
















General Neurology
Dysphagia
Mar. 18, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author explains the clinical presentation, pathophysiology, diagnostic work-up, and management of disequilibrium. Vestibular vertigo is a common problem, particularly in the elderly. Careful history and detailed examination, including focused evaluation of proprioception, vestibular function, directional bias of postural sway, ability to maintain stance with eyes open and closed (Romberg test), ability to maintain stance despite perturbations (eg, pull test), and gait will allow distinction of the major categories of disequilibrium in most cases and will often allow a specific etiologic diagnosis as well.
|
• Postural control is not simply a collection of righting and equilibrium reflexes but is instead a complex motor skill derived from the interaction of multiple sensorimotor processes. | |
|
• Postural control can be divided into two component abilities or subgoals: postural orientation and postural equilibrium (ie, balance). | |
|
• Disequilibrium is a state of nonvertiginous altered static (eg, standing) or dynamic (eg, walking) postural balance. | |
|
• Patients with disequilibrium often complain of unsteadiness, imbalance, and falls. | |
|
• Except in cases of visual-vestibular mismatch, patients with sensory disequilibrium generally do worse in the dark and frequently have a Romberg sign on examination, whereas motor disequilibrium caused by impaired motor performance is generally not exacerbated in the dark or by closing the eyes. |
Postural control is not simply a collection of righting and equilibrium reflexes but is instead a complex motor skill derived from the interaction of multiple sensorimotor processes (291; 165; 323; 173). Postural control can be divided into two component abilities or subgoals: postural orientation and postural equilibrium (ie, balance). To maintain postural orientation requires active control of body alignment and tone with respect to the visual environment, gravity (ie, components of the vestibular system), the support surface (ie, mediated by cutaneous mechanoreceptors), and internal cues that provide awareness of the position and movement of the body (ie, proprioception); thus, spatial orientation requires the interpretation of convergent sensory information from the visual, vestibular, and somatosensory systems. Postural equilibrium requires the coordination of multiple sensorimotor strategies to stabilize the body’s center of mass over the base of support (ie, the area beneath an object or person that includes every point of contact that the object or person makes with the supporting surface), during both self-initiated and externally triggered disturbances in postural stability (272; 165).
Disequilibrium is a state of nonvertiginous altered static (eg, standing) or dynamic (eg, walking) postural balance (188; 206). This framework for disequilibrium derives in part from an influential paper by Drachman in 1972 that employed a 4-fold categorization of dizziness: vertigo, disequilibrium (with sensory and motor subcategories), presyncope, and psychophysiological (psychogenic) dizziness (113); disequilibrium was further divided into sensory and motor subtypes to reflect the predominant clinical dysfunction responsible. However, an alternative approach might have been to consider vertiginous disequilibrium as an additional subcategory of disequilibrium.
The clinical literature contains many articles that use “disequilibrium” (or “dysequilibrium”) as a synonym or umbrella term for dizziness, often encompassing vertigo, orthostatic hypotension, and psychogenic conditions as well as motor and sensory disequilibrium. However, in this article, disequilibrium is to be understood as distinct from these other disorders, recognizing of course that patients can be imprecise in describing the sensations of dizziness that they experience. Although the imprecision of a patient’s report can complicate clinical assessment, it doesn’t change the task of sorting out the underlying process that is responsible for the patient’s complaints. Therefore, these terms should be used to indicate the underlying pathophysiology and not some label that the patient gives to his or her complaints.
Disequilibrium has been labeled as “unsteadiness” in the International Classification of Vestibular Disorders I (ICVD-I), the first consensus document of the Committee for the Classification of Vestibular Disorders of the Bárány Society (39).
Romberg sign. In the first half of the 19th century, European physicians described loss of postural control in darkness in patients with severely compromised proprioception, a phenomenon that became known as the “Romberg sign” (216). Early in its history, the sign was linked to tabes dorsalis (locomotor ataxia), later known to be a tertiary stage of syphilis. By the end of the 19th century, the Romberg sign had developed from a patient-reported symptom of a specific disease (ie, tabes dorsalis) into a bedside-elicited sign of deafferentation (216; 204; 205; 204).
