hypermelanotic in black children. The size of a nevus sebaceous is considered “giant” if the lesions are greater than 20 cm or greater than 1% of the total body surface area (30). A congenital area of alopecia on the scalp may be a sign of sebaceous nevus that should be distinguished of aplasia cutis congenita (125). Typical lesions are easily diagnosed, but the differential diagnosis may be difficult if the clinical features of the lesion are not distinctive (115).
Linear sebaceous nevus syndrome in a 16-year-old boy
(A) 16-year-old boy with several epidermal nevi, left complex choristoma, profound intellectual disability, and severe refractory epilepsy that caused the right frontal injury observed in the picture. (B) A large sebaceous nevus o...
Acanthosis nigricans-like lesions also are sometimes found on the face and neck (140). The distribution of the nevus in the scalp may be rendered indistinct by its broad patches, but it is said to follow the lines of Blaschko (69). The severity of the cutaneous lesions ranges from subtle, in which case they may go unrecognized, to extensive, disseminated nevi producing major cosmetic defects, particularly in those cases with severe, unilateral facial involvement.
Several cases of newborns with distinct syndromic presentations have been reported in the literature. It includes sebaceous nevus syndrome, central nervous system malformations (including hemimegalencephaly), aplasia cutis congenita, limbal dermoid, pigmented nevus (giant congenital melanocytic nevus) and neurocutaneous melanosis; the acronym SCALP was proposed for this distinctive presentation (90; 75). A more frequent phenotype in infants is characterized by scalp sebaceous nevus with ipsilateral ocular anomalies including complex choristoma and hemimegalencephaly but without melanocytic nevi (125).
Histopathologic examination of sebaceous nevi shows hyperplasia and a larger number of sebaceous glands even in areas where they are usually scarce, such as the trunk and extremities (78). However, in some sebaceous nevi, sebaceous glands may be minimal or even absent (108; 159; 182). Jadassohn referred to sebaceous nevi as organoid nevi because of the histopathological characteristics of involvement of multiple skin constituents besides the sebaceous glands. Other cutaneous alterations are found in more than one third of patients with epidermal nevus syndrome; these include hemangiomas, large hypopigmented patches, acanthosis nigricans-like lesions, giant and multiple café-au-lait spots, and melanocytic nevi. The risk of developing cutaneous neoplasms, particularly basal cell carcinoma, is 10% to 15% (108). The development of squamous cell epithelioma or carcinoma within a nevus sebaceous of Jadassohn is rare (126; 15). Viral warts commonly affect nevus sebaceous, from 2.3% to 11.6% of cases (34), including the putative human papillomavirus (HPV)-induced tricholemmoma (79). HPV DNA is prevalent in nevus sebaceous of Jadassohn, and HPV 16 is the most frequently detected genotype, suggesting maternal transmission and infection of an ectodermal stem cell, which could explain its distribution along Blaschko lines (26).
The uncommon phenotype of hemifacial hyperplasia with subcutaneous lipomatosis associated with both keratinocytic and sebaceous nervus associated with hemimegalencephaly corresponds to Heide’s syndrome (53; 51). In a few instances this hemifacial mass has been described as lipoma (45; 52).
Epidermal nevus syndrome in a 10-year-old boy
Face of a 10-year-old boy with a lightly pigmented epidermal nevus and a lipomatous mass on the right side of the face; he has right hemimegalencephaly and intellectual disability with left hemiparesis and left-sided epilepsia ...
This entity is often referred to as “facial hemihypertrophy,” “facial hypertrophy,” or “facial overgrowth” (127; 04; 183; 53). This lesion was defined as an entity under the term “congenital infiltrating lipomatosis of the face” (CILF), and the histopathological features were established (158). However, it is important to recognize that congenital hyperplasia of hemifacial structures and the ipsilateral lipomatosis occur simultaneously and correspond to a single entity. Therefore, “congenital hemifacial hyperplasia with lipomatosis” is an inclusive term for both anomalies (131; 55; 51). This anomaly is frequently associated with hemimegalencephaly (169; 11; 53; 54). Several authors have reported patients with hemimegalencephaly associated with this infiltrative lipomatous hemifacial lesion without recognizing it; in some cases, the epidermal nevus syndrome was also unrecognized (169; 41). Congenital hemifacial lipomatosis has a more aggressive behavior than a lipoma due to infiltration of surrounding tissues.
