








Epilepsy & Seizures
Ambiguous paroxysmal events
Mar. 22, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Focal clonic seizures are a type of neocortical seizure emanating from the contralateral primary motor cortex. They are repetitive, brief and rhythmic, unilateral, and rapidly alternating contractions and relaxations of localized groups of muscles. They may affect the thumb only, the thumb and ipsilateral side of the lips, the hand, the whole arm, or any other contralateral to the focus body part. They may remain focal or progress to a Jacksonian march and hemiclonic or generalized tonic-clonic seizures. Etiology is variable, ranging from genetic, metabolic, or any type of focal structural lesions. Rolandic epilepsy is a common idiopathic syndrome with focal clonic seizures. Brain tumors, infections, malformation of cortical development, and trauma are other common structural causes. In this updated article, the author details the historical aspects, classification, clinical manifestations, pathophysiology, EEG, differential diagnosis, and management of patients with focal clonic seizures.
• Focal clonic seizures are a type of neocortical seizure emanating from the contralateral primary motor cortex. | |
• They are repetitive, brief and rhythmic, unilateral, and rapidly alternating contractions and relaxations of localized groups of muscles. They may affect the thumb only, the thumb and ipsilateral side of the lips, the hand, the whole arm, or any other contralateral to the focus body part. | |
• They may remain focal or progress to a Jacksonian march and hemiclonic or generalized tonic-clonic seizures. | |
• They often occur in conjunction with tonic, atonic, myoclonic, somatosensory, and other ictal manifestations. These may precede, occur concurrently, or present at some stage after the onset of the clonic convulsions. | |
• Postictal paresis (Todd paralysis) is common. | |
• Etiology is variable, ranging from genetic, metabolic, or any type of focal structural lesions. Rolandic epilepsy is a common syndrome with focal clonic seizures. Brain tumors, infections, malformation of cortical development, and trauma are other common causes. | |
• Investigative procedures include brain MRI and EEG. | |
• Prognosis and management depend on the underlying cause. |
The first account of focal clonic seizures can be found as early as 1050 BC in the twenty-fifth Babylonian cuneiform tablet devoted to miqtu (a disease in which the person loses consciousness and foams at the mouth) (75):
In the time of his possession, while he is sitting down, his (left) eye moves to the side, a lip puckers, saliva flows from his mouth, and his hand, leg and trunk on the left side jerk (or, twitch) like a (newly)-slaughtered sheep, it is miqtu. If at the time of the possession his mind is consciously aware, (the demon) can be driven out; if at the time of the possession his mind is not so aware, (the demon) cannot be driven out. |
However, every student of neurology is familiar with the contributions of Louis Francois Bravais (08) and John Hughlings Jackson (31; 32; 33; 29; 30) in the clinical description of motor seizures from the primary motor cortex (ie, Bravais-Jackson seizure, Jacksonian seizure) (42; 15; 54).
The following are exact quotations from Jackson relevant to focal clonic seizures and postictal paralysis:
Convulsions and other paroxysms are owing to (1) sudden, (2) excessive, and (3) temporary nervous discharges.
