







Epilepsy & Seizures
Hippocampal and parahippocampal seizures
Apr. 22, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Preeclampsia or eclampsia is a multisystem disorder of pregnancy and the puerperium. Preeclampsia occurs after the twentieth week of gestation and is characterized by hypertension, proteinuria, and pathologic edema. Eclampsia is defined as the occurrence of generalized seizures in a woman with preexisting preeclampsia. Many reports have indicated that SARS-CoV-2 infection adversely affects pregnancy and can predispose pregnant women to preeclampsia and possibly to eclampsia as well. Approximately 10% to 15% of maternal deaths are associated with preeclampsia and eclampsia. Although the incidence of eclampsia and its complications have decreased significantly in developed countries, the incidence is still high in poor countries. The latest data from the United States indicated an approximately 10% decline in the risk of eclampsia between 2009 to 2017. Eclampsia occurring more than 48 hours, but less than 4 weeks, after delivery is known as late postpartum eclampsia. Postpartum preeclampsia or eclampsia may present without a history of preeclampsia during the pregnancy. Visual disturbances, epigastric pain, headache, and edema are four of the most frequent symptoms that can predict imminent eclampsia in ladies with preeclampsia. In eclampsia, reversible posterior leukoencephalopathy syndrome is an increasingly recognized cause of seizures, cortical blindness, and encephalopathy. In addition to posterior leukoencephalopathy syndrome, neuroimaging may reveal cerebral edema, infarction, cerebral venous thrombosis, and cerebral hemorrhage. Magnesium sulfate is the treatment of choice for the control of recurrent eclamptic seizures in pregnant women. In a study, a low-dose regimen of magnesium sulfate appeared comparable to the “standard” dose regimen. The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine recommend only short-term (usually less than 48 hours) use of magnesium sulfate. If given in excess, magnesium sulfate has a neuromuscular junction-blocking effect, and such patients could manifest with “pseudocoma.” Early combined treatment of critically raised blood pressure with intravenous antihypertensive drugs and magnesium sulfate is associated with a reduction in the frequency of eclampsia and severe maternal morbidity. The long-term risk of seizures in an eclamptic patient is low; however, preeclampsia/eclampsia is associated with increased risk of cognitive decline in later life. In this article, the author reviews the clinical features, epidemiology, pathophysiology, differential diagnosis, complications, and principles of treatment.
|
• Preeclampsia is a multisystem disorder occurring after the 20th week of gestation that is characterized by hypertension, proteinuria, and pathologic edema. | |
|
• Eclampsia is defined as the occurrence of generalized seizures in a woman with preexisting preeclampsia. | |
|
• The onset of eclamptic convulsions can be antepartum, intrapartum, postpartum, or late postpartum (48 hours after delivery). | |
|
• Brain MRI reveals bilateral, symmetrical, reversible hypodense lesions in the white matter of parietooccipital regions of the brain. | |
|
• Magnesium sulfate is considered the treatment of choice. | |
|
• Reduction in eclampsia can be achieved by good prenatal care, early detection of preeclampsia, and prophylactic use of magnesium sulfate in preeclampsia. |
Ancient accounts of eclampsia and childbirth are available in medical writings of Egyptian, Indian, Chinese, and Greek civilizations. The term “eclampsia” was used by ancient Greeks. Prior to the 18th century, the term “eclampsia” was used to refer to the visual phenomenon associated with this disorder. In 1673, Mauriceau, a noted French obstetrician, gave a detailed description of the subject in his book, and he believed that eclampsia improved after delivery (19; 47). The view that salt plays a crucial role in eclampsia was given by De Snoo (1877-1949), a Dutch obstetrician. In 1840, PF Rayer, a French pathologist, for the first time noted proteinuria in pregnant women. However, the discovery of proteinuria in eclampsia was made by LC Lever of London and JY Simpson of Scotland in 1843. Lever recommended periodic testing of urine for proteinuria in pregnancy. Georg Schmorl, in 1893, first demonstrated the presence of fetal cells in the maternal body and emphasized the importance of the placenta in eclampsia (52). Until the middle of the 19th century, treatment of eclampsia was mostly by physical methods and expediting the delivery. Physical methods were bleeding by venesection, blistering, immersion in hot water, and hot compress in kidney regions. Bleeding was considered an important procedure to get rid of toxins, and a large amount of blood used to be let out. Opening of the temporal artery had been advocated for bloodletting. By the end of the 19th century, bloodletting for eclampsia had generally been abandoned, replaced chiefly by expeditious delivery as the treatment of choice. Animal experimental studies conducted at the turn of the century resulted in the use of magnesium sulfate as an anticonvulsant in humans. As early as 1906, magnesium sulfate was injected intrathecally to prevent eclamptic seizures. Because of reports that intramuscular magnesium sulfate-controlled convulsions associated with tetanus, a similar regimen was used by Lazard and Dorsett in 1926 to prevent recurrent seizures in women with eclampsia. In 1933, the drug was given intravenously to hundreds of women with preeclampsia and eclampsia at the Los Angeles General Hospital (19; 74).
Eclampsia is a serious complication of preeclampsia with a high maternal and perinatal mortality and morbidity. Preeclampsia is a multisystem disorder after the 20th week of gestation that is characterized by hypertension, proteinuria, and pathologic edema. Eclampsia is defined as the occurrence of generalized seizures in a woman with preexisting preeclampsia. Preeclampsia and eclampsia may also be accompanied by several other clinical symptoms. These include an unremitting headache, visual disturbances, right upper-quadrant pain, mid-epigastric pain, nausea and vomiting, oliguria, and shortness of breath. Each of these symptoms often heralds some potentially dangerous complications, like intracerebral hemorrhage, hypertensive encephalopathy, hepatic involvement, renal failure, and pulmonary edema (08; 47; 82). The commonly occurring visual symptoms include blurring, blindness, scotoma, and visual processing deficits. The common findings during the neurologic exam are memory deficits, visual perception deficits, visual information processing deficits, altered mental status, increased deep tendon reflexes, and cranial nerve deficits (80).
