














































Behavioral & Cognitive Disorders
Academic underachievement
Apr. 18, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author explains the clinical presentation, pathophysiology, diagnostic workup, and management of meningococcal meningitis. Meningococcal meningitis may be indistinguishable from other bacterial meningitides, although the classic triad of fever, neck stiffness, and change in mental status is significantly less common in patients with meningococcal meningitis (27%) than in patients with pneumococcal meningitis (58%). Although less than one third of affected patients present with the classic triad of fever, nuchal rigidity, and change in mental status, nearly 90% have at least two of the following four signs on presentation: fever, nuchal rigidity, change in mental status, and rash. Guidelines for use of the various meningococcal vaccines are summarized.
|
• Meningococcemia presents abruptly with fever, chills, nausea, vomiting, headache, myalgias, malaise, prostration, and rash. Rash is somewhat variable and may be urticarial, maculopapular, or petechial. | |
|
• Acute fulminating cases of meningococcal septicemia (Waterhouse-Friderichsen syndrome) occur mainly in children younger than 10 years of age and are characterized by vomiting, diarrhea, extensive purpura, disseminated intravascular coagulation, cyanosis, convulsions, shock, coma, and often death within hours despite appropriate treatment; many of these cases have meningitis and adrenal insufficiency with hemorrhage into the adrenal glands or adrenal infarction. | |
|
• Meningococcal meningitis may be indistinguishable from other bacterial meningitides, although the classic triad of fever, neck stiffness, and change in mental status is significantly less common in patients with meningococcal meningitis (27%) than in patients with pneumococcal meningitis (58%). | |
|
• Although less than one third of affected patients present with the classic triad of fever, nuchal rigidity, and change in mental status, nearly 90% have at least two of the following four signs on presentation: fever, nuchal rigidity, change in mental status, and rash. | |
|
• The strains of Neisseria meningitidis most commonly implicated in systemic disease are A, B, C, W, and Y. In the United States, groups B, C, and Y are the most common serogroups implicated, and each account for about 30% of reported cases. | |
|
• North American outbreaks (as opposed to isolated cases) are confined primarily to serogroup C (less commonly to Y and W), although the frequency of serogroup Y outbreaks increased markedly during the 1990s. | |
|
• Although disease rates are highest among children younger than 2 years of age, almost two thirds of meningococcal disease in the United States occurs in those older than 10 years. Most cases (95% to 98%) are sporadic. However, meningococcal disease outbreaks have been occurring with increasing frequency in the United States. | |
|
• Meningococcal disease outbreaks are particularly likely to occur in semi-closed communities, such as daycare centers, schools, colleges, nursing homes, and military recruit camps. | |
|
• Almost all secondary cases in an outbreak occur within 8 days of the index case. | |
|
• The U.S. Centers for Disease Control and Prevention recommends routine vaccination with quadrivalent meningococcal conjugate vaccine of adolescents 11 to 18 years of age and vaccination of persons 2 to 55 years of age who have an increased risk of invasive meningococcal disease. | |
|
• The case-fatality ratio for meningococcal disease is approximately 10%, and 11% to 26% of survivors have serious sequelae, including neurologic disability (eg, focal neurologic deficits, seizures, etc.), limb loss, and deafness. | |
|
• Because of the risks of severe morbidity and death, appropriate antibiotic therapy should be rapidly initiated in patients suspected of having meningococcal disease. Before confirmation of meningococcal disease as the cause of the illness, empiric antibiotic coverage should be directed at the most likely pathogens based on epidemiologic considerations (eg, age, geographic location, etc.) and the known prevalence of antibiotic resistance for these organisms. No investigations should delay initiating antibiotic therapy once the diagnosis of meningococcal meningitis is suspected. | |
|
• Children who have suspected bacterial meningitis or meningococcal disease should be immediately treated with intravenous ceftriaxone, with the addition of amoxicillin or ampicillin for children younger than 3 months and the addition of vancomycin for those who have recently traveled outside of the country or who have had prolonged or multiple exposures to antibiotics. | |
|
• Recommendations for initial empiric antimicrobial therapy in adults with community-acquired bacterial meningitis are vancomycin plus a third-generation cephalosporin (eg, cefotaxime or ceftriaxone) for those aged 16 to 50 years and vancomycin plus a third-generation cephalosporin plus ampicillin for those older than 50 years, or for those with alcoholism or altered immune status. Generally, combination therapy should be continued until in vitro susceptibility testing results are available. |
Neisseria is a large genus of bacteria that colonize the mucosal surfaces of many animals. The genus is named after German physician Albert Ludwig Sigesmund Neisser (1885-1916), who discovered Neisseria gonorrhoeae in 1879. Of the 11 species of Neisseria that colonize humans, only two are pathogens: N. meningitidis (meningococcus) and N. gonorrhoeae. Neisseria species are gram-negative bacteria included among the proteobacteria. N. meningitidis is an aerobic or facultative anaerobic, non-motile, gram-negative, diplococcal bacterium that exclusively infects humans. Neisseria diplococci resemble coffee beans when viewed microscopically.
Meningococcal disease was first described by Geneva physician Gaspard Vieusseux (1746-1814) during an outbreak in Geneva in 1805. Another outbreak was described in 1806 in New Bedford, Massachusetts by Lothario Danielson (1765-1841), a Revolutionary War veteran, and Elias Mann (1778-1807). In 1884, Italian pathologists Ettore Marchiafava (1847-1935) and Angelo Celli (1886-1914) described intracellular micrococci in cerebrospinal fluid. In 1887, Austrian pathologist and bacteriologist Anton Wiechselbaum (1845-1920), working in Vienna, identified the meningococcus (designated as Diplococcus intracellularis meningitidis) in cerebrospinal fluid and established the connection between the organism and epidemic meningitis.
Wiechselbaum identified the meningococcus (designated as Diplococcus intracellularis meningitidis) in cerebrospinal fluid and established the connection between the organism and epidemic meningitis. (Courtesy of the U.S. Nation...
At the beginning of the twentieth century, the meningococcus was recognized as a habitant of the nasopharynx of healthy individuals, particularly at camps for military recruits.
Serum therapy was developed by German physiologist Emil von Behring (1854-1917) and German physician-scientist Paul Ehrlich (1854-1915) in the late 19th century to treat diphtheria. They had produced their diphtheria serum by repeatedly injecting the bacterial toxin into a horse. The serum was then used effectively during an epidemic in Germany. A chemical company offered a contract to both men, but Behring took the considerable financial rewards for himself. Behring was controversially awarded a solo Nobel Prize in Physiology or Medicine for this in 1901, but Ehrlich earned the 1908 Nobel Prize in Physiology or Medicine for his contributions to immunology. Commercial production of diphtheria serum depended at the time on injecting an increasing number of horses with the toxin to supply demand for the serum, which resulted in caricatures of the process in the mass media of the time (albeit inappropriately crediting Behring as the sole developer.
The development of serum therapy paved the way for its application to meningococcal disease. Several investigators reported beneficial effects of serum therapy in animals from 1905 to 1907, and some among these began human experiments. An early effective serum therapy for meningococcal disease was introduced by Simon Flexner (1863-1946) at the Rockefeller Institute for Medical Research (where he was the director).
Sulfonamides were introduced in 1937, but the emergence of resistance to sulfonamides in the 1960s stimulated the development of the first vaccines against meningococci.
In the first decade of the 20th century, untreated meningococcal meningitis had a case-fatality rate of 70% to 80% (171; 190). Following the introduction of intrathecal equine meningococcal antiserum in 1913, the case-fatality rate dropped to 20% to 31% by the late 1920s and early 1930s (190). In the 1930s, with the introduction of sulfonamides, the case-fatality rate dropped to 5% to 15%. Later therapies included high-dose penicillin and third-generation cephalosporins, but the case-fatality rate has generally stayed around 6% to 14% (37; 20; 31; 190; 206; 17; 147; 185; 105; 149; 179; 182).
Meningococcal meningitis continues to be a major cause of morbidity and mortality around the world and a significant contributor to healthcare costs, even in developed countries (147; 09; 62).
|
• Invasive meningococcal disease most commonly presents with meningitis or meningococcemia, which may rapidly progress to purpura fulminans, shock, and death. | |
|
• Meningococcemia presents abruptly with fever, chills, nausea, vomiting, headache, myalgias, breathing difficulty, malaise, prostration, and rash. | |
|
• Acute fulminating cases of meningococcal septicemia (Waterhouse-Friderichsen syndrome) occur mainly in children younger than 10 years of age and are characterized by vomiting, diarrhea, extensive purpura, disseminated intravascular coagulation, cyanosis, convulsions, shock, coma, and often death within hours despite appropriate treatment; many of these cases have meningitis and adrenal insufficiency with hemorrhage into the adrenal glands or adrenal infarction. | |
|
• Meningococcal meningitis may be indistinguishable from other bacterial meningitides, although the classic triad of fever, neck stiffness, and change in mental status is significantly less common in patients with meningococcal meningitis than in patients with pneumococcal meningitis. | |
|
• Most children with meningococcal meningitis have only nonspecific symptoms in the first 4 to 6 hours but may be close to death by 24 hours after onset. |
Invasive meningococcal disease most commonly presents with meningitis or meningococcemia, which may rapidly progress to purpura fulminans, shock, and death (34; 20). In a French study of invasive meningococcal disease spanning the years 2014 to 2016, most adult cases presented as meningococcal meningitis (59%), whereas the remainder presented with meningococcemia (25%), both (9%), or other and unspecified (7%) (98).
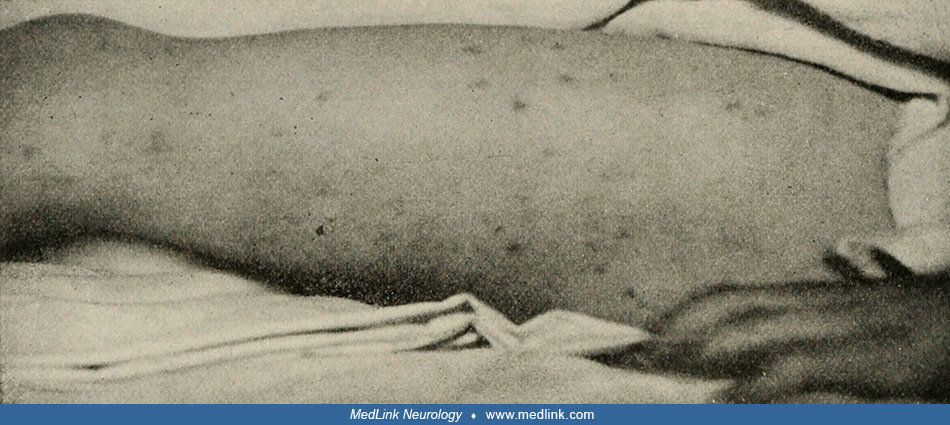
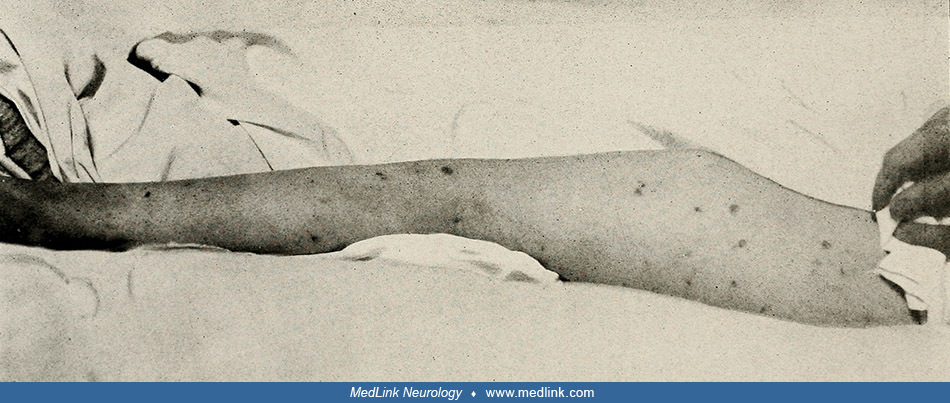
Meningococcemia may present abruptly with fever, chills, nausea, vomiting, headache, myalgias, breathing difficulty, malaise, prostration, and rash. Rash is non-blanching but somewhat variable and may be urticarial, maculopapular, or petechial. In darker-skinned people, rash may be less evident, so it is important to check the soles of the feet, the palms, and the conjunctivas (211). Limb pain with pale or cyanotic, cold extremities, hypotension, tachycardia, and prolonged capillary refill are clinical features that indicate impending shock (211). Acute fulminating cases of meningococcal septicemia (Waterhouse-Friderichsen syndrome) occur mainly in children younger than 10 years of age and are characterized by vomiting, diarrhea, extensive purpura, disseminated intravascular coagulation, cyanosis, convulsions, shock, coma, and often death within hours despite appropriate treatment; many of these cases have meningitis and adrenal insufficiency with hemorrhage into the adrenal glands or adrenal infarction.
At initial contact, fever is present in about three quarters of the cases, whereas specific symptoms, such as headache (about one third), a rash or petechiae (about one quarter), and stiffness of the neck (about one tenth), are infrequent (96). The rash may become widespread with erythematous patches or develop into bleeding spots under the skin (petechiae, ecchymoses, or purpura). There may be associated swelling, muscle pain, skin deterioration, or gangrene in the arms and legs.
Severe complications include purpura fulminans with cutaneous pain, extensive necrosis caused by disseminated intravascular coagulation, and gangrenous necrosis of the limbs. The gangrenous areas may necessitate amputation, which may involve multiple limbs.
Meningococcal meningitis may be indistinguishable from other bacterial meningitides, including Kernig and Brudzinski signs, although the classic triad of fever, neck stiffness, and change in mental status is significantly less common in patients with meningococcal meningitis (27%) than in patients with pneumococcal meningitis (58%) (206; 92).
(Source: Koplik H. The diseases of infancy and childhood designed for the use of students and practitioners of medicine. Fourth edition. Philadelphia and New York: Lea & Fibinger, 1918. Image edited and restored by Dr. Doug...
