


Sleep Disorders
Sleep-related bruxism
Apr. 14, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Limb dystonia is a type of dystonia consisting of involuntary contractions of the arms or legs associated with abnormal posturing, repetitive movements, and functional impairment. In this article, the authors review current knowledge on limb dystonias. They review updates on the classification, genetics, and pathophysiology of limb dystonia. The main clinical features of limb dystonia together with advances in the etiology, pathogenesis, and treatment of limb dystonia are also reviewed.
|
• Dystonia is classified based on both clinical characteristics (age of onset, body distribution, temporal pattern, and associated clinical features) and etiology (underlying nervous system pathology: inherited, acquired, or idiopathic). | |
|
• Early-onset dystonia is rare, usually affects one or both lower limbs, and often generalizes, whereas adult-onset dystonia is relatively common, typically starts in the upper limbs, and remains focal. Up to 20% of all dystonias have an identifiable genetic cause. | |
|
• Writer’s cramp is the most common task-specific upper limb dystonia. | |
|
• Suspected secondary limb dystonias should prompt a search for structural brain lesions and heredo-metabolic causes (eg, Wilson disease or neurodegeneration with brain iron accumulation). | |
|
• Limb dystonia may be the initial presenting sign in neurodegenerative disorders like Parkinson disease, progressive supranuclear palsy, and corticobasal ganglionic degeneration. | |
|
• The pathophysiology of dystonia involves abnormal plasticity in the somatosensory cortex and a loss of inhibition at both spinal and cortical levels. Environmental factors, such as repetitive injury, also play a significant role. | |
|
• Limb dystonia is successfully treated with botulinum toxin injections or deep brain stimulation. |
The term dystonia is defined as a sustained, involuntary contraction of muscle that produces an abnormal posture and frequently causes twisting and turning. The task specificity and presence of sensory tricks make dystonia unique among other neurologic symptoms. In 1830, Charles Bell described hand dystonia in professional writers followed by Gowers’ description of dystonia in musicians. Oppenheimer described generalized dystonia in the early 20th century, naming it dystonia musculorum deformans (21). As dystonia is not a disease of muscle, the term primary torsion dystonia is now preferred (71). Over the last century, the classification of this disorder has evolved from a clinical characterization, such as focal, segmental, or generalized dystonia, to encompass a parallel molecular biological dimension with acknowledgement of affected chromosomal loci, mutated proteins, and biochemical dysfunctions. Currently, dystonia is classified based on both clinical characteristics (age of onset, body distribution, and temporal pattern), as well as etiology (associated with structural abnormalities—inherited, acquired, and idiopathic) (03). Until recently, inherited dystonias have been named using DYT acronym followed by a number (eg, DYT1). However, a new nomenclature was introduced so that only isolated genetic dystonias are designated “DYT” followed by the affected gene (eg, DYT-TOR1A, instead of DYT1). The combined dystonias will be named using a double prefix, including both dystonia and the associated phenotype (eg, DYT/PARK-TAF1, instead of DYT3).
Focal dystonia is defined as a dystonia with only one body region affected. Typical examples of focal forms are blepharospasm, oromandibular dystonia, cervical dystonia, laryngeal dystonia, and writer’s cramp.
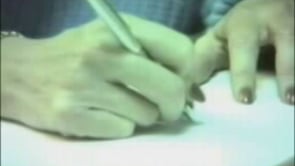
Writer's cramp, a task-specific and common dystonia of the hand, underscores many difficulties in the diagnosis of this disorder. Historically, patients may initially notice tightness or stiffness with writing prior to diminished writing speed and cramping with prolonged writing. The cramping of the hand will be present only with writing and will disappear almost immediately after stopping this activity. Physical examination of affected patients frequently reveals normal findings, except when performing certain tasks or adopting a certain posture. As a result of this, the condition was once thought to be of psychogenic origin (65). Fortunately, increasing electrophysiological studies and documentation of abnormal findings in patients with limb dystonia have improved the acceptance of this disorder as one resulting from neurologic mechanisms (27; 09).