The onset of eclamptic convulsions can be antepartum (38% to 53%), intrapartum (18% to 36%), or postpartum (11% to 44%) (82). Characteristically, postpartum eclampsia occurs either before or within 48 hours of delivery. Eclampsia occurring more than 48 hours, but less than 4 weeks, after delivery is known as late postpartum eclampsia. Late postpartum preeclampsia may not present with all the classical symptoms of intrapartum preeclampsia (08; 41). Data reveal an increase in the proportion of women who develop eclampsia beyond 48 hours after delivery (82). Seizures generally precede all other manifestations of eclampsia. The seizures are usually of generalized tonic-clonic convulsion type and may be preceded by visual auras and visual hallucinations, consistent with occipital lobe seizures. Most patients experience multiple seizures in clusters, single seizures being infrequent. Following a seizure, patients usually have prolonged alterations in sensorium and activity. Eclamptic seizures are almost always self-limiting and seldom last longer than 3 to 4 minutes.
Postpartum preeclampsia or eclampsia may present without a history of preeclampsia. In a series of 22 women, over half (55%) had not been diagnosed with preeclampsia in the ante- or peripartum period (100). In this series, common prodromal symptoms and signs included headache, visual changes, hypertension, edema, proteinuria, elevated uric acid, and elevated liver function tests. Women presented from 3 to 10 days postpartum. Nineteen women presented with diastolic blood pressures higher than 90 mm Hg, and only three of these had diastolic blood pressures of 110 mm Hg or greater.
|
Preeclampsia | |
|
Hypertension | |
|
• Sustained systolic blood pressure of >=140 mm Hg; sustained diastolic blood pressure of >=90 mm Hg | |
|
Proteinuria | |
|
• Excretion of 300 mg or more of protein every 24 hours | |
|
HELLP syndrome | |
|
• Hemolysis elevated liver enzymes, and low-platelet counts | |
|
Severe preeclampsia | |
|
Hypertension | |
|
• Sustained systolic blood pressure of >=160 mm Hg; sustained diastolic blood pressure of >=110 mm Hg | |
|
Proteinuria | |
|
• Urinary excretion of 5 grams or more of protein every 24 hours, or | |
|
Oliguria | |
|
• Less than 500 ml urine every 24 hours | |
|
Clinical (any of the following can be present) | |
|
• Headache, visual disturbances, upper abdominal pain, oliguria, increased serum creatinine (1.2 mg/dl or more), thrombocytopenia (platelet count less than 100,000), increased liver enzymes, fetal growth retardation, and pulmonary edema | |
|
Eclampsia | |
|
• Presence of new-onset generalized convulsive seizures and unexplained coma in mild or severe preeclampsia | |
|
| |
Reversible posterior leukoencephalopathy is a distinctive clinico-radiological syndrome seen in patients of eclampsia. In a study, posterior reversible encephalopathy syndrome was found in over 10% of women with severe preeclampsia. Predictors of posterior reversible encephalopathy syndrome were younger age, higher systolic and diastolic blood pressures, eclampsia, and lower platelet counts (77). This syndrome is characterized by headache, vomiting, altered sensorium, visual disturbances, seizures, and rarely focal deficits, associated with characteristic white matter lesions on neuroimaging predominantly affecting the posterior regions of the brain.
Some patients may have cortical blindness and denial of blindness (Anton syndrome). In posterior leukoencephalopathy syndrome, fundus and pupillary examination reveal no abnormality. The deep tendon reflexes are often brisk, and plantars are extensor (43; 39). Posterior leukoencephalopathy syndrome can be triggered by several conditions, including preeclampsia-eclampsia, and can frequently be seen in the postpartum period. Prompt recognition and early treatment is important because failure in early recognition and treatment can produce permanent brain damage, and the syndrome of posterior leukoencephalopathy may become irreversible (40).
In eclamptic and preeclamptic patients of posterior reversible encephalopathy syndrome, a relatively higher number of brain regions are involved, and there is a tendency for basal ganglia involvement (68). A study of 113 patients with reversible posterior leukoencephalopathy syndrome reported that preeclampsia or eclampsia was the etiology in 6% (38). The levels of blood pressure elevation are usually lower in eclamptic patients with posterior leukoencephalopathy syndrome than those reported in cases of posterior leukoencephalopathy syndrome because of hypertensive encephalopathy (97).
In a study that included 47 patients, headache was the most common presenting symptom (87.2%) of posterior reversible encephalopathy syndrome followed by altered mental status (51.1%), visual disturbances (34%), and nausea/vomiting (19.1%) (16). Severe systolic hypertension was present in 22 patients (47%). Neuroimaging revealed involvement of parietal, occipital, frontal, temporal, and basal ganglia/brainstem/cerebellum areas of the brain. There are some differences between pregnant and nonpregnant patients of posterior reversible encephalopathy syndrome. Nonpregnant patients usually have a relatively higher age, higher systolic blood pressure, and higher serum creatinine levels (62). Vision impairment, primigravida status, and unbooked pregnancy are independent predictors of posterior encephalopathy syndrome in eclampsia. Posterior encephalopathy syndrome in eclampsia is associated with poorer maternal and fetal outcomes (94).
Postpartum angiopathy is a cerebral vasoconstriction syndrome of uncertain cause that affects large and medium-sized cerebral arteries. Unlike in eclampsia, neither proteinuria nor hypertension has been observed in postpartum angiopathy syndrome. Patients usually have clinical manifestations consistent with posterior leukoencephalopathy syndrome. Neuroimaging demonstrates the occurrence of ischemic stroke or intracranial hemorrhages. Magnetic resonance imaging also shows transient nonischemic brain lesions resembling the white matter lesions seen in patients with reversible posterior leukoencephalopathy syndrome (86). Cerebral angiography may reveal areas of stenosis and ectasia in multiple intracranial vessels consistent with vasculitis or reversible diffuse vasospasm (92; 86).
