

Epilepsy & Seizures
Hippocampal and parahippocampal seizures
Apr. 22, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Typical absence seizures (previously known as petit mal) are brief (few seconds to half a minute) generalized epileptic seizures of abrupt onset and abrupt termination. They have two essential components: (1) clinically, the impairment of consciousness (absence) and (2) EEG generalized 2.5 to 4 Hz (not less than 2.5 Hz) spike-and-slow wave discharges. The impairment of consciousness may be conspicuous or inconspicuous, severe or less severe. Impairment of consciousness is a prerequisite of any definition of absence seizures. Typical absences are clusters of clinico-EEG manifestations that may be syndrome related. Absences may be the only type of seizures occurring in the patient, as in childhood absence epilepsy, or may be part of a phenotype in which other seizures eg, myoclonic, are the predominant type, as in juvenile myoclonic epilepsy. Typical absences are fundamentally different and pharmacologically unique compared to any other type of seizure, which also makes their treatment different. Antiepileptic drugs effective for focal seizures are contraindicated for absence seizures. In this article, the author details developments in the pathophysiology, genetics, and pharmacological treatment of absence seizures and related epileptic syndromes.
|
• Typical absence seizures (previously known as petit mal) are brief (few seconds to half a minute) generalized epileptic seizures of abrupt onset and abrupt termination. | |
|
• The defining manifestations of typical absence seizures are impairment of consciousness, conspicuous or inconspicuous, and generalized 2.5 to 4 Hz spike-wave discharges. | |
|
• Typical absences are fundamentally different and pharmacologically unique compared to any other type of seizures, which also makes their treatment different. | |
|
• The clinico-EEG manifestations of absence seizures are syndrome-related. Childhood and juvenile absence epilepsy are the archetypal syndromes of typical absences. | |
|
• Typical absence seizures are more frequent (pyknolepsy) in childhood absence epilepsy and less frequent (spaniolepsy) in Juvenile absence epilepsy. Briefer or even inconspicuous typical absence seizures are seen in juvenile myoclonic epilepsy concomitant or not with myoclonic jerks. | |
|
• Typical absences, particularly in adults, are frequently misdiagnosed as focal seizures with detrimental effect on patient management. | |
|
• Antiepileptic drugs effective for focal seizures are contraindicated for absence seizures. |
Poupart, in 1705, was the first to describe absences (150). Tissot described a girl with absences “avec un tres leger movement dans les yeux” and frequent generalized tonic-clonic seizures (157). The term “epileptic absence” was first used by Calmeil (22). Shortly thereafter, Esquirol coined “petit mal” (50). Gowers gave a most accurate description of the absence seizures “without conspicuous convulsions” (69). Friedman reported a long-term favorable prognosis but believed that these absences were not epileptic (58). Sauer coined the name “pyknolepsy” (from the Greek word pyknos, meaning closely packed, dense, or aggregated) (139). Adie defined pyknolepsy as follows (02):
|
…a disease with an explosive onset between the ages of 4 and 12 years, of frequent short, very slight, monotonous minor epileptiform seizures of uniform severity, which recur almost daily for weeks, months, or years, are uninfluenced by anti-epileptic remedies, do not impede normal and psychical development, and ultimately cease spontaneously never to return. At most, the eyeballs may roll upwards, the lids may flicker, and the arms may be raised by a feeble tonic spasm. Clonic movements, however slight, obvious vasomotor disturbances, palpitations, and lassitude or confusion after the attacks are equivocal symptoms strongly suggestive of oncoming grave epilepsy, and for the present they should be considered as foreign to the more favorable disease. I shall be well satisfied if I have made it appear probable to you that there does exist a form of epilepsy in children which is distinguishable by its clinical features and in which the prognosis is always good (02). |
Gibbs and colleagues described the clinico-EEG characteristics of absences (61). Lennox in 1945 referred to the petit mal triad as absence, myoclonic, and akinetic seizures, and the introduction of trimethadione revolutionized the treatment of absence seizures (88). The petit mal triad of Lennox, which was misused and misunderstood, was clarified by the Commission of the International League Against Epilepsy with the differentiation of typical from atypical absences (60). Both Penry and colleagues and Stefan and colleagues studied absences with video-EEG (126; 145). Panayiotopoulos and colleagues described syndrome-related characterization of typical absence seizures with video-EEG analysis (123; 121; 122; 119).
A more detailed history of typical absence seizures can be found in a review publication (20).
Typical absences are brief, generalized epileptic seizures of sudden onset and termination. They have two essential components: (1) clinically the impairment of consciousness (absence) and (2) EEG generalized 2.5 to 4 Hz spike-and-slow wave discharges (Commission on Classification and Terminology of the International League Against Epilepsy 1981; 37; 119).
Typical absences are a cluster of clinico-EEG manifestations that occur in idiopathic generalized epilepsies and may be syndrome related.
Impairment of consciousness may be conspicuous (severe or less severe) or inconspicuous (requiring a meticulous video-EEG assessment). Impairment of consciousness is prerequisite of any definition of absence seizures. Typical absence seizures are often associated with other symptoms, such as automatisms, autonomic disturbances, or regional (mouth or eyes) or widespread (head, limbs, and trunk) rhythmic or random myoclonia. The clinical expression of absence seizures is variable among children and during different absence seizures in the same child.
The EEG discharge may be brief or long (lasting 30 seconds or more); it may be continuous or fragmented; and it may be composed of single or multiple spikes, which may or may not be consistent with the slow wave.
The typical absence seizures may remit with age or be part of a phenotype with aberrant electroclinical features and variable evolution, requiring continuous treatment. Thus, the clinico-EEG manifestations of typical absences are, by definition, widespread and often not as classical as in their archetype, childhood absence epilepsy. The prefix “typical” is not to characterize them as “classical,” but to differentiate them from “atypical” absence seizures occurring mainly in symptomatic epilepsies.
Atypical absences differ from typical absences in the following ways (37; 36; 116; 117; 118):
|
• Atypical absences occur only in the context of mainly severe symptomatic or unknown (previously known as cryptogenic) epilepsies of children with learning difficulties, who also suffer from frequent seizures of other types such as atonic, tonic, and myoclonic seizures. | |
|
• In atypical absences, onset and termination is not as abrupt as in typical absences, and changes in tone are more pronounced, slower, and last longer than in typical absence seizures. | |
|
• Ictal EEG of atypical absence is of slow, less than 2.5 Hz, spike-and-slow wave. The discharge is heterogeneous, bilateral, often asymmetrical, and may include irregular spike wave and slow wave complexes and fast or other paroxysmal activity. Background interictal EEG is usually abnormal with widespread slow activity. | |
|
• The final distinguishing characteristic involves the neural circuitry involved in the spike-wave discharge. In typical absence seizures, the epileptiform activity is constrained within thalamocortical circuitry. In contrast, there are experimental, clinical, behavioral, and neuroimaging data for the involvement of both thalamocortical and limbic circuitry in atypical absence seizures. Thus, the progression of ictal events and the mechanisms by which these recruit several brain areas may provide an explanation for the differing characteristics of typical versus atypical absence seizures (160). See atypical absence seizures. |
In brief, typical absence seizures differ from atypical absence seizures in terms of network circuitry involved, clinical manifestations, morphology, frequency of spike-and-wave discharges, and cognitive outcome.
The ILAE classification core group recognized typical, phantom, myoclonic, and atypical absences and defined them as follows (49):
Typical absences. The pyknoleptic manifestations of typical absences in childhood absence epilepsy have been suggested to differ by shorter duration from the longer duration, less-frequent absences of juvenile absence epilepsy. However, based on what we currently know, it seems likely that they do not represent two mechanisms, but merely the evolution of a single mechanism as the brain matures.
Phantom absences. Phantom absences also are likely to be a result of brain maturation. A working group will be convened to study whether absences of childhood and juvenile absence epilepsy represent two seizure types or a spectrum of the same seizure type, and to better define associated motor components.
Myoclonic absences. The myoclonic components of these seizures are rhythmic (2.5 to 4.5 Hz) clonic rather than myoclonic and have a tonic component. The seizure type should be called something else, but there is no agreement on another name at this time.
Atypical absences. There are variable manifestations of this ictal event, some involving hypotonia and atonia. Atypical absences occur mainly in symptomatic or unknown etiology epilepsies and are concomitant with other seizures, such as tonic, atonic, and myoclonic. The onset and termination are less abrupt, and the changes in muscle tone are slower, more intense, and last longer than typical absences.
Absence seizures can rarely represent propagation from localized cortical areas, usually in the frontal lobe. There may be a continuum between these events and generalized atypical absences (49).
According to the 2014 ILAE Commission, absence seizures should be simplified in (A) typical absences, (B) atypical absences, and (C) absence with special features (eg, myoclonic absence, eyelid myoclonia) (12; 33). The latest ILAE position paper of the operational classification of seizure types recognizes typical absences, atypical absences, absences with eyelid myoclonia, and myoclonic absences (55; 56). In this paper, absences are classified as "generalized nonmotor (absence) seizures" though this (nonmotor) does not convey the complex semiology of absence seizures, which often manifest with significant motor manifestations as analyzed in a narrative review (158). The ILAE Commission diagnostic manual of epilepsies describes typical absence seizures as follows (33):
Typical absence seizure. A typical absence seizure is a generalized seizure with abrupt onset and offset of altered awareness, which can vary in severity (see specific syndromes). Memory for events during the seizures is usually impaired, although there may be some retained awareness particularly for adolescents. Clonic movements of eyelids, head, eyebrows, chin, perioral, or other facial parts may occur, most typically at 3 Hz. Myoclonus of limbs can rarely occur. Oral and manual automatisms are common, and there may be perseveration of behaviors occurring prior to seizure onset. Absence seizures were previously known as “petit mal” seizures. Absence status epilepticus can occur.
|
|
Caution. Individual absence seizure longer than 45 seconds or with a post-ictal phase, then consider focal seizure. |
|
|
Caution. Onset of absence seizures less than 4 years, then consider glucose transporter disorders. |
EEG. Background/interictal/activation: Please refer to specific syndromes and etiologies in which this seizure type occurs.
