


Neuro-Oncology
Atypical teratoid/rhabdoid tumors
Mar. 21, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author reviews the etiology, diagnosis, and management of vestibular schwannomas. Particular attention is given to treatment controversies, including the role of observation, surgery, and stereotactic radiosurgery/fractionated radiosurgery in the management of these tumors. The molecular etiology of these tumors is reviewed as new developments may lead to new medical treatment options for these tumors. Data on the role of noise exposure and the controversial role of cell phones in the development of vestibular schwannoma are reviewed.
|
• Treatment options for vestibular schwannomas are rapidly evolving as new outcome data relevant to tumor control and quality of life are reported. | |
|
• The molecular etiology of these tumors is being elucidated and may soon lead to novel medical treatments. | |
|
• The causative role of cell phone usage as a cause of vestibular schwannoma continues to be controversial. |
Previously, and incorrectly, called acoustic neuromas, vestibular schwannomas (acoustic schwannoma, acoustic neurinoma) are histologically benign neoplasms of Schwann cell origin arising from the vestibular branches of the eighth cranial nerve. Tumors originate distal to the point at which the oligodendroglial cells are replaced by Schwann cells, usually within the internal auditory canal. The majority of all schwannomas (85% to 90%) arise from the vestibular branches of cranial nerve VIII. Rarely, tumors can develop from the cochlear branch.
The tumor was described pathologically by Sandifort in 1777, but it was not for over a century that the diagnosis was first made clinically. The first successful removal was performed in 1894. However, early surgical approaches to these tumors were almost always fatal. Mortality in Henschen's series from 1910 was 85% (156). Improvements in surgical and anesthetic technique dropped this figure to 4% in Cushing's hands (81). It should be noted that Cushing restricted surgery to intracapsular decompression, believing total tumor excision to be too hazardous. Walter Dandy successfully added careful dissection of the residual capsule from surrounding structures and extirpated several acoustic tumors. The use of microsurgical techniques, a variety of surgical approaches, neurophysiological electrical monitoring, and improved neuroanesthesia have shifted the focus from patient survival to preservation of cranial nerve function.
The most common symptoms of vestibular schwannomas are unilateral sensorineural hearing loss (96%), unsteadiness (77%), tinnitus (71%), headache (29%), mastoid pain or otalgia (28%), facial numbness, diplopia, and vertigo (280; 183; 404; 248; 263). Publications have classified symptoms into four stages: intracanalicular, cisternal, brainstem compressive, and hydrocephalic (427). In the intracanalicular stage, the symptoms are hearing loss, tinnitus, and vertigo. In most patients the initial symptom is unilateral sensorineural hearing loss, which may have been present from 1 to 5 years (mean 3.7 years) (405; 263). The loss is gradually progressive in 80% to 90% of cases and sudden in 10% to 20% of cases (possibly caused by occlusion of the internal auditory artery). Sensorineural hearing loss develops from a combination of tumor-induced interference with cochlear vascular supply and compression of the cochlear nerve within the internal auditory canal. Mild unsteadiness is usually not the initial complaint but has been present for several years in most patients. Tinnitus is usually unilateral, confined to the affected ear, low grade in intensity, and constant. Tinnitus at presentation has been reported to increase the likelihood of subsequent tumor growth by 3-fold (05).
In the cisternal stage, auditory symptoms progress and headaches often occur (427). Headache, mastoid pain, and otalgia are often present in patients with larger tumors that impinge on local dural and osseous structures or have caused elevated intracranial pressure. Facial numbness is usually confined to the lower face; facial weakness is uncommon. Symptomatic paroxysmal vertigo is infrequent and is usually not accompanied by nausea.
In the brainstem compressive stage, adjacent cranial nerves may be affected, often with trigeminal symptoms or lower cranial nerve involvement with hoarseness, dysphagia, and dysarthria, and disequilibrium may worsen (427). In the hydrocephalic stage, rapid clinical deterioration can be accompanied by headache, diplopia, lower cranial nerve dysfunction, and long tract signs.
On neurologic examination of patients with vestibular schwannoma, the most common finding is unilateral sensorineural hearing loss, with loss of high frequency hearing and speech discrimination predominating (199; 280; 183; 404; 405; 248; 264). The loss of speech discrimination often exceeds the degree of pure tone loss. Approximately 90% to 95% of patients have abnormalities of hearing. Occasionally, sudden deafness or acute unsteadiness may result from occlusion of the internal auditory artery (481; 282). In 50% of patients at presentation, hearing loss is the only neurologic sign. Although the symptom of unsteadiness is common, most patients have normal or mildly affected gait and station. In many of these patients, unsteadiness is related to dizziness and other signs of vestibular dysfunction (264). Large tumors may cause frank ataxia or dysmetria from brainstem or cerebellar compression, but these signs are infrequent. In 7% to 15% of patients, particularly those with tumors larger than 4 cm in diameter, papilledema is present (280; 248). Horizontal nystagmus is often noted in patients with tumors greater than 2 cm in diameter (280; 248). Trigeminal dysfunction, typically in the form of a diminished corneal reflex or partial facial hypesthesia, is noted in more than half the patients; hemifacial anesthesia is rare (404). Diminished corneal sensation is present in 30% of medium- and 60% of large-sized vestibular tumors. The seventh nerve is resistant to stretch injury and is involved in less than 10% of cases (405). Paresis of the lower cranial nerves (IX, X, XI, XII) is uncommon and appears as a late sign in large tumors that grow in a medial and inferior direction toward the jugular foramen. Long tract signs (eg, hemiparesis, spasticity, hyperactive reflexes) from severe brainstem compression are rare in modern series (404).
In patients with bilateral tumors or a family history of nervous system tumors, a diagnosis of neurofibromatosis type 2 should be considered. In addition to bilateral vestibular schwannomas, neurofibromatosis type 2 is associated with cataracts, skin nodules and cafe au lait spots, peripheral nerve schwannomas, seizures, and other central nervous system tumors such as meningiomas and gliomas (298).
In general, these tumors are slow-growing, benign neoplasms that have an indolent evolution. In 75% to 80% of cases, the growth rate is estimated to be 1 to 2 mm per year (462; 441; 32; 300). The rate of growth may be slower in older patients. Tumor growth is rarely predictable. Charabi and colleagues followed 127 tumors with serial neuroimaging studies over several years (64). They noted some growth in over 80% of tumors, although growth patterns were varied and changing for individual tumors. Clinical deterioration is to be expected in vestibular schwannomas that are symptomatic and growing.
A 44-year-old man with an unremarkable past medical history developed episodes of dizziness, tinnitus, and mild left-sided hearing loss. The symptoms presented over several months and were slowly progressive. The initial evaluation by his physician was unremarkable with a normal neurologic examination. No stigmata of neurofibromatosis type 1 or type 2 were present. Audiometry revealed a mild degree of hearing loss on the left side. MRI demonstrated an enhancing mass 1.3 cm in diameter in the left cerebellopontine angle, with a tail that entered the internal auditory canal, but did not reach the fundus. The tumor was diagnosed as a vestibular schwannoma, and the patient elected surgery over observation or radiosurgery. Due to the presence of serviceable hearing, a suboccipital approach was used to expose the tumor. The cochlear division of cranial nerve VIII was draped over the mass but not adherent to it and a clean cleavage plane was found between the tumor capsule and the cochlear and facial nerves. The mass arose from and was attached to the inferior vestibular division of VIII. After the mass was dissected away from the cochlear division, the inferior vestibular nerve was divided and the tumor was removed piecemeal, with preservation of cranial nerve VII. After surgery the patient did well, with some preservation of left-sided hearing and only mild left facial weakness. The facial weakness improved to normal after several months. Recurrent tumor was not seen on follow-up MRI.
Concern has risen in recent years about the potential role of microwave radiation from cellular telephones in the genesis of brain tumors, including vestibular schwannomas. At least 40 epidemiological studies have been published (222; 221; 146; 142; 175; 362). Some studies have implicated long-term cellular phone use with an increased risk of vestibular schwannomas or other cranial tumors (291; 68; 222; 399; 146; 142; 143), especially with long latency and onset of use before the age of 20 (142; 57). Kundi reviewed 33 published studies and concluded that, although methodological flaws were found in every study, the weight of the evidence favored an increased risk for ipsilateral vestibular schwannomas with increasing duration of cellular phone usage, but the magnitude of that risk could not be assessed (222; 221). A similar conclusion was reached in a meta-analysis by Hardell in 2008 for ipsilateral glioma and vestibular schwannomas (145). Studies in rats and mice suggest a carcinogenic effect of whole body exposure to radiofrequency radiation (144). Cell cultures of human Schwann cells exposed to electromagnetic fields showed alterations in proliferation, intracellular signaling, metabolic pathways, and in the expression of genes related to hearing loss (73). In 2013 and 2019, Hardell and Carlberg concluded that emissions from wireless phones should be regarded as group 1 carcinogens (143; 144; 278).