The quantity of cortical grey matter varies not so much with the size of the muscles of a part of the body, as with the number of movements of that part. Thus the small muscles of the fingers will be represented by much more grey matter in the cortex than will be the voluminous muscles of the upper arm, because the former serve in more numerous, different, and in more specialized movements. Greater differentiation of function implies larger representation in the brain. I mention epileptiform seizures first because their localisation is not doubtful. (They were first described by Bravais in 1824). They are "middle level fits"—that is, they are produced by excessive discharges beginning in parts of the middle level (motor province) of the cerebral system ("motor region"). The three commonest varieties of epileptiform seizures are: (1) Fits starting in the hand (most often in the thumb or index finger or in both). (2) Fits starting in one side of the face (most often near the mouth) or in the tongue, or in both these parts. (3) Fits starting in the foot (nearly always in the great toe). Of necessity the three Varieties depend on the fact that the local discharging lesion is of cells of different parts of the "motor region"—of hand, face, and foot centre respectively. The starting point is almost invariably the same in each patient, but not always… Often enough there is "tingling" or some other crude sensation in the place of onset before convulsion starts. Admitting that there are many ranges, it is allowable to make arbitrary divisions (they must not be taken for real distinctions) into four ranges: (1) Terminal fit—the spasm involves, say the hand, or some part of it only; (2) monospasm—the arm becomes involved; (3) hemispasm; (4) bilateral convulsion—the second side being gained, the fit becomes universal. Observe the use of the word "become." In the range (4) there is a March of spasm from the part first seized all over the body, answering to increased spreading of the central excessive discharge beginning in some particular part of the motor region of the first half, and may be extending to the second half, of the brain. The second side of the body (in 4) is affected later, and commonly less than, the first side. We have not only to note how much of the body is ultimately involved, but also the order in which the several parts involved are affected—the March of the convulsion. There is not a simple, but a compound sequence of spasm; the convulsion does not cease in one part when another is involved. To observe, to give a simple example, how much of the arm has been involved when convulsion appears in the face will, I think, help us to clearer notions of localisation of movements of those two separate parts of the body in the centre discharging (anatomical localisation); or if not, at any rate as to the time relations of different elements of different centres (physiological localisation). From increasing discharge of a motor centre there is a double effect; there is not simply "more convulsion," there is (1) greater amount of convulsion of the part first seized, and there is (2) extension of convulsion to the next part of the same muscular region, or to some other part represented in the centre discharging (or in another centre connected with the one primarily discharging by particular time relations). The term post-epileptiform paralysis will be used to include all paralyses the immediate sequels of epileptiform seizures. Arbitrary divisions may be made, speaking of range only. (1) Terminal paralysis, as of a hand; (2) monoplegia, as of an arm; (3) hemiplegia; and (4) a range, which is not generally admitted—some degree of slight universal paralysis. I hold the hypothesis (essentially that of Todd* and Alexander Robertson) that there is exhaustion of central nervous elements, including fibres of the second segment of the kinetic route, and that this is produced by the sudden and excessive discharge in the prior paroxysms. These nervous elements are exhausted not otherwise injured. |
*This paralysis was long ago described by Todd under the name "epileptic hemiplegia."
The magnitude of Jackson’s contributions should be appreciated considering that his inferences encountered strong opposition during his lifetime, and the contemporary view was the notion that the cerebral convolutions were "for mentation" only (73). Gordon Holmes said of Jackson (28):
Local motor epilepsy was, it is true, recognized and described by Bravais in 1827, but it was Hughlings Jackson who first associated it with disease of the opposite hemisphere of the brain; his observations on it threw the first light on the localization and organization of the cortical motor apparatus. …. The chief features of Jacksonian epilepsy are well known, but its study helps to explain some of the phenomena of the rarer forms of local epilepsy. |
Foerster said of Jackson (20):
Jackson's ideas were revolutionary. In his days the prevalent view as to the cause of epilepsy was that it depended upon disturbances of the medulla or the pons, and nobody believed that the cortex of the brain, the organ of mind, contained motor nervous elements and that an epileptic convulsion was nothing but a sudden, rapid and excessive discharge of these cortical motor cells… Postparoxysmal paralysis was studied carefully by Jackson. He refers to previous observations of Todd and Robertson on epileptic hemiplegia, but Jackson was the first to give the physiological explanation of the paralysis subsequent to epileptic convulsions, an explanation which has been accepted by all succeeding investigators. The paralysis is due to exhaustion of the cortical motor nerve-cells, and on this depends the transient loss of function. |
It was Charcot who coined the name “Jacksonian epilepsy” in 1877, and later “epilepsie Bravais-Jacksonienne” in 1887 (15).