Ictal EEG. Generalized spike-and-wave is mandatory. Regular 3 Hz generalized spike-and-wave occurs with typical absence seizures in childhood absence epilepsy. In absence seizures beginning in adolescence, faster irregular 3.5 to 6 Hz generalized spike-and-wave and polyspike-and-wave occurs.
|
Caution. Slow spike-and-wave (less than 2.5 Hz), then consider atypical absence seizures. |
|
|
• Absence with eyelid myoclonia: repetitive, rhythmic, fast (greater than 4 Hz) jerks of the eyelids, with upward deviation of the eyeballs and with head extension; often very frequent and provoked on eye closure, voluntary or on command, and by photic stimulation. |
|
|
• Myoclonic absence: 3 Hz myoclonic jerks of upper limbs with tonic abduction. |
|
|
• Atypical absence: more prolonged subtle altered awareness often seen in individuals with intellectual disability. |
|
|
• Focal seizures with dyscognitive features. |
|
|
• Daydreaming or inattention or other. |
|
|
• Childhood absence epilepsy |
Transient loss of consciousness without conspicuous convulsions. In 1881 Gowers described transient loss of consciousness without conspicuous convulsions as follows (69):
|
A patient stops for a moment whatever he or she is doing, very often turns pale, may drop whatever is in the hand…There may be a slight stoop forward, or a slight quivering of the eyelids…The attack usually lasts only a few seconds. The return of the consciousness may be sudden and the patient, after the momentary lapse, may be in just the same state as before the attack, may even continue a sentence or action which was commenced before it came on, and suspended during the occurrence. |
The clinical manifestations of typical absence seizures vary significantly among patients (126; 31; 145; 123; 121; 122; 23; 119; 118; 79). Impairment of consciousness may be the only clinical symptom, but this is often combined with other manifestations.
Absence with impairment of consciousness only. The hallmark of the absence attack is a sudden onset and interruption of ongoing activities, often with a blank stare conspicuous or inconspicuous concomitant with brief generalized spike-and-wave discharges.
If the patient is speaking, speech is slowed or interrupted; if walking, he or she stands transfixed. Usually, the patient will be unresponsive when spoken to. The attack lasts from a few seconds to (rarely) half a minute and terminates as rapidly as it commenced.
In less severe absences, the patient may not stop his or her activities, though reaction time and speech may slow down. In their mildest form, absences may be inconspicuous to the patient and imperceptible to the observer, as disclosed on video-EEG recordings with errors and delays during breath-counting or other cognitive testing during hyperventilation. Typical absence seizures that are related to brief generalized spike-and-wave discharges are impossible to identify while the patient is counting or responding to a given world. This is particularly so in early childhood. Only when carefully assessing a video-EEG recording can we identify very brief loss of contacts. These brief typical absence seizures are seen in cases where myoclonic seizures and typical absence seizures coexist in the same phenotype of an idiopathic generalized epilepsy or syndrome.
Absence with clonic components. During the absence as above, clonic motor manifestations, rhythmic or arrhythmic and singular or repetitive, are particularly frequent at the onset. They may also occur at any other stage of the seizure. The most common are clonic jerking of the eyelids, eyebrows, and eyeballs, together or independently, as well as random or repetitive eye closures. Fast eyelid flickering is probably the most common ictal clinical manifestation and may occur during brief generalized discharges without discernible impairment of consciousness. Myoclonias at the corner of the mouth and jerking of the jaw are less common. Myoclonic jerks of the head, body, and limbs may be singular or rhythmical and repetitive, and they may be mild or violent.
Absence with atonic components. Diminution of muscle tone is not unusual and may lead to drooping of the head and, occasionally, slumping of the trunk, dropping of the arms, and relaxation of the grip. Rarely, tone is sufficiently diminished to cause falls.
Absence with tonic components. Tonic muscular contraction may affect the extensor or the flexor muscles symmetrically or asymmetrically. The head may be drawn backwards (retropulsion) or to one side, and the trunk may arch.
Absence with automatisms. Automatisms are common in typical absences when consciousness is sufficiently impaired, and they are more likely to occur 4 to 6 seconds after onset.
Automatisms are more or less coordinated, adapted (eupractic or dyspractic), involuntary movements that may be an unconscious continuation of the preservative automatisms, de novo automatisms, or both. They vary in location and character from seizure to seizure, the same patient having both simple and complex absences. Perioral automatisms such as lip licking, smacking, swallowing, or mute speech movements are the most common. Scratching, fumbling with the clothes, and other limb automatisms are also common. Automatisms can be evoked, and their pattern and distribution can be changed by passive movements, postural repositioning, or other ictal stimulations.
Absence with autonomic components. Autonomic components consist of pallor and, less frequently, flushing, sweating, dilatation of pupils, and incontinence of urine. Mixed forms of absence are the rule rather than the exception.
Visual hallucinations and other focal symptoms. Exceptionally, patients may have visual hallucinations or visual illusions during the absence or absence status. Epigastric sensations may also be an unusual manifestation of adult absence epilepsy (171).
Clinical and EEG correlations. The ictal EEG is characteristic with usually regular and symmetrical generalized discharges of 3 to 4 Hz spike wave and slow wave complexes at a duration of 3 to 30 seconds. The discharge spike-wave frequency varies from onset to termination. It is usually faster and unstable in the opening phase (first second), becomes more regular and stable in the initial phase (first 3 seconds), and slows down towards the terminal phase (last 3 seconds). The intradischarge frequency and the relation of spike or multiple spike wave and slow wave frequently vary.
The background interictal EEG is normal in typical absence seizures of childhood absence epilepsy. Variability in clinical and EEG characteristics are seen in childhood absence epilepsies with aberrant electroclinical features and in those idiopathic generalized epilepsies or syndromes where typical absence seizures are part of the phenotypic expression. Such aberrant electroclinical features are onset under 3 to 4 years or above 10 years, spaniolepsy, marked clonic-myoclonic component, generalized tonic-clonic seizures, inconspicuous absences, brief generalized discharges, focal spikes or slow spike-wave complexes, fragmented generalized discharges, and photosensitivity.
There are reports of a few adult patents with idiopathic typical absence seizures and generalized paroxysmal fast activity in their EEG; these patients are usually pharmaco-resistant with bad prognosis (51; 73; 09; 11).
The prognosis and complications are syndrome related. Childhood absence epilepsy if diagnosed with strict inclusion and exclusion criteria is a relatively benign syndrome of children, which usually remits within 2 to 5 years from onset (119; 118). In all other syndromes, there is probably a lifelong liability to absences, myoclonic jerks, and generalized tonic-clonic seizures. Response to appropriate treatment is often excellent, but 10% to 20% of the patients may not achieve control of seizures.
For clinical vignettes of classical typical absence seizures, see childhood absence epilepsy and juvenile absence epilepsy.
Typical absences are generalized epileptic seizures with generalized spike or multiple spike-wave and slow-wave discharges. This is often of higher amplitude in the anterior regions. A generalized discharge with onset or a higher amplitude in the posterior regions may indicate a bad prognosis (118).
The pathophysiological mechanisms of absence seizures have been studied in humans and in various animal models with generalized spike-and-wave discharges associated with behavioral arrest (40; 59; 141; 38; 92; 15; 16; 17; 160; 76; 06; 79; 167; 91; 108; 72; 161; 42). It appears that the generalized spike-and-wave discharges are generated and sustained by highly synchronized abnormal oscillatory rhythms in thalamocortical networks that mainly involve the neocortical pyramidal cells, the reticular nucleus, and the relay nuclei of the thalamus. Neither the cortex nor the thalamus alone can sustain these discharges, indicating that both structures are involved in their generation. Avoli reviewed the findings obtained over the past 70 years on the fundamental mechanisms underlying generalized spike-wave discharges associated with absence seizures (08). Studies in genetic animal models have demonstrated that spike-and-wave discharges are initiated in the primary somatosensory cortex and then rapidly propagate to motor cortices and thalamic nuclei. More specifically, deep layer pyramidal neurons of the somatosensory cortex are ictogenic neurons in absence seizures (42).
Further, it has been hypothesized that the mechanisms underlying focal epilepsy are distinctively diverse from those responsible for generalized epilepsies. Studying the dissimilarities between focal and generalized epilepsies in experimental animal models representative of the human condition has enabled the exploration of the underlying mechanisms of these disorders (110). The experimental approach to the rare coexistence of limbic focal epilepsy and absence epilepsy, as representative of genetic generalized epilepsies, points to the mutual cross-interaction of the circuits involved in typical absence seizures and limbic epilepsy in which seizures start from the mesial temporal lobe.
Studies in humans have demonstrated that absence seizures start in the frontal lobe and then spread to other brain areas (10), and most authors agree that the spike-wave discharges originate from reciprocal connections between neurons in the cortex and thalamus. Researchers have noted that there are complicated genetic mechanisms behind absence epilepsies, especially mutations in genes that code for GABA receptors, calcium channels, and ion channel proteins. These mutations impart an altered effect on the thalamocortical neuronal pathways. Simultaneous EEG and functional magnetic resonance imaging measurements document cortical deactivation and thalamic activation. Cortical deactivation is related to slow waves and disturbances of consciousness of varying degrees (97). Motor symptoms correspond to the spike component of the 3/s spike-and-wave-discharges, and thalamic activation can be interpreted as a response to overcome cortical deactivation (158). The cortico-thalamic-cortical circuit is thought to play a major role in the pathophysiology of absence seizures (111).
The involvement of thalamus as the generator of the generalized spike-and-wave discharges is documented by the following: (1) stimulation of the medial thalamus induces a cortical generalized spike-and-wave discharge without leading to self-sustained activity and (2) thalamic neurons can intrinsically generate action potentials in both a tonic and a burst-firing mode. In a study of MRI diffusion and volumetry abnormalities in subcortical nuclei, 11 patients with absence seizures and 11 controls, patients had increased mean diffusivity values bilaterally in thalamus, putamen, and left caudate nucleus; increased fractional anisotropy value in bilateral caudate nuclei; and loss of volume in bilateral thalamus, putamen, and pallidum (90). These findings of microstructural changes provide further evidence for the involvement of thalamus and basal ganglia in propagation and modulation of spike-wave discharges in absence seizures.
The relative importance of the cortex in the initiation and synchronization of the generalized spike-and-wave discharges is mainly documented by the finding that following thalamectomy, instigation of generalized spike-and-wave discharges persists even though the thalamus is required to maintain rhythmicity once the discharges are established. Additional reports from animal models indicate that absence seizures arise from the somatosensory cortex, thus, providing support of a "focal hypothesis" of absence epilepsy (99; 130). During the first cycles of the seizure, the cortex drives the thalamus; thereafter, the cortex and thalamus drive each other, thus, amplifying and maintaining the rhythmic discharge. In this way, the "cortical focus" theory for generalized absence epilepsy bridges cortical and thalamic theories (100). Aarabi and colleagues applied linear and nonlinear synchronization measures to characterize the synchrony between cortical regions and detect cerebral epileptic states in scalp EEG recordings recorded prior to and during typical absence seizures (01). An overall rapid increase in the synchronization level between different cerebral regions was observed during the ictal state. During the interictal state, the degree of interdependence between EEG channels was significantly less than that observed in the ictal state (p< 0.05). In 63% of the 35 seizures analyzed, a preictal state was identified by a significant decrease in the synchronization level with respect to the interictal state. However, in 31% of the seizures, the synchronization level in the preictal state was higher than that in the interictal state. In the remaining 6% of the seizures, no significant changes were found in the synchronization values in the interictal state prior to the seizure onset. In all the seizures analyzed, the interchannel synchrony persisted in the postictal state, with synchronization level significantly higher than that observed in the interictal state. The authors concluded that their findings support the hypothesis of having a focal susceptibility of the cerebral cortex prior to absence seizures and further underlie that this susceptibility is reproducible and patient specific.