Some are skeptical of this interpretation, citing the fact that cell phone emissions are not energetic enough to break molecular bonds within cells, a necessary step toward oncogenesis (277). For example, cell phone emissions were noted to be 240,000 times weaker than the green light photons that activate the rhodopsin molecules in the retina (277). Additionally, some epidemiologic evidence does not appear to implicate cellular telephone use in the etiology of vestibular schwannomas (283) or other brain tumors (06; 175; 401; 356; 224; 324; 86). A meta-analysis published in 2014 did not support the conclusion that mobile phones affect the occurrence of intracranial tumors but noted that limited data are available beyond 15 years of exposure (224). A meta-analysis of 88 studies in which human cells were exposed to radiofrequency fields and analyzed for genetic damage in the form of single or double strand breaks, chromosomal aberrations, micronuclei, and sister chromatid exchange did not find any support for a genotoxicity-based mechanism (457). The fact that tumor incidence rises in the elderly and not in younger patients with the heaviest cell phone usage does not support an etiological link (86; 362).
At least two studies have implicated loud noise exposure in the genesis of vestibular schwannoma (104; 52), but others have shown no increased risk (105; 365; 02) or an indeterminate risk (84). Childhood radiation to the head and neck has also been linked to increased risk of vestibular schwannoma (394). Inactivating mutations in the NF2 gene were found more commonly in the tumor specimens of smokers than in never smokers (229). At this time there is no definitive evidence for a genetic/molecular signature suggestive of radiation-related vestibular schwannoma.
An inherited but nonsyndromic contribution to sporadic vestibular schwannoma has been suggested by genealogic studies in veterans and residents of Utah (131).
Pathologic features. The tumors are variegated in color, with areas of gray, red, and yellow corresponding to areas of dense cellularity, increased vascularity, and xanthomatous degeneration (459). Histologically, the tumors are formed of interweaving bundles of spindle-shaped cells with cigar-shaped nuclei.
Distinct areas designated as Antoni A and B are seen. Antoni A areas are densely cellular and interwoven, whereas Antoni B areas are less cellular, less structured, and often contain areas of microcyst formation and hemorrhage. Occasional cells with large pleomorphic nuclei are common but are not indicative of anaplasia, which is rare or nonexistent in these tumors (459; 289). Reticulin stains or electron microscopy reveal a distinct basement membrane external to the plasma membrane, which distinguishes vestibular schwannoma from meningiomas with a similar appearance. Although the tumor surface is covered with connective tissue, this "capsule" is often no thicker than 3 to 5 µm in most areas (223). A nodular architecture has been reported to occur in 40% of NF2-associated tumors but is rare in sporadic cases (118). A current review of the neuropathologic features of schwannomas is available (39).
The distal location of the glia to Schwann cell transition in the vestibular nerves distinguishes them from other cranial nerves and has been thought to predispose them to neoplastic transformation (459). This theory has been questioned, and the incidence of vestibular tumors remains unexplained (436; 478). Because the Schwann cell-glial junction is variable, the tumor location may vary and can range from a lateral position near the inner ear, to a medial position at the porus acusticus, to entirely within the cerebellopontine angle (280; 248). Schwannomas can develop from either the superior or inferior division of the vestibular nerve, with an approximately equal incidence (183).
Molecular genetics. Specific loss of genetic material on chromosome 22 was a feature of 44% of informative cases of sporadic vestibular tumors when analyzed by the RFLP approach (403). This loss has been attributed to partial deletion or mitotic recombination (194). Further work with schwannomas from multiple locations narrowed the region of interest to an area between the CRYB2A and the MB loci (40), but cloning of the candidate gene came from analysis of neurofibromatosis type 2 cases.
Neurofibromatosis type 2 is an autosomal dominant disorder that occurs in 1 in 25,000 to 100,000 births (298; 22; 95). The hallmark of this disease is bilateral vestibular tumors, and individuals with the neurofibromatosis type 2 gene are greater than 95% likely to develop these lesions (445). In addition to eighth nerve tumors, multiple spinal and intracranial schwannomas, meningiomas, and ependymomas are common in this disease. The molecular genetics of neurofibromatosis type 2 were advanced significantly because cytogenetic analysis of meningiomas had already suggested that chromosome 22 was frequently abnormal (403; 101; 313). Analysis of a large family carrying this disorder using linkage analysis with special attention to chromosome 22 showed the responsible gene to be located on chromosome 22q12 and linked to the marker D22S1 (366). By using deletion mapping (368) and a patient with a constitutional breakpoint, the neurofibromatosis type 2 gene was mapped between markers D22S1 and LIF. Using positional cloning, a candidate gene was identified in 1993 and called merlin/schwannomin (17; 367; 445). Nonoverlapping deletions affecting this gene were detected in two independent families, suggesting that merlin/schwannomin is the neurofibromatosis type 2 gene product. Half of patients inherit a germ-line mutation and half acquire a new mutation (22; 95). Mosaicism is seen in a third to as high as 60% of patients (109; 111). The gene contains 17 coding exons spanning approximately 95 kilobases and encodes a protein of 595 residues, which is widely expressed and which has high homology to a family of proteins linking cytoskeletal components to the cell membrane, the band 4.1 superfamily, containing proteins such as ezrin, radixin, and moesin (34; 118). Transfection of abnormal proteins into mammalian cells has been shown to alter their adhesion to the substrate (423).
The occurrence of vestibular schwannomas and meningiomas in association with the loss of function of a gene suggests that the neurofibromatosis type 2 gene is a tumor suppressor gene involved with the growth control of cells of neural crest origin (259; 368). The protein is thought to exist in both an unfolded and a folded form, with the latter mediating the tumor suppressor activity (268). Missense mutations may disrupt the folded state (312). The protein PAK phosphorylates merlin at S518, disrupting the maintenance of the folded state and tumor suppressor function (209; 311). Early transfection experiments suggest an anti-ras function for the protein (442; 34). The NF2 gene product inhibits directly the kinase PAK1, which is essential for ras transformation, and may be a target for therapy in NF2 (158). Merlin tumor suppressor ability is also thought to relate to inhibition of the Rac pathway (118). Inhibition of PAK might allow merlin to continue to inhibit the Rac pathway. Merlin has been shown to be a negative regulator of the mammalian target of rapamycin complex 1 (mTORC1) with elevated mTORC1 signaling in NF2 tumors (125). Merlin has a FERM (four point one/ezrin/radixin/moesin) domain and is involved in the regulation of cell proliferation in response to adhesive signaling, activates anti-mitogenic signaling at intercellular tight junctions, and inhibits oncogene expression (95). Multiple publications provide an extensive discussion on knowledge of merlin molecular biology (118; 88; 78).
Merlin-deficient cells also have a larger non-inactivating outward potassium ion current than control cells, and blockage of this current with quinidine can reduce cellular proliferation (448). The role of the gene product in embryonic development, cellular adherence, and Schwann cell-axon interactions are slowly being elucidated (464). Valproic acid has the ability to induce neuronal differentiation, possibly through the upregulation of merlin and its interaction with the focal adhesion protein, paxillin (479). Aberrant EGFR activity has been detected in human vestibular schwannomas (12) and in the livers of mice, from which the merlin gene has been deleted (35).
It is possible that multiple transcription initiation sites, alternative splicing, and differential polyadenylation contribute to the altered gene activity (62). The lack of mutations in the neurofibromatosis-2 gene in some patients with clinical disease has been attributed to mosaicism, found in 24.8% of cases in one study, 30% to 33% of new mutations in another study, and as high as 59.7% with next-generation sequencing (210; 288; 109; 111). Genotype-phenotype correlation has also been noted, with constitutional missense mutations, splice-site mutations, large deletions, and somatic mosaicism associated with fewer tumors than constitutional nonsense or frameshift mutations (27; 109; 407; 136; 95). Additional mutations outside the NF-2 locus may herald more aggressive tumor behavior (54). Specific genetic and epigenetic changes in NF-2 may be related to the risk of hearing loss and other clinical manifestations of the disease (95).
The observation by Rouleau and colleagues of somatic mutations in the neurofibromatosis type 2 gene in sporadic schwannomas made it likely that the merlin/schwannomin gene would be involved in the pathogenesis of vestibular schwannomas not associated with neurofibromatosis type 2 as well (367). The presence of a variety of mutations in the merlin/schwannomin gene in sporadic schwannomas from multiple sites has been confirmed by other investigators (41; 179; 54). However, no merlin/schwannomin mutations were found in six families with unilateral vestibular schwannomas (42). Hypermethylation of the gene has not been demonstrated to be a means of silencing of merlin/schwannomin function (219; 232; 95).
The role of micro RNAs (miRNAs) in schwannoma development is also being investigated (108; 234). Alterations in various miRNAs have been correlated with radiographic tumor growth rate (389).