Limb dystonia consists of sustained, repetitive, and patterned contractions of muscles producing an abnormal posture of the upper or lower limb that may be present at rest, when changing position, or when performing a specific motor activity.
Focal, segmental, and generalized dystonic disorders may produce limb dystonia, and are increasingly related to genetic abnormalities. Involvement of the upper extremity is most often associated with "writer’s cramp," a task-specific, focal dystonia, and may evolve from a dystonia triggered by a single activity to one triggered by multiple other activities to one also present at rest. In adult-onset limb dystonia, the dystonia usually remains confined to the originally affected location; however, an initial presentation below 18 years of age or with bilateral lower extremity onset is usually associated with progression to generalized dystonia.
Writer’s cramp postures may produce any combination of finger flexion or extension, wrist flexion or extension, and elbow flexion.
Although symptoms of dystonia disappear with sleep, patients with limb contractures will not have diminished limb tone at this time. In addition to dystonic muscle contraction from sustained agonist and antagonist muscle contraction, less sustained, rhythmic alteration of agonist and antagonist pairs may produce hand tremor. Classification of "primary writing tremor" as a dystonic or tremor disorder remains controversial (53).
Patients with extensor muscle involvement may report increasing difficulty putting the pen on paper, the thumb or fingers lifting off the pen, and a need to lean further and further towards the writing surface to compensate for wrist. In this instance, a faint script may be noted, as the patient has difficulty maintaining contact between the pen and paper. Conversely, a flexor type writer’s cramp will produce bold and illegible script. Flexion of the fingers produces the illegibility by decreasing ability to produce space between letters and loops, whereas wrist flexion increases the boldness of the script. In either situation, patients may adopt a printing style of handwriting, perhaps to allow for each letter to become a discreet component, instead of using more prolonged sequences of activity.
Occupational dystonia is a term used to describe patients with dystonic muscle contractions producing employment disability. Occupations most often associated with these disorders are associated with chronic, stereotyped movements of the hands and fingers. Typists, stenographers, musicians, blackjack dealers, dentists, and surgeons have been reported to have this condition.
Rosenkranz and colleagues suggest that different mechanisms may be involved in writers, who use their hands no more than the average worker, and in musicians, where there is prolonged, repetitive use of the hands (61). Similar sports-related dystonias have also been reported in trap shooters, darts players, and golfers. The sudden jerk-like movement of the extensor muscles of the lead forearm, when moving the club toward the ball when putting, is in golfer’s terminology, the "yips" (18). A summary of this phenomenon by Smith and colleagues found that this phenomenon usually affected low-handicap golfers in their mid-40s, usually after 20 to 30 years of golf participation at a frequency greater than 75 rounds annually (70). Adler and colleagues report that yips-affected golfers usually have had greater exposure to the sport (37.6 vs. 25.9 years, p=0.03) and are better players (handicap 3.5 vs. 6.3, p=0.01) than nonaffected golfers (01).
Limb dystonia involving the legs usually produces knee extension, plantar flexion, and toe flexion, but may involve any leg muscle. The appearance of a spontaneously dorsiextended big toe may also be seen within the context of limb dystonia ("Babinski dystonia"-also known as striatal toe). Leg dystonia, in patients beyond 30 years of age, should prompt concern for idiopathic Parkinson disease. However, primary adult-onset focal lower extremity dystonia has been reported (64; 53). In children, the development of this posture may represent the initial onset of primary torsion dystonia or dopa-responsive dystonia.
The most significant prognostic indicator in limb dystonia is age of onset. Patients reporting the onset of symptoms, prior to the age of 18, are much more likely to develop generalized dystonia.
Usually, complications of limb dystonia are related to musculoskeletal changes in the affected extremity. In the leg tendon, contracture may lead to foot eversion or inversion, foot shortening, or Achilles tendon shortening that causes increasing gait disability. Involvement of the forearm and hand may also lead to tendon contracture, but also produces median and ulnar nerve entrapment symptoms.