In a study, Gupta and colleagues studied with magnetoencephalography the space-time network connectivity and cortical activations preceding spike-wave discharges in five patients with absence seizures (71). They found an increase in clustering and a decrease in path length preceding the onset of spike-wave discharges and a rhythmic pattern of increasing and decreasing connectivity during the discharges. Beamforming showed a consistent appearance of a low frequency frontal cortical source prior to the first generalized spikes. This source was preceded by a low frequency occipital source. The authors concluded that the changes in the connectivity networks with the onset of spike-wave discharges suggest a pathologically predisposed state towards synchronous seizure networks with increasing connectivity from interictal to preictal and ictal state, whereas the occipital and frontal low frequency early preictal sources demonstrate that the spike-wave discharges are not suddenly arising but gradually build up in a dynamic network (71).
Tenney and associates used magnetoencephalography to determine cortical and subcortical contributions to the formation of spike and wave discharges in 12 newly diagnosed, drug-naive children during 44 generalized absence seizures (151). Beamformer analysis using synthetic aperture magnetometry (SAM) was used to confirm the presence of independent thalamic activity, and standardized low resolution brain electromagnetic topography (sLORETA) was used to compute statistical maps indicating source locations during absence seizures. Sources detected in the 50 ms prior to the start of the seizure were more likely to be localized to the frontal cortex or thalamus. At the time of the first spike on EEG, focal source localization was seen in the lateral frontal cortex with decreased thalamic localization. Following the spike, localization became more widespread throughout the cortex. Comparison of the earliest spike and wave discharge (SWD) (ictal onset) and a SWD occurring 3 seconds into the seizure (mid-ictal) revealed significant differences during the slow wave portion of the SWDs. The authors concluded that their findings provide additional evidence that there are focal brain areas responsible for these seizures, which appear bilaterally symmetric and generalized with a conventional 10 to 20 placement scalp EEG.
In a study of 16 children with childhood absence epilepsy who were not on treatment, a total of 242 EEG epochs were used for distributed source localization with sLORETA software. The maximum current source density was mostly located in the frontal lobe (86 discharges, 71.1%), suggesting that the frontal lobe is involved in generating childhood absence epilepsy (83).
In another report, Jacobs-Brichford and colleagues studied with magnetoencephalography 44 absence seizures recorded from 12 children with drug-naive childhood absence seizures; time frequency analysis and source localization were performed prior to the onset of the seizures. Evidence of preictal magnetoencephalography frequency changes were detected a mean of 694 ms before the initial spike on the EEG. A consistent pattern of focal sources was present in the frontal cortex and thalamus during this preictal period, but source localization occurred synchronously so that independent activity between the two structures could not be distinguished (82).
Studies of absence seizures using EEG with fMRI (EEG-fMRI) show a consistent network with prominent thalamic activation and a variety of cortical changes of deactivation (101). Thalamic activation can be interpreted as a response to overcome cortical deactivation. Carney and colleagues studied 13 subjects with absence seizures during EEG-fMRI (26). Based on visual inspection of surface-rendered activation maps, they identified two subgroups that could be distinguished by the activation in the dorsolateral prefrontal cortex (DLPFC). One group of patients (n = 7) showed a primarily positive signal change (DLPFC-POS), whereas the other group (n = 6) showed a primarily negative signal change (DLFPC-NEG). When the DLPFC-POS group was compared to the DLPFC-NEG group, time-course analysis revealed a larger positive blood oxygenation level-dependent deflection following onset of the absence seizures in cortical and subcortical areas beyond the DLPFC. Masterton and associates examined absence epilepsy subnetworks revealed by event-related independent components analysis of fMRI (94). EEG-fMRI recordings from eight patients with childhood absence epilepsy were studied using event-related independent components analysis (eICA). Six eICA components were identified, representing distinct generalized spike-wave-related subnetworks. Activations were detected in a number of brain regions, including the striatum. These findings suggest that the earliest activity associated with generalized spike-wave may be in posterior cortical regions and provide new evidence that the thalamostriate network may play a more important role in the generation of generalized spike-wave than suggested by previous studies (94). Liao and associates studied the dynamical intrinsic functional architecture of the brain during absence seizures in order to understand the network mechanisms of seizure initiation, maintenance, and termination in absence epilepsy (89). They used simultaneous EEG to define the preictal, ictal, and postictal intervals of seizures. They measured dynamic connectivity maps of the thalamus network and the default mode network, as well as functional connectome topologies, during the three different seizure intervals. The analysis of dynamic changes of anticorrelation between the thalamus and the default mode network is consistent with an inhibitory effect of seizures on the default mode of brain function, which gradually fades out after seizure onset. Also, the authors observed complex transitions of functional network topology, implicating adaptive reconfiguration of functional brain networks (89).
Both inhibitory and excitatory neurotransmissions are involved in the genesis and control of absence seizures. This may be the result of an excessive cortical excitability due to an imbalance between inhibition and excitation or of excessive thalamic oscillations due to abnormal intrinsic neuronal properties under the control of inhibitory GABAergic mechanisms. It is likely that the generation of absences is due to a predominance of inhibitory activity, in contrast to generalized or focal convulsive seizures where an excess of excitatory activity is present (92).
Some of the neurons involved in the cortico-thalamic-cortical system include cortical glutamatergic neurons originating on cortical layer VI and projecting to the nucleus reticularis of the thalamus; thalamic relay neurons that have excitatory projections to cortical pyramidal neurons; and neurons from the thalamic nucleus reticularis containing inhibitory GABA-ergic projections that connect with other neurons from the same nucleus and with thalamic relay neurons. These neurons do not connect directly with the cortex (124). Neurons from the thalamic nucleus reticularis can fire in an oscillatory pattern (for example, rhythmic bursts involved in the generation of sleep spindles) or continuously in single spikes (tonic firing during wakefulness). Shifts between these two firing patterns in the thalamic nucleus reticularis are modulated by spikes present in thalamocortical networks and neurons from the thalamic nucleus reticularis. These are mediated through low-threshold, transient calcium channels known as T-type channels. After depolarization, T-type channels briefly allow calcium inflow before becoming inactivated. Reactivation requires a relatively long hyperpolarization facilitated by GABA-B receptors. Therefore, abnormal oscillatory rhythms can originate from T-type channel abnormalities, or from the increased GABA-B activity (124).
The basic intrinsic neuronal mechanisms involve low-threshold (T-type) calcium current elicited by activating the low-threshold calcium channels (29). These channels are present in high densities in thalamic neurons and trigger regenerative burst firing that drive normal and pathologic thalamocortical rhythms, including the spike-wave discharges of absence seizures. Ethosuximide exerts its anti-absence effect either by reducing thalamic low-threshold calcium currents probably through a direct channel-blocking action that is voltage dependent (35) or through a potent inhibitory effect in the perioral region of the primary somatosensory cortex (92).
Of neurotransmitters, GABA-B receptors play the most prominent role by eliciting long-standing hyperpolarization required to drive low threshold calcium channels for the initiation of sustained burst firing. GABA-B agonists, such as baclofen aggravate, and GABA-B antagonists suppress typical absences. GABAergic drugs (such as vigabatrin and tiagabine) are pro-absence substances; they interfere with the degradation of, and the re-uptake of, GABA (92; 118). The only exception of GABAergic activation inhibiting absences is that of the reticular thalamic nucleus, with exclusively GABA-A receptors; it functions as a pacemaker to synchronize thalamocortical oscillations (62; 78). Enhanced activation of GABA-A receptors in this nucleus decreases the pacemaking capacity of these cells, therefore, decreasing the likelihood of generating absence seizures.
Functional imaging with positron emission tomography demonstrates normal cerebral glucose metabolism and benzodiazepine receptor density in absence epilepsies with diffuse hypermetabolism during 3 Hz spike-and-wave discharges (136; 46). There is no evidence of any interictal overall abnormality of opioid receptors in idiopathic generalized epilepsy, but typical absences have been found to displace 11C-diprenorphine from the association areas of the neocortex. In contrast, binding of 11C-flumazenil to central benzodiazepine receptors has been shown to be unaffected by serial absences (46).
Ictal single photon emission computed tomography shows an overall increase in the cerebral blood flow (176) and may be useful in detecting secondarily generalized cases (81).
During absence seizures, there are pronounced changes in cerebral Hb-oxygenation (21). These start several seconds after the EEG-defined absence onset and outlast the clinically defined event by 20 s and 30 s. The changes consist of decrease in [oxy-Hb] and an increase in [deoxy-Hb] during absence seizures indicating a reduction of cortical activity.
In a magnetoencephalographic study of children with absence seizures, Westmijse and associates demonstrated that 3 to 4 Hz generalized spike-and-wave discharges have a local cortical onset of mainly the frontal and parietal regions (170).
A significant reduction in the amplitude of P300 on the visual and auditory continuous performance test was reported in patients with absence seizures (45). According to the authors, this indicates the impaired capacity of absence patients to mobilize and sustain attentional resources.
Microdysgenesis and other cerebral structural changes were reported in some patients with childhood absence epilepsy and juvenile absence epilepsy from autopsy (98) and MRI (173) studies. These results were not replicated in a blinded study (113). Microdysgenesis may be inconceivable for a benign, age-dependent, and age-limited epileptic syndrome such as childhood absence epilepsy, though the current ion channel hypothesis for the pathogenesis of idiopathic generalized epilepsy does not preclude microscopic or ultramicroscopic abnormalities.
Idiopathic generalized epilepsies with typical absences are genetically determined, as indicated by the high incidence of similar disorders among families. However, the precise mode of inheritance and the genes involved remain largely unidentified (38; 155).
Currently, various chromosomal loci have been identified for idiopathic generalized epilepsies with absences.
Available evidence suggests that mutations in genes encoding GABA receptors (54; 93) or brain expressed voltage-dependent calcium channels (28) may underlie childhood absence epilepsy.
Feucht and colleagues found a significant association between a polymorphism in GABRB 3 in chromosome 15q11 and in 50 families with childhood absence epilepsy (54). Marini and colleagues (93) found GABA-A receptor gamma2 subunit (GABRG2) gene mutations on chromosome 5 in a large family with childhood absence epilepsy and febrile seizures (including febrile seizures plus and other seizure phenotypes). This gene mutation segregated with febrile seizures and childhood absence epilepsy and also occurred in individuals with the other phenotypes. The clinical and molecular data suggested that the GABA-A receptor subunit mutation alone could account for the febrile seizure phenotype but that an interaction of this gene with another gene or genes was required for the childhood absence phenotype in this family. Linkage analysis for a putative second gene contributing to the childhood absence phenotype suggested possible loci on chromosome 10, chromosome 13, chromosome 14, and chromosome 15 (93). Chen and colleagues found 68 variations, including 12 missense mutations in the calcium channel CACNA1H gene in patients with childhood absence epilepsy (28). The identified missense mutations occurred in the highly conserved residues of the T-type calcium channel gene. However, another study of 33 nuclear families, each with two or more individuals with childhood absence epilepsy, provided conclusive evidence that genes encoding GABA-A and GABA-B receptors, voltage-dependent calcium channels, and the ECA1 region on chromosome 8q do not account independently for the childhood absence trait in a majority of the families (132).