In his Lectures on the Nervous System and its Diseases (1836), English physician Marshall Hall (1790 to 1857) described the loss of postural control in darkness among patients with severely compromised proprioception (153; 216):
|
I have this day seen a patient with a slight degree of paralysis of feeling and of voluntary motion of the lower limbs. He walks safely while his eyes are fixed upon the ground, but stumbles immediately if he attempts to walk in the dark. His own words are “my feet are numb; I cannot tell in the dark where they are, and I cannot poise myself.” The voluntary motions are regulated by the sense of touch, when this is unimpaired; or by that of sight, when touch is paralyzed (153). |
Hall recognized that: (1) proprioception and vision were important for postural control; (2) vision could at least partially compensate for defective proprioception; and (3) in the absence of vision (eg, in darkness) proprioceptive deficits can produce overt impairment of postural control.
Several years after Hall’s initial description, in the second edition of Lehrbook der Nervenkrankheiten des Menschen in 1851, and in a subsequent English translation in 1853, German neurologist Moritz Romberg (1795 to 1873) described the loss of postural control in patients with tabes dorsalis on closing their eyes or in darkness (299; 300). Romberg devised a bedside clinical test to demonstrate the phenomenon, although Romberg’s approach was simply to observe a change in postural control when patients were asked to close their eyes (without any stated preferred position of the feet).
|
If the patient [with tabes dorsalis] is told to shut his eyes while in the erect posture, he immediately begins to move from side to side, and the oscillations soon attain such a pitch that unless supported, he falls to the ground . . . The eyes of such patients are their regulators, or feelers; consequently in the dark, and when amaurosis supervenes, as is not unfrequently [sic] the case, their helplessness is extreme . . . The feet feel numbed [sic] in standing, walking, or lying down, and the patient has the sensation as if they were covered with a fur . . . The gait begins to be insecure, and the patient attempts to improve it by making a greater effort of the will; as he does not feel the tread to be firm, he puts down his heels with greater force. From the commencement of the disease, the individual keeps his eyes on his feet to prevent his movements from becoming still more unsteady. If he is ordered to close his eyes while in the erect posture, he at once commences to totter and swing from side to side; the insecurity of his gait also exhibits itself more in the dark. It is now ten years since I pointed out this pathognomonic sign [ie, c. 1840] (300). |
German physician Bernardus Brach (1799-?) described similar symptoms around the time that Romberg claimed to have recognized them, and he published them more than a decade before Romberg:
|
It is known that people with tabes dorsalis have an unusual gait . . . While other paralytics drag their legs, a patient with tabes dorsalis lifts his leg with a straight knee and with difficulties. When he steps with his feet hard and taps on the floor, his whole body is stiff and strained. With fearful eyes he watches his every step. He is dependent upon his cane for support . . . He doesn’t feel the movement he makes with his legs . . . Because of this, he raises his legs slowly to maintain balance . . . He has no sensation [proprioception] in his lower limbs, so he relies upon his other senses. When walking, he is very fearful of falling and uses his body and arms for counter-balance. He finds it nearly impossible to walk on a level walkway in conversation with others, or in the dark. With two patients I observed these symptoms. With tests such as cold and warm, pressure, pinching, scratching with a needle tip, or a hair, the patients responded just like a healthy person. Thus, one cannot say that they don’t have any sensation (52). |
Despite their inability to stand or walk in the dark, Brach noted that such patients were not weak; indeed, in the fall of 1838, a 36-year-old educated man made a 5-hour journey on foot to visit Brach and reported his symptoms in a letter to him (52):
|
I must watch carefully every step and stone. I must use my eyes to guide me. In the dark I have no sense of balance, and even though familiar with the area, I will certainly fall. When walking, I must fully concentrate on the task of walking and not on conversation with people . . . I step so hard on my feet that my soles are sore and inflamed after a short distance. My self-confidence is low when walking up steps, over crooked paths, strange places, or with many people (52). |
In A Manual of Diseases of the Nervous System (1888), British neurologist William Gowers (1845 to 1915) presented a clear account of how to optimally perform the Romberg test, adding instructions that the patient should assume a narrow base as part of the test (142):
|
The characteristic incoordination of movement [in tabes dorsalis] develops gradually. It is always increased (as Romberg first pointed out) by closure of the eyes and at first may only exist when the guiding influence of vision is, thus, withdrawn. Before it causes ataxy of movement, it may render difficult the maintenance of equilibrium when the base of support is narrowed by the feet being placed close together, toes and heels. If then the eyes are closed, the patient sways, and may even tend to fall. In health slight unsteadiness is thus produced, varying in degree in different persons, but never amounting to even a suggestion of a fall . . . The early defect in coordination may be discovered by the patient when he walks in the dark, or, not uncommonly, when he shuts his eyes in the process of washing the face. In a further degree of incoordination there is inability to stand with the feet together even when the eyes are open, and the patient is only steady when the feet are wide apart. If the feet are bare, the difficulty is greater, because muscular action has to replace the rigid base of the boot (142). |
Although some felt or implied that the Romberg phenomenon was a specific sign of tabes dorsalis, others soon recognized that it was a more general sign of deafferentation. Later authors recognized that the sign was not specific even to deafferentation, noting that it may be present in some patients with vestibular or even cerebellar lesions.