The first subject was a 15-year-old girl who was referred to a psychologist for poor school performance attributed to oppositional defiance disorder; she would not complete her writing assignments. The patient presented with her mother and reported difficulty with writing since first or second grade. She remembers being corrected for her poor handwriting posture by almost all of her elementary teachers, but could not make adjustments to hold the pen or pencil correctly. Several attempts at writing implement modifications also did not help. The remainder of her neurologic examination and further, limited work-up at the time were unremarkable. She was given the diagnosis of writer’s cramp and became successful with minor modification of her in-class work and the use of a home computer to complete her assignments.
The second subject was a 70-year old woman with a history of mild hypertension and a previous small, left putamen infarction. She was hospitalized for mild weakness that resolved satisfactorily within several days. Her work-up was otherwise negative, and she began taking 325 mg of aspirin daily. During the 8 months after discharge, she developed right great toe extension, toe abduction and increased plantar arch. She responded to botulinum toxin A or Botox(r) injection of 50 units to the extensor hallucis longus muscle and 30 units to her flexor hallucis brevis muscle.
Until recently, limb dystonia has been classified as primary or secondary based on etiology. Primary limb dystonia refers to a syndrome where dystonia is the only neurologic finding with the exception of tremor. Secondary dystonia refers to a dystonic syndrome with an identifiable cause and is frequently accompanied by other neurologic signs (ie, cognitive dysfunction, pyramidal tract signs, visual disturbances). An update in the classification changed the terminology from primary and secondary to isolated dystonia (dystonia is the only motor feature with the exception of tremor) and combined dystonia (dystonia with other movement disorders associated). Axis I off this classification focuses on the clinical characteristics of dystonia (age at dystonia onset, body distribution, and temporal pattern), whereas axis II focuses on etiology: dystonia associated with structural abnormalities, inherited, acquired, and idiopathic (03; 22).
Axis I: clinical features | ||
• Age at onset: | ||
- Infancy (birth to 2 years) | ||
• Body distribution | ||
- Focal (one isolated body region) | ||
• Temporal pattern: | ||
- Disease course (static vs. progressive) | ||
• Associated features: | ||
- Isolated (with or without tremor) | ||
Axis II: etiology | ||
• Nervous system pathology | ||
- Degenerative | ||
• Heritability | ||
- Inherited (eg, sex linked or autosomal, dominant or recessive, or mitochondrial) | ||
• Idiopathic | ||
- Sporadic | ||
Dystonias have been associated with genetic mutation in up to 19% of cases in a exome wide sequencing study of 728 families (82). Early-onset primary limb dystonia is rare, often genetic, and typically starts in one or both lower extremities, eventually generalizing. DYT1 dystonia (DYT-TOR1A) is the most frequent early-onset genetic limb dystonia and is caused by a GAG deletion in the TOR1 gene. In contrast to DYT1 dystonia, DYT6 dystonia (DYT-THAP1) is characterized by onset in cranial-cervical and laryngeal areas, but it also tends to generalize. Other genetic forms of dystonia involving the limb have been designated as DYT4 (DYT-TUB4A); DYT5 (DYT-GCH1), dopa-responsive dystonia; DYT11 (DYT-SGCE), myoclonus dystonia; or DYT12 (DYT-ATP1A3), rapidly progressive dystonia and parkinsonism.
In spite of growing evidence for the genetic inheritance of dystonia, the vast majority of cases of focal primary dystonia are sporadic, with no definite genetic factor having been identified. The current known genes that produce primary dystonia are summarized in Table 21. Whole-exome sequencing revealed several new genes that have been strongly associated with segmental dystonia: TUB4 (DYT4), CIZ1 (DYT23), ANO3 (DYT24), GNAL (DYT25), and ATP1A2 (DYT27). A couple of newly identified genes have been linked with dystonia: PRKRA, TAF1, KMT2B, VPS16, and VAC14 HPCA (35; 05; 30). EIF2AK and AOPEP have been shown to cause isolated dystonia (76).
