


Behavioral & Cognitive Disorders
Intellectual disability
Apr. 17, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The term “visual agnosia” encompasses a group of neurologic disorders. Patients with one of these disorders cannot recognize some or all objects by sight but can do so using other sensory modalities, such as sound or touch. Their problem also cannot be attributed to broader problems with language, memory, or basic visual functions. Agnosia can be general, affecting all types of objects, or specific to certain types of objects. In this article, the authors review the different forms of visual agnosia with respect to clinical characteristics, pathogenesis, structural localization, differential diagnosis, diagnostic evaluation, and rehabilitation.
• Visual agnosia is a rare problem characterized by an inability to recognize objects by sight, despite preserved ability to do so by sound or touch. | |
• The two main streams of visual processing beyond the primary visual cortex are the dorsal (“where”) stream and the ventral (“what”) stream. Visual agnosia is a problem of the latter. | |
• Visual agnosia is classified into general and selective visual agnosias. | |
• Subtypes of selective visual agnosia are named according to the class of visual objects affected. | |
• Rehabilitation programs for agnosia remain largely experimental. |
Visual agnosia is the inability to recognize objects by sight. Descriptions of visual agnosia have been around for over a century. One of the earliest experimental observations was that a dog with partial ablations of both occipital lobes lost its usual responses to familiar objects but could still navigate around them, suggesting that it could see but could not recognize (100). In 1890, Lissauer described this “mind-blindness” in humans (87). He also distinguished between two forms: an apperceptive one, in which subjects did not perceive objects well, and an associative one, in which subjects could not link what they saw with their stored knowledge about objects (110). In 1891, Freud introduced the term "agnosia," which was later defined more specifically as a failure to recognize objects that was not attributable to poor visual acuity, cognitive impairment, or aphasia.
General visual agnosia. General visual agnosia is the loss of visual recognition for all types of objects. Patients make gross misidentifications, such as the man who mistook his wife for a hat (109). Beyond the broad distinction between apperceptive and associative forms, recent years have seen the description of further subtypes of each and the emergence of a more refined taxonomy (73; 52).
Form agnosia. Form agnosia is a type of apperceptive agnosia. Patients with this type of agnosia have difficulty seeing even basic shapes, which are the building blocks of object structure (21); however, they can see elementary visual properties, such as brightness, contrast, and motion.
Integrative agnosia. Integrative agnosia is another type of apperceptive agnosia. Patients with this type of agnosia can see basic shapes but cannot integrate these shapes into the more complex structures of real objects (73). Hence, they may see two round wheels and two triangles but not realize they form a bicycle. These patients have trouble parsing a complex scene with multiple objects and figuring out which elements belong to which object. This deficit can be shown in their struggles with overlapping figures (73; 65).
Transformation agnosia. Transformation agnosia is a rare condition in which subjects cannot recognize objects shown from unusual (“non-canonical”) viewpoints. One interpretation is that this deficit reflects a problem with deriving a viewpoint-independent representation of an object’s three-dimensional structure (130). These subjects have no trouble with more typical views of objects and, thus, may not struggle with recognizing objects in daily life.
These perceptual functions are relatively intact in patients with associative forms of general visual agnosia. Patients with associative agnosias have trouble linking what they see with what they know, as in semantic access agnosia, or may have lost that visual knowledge, as in semantic agnosia (73). This knowledge may concern either what objects look like (ie, their “structural representations”) or general “semantic” facts about objects (eg, their function and where they are found). Some of these general agnosias exhibit a degree of category-specificity; knowledge about living things like plants and animals is more deficient than knowledge about man-made objects like tools, furniture, or vehicles (51; 84; 25). This deficit may be due to the greater visual complexity and similarity of natural objects (74).
Beyond the general visual agnosias, there are also selective visual agnosias. Patients with these deficits do not confuse people for apparel but struggle with finer distinctions. Sometimes their difficulties are referred to as problems with making “within-category” judgments (50) about objects (eg, “what type of car is this?”), in contrast to the “between-category” difficulties (eg, “is this a car or a boat?”) characteristic of patients with general visual agnosias. These deficits affect certain types of objects more than others for the different selective agnosias.