Station and postural sway. As noted in 1886 by Philadelphia neurologist Silas Weir Mitchell (1829 to 1914) and his trainee Morris Lewis (1852 to 1928):
|
[Station is] the relative power to stand steady, with eyes open or shut. This symptom can be made numerically accurate by standing the patient in front of a bar marked in inches and placed on a level with the ears. The extent of lateral sway of the head may thus be easily observed; a like observation records the anterior tendency. The first is rarely over half an inch in health; the second does not usually exceed an inch, even with closed eyes. Any large increase is suspicious (247). |
Mitchell developed a simple sway meter to measure postural sway as part of the clinical examination (246).
Mitchell’s sway meter consisted of 2 rulers, graduated in inches, placed perpendicular to each other on a stand. Applying the sway meter in patients with tabes dorsalis, Mitchell and Lewis found that impairment of station progressively worsened over the course of the disease and was associated with both progressive loss of muscle stretch reflexes and loss of the ability to augment these with reinforcement (247). Muscle stretch reflexes were lost early in the legs, even with reinforcement, while station (with eyes open) remained normal; by the time station became severely impaired, muscle stretch reflexes were also lost in the arms.
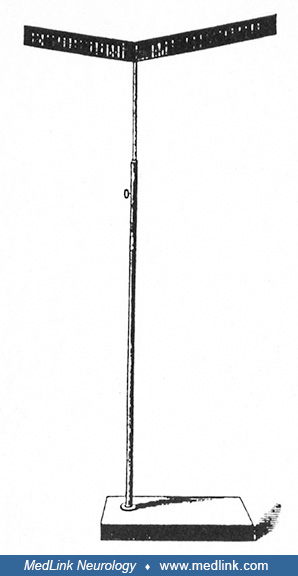
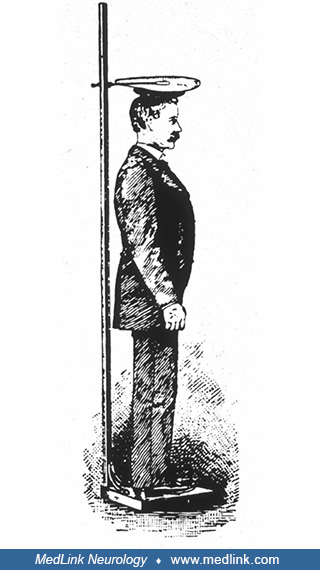
Philadelphia neurologist Guy Hinsdale (1858 to 1948), who served as an assistant to both Mitchell (in the mid-1880s) and William Osler (c. 1888 to 1889), published two studies of postural sway in the late 19th century using Mitchell’s sway meter and more refined graphical methods (161; 162). One graphical method employed a simple recording apparatus in practical use in Mitchell’s clinic contemporaneously with the sway meter:
|
Tracings were taken by attaching to the top of a man’s head a flat piece of cardboard, upon which was stretched some smoked paper. The subject was then placed under an index, free to move up and down, in a fixed line, and which traced curves on the paper as the subject who stood beneath swayed in any direction (161). |
Hinsdale measured postural sway using his apparatus in several groups of people, including normal adults and children, inmates of the Institution for the Blind, and individuals with various neurologic disorders (including tabes dorsalis). In normal individuals, Hinsdale observed postural sway that increased with the eyes closed. In experiments on themselves, Hinsdale and fellow Philadelphia physician William C. Lott found that the postural sway of normal individuals was exaggerated with ether. Blind individuals tended to sway about as much as healthy individuals with their eyes closed, whereas the sway of persons with tabes dorsalis was decidedly greater.
Other American neurologists developed similar devices, including an instrument developed by New York neurologist Charles Loomis Dana (1852 to 1935) around the turn of the century--the “ataxiagraph” (98).
Such nineteenth-century efforts to record and quantitate postural sway under various circumstances and in various pathologic conditions anticipated later physiologic studies as well as the introduction of computerized dynamic platform posturography in the 1970s and 1980s and, later, the less sophisticated but more easily applied technique of foam posturography.
The “dynamic Romberg sign.” In the late 1870s and 1880s, prior to the development of movie cameras or projectors, English-American photographer Eadweard Muybridge (1830-1904) photographed sequential images of people and animals in motion, using arrays of sequentially triggered single-image cameras (256; 209; 211; 215).