Congenital hemifacial hyperplasia with lipomatosis is a more accurate designation that denotes its marked asymmetry; further, “lipomatosis” already implies an infiltrative behavior and is not necessary in the title (53; 54). This anomaly also may be associated with Proteus syndrome and other neurocutaneous syndromes, such as Klippel-Trenaunay syndrome and hypomelanosis of Ito.
Musculoskeletal abnormalities. Various forms of skeletal involvement are reported in 68% of patients with epidermal nevus syndrome (159); they include localized alterations of the cranium consistent with fibrous dysplasia, and primary or secondary bony defects. Scoliosis may be present from early infancy (119); kyphoscoliosis is a common complication, but it may not become evident until late childhood. Unilateral hypoplasia may involve any skeletal structure, such as the calvarium, mandible, scapula, ribs, vertebrae, or long bones of the extremities. Several case reports associate vitamin D-resistant rickets and epidermal nevus syndrome (09; 120); the suggested cause is the production of phosphaturic substances by the epidermal nevi. Various studies support that phosphaturia, caused by circulating factor(s), may be secreted by an epidermal nevus. The nature of these phosphaturic factor(s), called "phosphatonin(s)," is not well understood, but elevated levels of circulating FGF-23 were reported in a patient with hypophosphatemic rickets (112). Clinical symptoms are marked bony abnormalities, muscle weakness, and bone pain. Another case with epidermal nevus syndrome and hypophosphatemic rickets with a long follow-up has been reported (119). Hemicorporal hypertrophy is reported rarely (140). Defects in or thickening of the cranial vault overlying the enlarged cerebral hemisphere in associated hemimegalencephaly may occur. Musculoskeletal and spinal anomalies are prominent in CLOVES syndrome (05).
Thickening of the cranial vault (MRI)
Coronal MRI of the previous patient (a 10-year-old boy with right facial epidermal nevus, hemifacial lipomatosis, and hemimegalencephaly) shows the cranial osseous dysplasia on the side overlying the dysplastic cerebral hemisphere...
Neurologic manifestations. Epilepsy, intellectual disability, and focal motor deficits are the principal manifestations observed in patients with the neurologic phenotypes of keratinocytic or sebaceous nevus syndrome. About one third of affected children have CNS involvement (159; 123). A minority has absence of the corpus callosum (64). When neurologic manifestations are present, the epidermal nevus usually affects the scalp or the face; however, its localization may also be outside of the head. Arachnoidal cysts frequently occur in the posterior fossa (117). A preterm infant with a rare presentation of sebaceous nevus syndrome had an extracranial congenital cylindromatous tumor of the scalp that was turban-like and larger than the head (133). A large sebaceous nevus on the left side of the face and multisystemic anomalies were found prenatally and confirmed at birth. She died in the immediate peripartum period.
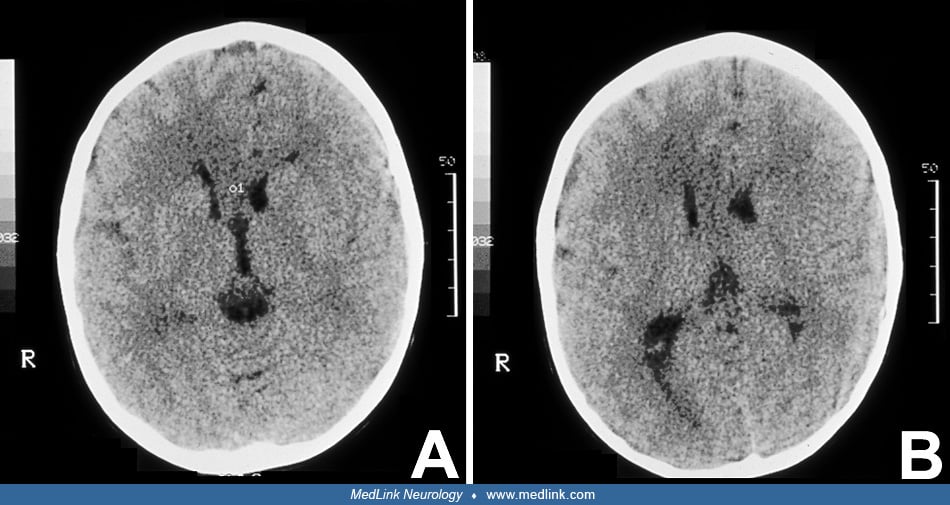
Midline nevus of Jadassohn (CT)
Axial CT scan of a 3-year-old girl with a midline nevus of Jadassohn involving the forehead and nasal bridge (not shown). Agenesis of the corpus callosum and right hemimegalencephaly are demonstrated; the right occipital horn show...