Although less than one third of affected patients present with the classic triad of fever, nuchal rigidity, and change in mental status, nearly 90% have at least two of the following four signs on presentation: fever, nuchal rigidity, change in mental status, and rash (92). Other manifestations may include headache, photophobia, nausea, vomiting, focal neurologic findings, Kernig and Brudzinski signs, a bulging fontanelle (in children under 2 years of age), stroke, seizures, and stupor or coma (31; 205; 211). A depressed level of consciousness may indicate altered blood flow, cerebral edema, and raised intracranial pressure. Stroke due to meningococcal meningitis can result from septic arteritis, venous thrombophlebitis, or thromboembolic events (207; 208). Meningitis can have a slower onset in infants, without nuchal rigidity, but with a bulging fontanelle and nonspecific clinical findings (171).
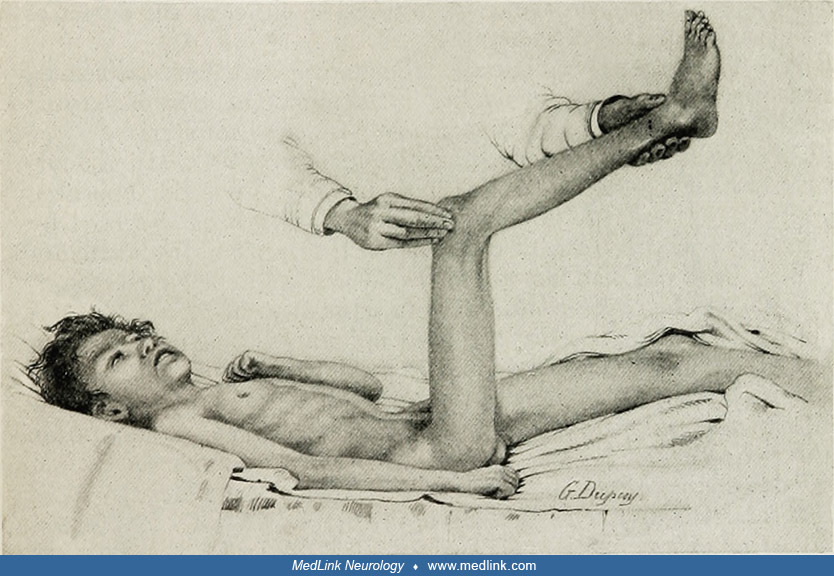
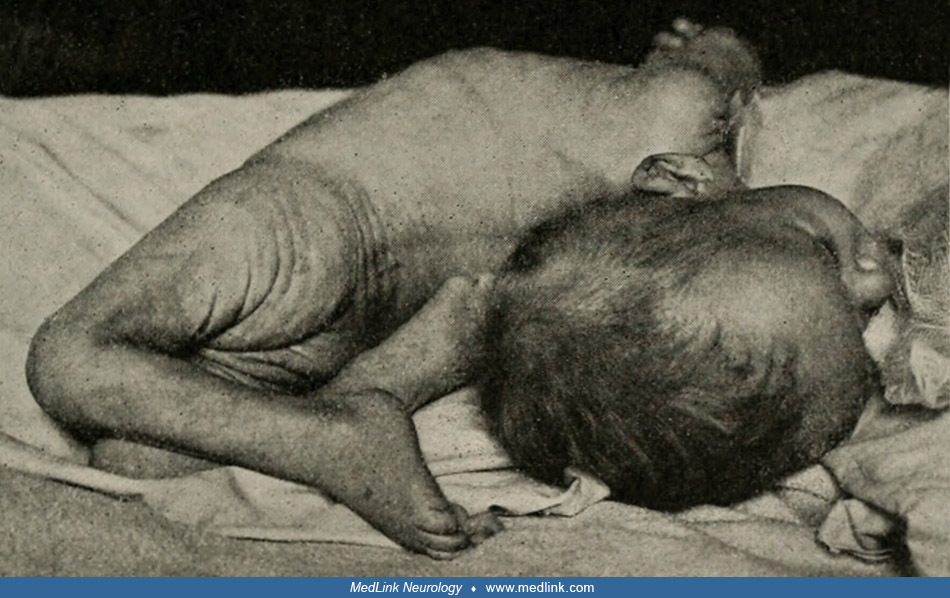
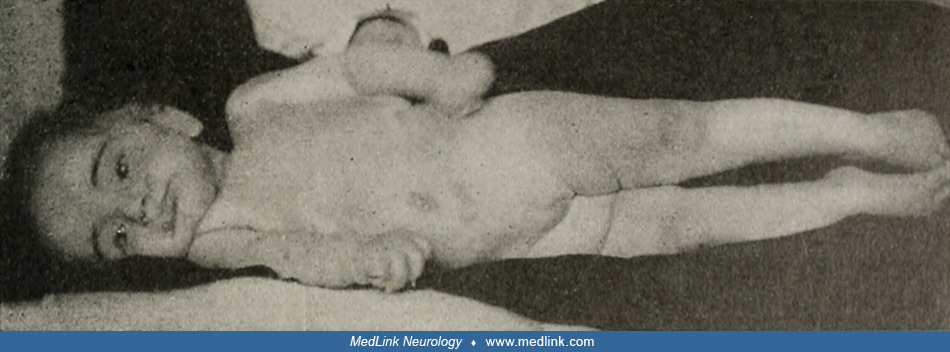
Associated with nuchal rigidity is a characteristic contraction of neck and back muscles that sometimes develops into frank opisthotonos and is often associated with hip flexion (183; 109; 84). In extreme cases, this may progress to decerebrate posturing.
(Source: Smith JL. Cerebro-spinal fever. In: Keating JM, editor. Cyclopaedia of the diseases of children: medical and surgical: the articles written especially for the work by American, British, and Canadian authors. Vol. 1. Ph...
(Source: Koplik H. The diseases of infancy and childhood designed for the use of students and practitioners of medicine. Fourth edition. Philadelphia and New York: Lea & Fibinger, 1918. Image edited and restored by Dr. Doug...
Children's Hospital of Philadelphia. (Source: Griffith CP. The diseases of infants and children. Vol. 1. Philadelphia, London: WB Saunders Company, 1919. Image edited and restored by Dr. Douglas J Lanska.)
|
[C]ontraction is most marked in muscles of the nucha [back of the neck], causing retraction of the head, but it is also common in the posterior muscles of the trunk, causing opisthotonus, and in less degree in those of the abdomen and lower extremities, and hence the flexed position of the thigs and legs, in which [position] patients obtain most relief. ... Attempts to overcome the rigidity, as by bringing forward the head, are very painful, and cause the patient to resist. ... The usual position of the patient in bed, in a typical or marked case, is with the head thrown back, the thighs and legs flexed, with or without [back extension]. | |
|
(183) |
In infants younger than 6 months of age, initial symptoms are typically fever and decreased activity. Seizures occur in the majority whereas a petechial or purpuric rash develops in only about one third (97).
Most children have only nonspecific symptoms in the first 4 to 6 hours but may be close to death by 24 hours after onset. Early symptoms of sepsis (eg, leg pains, cold hands and feet, and abnormal skin color) are present in nearly three quarters (72%) of children with meningococcal disease, are common presenting symptoms, and herald progression to shock. Signs of shock include tachycardia, hypotension, toxic or moribund state, depressed level of consciousness, breathing difficulty, poor urine output, leg pain, cold extremities with unusual skin color, and prolonged capillary refill time (longer than 2 seconds) (211). In children particularly, the classic features of hemorrhagic rash, meningeal signs, and impaired consciousness develop late (with median onset between 13 and 22 hours) (198).
Meningococci can also cause other organ involvement, including vasculitis, conjunctivitis, endophthalmitis, otitis media, epiglottitis, pleurisy, pneumonia, myocarditis, pericarditis, urethritis, and arthritis. Pneumonia is more common with serogroups Y and W meningococcal disease than with other serotypes (33; 171).
The case-fatality ratio for meningococcal disease is approximately 10% (general range from 6% to 14% though values as high as 17% have been reported for New York City from 1989 to 2000), and 11% to 26% of survivors have serious sequelae (70; 102; 32; 37; 175; 142; 31; 206; 17; 147; 185; 105; 149; 179; 182; 92; 94; 145).
The continued high case fatality is largely due to the rapid disease onset in susceptible hosts. Deaths typically occur within the first 24 hours of hospitalization and are generally associated with septic shock and severe cardiovascular and coagulation disturbances (31; 92). Mortality is significantly higher for meningococcal bacteremia (17%) than for meningococcal meningitis (approximately 3%) (175; 92). Risk factors for an unfavorable outcome include serogroup C infection, infants, young adult or college student status, advanced age, rapid progression with symptoms less than 24 hours, absence of rash or rash with more than 50 petechiae, low score on the Glasgow Coma Scale on admission, tachycardia, positive blood culture, severe septicemia with hypotension, elevated erythrocyte sedimentation rate, thrombocytopenia, acidosis, and a low cerebrospinal fluid white-cell count (206; 68; 185; 179; 182).
Long-term morbidities associated with bacterial meningitis and meningococcal septicemia include headache, hearing loss, neurologic disability (eg, focal neurologic deficits, seizures, cognitive impairment, etc.), neurodevelopment problems, renal failure, limb loss, skin complications (including scarring from necrosis), orthopedic problems (damage to bones and joints), and psychosocial problems (31; 92; 211; 210; 10; 71). In a systematic review, major sequelae (eg, cognitive deficit, bilateral hearing loss, seizures, motor deficit, visual impairment, hydrocephalus) occurred in approximately 7% of patients with meningococcal meningitis, with the risk greater in low-income countries (72). However, even in serogroup B meningococcal disease, which is the commonest cause of meningitis and septicemia in high-income countries, about one tenth of survivors have major disabling deficits, and more than one third have deficits in physical, cognitive, and psychological functioning (210). Chronic hearing impairment is the most common major sequela of meningococcal meningitis (72) and occurs in 8% to 15% of survivors (31; 92).
|
• Neisseria meningitidis is an aerobic gram-negative diplococcus with 13 different serogroups based on the antigenic characteristics of its capsular polysaccharide (ie, A, B, C, D, 29E, H, I, K, L, W-135, X, Y, and Z). | |
|
• The strains most commonly implicated in systemic disease around the world are A, B, C, W, X, and Y. In the Americas, groups B, C, and Y are the most common serogroups implicated, and each account for about 30% of reported cases. | |
|
• Historically, serogroup A has been most often associated with epidemics in sub-Saharan Africa and also in Asia, but serogroup C was also an important cause of outbreaks in Africa in the 1980s, and serogroup W and X have emerged as causes of significant epidemics in selected African countries since 2000. | |
|
• Mandatory meningococcal vaccination with the quadrivalent (A,C,Y,W) vaccine has prevented pilgrimage-associated meningococcal outbreaks and significantly reduced the incidence of the disease during the Hajj. | |
|
• Neisseria meningitidis commonly colonizes the upper respiratory tract, particularly the microvillous surface of nonciliated columnar mucosal cells in the nasopharynx. | |
|
• Bacterial outer membrane components are related to meningococcal adhesion and invasion. | |
|
• Following pilus-mediated adhesion to human brain endothelial cells, N meningitidis initiates signaling cascades, which facilitate opening of intercellular junctions, allowing meningeal colonization. | |
|
• N meningitidis uses multiple mechanisms to evade host defenses and avoid being killed by antimicrobial proteins, phagocytes, and the complement system. | |
|
• Serum bactericidal activity is dependent on the complement system (especially C2 and C5) and high antibody titers. | |
|
• After Neisseria meningitidis infection, convalescent patients develop a natural long-lasting cross-protective immunity. |
Neisseria meningitidis. Neisseria meningitidis is an aerobic gram-negative diplococcus with 13 different serogroups based on the antigenic characteristics of its capsular polysaccharide (ie, A, B, C, D, 29E, H, I, K, L, W-135, X, Y, and Z). The W-135 and 29E serogroup designations originated at the Walter Reed Army Institute of Research in the 1960s but were renamed as serogroups W and E, respectively, because the numbers are historic and supply no useful information (73; 90).
The strains most commonly implicated in systemic disease around the world are A, B, C, W, X, and Y (88). In the Americas, groups B, C, and Y are the most common serogroups implicated, and each account for about 30% of reported cases (170; 142; 107). North American outbreaks (as opposed to isolated cases) are confined primarily to serogroup C (less commonly to Y and W), although the frequency of serogroup Y outbreaks increased markedly during the 1990s (32; 33; 170; 110; 203; 142; 87; 215). Serogroups B and C are responsible for most cases in Europe (20; 95; 107), whereas serogroups A, C, and W135 predominate in Asia and Africa (107; 08).
Historically, serogroup A has been most often associated with epidemics in sub-Saharan Africa and also in Asia, but serogroup C was also an important cause of outbreaks in Africa in the 1980s, and serogroup W and X have emerged as causes of significant epidemics in selected African countries since 2000 (219; 81; 196; 113; 100; 112; 143; 221). Meningitis epidemics occur annually in Africa during the dry season (January to May) and stop with the first rains (113). Serogroup W caused significant epidemics in Burkina Faso and Niger in 2001 and 2002 (193; 64; 196; 215). Although serogroup X had been a rare cause of meningitis, serogroup X was responsible for significant outbreaks of meningococcal disease in Niger, Uganda, Kenya, Togo, and Burkina Faso from 2006 to 2010 (19; 221). After gradual introduction of mass vaccination with a monovalent meningococcal A conjugate vaccine beginning in 2010, serogroup A epidemics have been eliminated (27; 05; 28). However, serogroup C, W, and X meningococci continue to circulate in African meningitis belt countries and have been responsible for focal epidemics (05; 57; 74; 167; 181). Starting in 2013, the acquisition of capsule genes and virulence factors by a strain previously circulating asymptomatically in the African population led to the emergence of a virulent strain of serogroup C Neisseria meningitidis in Niger and Nigeria (27).
Mandatory meningococcal vaccination with the quadrivalent (A,C,Y,W) vaccine has prevented pilgrimage-associated meningococcal outbreaks and significantly reduced the incidence of the disease during the Hajj (222). Serogroup W emerged as an important cause of meningococcal epidemics in Saudi Arabia, especially during the Hajj, the annual Islamic pilgrimage to Mecca (Makkah) (191; 126).
By multilocus electrophoresis, hundreds of different electrophoretic types have been identified among invasive isolates, but less than 10 “hyperinvasive lineages” are responsible for most meningococcal disease worldwide (20; 187). Most strains are not pathogenic (171; 20; 187).