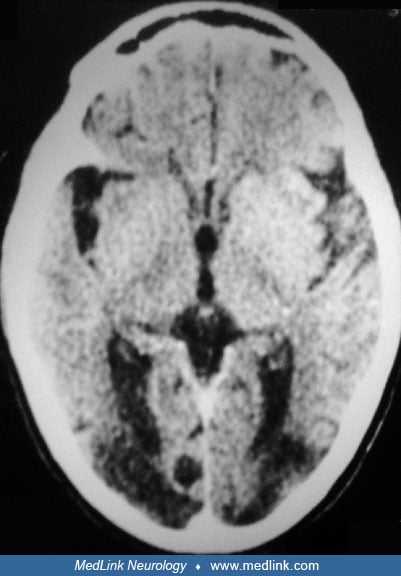
A 22-year-old primiparous woman normally delivered a normal female child at full term in a nursing home. Approximately 4 hours after delivery, the patient developed a severe diffuse bursting headache along with vomiting. Simultaneously, the patient noticed visual problems, and after a few hours, she was unable to see at all. On the next day, she had two episodes of generalized tonic-clonic convulsions at intervals of 1 hour. Immediately after her second seizure, she became confused and drowsy. Her blood pressure was 194/108 mm Hg, there was no pedal edema, and fundus examination was normal. She had complete blindness. The deep tendon reflexes were brisk and both planters were extensor. The rest of the neurologic examination, including pupillary reactions, was normal. Systemic examination did not reveal any abnormality. Her serum biochemical tests, electrocardiography, chest x-ray, and cerebrospinal fluid examination were normal. The urinalysis for protein was negative. Electroencephalography showed intermittent generalized delta activity. Computed tomography did not reveal any abnormality. Magnetic resonance imaging showed areas of abnormal signal in the cortical and subcortical white matter of occipital regions.
Antihypertensive treatment was immediately begun in the form of nifedipine (10 mg three times a day) along with furosemide (40 mg daily given orally). Advice was sought from an obstetrician who recommended that magnesium sulfate therapy be given immediately. Magnesium sulfate was administered in an initial 6 g intravenous bolus followed by intravenous infusion for 48 hours. The patient experienced no further seizures. On the 12th day after delivery, the patient was discharged with a blood pressure of 130/86 mm Hg and markedly improved vision, and he was seizure-free. Repeat magnetic resonance study 7 days after the discharge from the hospital was normal.
The overall maternal death rate varies from 0.4% to 7.2% in developed countries; the mortality rate may be as high as 25% in developing countries (01). The high maternal mortality reported from developing countries was noted primarily among patients who had multiple seizures outside the hospital and those without proper prenatal care. In addition, women who develop preeclampsia or eclampsia are at increased risk for a number of complications. A placental abruption is the most common complication encountered. HELLP syndrome can complicate up to 10% of eclamptic cases. Mortality resulting from the HELLP syndrome ranges from 2% to 24% of cases. Other potential maternal risks include intracranial hemorrhage, cardiopulmonary compromise with pulmonary edema, liver or renal failure, microangiopathic hemolytic anemia, and disseminated intravascular coagulation. Pulmonary edema and aspiration pneumonia often develop as a result of intravenous fluid overload and poor fluid and electrolyte management (96). Fetal complications include prematurity, growth restriction, placental insufficiency, and death (12; 82). Intracerebral hemorrhage, the most serious complication, has been shown to be fatal in 50% to 65% of the cases. Retinal detachment can also occur after an eclamptic seizure. A sudden increase in diastolic blood pressure above 120 mm Hg heightens the risk of death and the development of acute cardiovascular complications such as hypertensive encephalopathy, ventricular arrhythmias, and congestive heart failure.
Children exposed to mothers’ preeclampsia have a slightly increased risk of febrile convulsions, but the association is apparently caused by a shorter gestation in preeclamptic women. Eclampsia may be a risk factor for hippocampal sclerosis and temporal lobe epilepsy in later life (95; 53).
In women with eclampsia, the relative risk of long-term seizures is higher in comparison with unaffected women. However, the absolute risk of long-term seizures is low (approximately one seizure per 2200 person-years) (70).
Barber and colleagues systematically analyzed published reports on long-term seizure recurrence risk after eclampsia (11). Data on 1896 women were analyzed; only seven (0.37%) women had another seizure. The authors concluded that the risk of long-term seizure recurrence is low in women with eclampsia.
Mielke and colleagues examined the impact of hypertensive disorders of pregnancy on later-life cognition in 2239 women (66). The study found no immediate cognitive differences in women with any hypertensive disorders of pregnancy, but those with a history of preeclampsia/eclampsia showed greater cognitive decline over time, particularly in global cognition, language, and attention. Nulliparous women, especially those with less education, had lower cognitive performance. These findings suggest a specific long-term cognitive risk associated with preeclampsia/eclampsia (66).
Localization. Eclampsia is considered to evolve from preexisting preeclampsia. Eclampsia, however, may manifest without signs of preceding preeclampsia. It has been reported that up to 38% of eclamptic seizures occur without previous signs and symptoms (69). Eclampsia may present at various gestational ages, with the majority occurring in the third trimester of pregnancy. Infrequently, atypical eclampsia has been observed at or earlier than 20 weeks gestation; in such a situation a diagnosis of hydatidiform molar pregnancy or hydropic degeneration of the placenta should be considered. Despite intense efforts, the precise etiology of preeclampsia and eclampsia remains unknown. From time to time, a number of theories have been put forward to explain the etiopathogenesis of toxemia in pregnancy. These theories include placental abnormalities, immunologic disturbances, endothelial cell dysfunction, oxidant-antioxidant system, genetic susceptibility, and dietary influences. Several studies have demonstrated that the risk of preeclampsia and eclampsia is increased in women with a previous history of preeclampsia, the presence of antiphospholipids antibodies, diabetes mellitus, multiple (twin) pregnancy, nulliparity, family history of toxemia of pregnancy, raised blood pressure (80 mm Hg or greater) at booking, obesity, or maternal age of 40 years or more (for multiparous women). Several other studies have revealed that the risk of toxemia in pregnancy is also increased with an interval of 10 years or more since a previous pregnancy, autoimmune disorders, renal impairment, and chronic hypertension (28). Hereditary thrombophilic conditions most strongly associated with adverse pregnancy outcomes include factor V Leiden, prothrombin gene mutation, and deficiencies of protein S, protein C, protein Z deficiency, and antithrombin. Although the familial aspect has been recognized for some patients, the exact gene and the pattern of inheritance are not known.