Robert Bentley Todd described "epileptic hemiplegia," which is now known as Todd paralysis (05). Todd held that some patients “who recover from a severe fit, or from frequently repeated fits of epilepsy, are often found to labor under hemiplegia, or other modifications of palsy" (69). He believed that this resulted from "undue exaltation [resulting in] a state of depression or exhaustion. A paralytic state remains sometimes after the epileptic convulsion. This is more particularly the case when the convulsion has affected only one side or one limb: that limb or limbs will remain paralytic for some hours, or even days, after the cessation of the paroxysm, but it will ultimately perfectly recover” (69).
Aleksei Kozhevnikov described epilepsia partialis continua and its association with chronic encephalitis in 1894 (37; 55; 71; 24).
The history of the brain mapping with electrical stimulation can be found in the writings of Penfield and associates, from Fritsch and Hitzig’s research in electrical stimulation (who, by applying galvanic currents through bipolar electrodes to the anterior half of the dog's hemisphere, obtained movements of muscle groups in the opposite half of the body) to the pioneering work of Foerster, Penfield and Jasper, and Penfield’s formulation of the homunculus (59; 60; 61).
Terminology and classification. The 2010 and 2014 ILAE reports define focal clonic seizures as follows (04; 12):
Focal epileptic seizures are conceptualized as originating within networks limited to one hemisphere. They may be discretely localized or more widely distributed. Focal seizures may originate in subcortical structures. For each seizure type, ictal onset is consistent from one seizure to another, with preferential propagation patterns that can involve the contralateral hemisphere. In some cases, however, there is more than one network, and more than one seizure type, but each individual seizure type has a consistent site of onset. Focal seizures do not fall into any recognized set of natural classes based on any current understanding of the mechanisms involved. In the 2014 ILAE epilepsy diagnosis manual, focal motor seizures are classified among those with elementary motor features that involve a stereotyped contraction of a muscle or group of muscles. Such motor features may be predominantly convulsive (rhythmic jerking (clonic activity)) (12). |
In 1981, the ILAE Commission of Classification and Terminology classified focal clonic seizures amongst “partial seizures with motor signs” (10):
A. Partial Seizures 1. With motor signs. Any portion of the body may be involved in focal seizure activity depending on the site of origin of the attack in the motor strip. Focal motor seizures may remain strictly focal or they may spread to contiguous cortical areas producing a sequential involvement of body parts in an epileptic “march.” The seizure is then known as a Jacksonian seizure. Consciousness is usually preserved; however, the discharge may spread to those structures whose participation is likely to result in loss of consciousness and generalized convulsive movements. Other focal motor attacks may be versive with head turning to one side, usually contraversive to the discharge. If speech is involved, this is either in the form of speech arrest or occasionally vocalization. Occasionally a partial dysphasia is seen in the form of epileptic palilalia with involuntary repetition of a syllable or phrase. Following focal seizure activity, there may be a localized paralysis in the previously involved region. This is known as Todd paralysis and may last from minutes to hours. When focal motor seizure activity is continuous it is known as epilepsia partialis continua. Postictal Paralysis (Todd Paralysis): This category refers to the transient paralysis that may occur following some partial epileptic seizures with focal motor components or with somatosensory symptoms. Postictal paralysis has been ascribed to neuronal exhaustion due to the increased metabolic activity of the discharging focus, but it may also be attributable to increased inhibition in the region of the focus, which may account for its appearance in non-motor somatosensory seizures. |