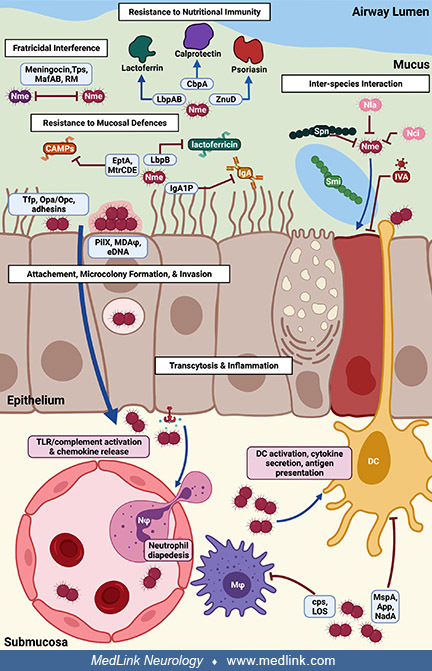
Colonization of the upper respiratory tract. Neisseria meningitidis commonly colonizes the upper respiratory tract and, particularly, the microvillous surface of non-ciliated columnar mucosal cells in the nasopharynx (171). Meningococcal carriage prevalence increases through childhood from approximately 5% in infants to a peak of 24% at 19 years of age and subsequently decreases in adulthood to 8% by 50 years of age (50).
Following acquisition, N meningitidis must compete against host defenses and interactions with other microbiome members to inhabit the nasopharynx mucus (138). Pathogenic meningococci associated with invasive disease have a capsule, which protects the bacteria from desiccation and host-mediated, complement-dependent bacteriolysis and phagocytosis (171). Eventual binding of N meningitidis to the epithelial surface of the nasopharynx results in passage into the submucosa by transcytosis. Binding of N meningitidis to epithelial cells occurs by interaction of bacterial surface structures with their cognate receptors, resulting in inflammation, cellular restructuring, and transcytosis (138).
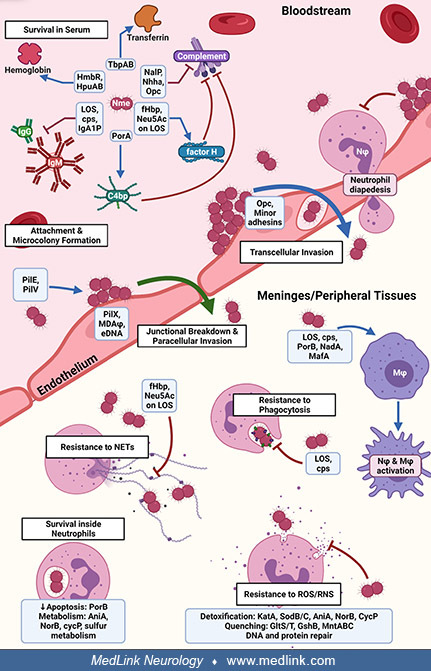
Evading host defenses. To survive in the bloodstream and proceed to transcellular invasion, N meningitidis must avoid or resist antibody- and complement-mediated killing, acquire iron, and attach to the capillary endothelial surface to form microcolonies (138).
N meningitidis uses multiple mechanisms to evade host defenses and avoid being killed by antimicrobial proteins, phagocytes, and the complement system (116; 88; 117). Such strategies include mimicry of host molecules by bacterial structures (eg, capsular proteins) as well as frequent antigenic variation (116; 88; 94). The mechanisms involved in meningococcal immune evasion and resistance against complement increase in response to an increase in ambient temperature (eg, with inflammation); the increased temperature acts as a “danger signal” for the meningococcus, which responds by enhancing its defense against human immune killing (117). Unfortunately, continuous adaptation of meningococcal surface structures has produced genetic shifts of potential vaccine-target epitopes, impeding development of a universal meningococcal vaccine that could be used against all serogroups, especially serogroup B (116; 94). In addition, the alpha-2,8-linked polysialic acid capsule modifies the interaction of serogroup B meningococci with human macrophages at multiple steps, including adherence to the macrophage surface and phagosome-lysosome fusion (165).
Meningococcal adhesion and invasion. Like the binding of N meningitidis to the epithelial surface of the nasopharynx, binding of N meningitidis to endothelial cells occurs by interaction of meningococcal surface structures with their cognate receptors, resulting in cortical plaque formation, transcytosis, and breakdown of tight junctions (138).
Binding of endothelial cells occurs by interaction of meningococcal surface structures with their cognate receptors, resulting in cortical plaque formation, transcytosis, and breakdown of tight junctions. (Source: Mikucki A, Mc...
Bacterial outer membrane components are related to meningococcal adhesion and invasion. Bacterial capsular adhesion molecules (including pili and opacity-associated proteins Opa and Opc) are responsible for binding specific human membrane proteins.
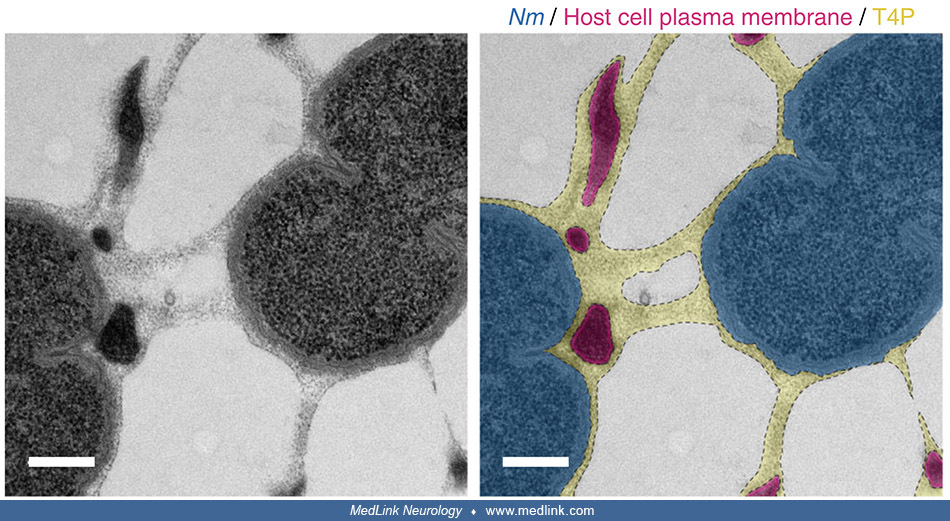
Bacterial type IV pili—long retractile fibers with a diameter of 6 nm—are necessary both for adhesion to human cells and for plasma membrane remodeling (49). Remodeling of the plasma membrane of endothelial cells by N meningitidis during the blood phase of meningococcal infection is tightly linked to the amount of type IV pili expressed by the bacteria. Plasma membrane remodeling occurs independently of F-actin, along meningococcal type IV pili fibers (49).
Scanning electron micrograph of a single N meningitidis cell (colorized in blue) with its dense meshwork of pili (colorized in yellow). The scale bar is 1 μm. (Courtesy of Arthur Charles-Orszag, adapted by him from: Ch...
Arrowheads show plasma membrane protrusions. Scale bar, 500 nm. (Source: Charles-Orszag A, Tsai FC, Bonazzi D, et al. Adhesion to nanofibers drives cell membrane remodeling through one-dimensional wetting. Nat Commun 2018;9[1]:...
Colorized crop shows plasma membrane protrusions (magenta, dotted lined) attached alongside bacterial type IV pili (yellow). Bacterial type IV pili have been stabilized with a monoclonal antibody. Abbreviation: T4P, bacterial t...
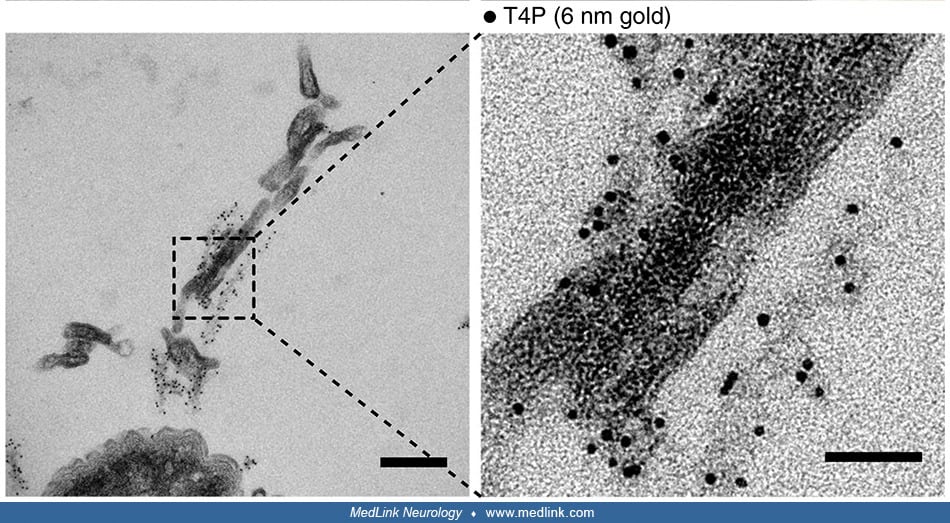
Bacterial type IV pili have been labeled with immunogold. Bacterial type IV pili have been stabilized with a monoclonal antibody and labeled with immunogold. Abbreviations: Protr, protrusions; T4P, bacterial type IV pili. Scale...
Transmission electron micrograph shows plasma membrane protrusions embedded in a meshwork of bacterial type IV pili. Abbreviation: T4P, bacterial type IV pili. Scale bars, 200 nm. (Source: Charles-Orszag A, Tsai FC, Bonazzi D, ...
Transmission electron micrograph shows plasma membrane protrusions embedded in a meshwork of bacterial type IV pili labeled with immunogold. Abbreviation: T4P, bacterial type IV pili. Scale bars, 200 nm and 50 nm. (Source: Char...
N meningitidis produces type IV pili as a meshwork of fibers. On adhesion to the host endothelial cell, the high adhesiveness of type IV pili enables "one-dimensional membrane wetting" of the plasma membrane, thus, remodeling the membrane alongside the type IV pili fibers. As the bacteria proliferate and aggregate extracellularly, plasma membrane protrusions remain attached to type IV pili fibers and end up embedded in a dense extracellular type IV pili meshwork that provides the microcolony with sufficient mechanical coherence to resist blood flow–generated shear stress (49).
N meningitidis produces type IV pili as a meshwork of fibers. On adhesion to the host endothelial cell, the high adhesiveness of type IV pili allows “one-dimensional” membrane wetting of the plasma membrane and, thus, ...
Expression of a specific human carcinoembryonic antigen-related cell adhesion molecule (CEACAM1) is necessary for binding the neisserial Opa protein adhesions, and for establishing intranasal colonization with Neisseria meningitides (104). Binding stimulates bacterial engulfment by mucosal epithelial cells, and subsequent passage of bacteria through the mucosa in phagocytic vacuoles (171). Meningococcal vascular adhesion is restricted to capillaries that exhibit transient reductions in flow (121). Initial adhesion of pathogenic strains of Neisseria meningitidis to endothelial cells relies on meningococcal type IV pili (15). The immunoglobulin superfamily member CD147, which is also known as extracellular matrix metalloproteinase inducer (EMMPRIN), is a critical host receptor for the meningococcal pilus components PilE and PilV (15). Interrupting the interaction of this endothelial receptor for bacterial adhesion potently inhibits the attachment of meningococci to human endothelial cells in vitro and prevents colonization of vessels in human brain tissue explants ex vivo and in mice in vivo (15).
Following pilus-mediated adhesion to human brain endothelial cells, N meningitidis initiates signaling cascades, which facilitate opening of intercellular junctions, allowing meningeal colonization (60). N meningitidis specifically stimulates a beta-2-adrenoceptor/beta-arrestin signaling pathway in endothelial cells, which traps beta-arrestin-interacting partners (eg, the Src tyrosine kinase and junctional proteins) under bacterial colonies; these in turn mediate cytoskeletal reorganization, which stabilizes bacterial adhesion to endothelial cells, and produce anatomical gaps used by bacteria to penetrate into tissues (60). Mutations in the N meningitidis surface-exposed proteins glyceraldehyde 3-phosphate dehydrogenase (GapA-1) and fructose-1, 6-bisphosphate aldolase also significantly affect the ability of the bacterium to adhere to human epithelial and endothelial cells (201; 202).
Bacterium-host interactions. Bacterium-host interactions are key determinants of the clinical course and risk of fatal outcomes. The interaction of meningococci with host endothelial cells is mediated by type IV pili, which are responsible for the formation of microcolonies on the apical surfaces of the cells (pili are hairlike appendages on the bacterial surface, and type IV pili, in particular, can generate motile forces that can pull the bacteria forward like a grappling hook, so-called twitching motility) (59). A low level of bacteremia favors colonization of brain blood vessels and development of meningitis, whereas colonization of many blood vessels during high-level bacteremia results in septic shock and purpura fulminates (59). In the bloodstream, meningococci release a lipo-oligosaccharide endotoxin (structurally distinct from the endotoxin of enteric gram-negative bacteria) and other cell-wall components, which stimulate cytokine production and induce the inflammatory cascade (171). Toll-like receptor 9 (TLR9) recognizes bacterial DNA leading to intracellular inflammatory signaling, and specific TLR9 single nucleotide polymorphisms are associated with susceptibility to meningococcal meningitis (173).
Serum bactericidal activity is dependent on the complement system (especially C2 and C5) and high antibody titers (93; 194). Therefore, terminal complement component defects and alterations in complement regulators are associated with an increased risk of developing N meningitidis infections (93). The polysaccharide capsule protects against complement-mediated bacterial killing, opsonization, and phagocytosis (194). In addition, during invasive disease, N meningitidis releases the contents of outer membrane vesicles into the bloodstream: these contents include lipo-oligosaccharide and outer-membrane proteins that confound the immune response to the bacteria (194).
After N meningitidis infection, convalescent patients develop a natural long-lasting cross-protective immunity, but the antigens that mediate this response have not been fully identified (136). One potential such antigen, GNA2132, is an N meningitidis protein of unknown function discovered by reverse vaccinology (178). GNA2132 has been shown to induce bactericidal antibodies in animal models, to induce protective immunity in humans, and to be recognized by sera of patients after meningococcal disease; because the protein binds heparin in vitro and because this property correlates with increased survival of the unencapsulated bacterium in human serum, the protein was renamed “Neisserial heparin binding antigen.”