Hemimegalencephaly is the most important and severe cerebral lesion associated with keratinocytic and linear nevus sebaceous syndromes (73; 157). The usual manifestations are epilepsy and intellectual disability. This association plus the presence of congenital hemifacial hyperplasia with lipomatosis corresponds to Heide’s syndrome; infantile spasms are frequent with onset in infancy (143; 51). Patients with this triad in which hemifacial lipomatosis or sometimes one of the other two components are present suggest Heide’s syndrome (140; 141; 127; 47; 37; 174; 04; 170).
-
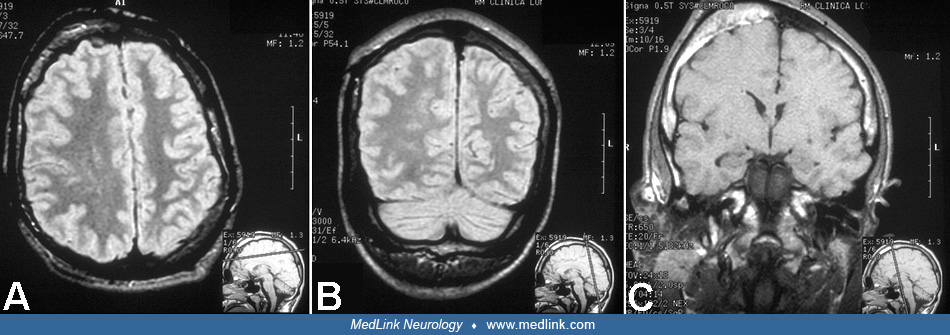
Right epidermal nevus syndrome and hemifacial lipomatosis (MRI)
(A, B) MRI of axial and coronal views of the brain, showing right hemimegalencephaly and islands of heterotopic gray matter within deep subcortical white matter of centrum semiovale. (C) Coronal MRI shows an expansion of the right...
-
Midline nevus of Jadassohn (CT)
Axial CT scan of a 3-year-old girl with a midline nevus of Jadassohn involving the forehead and nasal bridge (not shown). Agenesis of the corpus callosum and right hemimegalencephaly are demonstrated; the right occipital horn show...
-
Nevus of Jadassohn in a 5-year-old boy
(A) Face of a 5-year-old boy with a typical nevus of Jadassohn in the frontal region, dorsum of the nose and neck on the left side. A continuous line extends from the forehead onto the nose. He has epilepsy and mild intellectual d...
When the epidermal nevus is located in the midline of the face (nevus of Jadassohn, linear sebaceous nevus) the hemimegalencephaly may be on either the right or left side. However, when the facial nevus is lateralized, the hemimegalencephaly is on the same side. The proposal of the term “Heide’s syndrome” to honor this girl and to draw attention to this entity is justified (54). The largest series to date of cases characteristic of Heide’s syndrome was published by Pavone and colleagues (127). Patients with epidermal nevus syndrome and hemimegalencephaly without hemifacial lipomatosis also may be seen (20; 50; 52).
Epilepsy is the most constant feature (25% of all patients) but is expressed in 61% to 75% of those with linear sebaceous nevus syndrome (09; 170). In patients with hemimegalencephaly, epilepsy is present in almost all (52). The onset of seizures is early, sometimes in the first postnatal days, and, in most cases, within the first 8 months of life. Several forms of epilepsy are recognized and may be classified into a series of epileptic syndromes (50). They include infantile spasms or West syndrome, sometimes evolving into Lennox-Gastaut syndrome (88; 170; 142), and Ohtahara syndrome progressing to Lennox-Gastaut syndrome (111). The Ohtahara syndrome is observed in newborns and is occasionally associated with epidermal nevus syndrome (52). Epidermal nevus syndrome may also be the underlying factor in partial motor seizures and generalized major motor seizures (12). Infantile spasms are the usual presentation of onset (72; 88; 12; 142). Epilepsia partialis continua is an infrequent but severe form of presentation. Hemimegalencephaly with enlargement of the parietotemporal region (88) or temporal lobe (89) also may be associated with infantile spasms.