Prosopagnosia. Prosopagnosia is the inability to recognize the identity of previously learned faces as being familiar (08; 39). This deficit may or may not spare the perception of other types of face information, such as expression, age, and gender. Whether this problem with object identity is truly specific to faces alone is a matter of much debate. More rigorous testing suggests that most but not all patients with prosopagnosia have some difficulty identifying other types of objects, such as cars, bicycles, and animals (60; 09).
There are apperceptive, associative, and amnestic variants of prosopagnosia (37). Those with the apperceptive variant cannot see differences in the facial structure of different people. Those with the amnestic variant do better but cannot recall what specific faces look like, which can be tested using a questionnaire about what they remember about famous people’s faces (10). Those with the associative form have good facial perception and preserved facial memories but cannot match the former to the latter. In addition to the acquired form, there is a developmental variant (118).
Pure alexia. Pure alexia is also known as “word blindness” or “alexia without agraphia.” Patients with this condition have an acquired inefficiency in the reading of words. At the severe end are patients with global alexia, who cannot read words at all (22); this deficit may extend to letters and numbers and other forms of visual symbolic communication, such as musical notation or map symbols (72; 19). At the milder end are “letter-by-letter” readers, who can read but do so slowly, exhibiting a characteristically increased “word-length effect,” which is the correlation between the number of letters in the word and the time it takes to read it (14).
Topographic disorientation. Topographic disorientation is manifest as getting lost in familiar surroundings. This navigation failure has a number of possible causes (28). Landmark agnosia is the inability to recognize landmarks, such as buildings and scenes (119). Impaired cognitive map formation is the inability to place these landmarks in a mental map of the environment, which is the most flexible means of navigation. Heading disorientation is the inability to orient oneself correctly within this environment. Topographic disorientation also has a developmental variant (76; 75).
Patients with visual agnosia may have vague complaints about “not being able to see right” or very specific complaints, such as not being able to recognize people any longer. In some cases, the patient may falsely attribute these deficits to more obvious problems, such as hemianopia. Some patients will attempt to improve their vision by having several sets of new glasses made. Diagnosis often requires directed questions or testing to realize that their struggles are due to poor object recognition. Subjects with the developmental forms may not have good insight into their problem (102) and only come to attention when they realize that other people are seeing things that they are not seeing. Hence, eliciting the problem may depend on a high index of suspicion on the part of the examiner, given the clinical setting and neuroimaging findings, and an awareness of what types of difficulties can be explained by other deficits like hemianopia.
Patients with general visual agnosia struggle with many daily tasks. They may not be able to tell coins apart, know which buttons to press on their phone, or recognize where they are. A common complaint is that they cannot find things, such as food in their refrigerator or tools in a toolbox, which leads them to make errors in what they eventually select and only realize the error when they grasp the object. This difficulty will be true for any variants of general visual agnosia described above.
Selective visual agnosia is less disruptive. Patients with acquired prosopagnosia are often aware that they cannot recognize faces anymore. Those with the apperceptive variant may complain that all faces look similar, like pebbles on a beach. They may rely on other visual cues, like hairstyle (which unfortunately can change easily), unusual facial features (for example, John Travolta’s chin), or dynamic cues, such as gait or mannerisms. Almost all afflicted patients report that they depend heavily on recognizing voices.
Patients with alexia report slow, error-prone reading. Print size does not help, and it makes no difference whether they are reading something close to them or at a distance. On the other hand, they can write with relative ease.
Those with topographic disorientation get lost in familiar surroundings. Anyone can get lost in a new place, but these patients get lost in places they have known for years, such as their neighborhood, even within their own house or those of their friends. Patients with place agnosia may seize on the expedient of reading street signs to find their way, but this will not help those who cannot form a cognitive map. Both types of patients may come to rely on GPS devices.