Alternate routes of entry into CNS. N meningitidis readily infects trigeminal Schwann cells (the glial cells of the trigeminal nerve) (66). Infection of trigeminal Schwann cells may be one mechanism by which N meningitidis can invade the CNS. Infection of trigeminal Schwann cells leads to multinucleation and the appearance of atypical nuclei, with progressive increases over time in the presence of horseshoe nuclei and the budding of nuclei (66).
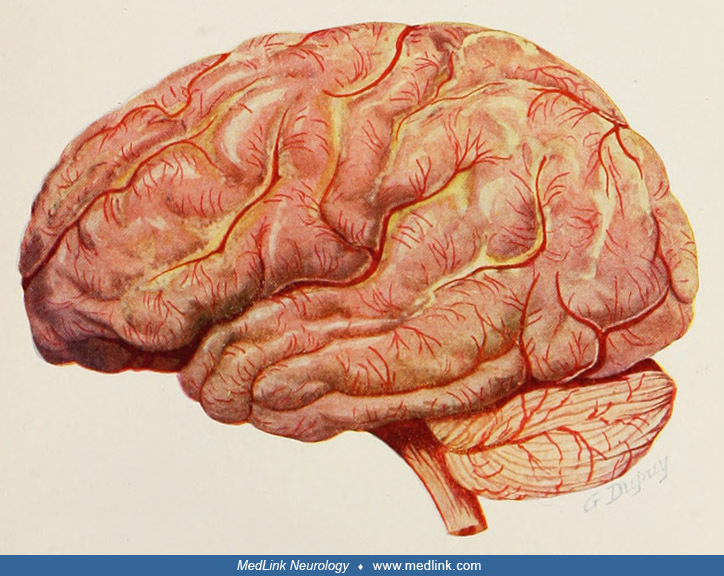
Meningitis and secondary brain complications. Meningococcal meningitis produces a purulent exudate over the surface of the brain and spinal cord. Leptomeningeal inflammatory infiltrates consist of neutrophilic granulocytes.
Note how the sulci are obscured by the exudate. (Source: Koplik H. The diseases of infancy and childhood designed for the use of students and practitioners of medicine. Fourth edition. Philadelphia and New York: Lea & Fibin...
Note how the sulci are obscured by the exudate. (Source: Koplik H. The diseases of infancy and childhood designed for the use of students and practitioners of medicine. Fourth edition. Philadelphia and New York: Lea & Fibin...
Section of the spinal cord, showing the purulent exudate on the surface, more marked posteriorly and involving the anterior and posterior nerve roots. (Source: Koplik H. The diseases of infancy and childhood designed for the us...
The inflammatory response produced to eradicate infectious pathogens can have further negative consequences, including ischemic stroke. Bacterial virulence factors and pathogen-associated molecular reactions cause direct damage to the blood-brain barrier and activate leukocytes to respond to the infection. Cytokine release further damages the blood-brain barrier, leads to neuronal death, and activates the coagulation cascade through the complement system. This inflammatory response causes vasculopathy and promotes coagulation of cerebral blood vessels, leading to cerebral ischemia.
|
• Humans are the only natural reservoir of Neisseria meningitidis. | |
|
• N meningitidis is essentially a human commensal, with most infections producing harmless nasopharyngeal colonization rather than invasive disease. | |
|
• Most cases of meningococcal invasive disease occur in children and young adults. | |
|
• Worldwide, there are 1.2 million cases of invasive meningococcal disease, with some 135,000 deaths annually. | |
|
• The vast majority of cases (95% to 98%) of invasive meningococcal disease are sporadic. | |
|
• Periodic outbreaks of meningococcal disease have been persistent problems in specific geographical areas, including the “meningitis belt” of sub-Saharan Africa. | |
|
• In non-African countries over the 50 years from 1966 to 2017, the predominant serogroup in most outbreaks was serogroup C. | |
|
• Serogroups B, C, and Y are the major causes of meningococcal disease in the United States, with each responsible for about one third of cases. | |
|
• Meningococcal disease is the leading infectious cause of death in early childhood. | |
|
• Even though the incidence of invasive meningococcal disease is declining in some populations, there has been a countermining trend of decreasing rates of penicillin susceptibility. | |
|
• In the “meningitis belt” of sub-Saharan Africa, outbreaks of serogroup A meningitis usually start in the dry season. | |
|
• Prior attempts to control epidemic meningococcal meningitis in Africa by vaccination with meningococcal polysaccharide vaccines were not successful because polysaccharide vaccines are poorly immunogenic in young children, do not induce immunological memory, and do not significantly alter pharyngeal carriage. | |
|
• With the reduction in the incidence of serogroup A meningococcal meningitis in the meningitis belt as a result of mass meningitis vaccination specific to that serogroup, there has been so-called “serogroup replacement” with an increase in the incidence of serogroups W, X, and C, and also an increase in pneumococcal meningitis. | |
|
• In the African meningitis belt, carriers of Neisseria meningitidis are a key source of transmission. |
Humans are the only natural reservoir of Neisseria meningitidis. N meningitidis is essentially a human commensal, with the great majority of infections producing harmless nasopharyngeal colonization rather than invasive disease (95; 187; 116; 94; 194). Meningococci are transmitted person-to-person through respiratory droplets. Nasal carriage rates average about 8% to 15% (77; 171), but some studies report yields of more than 30% with nasopharyngeal swabs (154). There is a low prevalence of carriage in saliva (less than 1%), indicating that saliva contact is unlikely to transmit meningococci (154). Although meningococci can be transmitted throughout the year, most cases in developed countries occur during the winter and early spring (171; 149; 179).
Most cases of invasive disease occur in children and young adults (102; 175). The highest rates are among infants under 6 months of age, who have the lowest serum bactericidal antibody titers because they do not have meningococcal-specific maternal bactericidal antibodies (194). Although rates of disease are highest among children under 2 years of age (and especially in infants younger than 6 months), almost two thirds of meningococcal disease in the United States occurs in those older than 10 years. Infants under 1 year of age have the highest incidence of meningococcal disease (5.38 cases per population of 100,000) (51). Adolescents and young adults continue to have the second-highest disease incidence from N meningitidis infection (24).
Worldwide there are 1.2 million cases of invasive meningococcal disease, with some 135,000 deaths annually.
Meningococcal disease is the leading infectious cause of death in early childhood (160).
Even though the incidence of invasive meningococcal disease is declining in some populations, there has been an opposing trend of decreasing rates of penicillin susceptibility (16).
Risk factors for invasive meningococcal disease. Risk factors for invasive meningococcal disease are outlined in the table below (34; 36; 37; 76; 52; 171; 110; 203; 187; 218; 189; 83; 69).
|
• Age less than 5 years | |
|
• Blacks | |
|
• Low socioeconomic status | |
|
• Attendees at daycare centers | |
|
• College freshmen, especially dormitory residents (44) | |
|
• Military recruits (44) | |
|
• Household crowding | |
|
• Bar or nightclub patronage during community outbreaks | |
|
• Travel to countries with hyperendemic or epidemic meningococcal disease (eg, West Africa), particularly associated with the dry wind known as Harmattan during the peak months from February to May (44) | |
|
• Homelessness (11) | |
|
• Refugees and migrants (11) | |
|
• Microbiologists frequently exposed to isolates of N meningitides (44). Occupational transmission of Neisseria meningitides has also been reported in first responders and healthcare workers (45). | |
|
• Cigarette smoking, both active and passive (including maternal smoking as a risk factor for meningococcal meningitis in children) | |
|
• Other forms of smoke, including kitchen smoke in underdeveloped countries (143) | |
|
• Viral infection of the upper respiratory tract, particularly with influenza A, but also with unspecified flu-like illnesses (143) | |
|
• Chronic underlying disease | |
|
• Human immunodeficiency virus infection | |
|
• Hepatitis C virus infection | |
|
• Asplenia, functional or anatomic (44) | |
|
• Deficiencies of the complement system, including properdin deficiency (component of the alternative pathway), terminal complement component deficiency (especially C5), C2 complement deficiency, or alterations in complement regulators (174; 44; 93; 194) |
Meningococcal serogroup trends. In non-African countries over the 50-year period from 1966 to 2017, the predominant serogroup in most outbreaks was serogroup C (61%), followed by serogroup B (29%), serogroup A (5%), and serogroup W135 (4%) (209). Outbreaks showed a peak in the colder months of both the northern and southern hemispheres (209). In Eastern Europe, the predominate serogroups are B and C, followed by A, and cases attributable to serogroups W, X and Y are emerging (12).
Serogroups B, C, and Y are the major causes of meningococcal disease in the United States, with each responsible for about one third of cases (17). However, the proportion of cases caused by each serogroup varies by age. Among infants, most cases are caused by serogroup B (17). In contrast, for persons older than 10 years, more than three quarters of cases are caused by serogroups C, Y, or W, all of which are included in licensed vaccines in the United States (17). In 2016, a serogroup C meningococcal disease outbreak occurred in Southern California, primarily affecting homosexual men (146).
From 2014 to 2018, 822 cases of serogroup A, C, W, and Y meningococcal disease were reported in the Netherlands, of which 34 (4%) were in patients who previously received at least one dose of MenACWY vaccine (23 were up to date on MenACWY vaccine, per recommendations) (18). A significantly higher proportion of vaccinated patients were people living with HIV compared to unvaccinated patients. Eight of the 34 vaccinated patients were immunosuppressed, including five with HIV, one taking eculizumab, and two taking other immunosuppressive medications.
United States. The annual incidence in the United States decreased from 0.92 cases per population of 100,000 in 1998 to 0.33 cases per 100,000 in 2007 (51). Before the introduction of the quadrivalent meningococcal conjugate vaccine, the incidence of meningococcal disease in the United States decreased to a historic low, but no further significant decrease in serogroup C or Y meningococcal disease has been observed after the introduction of the quadrivalent meningococcal conjugate vaccine among those aged 11 to 19 years (ie, when assessed for 2006 to 2007, compared with 2004 to 2005) (51).
The vast majority of cases (95% to 98%) are sporadic (95; 17). However, outbreaks of meningococcal disease in the United States have been occurring with increasing frequency since 1990 (17). Meningococcal disease outbreaks are particularly likely in semi-closed communities, such as daycare centers, schools, colleges, nursing homes, and military recruit camps (20; 17). Almost all secondary cases in an outbreak occur within 8 days of the index case (95).
The emergence of beta-lactamase-positive and ciprofloxacin-resistant meningococci in the United States is a major concern (11).
Europe. Incidence rates are higher in Europe (1.01 per population of 100,000 per year) than in the United States, but some European countries have also documented a declining incidence of invasive meningococcal disease as a consequence of improved vaccines (particularly with the introduction of effective meningococcal conjugate vaccines in the 1990s) or broader penetration of vaccination (16; 122; 153).
Patients admitted to hospitals for invasive meningococcal disease between 2014 and 2016 were selected from the French hospital discharge database (98). Of the 1344 patients identified, about 30% of cases were in children younger than 5 years old and 25% in children aged 10 to 24 years. There is a seasonal variation in the incidence of meningococcal meningitis, with cases increasing in March and April (98). Most patients presented with meningococcal meningitis (59%), 25% with meningococcemia, and 9% with both. The case fatality rate during the index hospitalization was 6%. About 15% of patients had at least one sequela at hospital discharge.
(Source: Huang L, Fievez S, Goguillot M, et al. A database study of clinical and economic burden of invasive meningococcal disease in France. PLoS One 2022;17[4]:e0267786. Creative Commons Attribution 4.0 International License,...
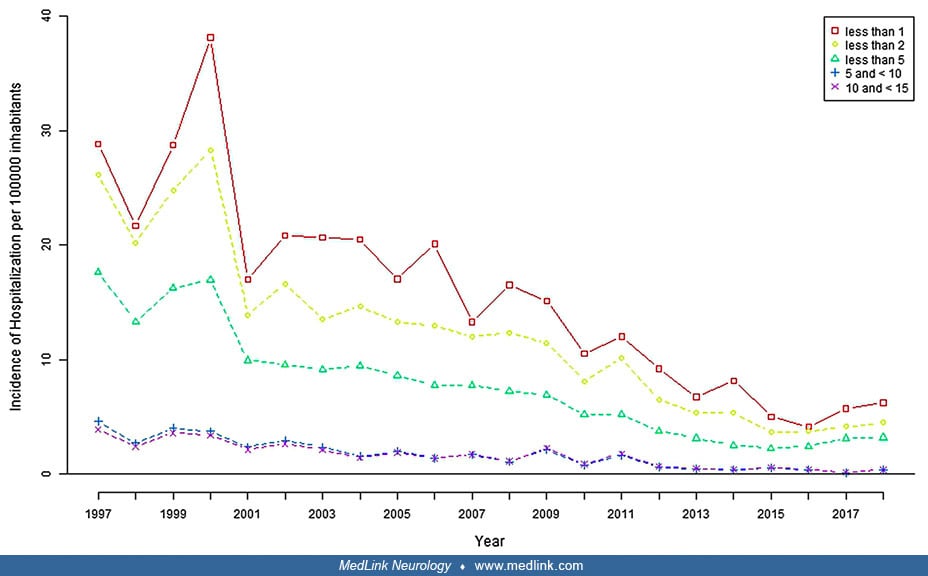
In Spain, the average hospitalization rate for meningococcal infection was 1.64 hospitalizations per 100,000 inhabitants from 1997 through 2018, with a significant declining trend over that interval (212). Hospitalization rates of meningococcal infection, meningococcal meningitis, and meningococcemia all declined from 1997 to 2018. Hospitalizations for meningococcal infection decreased significantly with increasing age and were concentrated in young children, with almost half (46%) in children under 5 years of age (46%). The hospitalization rates reached 29 per 100,000 and 24 per 100,000 in children under 1 and 2 years of age, respectively. The case fatality rates overall were 7.5% for meningococcal infection, 4.0% for meningococcal meningitis, and 9.6% for meningococcemia. Case fatality rates increased with increasing age. Thirty percent of the deaths occurred in children under 5 years of age, and more than half occurred in adults.