Of significant interest are reports documenting absence seizures mainly of early onset as a key feature of familial glucose transporter 1 (GLUT1) deficiency; these are discussed in detail in the Differential diagnosis section. GLUT1 facilitates the transport of glucose across the blood-brain barrier.
Studies in genetic animal models, especially rats with spike-and-wave discharges have demonstrated that spike-and-wave discharges are initiated in the primary somatosensory cortex and then rapidly propagate to motor cortices and thalamic nuclei. More specifically, in vivo electrophysiological intracellular recordings showed that the pyramidal neurons of the deep layers of this cortex exhibit fast activation, hyperexcitability, and hypersynchronizing characteristics in favor of their role as ictogenic neurons in absence seizures (42).
Genetic heterogeneity of the spike-wave phenotype in animal models of absences favors a similar, and probably much wider, genetic heterogeneity in humans (141; 38; 92).
Despite much progress in our understanding of the neuropathological mechanisms, researchers still do not have a clear picture of the “widespread synchrony accounting for absence seizures” (80). Furthermore, following the traditional, strict dichotomy of “generalized” versus “focal,” generalized absence seizures may be counterproductive to the development of new ideas and treatment. In a 2022 publication, childhood absence seizures were discussed with respect to changing scientific concepts and newer findings (146). The data from semiology and structural and functional studies using quantitative electroencephalography, video-EEG monitoring, magnetoencephalography, magnetic resonance imaging, and positron emission tomography, as well as neuropathology, suggest a nosological spectrum from focal to generalized seizure-generating mechanisms. In fact, functional findings indicate that the frontal lobe, with its projections to other brain areas, may play an important role in generalized absence seizures and suggest new research approaches for diagnosis and treatment. Therefore, the distinction between generalized and focal epilepsy is, at times, imperfect. Frontal-onset absences constitute a specific subtype of childhood absence epilepsy, and the cortical initiating network is the major player in generating absence seizures (146).
Furthermore, typical absence seizures can be present with other seizure types and are commonly associated with being difficult to treat. Understanding better the underlying mechanisms of how absence seizures are generated and maintained may help to improve treatment outcomes. One study provides fMRI-informed magnetoencephalography multilayer network analyses showing beta/gamma cross-frequency and within-frequency coupling in the frontoparietal and frontofrontal regions during childhood absence seizures (153). These results provide a possible mechanistic explanation for previous fMRI and neurophysiology studies showing that focal areas of the precuneus and frontal lobe are critically important for the initiation and maintenance of generalized rhythmic spike-wave discharges characterizing absence seizures. In another study, the simultaneous changes in electrical (neuronal) and optical dynamics (hemodynamic, with changes in (Hb) and cerebral blood flow) of eight pediatric patients experiencing 25 typical childhood absence seizures during the transition from the interictal state to the absence seizure by simultaneously performing EEG, functional near-infrared spectroscopy (fNIRS), and diffuse correlation spectroscopy (DCS) approach were studied (107). About 20 seconds before the onset of the spike-and-wave discharge, they observed a transient direct current potential shift that correlated with alterations in fNIRS and DCS measurements of the cerebral hemodynamics detecting the preictal changes. Whether such information may ultimately be relevant for diagnostic and therapeutic approaches requires future confirmation.
Typical absences are more common in children than in adults and have a female prevalence. The female-to-male ratio was reported as 1.3:1 for the age group 4 to 8 years, 2:1 for children under the age of 4 years, and 1:1 for those older than 8 years of age (37; 36). The annual incidence rate of childhood absence epilepsy in children younger than 15 years of age has been estimated between 6.3 and 8.0 out of 100,000. Recruitment bias explains that the frequency of childhood absence epilepsy in childhood epilepsies has been differently assessed, ranging from 2.3% to 37.7% of cases. In two prospective community-based studies, prevalence of childhood absence epilepsy was 10% and 12.3% for children younger than 16 years of age with epilepsy. For references, see childhood absence epilepsy.
Myoclonic absence seizures are very rare, probably accounting for 1% to 2% of absences in children. Though more common in children, typical absences also occur in approximately 10% of adults with epilepsies often combined with other types of generalized seizure (121). Exact prevalence of juvenile absence epilepsy is uncertain because of variable criteria. In adults older than 20 years, its prevalence may be around 2% to 3% of all epilepsies and around 8% to 10% of idiopathic generalized epilepsies. For references, see juvenile absence epilepsy.
Absence status epilepticus may occur in 5% to 16% of cases, with typical absence seizures starting before the age of 10 years (44). Absence status occurs in patients who have idiopathic generalized epilepsy with typical absences, and consists of generalized, nonconvulsive seizures characterized by impairment of awareness. Other intermittent manifestations include automatisms or subtle myoclonic, tonic, atonic, or autonomic phenomena. Persistent confusion or stupor are associated with characteristic 1- to 4-Hz spike-and-wave or polyspike-and-wave discharges on EEG, usually without other typical clinical manifestations of absence seizures. Absence status is rare among children in population-based studies (0% to 3%) (41). An absence seizure becomes absence status when it lasts longer than 10 to 15 minutes (time point t1). The time point t2 that may cause long-term consequences has not as yet been defined (154).
The prevalence of typical absence status appears to be syndrome related, ranging from as high as 57.1% in perioral myoclonia and absences and 46.2% in “phantom” absences with generalized tonic-clonic seizure to as low as 6.7% in juvenile myoclonic epilepsy (03).
The best way to prevent absence seizures is to appropriately diagnose and treat early.
The diagnosis of typical absence seizures with conspicuous, profound impairment of consciousness in childhood is relatively straightforward. Their brief duration with abrupt onset and termination, the high frequency (as a rule), and nearly invariable provocation with hyperventilation makes them one of the easiest types of seizures to diagnose. Automatisms, such as lip smacking or licking, swallowing, fumbling, or aimless walking are common, and these should not be taken as evidence of focal impaired awareness seizures. In focal seizures, the semiology of automatisms is variable, depending on the area of the cerebral cortex in which the seizures originate, and their treatment is entirely different. The detailed sleep-awake EEG, particularly video-EEG will confirm the correlation of clinical events, unprovoked or provoked, with generalized spike-and-slow wave discharges. This may reveal features favoring a specific epileptic syndrome and, therefore, may determine long-term prognosis and management.
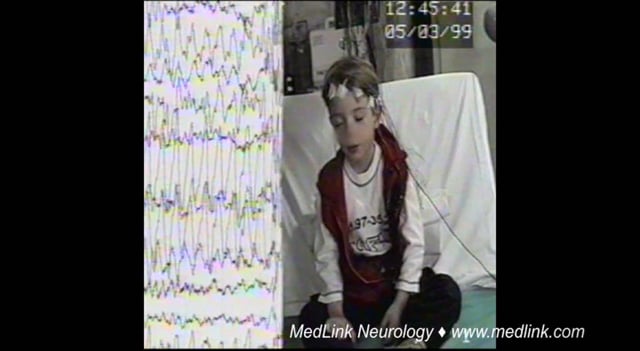
In practical terms, a child suspected of typical absences should be asked to overbreathe for 3 minutes, counting his or her breaths while standing with hands extended in front. Hyperventilation will provoke an absence in more than 90% of those who suffer. This procedure should preferably be videotaped for documentation of the clinical features. In infancy and childhood, hyperventilation is encouraged by blowing either a paper, a paper streamer, or a straw inside a cup with fluid causing bubbles (36). In addition, in children under the age of 3 or 4 years, the presenting symptom may be myoclonic jerks or a generalized tonic-clonic seizure or, rarely, the very brief inconspicuous absence seizures. This type of typical absence seizures will be discovered by careful observation of facial expression during the brief generalized spike-wave discharges. Rarely in this age group, absence seizures are the only seizure type, either pyknoleptic or spanioleptic, reminiscent of childhood or juvenile absence epilepsy, respectively.
Absences may be the only seizure type for a patient, particularly in childhood absence epilepsy. However, in other syndromes, such as juvenile absence epilepsy, typical absences may be the predominant type amongst other coexistent seizures (eg, myoclonic jerks and generalized tonic-clonic seizures). They may be mild and nonpredominant with myoclonic jerks and generalized tonic-clonic seizures as the main seizure type, as in juvenile myoclonic epilepsy. Typical absence status epilepticus may occur in approximately one third of patients.
The video-EEG documentation may be particularly useful if absences prove resistant to treatment, if other seizures develop, or for future genetic counsel. Focal spike abnormalities and asymmetrical onset of the ictal 2.5 to 4 Hz spike-wave discharges are common and may be a cause of misdiagnosis, particularly in resistant cases.
The incidence of absence seizures is between 0.7 and 4.6 per 100,000 in the general population and around 6 to 8 per 100,000 in the pediatric population younger than 15 years (109; 138). Contrary to the dominant view, typical absence seizures occur in approximately 10% of adults with epilepsies and are often combined with other types of generalized seizures (121).
Many physicians are unfamiliar with the syndromic classification of absence epilepsies. Eyelid myoclonia and absences is the most straightforward diagnosis because it is betrayed by the characteristic, easily recognizable eyelid myoclonia on voluntary or on-command eye closure in the light and commonly inconspicuous absences. Equally simple to diagnose is the syndrome of myoclonic absence epilepsy with characteristically rhythmic myoclonic jerks, mainly of the upper extremities. Eyelid myoclonia with absences (previously known as Jeavons syndrome) has been recognized as a distinct genetic generalized epilepsy syndrome by the ILAE (144).
Facial myoclonia (perioral and or eyebrow jerking) with absences is often erroneously diagnosed as motor focal epilepsy in adults and as childhood absence epilepsy in children. In children, facial myoclonia and absences represents 1% of childhood absence seizures. Clinically, absence seizures are combined with perioral, eyebrow, or perioral and eyebrow jerks, concomitant with generalized spike-and-wave discharges. Based on 22 cases of facial myoclonia and absences, in 45.5% absence seizures were combined with perioral jerks, 40.9% with eyebrow, and 13.6% perioral and eyebrow rhythmic jerks. The concomitant generalized spike-and-wave discharges 2 to 4.5 Hz lasted 0.25 to 20 seconds. The mean age of onset was 4.38±2.05 (1 to 8.2) years, and the male:female ratio was 2:1. Family history was positive for epilepsy in 23%, and 13.6% had a positive history of febrile seizures. All cases were assessed with sleep-awake video-EEG following sleep deprivation. The response to valproate was complete in 17 cases (77.3%) and in another three (13.6%) when ethosuximide was added. The other two cases were not followed-up. After a mean duration of treatment (3.97±1.47 [2.5-5.8] years) in eight cases, treatment was withdrawn and four relapsed.