The ILAE core group classified focal clonic seizures as follows (17):
A. Local | ||
(1) Neocortical | ||
(a) Without local spread. Focal clonic seizures are brief focal motor events that are distinguished from focal myoclonic seizures by their rhythmic repetition. Localization to the primary motor cortex is implied. | ||
(b) With local spread. Jacksonian march seizures refer to the clinical manifestations of the slow ephaptic propagation of epileptic discharge along the motor cortex, although similar progression can sometimes be seen in other primary cortical areas as well. | ||
B. With ipsilateral propagation to: | ||
(1) Neocortical areas (includes hemiclonic seizures) | ||
The most recent ILAE positional papers on the operational classification of seizure types classify seizures of focal onset as follows:
• Aware or impaired awareness | |
• Motor onset (automatisms, atonic, clonic, epileptic spasms, hyperkinetic, myoclonic, tonic) | |
• Nonmotor onset (autonomic, behavior arrest, cognitive, emotional, sensory) | |
• Focal to bilateral tonic-clonic |
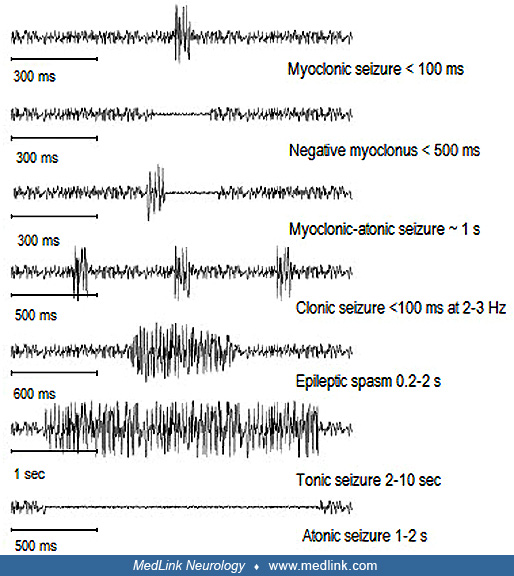
According to the various ILAE classifications and definitions, clonic seizures are mainly distinguished from myoclonic seizures by their rhythmicity. This has created significant overlap in what to call clonic or myoclonic seizures, and these terms are often used interchangeably. Relevant ILAE terminologies are cited in Tables 1 and 2.
The 2022 ILAE report from The Task Force on Nosology and Definitions uses the terms focal clonic and hemiclonic interchangeably (77).
Clonic | Myoclonus that is regularly repetitive and involves the same muscle groups, at a frequency of approximately 2 to 3 c/s, and is prolonged. Synonym: rhythmic myoclonus. |
Focal | A seizure whose initial semiology indicates, or is consistent with, initial activation of only part of one cerebral hemisphere. Synonym: partial. |
Jacksonian march | Traditional term indicating spread of clonic movements through contiguous body parts unilaterally. |
Lateralizing [Todd (or Bravais)] phenomenon | Any unilateral postictal dysfunction relating to motor, language, sensory, and/or integrative functions, including visual, auditory, or somatosensory neglect phenomena. |
Myoclonic (adjective) | Sudden, brief (< 100 ms), involuntary single or multiple contraction(s) of muscles(s) or muscle groups of variable topography (axial, proximal limb, distal) |
| |
Clonic | Jerking, either symmetric or asymmetric, that is regularly repetitive and involves the same muscle groups |
Focal onset | Originating within networks limited to one hemisphere. They may be discretely localized or more widely distributed. Focal seizures may originate in subcortical structures. |
Focal to bilateral tonic-clonic | Replaces the older term “secondarily generalized tonic-clonic” |
Focal aware | Corresponds to the prior term “simple partial seizure” |
Focal impaired awareness | Corresponds to the prior term “complex partial seizure” |
Focal aware or impaired awareness | Optionally may further be characterized by one of the motor-onset or nonmotor-onset symptoms reflecting the first prominent sign or symptom in the seizure. Seizures should be classified by the earliest prominent feature. |
Fencer motor | A focal motor seizure type with extension of one arm and flexion at the contralateral elbow and wrist, giving an imitation of swordplay with a foil; also called a supplementary motor area seizure |
Jacksonian | Traditional term indicating spread of clonic movements through contiguous body parts unilaterally |
Myoclonic | Sudden, brief (< 100 msec) involuntary single or multiple contraction(s) of muscles(s) or muscle groups of variable topography (axial, proximal limb, distal). Myoclonus is less regularly repetitive and less sustained than is clonus. |
| |
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125