DYT1-TOR1 (Oppenheim dystonia; DYT1) | |
• Location: 9q34 (GAG deletion); Torsin A | |
DYT-HPCA (DYT2) | |
• Location: 1p35.1 | |
DYT-TAF1 (Lubag; DYT3) | |
• Location: Xq13.1, TAF1 | |
DYT-TUB4A (DYT4) | |
• Location: 19p.13.12-13, TUBB4a | |
DYT-GCH1 (Segawa disease; DYT5/DYT14) | |
• Location: 14q22.1, GTP cyclohydrolase 1 (DYT5a) and 11p11.5 tyrosine hydroxylase (DYT5b) | |
DYT-THAP1 (DYT6) | |
• Location: 8p21-p22, THAP1 | |
DYT7 | |
• Location: 18p | |
DYT-MR1 (DYT8) | |
• Location: 2q34, MR1 (myofibrillogenesis regulator 1) | |
DYT-SLC2A1 (DYT9) | |
• Location: 1p21, SLC2A1 | |
DYT-PRRT2 (DYT10) | |
• Location: 16p11.2-q12.1, PRRT2 | |
DYT-SGCE (myoclonus dystonia; DYT11) | |
• Location: 7q21, SGCE, epilson sarcoglycan | |
DYT-ATP1A3 (DYT12) | |
• Location: 19q13, ATP1A3 | |
DYT13 | |
• Location: 1p36.13-32 | |
DYT15 | |
• Location: 18p11 | |
DYT16 (PRKRA) | |
• Location: 2q31.2, stress response protein PRKRA | |
DYT17 | |
• Location: 20p11.2-q13.12 | |
DYT-SLC2A1 (DYT18) | |
• Location: 1p35-p31.3 SLC2A1 gene- GLUT1 | |
DYT19 | |
• Location: 16q13-q22 | |
DYT20 | |
• Location: 2q31 | |
DYT-CIZ1 (DYT23) | |
• Location: 9q34 CIZ1 | |
DYT-ANO3 (DYT24) | |
• Location: 11p14.2 ANO3 | |
DYT-GNAL (DYT25) | |
• Location: 18p11.21 | |
DYT-KCTD17 (DYT26) | |
• Location: 22q12.3 | |
DYT-ATP1A2 (DYT27) | |
• Location: 2q37.3 COL 6A3 | |
DYT- KMT2B (DYT28) | |
• Location: 19p13 | |
DYT MECR(DYT 29) | |
• Location: 1p35 | |
DYT- VPS16 (DYT30) | |
• Location: 20p13 | |
| |
Idiopathic (primary) dystonia | |||
Sporadic (idiopathic torsion dystonia, ITD) | |||
Inherited (hereditary torsion dystonia) | |||
• Autosomal dominant ITD (DYT1TOR1, DYT-GCH1, DYT-THAP1, DYT-ATP1A3) | |||
Secondary dystonia | |||
Dystonia-plus syndromes | |||
• Myoclonus dystonia | |||
Associated with neurodegenerative and dymyelinating disorders | |||
• Sporadic | |||
- Parkinson disease | |||
• Inherited | |||
- Huntington disease | |||
Associated with metabolic disorders | |||
• Amino acid disorders | |||
- Glutamic acidemia | |||
• Lipid disorders | |||
- Metachromatic leukodystrophy | |||
• Miscellaneous metabolic disorders | |||
- Wilson disease | |||
Due to a known specific cause | |||
• Perinatal cerebral injury and kernicterus (athetoid cerebral palsy, delayed onset dystonia) | |||
Other hyperkinetic syndromes associated with dystonia | |||
Tic disorders with dystonic tics | |||
Paroxysmal dyskinesias | |||
• Paroxysmal kinesigenic choreoathetosis | |||
Psychogenic | |||
Pseudodystonia | |||
Atlantoaxial subluxation | |||
| |||
Adult-onset primary limb dystonia affects mainly the upper limb, whereas lower limb involvement is uncommon (41). Musician dystonia has been linked with arylsulfatase G (ARSG) gene locus (36). A systematic review found that KMT2B mutation carriers frequently present with the lower limb dystonia, whereas TOR1A, PRKRA, and HPCA were frequently observed in both upper and lower ones (33). Similarly, THAP1 and ANO3 patients manifest in the upper half of the body (upper limb, neck), whereas onset in GNAL mutations present with neck dystonia.