Juvenile myoclonic epilepsy should not be difficult to diagnose if fully developed by the mid-teens. Myoclonic jerks on awakening are the hallmark of this syndrome. However, one third of the patients also have absences that are often simple (with no automatisms or localized limb jerks). Impairment of consciousness is usually mild, and the EEG discharges are often fragmented and brief and have multiple spikes. In adolescents, it may be difficult to differentiate juvenile absence epilepsy from juvenile myoclonic epilepsy. However, in juvenile absence epilepsy, absences are more frequent and there is severe impairment of consciousness, whereas in juvenile myoclonic epilepsy, absences are often so mild that they are not easily discernible.
Childhood and juvenile absence epilepsy are the most pure syndromes of typical absence seizures, pyknoleptic and spanioleptic, respectively. In childhood absence epilepsy, absences are the primary, the most disturbing, and the most characteristic seizure type. Childhood absence epilepsy is manifested only with age-related typical absences. There are no myoclonic jerks, generalized tonic-clonic seizures, or photosensitivity. The impairment of consciousness is more conspicuous than in any other syndrome, and the EEG discharge is harmonious with no polyspikes or fragmentations.
Juvenile absence epilepsy is the only syndrome wherein the ictal manifestations of absence seizures show similar clinical and EEG similarities to those of childhood absence epilepsy. However, in juvenile absence epilepsy they are milder and less frequent. Furthermore, juvenile absence epilepsy often manifests with infrequent generalized tonic-clonic seizures and sporadic, infrequent myoclonic jerks.
Absence seizures of early onset (a few months to 4 years) are particularly demanding in their diagnosis and management (36; 75; 118). There are two main categories in this age group: the nonmyoclonic and the myoclonic. In the nonmyoclonic group, there are cases with spanioleptic and pyknoleptic absence seizures. The spanioleptic are reminiscent of juvenile absence epilepsy, whereas the pyknoleptic are either childhood absence epilepsy-like or an early expression of juvenile myoclonic epilepsy with or without positive response to intermittent photic stimulation (36). These are not a specific expression of a distinct syndrome. The only syndrome recognized easier in this age group is eyelid myoclonia and absences evoked with voluntary or on-command eye closure (36). Absence seizures of early onset may also herald more severe forms of idiopathic and symptomatic generalized epilepsies (24; 63; 165; 04; 64). In the myoclonic group, jerks may be the only seizure type or jerks may combine with typical absences or generalized tonic-clonic seizures or even with absence seizures and generalized tonic-clonic seizures. Conspicuous or inconspicuous absences may precede or follow a brief jerk.
Of clinical importance is the diagnosis of absence seizures associated with glucose transporter-1 (GLUT1) deficiency syndrome (134; 148; 87; 102; 133; 63; 68; 164; 114) that responds to ketogenic diet (84). GLUT1 deficiency syndrome (OMIM 606777) is an autosomal dominant disorder due to SLC2A1 gene mutations that results in abnormal transport of glucose into the brain. GLUT1 deficiency syndrome has been associated with a variety of clinical phenotypes and severity (87; 104). GLUT1 deficiency syndrome is characterized by seizures mainly of early onset and refractory to antiepileptic drugs; deceleration of head growth; delays in mental and motor development; spasticity; ataxia; dystonia; dysarthria; opsoclonus; paroxysmal, exercise-induced dyskinesia; and other paroxysmal neurologic manifestations, often worse prior to meals. Affected infants appear normal at birth. Apneic episodes and abnormal episodic eye movements simulating opsoclonus may precede the onset of seizures by several months. Seizures begin between the ages of 1 and 4 months in 90% of cases. The frequency and severity of seizures varies among affected individuals. Typical or atypical absences, mainly of early onset, are the most prominent seizure types. Typical absences may imitate various syndromes of idiopathic generalized epilepsy with absences, such as epilepsy with myoclonic absences or childhood or juvenile absence epilepsy. Ketogenic diet is highly effective in controlling the seizures. An early diagnosis and early start of a ketogenic diet may prevent deterioration. Phenobarbital is contraindicated.
Clinical diagnostic clues for GLUT1 deficiency syndrome include early onset drug-resistant epilepsy, delayed development, cognitive impairment, movement disorders such as dystonia or ataxia, and family history. Symptoms and EEG abnormalities often worsen during the fasted state and improve after eating. Cerebral imaging is normal. In GLUT1 deficiency there is (1) reduced CSF glucose concentration (hypoglycorrhachia) that seldomly exceeds 40 mg/dL; (2) low ratio of CSF glucose concentration to blood glucose concentration (approximately 0.33±0.01; normal ratio: 0.65±0.01); and (3) normal blood glucose concentration. Molecular genetic testing for SLC2A, which is the only gene known to be associated with GLUT1 deficiency is now clinically available. Families with members manifesting various types of idiopathic generalized epilepsy with absences (early onset absence seizures, childhood or juvenile absence epilepsy, juvenile myoclonic epilepsy) should be tested for SLC2A1 gene mutations (147). However, in a study of 84 children with rigorous diagnosis of early onset absence seizures, no mutations in the SLC2A1 gene were detected (05). Similarly, SLC2A1 gene analysis in 12 children with onset of absences in the first year of life failed to reveal GLUT1 deficiency (64).
Symptomatic absences mainly originating from frontal lobe pathology are detailed in the next section of the diagnostic workup. Refer also to MedLink Neurology article Focal onset generalized absence seizures.
Typical absence seizures of idiopathic generalized epilepsies are also easy to differentiate from atypical absences that occur only in the context of mainly severe symptomatic or cryptogenic epilepsies in children with learning difficulties who also suffer from frequent seizures of other types, such as atonic, tonic, and myoclonic seizures. These seizure types are discussed in the Terminology and clarifications section.
Although the differential diagnosis of typical absence seizures should be straightforward, they are frequently misdiagnosed as focal impaired awareness seizures, especially in adults (Table 1) (121; 118). A typical absence seizure can be reproduced by the hyperventilation test, whereas a focal impaired awareness seizure cannot. Further, typical absence seizures occur daily, are shorter than 30 seconds, are frequently associated with bilateral facial myoclonic jerks or eyelid fluttering, are of sudden onset and termination, are not associated with complex behavioral automatisms or complex hallucinations or illusions, and there are no postictal manifestations.
In general, a detailed clinical history will differentiate between absence seizures and nonepileptic staring spells in the majority of cases. Such paroxysmal nonepileptic events are observed in children with attention disturbance, vacant looks related to masturbation (self-gratification), Munchausen by proxy-reported apneas, and nonepileptic absence episodes related to Rett syndrome. During routine examination, typical absence seizures can be provoked by hyperventilation in almost 90% of the cases. The abrupt onset and termination of typical absence seizures and the provocation by hyperventilation makes the diagnosis easy, particularly when capturing an episode during a video-EEG recording.
|
Typical absences |
Focal impaired awareness | |
|
Clinical criteria |
|
|
|
Duration for less than 30 seconds* |
As a rule |
Exceptional |
|
Daily in frequency |
As a rule |
Rare |
|
Reproduced by hyperventilation |
As a rule |
Exceptional |
|
EEG criteria | ||
|
Ictal generalized 3 to 4 Hz spike-and-wave |
Exclusive |
Never |
|
Normal EEG in untreated state |
Exceptional |
Frequent |
|
|
An epileptic syndrome, by definition, requires the nonfortuitous clustering of many symptoms and signs. The Commission has recognized four epileptic syndromes with typical absences: (1) childhood absence epilepsy, (2) juvenile absence epilepsy, (3) juvenile myoclonic epilepsy, and (4) myoclonic absence epilepsy (32) and similar is the view of the ILAE reports (48; 12; 33). There may be more epileptic syndromes with typical absences, such as eyelid myoclonia and absences (previously known as Jeavons syndrome), facial (perioral or eyebrow) myoclonia and absences, stimulus-sensitive absence epilepsies, idiopathic generalized epilepsy with phantom absences, and others awaiting further studies and confirmation. The absence syndromes in childhood and adolescence comprise several groups and subgroups of syndromes with or without photosensitivity. A practical classification of epilepsy syndromes where typical absence seizures are the prominent type of seizure, or part of the phenotype, is provided elsewhere (36).
Childhood absence epilepsy. Previously known as pyknolepsy, childhood absence epilepsy is the archetypal syndrome of typical absence seizures (74; 118; 96). This is an idiopathic (genetic) generalized epilepsy with frequent (tens or hundreds per day) typical absence seizures, characterized by an abrupt onset and termination of a brief (4 to 30 seconds but usually around 10 seconds), complete or partial loss of consciousness that occur in otherwise normal children. The associated EEG 3 Hz generalized spike-and-wave discharge (range 2.5 to 4Hz) is bilateral, symmetrical, synchronous, and usually most prominent in frontocentral regions (36). Typical age of onset is before 10 years, with a peak at 5 years of age. Remission occurs in more than 90% of the children before the age of 12 years. Clinically, there is abrupt and severe impairment of consciousness. The eyes spontaneously open, and overbreathing, speech, and other voluntary activity stop within the first 3 seconds of the discharge. Automatisms are frequent. The eyes stare or move slowly; random eyelid blinking (usually not sustained) may occur. The background EEG is normal.
Exclusion criteria for childhood absence epilepsy. The following five seizure activities may be incompatible with childhood absence epilepsy:
(1) Other than typical absence, generalized seizures such as generalized tonic-clonic seizures, or myoclonic jerks prior to or during the active stage of absences.
(2) Eyelid myoclonia, facial (perioral or eyebrow) myoclonus, rhythmic massive limb jerking, and single or arrhythmic myoclonic jerks of the head, trunk, or limbs.
(3) No impairment of consciousness during the 3 to 4 Hz discharges.
(4) Brief EEG discharges of less than 4 seconds.
(5) Visual (photic) and other sensory precipitation.
In a study of 124 children with typical absence epilepsy, 12% with onset of symptoms before the age of 4 years, 51% with onset between 4 and 8 years of age, and 37% older than 8 years, the following factors predicted unfavorable outcome: (A) poor initial response to treatment or polytherapy, (B) lateralized single spikes or spike-and-slow wave complexes or marked photosensitivity, (C) absence seizures with marked clonic component, followed or not by generalized tonic-clonic seizures and evolution to myoclonic epilepsy, and (D) early withdrawal of treatment (37). In a multicenter, retrospective study of patients with typical absence seizures starting before the age of 3 years, Agostinelli and collaborators found that those who did meet Panayiotopoulos's inclusion criteria of childhood absence epilepsy showed a favorable course of epilepsy, whereas patients not fulfilling Panayiotopoulos's criteria showed increased risk of relapse at long-term follow-up (04; 166). Similarly, Grosso and colleagues demonstrated the strong influence of inclusion and exclusion criteria on the outcome (70). Conversely, refractory absence seizures occur in children that have been classified as having childhood absence epilepsy (57).