Rates are graphed for meningococcal infection (red), meningococcal meningitis (green), and meningococcemia (blue). (Source: Walter S, Gil-Prieto R, Gil-Conesa M, Rodriguez-Caravaca G, San Román J, Gil de Miguel A. Hospitalizati...
Rates are graphed for ages less than 1 (red), less than 2 (yellow), less than 5 (green), 5 to 9 (blue), and 10 to 14 (purple). Note that the first three age groups overlap. (Source: Walter S, Gil-Prieto R, Gil-Conesa M, Rodrigu...
Rates are graphed for ages less than 1 (red), less than 2 (yellow), less than 5 (green), 5 to 9 (blue), and 10 to 14 (purple). Note that the first three age groups overlap. (Source: Walter S, Gil-Prieto R, Gil-Conesa M, Rodrigu...
(Figure by Dr. Douglas J Lanska, based on tabular data in: Walter S, Gil-Prieto R, Gil-Conesa M, Rodriguez-Caravaca G, San Román J, Gil de Miguel A. Hospitalizations related to meningococcal infection in Spain from 1997 to 2018...
Africa. The major burden of invasive meningococcal disease is in nonindustrialized countries: in particular, Africa has been, and remains, the continent most affected by invasive meningococcal disease. Formerly heavily concentrated in the region of the "meningitis belt" of sub-Saharan Africa, invasive meningococcal disease now extends outside of its historical limits, involving more forested regions in the central and southern parts of the continent (eg, Burundi, Rwanda, the Republic of Tanzania in the Greater Lakes area, and South Africa) (215; 127; 132).
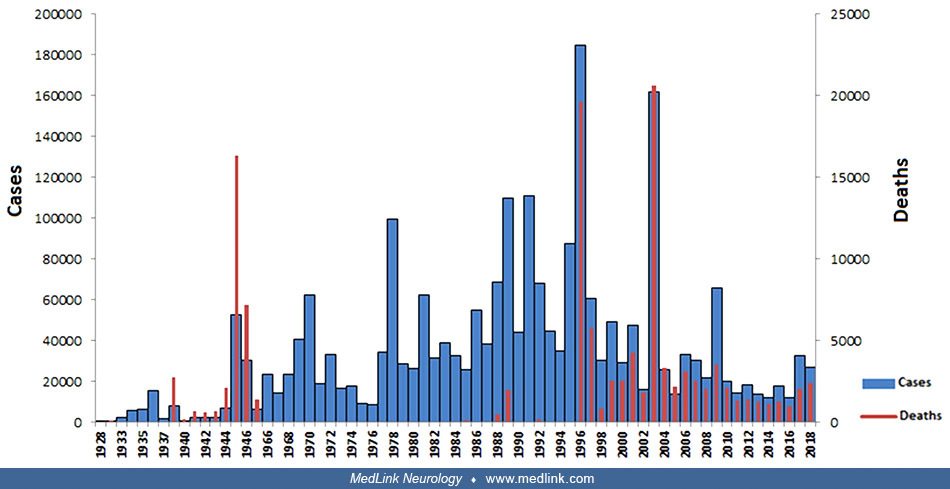
In Africa, in the interval from 1928 to 2018 (excluding 1948–1957, years for which data were unavailable), very high case counts (> 50,000) occurred in 1946, 1970, 1978, 1981, 1986, 1988–89, 1991–2, 1995–7, 2003, and 2009 (127). Very high death counts (> 5000) occurred in 1945–6, 1996–7, and 2003. Death counts were extremely high (> 15,000) in 1945, 1996, and 2003. Very high rates occurred in the meningitis belt but extended well beyond it during some periods (127).
Bar graph of annual meningitis cases (blue bars) and deaths (blue bars) from meningitis reported from 1928 to 2018 in countries within the African meningitis belt. Note that meningitis case information is unavailable for the pe...
The areas in grey illustrate the different countries belonging to the meningitis belt. Note that meningitis case information is unavailable for the period 1948–1957. Typographical errors in the figure legend in the original hav...
Outside of the African meningitis belt, case counts were below 70,000 for all countries in the interval from 1928 to 2018 (excluding 1948–1957, years for which data were unavailable) but were highest in Ghana and RD-Congo (République démocratique du Congo, or the Democratic Republic of Congo) (127). Death counts were also highest in these two countries, although the case fatality rate was higher in RD-Congo than in Ghana.
Bar graph of case counts (blue bars) and death counts (blue bars) of meningitis reported from 1928 to 2018 in countries outside of the African meningitis belt. Countries are ranked from left to right according to the number of ...
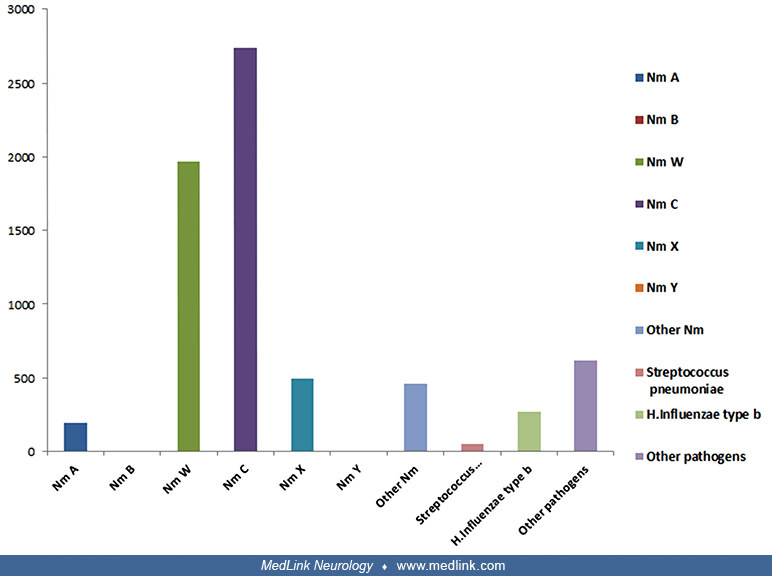
Among cases of meningococcal meningitis in Africa from 2000 to 2017, the most common serotypes were (in descending order) W, C, A, and X (127).
|
Pathogens |
Number of positive CSF |
Percentage |
|
Streptococcus pneumoniae |
2826 |
24.39 |
|
Haemophilus influenzae |
362 |
3.12 |
|
Neisseria meningitidis |
7747 |
66.87 |
|
Neisseria meningitidis A |
1161 |
10.02 |
|
Neisseria meningitidis B |
1 |
0.01 |
|
Neisseria meningitidis C |
2271 |
23.92 |
|
Neisseria meningitidis W |
2796 |
24.13 |
|
Neisseria meningitidis X |
552 |
4.76 |
|
Neisseria meningitidis Y |
6 |
0.05 |
|
Other Neisseria meningitidis |
460 |
3.97 |
|
Other pathogensa |
620 |
5.35 |
|
Positive Latex testa |
30 |
0.26 |
|
Total of positive CSF |
11,585 |
100.00 |
|
a Other pathogens include Streptococcus spp, Streptococcus group D, Salmonella sp, Enterobacter spp, Citrobacter spp, Staphylococcus aureus, Escherichia coli, Klebsiella sp, Candida sp, Acinetobacter sp, Listeria sp, Cryptococcus neoformans, and Pseudomonas sp (Source: WHO) | ||
|
Source: (127). Creative Commons Attribution (By 4.0) License (http://creativecommons.org/licenses/by/4.0/). | ||
Serotypes W and C together accounted for almost half (48%) of all meningitis cases in Africa in this interval, with the remainder as follows: S pneumoniae (24%), other serotypes of N meningitidis (19%), H influenza (3%), and other (5%). In Africa during the 20th century, serogroup A was responsible for up to 80% to 85% of meningococcal meningitis cases, but since 2000, other serogroups (including W, X, and C) have also been responsible for epidemics (127). The distribution of pathogens changed after the introduction of the MenAfrivac vaccine, which targeted N meningitidis serotype A (developed for use in sub-Saharan Africa for children and adults between 9 months and 29 years of age) (127). The impact of the MenAfrivac vaccine on the distribution of responsible pathogens within the African meningitis belt can also be seen spatially.
The African “meningitis belt.” Peak incidence rates of invasive meningococcal disease approach 1000 per 100,000 per year in the "African meningitis belt" of sub-Saharan Africa (133; 194). In the “meningitis belt,” outbreaks of serogroup A meningitis usually start in the dry season (25; 113; 100). Large epidemic waves occur in this area with a periodicity of 5 to 14 years, corresponding to molecular changes in the expression of capsular or subcapsular antigens (196; 100). The last large-scale meningitis epidemic in the African meningitis belt occurred in 2009 with 80,000 cases and 4300 deaths (08). During the 2013 epidemic season from January through June, there were 12,464 suspected meningitis cases and 1131 deaths (case fatality rate of 9.1%) reported from 18 African countries (08). The irregular timing of meningitis epidemics results from the interaction between changes in immunity and seasonal changes in the transmissibility of infection (100). The major virulence factor for Group A infections is a capsular polysaccharide comprised of a repeating unit of partly O-acetylated alpha-1,6-linked N-acetylmannosamine phosphate (113). Meningitis attack rates increased significantly in Africa in 2006 due to a new serogroup A strain, apparently heralding a new meningitis epidemic wave (196; 215).
In the interval from 1928 to 2018, cases and death counts varied by country, with the highest case counts (exceeding 100,000 and in descending order) in Nigeria, Niger, Burkina Faso, Soundan, and Ethiopia and the highest death counts (exceeding 10,000 and in descending order) in Burkina Faso, Niger, and Nigeria (127). Case counts exceeded 300,000 in Nigeria and Niger. Case fatality rates were extremely high in Cote d'Ivoire (Ivory Coast) and were also high in Burkina Faso, whereas case fatality was relatively low (among the worst affected countries) in Soudan and Ethiopia (easily seen visually in the graph by the relative height of death and case counts).
Bar graph of case counts (blue bars) and death counts (blue bars) of meningitis reported from 1928 to 2018 in countries within the African meningitis belt. Countries are ranked from left to right according to the number of case...
Seasonal hyperendemicity in the African meningitis belt is likely predominantly caused by increased invasion rates partly due to environmental factors, such as dust and low humidity (02). Sporadic localized epidemics occur with increased transmission rates, probably related in part to human contact rates and coinfections, whereas the larger pluriannual epidemic waves result from changing population immunity. Factors that contribute to the higher transmission rates in the African meningitis belt include the dry, dusty climate; overcrowding; low standards of living; the relatively low immunocompetence of the inhabitants; and poor nutritional status of the population.
Prior attempts to control epidemic meningococcal meningitis in Africa by vaccination with meningococcal polysaccharide vaccines were not successful because polysaccharide vaccines are poorly immunogenic in young children, do not induce immunological memory, and do not significantly alter pharyngeal carriage (139). A conjugate meningococcal vaccine against serotype A (MenAfriVac) was developed between 2001 and 2009 and deployed in 2010. There has subsequently been a dramatic decrease in Neisseria meningitidis A disease cases in the meningitis belt, especially since 2010, in countries that have introduced the meningococcal A conjugate vaccine (08; 07; 135; 139; 05; 28; 158; 101). The vaccine was introduced at different times in different countries: it was introduced in 2010 across Burkina Faso, Mali, and Niger, whereas it was introduced from 2011 to 2016 in other countries (101). Nevertheless, since this vaccine was introduced, there has been a decrease in the number of cases in the countries that adopted the vaccine
With the reduction in the incidence of serogroup A meningococcal meningitis in the meningitis belt as a result of mass meningitis vaccination specific to that serogroup, there has been so-called “serogroup replacement” with an increase in the incidence of serogroups W, X, and C, and also an increase in pneumococcal meningitis (02; 139; 05; 57; 74; 167; 181; 199). In 2015 an epidemic of serogroup C meningitis occurred in Niger and Nigeria with around 11,000 cases and 800 deaths (07). The World Health Organization has concluded that there is a high risk of continuing expansion of serogroup C meningitis epidemics across the meningitis belt of sub-Saharan Africa (07). The ongoing wave of serogroup C meningitis in sub-Saharan Africa is caused by a unique clone genetically distant from other known serogroup C strains. Unfortunately, population immunity to serogroup C across the meningitis belt is low because the last serogroup C epidemics in the area were in the late 1970s, and few vaccination campaigns with a serogroup C-containing vaccine have been conducted (07). It is now clear that effective control of meningococcal meningitis in the African meningitis belt cannot be achieved and will require an improved surveillance system, provision of rapid antigen detection kits, and availability of an affordable vaccine that provides protection against the main serogroups causing meningitis in the region (02; 139).
In the African meningitis belt, carriers of Neisseria meningitidis are a key source of transmission (13). In this area, the duration of carriage with any Neisseria meningitidis averages 3 months (13). Meningococcal carriage in the African meningitis belt peaks at a younger age compared to Europe, with a low prevalence in infants (0.6% in the rainy season) and a broad peak at the age of 10 (1.9%) (55; 56). The odds of meningococcal carriage are significantly increased during the dry season (OR 1.5) and during outbreaks (OR 6.7) (55). Sore throat symptoms during the dry season, but not during the rainy season, were associated with a higher risk of acquisition of meningococcal carriage (56). Males and children acquire and lose carriage more frequently in urban settings within the African meningitis belt (13).
The Hajj. Outbreaks of invasive meningococcal disease have repeatedly occurred during the Hajj, the annual Islamic pilgrimage to Mecca (Makkah) in Saudi Arabia (133). The latest outbreaks occurred during the Hajj pilgrimages of 2000 and 2001 and were associated with a shift from serogroup A to serogroup W135 disease (133; 106).