Genetic susceptibility may play an important role in the pathogenesis of eclampsia. For example, Glu298Asp polymorphism in the eNOS gene could be an individual's risk factor and may modulate the progression to eclampsia in patients with preeclampsia in the Turkish population (72).
Because preeclampsia is primarily a disorder of pregnancy, and its symptoms resolve after delivery, the placenta is considered the primary site of pathology. In normal pregnancies, the uteroplacental arteries are invaded by trophoblast cells. Endovascular trophoblast cells initially replace the endothelium of spiral arteries of the uterus and then invade the media, resulting in the destruction of the medial elastic, muscular, and neural tissues. This trophoblast migration transforms the small, musculoelastic spiral arteries into large bore (tenfold increase in diameter) sinusoidal vessels enabling adequate perfusion of the placenta with maternal blood. These physiological changes help provide an adequate supply of nutrients and oxygen to the placenta and fetus. The growth factors, vascular endothelial growth factor, epidermal growth factor, and fibroblast growth factor are placental growth factors that activate degradation of the extracellular matrix, and specific growth factors modulate the invasive potential of trophoblasts and, therefore, may play an important role in early placental development (09).
In preeclampsia, the trophoblastic invasion of the uterine spiral arteries is incomplete, and vessels remain thick-walled and muscular. This failure of the normal cardiovascular changes of pregnancy results in hypertension, reduction in plasma volume, and impaired perfusion to virtually every vital organ of the body (17; 49). In preeclampsia, there is diffuse vasospasm and activation of platelets and the coagulation system, resulting in extensive microthrombi formation. In addition, placental ischemia or hypoxia also produces widespread dysfunction of the maternal vascular endothelium, which results in enhanced formation of endothelin, thromboxane, and superoxide, increased vascular sensitivity to angiotensin-II, and decreased formation of vasodilators such as nitric oxide and prostacyclin. The concentration of tumor necrosis factor-alpha, an inflammatory cytokine produced by macrophages, has been observed to be significantly increased in blood. Tumor necrosis factor-alpha overproduction by the placenta also contributes to endothelial dysfunction. These endothelial abnormalities, in turn, cause hypertension by producing renal dysfunction and increasing peripheral vascular resistance (60; 82).
Preeclampsia may have an immunological basis. Human leukocyte antigen-G is thought to play an important role in maintaining a local immunosuppressive state and the maternal acceptance of the semiallogenic fetus. Thus, it plays an important role in fetal protection. Human leukocyte antigen-G is expressed by extravillous cytotrophoblast cells in the fetus-maternal contact zone. Aberrant human leukocyte antigen-G expression may result in pregnancy disorders, including preeclampsia. Natural killer cells are identified morphologically as lymphocytes but functionally as one component of the innate immune system. Natural killer cells are the most abundant lymphocyte population at the maternal-fetal interface. Natural killer cells instead of T cells are suggested to be important during placentation by controlling trophoblast invasion. Decreased expression of human leukocyte antigen-G leads to an abnormal interaction with decidual natural killer cells, resulting in an excessive maternal inflammatory response directed against foreign fetal antigens. Consequently, there is a chain of changes in the placenta, including defective transformation of spiral arteries, hypoxia, thrombosis, infarction of the placenta, and release of proinflammatory cytokines and placental fragments in the systemic circulation (18; 67; 78).
Apoptosis plays an important role in the normal development, remodeling, and aging of the placenta. It has been demonstrated that the amount of apoptosis increases as pregnancy progresses, suggesting that it is a normal physiological phenomenon throughout gestation. Regulation of apoptotic events is important to allow correct development, differentiation, and function of the placenta throughout pregnancy, and an unbalance of this process leads to severe pathologies such as preeclampsia and intrauterine growth retardation. Deficient apoptosis may induce a maternal immune response against the fetus, and enhanced apoptosis may interfere with the process of placentation, placental ischemia, and subsequently, systemic endothelial damage (23; 44).
It has been demonstrated that preeclampsia may be caused by an imbalance of angiogenic factors. High serum levels of soluble fms-like tyrosine kinase-1, an antiangiogenic protein, and low levels of placental growth factor, a proangiogenic protein, predict subsequent development of preeclampsia (55). Limited data suggest that excess circulating soluble fms-like tyrosine kinase-1, which binds placental growth factor and vascular endothelial growth factor, may have a pathogenic role.
The exact etiopathogenesis of seizures in eclampsia is not known with certainty. Neurologic complications of eclampsia are thought to be similar to those of hypertensive encephalopathy, in which a rapid elevation in blood pressure causes disruption of the blood-brain barrier and development of cerebral edema. This rapid rise in blood pressure overcomes the brain's normal autoregulatory mechanisms of cerebral blood flow. Disturbance of autoregulation produces dilatation of cerebral arterioles with the opening of endothelial tight junctions and leakage of plasma and red cells into the extracellular space, producing cerebral edema (43; 39). It has been suggested that pregnancy and the postpartum period predispose the cerebral circulation to forced dilatation of intrinsic myogenic tone of cerebral arteries and arterioles at lower pressures, a response that may lower cerebrovascular resistance and promote hyperperfusion when blood pressure is elevated (21). Results of another experimental study also suggest a pregnancy-specific effect on the cerebral endothelium that may promote enhanced vascular permeability during acute hypertension and may contribute to the edema formation and neurologic complications of eclampsia (20). Nitric oxide has been suggested as a potential mediator of transient blood-brain barrier breakdown that leads to vasogenic edema and secondary brain damage (58).
The cerebral white matter is composed of myelinated fiber tracts in a cellular matrix of glial cells, arterioles, and capillaries that make this structure more susceptible to accumulation of fluid in the extracellular spaces (43; 39). Adrenergic sympathetic innervation of cerebral vessels is an important component in the physiological mechanism of cerebral blood flow autoregulation. The vessels of the carotid system are better supplied with sympathetic adrenergic innervation than those of the vertebrobasilar system. This inherent deficiency of adrenergic innervation may result in a loss of vasoconstrictor properties of cerebral blood vessels, mainly in the posterior cerebral areas. Using magnetic resonance imaging in preeclamptic women with neurologic symptoms, it was demonstrated that the presence of brain edema was associated with abnormal red blood cell morphology and elevated lactate dehydrogenase levels. This suggested that microangiopathic hemolysis and endothelial damage were present, and endothelial damage may have resulted in a disturbed autoregulatory system (79). The recent studies on hypertensive disorders of pregnancy emphasizes the impact of conditions like preeclampsia on the blood-brain. Studies show increased perivascular macrophage activity, extracellular vesicles, and impaired cerebral blood flow autoregulation in hypertensive disorders of pregnancy (48).