In 1885, Philadelphia neurologist Francis Dercum (1856-1931) collaborated with Muybridge at the University of Pennsylvania to photograph sequential images of patients with various neurologic disorders involving abnormal movements and, particularly, various gait disorders, including the sensory ataxic gait of tabes dorsalis (256; 106; 107; 216; 209; 215).
The Dercum-Muybridge collaboration produced the first motion-picture sequences of neurologic gait disorders ever filmed. In particular, Muybridge’s Plate 550 is remarkably informative in demonstrating the clinical features of the sensory ataxic gait, with fairly normal gait while walking with eyes open but with marked decompensation and evident ataxia while trying to walk with eyes closed, a phenomenon I have previously labeled the “dynamic Romberg sign” (216).
Internist William Osler (1849-1919), who had been appointed Chair of Clinical Medicine at the University of Pennsylvania in Philadelphia in 1884, was present there during the Dercum-Muybridge collaboration in 1885. One of Osler’s later aphorisms succinctly expressed the dynamic Romberg phenomenon in such patients: “The normal man walks by faith, the tabetic by sight” (273; 210; 215).
Postural instability in Parkinson disease. Postural instability was first described as a feature of Parkinson disease by Romberg in 1853 (300; 169). In the 1880s, French neurologist Jean-Martin Charcot (1825-1893) recognized a tendency to propulsion and retropulsion in patients with Parkinson disease and then began attempts to evaluate postural instability by pulling the clothes of patients (75; 169; 254).
Several clinicians noted postural instability, and some offered simple clinical assessments or tests that can, in retrospect, be seen as precursors of the modern pull test (142; 240; 53; 244; 249; 103; 235). In the 1960s, neurologists Margaret Hoehn (1930-2005) and Melvin Yahr (1917-2004) assessed postural instability in patients with Parkinson disease using a push on the sternum (163). The modern form of the pull test was proposed by neurologist Stanley Fahn in the 1980s; in 1987, the pull test was incorporated into the Unified Parkinson's Disease Rating Scale (UPDRS) (123).
Postural instability in bilateral vestibulopathy. In the late 19th century, several investigators, including American psychologist and philosopher William James (1842-1910), studied the manifestations of absent labyrinthine function in deaf-mute patients.
James found that manifestations included dysequilibrium, ataxia, absence of vertigo during or after rotation, reduced caloric and rotation-induced nystagmus, and resistance to seasickness (175; 213).
In 1941, neurosurgeon Walter Dandy at Johns Hopkins reported disequilibrium (especially in the dark) and oscillopsia in patients with Meniere disease who underwent bilateral vestibular nerve section (99; 207).
|
Division of both vestibular nerves is attended by one rather surprising after effect, jumbling of objects (visual) when the patient is motion. As soon as the patient is at rest, the objects are again perfectly clear. The other disturbance is uncertainty when the patient is walking in the dark. Both of these effects persist, though with gradual lessening in severity (99). |
Although these manifestations of bilateral vestibulopathy were later called “Dandy syndrome,” similar observations following bilateral vestibular nerve section had been reported earlier by neurologist Frank R Ford (1892-1970) and neuro-ophthalmologist Frank B Walsh (1895-1978) in a surgical patient of Dandy’s (130; 207; 212):
|
During convalescence [following bilateral vestibular nerve section], it became evident that a new series of symptoms had developed. Objects seemed to move before his eyes unless his head was kept perfectly still. Walking caused objects to “jump” before his eyes to some extent . . . He was also very unsteady in the dark. (130). |
In 1950, Ford summarized the observations he made with Walsh in the 1930s:
|
Destruction of the vestibular apparatus on both sides in man produces a constant unsteadiness of station and gait, which is exaggerated in the dark and also by sudden movements of the head. There is also a striking inability to fix objects with the eyes when the head is in movement so that the patients complain of objects seeming to dance or oscillate before their eyes when they are walking or riding in a car. This oscillation ceases as soon as the head is held still (129). |
Similar observations in nonsurgical patients were also made by neurologist Paul M Levin (1906-1978) before Dandy's report (225). Levin had also been at Johns Hopkins at the time of Ford and Walsh’s initial report.
With the widespread use of streptomycin in the late 1940s, clinicians began to recognize the full clinical syndrome of acquired bilateral vestibulopathy. Some patients treated with streptomycin for tuberculosis developed disabling disequilibrium, ataxia, and oscillopsia, and the clinical features of these patients resembled those described earlier by Dandy (87; 88; 89; 214). The most important report from that period was a case of “JC,” anonymously reported by a 30-year-old physician in 1952 (87). “JC” was John “Jack” Douglas Crawford II (1920-2005), an identity that Crawford acknowledged in a separate publication the same year as his original report (88).