For completeness, the schwannomatosis genes have also been traced to chromosome 22, located proximally to the neurofibromatosis type 2 gene, and they appear to involve the INI1/SMARCB1 or LZTR1 genes (475; 51). Vestibular schwannoma can be seen in schwannomatosis, and in the presence of (130) or in the absence of a detected LZTR1 mutation (272). Schwannomatosis should be considered when a unilateral vestibular schwannoma is found in conjunction with other neural tumors or in very young patients (130; 417; 373). Several syndromes are now recognized, including SMARCB1-related (SWNTS1), LZTR1-related (SWNTS2), and SMARCB1/LZTR1-negative schwannomatosis (51). Whole gene deletion of LZTR1 does not appear to predispose to schwannomatosis, and only one patient in 110 with an apparently sporadic schwannoma had a constitutional whole gene deletion of LZTR1 (112). In contrast to patients harboring rhabdoid tumors, thought to be due to complete loss of SMARCB1 function, schwannomatosis may be due to hypofunctioning protein(s) in combination with a second hit at the NF2 gene site (197; 417). In a British population, the birth incidence of schwannomatosis was 1 of 27,956 versus NF-2 in 1 of 68,956, making it more common than NF-2 (110).
Oncogenes, growth factors, and other biochemical observations. Genetic events underlying Schwann cell transformation were reviewed in 2021 (455). NF1 or NF2 loss are necessary but not sufficient for transformation; other genetic changes are also required. These include progressive loss of Sox10, S100, and GFAP positivity and other noncell autonomous contributions. A preliminary report of detection of the neu oncogene in nearly all 3T3 cells transformed by DNA from a group of rodent schwannomas induced by transplacental N-nitrosoethylurea has appeared (358). The neu oncogene is a transmembrane receptor protein with tyrosine kinase activity like the epidermal growth factor receptor. Almost all of the transformants contained a neu gene with an activating point mutation, which was not present in any glial tumors tested. The same finding was present in several rodent species. Neu mutation may, therefore, represent a major pathway for transformation of nerve sheath tissue.
Transforming growth factor beta-1 has been shown to stimulate DNA synthesis in cultured human vestibular schwannoma cells, and these same cells express transforming growth factor beta-1 mRNA (463). This suggests that transforming growth factor beta-1 may participate in an autocrine loop in vivo. Basic fibroblast growth factor had no effect in the same model.
Schwann cells from neurofibromatosis type 2 patients have been shown to have larger outward potassium currents than those from control subjects (363). Inhibitors of potassium currents, such as quinidine, have been shown to slow the growth of neurofibromatosis type 2 Schwann cells in culture, but not the growth of normal Schwann cells (363).
CDK2, part of the retinoblastoma protein cyclin-dependent kinase pathway, has been shown to be underexpressed in seven or eight vestibular schwannomas examined (228).
Altered structure, increased expression, and an increase in the phosphorylated form of the Rb1 (retinoblastoma) gene have been demonstrated in human vestibular schwannoma tissue (440). This altered pattern of expression suggests an antiapoptotic function in these tumors.
The concentration of vascular endothelial growth factor (VEGF) and its receptor, VEGFR-1, have been found to correlate with tumor growth rate, indicating a possible role for this molecule in the growth of vestibular schwannoma (60; 218). Another study of 182 sporadic tumors found expression of both VEGF and its receptors in 100% of tumors, and a correlation with expression and recurrence (218). VEGF was expressed in 100% of 22 sporadic tumors and 21 associated with NF2 (331). In addition, neuregulin-1, a glial growth factor, and its receptor, ErbB2, have been found in vestibular schwannoma cells and may constitute an autocrine pathway driving the growth of tumor cells (140). Upregulation of the related hepatocyte growth factor and its receptor cMET is also found in tumor samples with upregulated VEGF-A signaling (92). Simultaneous inhibition of c-Met and Src suppresses the growth of schwannoma cells and can induce apoptosis (121).
Intratumoral macrophages have been of interest in many tumor types, including vestibular schwannomas (87). M2 macrophages positive for CD163, which have been associated with angiogenesis, tumor growth, and interference with antitumor immune responses, have been reported to be significantly higher in vestibular schwannomas growing rapidly on MRI prior to surgery (87). Increased levels of M1, CD 163+ tumor-associated macrophages have also been reported in tumors progressing after subtotal resection in association with PD-L1 expression, which might be a potential treatment target (322). The entire inflammatory microenvironment in vestibular schwannoma is now an area of intense interest (138). The presence of an elevated C-reactive protein level prior to surgery has also been linked to shortened progression-free survival (460).
Human primary schwannoma cell cultures show enhanced basal Raf/mitogen-activated protein/ERK kinase/ERK1/2 pathway activity when compared with healthy Schwann cells (13). Due to overexpression and activation of PDGF receptor beta, ERK1/2 and AKT activation is also detected in schwannoma, leading to proliferative increases. Specific inhibitors for these pathways may lead to new treatment options (13).
Microarray analysis of tumors examining 23,055 genes detected 1650 differentially expressed genes when compared to tibial nerve (01). The ERK pathway was involved in many of the differentially expressed genes. Downregulation of the CAV1 gene was notable as this gene is normally expressed in Schwann cells. Another gene expression profile of 49 schwannomas and seven control vestibular nerves identified over 4000 differentially expressed genes (04). No subtypes of tumors were identified and no differences between sporadic and NF2-associated tumors were detected. The P13K/AKT/mTOR pathway overexpression was frequently seen. Fourteen pathways were found to be associated with faster growing tumors when global gene expression was examined in 16 human tumors for which preoperative growth rates were determined (388). Gene expression profiles may differ in solid and cystic vestibular schwannomas (480) and in cyst and previously irradiated tumors, which may have an increased mutation burden compared to sporadic tumors (03).
COX-2 expression was detected in 29 of 30 vestibular schwannomas from both sporadic and NF2-associated cases, and the expression of COX-2 was found to correlate with the Ki-67 index of proliferative activity (161). However, clinical studies found no correlation between aspirin or other NSAID use and tumor growth or growth rate on serial MRIs (170; 33).
The phosphatidylinositol 3-kinase/AKT pathway has been found to activated in vestibular schwannomas, promoting cell proliferation and survival. This has led to testing of a compound called AR42, a novel histone deacetylase inhibitor, to inactivate AKT. AR42 was shown to suppress the growth of both murine schwannoma allografts and murine human vestibular schwannoma xenografts with no detectable toxicity (184).
The merlin/schwannomin gene has been shown to regulate angiogenesis through a Rac1/semaphoring 3F dependent pathway (474). Reintroduction of semaphoring 3F was therapeutic in nude mice bearing merlin-deficient tumors.
Aberrations of the p14ARF/MDM2/p53 pathway have been found in a high percentage of 58 sporadic vestibular schwannomas (66).
Schwannomas account for 6% to 8% of all primary brain tumors, with the majority occurring in adulthood (301). Over 85% to 90% of intracranial schwannomas affect the vestibular portion of cranial nerve VIII in the cerebellopontine angle (280; 183; 248). The great majority of schwannomas are sporadic and unrelated to either neurofibromatosis type 1, neurofibromatosis type 2, or to a third entity, schwannomatosis (355; 475).
Vestibular schwannomas are most common in the fifth and sixth decades of life and occur with a slight female preponderance (459). In the era of magnetic resonance imaging, vestibular schwannomas have been estimated to afflict 19.3 persons per million per year, with 2000 to 3000 new tumors per year in the United States (298; 77; 421; 472). A steadily rising incidence in Denmark from 1976 to 2001 has been attributed to better detection rather than to an increase in the actual number of tumors (421). An international systematic review concluded that the incidence was more likely to be 5 per 100,000 in all age groups and 20 per 100,000 in higher risk older patients, with a lifetime prevalence of 1 per 500 persons (254). Approximately 95% of tumors are unilateral, whereas 5% are bilateral and are associated with neurofibromatosis type 2. Asymptomatic tumors have been found at autopsy in 0.8% to 2.7% of cases (77).
Pediatric tumors are rare but have been described (251). In a meta-analysis of 96 cases, the average age at presentation was 12.1 years and tumors were more likely to recur than in older patients (251).
Although not currently available, further understanding of the molecular genetics of schwannoma pathogenesis could conceivably lead to both specific therapy for existing tumors and preventative strategies for patients with neurofibromatosis type 2.
Vestibular schwannomas make up 80% to 90% of the masses found in the cerebellopontine angle (225; 416; 270). The differential diagnosis of a mass in the cerebellopontine angle includes meningioma, epidermoid cyst, arachnoid cyst, exophytic glioma, cerebellar hemangioblastoma, metastasis, choroid plexus papillomas, glomus tumor, and primary bone tumors. Meningioma is the second most common cerebellopontine angle tumor (10% to 15% of cerebellopontine angle lesions). Distinguishing clinical features of meningiomas include their propensity to cause facial nerve dysfunction or trigeminal neuralgia rather than isolated hearing loss. Radiologically, meningiomas often lack extension into and expansion of the internal auditory canal, have a sessile base, cause underlying hyperostosis of the petrous bone, tend to be more homogeneously enhancing, have a "dural tail," and sometimes allow visualization of the seventh and eighth nerve complex, even in large tumors (290).