According to the vasospasm hypothesis, patients with posterior leukoencephalopathy develop vasospasm secondary to sudden and severe rises in blood pressure and ischemia of brain tissue. Ischemic damage to brain tissue first produces cytotoxic edema and then extracellular edema and infarction.
Coronavirus infection (COVID-19), which is caused by SARS-CoV-2, has led to a pandemic affecting all continents of the world. Many reports have indicated that COVID-19 adversely affects pregnant women. Mendoza and colleagues presented data that support a link between SARS-CoV-2 infection and the occurrence of a preeclampsia‐like syndrome (65). On review of 42 pregnancies with COVID-19, the authors noted that five women with severe COVID-19 had preeclampsia‐like syndrome. In one case, recovery from severe pneumonia led to a reversal of the preeclampsia‐like syndrome.
Cellular entry of SARS‐CoV‐2 is mediated by angiotensin-converting enzyme 2 receptor. It has been hypothesized that pregnancy enhances the expression of the angiotensin-converting enzyme 2 receptor. Demonstration of SARS‐CoV‐2 in the placenta suggests that SARS‐CoV‐2 can adversely affect pregnancy (93).
Over half a million women worldwide die each year from pregnancy-related causes; the majority of them are from low- and middle-income countries. Approximately 10% to 15% of maternal deaths are associated with preeclampsia and eclampsia. Perinatal mortality is high following preeclampsia and even higher following eclampsia (29). Preeclampsia affects up to 7% of pregnancies, and less than 1% of these women with preeclampsia develop eclampsia (98; 56). The national incidence of eclampsia in the United Kingdom in the early nineties was found to be 4.9 per 10,000 maternities. Most convulsions occurred despite good antenatal care (70%) and within 1 week of the woman's last visit to a doctor or midwife (85%). Three quarters of first seizures occurred in the hospital, of which 38% developed before both proteinuria and hypertension had been documented. Forty-four percent of cases occurred postpartum, more than a third (38%) antepartum, and the remainder (18%) intrapartum (27). In a 5-year prospective study involving 16 maternity units in Yorkshire, a total of 210,631 women delivered babies between 1999 and 2003 (90). One thousand eighty-seven women were diagnosed with severe preeclampsia or eclampsia (5.2 per 1000). One hundred and fifty-one women had serious complications, including 82 women (39 per 10,000) who had eclamptic seizures and 49 women (23 per 10,000) who required intensive care. In a study from Scotland, authors identified 4188 patients with preeclampsia in 20 years (1981 to 2000), and the percentage of eclampsia was 1.6% (15). The incidence of eclampsia and its complications have decreased significantly in the United Kingdom since 1992 following the introduction of management guidelines for eclampsia and preeclampsia. A study including all women delivering between 2005 and 2006 revealed the incidence of eclampsia as 2.7 cases per 10,000 births (50). Thirty-eight percent of women had established hypertension and proteinuria in the week before their first fit. No women in the study died. Fifty-four women (26%) had recurrent fits.
In the United States, the incidence of eclampsia decreased from 8.0 cases per 10,000 deliveries in 2001 to 5.6 cases per 10,000 deliveries in 2007 (36). Non-Hispanic blacks were associated with the highest risk of eclampsia, whereas Asians had the lowest risk. Several antepartum diseases had increased associations with eclampsia, including preexisting cardiac disease, lupus erythematosus, and twin gestations. Peripartum medical complications that are increased in eclampsia include cerebrovascular hemorrhage and disorders, peripartum cardiomyopathy, amniotic fluid embolism, and venous thromboembolism. The latest data from the United States indicated that between the years 2009 to 2017, the risk of eclampsia declined by 10% (99). Between 2009 and 2017, 83,000 (0.30%) of 27,866,714 live births were associated with eclampsia. In comparison to 2009, the risk of eclampsia in 2017 was significantly less among women with chronic hypertension and those with hypertensive pregnancy disorders. However, there was a marginal increase in the risk of eclampsia in normotensive women in 2017 versus that in 2009.
According to a report from Finland, 46 women with eclampsia were identified out of 295,447 registered deliveries from 2006 to 2010 (46). The incidence of eclampsia was 1.5 per 10,000 deliveries. No maternal deaths due to eclampsia were recorded, but 46% of the women had severe complications. Eighty-seven percent of the women with eclampsia received magnesium sulfate for treatment. Seven percent of the women received magnesium sulfate for the prevention of eclampsia. The perinatal mortality rate was 8%. In another study from Nova Scotia, the authors noted that among 142,362 births, 39 women developed eclampsia (0.27 per 1000) (54). For the period 1988 to 2000, the prevalence of severe preeclampsia fell from 2.08% to 1.63%, and the diagnosis of HELLP syndrome increased from 0.03% to 0.31%. Sixty-one percent of first convulsions were noted during the antepartum period, 13% of seizures occurred intrapartum, and 26% occurred during the postpartum period. In a population-based study from Australia, 10,379 (4.2%) of 250,173 women had preeclampsia and 731 (0.3%) had chronic hypertension with superimposed preeclampsia (75). Almost all cases (91%) of eclampsia develop at or beyond 28 weeks. The remaining cases occur between 21 and 27 weeks of gestation (7.5%) or at 20 weeks of gestation or earlier (1.5%).