Postural instability and sensory ataxia in neuronopathies. Postural instability and sensory ataxia were recognized sporadically with multiple disorders that produced neuronopathies. Initially, in the mid-19th century, tabes dorsalis (“locomotor ataxia”) was most closely linked with this type of disequilibrium.
The sensory ataxic gait results from loss of proprioceptive input. Key clinical features of the sensory ataxic gait include: (1) relatively normal gait with eyes open but gait ataxia with eyes closed, (2) Romberg sign, (3) impaired joint-position sense, (4) pseudoathetosis, and (5) sensory drift (as distinct from pronator drift).
The sensory ataxic gait is sometimes called a “stomping gait” because patients learn to compensate for their proprioceptive deficits by using an auditory cue (ie, the sound from forcefully striking the ground). To accomplish this some may, with eyes open, lift their legs higher than normal to strike the ground with sufficient force. Consequently, from continued excessive joint trauma, their joints may be damaged over time, producing what has been variously labeled “Charcot joints” or neuropathic arthropathy.
In the 1980s, multiple investigators reported that pyridoxine overdose causes a pure sensory neuronopathy with sensory ataxia, poor coordination, numbness, and decreased sensation to touch, temperature, and vibration. Sensory neuronopathy from pyridoxine abuse was first recognized by neurologist Herbert H Schaumburg and colleagues at Albert Einstein College of Medicine in 1983 (303). Subsequently, multiple authors described sensory neuronopathy (and less commonly a sensorimotor neuropathy) in patients who consumed high doses of pyridoxine (ie, most consumed greater than 2 g/day) (320; 281; 95; 04; 97; 03; 241; 202; 101; 136; 71; 137; 201; 118). Some of these cases were iatrogenic, resulting from pyridoxine treatment of pyridoxine-dependent epilepsy, homocystinuria, mushroom poisoning, and premenstrual syndrome (04; 97; 03; 241; 118). The pyridoxine dose varied from 200 mg to 10 grams per day for periods of up to 20 years (307). Symptoms began one month to several years after starting pyridoxine. Duration of consumption prior to symptom onset was inversely proportional to dose. In many cases, symptoms partially improved following discontinuation of pyridoxine, but many were still left with severe disability. The relationship between pyridoxine overdose levels and histological damage has now been well characterized in both humans and animals. Pyridoxine given in large doses selectively destroys large-diameter peripheral sensory nerve fibers, leaving motor fibers intact.
Cerebral balance disorders. Over the past century, there have been significant advances in the classification of balance disorders, although significant gaps in our understanding remain. For example, late in the 19th century, Bruns coined the term frontal ataxia to describe cerebral-related (mainly frontal lobe) balance and gait disorders, but his term fell out of favor; the concept of frontal gait apraxia began to be used during the first quarter of the 20th century and continues to be used, with some controversy, into the 21st century. Gerstmann and Schilder in 1926 described two patients with frontal lesions and what they labeled as “gait apraxia”; the patients were unable to lift their feet to walk and could not stand or sit without falling backwards (329). Despite the confusing terminology surrounding cerebral balance disorders and despite our limited understanding of their pathophysiology, historical cases show that cerebral balance disorders are caused by mainly subcortical, frontal, and occasionally parietal lesions (336; 133; 104) and that cerebral balance disorders are characterized by varying combinations of parkinsonian, ataxic, spastic, “magnetic” (feet stuck to ground), and “apractic” qualities. For simplification, this article adopts a generic term, cerebral balance disorders, to refer to balance disorders due to cortical or subcortical lesions.
Psychiatric, psychogenic, and somatoform disorders. In 1860, Swiss physician Sigismond Jaccoud (1830-1913) described the inability to stand (ie, “astasia”) in the face of normal limb movement (187; 328).
In 1888, French neuropathologist Paul Blocq (1860-1896) first used the term “astasia-abasia,” which came to refer to any “nonorganic” gait (271); such use, however, is not precise and should be discouraged. Instead, either the term “psychiatric balance disorder” (ie, referring to balance disorders attributable to psychiatric ailments, such as schizophrenia or depression) or “psychogenic balance disorder” (ie, referring to balance disorders due to a somatoform disorder when a known stress is present) or “somatoform disorder not otherwise specified” (when no known stressful event is present) should be used (08).
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125