Juvenile absence epilepsy. Juvenile absence epilepsy is an idiopathic generalized epilepsy mainly characterized by typical absences that are less frequent (spaniolepsy) and probably not as severe as, childhood absence epilepsy (74; 118). Generalized tonic-clonic seizures and myoclonic jerks are part of the phenotype in 80% and 15% to 30% respectively, and absence status epilepticus occurs in about 20% of cases (36). Age at onset is between 7 and 16 years with a peak at 10 to 12 years. Juvenile absence epilepsy is a lifelong disorder, but absences tend to become less severe with age. Almost half of patients have poor seizure control with a high rate of pharmacoresistance (39). The ictal EEG shows generalized, spike or multiple spike-and-slow waves at 2.5 to 4 Hz.
Exclusion criteria for juvenile absence epilepsy. Mild impairment of consciousness, brief ictal discharges (less than 4 seconds), eyelid or perioral myoclonus, rhythmic limb jerking, and single or arrhythmic myoclonic jerks during the absence ictus are incompatible with juvenile absence epilepsy. Visual, photo-sensitive, and other sensory precipitation of absences may be against the diagnosis of juvenile absence epilepsy.
Myoclonic absence epilepsy. Myoclonic absence epilepsy is a rare generalized unknown (cryptogenic) or symptomatic epilepsy, where typical absence and myoclonic jerks are the predominant type of seizures in the phenotype (36). Severe bilateral rhythmical clonic jerks, often associated with a tonic contraction, occur during the absence concomitant with generalized spike-and-wave discharges in the EEG. Each spike correlates with a jerk and the slow wave with the tonic contraction. Two thirds are symptomatic and one third idiopathic or unknown. Approximately 45% have intellectual disability from start and 70% final. Almost 50% persist above the age of 20 years old.
Eyelid myoclonia and absences (formerly known as Jeavons syndrome). Eyelid myoclonia “and absences” is preferable to “with absences” for the reason that absence seizures provoked during photic stimulation are evoked independent to eye closure and with eyes open. Eyelid myoclonia and absences is an idiopathic generalized epilepsy manifested with eyelid myoclonia and typical absences as the predominant seizures in the phenotype (36). Eyelid myoclonia consists of marked, rhythmic, and fast jerks of the eyelids immediately after voluntary or on-command eye closure in the light and is often associated with jerky upward deviation of the eyeballs and retropulsion of the head. The seizures are brief (3 to 6 seconds) and occur mainly after eye closure. Onset is usually in early childhood. All patients are highly photosensitive in childhood, but this declines with age. Infrequent generalized tonic-clonic seizures are inevitable in the long term, and they are likely to occur after sleep deprivation, fatigue, and alcohol indulgence. Myoclonic jerks of the limbs may occur but are infrequent and random. Eyelid myoclonia and absences may be resistant to treatment and lifelong. The EEG ictal manifestations consist mainly of generalized polyspikes and slow waves at 3 to 6 Hz, though these are more likely to occur immediately after eye closure in an illuminated room. Total darkness abolishes the abnormalities related to eye closure. Photoparoxysmal responses are recorded from all untreated young patients.
Juvenile myoclonic epilepsy. Juvenile myoclonic epilepsy is a genetically determined, common idiopathic generalized epilepsy. Prevalence is 5% to 11% among adult and adolescent patients with other epilepsies, and both sexes are equally affected. Juvenile myoclonic epilepsy is characterized by myoclonic jerks on awakening, generalized tonic-clonic seizures, and typical absences in more than one third of the patients. The seizures have an age-related onset with absences first appearing either in childhood or adolescence, followed by myoclonic jerks and generalized tonic-clonic seizures in the middle teens. Rarely, absence seizures concomitant with myoclonic seizures appearing before the age of 3 years may herald juvenile myoclonic epilepsy. In such cases, the final diagnosis is made at an older age when relapses occur after treatment is discontinued and the classical electroclinical features of juvenile myoclonic epilepsy are recorded. Seizure-precipitating factors like sleep deprivation and fatigue, alcohol, photosensitivity, and mental and psychological arousal are prominent. All seizures are probably lifelong, although absences may become less severe with age; jerks and generalized tonic-clonic seizures commonly improve after the fourth decade of life. Typical absences are usually highly mild and simple (with no automatisms or localized limb jerks), and impairment of consciousness is subtle. Generalized discharges of 3 to 6 Hz spike-and-waves have an unstable intradischarge frequency with fragmentations and multiple spikes. In the author’s experience, myoclonic jerks occur in all by definition and typical absences in at least 48%, generalized tonic-clonic in 60%, and positive response to intermittent photic stimulation in 75% of cases (36). Absence seizures (conspicuous or inconspicuous) are usually evoked during photic stimulation and may precede or follow a jerk.
The following are possible syndromes with typical absence seizures (116; 117; 118):
Facial (perioral, eyebrow, or mixed) myoclonia and absences. This is an idiopathic generalized epilepsy with onset in childhood or early adolescence (36; 118). Rhythmic myoclonus of the perioral or eyebrow muscles occurs during the absence, together with a variable impairment of consciousness. The absences are frequent and may be brief. Absence status is common. Generalized tonic-clonic seizures, usually infrequent, always occur either early or many years after the onset of absences. Clusters of absences or absence status usually precede generalized tonic-clonic seizures. Absences and generalized tonic-clonic seizures may be resistant to medication, unremitting, and possibly lifelong. Other patients may have a mild but long-standing course. Ictal EEG shows high-amplitude generalized discharges of typical but often irregular, rhythmic multiple spike waves and slow waves at 2 to 4.5 Hz. Photosensitivity is rare, occurring around 18% of cases.
The syndrome of phantom absences and generalized tonic-clonic seizures. “Phantom absences” denote typical absences that are so mild that they are inconspicuous to the patient and imperceptible to the observer. They are disclosed by video-EEG recording and breath-counting or other cognitive testing during hyperventilation with brief (usually 3 to 4 seconds) 3 to 4 Hz spike or multiple spike wave and slow wave discharges. The absences are simple, occasionally with eyelid blinking. They may be clinically unrecognized, but they usually manifest in adult life with generalized tonic-clonic seizures, and often with absence status epilepticus (122; 86).
Typical absences with specific modes of precipitation (reflex absences). Absence seizures can be provoked with specific modes of precipitation (eg, photic, pattern, video games, thinking, reading, fixation-off).
Absences with single myoclonic jerks during the absence ictus. Typical absences with single, often violent jerks of the head, body, or limbs during the absences ictus may appear in early childhood and continue in adult life, often with other types of generalized seizures. They are frequently difficult to treat and may be associated with a bad prognosis.
Symptomatic and unknown (cryptogenic) absences. Although typical absences are considered the paradigm seizure type of idiopathic generalized epilepsy, they may occasionally be symptomatic, arising as a consequence of a known disorder of the central nervous system (53). Symptomatic and cryptogenic absences may be focal or diffuse, traumatic, metabolic, or inflammatory. In most cases an etiologic link is not proven, and it is likely that they are coincidental. The mesial surfaces of the frontal lobe are most likely to generate typical absences. “Brief blank spells” with 3 Hz spike-wave EEG paroxysms mainly due to subependymal heterotopia have been reported (131).
The absence seizures in Dravet syndrome have been studied by Tsuda and colleagues (156). The mean age at their onset was 16.2 +/- 7.1 months, their duration ranged from 2 to 180 seconds, and the frequency of the EEG discharge was from 2 to 4 Hz (median=3 Hz). Clinical manifestations included eyelid-myoclonus (17%) and generalized myoclonus (44%). Absence seizures in Dravet syndrome are characterized by an early age of onset, a high incidence of irregular and disorganized 3 Hz generalized spike-and-wave morphology, and the frequent association of generalized myoclonic movement as well as the absence of automatism as compared to typical absence seizures.
It is apparent from the above description of syndromes with typical absences that most of them are lifelong and manifest with myoclonic jerks and generalized tonic-clonic seizures.
Factors influencing the clinical and EEG features of typical absence seizures. Features of typical absences, as with any other type of seizure, depend on brain maturity, the sleep-wake cycle, provocation, and a variety of other factors. Overall, children with childhood absence epilepsy have typical absences with conspicuous and profound impairment of consciousness and lengthy duration more often than adults (36). Spontaneous eye-opening (when not caused by motor events), like all other automatisms, occurs only when consciousness is severely impaired (119). The variability of impairment of consciousness, conspicuous or inconspicuous, and duration of typical absences by age also contributes to shaping the clinical presentation of syndromes of idiopathic generalized epilepsy that, as with many other epileptic syndromes (eg, self-limited epilepsy with centrotemporal spikes rolandic), may be age-dependent and age-limited. Conversely, even age-influenced individual features of typical absences are also syndrome-related as indicated by the fact that children may also have brief and mild absences, and conversely adults may also manifest with severe and lengthy absences. Follow-up studies have shown that absences become milder with age, but this may be delayed for decades as in juvenile myoclonic epilepsy (118). Sleep modifies the clinical and EEG features of absences; in sleep, EEG discharges of spike-polyspike and slow wave are usually shorter and devoid of discernible clinical manifestations—even in those patients who have numerous clinical seizures during the alert state.
Are features of absence seizures syndrome related? The syndromes of idiopathic generalized epilepsy with typical absences, like all other medical and epileptic disorders, require rigorous and detailed clinico-laboratory documentation for their validation. An individual symptom, EEG discharge, or even a type of seizure does not constitute an epileptic syndrome; rather, it is the nonfortuitous clustering of historical, clinical, and video-EEG symptoms and signs that makes a syndrome (32). Follow-up studies are particularly important in children in whom syndromes often progress to seizures other than those in the initial presentation within days, weeks, months, or years.