Limb dystonia may be present, isolated, or in association with dystonia plus syndromes. In dopa-responsive dystonia (DRDDYT GCH1, DYT 5), dystonic posturing of lower extremities is often present together with parkinsonian features. The most common cause of dopa-responsive dystonia is Segawa disease, an autosomal dominant disorder due to mutation in the GTP cyclohydrolase 1 gene followed by an autosomal recessive form related to mutation of the tyrosine hydroxylase gene. More than 100 mutations have been described in the GCH1 gene, and clinical presentations are heterogeneous with dystonia, parkinsonism, and mood disorders.
Myoclonus-dystonia (DYT-SGCE, DYT 11) is an autosomal dominant disease that presents with myoclonic jerks of the arms with focal or segmental dystonia and is related to mutations in the epsilon sarcoglycan gene. More than 80 mutations have been described, causing dystonia and myoclonus in childhood or adolescence and frequently associated with psychiatric disorders (42).
In rapid-onset dystonia parkinsonism (DYT-ATP1A3, DYT12), the typical presenting symptom is upper limb dystonia with acute onset. More than 20 mutations have been described and associated with a variety of clinical presentations (35).
The common biological pathways affected in the etiology of dystonia are defects in dopamine signaling, metabolic abnormalities, heavy metal storage, dysregulation of ion channels, abnormal gene regulation, and mitochondrial dysfunction (29).
Secondary dystonias are rare, with a prevalence of 7 in 100,000 (51). Secondary limb dystonias may be due to structural brain lesions. Putaminal lesions often produce limb dystonia or hemidystonia whereas thalamic lesions produce mainly hand dystonia (52; 07).
Extrapyramidal syndromes, such as Wilson disease, Parkinson disease, progressive supranuclear palsy, and multiple system atrophy, may be associated with limb dystonia. Parkinson disease may present with symptoms of lower limb dystonia. Patients with progressive supranuclear palsy often present with dystonic muscle contraction of the axial muscles, and some patients with corticobasal degeneration will exhibit profound limb dystonia in addition to, and sometimes masking, symptoms of the "alien-limb" phenomenon. Limb dystonia with diurnal fluctuations may be caused by dopa-responsive dystonia. Paroxysmal dystonias in the limbs may be observed in paroxysmal kinesogenic and dystonic choreoathetosis. Tonic spasms of multiple sclerosis are typically transient attacks of hemidystonia of the limbs. Reported secondary causes of dystonia include exposure to DA receptor-blocking drugs ("tardive dystonia"), hypoxic encephalopathy, head trauma, encephalitis, human immunodeficiency virus and other infections, peripheral or segmental nerve injury, reflex sympathetic dystrophy, inherited disorders (eg, Wilson disease), metabolic disorders and other inborn errors of metabolism, mitochondrial disorders, and chromosomal abnormalities (See Table 3).
Central nervous system lesions are well recognized as causes of limb dystonia. Chuang and colleagues (07) reviewed 190 cases of hemidystonia and found the most common etiologies of hemidystonia to be stroke, trauma, and perinatal injury. Mean age of onset was 20 years to 25.7 years, and the average latency from insult to dystonia was 2.8 years to 4.1 years. Basal ganglia lesions were seen in almost 50% of patients with the putamen most commonly involved. Cerebral infarction in the posterolateral thalamic nuclei may be associated with contralateral hand dystonia, and large lenticular or caudo-capsulo-lenticular lesions may give rise to foot dystonia (52). Other structural abnormalities associated with limb dystonia include cavernous angioma of the basal ganglia (37), subdural hematoma (19), left frontal meningioma (44), calcification of the head of the right caudate nucleus (43), and cervical cord lesion secondary to multiple sclerosis (78). Movement disorders after severe head injury have been reported in 13% to 66% of patients (31).