In poor countries, the incidence of eclampsia is high. In Dar es Salaam, Tanzania, hospital- and population-based incidences of eclampsia are 200 per 10,000 and 67 per 10,000, respectively (91). Human immunodeficiency virus infection treated with highly active antiretroviral therapy prior to pregnancy is associated with a significantly higher risk for preeclampsia and fetal death (88). Nigerian authors conducted a retrospective study of the management and outcome of eclampsia patients in the intensive care unit between November 2001 and April 2005 (71). During the study period, there were a total of 4857 deliveries with 5051 total births (including multiple births) and 4854 live births. Forty eclamptic patients were admitted to the intensive care unit, giving an intensive care unit admission rate of 8.2 per 1000 live births. Twenty patients (52.6%) had antepartum eclampsia, 12 (31.6%) had postpartum eclampsia, and six (15.8%) presented with intrapartum eclampsia. There were 11 maternal deaths, giving a case fatality rate of 29%.
The risk of eclampsia was greater in nulliparous compared to parous women. A young age (younger than 20 years) or an older mother (older than 35 years), longer birth interval, low socioeconomic status, gestational diabetes, prepregnancy obesity, and weight gain during pregnancy were positively associated with eclampsia (22).
Tantillo and colleagues retrospectively analyzed factors associated with seizure- and epilepsy-related readmissions in women who were initially admitted for delivery (89). The authors analyzed data for 633,714 index admissions. A 30-day readmission rate for seizures and epilepsy was 19.69 per 100,000 index admissions, with a total of 295 readmissions. Of these, 236 were leveled as eclampsia; in 59 cases, seizures were due to other causes. The mean number of days to readmission after delivery was 6.43 days. Lower-income quartile, preexisting epilepsy, preeclampsia, and eclampsia predicted the risk of readmission.
A significant percentage of eclampsia cases are potentially preventable by patient education or health care response. In fact, the marked reduction in the incidence of eclampsia in developed countries over the years can be attributed to good prenatal care, early detection of signs and symptoms of preeclampsia, and prophylactic use of magnesium sulfate during labor and after delivery in women with preeclampsia. An adequate diet and iron and folic acid supplementation in pregnancy were associated with a reduced occurrence of symptoms of preeclampsia or eclampsia in Indian women (04). Antiplatelet agents, largely low-dose aspirin, have moderate benefits when used for the prevention of preeclampsia. A 17% reduction in the risk of preeclampsia associated with the use of antiplatelet agents has been reported (10; 33).
Early combined treatment of critically raised blood pressure with intravenous antihypertensive drugs and magnesium sulfate is associated with a reduction in the frequency of eclampsia and severe maternal morbidity. In a study, early treatment with intravenous blood pressure medication and magnesium sulfate for sustained critical maternal blood pressure resulted in a significant reduction in the rate of eclampsia and severe maternal morbidity (81). The authors thought that an additive or synergistic effect of the combined treatment of antihypertensive medication and magnesium sulfate had a significant impact on the rate of eclampsia and severe maternal morbidity.
However, concomitant supplementation with vitamin C and vitamin E does not prevent preeclampsia in women at risk but does increase the rate of babies born with a low birth weight (73). Evidence from the latest Cochrane review does not support routine antioxidant administration during pregnancy to reduce the risk of preeclampsia and other serious complications in pregnancy (76).
Several clinical symptoms are potentially helpful in establishing the diagnosis of eclampsia. These symptoms may occur before or after the onset of convulsions, and they include persistent occipital or frontal headaches, vision loss, photophobia, epigastric or right upper-quadrant pain, and altered sensorium. A systemic review tried to analyze all predictive signs and symptoms that can occur before the onset of eclampsia in a preeclamptic lady and noted that visual disturbances, epigastric pain, headache, and edema are four of the most frequent heralding symptoms (42).
Eclampsia is rare after 48 days after delivery, and in such a situation a diagnosis is needed to rule out the presence of other brain disorders. In late postpartum eclampsia, manifestations are often nonspecific. Headache is usually a dominant clinical feature and often is without a significant rise in blood pressure (13). The common differential diagnosis of seizures late in the postpartum period includes cerebral venous thrombosis, intracerebral hemorrhage, hypertensive encephalopathy, space-occupying lesions of the brain, and metabolic disorders such as hypoglycemia and hyponatremia. In developing countries, infectious diseases like bacterial meningitis, acute viral hepatitis with fulminant hepatic failure, and cerebral malaria are important causes of late puerperal seizures. Acute intermittent porphyria produces seizures and hypertension closely mimicking eclampsia. Lumbar puncture should always be performed if meningitis is suspected. Imaging studies of the brain are recommended when persistent coma or focal neurologic deficit is present. Neurocysticercosis should be considered in the differential diagnosis of pregnant patients with coma and seizures, especially if the patient is a resident of an endemic area or has emigrated from or traveled to an endemic area (87).
Cerebral infarcts and hemorrhages are uncommon but serious complications of pregnancy. The majority of strokes are seen in the third trimester and postpartum period. Cerebral infarcts and hemorrhages are caused either by reversible cerebral vasoconstriction syndrome, preeclampsia/eclampsia, or cerebral venous thrombosis (85).
|
• Cerebrovascular events |
Limited data suggest that excess circulating soluble fms-like tyrosine kinase-1, which binds placental growth factor and vascular endothelial growth factor, may have a pathogenic role. Increased levels of fms-like tyrosine kinase-1 and reduced levels of placental growth factor predict the subsequent development of preeclampsia (55). Decreased urinary placental growth factor at midgestation is strongly associated with the subsequent early development of preeclampsia.
Abnormal electroencephalographic findings are frequent in preeclamptic-eclamptic patients. Electroencephalographic findings in such patients are not altered by serum magnesium levels achieved in the clinical management of these patients. In a series, electroencephalograms were recorded in 36 eclamptic, 14 preeclamptic, and 13 normotensive control patients. Twenty-seven eclamptic patients had abnormal electroencephalographic studies, four patients showed paroxysmal spike activity, and the others showed focal or diffuse slowing (delta waves). Seven preeclamptic women had abnormal electroencephalographic studies (all had generalized slowing). In preeclamptic-eclamptic patients who had serial electroencephalographic recordings, the gross electroencephalographic findings obtained during magnesium sulfate infusion and in the absence of magnesium sulfate were similar (84).
Early computed tomography reveals bilateral, often symmetrical, reversible hypodense lesions in the white matter of parieto-occipital regions of the brain. It is not uncommon to find a normal computed tomography.