Sadleir and associates have different views, but their study was based on weak diagnostic procedures (retrospective, semiological study based on video-EEG-recorded seizures without standardized methodology, follow-up, and verification of diagnosis) and debatable definitions (137). They defined as absence seizure any type of greater than 2.5 Hz spike-polyspike wave associated with clinical signs--even if this is not associated with impairment of consciousness. The classification of their patients was equally questionable, with contradicting principles of definitions. In their attempt for “a cleaner gestalt of the majority of patients presenting with each syndrome rather than the ‘’overlap’’ cases” (140), they arbitrarily considered myoclonic jerks as an exclusion criterion for juvenile absence epilepsy (though one third of these patients have myoclonic jerks). And absence seizures of juvenile myoclonic epilepsy were studied only when onset was at 11 years and older (which means that juvenile myoclonic epilepsy subjects with onset of absences between 8 and 11 years of age were either absent or misplaced in childhood absence epilepsy). Contrary to this intention “of a cleaner gestalt” was the classification of childhood absence epilepsy that included any patient with onset of absences between 2 and 10 years of age (which comprises a vastly heterogeneous group of absence syndromes, including epilepsy with myoclonic absences that may start with typical absences devoid of myoclonic components, myoclonic epilepsy in infancy and childhood with onset under 4 years and absence seizures in one third of cases, juvenile myoclonic epilepsy with onset before 10 years of age, eyelid myoclonia and absences, and so forth). These contradicting criteria of definitions explain the small number of patients with juvenile myoclonic epilepsy (6 patients) and juvenile absence epilepsy (8 patients) as opposed to childhood absence epilepsy (47 patients). It is because of all these problems that Sadleir and colleagues found that opening of the eyes (an automatism) is as common in juvenile myoclonic epilepsy as in childhood absence epilepsy (137). In their companion commentary, Scheffer and Berg rightly emphasized the following (140):
|
We should not strive to achieve a specific result but to use valid, accepted methods that lead us to the most reliable result, one we hope is as close as possible to an elusive truth, whatever that may be. As researchers, we need to remain dispassionate about our findings and accepting of new data that challenge or even refute our previously held views of epilepsy syndromes, constantly but methodically revising and refining our understanding to make it more robust. |
To achieve this goal in idiopathic generalized epilepsy with absences, we need true evidence based on robust and consistent standardized methodology and diagnostic precision.
The EEG, preferably sleep-awake video-EEG and particularly in infancy and early childhood, is the single most important procedure in diagnosing typical absence seizures. Ictal EEG demonstrates high amplitude discharges of spike, multiple spike, and slow-wave discharges usually 3 to 4 Hz (range 2.5 to 6 Hz). These discharges can sometimes have maximum frontal or begin with unilateral spikes (158).
Hyperventilation induces absence seizures in almost all (more than 90%) untreated or treated with inappropriate drug cases. Hyperventilation is preferably done while standing in order to identify concomitant unsteadiness or perseverative movements. They are best studied with video EEG. Ideally, all children with absence seizures should have video-EEG recordings in an untreated state, as this may reveal features favoring a specific epileptic syndrome and may, therefore, determine long-term prognosis and management. If this is not possible, the clinical manifestations of the seizures should be documented with camcorders by the parents or the treating physicians. The absences are videotaped while the patient is holding hands in front of him or her and counting his or her breaths while overbreathing for 3 minutes. In a randomized multicenter controlled trial among 20 children (4 to 10 years old) with typical absence seizures, hyperventilation while sitting without backrest provoked 17 absences and while being in supine position 13 absences (p = 0.031) (135). All patients that had absence seizures during supine hyperventilation also had seizures during sitting hyperventilation and were of shorter duration (mean 8.69 seconds).
Breath-counting during hyperventilation (wherein the patient is asked to count his or her deep breaths) is an important, often neglected, method to detect impairment of consciousness during the discharge. Practical, easy to perform, and clinically relevant, this method may reflect impaired performance in daily life. Frequently, the patients are able to recall numbers or phrases told to them during the spike wave and slow wave discharge, whereas these may be associated with serious errors in breath-counting (118). Despite its practicality, breath-counting is rarely performed in EEG examinations of these patients; unfortunately, absences are often not apparent without this procedure. The significance of breath-counting may be appreciated by reviewing the video clips with the volume off.
Be aware that the ability to recall numbers or phrases or count may not be affected during brief spike-and-slow wave discharges. This diagnostic method is also difficult in early childhood and infancy. In addition, the given message or counting rate should be quicker than the brief discharge in order to identify concomitant impaired awareness. Only by observing carefully the video-EEG during brief generalized spike-wave discharges, we may observe concomitant relevant transient impassive facial expression and a vague look. Furthermore, in the younger age group, hyperventilation is encouraged by blowing either a paper, a paper streamer, pinwheel, spinning wheel, or a straw inside a cup with fluid causing bubbles (36).
Sleep EEG patterns are normal. Generalized discharges of polyspike waves and slow waves are more likely to increase, but a reduction is also observed during sleep. The discharges are shorter, may be fragmented, and usually are devoid of discernible clinical manifestations, even in those patients who have numerous clinical seizures with motor manifestations during the alert state.
If diagnosis of epilepsies by age at onset is to be followed, idiopathic generalized epilepsies exist in infancy and childhood, whereas typical absence seizures are part of the phenotype either as the only seizure type or combined with myoclonic jerks or generalized tonic-clonic seizures. In this respect, not all typical absence seizures occurring in childhood belong to the syndrome childhood absence epilepsy. Some of these epilepsies are well recognized or not yet as syndromes by the ILAE commission on classification, and some other in infancy and early childhood remind us of syndromes we see in childhood and adolescence. A practical classification of idiopathic generalized epilepsies appearing from infancy to adolescence with typical absence seizures in their phenotype was reported in 2010 (36).
In the few cases for which an accurate and complete diagnosis of absence seizures is difficult, particularly in early childhood, the use of low-cost, portable EEG device monitoring may be useful in facilitating diagnosis. For example, EEG home monitoring is feasible in pediatric patients as long as an EEG wearable is easy to put on and is comfortable. Remote seizure monitoring will be one of the elements of personalized treatment for childhood absence epilepsy and juvenile absence epilepsy, similar to personalized drug titration and determining the duration of pharmacotherapy (65).
Twenty-four-hour EEG recording is the gold standard for assessing patients with an absence epilepsy sensitivity of less than 10% of their absences. It is often performed in the hospital and is expensive, obtrusive, and time-consuming to review. A study investigated the performance of an unobtrusive, two-channel, behind-the-ear EEG- based wearable, the Sensor Dot monitoring at home, to detect typical absences in adults and children (149). The authors concomitantly recorded 284 absences on video-EEG and Sensor Dot. Using the wearable Sensor Dot, epileptologists were able to reliably detect (F1 score = .73) typical absence seizures and reduced the review time of a 24-hour recording from 1 to 2 hours to around 5 to10 minutes. However, for research purposes, absence seizures were defined as having 3 Hz generalized spike-wave discharges for at least 3 seconds. Although the accuracy is not perfect, absences usually occur very frequently; therefore, it seems that this method will not significantly influence the outcome. In this author’s opinion, this method can be useful for quantifying the absence seizures only in well-documented cases of the syndrome, with proper routine EEG recording methodology.
Children with absence seizures, particularly those with childhood absence epilepsy, eyelid myoclonia and absences, and facial myoclonia and absences should also be assessed neurophysiologically. Some children have deficits involving attention, executive function, visuospatial memory, and reading. Such an assessment should be periodically performed to provide appropriate supportive help. Depression, anxiety, and attention deficit hyperactivity disorder have also been reported in children with childhood absence epilepsy (96).
In a systematic literature search, 33 studies reporting on cognitive performance in children with absence epilepsy were considered (169). Neuropsychological tests were classified into the following domains: intelligence; executive function; attention; language; motor and sensory-perceptual examinations; visuoperceptual/visuospatial/visuoconstructional function; memory and learning; and achievement. In contrast to the common belief that cognition in absence epilepsy is generally undisturbed, lower than average neurocognitive performance was noted in multiple cognitive domains, which may influence academic and psychosocial development. This, together with the failure of antiseizure drug monotherapy in children with absence epilepsy, the persistence of cognitive impairments even after apparent seizure suppression, the high probability of the development of generalized tonic-clonic seizures (152), and absence-associated comorbidities (anxiety and depression) (159), necessitates the identification of novel therapeutic targets.
Children with childhood absence epilepsy have elevated rates of adverse behavioral, psychiatric, language, and cognitive comorbidities, including attention problems, anxiety, depression, social isolation, and low self-esteem (152). These psychiatric and cognitive abnormalities were correlated with disease duration and interictal spike load in a publication (47).
In a Danish cohort study, school performance and psychiatric comorbidity in 114 children with childhood absence epilepsy were compared with both population controls and nonneurologic chronically ill children. Children with childhood absence epilepsy had increased psychiatric comorbidity, and a considerable proportion of these children receive special needs education in primary/secondary school, albeit insufficient to normalize their considerably lower grade point average in the 9th grade by 1.7 grade points (18).
In general, it is known that genes coding for T-type calcium channels and for GABA receptors have been associated with the etiopathogenesis of childhood absence epilepsy, and abnormal oscillatory rhythms can originate either from T-type channel abnormalities or from the increased GABA-B activity (124). Therefore, antiseizure drugs that suppress T-type calcium channels (eg, ethosuximide, valproate) are effective anti-absence drugs, whereas those that increase GABA-B activity (eg, carbamazepine, vigabatrin), exacerbate the frequency of absence seizures. Furthermore, GABA-A agonists (eg, benzodiazepines), which preferentially enhance GABA-ergic activity in neurons from the thalamic nucleus reticularis, can suppress absence seizures (124).
Monotherapy if typical absences are the only type of seizures. Treatment is mainly with sodium valproate or ethosuximide, which are of equal efficacy controlling absences in around 85% of patients (37). The rest (15%) responded to the combination of sodium valproate and ethosuximide or levetiracetam, lamotrigine, and benzodiazepines. Ethosuximide should be preferred as monotherapy in idiopathic generalized epilepsies with typical absence seizures only, whereas valproate should be added or used as monotherapy for those cases with aberrant electroclinical features, particularly generalized tonic-clonic seizures. Lamotrigine monotherapy is less effective with nearly half of the patients becoming seizure free (34; 76; 66; 175; 19; 143). Glauser and colleagues performed a double-blind, randomized, controlled clinical trial to compare the efficacy, tolerability, and neuropsychological effects of ethosuximide, valproic acid, and lamotrigine in children with newly diagnosed childhood absence epilepsy (66). Drug doses were incrementally increased until the children were free of seizures, the maximal allowable or highest tolerable dose was reached, or a criterion indicating treatment failure was met. The primary outcome was freedom from treatment failure after 16 weeks of therapy; the secondary outcome was attentional dysfunction. Differential drug effects were determined by means of pairwise comparisons. The 453 children who were randomly assigned to treatment with ethosuximide (156), lamotrigine (149), or valproic acid (148) were similar with respect to their demographic characteristics. After 16 weeks of therapy, the freedom-from-failure rates for ethosuximide and valproic acid were similar (53% and 58%, respectively; odds ratio with valproic acid vs. ethosuximide, 1.26; 95% confidence interval [CI], 0.80 to 1.98; P=0.35) and were higher than the rate for lamotrigine (29%; odds ratio with ethosuximide vs. lamotrigine, 2.66; 95% CI, 1.65 to 4.28; odds ratio with valproic acid vs. lamotrigine, 3.34; 95% CI, 2.06 to 5.42; P< 0.001 for both comparisons). There were no significant differences among the three drugs with regard to discontinuation because of adverse events. Attentional dysfunction was more common with valproic acid than with ethosuximide (in 49% of the children vs. 33%; odds ratio, 1.95; 95% CI, 1.12 to 3.41; P=0.03) (66).