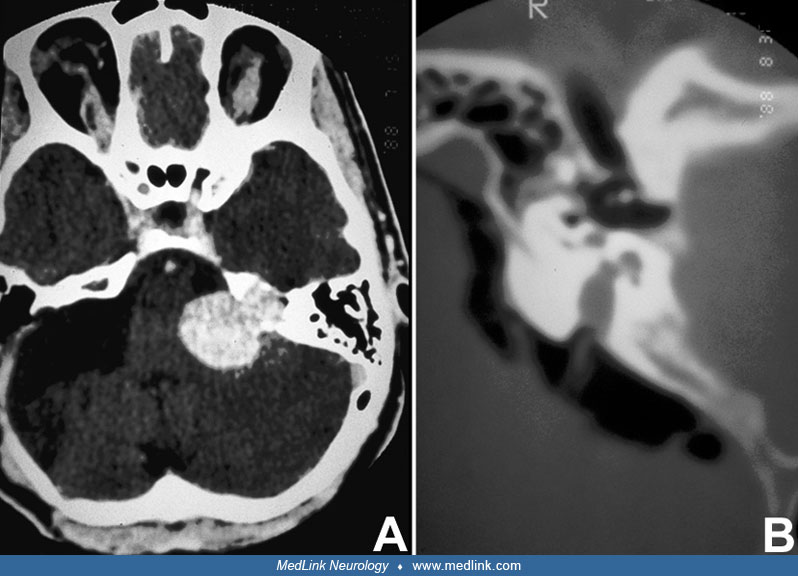
The third most common mass of the cerebellopontine angle is the epidermoid inclusion cyst, making up 5% to 9% of all lesions (225; 416). Patients often have a long history of hearing loss and tinnitus. On CT, epidermoid cysts are usually hypodense compared to brain (similar to water or CSF). Calcification of the cyst rim is noted in 25% of cases. Enhancement is negligible within the cyst but may occur along the rim. On MRI, epidermoid cysts are usually isointense to CSF (ie, low signal intensity on T1 images and high signal intensity on T2 images) and may have a lamellated appearance. Similar to CT, the cyst does not enhance with gadolinium, except for the rim.
Arachnoid cysts can also occur in the cerebellopontine angle. They have signal intensity and attenuation characteristics identical to CSF and do not enhance with contrast. Many other lesions can arise in the cerebellopontine angle, each of which accounts for less than 1% of all cases. Tumors that may extend into, but not arise from, the cerebellopontine angle include exophytic brainstem gliomas, ependymomas, choroid plexus papillomas, schwannomas of cranial nerves V, VII, IX, X, and XI, jugular foramen paragangliomas, lipomas, and metastases (225; 416). Facial nerve schwannoma can be difficult to distinguish from vestibular schwannoma on imaging (247). Vascular processes such as aneurysm, malformations, and aberrant loops of normal blood vessels can develop in the cerebellopontine angle. Enhancement on CT and a flow void on MRI are diagnostic of a vascular process. Rarely, infectious processes can develop in the cerebellopontine angle, such as tuberculomas and cysticercosis. Benign vestibular conditions (eg, Meniere disease) can suggest vestibular schwannoma with symptoms and signs of hearing loss, tinnitus, nystagmus, and vertigo (250). However, tumor can be ruled out by a careful history (ie, fluctuating symptoms that occur in attacks, bilateral involvement in approximately 20%) and a normal enhanced MRI scan.
Delays in the diagnosis of vestibular schwannoma are reported to be common (452), but the progressive decrease in the size of detected tumors indicates that the diagnosis is being made earlier with MRI and other modalities (427). After appropriate history and physical examination, the evaluation of a patient suspected of harboring a vestibular schwannoma usually begins with audiometry. A standard audiogram should be performed, including speech reception thresholds and speech discrimination testing. Very specific audiometric protocols might improve the early detection of vestibular schwannoma and obviate some MRI scans (458). Brainstem auditory evoked responses and assessment of the acoustic reflex threshold and decay are of additional value in diagnosis (199; 298). Brainstem auditory evoked response has a 94% to 96% detection rate, an 8% false-positive rate, and a 4% false-negative rate (406; 298), and it has been shown to be sensitive to even small tumors (98), but other studies have called these data into question (50; 294; 370; 314). The false negative rate in intracanalicular tumors may be as high as 17% (471; 314). A technique called stacked derived band auditory brainstem response has been reported to be more sensitive to smaller tumors than conventional auditory brainstem response (97; 427). The cost savings of obtaining auditory brain responses prior to MRI does not outweigh the number of potentially missed vestibular schwannomas or other clinically important pathologies that would be discovered with MRI alone (469).
The typical audiometry profile in a patient with a vestibular schwannoma is unilateral sensorineural hearing loss with speech discrimination impairment worse than pure tone loss, normal tympanometry and compliance, an absent acoustic reflex (the contraction of the stapedius muscle in response to a high-intensity sound) or reflex decay, and delayed conduction on brainstem auditory evoked response (199; 427). Auditory brainstem response (ABR) testing is non-invasive, painless, and not affected by patient cooperation, but can be unreliable when hearing is poor (427). The sensitivity of ABR has been reported to be between 63% and 95%, with lower sensitivity for tumors less than 1 cm in diameter. Stacked ABR may improve detection of smaller tumors. In a large study, over 10% of tumors were missed on audiologic screening; these atypical tumors were larger and presumably less likely to be successfully treated (281).
CT scan shows an isodense, enhancing mass, originating at the internal auditory meatus and occupying the cerebellopontine angle. Bone window settings on CT often show internal auditory canal erosion, even by small tumors.
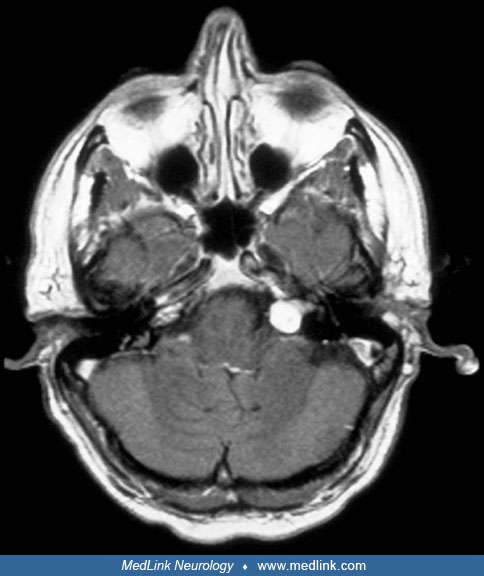
MRI is the definitive diagnostic test, especially for small, intracanalicular tumors (79). However, due to its expense, the recommendation in the past has been that MRI should be reserved for patients whose history, examination, and audiometry are suggestive of a tumor; MRI should not be recommended as a screening tool according to multiple authors (199; 298; 115). However, some authors report that a limited MRI examination may be more cost effective in some patients, and careful clinical decision analysis has shown that the most cost-effective diagnostic pathway is dependent on the value assigned to a missed diagnosis (25; 374; 58; 471; 427; 434). Reviews of the auditory brainstem response versus MRI debate concluded that a limited enhanced or non-enhanced MRI may be the most cost-effective screen (471; 427). No comparison has yet appeared between limited MRI and stacked derived band auditory brainstem response for sensitivity, specificity, and cost effectiveness. In a systematic review from 2018, MRI was recommended for patients with unilateral hearing loss greater than or equal to 10 dB at two frequencies or greater than or equal to 15 dB at one frequency, especially at 3000 Hz (434). MRI was recommended for unilateral tinnitus, but the yield was expected to be less than 1%, but for sudden unilateral hearing loss the yield was expected to be greater than 3%.
When imaged by MRI, about two thirds of tumors are hypointense when compared to brain on T1-weighted images; about one third are isointense (290). Tumors are characteristically hyperintense compared to brain on T2-weighted sequences. About two thirds of tumors enhance homogeneously with contrast; about one third enhance inhomogeneously.
Intratumoral areas of cystic degeneration and peritumoral arachnoid cysts are common. A “dural tail” is seen in less than 10% of tumors but might be indicative of tumor adherence and more difficulty separating the tumor from the facial nerve at surgery (319). The technique of Eigen image filtering has been reported to give more accurate volume determinations and, thereby, growth rate estimates for vestibular schwannomas and may be a promising clinical research tool (285).
Diffusion imaging tractography may improve the visualization of the distorted cranial nerves in the region of the tumor (65; 476), especially with larger tumors (369), but even when combined with FIESTA imaging, the overall rate of detection of the facial and cochlear nerves was low (486). Multishell diffusion tractography may improve facial nerve detection preoperatively (59).