Epidermal nevus syndrome in a 10-year-old boy
Face of a 10-year-old boy with a lightly pigmented epidermal nevus and a lipomatous mass on the right side of the face; he has right hemimegalencephaly and intellectual disability with left hemiparesis and left-sided epilepsia ...
Infantile spasms are frequent. The EEG generally shows bilateral hypsarrhythmia, but sometimes asymmetrical or unilateral hypsarrhythmic patterns are observed (88; 17). The outcome in this group of patients is poor. Many of these cases are associated with hemimegalencephaly (140; 127; 47; 52).
When hemimegalencephaly is not present, seizures may not appear until several years of age. Partial motor seizures, contralateral to the brain lesion, or partial complex seizures characterize a frequent type of epilepsy in these patients. Partial seizures sometimes progress to secondary generalization (64). Generalized seizures are reported as tonic-clonic in type (64), but in these cases, the EEG may nevertheless reveal intermittent focal paroxysmal discharges (137) or even continuous unilateral irregular paroxysmal activity with single spike-wave complexes (20). An uncommon type of seizure also reported in epidermal nevus syndrome is startle epilepsy, which presented at 3 years of age as massive myoclonus followed by tonic extension and precipitated by unexpected loud auditory stimuli but was not associated with other types of epileptic activity (149). In a rare case of a young woman with a left congenital linear verrucous nevus and hemifacial lipomatosis, ipsilateral cerebellar hypertrophy without apparent supratentorial involvement was found by MRI (128). Arachnoidal cyst in the left middle cranial fossa can occur underlying facial and scalp plaques of sebaceous nevi on the left temporal region (94).
Intellectual disability is the second neurologic manifestation in epidermal nevus syndromes, affecting approximately 50% to 60% of patients with linear sebaceous nevus syndrome (101; 64). It is more frequent in patients with hemimegalencephaly as a moderate to severe degree of intellectual impairment (127).
A less frequent neurologic manifestation is the presence of focal motor deficit, mainly hemiparesis and diparesis, either spastic or hypotonic. Hemiparesis may be seen in cases with hemimegalencephaly, though some exhibit remarkably little or no asymmetry of muscle tone, reflexes, and motor function, perhaps because of the early development of bilateral corticospinal tract projections from the uninvolved cerebral hemisphere (146). Hemiparesis also may be the result of vascular complications such as cerebral infarction with subsequent porencephaly (12; 42). Intraspinal lipomas have been identified as a cause of motor deficit (104); in the same report, the authors included a case of intracranial lipoma at the cerebellopontine angle. Another report of two patients with intraspinal lipomas describes an infant without cord symptoms (21). A male infant with a keratinocytic nevus in the trunk developed atrophy of the spinal cord with progressive paraparesis secondary to a paravertebral intraneural tumor with Schwann cell proliferation in addition to a large intraspinal lipoma causing spinal cord compression; a mosaic KRAS mutation was confirmed in adolescence (48). Vascular anomalies are a rare cause of neurologic signs. A 30-month-old girl with epidermal nevus syndrome presented vascular malformations of the azygos vein and anterior cerebral artery, a cortical aneurysm, and right internal carotid artery hypoplasia (81). An uncommon presentation, paraplegia resulting from spinal cord hemorrhage, was reported in a patient with epidermal nevus syndrome who exhibited many vascular and skeletal anomalies (84).
One 21-year-old man was reported with a fusiform dilated aneurysm of the left intracavernous carotid artery associated with hypervascularity throughout the left parieto-occipital areas supplied by both the middle and posterior cerebral arteries and a second large, fusiform eccentric basilar summit aneurysm, which was demonstrated by cerebral angiography. These vascular anomalies were associated with CT demonstration of extensive calcifications in the left posterior parietal lobe with contrast enhancement in the same region, but the aneurysms did not rupture to cause subarachnoid or intracerebral hemorrhage (12). At surgery, the carotid aneurysm was too large to clip, so it was coated to reinforce the integrity of the vessel wall. Another case of aneurysm in the internal carotid and extensive epidermal nevus was associated with a Chiari I malformation (122).