Coudeville and colleagues categorized countries or territories into five N meningitidis transmission clusters (58). First, countries were divided into three clusters (or zones) based on the prevalence of meningitis and infection risk labelled as high, medium, and low transmission clusters. In addition, Mecca and the Kingdom of Saudi Arabia outside of Mecca were considered separate clusters due to their strategic locations (subject to increased risk during the Hajj of meningitis transmission for the population belonging to these areas). Carriage rates varied across these clusters or zones.
|
Clusters |
Country of territories |
Carriage rate (%) |
|
Cluster 1: Mecca |
Mecca (Hajj city) |
4.2 [2.0, 17.8] |
|
Cluster 2: KSA outside Mecca |
Kingdom of Saudi Arabia (Hajj country) except Mecca |
1.2 [0.5, 3.2] |
|
Cluster 3: High transmission |
African meningitis belt countries (Benin, Burkina Faso, Cameroon, Central African Republic, Chad, Ivory Coast, Congo, Democratic Republic of Congo, Ethiopia, Gambia, Guinea, Ghana, Mali, Mauritania, Niger, Nigeria, Senegal, South Sudan, Sudan, Togo |
6.3 |
|
Cluster 4: Medium transmission |
South Africa, Asia (except Turkey, Malaysia, The Philippines, Indonesia, Russia, China), Arabic Non-GCC |
4.0 |
|
Cluster 5: Low transmission |
Gulf Cooperation Council countries (except KSA), Europe, Americas, Australia, Turkey, Malaysia, The Philippines, Indonesia, Russia, China |
2.0 |
|
| ||
Increased density of contacts during Hajj generates an estimated 78-fold increase in disease transmission that impacts not only pilgrims but also the local population (58). Hajj has a limited, though not negligible, impact on invasive meningococcal disease transmission and exportation in the countries of origin of the pilgrims. Quadrivalent ACWY vaccination is effective in reducing the outbreak risk during Hajj.
|
• Meningococcal disease risk can be decreased by approximately 90% in patient household contacts by administration of antibiotics known to eradicate meningococcal carriage. | |
|
• There are no high-quality experimental trials addressing control policies for meningococcal disease and no adequate studies of chemoprophylaxis in daycare settings. Nevertheless, management guidelines support chemoprophylaxis within 24 hours for all close contacts. | |
|
• Rifampin, ceftriaxone, and ciprofloxacin are acceptable for chemoprophylaxis in adults, whereas in children, rifampin or ceftriaxone are acceptable. | |
|
• Close contacts (eg, same household, school, or daycare center) must be observed carefully for development of febrile illness. Contacts who develop a febrile illness should receive urgent medical evaluation and, if indicated, appropriate antimicrobial therapy for invasive meningococcal disease. | |
|
• In hospitalized patients, droplet precautions are recommended for the first 24 hours after initiation of effective therapy. | |
|
• The United States Centers for Disease Control and Prevention recommends routine vaccination with quadrivalent meningococcal conjugate vaccine of adolescents 11 to 18 years of age and vaccination of persons 9 months to 55 years of age who have an increased risk of invasive meningococcal disease. | |
|
• There are two types of meningococcal vaccines available in the United States: (1) meningococcal polysaccharide vaccine and (2) meningococcal conjugate vaccines. |
Meningococcal disease risk can be decreased by approximately 90% in a patient’s household contacts by administration of antibiotics known to eradicate meningococcal carriage (161). This is based on a meta-analysis of four retrospective studies and one small trial with 1249 cases of meningococcal disease and more than 4200 household contacts (161). Chemoprophylaxis significantly decreased the risk of meningococcal disease for household contacts with a risk ratio of 0.11 for those receiving chemoprophylaxis (161). The number needed to treat to prevent a single secondary household case was 218 (161). Therefore, chemoprophylaxis should be recommended for the index patient with meningococcal disease and all household contacts within 24 hours of diagnosis of the primary case. In the United States, antimicrobial chemoprophylaxis is the primary means of preventing meningococcal disease among close contacts of a patient with invasive meningococcal disease (17).
There are no high-quality experimental trials addressing control policies for meningococcal disease and no adequate studies of chemoprophylaxis in daycare settings. Nevertheless, management guidelines support chemoprophylaxis within 24 hours for all close contacts (52). Chemoprophylaxis administered more than 14 days after contact with an index case is probably of no value. Also, chemoprophylaxis does not protect against subsequent reacquisition of N meningitidis.
|
• Household contacts (including persons who ate or slept in the same dwelling as the patient during the 7 days before disease onset) | |
|
• Childcare and nursery school contacts | |
|
• Persons having contact with patient’s oral secretions during the 7 days before disease onset | |
|
-- Kissing | |
|
• Aircraft contacts for persons seated next to the patient during flights of more than 8 hours, including ground time | |
|
• Casual contact (eg, at school or work) without direct exposure to patient’s oral secretions | |
Rifampin, ceftriaxone, and ciprofloxacin are acceptable for chemoprophylaxis in adults, whereas in children rifampin or ceftriaxone are acceptable (37; 38; 52). A single 500 mg oral dose of azithromycin was also reported to be effective in eradicating nasopharyngeal carriage of N meningitidis (82; 17). In most instances, for both adults and children, the drug of choice is rifampin, which is both effective and inexpensive. For young children, rifampin can be administered with greater patient acceptance in a flavored syrup. Rifampin is not recommended for use in pregnant women. Rifampin may interfere with the efficacy of oral contraceptives, and some antiepileptic and anticoagulant medications. Rifampin may also stain the urine orange for a couple of days and may stain soft contact lenses. Ciprofloxacin is also not recommended for use in pregnant women.
|
Drug |
Dose |
Route and duration | ||
|
Rifampin | ||||
|
1 month or less |
5 mg/kg q12 hours |
orally, 2d | ||
|
More than 1 month |
10 mg/kg q12 hours |
orally, 2d | ||
|
Adults |
600 mg q12 hours |
orally, 2d | ||
|
Ceftriaxone* | ||||
|
15 years or less |
125 mg |
intramuscularly, single dose | ||
|
More than 15 years |
250 mg |
intramuscularly, single dose | ||
|
Ciprofloxacin | ||||
|
Adults |
500 mg |
orally, single dose | ||
|
| ||||
Close contacts (eg, same household, school, or daycare center) must be observed carefully for the development of febrile illness. Contacts who develop a febrile illness should receive urgent medical evaluation and, if indicated, appropriate antimicrobial therapy for invasive meningococcal disease (52).
In hospitalized patients, droplet precautions are recommended for the first 24 hours after initiation of effective therapy (52).
Indications and contraindications for meningococcal vaccination. The United States Centers for Disease Control and Prevention recommends routine vaccination with quadrivalent meningococcal conjugate vaccine of adolescents 11 to 18 years of age and vaccination of persons 9 months to 55 years of age who have an increased risk of invasive meningococcal disease (43; 46; 38b; 48). Vaccination coverage of adolescents remains low in the United States but is improving (88; 118). Indications and contraindications for meningococcal immunization are listed below (34; 36; 37; 46; 47; 48; 52; 110; 203; 215). Travelers to the African sub-Saharan meningitis belt or the African Greater Lakes area during the dry season (December through June) or to Saudi Arabia during the Hajj should receive a meningococcal vaccine that provides coverage of all four serogroups (215).
|
• Adolescents (aged 11 through 18 years) | ||
|
• Decreased resistance | ||
|
- Persons (aged 9 months to 55 years) with persistent complement component deficiency1 | ||
|
• Increased exposure risk | ||
|
- Travelers to or residents of countries (aged 9 months to 55 years) with hyperendemic or epidemic meningococcal disease 3 | ||
|
Notes: (1) C5-C9, properdin, factor H, or factor D (2) Infants with asplenia should not be vaccinated against meningococcal disease because of potential interference with pneumococcal vaccine (3) West Africa during the dry season from December to June and Saudi Arabia during the annual Hajj (4) For serogroups contained in the vaccine | ||
|
• Severe (life-threatening) allergic reaction to a previous dose of MCV4 or MPSV4 vaccine. (Such individuals should not get another dose of either vaccine.) |
|
• Severe (life-threatening) allergy to any vaccine component |
|
• Moderate or severe illness at the time the shot is scheduled |
Routine immunization of children is not recommended by the Centers for Disease Control or the Committee on Infectious Disease of the American Academy of Pediatrics, in part because the infection rate is low, the immunogenic response to the vaccine is poor in young children, the immunity is relatively transient, and the quadrivalent vaccine is unlikely to be cost-effective under these circumstances (01). Parents can, nevertheless, reasonably choose to have older children receive the vaccine because the vaccine is safe and effective (150).
Barriers to vaccination. Recommendations for invasive meningococcal disease vaccination vary markedly among countries (192). Vaccination programs have targeted mainly infants and toddlers, and although they have successfully reduced the number of cases in those groups, meningococcal disease now affects more adults (192).
In the United Kingdom, France, Germany, Italy, Brazil, Argentina, Australia, and the United States, pediatric vaccination rates declined during the COVID-19 pandemic. Thirty percent of meningitidis vaccination appointments were canceled or delayed during the pandemic, and 21% of parents did not intend to reschedule them because of lockdown or stay-at-home regulations and fear of catching COVID-19 in public places (195).
In a meta-analysis of studies of predictors of meningococcal vaccine uptake among university and college students, the most common carriers of meningococcal disease, higher vaccination uptake was associated with being a first-year or undergraduate student, not being an international student, perceiving meningococcal disease as a risk, and being female (214).
Types of meningococcal vaccines. There are two types of meningococcal vaccines available in the United States: (1) meningococcal polysaccharide vaccine, and (2) meningococcal conjugate vaccines. Quadrivalent conjugate vaccines (MCV4) have immunogenicity comparable to quadrivalent polysaccharide vaccines (MPSV4) and a similar adverse reaction profile, but quadrivalent conjugate vaccines will likely provide a longer duration of protection from meningococcal disease; so, according to the Advisory Committee on Immunization Practices and the Centers for Disease Control and Prevention, conjugate vaccines (MCV4) are preferred for persons 55 years of age and younger (131; 42; 44; 169). For short-term (3 to 5 years) protection against meningococcal disease, or if quadrivalent conjugate vaccines (MCV4) are not available, the quadrivalent polysaccharide vaccine (MPSV4) is an acceptable alternative for persons aged 2 to 55 years (17; 42). The quadrivalent polysaccharide vaccine (MPSV4) continues to be recommended for persons aged older than 55 years (44). Meningococcal vaccines can be given during pregnancy. Except for children with sickle cell disease or without a working spleen, meningococcal vaccines may be given at the same time as other vaccines.
The quadrivalent polysaccharide vaccine. Meningococcal polysaccharide vaccines were initially developed in the 1970s (223). The immunogenicity and clinical efficacy of serogroup A and C meningococcal polysaccharide vaccines are well-established (17; 159). Estimated clinical efficacy of these vaccines is at least 85% among school-aged children and adults. Clinical efficacy has not been similarly documented for serogroup Y and W polysaccharide vaccines, but these vaccines have been demonstrated to be safe and immunogenic for persons older than 2 years.
A quadrivalent meningococcal polysaccharide vaccine effective against meningococci in groups A, C, Y, and W (Menomune) was licensed in 1981 in the United States for adults and for children 2 years of age and older. For both adults and older children, the vaccine is administered subcutaneously as a single 0.5 ml dose. Children between 3 months to 2 years of age who need the vaccine are generally given two 0.5 ml doses three months apart. Protective antibody levels are typically achieved by 7 to 10 days after vaccination. MPSV4 can be administered concurrently with other vaccines, but at different anatomic sites. Because antibody concentrations decline over several years after MPSV4 vaccination, high-risk patients should be re-immunized within 3 to 5 years; this applies to those with terminal complement component deficiencies or asplenia and travelers or residents of hyperendemic or epidemic areas.
Adverse reactions to meningococcal polysaccharide vaccines are generally mild, including most commonly injection site pain and redness or transient fever (17). Severe reactions are uncommon but can include systemic allergic reactions (eg, urticaria, wheezing, rash, or anaphylaxis) and neurologic reactions (eg, seizures or paresthesias).
In general, meningococcal polysaccharide vaccines are generally poorly immunogenic in children, often require repeated doses in children, do not produce long-lasting immunity, do not cause a sustained reduction in nasopharyngeal carriage, and do not interrupt transmission sufficiently to elicit herd immunity (223; 17; 159; 194). This is because bacterial polysaccharides, including capsular polysaccharides of N meningitidis, are T-cell-independent antigens (17). Such antigens stimulate mature B-lymphocytes but not T-lymphocytes, so the immunological response is neither long-lasting nor capable of eliciting a memory response after repeated challenge with the same antigen (17; 194). Therefore, dosing is required every 3 to 5 years.
Conjugate vaccines. Meningococcal conjugate vaccines (ie, in which meningococcal polysaccharides have been conjugated to carrier proteins) are licensed in the United States and other countries. Conjugate vaccines are immunogenic, can induce high concentrations of bactericidal antibodies, induce immunologic memory, reduce colonization, and provide herd immunity to the general population (150; 17; 81; 194; 120; 134). They are highly effective in preventing meningococcal disease for all age groups, including infants and young children, they avoid the need for revaccination, and they have been associated with minimal side effects (150; 223; 17). The benefits of conjugate vaccines compared with polysaccharide vaccines result from covalent bonding (ie, conjugation) of a bacterial polysaccharide with a protein carrier that contains T-cell epitopes, which produces a T-cell-dependent immune response. This substantially increases the primary immune response to vaccination among infants and young children and produces a strong memory response with re-exposure (17). Unlike the situation with pneumococcal vaccination, there is little evidence for the spread of virulent escape variants of N meningitides as a result of the development of conjugate vaccines (120).
A serogroup C meningococcal conjugate vaccine has been highly effective at reducing the incidence of serogroup C invasive meningococcal disease and has shown a high level of safety, with rare mild transient adverse effects (151; 200; 29; 115; 172; 03; 61). In the United Kingdom, beginning in 1999, meningococcal serogroup C vaccination with a conjugate vaccine (MenC) was introduced into the routine immunization schedule for children at 2, 3, and 4 months of age (150; 151; 200; 194). Vaccine effectiveness for children vaccinated in the routine immunization program fell to low levels after 1 year (151; 200; 29). Vaccine effectiveness, however, remained high (ie, greater than 90% after 4 years of follow-up) for older children vaccinated between the ages of 5 months and 18 years in a “catch-up” campaign (151; 200; 194). MenC provided significant herd immunity and led to a decline in disease even among unvaccinated people, due to reduced carriage among teenagers (the main reservoir for meningococcal transmission) (163; 29; 194). Overall, the serogroup C immunization program in the United Kingdom caused a noticeable decrease in the number of meningococcal cases, without simply shifting the distribution of cases to other serotypes (especially serogroup B). Similarly, from 2001 to 2005 all Canadian provinces introduced a meningococcal serogroup C conjugate vaccine into their routine infant immunization schedule (172). However, in some countries, such as Brazil, the timing of changes in invasive meningococcal disease incidence did not correspond to the dissemination of serogroup C meningococcal conjugate vaccine and suggested that other factors were responsible for much of the change in disease incidence (61). From implementation during 2001 to 2005 through 2012, this vaccine dramatically reduced the incidence of serogroup C invasive meningococcal disease in Canada through both direct and indirect effects (67; 172).