Most of our understanding of the mechanisms of dystonia comes from focal hand dystonia studies (72). Task-specific dystonia is considered to be due to a combination of environmental factors and individual vulnerability. The environmental factors like peripheral injury or repetitive use together with abnormal mechanisms of plasticity have been invoked in the pathophysiology of dystonia (54). Some of the best-studied mechanisms include reduced inhibition at cortical, subcortical, and spinal levels, abnormalities of sensory-motor integration, and maladaptive plasticity (34; 20). Writer's cramp is a task-specific dystonia that leads to involuntary hand postures during writing. Physiologically, co-activation of antagonistic groups of muscles in the upper limb muscles is seen during dystonic muscle activity (27; 10), and the impaired antagonist muscle relaxation may be impaired as a result of reduced reciprocal inhibition of H reflexes (48).
The understanding of dystonia pathophysiology has progressed with the advances in electrophysiologic and neuroimaging techniques. These studies have linked dystonia with malfunction in the basal ganglia, sensorimotor network, and cerebello-thalamo-cortical pathway (50). fMRI and PET studies revealed functional abnormalities in patients with dystonia in the primary motor area, supplementary motor area, dorsal premotor cortex, basal ganglia, and sensorimotor areas. Electrophysiological studies using transcranial magnetic stimulation have identified abnormal neurophysiologic changes in the basal ganglia, the sensorimotor cortex, and, more recently, the cerebellum. These changes include: 1) loss of inhibition at multiple levels in the CNS with resulting excess movement, 2) an impairment of somatosensory processing and sensorimotor integration, and 3) maladaptive plasticity of sensorimotor circuits (56).
There is evidence of abnormal inhibition in the nervous system at multiple levels: lack of reciprocal inhibition at the spinal level, abnormal inhibition at the cortical level as measured by transcranial magnetic stimulation, and abnormal surround inhibition as a result of impaired GABA interneurons (34; 54; 12).
The mechanism of impaired motor regulation is unknown but may relate to abnormal cortical sensory processing. Functional neuroimaging studies suggest that somatosensory receptive fields are abnormally enlarged and disorganized in patients with focal hand dystonia, and spatial discrimination is abnormal. These abnormalities in the cortical sensory processing may lead to defective sensorimotor integration (34).
Another mechanism involved in dystonia pathophysiology is the altered plasticity. The nervous system uses plasticity as a mean to adapt flexibly to changes required in a dynamic environment and to facilitate learning and memory. Abnormally enhanced plasticity was demonstrated in patients with dystonia, suggesting that maladaptive plasticity associated with repetitive hand use modulates sensory motor maps and induces dystonia (81).
Dystonia is the third most frequent movement disorder after essential tremor and Parkinson disease. The prevalence of early-onset dystonia (before 26 years of age) is reported to be 3 to 50 per million whereas adult-onset dystonia has a much higher prevalence of up to 7,320 per million in one study (14).The prevalence of focal dystonia per 100,000 population has been reported as 14.4 in Japan (75), 29.5 in the United States (51), and 40 in India (13). In Europe, the prevalence of focal dystonia was reported as 11.7 per 100,000 compared to 3.5 for generalized dystonia. Among focal dystonia, cervical dystonia is the most common focal dystonia with a prevalence of 5.0 per 100,000, followed by blepharospasm with 4.2 per 100,000 (73). A review of the existing studies on adult-onset dystonia estimated the prevalence to vary from 2.7 to 71.2 per 100,000 (15).
Although repetitive training and peripheral injury has been suggested to play a role in some of the limb dystonias, genetic predisposition is probably even more important (58). Although the genetic factors that may predispose to maladaptive plasticity and subsequent interference with the motor tasks cannot be modified, the avoidance of repetitive behavior or peripheral injuries is attainable. On the basis of various current pathophysiology theories for task-specific dystonia, different sensory and motor training therapies for task-specific dystonia that selectively activate certain muscles have been proposed (83).
With regards to the prevention of musician dystonia, exaggerated perfectionism and anxiety as triggering factors have been identified as possible tigers of dystonia and should be addressed in the education of musicians (04). However, in most cases of musician’s dystonia, no particular predisposition is found (28).