In a study, ethosuximide was associated with a higher rate of complete remission than valproate in childhood absence epilepsy, which may suggest that ethosuximide has a beneficial potential disease-modifying effect on this epileptic syndrome (13). Furthermore, in another study, class 1 evidence was provided that valproate is associated with more significant attentional dysfunction than ethosuximide or lamotrigine in children with newly diagnosed childhood absence epilepsy (95).
As second monotherapy, ethosuximide and valproate demonstrate higher freedom from failure proportions and greater efficacy than lamotrigine; valproate is more often associated with attentional dysfunction (30). When valproate does not control typical absence seizures, ethosuximide is the drug of second choice. The most frequent side effects of ethosuximide are abdominal pain and nausea. For this reason, it should be taken with meals. In a publication, two cases of childhood absence epilepsy were reported that showed seizure disappearance after ethosuximide was added to valproate and ethosuximide drug eruption occurred, suggesting the possibility that the epilepsy disappears due to immune responses to antiseizure medication (103).
Genetic variation plays a role in differential drug response of childhood absence epilepsy (67).
If monotherapy fails or unacceptable adverse reactions appear, replacement the antiepileptic drug by another of the three drugs is the alternative. The most effective combination treatment is valproate with small doses of lamotrigine, which is possibly due to a pharmacodynamic interaction between these two drugs (120; 85), or levetiracetam slow titration when absence and myoclonic seizures co-exist. Inhaling medical carbogen containing 5% CO2 and 95% O2 can suppress hyperventilation-induced absence seizures and spike-and-wave discharges and, therefore, it could be a therapeutic approach for hyperventilation-related absence seizures (174).
In 20 patients with childhood absence epilepsy and incomplete seizure control in therapy with first antiseizure medication (seven ethosuximide, five valproate, five levetiracetam, and three lamotrigine), perampanel was added as first add-on antiseizure drug (112). None of the patients had generalized tonic-clonic seizures. Fifteen cases became seizure-free, and video EEG was negative for epileptic abnormalities (five with valproate, five with levetiracetam, three with ethosuximide, and two with lamotrigine). The retention rate after 12 months of follow-up was 75%. The tolerability profile was favorable. The patients who were seizure-free with adjunctive perampanel were switched to perampanel monotherapy (mean follow-up on perampanel monotherapy = 5.56 ± 1.59 months). Nine of 15 remained seizure free in monotherapy with perampanel, whereas the other six relapsed and the double antiseizure therapy was restored (112).
Monotherapy in syndromes of idiopathic generalized epilepsy with typical absence seizures and other types of generalized seizures such as myoclonic jerks, generalized tonic-clonic seizures, or both. Established first-line monotherapy is with sodium valproate, which controls absence seizures in 75% to 85%, generalized tonic-clonic seizures in 70% and myoclonic jerks in 75% (37; 36; 115; 118). A major problem is that sodium valproate is undesirable in women because of teratogenic effects, weight gain, and polycystic ovarian syndrome. Therefore, it should not be used in females of childbearing age, particularly if contraception is not being used.
The adverse effects of valproate and its lack of efficacy in 25% of patients have prompted the search for alternatives among newer AEDs. Levetiracetam appears to be most promising of all because it is highly effective in controlling generalized tonic-clonic seizures, myoclonic jerks, photosensitivity (14; 162; 105), and probably absence seizures (27; 43; 163; 52). In a report, aggravation of absences with levetiracetam has been reported in six patients resistant to other AEDs (07). These six patients were retrospectively found from an unspecified number of probably a large population of children with absence epilepsy from three pediatric neurology departments in France; how many patients benefitted from this drug has not been reported. In another study, only about one-quarter of children with absence epilepsy became seizure free with levetiracetam (106). When effective, this occurred at a relative low dose.
Lamotrigine is effective in controlling generalized tonic-clonic seizures and absence seizures, but it exaggerates myoclonic jerks (118). Topiramate is totally ineffective in absence seizures of childhood absence epilepsy (128) and often has serious cognitive and other adverse reactions.
Monotherapy should not be abandoned before making sure that maximum tolerated dose has been achieved if smaller doses have failed. If monotherapy fails or unacceptable adverse reactions appear, then replacement of one by the other is the alternative.
Polytherapy in syndromes of idiopathic generalized epilepsy with typical absence seizures and other types of generalized seizures such as myoclonic jerks, generalized tonic-clonic seizures, or both. For monotherapy failures, sodium valproate, levetiracetam, lamotrigine, and probably zonisamide appear to be effective in polytherapy. Small, minute doses of lamotrigine added to adequate doses of sodium valproate may have a dramatic beneficial effect in more than half of the patients. In persistent myoclonic jerks, the best add-on drug is clonazepam that in small doses (0.5 to 2 mg) prior to sleep may have a dramatic beneficial effect. Ethosuximide should be added only for uncontrolled absence seizures. Zonisamide is efficacious in approximately half of patients with absence seizures (125). In 2005, a chart review of 45 patients (mean age 11.4 years; range 2.8 to 17.9 years) with absence seizures was conducted to assess the effectiveness and safety of zonisamide in absence epilepsy. Patients received a mean daily dose of zonisamide 343 mg or 9.0 mg/kg (range, 100 to 600 mg or 2 to 24 mg/kg). Twenty-three of 45 patients (51.1%) obtained seizure freedom, whereas 16 of 45 patients (35.6%) experienced 50% or greater seizure reduction. Five patients (11.1%) had less than 50% seizure reduction, whereas one patient (2.2%) had an increase in seizure frequency. Nineteen patients (42.2%) reported one or more unwanted effects, with decreased appetite (15.5%) and sleepiness (11.1%) being the most common. Two patients discontinued zonisamide therapy, one for an increase in seizure frequency and apparent inefficacy and sleepiness in the other (172).
Newer antiseizure medications, such as brivaracetam and perampanel, seem to be promising options. Well-conducted clinical trials aimed at evaluating the efficacy of alternative monotherapy (beyond ethosuximide, valproic acid or lamotrigine) or the combination of antiseizure medications on difficult-to-treat typical absences, are warranted.
Amantadine may constitute an efficacious alternative treatment for refractory absence seizures (127). In one study, a response of at least 50% seizure reduction was reported in more than 50% of patients; among responders, a majority had greater than 90% reduction in seizure frequency (127).
Furthermore, chronic treatment with the sodium channel blocker, lacosamide, in genetic absence epilepsy rats modified the development of absence seizures, suggesting that lacosamide exerts beneficial effects on absence seizure epileptogenesis (25).
In summary, ethosuximide should be used as monotherapy in those cases that experience absence seizures only. Sodium valproate, or even lamotrigine, should be used in absence seizures with aberrant electroclinical features, alone or in combination. Alternative choices are levetiracetam, benzodiazepines, zonisamide, brivaracetam, perampanel, and topiramate. Any relevant trigger factors such as lack of sleep or noncompliance should also be avoided. Absence status emergency treatment includes lorazepam or diazepam, or even sodium valproate. As with any other seizure-type epilepsy, a basic neuropsychological assessment, follow-up, and appropriate intervention is advisable.
Be aware in adult patients, even for absence seizures, there is a self-reporting dependency on seizure reporting in order to determine seizure frequency for epilepsy management. A study showed that absence seizures in adults are highly misreported. Using inpatient video-EEG telemetry or outpatient ambulatory electroencephalography, only 24% and 26% of seizures were correctly identified in the over- and underreporting assessment groups, respectively (129).
Contraindicated drugs. The treatment of idiopathic generalized epilepsy is demanding because many antiepileptic drugs are either ineffective or exaggerate absences and myoclonic jerks (142; 118). An antiepileptic drug is contraindicated not only when it exaggerates seizures but also when it is ineffective in controlling the seizures that it is supposed to treat. It may cause unnecessary adverse reactions and deprives the patient of the therapeutic effect that could be provided by another antiepileptic drug. In general, GABA-ergic anticonvulsants, such as carbamazepine, vigabatrin, and tiagabine are contraindicated in the treatment of absence seizures, irrespective of cause and severity. This is based on clinical and experimental evidence. In particular, the GABA agonists vigabatrin and tiagabine are used to induce, not to treat, absence seizures and absence status epilepticus (92; 118). The error of prescribing these drugs in the treatment of absence seizures may be of the same magnitude as prescribing a gluten-rich diet in the treatment of celiac disease. Similarly, phenytoin, phenobarbital, gabapentin, and pregabalin should not be used in the treatment of absence seizures (118).
Recognizing GLUT1 deficiency syndrome is important, because a ketogenic diet is effective in improving epileptic seizures and may also reduce some neurologic symptoms. Most antiepileptic drugs are contraindicated either because they are ineffective or because they exaggerate seizures (84; 87). Phenobarbital, but also chloral hydrate and diazepam, may further impair GLUT1 and should not be used in these patients.
Withdrawing antiepileptic medication. Withdrawal of the medication is dependent on the syndrome (118). In the pure form of childhood absence epilepsy--with no aberrant electroclinical features (the syndrome), drug therapy can be gradually withdrawn (within 3 to 6 months) after 2 to 3 seizure-free years (37). In others, such as juvenile absence epilepsy, juvenile myoclonic epilepsy, or eyelid myoclonia and absences, treatment may be lifelong (116; 117; 118).
In general, early correct diagnosis and management leads to better outcome. The evolution of epilepsies with typical absence seizures in their phenotype is variable from excellent to less favorable, depending on the underlying epilepsy syndrome. In a video-EEG recording analysis of 213 typical absence seizures from 61 patients with idiopathic generalized epilepsy, the presence of polyspikes had a high positive predictive value for unfavorable therapeutic outcome. In contrast, none of the semiological features, alone or in combination, were predictors of therapeutic outcome (Vlachou et al 2022).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Thanos Covanis MD DCH PhD
Dr. Covanis of Childrens’ Hospital Agia Sophia in Athens, Greece has no relevant financial relationship to disclose.
See Profile
Solomon L Moshé MD
Dr. Moshé of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Apr. 22, 2024
Behavioral & Cognitive Disorders
Apr. 18, 2024
Behavioral & Cognitive Disorders
Apr. 17, 2024
General Child Neurology
Apr. 05, 2024
Epilepsy & Seizures
Apr. 03, 2024
Epilepsy & Seizures
Apr. 02, 2024
General Child Neurology
Apr. 01, 2024
General Child Neurology
Mar. 29, 2024