When gadolinium enhancement cannot be used or cost saving is important, heavily T2-weighted fast spin echo imaging or 3-dimensional Fourier transform-constructive interference in steady state (3DFT-CISS) imaging can provide high-resolution imaging of the cerebellopontine angle sufficient to detect most vestibular schwannomas (427). Gadolinium may be also be unnecessary for routine surveillance imaging (328).
Protein profiling of cerebrospinal fluid may show some promise in presurgical confirmation of vestibular schwannoma (166). This is not yet part of routine care, however.
Treatment options include observation, subtotal resection, total resection, radiation, and potentially, chemotherapy. Although total excision has been considered the treatment of choice (298), this issue has been debated (77; 188; 213; 85; 196). Considerable controversy still exists about the roles of surgery and radiosurgery (196; 332; 26, 72; 292; 473). Treatment algorithms have been published based on patient age, hearing status, tumor size, and symptoms (412) as well as cost of care (26) and patient satisfaction (293). Some of these studies report better outcomes for radiosurgery than surgery (292; 466; 473), but others have reported no differences with observation, surgery, or radiosurgery (93; 360).
Observation. With the increasing rate of discovery of small or asymptomatic tumors, observation has been advocated, especially in older patients or patients with bilateral tumors and useful hearing. Indeed, there has been some concern that the general approach to these tumors has been too aggressive, although debate is ongoing (77; 350; 230). The growth rate of vestibular tumors is highly variable, and regression or stabilization after a period of growth is possible (411; 30; 165; 169; 398; 256; 255). In a number of series, approximately half of tumors observed with serial imaging did not grow at all, and the growth rate of those that did enlarge averaged less than 2 mm per year (32; 77; 364; 424; 468; 411; 446; 461; 485; 30; 135; 23; 169; 256). In several studies, the growth rate in the first year of follow-up was predictive of subsequent growth (32; 446). A 2005 meta-analysis of 1345 patients reported that 57% of tumors were stable or regressed over an average of 3.2 years, and a growth rate average of 1.9 mm/year in those that did enlarge (418). A similar literature analysis showed that for 1340 reported cases followed for a mean of 38 months: 46% enlarged, 8% regressed, and 18% required treatment (485). Another single-center series reported the need for intervention in 23.7% of patients initially treated conservatively (23). In a large series of 564 patients observed for an average of 23 months, 40.8% demonstrated growth and 32.1% underwent intervention (169). Larger tumors and those presenting with disequilibrium were more likely to enlarge. In a series of 178 patients managed with observation, the mean growth rate was 0.66 mm per year or 0.19 cubic cm per year, and the volume doubling time was 4.40 years (454). Two thousand three hundred and twelve patients in Denmark were treated initially with observation, of whom 434 (19%) had converted to active treatment at a mean of 7.33 years (357). Using receiver operating characteristic curve analysis, the volume doubling time was found to be the most realistic growth model, with a cutoff of 5.22 years distinguishing growing from nongrowing tumors. In 243 patients initially selected for observation, local control was still present at 10 years in 58% (371). Initial conservative management does not appear to jeopardize results of future treatment (135; 258) and offers better cranial nerve preservation rates than primarily surgically treated tumors (258), but one report suggested better facial nerve outcomes with earlier surgery (341). Serial volumetric analysis has been reported to be more sensitive than linear tumor measurements in detecting significant changes in tumor size (149; 233; 398). In a series of 212 patients followed volumetrically, a volumetric growth rate of 33.5% per year was observed (398). A lobulated appearance has been associated with a more aggressive course (173) as has a cystic appearance (102). Tumor growth rate has not been associated with any specific genetic abnormality (177).
Of 466 patients treated with initial observation and hearing, serviceable hearing was maintained in 94% at 1 year, 66% at 5 years, and 44% at 10 years (168). Tumors more than 5 mm in size are associated with progressive hearing loss even without growth; nongrowing tumors less than 5 mm were not associated with ongoing hearing loss (245). In another systematic review of 3652 observation patients from 26 studies, a conservative benchmark was suggested: serviceable hearing would be retained in 75% at 3 years, 60% at 5 years, and 42% at 10 years (201).
Determining how much growth or at what rate of growth intervention should be offered has not been established. One study suggests that the probability of less optimal surgical outcomes begins to significantly increase when the extra-meatal size of the tumor reaches 14 to 20 mm and that this threshold should trigger intervention rather than a criterion like more than 2 mm of growth in a year, as suggested by others (249). Cochlear implant is an option for patients with poor hearing and tumors under observation without treatment (241).
Guidelines from the Congress of Neurological Surgeons in 2018 suggested MRIs be obtained yearly for 5 years, then less frequently if stability has been confirmed (102). More frequent imaging was recommended in patients with NF-2. However, no definite monitoring interval could be recommended by another study (400). There is interest in using noncontrast MRI monitoring to avoid repeated exposure to enhancing agents and for cost saving (80; 207).
Sporadic vestibular schwannomas have been retrospectively observed to grow less in aspirin users than in those who did not use aspirin (193) but other studies could not confirm this (170; 33).
Prediction of tumor growth rate in neurofibromatosis type 2 patients does not seem possible based on tumor behavior in other affected family members, but tumors do seem to grow faster in younger patients (28; 265; 325). In a report of NF2-associated tumors, 29.6% exhibited linear growth, 11.2% exponential growth, and 59.2% saltatory growth (96). Therefore, caution is needed in analyzing short-term growth patterns in these patients. Another report noted that mean tumor growth rate in 92 tumors in 46 NF2 patients was 1.8 mm/year and the surgery free rate was 88% at 5 years (325). The United Kingdom NF2 Genetic Severity Score may be useful in predicting aspects of clinical severity, with constitutional truncating NF2 mutation associated with severe disease, whereas missense or mosaic mutations present with a milder phenotype (136). Serial hearing testing in NF2-related tumors treated with observation showed that pure tone thresholds increased by 1.3 to 2 decibels per year and that patients maintained serviceable hearing for an average of 7.6 years (215). Hearing loss did not correlate with tumor growth. These authors concluded that conservative management was an attractive option for these patients (215).
A Markov decision analysis looking at the quality-adjusted life years derived from various treatment strategies concluded that a period of observation offered the best strategy for patients with tumors less than 1.5 cm in size (286). Alternatively, another meta-analysis of quality of life 5 years after treatment reported that radiosurgery had an advantage over surgery, which was, in turn, better than observation (466). One observation of worsening tinnitus in observed patients has been reported (451). Some have argued that vestibular schwannomas are currently overtreated in the United States (230).
The lack of growth in some patients makes it reasonable to follow some tumors with serial imaging when the clinical situation is appropriate. The slow growth may also support the use of subtotal resection due to the lower morbidity of this approach (242; 364). In addition, these data mandate caution in interpreting the results of therapy, as the lack of growth of some tumors may be falsely attributed to treatment, and spontaneous regression has been reported (200; 352; 30; 165). Alternatively, the view has been expressed that elderly patients tolerate surgery well and that surgical removal is the treatment of choice for patients in good health regardless of age (349; 345; 449; 246). However, an increased risk of poor facial nerve function may be expected in some series (154) but not in others (246).
Biomarkers of more rapid growth are being sought to aid in determining which patients are safe to observe initially (488). These include merlin pathway proteins, inflammatory signals, tumor miRNAs, tumor proteins, and CSF components.
Surgery. If surgery is indicated, preservation of hearing and facial nerve function are now the primary goals of surgery. Surgical mortality and major morbidity have declined considerably in experienced centers (128; 263). Hearing preservation has become more common in the microsurgical era and has become the focus of work in some centers (264). The data indicate that the preservation of useful hearing is unlikely in most centers in tumors over 2 cm in diameter or if the tumor fills the fundus of the internal auditory canal, regardless of the degree of preoperative hearing (198; 410; 298). There is a 25% to 83% chance of useful postoperative hearing in favorable small tumors (126; 340). Individualizing the surgical approach when hearing preservation is the goal may improve results (18). Invasion of the eighth nerve by tumor cells may make hearing preservation difficult in some cases (262). Hearing preservation is more likely if the brainstem auditory evoked response was normal preoperatively and with subtotal resection (216; 378; 483; 242). Intraoperative brainstem auditory evoked response and cochlear nerve action potential monitoring have been reported to improve the chances for hearing preservation (487). Electrocochleography may be superior to auditory brainstem responses for predicting postoperative hearing function when these modalities were compared directly during surgery (220). Since that report, intraoperative auditory steady-state monitoring has been suggested to be superior to auditory brainstem response in predicting postoperative hearing class in hearing preservation surgery (348).
Delayed postoperative hearing loss after initial preservation of function is, unfortunately, possible but not inevitable (298; 425; 299; 447; 263; 346). Efforts are underway to standardize reporting of hearing results (75). Perioperative use of nimodipine, known to improve outcome in aneurysmal subarachnoid hemorrhage (393), and hydroxyethyl starch may improve outcome (487). The parenteral form of nimodipine may be more effective than enteral dosing (393). A subsequent study reported no benefit with nimodipine (391), but another reported significant benefit with nimodipine and hydroxyethyl starch (392). Nimodipine may be more likely to benefit male patients but larger tumors in the female group may have obscured benefit (390). A meta-analysis did find benefit from nimodipine for cochlear nerve, but not facial nerve, preservation (67).