Severe epilepsy and chronic inappropriate antidiuretic hormone secretion since birth was described in a 1-year-old boy with hypermelanosis as well as epidermal nevus syndrome (181). A congenital cylindromatous turban tumor with cerebral infarcts was reported in a preterm infant (133).
Neuropathologic examination of the hemimegalencephalic brain reveals increased volume of white matter, polymicrogyria and pachygyria, many heterotopic neurons, and prominent astrogliosis or even gliomatosis cerebri (31; 67; 141); hypertrophic neurons with increased dendrites and dendritic spines are disclosed by Golgi impregnation (141). Immunocytochemical studies demonstrate mixed cellular lineage as the pathogenesis of hemimegalencephaly, with abnormal cellular migration being a secondary defect, with similarities to tuberous sclerosis (56). Overexpression of abnormally phosphorylated tau, a microtubule-associated protein, in dysmorphic neurons, glial cells and neuropil of the hemimegalencephalic malformation has been demonstrated that corresponds to an early defect in microtubules (148). Microtubules are amongst the earliest structures of cellular differentiation, forming the strands in mitotic spindles and determining cellular polarity, lineage, morphology, growth, and migration so that the similar cytological dysmorphism in hemimegalencephaly and tuberous sclerosis can be explained by defective tau in both; the two disorders also both exhibit similar abnormalities of the mTOR pathway (35; 148). Tauopathies acquired in late adult life, by contrast, cause neuronal degeneration clinically expressed as dementia.
Ocular abnormalities. Ocular anomalies occur in 22% to 68% of patients with epidermal nevus syndrome (123). Solomon and Esterly reported an incidence of 33%, and they were found in 13 in a series of 39 children (33%) with strabismus as the principal manifestation (159; 137). Epibulbar choristoma is one of the most common ocular anomalies in linear nevus sebaceous syndrome. The first report of a patient with ocular anomalies ipsilateral to an extensive nevus sebaceous in the scalp, face and neck, and on the left side was made by Bogel in an 8-year-old boy (19). This is the same phenotype as the patient reported by Schimmelpenning in 1957.
Ocular anomalies are predominantly associated with linear sebaceous nevus syndrome and are always present at birth (51).
-
Linear sebaceous nevus syndrome in a 16-year-old boy
(A) 16-year-old boy with several epidermal nevi, left complex choristoma, profound intellectual disability, and severe refractory epilepsy that caused the right frontal injury observed in the picture. (B) A large sebaceous nevus o...
-
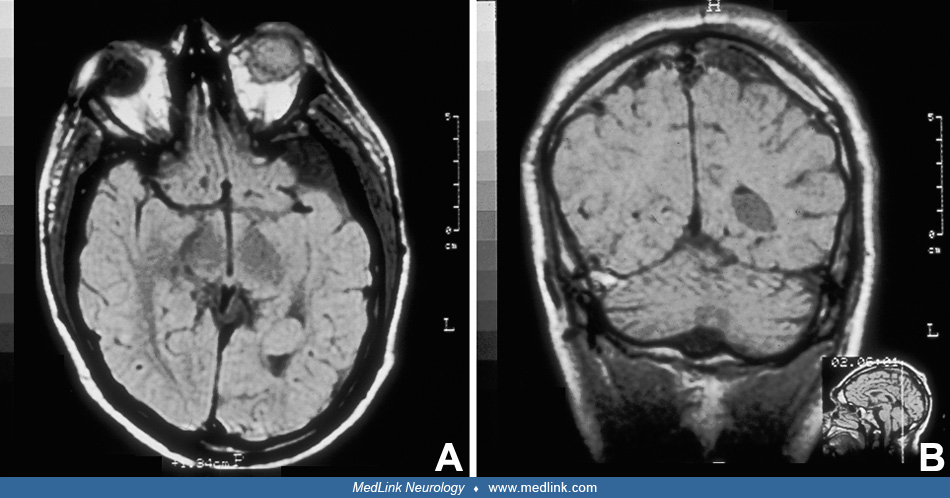
Epidermal nevus syndrome in a 16-year-old boy (MRI)
(A) Axial MRI at level of orbits reveals a left ocular hamartoma and also shows a mass in the occipital horn of the left lateral ventricle that does not obstruct the flow of CSF. (B) Coronal view of MRI at the level of the parieta...