Although the optimum dose priming schedule of serogroup C meningococcal conjugate vaccine (MenC) in infants has not been established, vaccination programs with two priming doses can be reduced to a single priming dose without reducing post-boost antibody titers (157). Because of rapid waning of bactericidal antibody induced by a single conjugate vaccine dose at 12 months of age without infant priming (ie, “a toddler-only schedule”), programs using toddler-only schedules need to rely on herd protection to protect infants and young children (157).
A meningococcal serogroup C (MenC) vaccine was included in an investigational heptavalent combination vaccine that also included diphtheria, tetanus, acellular pertussis, hepatitis B, poliomyelitis, and Haemophilus influenzae type b (Hib) (197). In an open, phase II, randomized study, this heptavalent vaccine induced non-inferior MenC responses and had a similar safety profile compared with control vaccines (197).
Control of meningitis epidemics in Africa has relied on a complicated reactive vaccination strategy with polysaccharide vaccines that have not been successful in halting the recurrent epidemics (113). An affordable meningococcal A polysaccharide/tetanus toxoid conjugate vaccine (PsA-TT, MenAfriVac™) has now been developed and tested in clinical trials in Africa; these trials demonstrated the vaccine to be safe and to generate a sustained immunological response with high antibody titers (20 times those achieved with polysaccharide vaccine) (113; 194; 112; 186; 134; 63). The meningococcal A conjugate vaccine is highly effective at preventing serogroup A invasive meningococcal disease or carriage (63). No licensed vaccine is currently available against serogroup X meningococci, but a candidate conjugate vaccine against serogroup X meningococcal disease is in development (137; 221).
The World Health Organization now strongly promotes mass vaccination campaigns in individuals aged 1 to 29 years in all countries in the African meningitis belt (220). The World Health Organization recommends a 1-dose schedule, with vaccine administration by deep intramuscular injection (preferably in the anterolateral aspect of the thigh) at 9 to 18 months of age (220). MenAfriVac 5 mg should be used for routine immunization of infants and young children from 3 to 24 months of age, but MenAfriVac 10 mg should be used for catch-up and periodic campaigns from individuals who are 12 months of age and older (220). Because vaccination of pregnant women is safe, pregnant women should be included in the mass vaccination campaigns (220).
Because of the relatively high incidence of group Y disease, quadrivalent meningococcal conjugate vaccines that are effective against meningococci in groups A, C, Y, and W (MCV4) have been developed. Menveo® (MenACWY‐CRM) (Novartis) is administered as a single intramuscular dose, requires reconstitution, and is licensed for persons aged 2 to 55 years (54). Menactra™ (MenACWY‐D) (Sanofi Pasteur) is administered as a single intramuscular dose, does not require reconstitution, and is licensed for persons aged 9 months to 55 years. Protective levels of antibodies are usually achieved within 7 to 10 days of vaccination. MCV4 vaccines also elicit a T-cell-dependent immune response and are, therefore, anticipated to provide immunity for more than 8 years. MCV4 can be administered concurrently with other vaccines but at different anatomic sites (65; 80). Unfortunately, the immunogenicity of conjugate vaccines is generally poor in infants and young children, the most vulnerable group (184). In a phase 3, observer-blind, randomized controlled trial, MenACWY-CRM reduced meningococcal carriage rates among university students aged 18 to 24 years during 12 months after vaccination (164). Post-licensure safety surveillance of complications associated with routine use of quadrivalent meningococcal diphtheria toxoid conjugate vaccine (MenACWY-D) in infants and children did not identify any new safety concerns (86). Vaccine-induced serogroup replacement has not been observed in the United States after licensure of the quadrivalent meningococcal conjugate vaccine (213).
In response to an epidemic of invasive meningococcal disease due to serogroup W in the Netherlands, the meningococcal-serogroup-C-conjugated-to-tetanus-toxoid (MenC-TT) vaccine for toddlers was replaced by the MenACWY-TT vaccine in May 2018. A mass vaccination campaign targeting individuals aged 14 to 18 years was implemented in 2018 and 2019, and the quadrivalent vaccine was introduced for all individuals aged 14 years old in a national immunization program in 2020 (152). The MenACWY vaccination program was effective in preventing serogroup W invasive meningococcal disease in the target population.
Because of the risk from meningococcal disease, the Centers for Disease Control and Prevention continue to recommend routine vaccination with MCV4 for adolescents, college freshmen living in dormitories, and other high-risk populations (40; 41; 24).
|
Risk group |
Primary series |
Booster dose |
|
Persons aged 11 to 18 years |
One dose, preferably at age 11 or 12 years |
At age 16 years, if primary dose at age 11 to 12 years At age 16 to 18 years, if primary dose at age 13 to 15 years No booster needed if primary dose on or after age 16 years |
|
HIV-infected persons aged 11 to 18 years |
Two doses, 2 months apart |
At age 16 years, if primary dose at age 11 to 12 years At age 16 to 18 years, if primary dose at age 13 to 15 years No booster needed if primary dose on or after age 16 years |
|
Children aged 9 through 23 months at high risk for invasive meningococcal disease (except children with functional or anatomic asplenia)# |
Two doses, 3 months apart (if dose two is not received on schedule: administer a catch-up dose at the earliest opportunity) |
Initial booster 3 years after completing the primary series (if the child remains at increased risk for meningococcal disease) Continued boosters at 5-year intervals after the initial booster |
|
Persons aged 2 to 55 years with persistent complement component deficiency (eg, C5 to C9, properdin, or factor D) or functional or anatomical asplenia |
Two doses, 2 months apart |
Every 5 years At the earliest opportunity, if a 1-dose primary series is administered, then every 5 years |
|
Persons aged 2 to 55 years with prolonged increased risk for exposure† |
One dose |
Persons aged 2 to 6 years: after 3 years Persons aged 7 years or older: after 5 years if person remains at increased exposure |
|
# Children who have persistent complement component deficiencies (eg, C5-C9, properdin, factor H, or factor D), children who are traveling to or residents of countries where meningococcal disease is hyperendemic or epidemic, and children who are in a defined risk group during a community or institutional meningococcal outbreak. † Microbiologists routinely working with Neisseria meningitidis and travelers to or residents of countries where meningococcal disease is hyperendemic or epidemic. Adapted from (46; 47; 48) | ||
In general, adverse reactions to meningococcal conjugate vaccines are generally mild (114; 115), although local adverse reactions are somewhat more common than among those receiving meningococcal polysaccharide vaccines (17). Severe reactions are uncommon (estimated at 7 per 100,000) and similar in frequency to those reported with meningococcal polysaccharide vaccines (17; 114). Data suggest a small increased risk for Guillain-Barré syndrome after MCV4 vaccination, with a peak onset time from 9 to 15 days after vaccination (39; 40; 41; 42; 24). In general, persons with a history of Guillain-Barré syndrome should not be vaccinated with MCV4 (39; 41), although the language in recommendations from the Centers for Disease Control and Prevention considers a history of Guillain-Barré syndrome to be “a caution to administering MCV4” (42).
Bivalent conjugate vaccine (Serogroups C and Y). On June 14, 2012, the Food and Drug Administration approved a combination vaccine against two types of meningococcal diseases and Hib disease for infants and children 6 weeks to 18 months old. The vaccine, Menhibrix, is a tetanus toxoid conjugate vaccine that prevents disease caused by Neisseria meningitidis serogroups C and Y and Haemophilus influenzae type b. This is the first meningococcal vaccine that can be given to infants as young as 6 weeks old. Menhibrix is given as a 4-dose series, usually at 2, 4, 6, and 12 through 15 months of age, although the first dose may be given as early as 6 weeks of age and the fourth dose may be given as late as 18 months of age.
Group B meningococcal disease. Development of an effective vaccine for prevention of group B meningococcal disease had been long delayed because the serogroup B capsular polysaccharide is poorly immunogenic in humans (17; 24; 51). The serogroup B capsular polysaccharide is composed of alpha-2,8-linked polysialic acid, which is structurally identical to the posttranslational modification that occurs on neural cell adhesion molecules; therefore, it has immune tolerance (75; 165; 194).
Subsequent efforts at vaccine development focused on identifying potential outer membrane protein targets that elicit broadly protective immune responses across strains (78; 130; 194; 79; 216). In 2004, Fletcher and colleagues at Wyeth Vaccines Research identified LP2086 as a novel Neisseria meningitidis antigen with vaccine potential (78). LP2086 is a family of approximately 28-kDa lipoproteins localized to the outer surface of Neisseria meningitidis (78; 130). More than 600 LP2086 amino acid sequence variants have been identified that can be classified into two subfamilies, subfamily A and B (78; 155; 144; 108). Because LP2086 selectively binds to human factor H, the key regulator of the alternative complement pathway, LP2086 is also known as factor H binding protein (fHbp) (176). Binding of factor H to fHbp enables Neisseria meningitidis to evade killing by the innate immune system (177). A further designation for LP2086 is GNA1870, indicating a specific genome-derived antigen (156).
Preclinical studies demonstrated that LP2086 induces cross-reactive bactericidal antibodies against various Neisseria meningitidis strains (78; 155). The bactericidal antibody response correlates with the amount of LP2086 expressed on the bacterial surface (176). Preliminary work at Wyeth Vaccines Research showed that a formulation containing both subfamilies of LP2086 could potentially provide broad protection against a majority of Neisseria meningitidis strains, and later studies confirmed the broad coverage potential of a bivalent recombinant LP2086 vaccine (155; 103; 124). LP2086 is expressed in vivo during both carriage and invasive disease at levels high enough to elicit a robust antibody response (04).
Two recombinant protein-based serogroup B vaccines have been developed and licensed in the United States under an accelerated approval process, both of which incorporate LP2086: bivalent rLP2086 (MenB-FHbp; Trumenba®) and 4CMenB (MenB-4 C; Bexsero®) (123).
Bivalent rLP2086 vaccine comprises two fHbp variants, where each antigen represents one of the two known LP2086 subfamilies recombinantly expressed in Escherichia coli. In young adults, bivalent rLP2086 vaccine is well-tolerated and induces potent bactericidal antibodies against diverse serogroup B strains (168; 180; 119). Bivalent rLP2086 vaccine is also well-tolerated and immunogenic in healthy children and adolescents (148). Because of high rates of fever in phase I and II trials in infants, further investigations in this age group are not being pursued (125; 22). Bivalent rLP2086 received accelerated approval from the U.S. Food and Drug Administration in October 2014. The vaccine is licensed to prevent meningococcal meningitis disease caused by N meningitidis serogroup B in individuals 10 to 25 years of age.
4CMenB is a multicomponent meningococcal serogroup B vaccine that has been licensed for use in Europe (January 2013), Australia (August 2013), Canada (December 2013), and the United States (January 2015). The vaccine contains four main immunogenic components: three recombinant proteins combined with outer membrane vesicles derived from a specific meningococcal strain (NZ98/254) (30; 06). Before licensure in the United States, the Food and Drug Administration allowed the use of the vaccine under an Investigational New Drug application to help control a specific outbreak of serogroup B meningococcal disease at Princeton University in 2013–2014 (129; 14). In that outbreak, no serogroup B meningococcal disease cases occurred in persons who received at least one dose of the 4CMenB vaccine, suggesting that 4CMenB may have protected vaccinated individuals from disease even though carriage of serogroup B Neisseria meningitidis among vaccinated persons was not eliminated (129). In a phase 3, observer-blind, randomized controlled trial conducted at 10 sites in England, 4CMenB reduced meningococcal carriage rates among university students aged 18 to 24 years during 12 months after vaccination (164). The breadth of protection the vaccine may induce against the diverse pathogenic serogroup B strains is still uncertain (06). Nevertheless, modeling has suggested an optimal vaccination strategy of routine vaccination at ages 2 months, 3 months, 4 months, 12 months, and 14 years combined with a 5-year catch-up program in toddlers aged 12 to 24 months and adolescents aged 15 to 18 years (99). Although 4CMenB may have a protective role in clusters and outbreaks, early protection offered after a single dose of Bexsero® is likely to be low, particularly in young children who are at higher risk of secondary infection (111). Indeed, for infants, the percent reduction in cases at 1-year follow-up is only 50%, but this rises to 90% to 94% at 3 to 4 years, respectively (123). The safety profile of 4CMenB administered in real-world settings is consistent with pre-licensure clinical trial data (123).
Since serogroup B meningococcal (MenB) vaccines became available in the United States, six serogroup B meningococcal disease cases were reported in MenB-4C (n = 4) or MenB-FHbp (n = 2) recipients (166). Patient risk factors, incomplete vaccine series completion, waning immunity, and strain resistance likely contributed to disease in these patients.
In neonates, bacterial meningitis is typically caused by organisms acquired from the maternal genital tract and gastrointestinal tract around the time of birth (eg, Streptococcus group B, Escherichia coli, Streptococcus pneumoniae, and Listeria monocytogenes), whereas in older children and young people, bacterial meningitis is usually caused by organisms that can colonize the upper respiratory tract and cause invasive disease in susceptible people (eg, N meningitides, Streptococcus pneumoniae, or Haemophilus influenzae type b). N meningitidis and Streptococcus pneumoniae are the most commonly identified organisms in cases of meningitis in children 1 to 23 months of age (175). N meningitidis causes most cases of meningitis in children between ages 2 and 18 years. The highest incidence of meningococcal disease occurs in children under age 2 years, with further peaks in incidence occurring in adolescence and early adulthood.