Electrophysiologic monitoring of the facial nerve is now considered essential for preservation of function (148; 298; 384; 487). Good facial nerve function in the immediate postoperative period with an anatomically intact nerve may deteriorate subsequently but has a good long-term prognosis (21). Severely impaired function immediately postoperatively has a poorer prognosis but may still show considerable improvement. The proximal nerve stimulation threshold at the end of the procedure may be a good predictor of long-term nerve function (226; 413). In a large series of patients operated on with facial nerve monitoring, facial nerve function was good at 1 month postoperatively in 52% of tumors greater than 3 cm, 81% of tumors 2 to 3 cm, and 92% of tumors less than 2 cm (422). In most cases, function improves with time after surgery; in one series, 92.1% of patients with smaller tumors and 75% of patients with large tumors had normal function at 6 months (384). Oh and colleagues reviewed electrophysiologic monitoring techniques useful during vestibular schwannoma surgery (310).
The extent of removal is decided on an individual case basis. For some patients, total resection will be the goal. For others, subtotal resection in order to preserve facial nerve function or intracapsular resection to preserve hearing may be indicated (242; 402; 435; 44). Tumor involvement of the fundus of the internal auditory canal may herald more difficulty in preserving hearing and facial nerve function (102). For large tumors, near total or subtotal resection has been reported to result in higher facial nerve function preservation and lower need for eye treatments (402), but subtotal resection may result in higher recurrence rates compared to total or near total resection in some reports (284) but not in others (435). In all cases, long-term follow-up is indicated to detect recurrence or growth of residual tumor. Recurrence after subtotal resection is likely, with a reported radiographic recurrence rate of 44% and need for additional therapy of 26%, at a mean follow-up of 6.2 years (107). In a long-term follow-up of 772 patients followed for 3 to 266 months, however, the risk of recurrence did not correlate with the extent of resection (431) nor was there a difference in recurrence rate between subtotal or near total resection in 42 patients with intentionally residual tumor among 450 patients in another study (435). The recurrence rate after total resection is low, and some authors have suggested that frequent imaging may not be indicated (409), but a long-term follow-up of 571 patients who underwent gross total resection at one institution showed an 8.8% recurrence rate (431). Recurrence rates may be higher in patients over age 70 (449). Surgery appears to provide durable remission, with an 89% freedom from recurrence or progression at 15 years in a series of 204 patients operated on at less than 40 years of age (430). Another long-term follow-up after gross total resection observed a recurrence free survival rate of only 56% at 20 years (297). Ki-67 index may be predictive of the probability of recurrence (174; 342). Care must be exercised in interpreting postoperative images (267; 102).
Surgery is generally performed by an experienced team that includes neurosurgeons, neuro-otologists, and neurophysiologists. Centers caring for these patients should also be skilled in the rehabilitative aspects of care, such as facial nerve reconstruction, prosthetic hearing devices, vestibular rehabilitation, etc. Three basic surgical approaches are utilized: (1) posterior fossa, (2) translabyrinthine, and (3) subtemporal (middle fossa) approaches. A fourth avenue, an endoscopic, transcanal transpromontorial approach, has also been reported for small, intracanalicular tumors (10; 252; 253). Data from a multi-institutional series of 1579 operated patients are available (467). Individual surgeons have also accumulated considerable experience with these tumors (263).
The posterior fossa approach is indicated for attempted hearing preservation and for large tumors. This approach requires brain retraction but is rapid, does not destroy the hearing apparatus, affords a large opening necessary for removal of large tumors, and allows exposure of all involved cranial nerves. In the Mayo Clinic series of 335 procedures, the facial nerve was preserved in 86.3% and hearing in 13.4% (147; 103). Total removal was achieved in all but eight cases; one of the eight recurred, and five of the total resections also recurred. Excellent results have been reported for this approach when treating intracanalicular tumors (381; 263). Several institutions have reported that the posterior semicircular canal can be resected with hearing preservation as part of a combined pre- and retro-sigmoid approach (315; 19). Use of endoscopes has been reported to allow better visualization through smaller craniotomies (326). This approach is described in detail by Elhammady (106).
The translabyrinthine approach is destructive of hearing and is, therefore, indicated in patients without useful hearing or for whom hearing preservation is not likely. The opening for this approach is more time consuming and is not suitable for large tumors. It has the advantages of avoiding brain retraction, exposing the entire internal auditory canal, allowing exposure of the facial nerve distal to the tumor, which some believe improves the chance of preservation of the nerve, and allowing for immediate grafting of the nerve if required. The House group has enormous experience with this technique, reporting the results of over 1600 cases (162; 46). Some large series have reported total resections in 99%, facial nerve function of House grade III or better in 86%, and mortality of 1.75% (321). Some reports indicate better facial nerve preservation rates with the translabyrinthine approach than with the posterior fossa approach (160). In a series of 512 patients treated with the translabyrinthine approach, total tumor removal was accomplished in 94.5%, and anatomic preservation of the facial nerve in 97.5% (46). At 1 year, 81% of patients had facial nerve function of House-Brackmann grade I or II. In patients with small tumors and no hearing, the translabyrinthine approach has been reported to result in less posttreatment dysequilibrium than radiosurgery with comparable morbidity (72). The recurrence rate after gross total resection may be slightly lower with the translabyrinthine approach than with other approaches (07). CSF leakage may be more common with this approach than with others but has decreased with improved closure techniques (20). This surgical technique is described in detail by Arriaga and Lin (20). The translabyrinthine approach may result in shorter hospital length of stay and lower costs than the retrosigmoid approach, even when controlled for tumor size (408). Simultaneous cochlear implant placement has been reported (83). There is insufficient evidence to recommend the translabyrinthine or posterior fossa approach in terms of extent of resection or facial nerve preservation when serviceable hearing is not present (133).
The subtemporal extradural or middle fossa approach is used by only a few centers, but is suitable for hearing preservation surgery, with tumors confined to the internal auditory canal with less than 1 cm of medial extension and in some centers for larger tumors (134; 415; 16). Tumors that do not reach the fundus of the internal auditory canal are also more suitable for attempts at hearing preservation (16). The falciform crest obscures the inferior half of the fundus of the internal auditory canal when viewed from above, which may limit the resection in this area in hearing preservation cases (132). This approach may be most useful in tumors arising from the superior vestibular nerve. Preoperative determination of the vestibular nerve from which the tumor arises may be improved with a sophisticated battery of testing but remains imperfect (347). It may also be used for decompression of the internal auditory canal in only hearing ears in order to temporarily preserve hearing (122). In centers using multiple approaches, hearing preservation has been reported to be more likely with the middle fossa approach (178), but others have reported equal hearing preservation with the posterior fossa approach and fewer overall complications with the latter approach (377). The surgical technique is well described by Angeli (16).
Complications of surgery other than cranial nerve injury involving nerves VII and VIII have been investigated in a comprehensive review of 32,870 patients (432; 431). Twenty-two percent of patients experienced at least one surgical complication; mortality rate was 0.2%. Cerebrospinal fluid leak occurred in 8.5% of cases and was more common with the translabyrinthine approach. Ischemic stroke or hemorrhage occurred in 1% of patients. Infection developed in 3.8% of cases. Another database study reported a 30-day mortality rate of 0.5%, suggesting this is the number that should be compared to alternative treatment outcomes (269).
The vast majority of patients with vestibular schwannomas are left with some degree of hearing loss in the involved ear as a result of damage from the tumor and treatment (183; 126; 248; 385; 263). Overall, less than 10% of patients have functional hearing after surgical resection. Even as hearing preservation surgery improves, there may be some rate of progressive hearing loss over time after surgery (296; 99). About one half of patients with preoperative tinnitus may improve, but this does not appear to correlate with preservation or resection of the eighth nerve (155; 113; 191). Tinnitus may arise in the brain, such as the Heschl gyrus or other frontal, temporal, or subcortical areas, including the caudate nucleus (444) rather than the ear itself (205). Difficulties with gaze stability, mobility, and balance are seen after surgery, but the role of vestibular rehabilitation is not yet clear (316).
Although the facial nerve is anatomically intact after surgery in 90% of large tumors and almost 100% of small tumors (ie, intracanalicular and small cisternal), many patients have facial weakness (183; 287; 264). The degree of facial weakness can vary: 70% of patients with large tumors, 50% of those with medium tumors, and 30% of those with small tumors have neurapraxia of the facial nerve after resection. The weakness is permanent in 30% of cases involving large tumors and 10% of cases involving small- and medium-sized tumors. Cystic schwannomas may be more difficult to resect, with high rates of facial nerve dysfunction (276; 477). Some authors recommend aggressive, early nerve reconstruction in patients with facial nerve discontinuity (264). Using various methods of reconstruction of the severed nerve, more than 70% of patients can achieve satisfactory results (264).