Some ocular lesions are bilateral, even if asymmetrical cerebral involvement, including hemimegalencephaly, is present (64). Ipsilateral hypoplasia of the optic radiation with hemimegalencephaly also is described (22). Colobomata may affect the retina, choroid, iris, and eyelid (113), or the pupil may be ectopic as a minimal expression. Ocular histologic immaturity suggesting developmental arrest also was reported (154). Other anomalies include microphthalmia, macrophthalmia, cataracts (usually unilateral), corneal vascularization, and ocular hemangiomas. In linear sebaceous nevus, the palpebral and bulbar conjunctivae commonly are involved. Choristomas represent congenital overgrowths of normal tissue in an abnormal location. Histologically, they may be divided into dermoids, lipodermoids, and simple or complex choristomas (46; 156). Simple choristomas have ectopic tissue of only one type (dermis-like tissue, lacrimal gland, bone, etc.), whereas complex choristomas have ectopic tissue of ectodermal and mesodermal origin and may be composed of lacrimal gland, bone, cartilage, adipose tissue, neural tissue, or smooth muscle (46; 156). Complex choristomas are rare. They are usually unilateral and highly vascularized; when composed mainly of acinar elements, they have raised nodules as well (156). Complex limbal choristomas, unilateral choristoma of the upper fornix, and bilateral choristoma of the upper fornix and bilateral choroidal osteoma also are reported (113; 44). Bilateral anomalies are uncommon (82; 29). Cortical blindness (12; 67) and other forms of neuro-ophthalmological alterations such as oculomotor dysfunction and nystagmus are described (123). Neoplasms are not a frequent complication, but optic nerve glioma has been reported (150). A child with unilateral orbital lipoma also presented another lipoma in the cerebellopontine angle (153; 25). A rare case of rod-cone dystrophy was confirmed in a patient with linear sebaceous nevus syndrome confirmed by electroretinographic study; it should be differentiated from the findings in high myopia (93). MRI can demonstrate hypoplasia of the optic nerve and the optic chiasm (29).
Cardiovascular abnormalities. Patent ductus arteriosus and coarctation of the aorta are the most common cardiovascular anomalies described in epidermal nevus syndrome (160; 162; 173). A child with patent ductus arteriosus and chronic occlusion of the left distal internal carotid artery showed resulting ipsilateral cerebral atrophy (25). A study found that vascular malformations occur with a higher frequency (12.6% to 33%) in these patients as compared with the general population (less than 1%) (60). Severe cardiac arrhythmia has been reported in neonates with sebaceous nevus syndrome (167; 36). Hypertension was incidentally discovered in a 3-year-old boy with congenital right hemifacial and cervical sebaceous nevi and conjunctival lipodermoid at the time of surgery for the cervical nevi (06). He also had a mild coarctation of the aorta and stenosis of renal arteries. A female neonate born at 36 weeks presented with extensive sebaceous nevi in the scalp, face, neck, arm, and chest associated with aortic coarctation that was surgically repaired at 1 week of age (86). Her magnetic resonance angiogram revealed diffuse aortopathy extending from the aortic arch to the abdominal aorta. Her blood pressure was controlled medically.
Endocrine involvement. The association of epidermal nevus syndrome with central precocious puberty is reported in several patients (180; 64; 166). Magnetic resonance imaging of the brain in these cases may be normal or may reveal an enlarged hamartomatous pineal body and macrocephaly, but hypothalamic or pituitary lesions have not been demonstrated (64). Precocious puberty may also be associated with adnexal tumors like ovarian cysts, but normal endocrine status is reported in these cases (89). The case of a female neonate with congenital rhabdomyosarcoma who later developed central precocious puberty, hemihypertrophy, and vitamin D3-responsive hypophosphatemic rickets at the age of 14 months is a rare association in epidermal nevus syndrome (152).