Developmental disorders of object recognition are stable, lifelong problems. Subjects often learn strategies for living with their difficulties, but some agnosia forms still have psychosocial consequences. Those with developmental prosopagnosia must deal with the perception that they are aloof and unsociable (35). Those with developmental topographagnosia may have to rely on the assistance of others when traveling even the mundane routes to work and home. For them, GPS technology is a godsend.
For acquired disorders, the prognosis depends on the nature and extent of the pathology causing agnosia. Rapidly reversible causes include migraine, whereas slower remissions can occur with posterior reversible encephalopathy syndrome. Those who suffer a stroke may have partial recovery, depending on the size of the lesion and whether there are bilateral lesions. On the other hand, those with carbon monoxide poisoning, herpes encephalitis, or iatrogenic deficits after temporal lobectomy often have a persistent deficit. Unrelenting slow deterioration is the rule with posterior cortical atrophy, a right-dominant form of frontotemporal degeneration, or the Heidenhain variant of prion disease.
General visual (form) agnosia. A 60-year-old woman began to have visual symptoms 3 years prior to assessment. She had trouble reading, but she was able to write. This deficit evolved into problems recognizing the faces of her friends, and she had to rely on their voices to identify them. She could not locate objects in the refrigerator or on the kitchen counter. She began to have problems finding her way around and required an escort on her visits to the clinic.
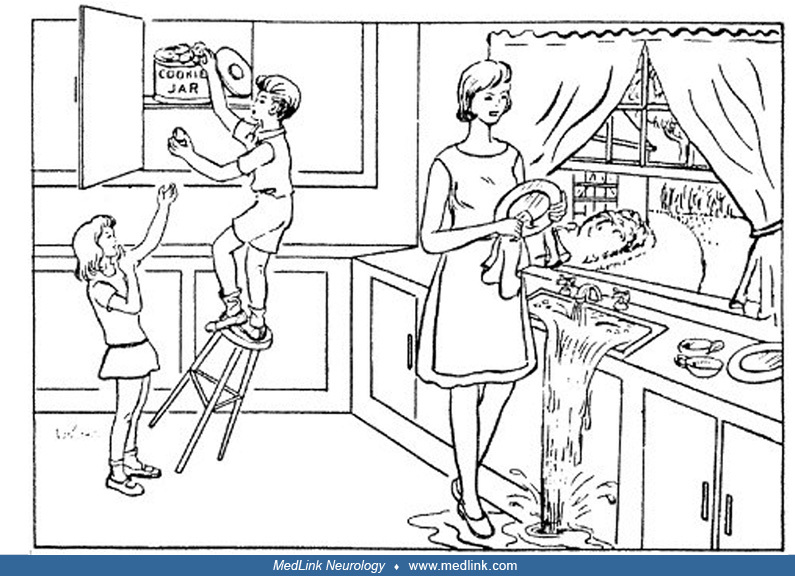
Acuity for single letters was 20/25. Visual fields were full on Goldmann perimetry. Eye movements were normal. Identifying objects in line drawings was slow, and she tended to report just small details: she could not name a hand, saw only the “O” in the handle of a key, called a feather a “leaf,” identified “grass…something to sit on” for a picture of a chair, and said that a cactus was “faces.” She correctly but slowly identified simple two-dimensional shapes such as squares, circles, and triangles but had trouble with three-dimensional shapes, saying for a cube, “all these angles, octagon,” and for a pyramid “triangles in it, a tent.” After viewing the standard Cookie theft picture, she reported only “a woman washing dishes, something spilling,” and showed perseveration, “two women with aprons.” She said it “must be a restaurant.” Copying or drawing of a flower from memory was disorganized.