The neuroimaging hallmark of eclampsia is reversible parieto-occipital white matter signal abnormalities as seen on magnetic resonance imaging.
Specific magnetic resonance techniques, such as FLAIR and diffusion-weighted image sequences, have improved the ability to identify subcortical or cortical lesions and help to clarify the underlying pathophysiological mechanisms. Diffusion-weighted magnetic resonance imaging differentiates between cytotoxic and vasogenic cerebral edema in a patient with eclampsia. Typical brain lesions predominate in the posterior white matter with some involvement of the overlying cortex. Lesions are hyperintense on T2-weighted images and are usually hypointense or isointense on diffusion-weighted images, with an increase in the apparent diffusion coefficient, indicating vasogenic edema. Cytotoxic or ischemic edema is characterized by restricted water diffusion and appears markedly hyperintense on diffusion-weighted images and hypointense on apparent diffusion coefficient maps (58). In a study, 27 nulliparous women with eclampsia were evaluated with diffusion-weighted magnetic resonance imaging and apparent diffusion coefficient mapping (101). Those with findings of restricted diffusion suggestive of cytotoxic edema underwent neuroimaging again 6 weeks postpartum. All but two of these 27 women had reversible vasogenic edema. Six were also found to have areas of cytotoxic edema consistent with cerebral infarction. Five of these six women had persistent imaging findings of infarction when studied postpartum, however, without clinical neurologic deficits.
Neuroimaging should always be performed in pregnant women with recent onset of neurologic manifestations irrespective of the development of eclampsia (64). A variety of other neuroimaging abnormalities can also be encountered. In a study of 41 patients with eclampsia, 36 (89%) had abnormal neuroimaging findings, including cerebral edema, cerebral infarction, cerebral venous thrombosis, and cerebral hemorrhage (25). Of the 38 cases of severe preeclampsia, 21 (55%) cases had abnormal neuroimaging. Twenty patients had cerebral edema, and one case had a cerebral hemorrhage.
Magnesium sulfate is considered to be the agent of choice for the control of recurrent eclamptic seizures in pregnant women. Magnesium sulfate is also the first-line agent for prophylaxis of seizures in eclampsia and preeclampsia. Severe preeclampsia should be treated with magnesium to prevent progression to eclampsia. The mechanisms of action of magnesium sulfate are still not clear. Magnesium sulfate is considered to act as a peripheral and central vasodilator to decrease peripheral vascular resistance or relieve vasoconstriction. Additionally, magnesium sulfate may also protect the blood-brain barrier and limit cerebral edema formation. Magnesium sulfate has a potent central anticonvulsant action as well (35).
In 1995, the efficacy of magnesium sulfate in eclampsia was established in a landmark trial. The Eclamptic Trial Collaborative Group randomized 910 women at 23 centers in eight countries to receive magnesium sulfate or diazepam. This study unequivocally showed that magnesium sulfate given intramuscularly or intravenously is superior to phenytoin or diazepam in reducing recurrent eclamptic seizures. Seizures were a half or a third less likely to recur after treatment with magnesium. In women assigned to the magnesium group, 5.7% had recurrent seizures compared with 17.1% in those assigned to receive phenytoin (07). Another study comparing magnesium sulfate with phenytoin for the prevention of eclamptic seizures in women with the diagnosis of severe preeclampsia revealed that magnesium was superior to phenytoin for prophylaxis against eclamptic seizures (59). In this study, a total of 2138 women were randomized to receive magnesium or phenytoin after preeclampsia was diagnosed on admission in labor. Magnesium sulfate was administered at an initial dose of 5 g in each hip, and then 5 g every 4 hours. Reflexes and respirations were checked before each dose. Magnesium was continued until 24 hours after delivery. Phenytoin was given by intravenous infusion of 1000 mg over 1 hour, followed by a 500-mg extended-release capsule 10 hours later. Ten of the 1089 women assigned to receive phenytoin experienced eclamptic seizures compared with no patients in the magnesium group.
In a Cochrane review, authors assessed the effects of magnesium sulfate compared with phenytoin. Seven randomized controlled trials involving 972 women are included. For women with eclampsia, magnesium sulfate, rather than phenytoin, reduces the risk ratio of recurrence of seizures, probably reduces the risk of maternal death, and improves outcomes for the baby (32). The authors concluded that magnesium sulfate should be considered the drug of choice for women with eclampsia. The use of phenytoin should be abandoned. In another Cochrane review, magnesium sulfate was demonstrated to be substantially more effective than diazepam for the treatment of eclampsia (34). In a later review, the same group of authors assessed the effects of magnesium sulfate compared with a lytic cocktail (comprised of chlorpromazine, promethazine, and pethidine) (30). These authors suggested that for women with eclampsia, magnesium sulfate, rather than a lytic cocktail, reduces the risk ratio of maternal death, of further seizures, and of serious maternal morbidity (respiratory depression, coma, pneumonia). It was concluded that the use of a lytic cocktail should be abandoned.
Severe preeclampsia should also be treated with magnesium sulfate to prevent progression to eclampsia. In another landmark magnesium sulfate for Prevention of Eclampsia (Magpie) trial, 10,141 women with preeclampsia were randomized to receive magnesium sulfate before or during labor or after giving birth, in 33 countries. About two thirds of the women in this study were from developing countries with high or moderate perinatal mortality. Follow-up data were available for 10,110 (99.7%) women, 9992 (99%) of whom received the allocated treatment. Women allocated magnesium sulfate had a 58% lower risk of eclampsia than those allocated placebo (11 fewer women with eclampsia per 1000 women). Maternal mortality was also lower among women allocated magnesium sulfate. Twenty-four percent of women given magnesium sulfate reported side effects versus 228 of 4993 (5%) given placebo (05). A Cochrane analysis reviewed the effects of magnesium sulfate and other anticonvulsants for prevention of eclampsia (31). The authors noted that magnesium sulfate reduces the risk of eclampsia by more than one half and probably reduces maternal death. The main side effect was flushing. Nimodipine is a calcium channel blocker with specific cerebral vasodilator activity. Magnesium sulfate is more effective than nimodipine for prophylaxis against seizures in women with severe preeclampsia (14).