An acute fulminating presentation with fever, petechial or purpuric rash, prostration, and hypotension is strong evidence of meningococcal disease. Often, however, meningococcal meningitis cannot be distinguished clinically from other causes of bacterial meningitis. Many cases of meningococcal meningitis present atypically without the classic triad of fever, neck stiffness, and change in mental status (206). A high index of suspicion is needed, particularly in infants and small children.
|
• Signs indicating a high risk of meningococcal disease in children and young people with a petechial rash include changes in the rash in which either petechiae start to spread or the rash becomes purpuric, development of signs of bacterial meningitis or of meningococcal septicemia, or appearing seriously ill. According to the United Kingdom's National Institute for Health and Clinical Excellence (NICE) Guidelines, such individuals should receive intravenous ceftriaxone immediately without waiting for other diagnostic studies. | |
|
• Lumbar puncture is indicated for suspected meningitis or suspected meningococcal disease unless contraindications are present. | |
|
• Bacterial antigen detection tests, gram stains, and culture are generally considered the most useful diagnostic tests. | |
|
• Polymerase-chain reaction analysis can detect serogroup-specific Neisseria meningitidis DNA with high sensitivity and specificity even with dead organisms. |
Signs indicating a high risk of meningococcal disease in children and young people with a petechial rash include changes in the rash in which either petechiae start to spread or the rash becomes purpuric, development of signs of bacterial meningitis or of meningococcal septicemia, or appearing seriously ill (ie, to a healthcare professional) (211). According to the United Kingdom's National Institute for Health and Clinical Excellence (NICE) Guidelines, such individuals should receive intravenous ceftriaxone immediately without waiting for other diagnostic studies (211).
If a child or young person has an unexplained petechial rash and fever (or history of fever) without high-risk clinical manifestations, the NICE Guidelines recommend the following studies: complete blood count, C reactive protein, coagulation screen, blood culture, whole blood polymerase chain reaction for N meningitidis, blood glucose, and arterial blood gas (211). Although a normal C reactive protein concentration and normal white blood cell count make meningococcal disease less likely, these measures may be normal or low even in severe meningococcal disease.
Lumbar puncture is indicated for suspected meningitis or suspected meningococcal disease unless contraindications are present (211). N meningitidis diplococci are typically evident on Gram stain of cerebrospinal fluid, along with a profusion of polymorphonuclear leukocytes. The CSF is characterized by a markedly elevated white blood cell count (> 500 cells/ml), with predominant neutrophils and a markedly elevated protein (> 100 mg/dl or > 1 g/l), indicating severe blood-CSF barrier disruption.
According to the NICE Guidelines, contraindications to lumber puncture in children and young people include the presence of signs of increased intracranial pressure (ie, a reduced or fluctuating level of consciousness with a score of less than 9 or a drop of at least 3 points on the Glasgow Coma Scale; relative bradycardia and hypertension; focal neurologic signs; abnormal posture or posturing; unequal, dilated, or poorly responsive pupils; papilledema; and abnormal "doll's eye" movements), shock, extensive or spreading purport, not yet stabilized from recent convulsions, coagulopathy (abnormal coagulation results if obtained), platelet count below 100 x 10(9)/L, local skin infection at lumbar puncture site, and respiratory insufficiency (211).
Bacterial antigen detection tests, gram stains, and culture are generally considered the most useful diagnostic tests. Bacterial antigen detection tests (eg, latex agglutination tests) in CSF are useful for rapid diagnosis. Rapid antigen tests from urine or serum samples are unreliable (35; 52). Gram stains of normally sterile body fluids can help establish a presumptive diagnosis of meningococcal disease (52). Cultures of blood and cerebrospinal fluid are indicated in all patients with suspected invasive meningococcal disease, and additional cultures from petechial scrapings, sputum, and other normally sterile body fluids can also sometimes be helpful (52).
Polymerase-chain reaction analysis can detect serogroup-specific Neisseria meningitidis DNA with high sensitivity and specificity even with dead organisms (26; 141). PCR can confirm the diagnosis, even when the number of bacteria is below the threshold for successful culturing, or after antibiotic administration (26). The NICE Guidelines recommend whole blood real-time PCR testing for N meningitidis to confirm a diagnosis of meningococcal disease (211).
Skin biopsy with conventional culture and meningococcal PCR has a sensitivity of 88% and should be considered in case of suspected meningococcal purpura fulminans even after initiation of antimicrobial treatment (53).
A probable case of meningococcal disease can be established with a positive antigen test in CSF or clinical purpura fulminans in the absence of a positive blood culture (35; 52). Polysaccharide can be demonstrated in cerebrospinal fluid by latex agglutination or immunohistochemistry, and DNA can be demonstrated by PCR (17). False-negative antigen test results are common, especially with serogroup B disease (171).
A presumptive case of meningococcal disease can be established by demonstration of gram-negative diplococci in a normally sterile body fluid, such as cerebrospinal fluid, an aspirate from a petechial or purpuric lesion, buffy coat smear of blood, synovial fluid, etc. (52).
A confirmed case of meningococcal disease is one with compatible clinical features and laboratory confirmation (35). Laboratory criteria for diagnosis of meningococcal disease are isolation of Neisseria meningitidis from a normally sterile site, such as the blood or cerebrospinal fluid (or less commonly from a petechial or purpuric lesion, synovial fluid, pericardial fluid, or pleural fluid) (35; 52).
|
• Because of the risks of severe morbidity and death, appropriate antibiotic therapy should be rapidly initiated in patients suspected of having meningococcal disease. | |
|
• Before confirmation of meningococcal disease as the cause of the illness, empiric antibiotic coverage should be directed at the most likely pathogens based on epidemiologic considerations (eg, age, geographic location, etc.) and the known prevalence of antibiotic resistance for these organisms. | |
|
• No investigations should delay initiating antibiotic therapy once the diagnosis of meningococcal meningitis is suspected. | |
|
• According to the NICE Guidelines, children who have suspected bacterial meningitis or meningococcal disease should be immediately treated with intravenous ceftriaxone, with the addition of amoxicillin or ampicillin for children younger than 3 months. | |
|
• Recommendations for initial empiric antimicrobial therapy in adults with community-acquired bacterial meningitis are vancomycin plus a third-generation cephalosporin (eg, cefotaxime or ceftriaxone) for those aged 16 to 50 years and vancomycin plus a third-generation cephalosporin plus ampicillin for those older than 50 years, or for those with alcoholism or altered immune status. Generally, combination therapy should be continued until in vitro susceptibility testing results are available. | |
|
• Once in vitro susceptibility testing results are available, 5 to 7 days of appropriate antimicrobial therapy are usually adequate to treat invasive meningococcal disease. | |
|
• Systemic antibiotic therapy with agents other than ceftriaxone or other third-generation cephalosporins may not reliably eradicate nasopharyngeal carriage of N meningitidis. | |
|
• Corticosteroid therapy has no demonstrated efficacy for meningococcal disease. | |
|
• Patients commonly need additional therapies for seizures and hemodynamic instability, both of which occur in up to 20% of patients on presentation. | |
|
• Droplet precautions should be instituted until 24 hours after initiation of antibiotic therapy. | |
|
• In persons with bacterial meningitis, fluids should not be restricted unless there is evidence of increased intracranial pressure or increased antidiuretic hormone secretion. | |
|
• Patients should be monitored closely for evidence of deterioration, using frequent assessment of pulse, blood pressure, respiration, oxygen saturation, and Glasgow Coma Scale score. | |
|
• As part of the long-term management of children and young people with severe or profound deafness due to meningococcal meningitis, assessment for cochlear implantation should be offered as soon as possible once the patient can undergo testing. |
Because of the risks of severe morbidity and death, appropriate antibiotic therapy should be rapidly initiated in patients suspected of having meningococcal disease. Before confirmation of meningococcal disease as the cause of the illness, empiric antibiotic coverage should be directed at the most likely pathogens based on epidemiologic considerations (eg, age, geographic location, etc.) and the known prevalence of antibiotic resistance for these organisms. No investigations should delay initiating antibiotic therapy once the diagnosis of meningococcal meningitis is suspected (21). Unfortunately, antibiotic therapy is often delayed by waiting for neuroimaging and then lumbar puncture; in a Dutch study, antibiotics were not initiated before computed tomography in 85% of patients who underwent imaging before lumbar puncture (92). According to a Cochrane review, there is no reliable evidence concerning the use of pre-admission antibiotics for suspected cases of non-severe meningococcal disease, although evidence of moderate quality from one randomized controlled trial indicated that single intramuscular injections of ceftriaxone and long-acting chloramphenicol were equally effective in reducing serious outcomes (188).
According to the NICE Guidelines, children and young people with an unexplained petechial rash and fever (or a history of fever) but without high-risk clinical manifestations should be treated immediately with intravenous ceftriaxone if a C reactive protein level or white blood cell count (especially neutrophil count) is raised because either of these indicates an increased risk of meningococcal disease (211).
According to the NICE Guidelines, children who have suspected bacterial meningitis or meningococcal disease should be immediately treated with intravenous ceftriaxone, with the addition of amoxicillin or ampicillin for children younger than 3 months (211). Vancomycin should be added for those who have recently traveled outside the country or had prolonged or multiple antibiotic exposures (211). Cefotaxime should be substituted for ceftriaxone if there are calcium-containing infusions (211).
Recommendations for initial empiric antimicrobial therapy in adults with community-acquired bacterial meningitis are vancomycin plus a third-generation cephalosporin (eg, cefotaxime or ceftriaxone) for those aged 16 to 50 years and vancomycin plus a third-generation cephalosporin plus ampicillin for those older than 50 years, or for those with alcoholism or altered immune status (207). Generally, combination therapy should be continued until in vitro susceptibility testing results are available.
Once in vitro susceptibility testing results are available, 5 to 7 days of appropriate antimicrobial therapy are usually adequate to treat invasive meningococcal disease (162; 52). Antibiotic resistance is relatively uncommon in N meningitidis isolates (94). Penicillin is the drug of choice. Generally, high-dose intravenous penicillin G should be administered every 4 to 6 hours for patients with invasive meningococcal disease (52). Acceptable alternatives to penicillin G are ampicillin, cefotaxime, and ceftriaxone (162; 52). Most reported strains are moderately susceptible to high-dose penicillin G, cefotaxime, and ceftriaxone (162; 52). Other effective regimens include 3 days of intravenous benzylpenicillin (23). Chloramphenicol is indicated for patients with anaphylactic allergic reactions to penicillin (52). Chloramphenicol has also been used routinely in underdeveloped countries, but single-dose ceftriaxone is an efficacious, easy-to-use, and low-cost alternative (147). Whereas most isolates of meningococcus remain penicillin-susceptible, fluoroquinolone resistance has now been documented in the U.S. (24). Because of high rates of penicillin resistance in Spain, Italy, and parts of Africa, other agents (eg, cefotaxime, ceftriaxone, or chloramphenicol) are recommended for travelers returning from these areas (52). For patients with inadequate responses to initial therapy, bacterial isolates should be tested, and therapy should be changed to a third-generation cephalosporin if the isolate is resistant to penicillin (162).
From 2010 to 2019, 126 of 4122 invasive meningococcal disease isolates (2.9%) in England, Wales, and Northern Ireland exhibited antibiotic resistance: penicillin (n=113), ciprofloxacin (n=5), rifampicin (n=2), and cefotaxime (n=1) (217).
Systemic antibiotic therapy with agents other than ceftriaxone or other third-generation cephalosporins may not reliably eradicate nasopharyngeal carriage of N meningitidis (17). If other agents have been used for treating invasive meningococcal disease, the patient should receive chemoprophylactic antibiotics to eradicate nasopharyngeal carriage before hospital discharge (17).
Although corticosteroids may decrease the risk of hearing loss in patients with meningitis caused by other organisms, corticosteroid therapy has no demonstrated efficacy for meningococcal disease (171; 85; 204; 128; 140). However, in a systematic review for the Cochrane Collaborative, corticosteroids showed a non-significant favorable trend in mortality from meningococcal meningitis, and the lack of demonstrated benefit has been hypothesized to be due to limited power to detect a benefit rather than to no benefit (128). In any case, there is no evidence of a detrimental effect, and, in particular, dexamethasone does not appear to increase the risk of deafness or death (91). Low-dose corticosteroids have been recommended in patients with meningococcal disease and refractory shock (21). For children aged 3 months or older and young people with suspected or confirmed bacterial meningitis (including that due to N meningitidis), the NICE Guidelines recommend giving dexamethasone (0.15 mg/kg to a maximum dose of 10 mg, four times daily for 4 days) as soon as possible if lumbar puncture shows frankly purulent cerebrospinal fluid, CSF white blood cell count greater than 1000/μl, raised CSF white blood cell count with protein concentration greater than 1 g/l, or bacteria on Gram stain (211). Corticosteroids should not be used in children younger than 3 months who have suspected or confirmed bacterial meningitis (211).
Patients commonly need additional therapies for seizures and hemodynamic instability, both of which occur in up to 20% of patients on presentation (31).
Droplet precautions should be instituted until 24 hours after initiation of antibiotic therapy (52).
In persons with bacterial meningitis, fluids should not be restricted unless there is evidence of increased intracranial pressure or increased secretion of antidiuretic hormone (211). Shock should be treated with an immediate parenteral bolus of sodium chloride 0.9%. In children and young people, NICE Guidelines recommend intravenous or intraosseous sodium chloride 0.9% 20 ml/kg over 5 to 10 minutes, followed if necessary by an immediate second bolus of 20 ml/kg of intravenous or intraosseous sodium chloride 0.9% or human albumin 4.5% solution over 5 to 10 minutes (211). If the signs of shock still persist after the first 40 ml/kg, a third bolus of 20 ml/kg of intravenous or intraosseous sodium chloride 0.9% or human albumin 4.5% solution should be given over 5 to 10 minutes, in conjunction with urgent tracheal intubation and mechanical ventilation and treatment with vasoactive drugs (211). Additional fluid boluses may be required because some children and young people may require large volumes of fluid over a short period to restore their circulating volume.
Patients should be monitored closely for evidence of deterioration, using frequent assessment of pulse, blood pressure, respiration, oxygen saturation, and Glasgow Coma Scale score (211).
As part of the long-term management of children and young people with severe or profound deafness due to meningococcal meningitis, assessment for cochlear implantation should be offered as soon as possible once the patient can undergo testing (211).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD FAAN MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Behavioral & Cognitive Disorders
Apr. 18, 2024
Behavioral & Cognitive Disorders
Apr. 17, 2024
General Child Neurology
Apr. 05, 2024
Infectious Disorders
Apr. 02, 2024
General Child Neurology
Apr. 01, 2024
General Child Neurology
Mar. 29, 2024
General Child Neurology
Mar. 29, 2024
General Child Neurology
Mar. 27, 2024