Neuropsychological tests showed normal general knowledge, expressive vocabulary, and comprehension. Digit span was 6 forward and 4 backward. Reading proceeded by deciphering one letter at a time. She could write to dictation, with only occasional spelling errors. She performed in the average range on tests of auditory and verbal learning and memory. Abstract verbal reasoning was average to superior. In contrast, she was severely impaired on all visual tasks. She had difficulty with line bisection, line cancellation, and visual search. Her accuracy was only 20% on the Benton Line Orientation Test. She was poor at discriminating the shape of triangles. She was severely impaired on the Boston Naming Test. On a famous faces test, her score was only 0.12. On the other hand, her imagery for famous faces was nearly normal.
A technetium scan showed marked hypoperfusion of the posterior parietal and temporal lobes. CT scan 6 years after onset showed occipital gyral thinning, consistent with posterior cortical atrophy. An experimental study of her scanning of scenes showed that, when given a task, she did not look at the most relevant areas of a scene but, rather, at areas of brightness, color, or contrast that attract attention (55).
Ventral visual syndrome. A 41-year-old man awoke one day with distortions in his left visual field. In the emergency department, a CT scan showed a left posterior cerebral artery infarct and a filling defect in the right vertebral artery. He was treated with intravenous TPA. Later that night, he had a second stroke involving the right thalamus and distal posterior cerebral arterial territory. Subsequently, he noted many visual problems, with some gradual improvement over months. He had trouble recognizing faces, seeing their shapes, and identifying the ethnicity or age of faces. Everyone appeared good-looking. He recognized people by their voices, clothes, body posture, facial moles, or hairstyles. He could not visualize the faces of people when he heard their names. The world appeared black and white. Although he was starting to see more tint, he still struggled with distinguishing similar colors, such as telling blue from green. He had trouble finding his way around his neighborhood. He could not follow a short but complicated route to the supermarket across the street, which he had used for years. He could not recognize buildings, as they all looked like a “bunch of squares.” Although he was a sports car enthusiast, all cars now looked the same. However, he did not make gross errors in distinguishing one type of object from another. Reading was slow. Examination showed normal visual acuity but homonymous superior altitudinal defects. He correctly identified objects in line drawings as well as two-dimensional shapes and letters. Reading showed a mild word-length effect. Drawings of objects were accurate. Color discrimination was poor on the Farnsworth-Munsell 100-hue test- (he is subject B-IOT1 in the study by Moroz and colleagues) (99). Neuropsychological testing showed normal IQ and attention. He had mild difficulties with verbal and visual memory. Visuospatial perception was intact. On the Warrington Recognition Memory test, he scored well for recalling words (47/50), but poorly for remembering faces (28/50). He had a low score on the Cambridge Face Memory Test and identified fewer than half of Famous Faces. This man presents a classic example of the ventral visual syndrome from bilateral occipitotemporal infarcts. He had prosopagnosia, topographic disorientation with landmark agnosia, dyschromatopsia, and homonymous superior field defects.
Pure alexia. A 41-year-old mechanical engineer who owned an automotive repair shop awoke with numbness of the right face and leg 1 week after an airplane trip. MRI showed a left occipital stroke, eventually attributed to paradoxical emboli through a patent foramen ovale. Angiography showed a fetal pattern, with the posterior cerebral artery originating from the carotid circulation. His memory for events was poor initially but quickly returned to normal. He had experienced trouble naming objects, but this too was now normal. His right-sided numbness recovered quickly, but he had a single generalized seizure a few months later and was started on levetiracetam. His persistent symptoms included trouble seeing to the right, and he had learned to stop bumping into obstacles on that side when walking. His reading was very slow, proceeding one letter at a time. He could identify single letters and write well. His partner had researched rehabilitative reading strategies, and he had tried scrolling text and manually tracing letters with modest improvement.
He knew which faces were familiar but had trouble recalling the name or other information about the individuals. There was a right homonymous hemianopia. Neuropsychological testing showed some difficulties with verbal memory but normal performance on the visual object and space perception battery. On the Warrington Recognition Memory Test, he scored 37/50 for words and 44/50 for faces. His car recognition was superb. Measures of his reading of single words showed a markedly elevated word-length effect of 1.5 seconds per letter. He is subject CJ in a study by Sheldon and colleagues (111).