Limb dystonia diagnosis is frequently misdiagnosed as essential tremor, myoclonus, scoliosis, or functional dystonia. Hand dystonia may sometimes resemble carpal tunnel syndrome; however, muscle weakness, wasting, and sensory impairment are not present in the former condition. Differentiating dystonia from parkinsonism can challenging because Parkinson disease can present with limb dystonia. The presence of a task specific tremor or position-specific tremor and lack of improvement with dopaminergic therapy would imply dystonia. Other diagnoses such as "tennis elbow," muscle strain, muscle cramp, fasciitis, arthritis, and reflex sympathetic dystrophy may present with abnormal posturing of limbs. Typically in this condition pain is prominent, and a preceding history of local injury is common.
The diagnosis of primary dystonia should be considered in any patient with an abnormal posture and a family history of cramps, spasms, tremor, and crippling conditions. Information concerning age at onset, initial and subsequent areas of involvement, course and progression, tremor or other movement disorders, possible birth injury, developmental milestones, and exposure to neuroleptic medications as well as a family history of dystonia, parkinsonism, or other movement disorders should be reviewed. As phenotypic expression of dystonia is highly varied in this population, extreme care should be taken in recording family data, with particular attention to consanguinity or genetic background. Evidence of other conditions known to produce dystonia, but associated with other neurologic dysfunctions (eg, cognitive, pyramidal, sensory, or cerebellar deficits) should be evaluated along with secondary causes of dystonia. Ceruloplasmin should be obtained in all patients under the age of 50. Genetic testing should be done in all patients with early-onset limb dystonia (02). Blood sample for genetic assessment, storage diseases, and metabolic disorders should be evaluated individually. Electromyography may be performed if carpal tunnel syndrome is suspected as a complication of the dystonia. Imaging of the brain (MRI or CT scan) should be performed in adult-onset patients with a short history of limb dystonia to screen for secondary forms of dystonia. F-DOPA scans are useful to differentiate between dopa-responsive dystonia and juvenile Parkinson disease presenting with dystonia.
Therapy of dystonia can be classified in the following categories: (1) pharmacologic treatment, (2) chemodenervation with botulinum toxin, (3) surgical (deep brain stimulation), and (4) physical therapy.
Anticholinergic drugs are effective in most types of dystonia but especially in the focal dystonia. Trihexyphenidyl and benztropine can be used with variable degree of efficacy. Side effects are numerous and include dryness of the mouth, constipation, urinary retention, aggravation of glaucoma, blurred vision, and drowsiness (32). In some patients with a component of tremor, beta-blocking agents may be useful (60). Baclofen or tizanidine are commonly used in treating symptoms of dystonia and may be most appropriate in patients with a history of hypoxic or traumatic brain injury. Benzodiazepines, particularly if patients report sleep difficulty, are useful as adjunct therapy. In one series of 190 patients, approximately one-third of patients experienced some benefit from medical therapy, and included anticholinergics, benzodiazepines, clonazepam, and diazepam (07). Other muscle relaxants with possible beneficial effects for muscular pain in dystonia include cyclobenzaprine, methocarbamol, orphenadrine, or chlorzoxazone. Tetrabenazine, a dopamine depleting drug, has been used in patients with dystonia, particularly those with tardive dystonia, and it represents another option for those patients that do not respond to anticholinergics. Dopaminergic therapy should be used if dopa responsive dystonia is suspected. In paroxysmal kinesigenic dyskinesias, carbamazepine in low dose is frequently highly effective.
When medical treatment is failing, botulinum toxin is usually the most effective treatment in focal dystonia (38; 23). Botulinum toxin injections are highly effective in the treatment of limb dystonia (11). The American Academy of Neurology concluded in 2008 that botulinum toxin should be offered for focal upper extremity dystonia (level B evidence) and can be considered for lower limb dystonia (level C) (66). An appraisal of the evidence available for use of botulinum toxin in limb dystonia supported a level B recommendation for both abobotulinumtoxinA and onabotulinumtoxinA (24; 67). DaxibotulinumtoxinA is a novel toxin that is now being studied in cervical dystonia and may provide a longer duration of action.