Chronic postoperative headaches affect over 25% to 50% of patients and may be difficult to treat (141; 56; 08; 372); this includes some patients whose tumors are small. A C-type incision may be associated with less headache (08), as is craniotomy instead of craniectomy (372). Vertigo is a common problem postoperatively but is usually transient; persistent vertigo is rare. Vertigo occurs more often with small tumors and typically resolves after several weeks to months (383). Persistent dysequilibrium can occur, the likelihood of which has been correlated with age greater than 55 years, the presence of preoperative dysequilibrium, duration of preoperative dysequilibrium for more than 3.5 months, and central findings on electronystagmography (100). Long term dizziness has not been correlated with treatment modality but may be correlated with post treatment headache (55).
On occasion, patients have persistent cerebellar dysmetria as a result of tumor compression of the brainstem or cerebellar retraction during surgery. Impairment of the trigeminal nerve or nerves of the jugular complex (IX, X, XI) can rarely be persistent after treatment of large tumors. Other uncommon complications of schwannomas include hydrocephalus, intratumoral hemorrhage, subarachnoid hemorrhage, rapid cyst expansion, and malignant degeneration (280; 183; 248; 426). It is extremely rare for a sporadic schwannoma to degenerate into a malignant tumor (29). This complication usually occurs with tumors from patients with neurofibromatosis type 1 or neurofibromatosis type 2 or after radiation treatment. Malignant transformation may be accompanied by large copy number aberrations and homozygous deletion of the CDKN2A gene (152).
Studies attempting to assess quality of life show in many patients a significant negative impact of surgery that does not correlate with tumor size (303). In a small series, over half of the patients reported a postoperative decline in quality of life, and 20% were unable to continue their occupations following surgery. This finding has been confirmed by others (189). However, other studies have found better quality of life in patients treated with surgery than with other modalities (208) or only minor differences based on treatment modality, with declines more related to the diagnosis than the treatment (56). Quality of life in patients with tumors less than 10 mm showed a preference for observation over any active treatment (420).
Most current studies do not suggest that proliferation indices or other pathologic markers can predict the postoperative course for patients who undergo surgical resection (429), but one does suggest a correlation with Ki67 index as a predictor of recurrence (342). Macrophage infiltration may suggest a risk of recurrence (129).
Reports are appearing describing a transcanal transpromontorial microscopic/endoscopic approach for vestibular schwannomas, even with larger-sized tumors reaching the brainstem (253).
Radiosurgery. Experience with radiosurgical treatment of vestibular schwannomas generally supports its safety and effectiveness for tumors less than 3 cm in diameter. The role of radiosurgery versus open surgery continues to be debated in terms of tumor control, morbidity, and cost (213; 167; 217; 336; 339; 453; 214; 26). Attempts at direct comparison of outcomes and patient satisfaction between surgery and radiosurgery indicate an advantage for radiosurgery in the short term (195; 354; 293).
This form of treatment dates back to 1969 at the Karolinska Institute in Stockholm. Several early series reported short-term local tumor control rates of 86% to 100% (159; 117; 116; 275; 214; 182), but with higher cranial nerve injury rates at doses higher than currently recommended. New cranial neuropathies, mainly of the fifth and seventh nerve, have become less common with more advanced treatment planning (117; 116; 275; 308; 361) and dose reductions (182). New cranial neuropathy other than hearing loss more than 28 months after treatment is rare (117; 116).
A University of Pittsburgh series using currently advocated lower margin doses of 12 to 13 Gray in 829 patients reported a 10-year clinical control rate of 97%, with preservation of facial nerve function in 99% and trigeminal nerve dysfunction in 3% of tumors that reached the trigeminal nerve (244). Hearing preservation was achieved in 50% to 77%, depending on tumor size. An updated report from 2019 described 94% progression-free survival at 10 years and freedom from surgical resection in 98.7% (186). The University of Florida reported on 390 patients treated with linear accelerator-based radiosurgery (120). The 5-year actuarial control rate was 90%, with only four patients (1%) requiring subsequent surgery. After doses were reduced to 1250 cGray in 1994, trigeminal and facial nerve complications were reduced to 0.7% each. Some reports now indicate tumor control rates and complications similar to smaller tumors for tumors larger than 3 cm (307; 327).
For intracanalicular tumors with a mean follow-up of 42 months, serviceable hearing was preserved in 77.5% of those with excellent pretreatment hearing and in 85% of those with useful pretreatment hearing (304). Another series of intracanalicular tumors showed sustained tumor control in more than 90% at 10 years, freedom from need for other intervention in 98% at 10 years, and hearing preservation in 38.1% at 10 years (306). Among 74 patients with Gardner-Robertson Class I hearing treated with radiosurgery in Marseille, 78.4% had functional hearing after a minimum of 3 years of follow-up (437). Hearing preservation has been correlated to the maximum radiation dose delivered to the cochlea (437; 443; 49; 237; 261), but there is not universal agreement with this observation (185).
In a series of 51 patients followed for greater than 10 years after lower dose range radiosurgery, the local control rate was 97.7%, with only a single patient requiring surgery 10 years after treatment (361). Kaplan-Meier estimates of useful hearing preservation were 57% at 5 years and 24% at 10 years. There were no permanent new cranial nerve deficits. Indeed, progressive hearing loss may occur with longer follow up, with only 23% serviceable hearing remaining at 10 years in another long-term follow-up report (53). A 10-year follow-up study of 440 patients treated with a median marginal dose of 12.8 Gray noted 5- and 10-year progression-free survival rates of 93% and 92% (150). The 10-year facial nerve preservation rate was 97%.
Tumors growing more than 2.5 mm per year (257) or doubling times of less than 15 months (227) prior to radiosurgery may be less likely to respond to radiosurgery. It has been argued that if nongrowing tumors are excluded, 10-year local control rates may be as low as 77% (227). Cystic tumors may respond dramatically to radiosurgery (45; 94) without less effectiveness than seen in solid tumors (Massaad et al 2021). Transient tumor enlargement is common after radiosurgery and so should not be used as the sole criteria for treatment failure, even up to 3.5 years after treatment (151; 332; 295; 338; 48). Because radiosurgery does not often eliminate the radiographic tumor, long-term radiographic follow-up is necessary, and caution has been advised in differentiating the effect of radiosurgery from the natural history of untreated tumors (30). Retreatment with radiosurgery has also been reported with acceptable short-term morbidity and good tumor control (89; 484; 176).
Useful pretreatment hearing may be preserved in 35% to 85% of patients 2 years after treatment (117; 116; 309; 157; 182; 304; 482), but may continue to deteriorate in long-term follow-up (361; 386), leading some to recommend against prophylactic radiation and waiting for proven growth before treating (386). Some reports suggest that hearing loss is greater with radiosurgery than observation and do not recommend treatment for patients with excellent hearing under observation (119). Some report no difference in hearing loss between patients managed with radiosurgery or observation alone (397). Others have reported better long-term hearing preservation when radiosurgery was administered prior to hearing deterioration rather than after (09; 305). A group of 307 patients with serviceable hearing followed for a median of 7.6 years had 95% tumor control and serviceable hearing maintained in 77.8% at 3 years, 68.8% at 5 years, and 51.8% at 10 years (187). The Pittsburgh Hearing Prediction Score had predictive value. In a meta-analysis of 4234 cases from 45 publications, hearing preservation was noted at a mean follow-up of 44 months in 51% of patients, without correlation with age or tumor size, but with correlation to treatment doses of less than 13 Gray (482). Another meta-analysis of 2195 patients from 47 reports found 58% hearing preservation at 47 months (76). Doses to the cochlea above 5.3 Gray may correlate with hearing loss, and newer treatment plans may try to spare the cochlea for this reason (49; 317), with suggested doses below 4 Gray (236; 71). A fluid-filled gap between the tumor and the fundus may improve hearing preservation rates, possibly by reducing radiation to the labyrinth (43). Smaller tumors farther away from the cochlea may offer the best chance for long-term hearing preservation (37).
For patients with intracanalicular tumors, radiosurgery was reported to result in better hearing preservation rates that observation (353). Early radiosurgery may result in a higher hearing preservation rate than delayed treatment (09; 305). The reasons for hearing loss after radiosurgery are not well understood. One report has suggested that preoperative auditory brainstem response parameters may suggest elevated pressure in the auditory canal, which in turn may render the cochlear nerve vulnerable during the phase of transient tumor expansion frequently seen on MRI after radiosurgery (137). Genetics and epigenetics may also play a role in susceptibility to hearing loss with vestibular schwannomas (95).