MRI scan showed a small stroke involving the left medial occipital lobe and fusiform gyrus. He was diagnosed with alexia without agraphia (pure alexia) and right homonymous hemianopia. Experimental studies showed that his problem with visual processing of language affected written words and the ability to lip-read from faces even though his ability to recognize the identity of faces was intact (03).
The ability to recognize objects is a complex process involving cerebral networks with multiple stages of visual processing. Three of the key challenges in research are: (1) understanding what each part of the network contributes to visual processing, (2) how the two hemispheres work together (the degree to which their contributions are redundant or complementary, and if the latter, in what way), and (3) how distinct these networks are for different types of objects.
After proceeding through the striate cortex and early occipital visual areas, such as V2 and V3, visual processing is distributed to a wide array of cortical regions. These pathways have been grouped into two broad streams (127). The first is the dorsal (occipitoparietal) stream, which is devoted to spatial and likely also temporal aspects of vision; hence, it is sometimes referred to as the “where” stream or one for preparing for action (96). The second is the ventral (occipitotemporal) stream, which is focused on object recognition. Both have an intermediate level of processing, with areas V5 and V5a involved in motion processing in the dorsal stream (135) and areas V4 and V4a performing color analysis in the ventral stream (136).
In the occipitotemporal stream, higher levels of processing are marked by responses to objects that are independent of the viewpoint from which the object is seen and the size of the object (64), as found in the lateral occipital complex (80; 121). The fusiform gyrus may be of particular importance in higher-level object recognition (133) and is likely a key structure for expert processes, such as word recognition (with a left hemispheric dominance) and face recognition (with a right hemispheric dominance).
Processing of any object involves not just one cortical region but a network of regions (17), which can be demonstrated with functional magnetic resonance imaging. Interestingly, the occipitotemporal cortex contains a recurring series of object-selective patches, with a parallel set for faces, places, and colors, processing from posterior to anterior (29; 04). In the anterior temporal lobes, these networks interact with memory and semantic representations along with information from other sensory modalities.
Form agnosia. Form agnosia is associated with widespread bilateral occipital lesions, particularly with damage of medial structures, such as the lingual gyri (79). It is especially likely to occur with more diffuse pathology, such as carbon monoxide poisoning, mercury poisoning, or anoxia (02; 18; 85; 24; 97).
Integrative agnosia. Integrative agnosia occurs with bilateral lesions of the lateral and inferior occipital cortex (81), most commonly from peri-striate infarcts or posterior cortical atrophy (73; 65). Damage to the right cerebral hemisphere alone can cause a milder version with prolonged reaction times for naming objects in line drawings (58).
Associative visual agnosias. For associative visual agnosias, knowledge of what objects look like may be stored in both hemispheres, perhaps with a greater “part-based” representation of features in the left hemisphere and more “whole-object” representations in the right hemisphere (51; 82). The lesions that cause associative visual agnosia may be related to anterior occipital and posterior temporal damage (105), possibly bilaterally. Loss of semantic knowledge about objects may occur when left-sided lesions disconnect posterior occipital areas from more anterior temporal areas (26) or involve the left parahippocampal, fusiform, and lingual gyri (54). In Alzheimer disease, neurofibrillary tangles in Brodmann areas 18, 19, and 37 are correlated with associative deficits in object recognition (61).
Prosopagnosia. Prosopagnosia is caused by right hemispheric or bilateral hemispheric lesions. There are rare cases with left-sided lesions, but some subjects were left-handed and may have had atypical hemispheric dominance (125; 92; 07), whereas others had subtle right-sided anomalies and perhaps should have been considered as having bilateral damage (134).
Functional magnetic resonance imaging studies show a network of face areas (69; 62), including the occipital face area, the fusiform face area, and the superior temporal sulcus, but there is also evidence for an anterior inferotemporal area (83; 124). Beyond this core network, an extended network, including the precuneus and inferior frontal gyrus, is sometimes activated by faces (69).