Injection strategy is determined by a combination of functional observation, muscle palpation, ultrasound guidance, and electrophysiologic assessment. Muscle identification methods vary from clinician to clinician. Examples include using mirror dystonia as guidance (68; 69) in addition to plain observation of the dystonic posture while performing the task. Data confirming the additional benefit of electromyographic guidance or electrical stimulation remain controversial (45; 06), and functional benefit may be a combination of chemodenervation of muscle fibers as well as intrafusal fibers. Prolonged benefit in subjects with writer’s cramp has been associated with delayed recovery of the tonic vibration reflex, perhaps indicating a physiologic alteration of intrafusal-fiber-mediated sensorimotor integration (77). Because approximately 20% of patients will eventually stop the botulinum injections due to treatment failure it was proposed that ultrasound guidance or electromyography be used in these patients (39).
Because focal hand dystonia is difficult to treat pharmacologically and the injections with botulinum toxin can be challenging, alternative treatments are necessary. Based on the identification of impaired plasticity in the somatosensory cortex of dystonia patients, several rehabilitation techniques have been proposed, such as limb or finger immobilization and sensory motor retraining (84). Advances in our understanding of the pathophysiology of dystonia have led to new treatment strategies, including behavioral training strategies and noninvasive brain stimulation techniques (08).
Transcranial magnetic stimulation has been used in writer’s cramp as a therapeutic approach (47). TMS can be used as a therapeutic tool to treat focal hand dystonia when pharmacological options or injections of botulinum toxin are ineffective (56; 59). Sensorimotor training in conjunction with transcranial direct current stimulation seems to be effective in task-specific dystonia (62; 55).
In a study of 54 pianists with musician’s dystonia, the following multiple therapies have been tried: retraining (87%), hand therapy (42%), relaxation techniques (38%), physiotherapy (30%), psychotherapy (23%), acupuncture (21%) and body techniques (21%); 81.5% reported improvement, and 5.6% reported complete recovery, but only 43% had objective evidence of improvement in task-specific motor performance (79).
Deep brain stimulation (DBS) should be considered in patients with disabling limb dystonia refractory to medical or botulinum toxin treatment (31). Most often, this therapy is considered in patients with generalized or posttraumatic dystonia; however, patients with segmental or focal dystonia may benefit as well. Many studies have identified GPI as the target of choice for dystonia (16), and controlled studies showed that deep brain stimulation of GPI is efficient in treating dystonia and efficacious 5 years after the surgery (80). In a study of 15 patients with musician’s dystonia who were followed for an average of 2.5 years (up to about 9 years) following ventro-oral thalamotomy, all patients except one (93%) experienced marked improvement in symptoms without deterioration during the follow-up period (25). In a systematic review of 523 patients from 24 studies, the improvement in Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) motor score after GPI deep brain stimulation in idiopathic dystonia was 65.2% (46). Isolated general dystonia, younger age of onset, normal MRI, and no other coexistent movement disorders were associated with better outcomes (74).
Besides deep brain stimulation, lesioning techniques such as MR-guided focused ultrasound have been used with benefit successfully in patients with task specific dystonia (26).
Pregnancy is not known to affect the symptoms of limb dystonia.
Anesthesia does not affect the course of limb dystonia.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Corneliu Luca MD PhD
Dr. Luca of the University of Miami received consulting fees from Abbott, Boston Scientific, and Medtronic.
See ProfileCarlos Singer MD
Dr. Singer of the University of Miami School of Medicine has no relevant financial relationships to disclose.
See Profile
Robert Fekete MD
Dr. Fekete of New York Medical College received consultation fees from Acadia Pharmaceutical, Acorda, Adamas/Supernus Pharmaceuticals, Amneal/Impax, Kyowa Kirin, Lundbeck Inc., Neurocrine Inc., and Teva Pharmaceutical, Inc.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Apr. 14, 2024
Movement Disorders
Mar. 24, 2024
Movement Disorders
Mar. 18, 2024
Sleep Disorders
Mar. 13, 2024
Movement Disorders
Mar. 08, 2024
Movement Disorders
Mar. 06, 2024
Movement Disorders
Mar. 06, 2024
Movement Disorders
Mar. 06, 2024