In a Markov decision analysis using quality-adjusted life years as the outcome measure, radiosurgery was the preferred treatment for patients with small tumors that enlarged during a period of observation (286). Similarly, an analysis of published literature led another group to also report that radiosurgery showed the best treatment outcomes when compared to surgery for tumors less than 30 mm in diameter, with no direct mortality, better facial nerve and hearing outcomes, and better quality of life (473). In a matched cohort study of surgery versus radiosurgery for tumors smaller than 2.8 cm, there was no difference in the need for subsequent intervention, but radiosurgery was associated with better hearing and facial nerve preservation (127). When radiosurgery was compared to observation, the rate of hearing loss and quality of life was similar in both groups, but the need for additional treatment was significantly less in the treated group (47). Radiosurgery is less costly when compared to resection both in initial and follow-up costs (396).
Radiosurgery is a useful alternative in patients who have failed previous microsurgery, but the cranial nerve complication rate seems to be higher than for treating previously unoperated patients (335; 181; 164). There does not appear to be an advantage to immediate postoperative radiosurgery versus following patients with postoperative residual tumor and treating only after evidence of growth (90).
There is ongoing debate as to whether radiosurgery makes subsequent microsurgery more difficult (414; 337; 231; 235; 124; 172; 338; 382). Surgery after previous partial resection and radiosurgery may be the most challenging (124), but when there is good facial nerve function preoperatively, good results can be achieved by skilled surgeons (382). Others have reported poor facial nerve recovery, more disequilibrium, and a higher risk of pneumonia postoperatively after prior radiosurgery (163).
Repeated radiosurgery is an option for recurrence after prior radiation. Rates of tumor control, facial nerve injury, and hearing loss are similar to those reported for first radiosurgical treatment (24; 351).
Fractionated stereotactic radiotherapy (a combination of stereotactic, single fraction radiosurgery, and standard radiation fractionation schemes) has been tried in several centers. Preliminary results indicate tumor control rates equivalent to single fraction radiosurgery, with a possible reduction in cranial neuropathy rates in some studies but no advantage in others (274; 273; 470; 61; 74; 139; 271; 376; 15; 343; 344; 318; 323; 239; 302; 419). Two studies have reported greater decrease in tumor size after fractionated treatment than after single dose treatment (395; 171). Five dose fractionation with a resulting lower biologic equivalent dose than radiosurgery may increase the risk of recurrence (202). Hearing preservation has been reported to be more likely with fractionation (203; 344). For a group of 28 patients with serviceable hearing, a three fraction, 18 Gray treatment was reported to result in 65% hearing preservation at 8 years (344). Hearing preservation may correlate with cochlear doses below 4 Gray (36). More data are needed.
Conventionally fractionated radiotherapy may still have a role for large tumors (190).
Proton irradiation has been used to treat vestibular schwannoma, but data on comparison with photon therapy are sparse (212). Hearing preservation was not better than with other treatment modalities (387).
The risk of a radiation-induced neoplasm after stereotactic surgery is low and has been estimated at 0.04% at 15 years after treatment to 0.3% at 4.9 years (320; 334). Genetic analysis of tumors resected after prior radiosurgery did not show an increased number of mutations compared to tumors not previously irradiated (153).
Radiosurgery has been reported to be effective in patients with neurofibromatosis type 2 as well (204; 69; 70), with high rates of local control and lower facial nerve complications than surgery, but lower hearing preservation rates than surgery (70).
Chemotherapy. Drug therapy in the treatment of vestibular schwannoma was reviewed in 2021 (240) and 2022 (438). Drugs reviewed include protein tyrosine kinase inhibitors (including ErbB family protein inhibitors, PDGFR family protein inhibitors, VGEFR inhibitors, HGFR inhibitors), inhibitors of Akt signal transduction, mTORCI inhibitors, chemokine receptor-4 inhibitors, and inflammatory factor inhibitors (COX2 inhibitors, NF-kappaB inhibitors).
Reports have indicated responsiveness of some vestibular schwannomas to bevacizumab, an antivascular endothelial growth factor antibody (331; 266; 433; 206). In a study of 10 patients with neurofibromatosis type 2, tumors shrank in nine patients and the response was maintained in four patients over 11 to 16 months (331). Another report on 17 patients reported hearing improvement in 56% and decrease tumor volume in 47% (433). Toxicity may limit its use (243). Some of the systemic toxicity of bevacizumab may be avoided by selective intra-arterial infusion (359). However, intraarterial administration of bevacizumab would not be deemed routine as the systemic toxicity of bevacizumab can often be easily managed. Preoperative indium-bevacizumab scintography predicted tumor response in one of the bilateral tumors in a patient with NF2 (456). The response to radiation therapy may be enhanced by bevacizumab in an animal model (123).
The presence of proinflammatory cytokines TGF-beta1, IL-1beta, and IL-6 in vestibular schwannomas compared with normal vestibular nerves suggests a role for inflammation in the growth of these tumors (439). Aberrant COX-2 expression and aberrant expression of the downstream product prostaglandin E2 have led to trials of salicylates in primary vestibular schwannoma cell cultures and reports of reduced tumor growth in patients taking these agents (91; 192). Aspirin may be considered for use in tumors under observation (450). OSU-03012, a novel derivative of COX-2, is another potentially useful agent (240).
Erlotinib, a small molecule EGFR-specific tyrosine kinase inhibitor, has also been tried to control the tumor after contralateral resection (330); however, 11 other patients did not respond to this agent (329). It is currently not recommended for use (450). The use of trastuzumab and lapatinib have also been reported (240).
Activation of EGFR family receptors in human tissue samples leads to a trial of the small-molecule EGFR/ErbB2 kinase inhibitor, lapatinib, in an in vitro human schwannoma model (12). Antiproliferative activity was shown, and a human trial is reportedly underway. Lapatinib may be considered for use in NF-2 related tumors (450). Another EGFR tyrosine kinase inhibitor, icotinib, has also shown radiographic and hearing responses in NF2 patients (489).
PDGFR family protein inhibitors, such as imatinib, nilotinib, and ponatinib, have also been reported to have activity (240). Nilotinib alone, or in combination with selumetinib, has been shown to inhibit schwannoma growth in vitro through the platelet-derived growth factor receptor/c-KIT pathway and MEK1/2 pathway respectively (14). Similarly, imatinib has also been shown to inhibit in vitro tumor proliferation through the platelet-derived growth factor receptor/c-KIT pathway (11).
The role of c-MET inhibition is being investigated in these tumors (121). The c-MET and anaplastic lymphoma kinase inhibitor crizotinib is in phase 2 trials for NF2 patients with progressive vestibular schwannomas (240).
As merlin is thought to be a negative regulator of the mammalian target of rapamycin complex 1 (mTORC1), the mTORC1 inhibitor rapamycin has been shown to inhibit in a mouse allograft model of NF2 schwannoma (125). By extension, the rapamycin analog sirolimus was then shown to induce tumor growth arrest in a human NF2 patient (125). Everolimus, a derivative of rapamycin, was not effective in one trial but was reported to reduce tumor growth rate in another (240). In cultured vestibular schwannoma tumor cells, a dual mTORC1/2 inhibitor and dasatinib exhibited a therapeutic effect (375).
As the molecular pathways giving rise to schwannomas are elucidated, it is expected that more novel treatment strategies will appear (118; 279; 428; 240).
An association between metformin use and slower growth of vestibular schwannoma has been reported (114).
Bilateral tumors. A patient with bilateral vestibular schwannomas represents a more difficult situation. Intervention risks bilateral hearing loss and bilateral facial paralysis, both of which are major deficits. If one tumor progresses more rapidly or one ear loses useful hearing, then the side of first intervention may be dictated by clinical circumstances. Intracapsular, subtotal resection may be indicated to preserve hearing in the remaining hearing ear, or internal auditory canal decompression without tumor resection may also preserve hearing for some time (38; 44). Radiosurgery may be indicated in some patients (238; 139; 69). However, sudden deafness complicates radiosurgery in some of these cases, particularly with larger tumors (180; 63). Some argue for early intervention when the chances for hearing preservation are highest, whereas others prefer observation for as long as possible. Bevacizumab may offer some hope for these patients (330; 331), as do some other novel therapies (428). All agree that patients and their family should learn to sign while still able to hear.
Simultaneous tumor resection and cochlear implantation is now being reported (82; 465).
Pregnancy does not appear to influence the growth of vestibular schwannomas (31).
Atypical vestibular schwannomas are rare but have been reported (211).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Donald A Ross MD
Dr. Ross of Oregon Health and Science University has no relevant financial relationships to disclose.
See Profile
Deric M Park MD FACP
Dr. Park of the University of Chicago has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
Mar. 21, 2024
Neuro-Oncology
Mar. 01, 2024
Stroke & Vascular Disorders
Feb. 26, 2024
Neuro-Oncology
Feb. 21, 2024
Neuro-Ophthalmology & Neuro-Otology
Feb. 15, 2024
Neuro-Oncology
Feb. 12, 2024
General Neurology
Feb. 07, 2024
Neuromuscular Disorders
Jan. 29, 2024