There is no definite place of magnesium sulfate in the management of mild preeclampsia because the rate of seizures in women with mild preeclampsia not receiving magnesium sulfate is low. To determine whether magnesium sulfate prevents disease progression in women with mild preeclampsia to severe eclampsia or eclampsia, a total of 222 women with mild preeclampsia were randomized to receive intravenous magnesium sulfate (n = 109) or matched placebo (n = 113). Fourteen women (12.8%) in the magnesium group and 19 (16.8%) in the placebo group developed severe preeclampsia after randomization. None in either group developed eclampsia or thrombocytopenia (57).
The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine recommend only short-term (usually less than 48 hours) use of magnesium sulfate in obstetric care, which includes the prevention and treatment of seizures in women with preeclampsia or eclampsia, fetal neuroprotection before anticipated early preterm (less than 32 weeks of gestation) delivery, and short-term prolongation of pregnancy (up to 48 hours) to allow for the administration of antenatal corticosteroids in pregnant women between 24 weeks of gestation and 34 weeks of gestation who are at risk of preterm delivery within 7 days (06).
Magnesium sulfate is administered most commonly as a continuous intravenous infusion at rates of 2 to 3 grams per hour after an intravenous loading bolus of 4 to 6 grams. Alternatively, an intramuscular regimen can be used with a loading dose of 5 g intramuscular into each buttock, followed by 5 g every 4 hours after assessment of respirations, urine output, and deep tendon reflexes. Magnesium sulfate treatment is frequently started before delivery and continued for varying periods, usually 12 or 24 hours after delivery (82). The onset of diuresis in the postpartum period may be used as a clinical determinant for the discontinuation of magnesium sulfate therapy in patients with severe preeclampsia (45; 37). In one study, a low-dose regimen of magnesium sulfate appeared comparable to the “standard dose regimen” (02). Thirty-nine patients randomized into the low-dose regimen group received a loading dose of 9 g (4 g intravenous and 5 g intramuscular) and intramuscular maintenance of 2.5 g every 4 hours for 24 hours after delivery or after the last fit, whereas the 33 patients in the standard-dose regimen group received a loading dose of 14 g followed by an intramuscular maintenance dose of 5 g every 4 hours. In both study groups, 2 g intravenous of magnesium sulfate was given for breakthrough fits, and 10 ml of 10% calcium gluconate (slowly intravenous) was administered in the event of toxicity. Postdelivery diuresis heralds the reversal of the pathophysiologic abnormalities in this disorder. Polypharmacy should be avoided in patients with eclampsia because medically induced alterations in mental status may make it more difficult to evaluate changes in patient status. In patients with eclampsia, mannitol was not found superior to magnesium sulfate in achieving neurologic recovery. Magnesium sulfate remains the agent of choice for the treatment of posterior reversible encephalopathy syndrome (24). A Cochrane review evaluated various magnesium sulphate regimens for preventing and treating eclampsia. It included 16 trials with 3020 women, mainly from low- and middle-income countries. The review found very low-certainty evidence on the effectiveness of different regimens in reducing convulsions, morbidity, and mortality in women with eclampsia or preeclampsia. Due to limited high-quality data, no regimen was conclusively more effective than others (26).
The potential neuromuscular junction-blocking effect of magnesium sulfate is an important consideration. Magnesium competes with calcium in the process of trans-synaptic transmission of nerve impulses. Korn and colleagues reported two women who developed a pseudo-coma state immediately after emergency cesarean sections. Pseudo-coma was characterized by lower motor neuron quadriparesis, ophthalmoplegia, absent respiratory effort, and vestibular-ocular reflexes. Pupillary responses were well preserved. Magnesium sulfate was inadvertently continued throughout surgery in place of normal saline. Administration of calcium gluconate reversed the condition within 15 minutes. Another woman with undiagnosed myasthenia gravis developed exacerbations of clinical manifestations of myasthenia following treatment with magnesium sulfate. She was treated with plasmapheresis, immunosuppressive treatment, and thymectomy with full recovery (51).
Blood pressure higher than 160/110 mm Hg is generally treated with intravenous antihypertensive agents such as labetalol, hydralazine, or nifedipine. No single antihypertensive has been proven to be better than another, although hydralazine is probably the initial intravenous agent of choice. Sodium nitroprusside should be avoided in most neurologic emergencies because of its tendency to raise intracranial pressure. The starting dose is usually 5 mg given intravenously followed by a subsequent dose of 5 to 10 mg every 20 to 30 minutes as needed. Another agent commonly used in severe hypertension is the intravenous form of labetalol. Nifedipine can also be used in the treatment of acute hypertension.
Delivery remains the definitive treatment for preeclampsia, but there may be initial deterioration after birth, especially in HELLP syndrome. In the eclamptic patient, delivery should be undertaken after stabilization of the patient. The route of delivery is dictated by other obstetric indications. Cervical ripening agents and induction of labor are not contraindicated. Evaluation of maternal and fetal status must be done before proceeding with induction. A report described two patients with refractory late postpartum eclampsia; these patients had rapid recovery following uterine curettage (63).
Although general anesthesia can be safely used in preeclamptic women, it is fraught with greater maternal morbidity and mortality. Currently, the safety of regional anesthesia techniques is well established, and they can provide better obstetrical outcomes when chosen properly. Thus, regional anesthesia is extensively used for the management of pain and labor in women with preeclampsia. This article highlights the advantages and disadvantages of regional anesthetic techniques, including epidural, spinal, and combined spinal-epidural analgesia used as a part of the management of preeclampsia (61).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Ravindra Kumar Garg DM FRCP
Dr. Garg of King George's Medical University in Lucknow, India, has no relevant financial relationships to disclose.
See Profile
Solomon L Moshé MD
Dr. Moshé of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Apr. 22, 2024
Epilepsy & Seizures
Mar. 22, 2024
Epilepsy & Seizures
Mar. 20, 2024
Epilepsy & Seizures
Mar. 11, 2024
Epilepsy & Seizures
Mar. 07, 2024
Epilepsy & Seizures
Mar. 06, 2024
Epilepsy & Seizures
Mar. 05, 2024
Epilepsy & Seizures
Mar. 05, 2024