Renal anomalies. They include fused (horseshoe) kidneys, Wilms tumor (111), and renal artery stenosis with subsequent hypertension (02). The association of multicystic dysplastic kidney with Wilms tumor was reported (116). A female neonate with linear nevus sebaceous syndrome who presented with chorioretinal coloboma and multiple nevus sebaceous since birth also had cystic kidney disease and diffuse aortopathy with bilateral renal artery stenosis (86). She developed hypertension requiring oral antihypertensive medications. Aortic coarctation was treated surgically at 1 week of life. Her magnetic resonance angiogram revealed diffuse aortopathy extending from the aortic arch to the abdominal aorta. Branches of the aorta, including the celiac trunk, superior mesenteric arteries, and renal arteries were also narrowed. Multiple renal cysts were identified in her right kidney. The authors stated that renal Involvement in linear nevus sebaceous syndrome might be underrecognized.
Orodental anomalies. Orodental anomalies have been observed since early reports of epidermal nevus syndromes. Hypoplastic dental enamel has been reported by several authors, particularly in Proteus syndrome (83). In patients with keratinocytic nevus syndrome, the warty lesion in the face can extend to the mucous membrane of the lips, buccal mucosa, gingiva, and soft palate (83; 24). In patients with keratinocytic nevus syndrome, oral linear papillomatous lesions can be so extensive that they reach the hard palate and laryngopharyngeal structures, causing obstruction and difficultly swallowing food (01). Anomalies such as mandibular ameloblastoma are rare (14). Sensorineural deafness, partial anodontia, blocked tear ducts, and labiopalatoschisis are unusual associations to epidermal nevus syndrome (121).
Orthopantomography shows poor development of the right upper and lower jaw bones as well as the alveolar bone (124).
Prognosis and complications
The prognosis depends largely on the associated complications, the degree of intellectual deficit and the severity of epilepsy, and its response to pharmacological control. Hemispherectomy is a high-risk procedure in cases associated with hemimegalencephaly, but in several patients, it has provided control or at least partial improvement of epilepsy refractory to anticonvulsants alone. Associated systemic involvement that includes cardiovascular anomalies (patent ductus arteriosus, coarctation of the aorta), ocular (choristomas, colobomata, microphthalmia), musculoskeletal (scoliosis, hypoplasia, or aplasia of multiple bones), and endocrine (precocious puberty), increase morbidity. Congenital hemifacial hyperplasia with lipomatosis is an indication to look for hemimegalencephaly and Heide’s syndrome. One of the risks in these patients is anesthetic complications during surgical interventions (39). Basal cell carcinoma and other cutaneous neoplasms occur in 15% of nevi. CNS neoplasms are uncommon and may arise within the dysplastic cerebral tissue. Malignant transformation of nevus sebaceous can occur in childhood or adolescence and may undergo malignant transformation to basal cell carcinoma (139). They believe all nevus syndromes should be excised; however, timing of excision can be flexible. Optic glioma has been infrequently reported in association with linear sebaceous nevus syndrome (150). Surgical resection of hemifacial lipomatosis is difficult because of infiltration and lack of encapsulation; it usually requires reintervention (169). A severe form of epidermal nevus syndrome is associated with brainstem and cerebellar malformations and neonatal medulloblastoma (118).
Clinical vignette
A 2700 g girl was born at 37 weeks’ gestation to a 24-year-old healthy mother. On examination, she showed macrocephaly with head circumference of 37 cm (90 percentile) and generalized hypotonia with head drop. On day 3 she began episodes of cyanosis, rolling up of the eyes, and tonic spasms, unresponsive to phenobarbital. Her EEG showed continuous paroxysmal activity with asymmetric suppression-burst on the left. Her CT scan and MRI of the head showed overt asymmetry with enlargement of the left hemisphere, distorted ventricular system and corpus callosum on the same side, and severe cortical dysplasia, suggesting lissencephaly/pachygyria. A linear sebaceous nevus was noted in the midline of the forehead. Later she also developed asymmetric left infantile spasms unresponsive to phenobarbital, valproic acid, and vigabatrin. Her development was severely delayed; she did not have visual tracking, smile, or grasp. She developed hypertonia and adducted thumbs. She persisted in status epilepticus for several weeks. At 4 months of age, she underwent left anatomical hemispherectomy, but complications ensued during surgery, and she died during the procedure.
Midline epidermal nevus and intractable tonic spasms in an infant (video-EEG)
(A) A 1-month-old, term-infant girl with intractable tonic spasms since the second week of life and a midline epidermal nevus. CT and MR imaging studies demonstrated left hemimegalencephaly. The EEG shows a hemisuppression-burst p...