Lesions that cause the apperceptive variant of prosopagnosia are located in the inferior occipitotemporal cortex, with loss of the occipital face area, fusiform face area, or both, on the right or both sides (13; 108; 39). Lesions that cause the amnestic variant are located in the right or bilateral anterior temporal cortex. Some patients have both occipitotemporal and anterior temporal damage. In contrast, a lesion of the superior temporal sulcus may impair perception of facial expression but leave face identification relatively intact (56).
There is not yet a consensus about the structural basis of developmental prosopagnosia. These subjects do not have gross structural lesions on clinical scans. Some investigators have found decreased fusiform face area activation (67), but others have not (68; 06). Some investigators report decreased cortical thickness of the fusiform gyrus (57). Others have argued more for reduced connectivity or white matter damage either in the vicinity of the fusiform gyrus or in the inferior longitudinal fasciculus, which may carry connections between the occipitotemporal face areas and those in the anterior temporal cortex (63; 114; 115; 89; 137; 138).
Pure alexia. Pure alexia has two possible explanations. The first is that it is a disconnection syndrome (43; 59). A left occipital lesion may cause a complete right hemianopia so that left-hemispheric language processors are now dependent on visual input from the left hemifield, which is initially processed by the right striate cortex. Visual information from the right striate cortex must cross via callosal fibers in the splenium to reach language regions devoted to reading. However, reading is not possible if the left occipital lesion also damages these fibers, although writing is spared. In the rare cases without hemianopia, it is speculated that there is an intra-hemispheric disconnection as well (126; 70; 86).
Disconnection may well be the cause in some patients (47), particularly in those with unusual combinations of lesions of the splenium and right hemianopia from damage to the lateral geniculate nucleus (113; 117). However, in those cases with cortical damage that extends to the left fusiform gyrus, an alternate possibility is that the patient has a word form agnosia (132; 20), independent of whether or not there is also a right hemianopia.
Topographic disorientation. In right-handed normal subjects, the bilateral parahippocampal gyri and parieto-occipital junctions are involved in processing scene perception. In functional magnetic resonance imaging, the region activated during scene perception is known as the parahippocampal place area (48). Dysfunction of this region likely explains the association of right occipitotemporal damage with landmark agnosia (28). The parahippocampal place area is located just medial to the fusiform face area, so landmark agnosia is a frequent companion of prosopagnosia. Functional imaging during cognitive map formation shows hippocampus and retrosplenial cortex activation (77).
Beyond the parahippocampal place area, the occipitotemporal cortex has a series of cortical patches sensitive to places (05). More anterior temporal damage has also been associated with difficulty recognizing scenes (31). On the other hand, impaired cognitive map formation occurs mainly with right occipitotemporal lesions. Decreased activation of the hippocampus during cognitive map formation has been reported in at least one case of developmental topographic disorientation (76).
All acquired forms of visual agnosia are rare, but accurate incidence estimates are not available. Their rarity may reflect the necessity in many cases for bilateral lesions, with preservation of the optic radiations and striate cortex so that the patient is not rendered blind. It is also likely that these acquired forms have been under-recognized by both patients and clinicians.
Pure alexia may be the most common disorder of visual recognition, as it requires only a unilateral left occipitotemporal lesion. Although prosopagnosia can occur after a unilateral right occipitotemporal or anterior temporal lesion (40; 39), it appears in some cases to require bilateral lesions (49), perhaps reflecting variable degrees to which face processing is lateralized to the right.
Developmental conditions may be more common than acquired conditions. Developmental prosopagnosia reportedly has a prevalence of 2% to 3% (23). However, this estimate may simply reflect tautologic reasoning. If one diagnoses the condition when a subject’s score on a face recognition test falls two standard deviations below a group mean, a prevalence of 2% will be the result (12).
For general visual agnosia, the first important point is to ensure that the peripheral and especially the parafoveal visual field is intact. Widespread homonymous vision loss that leaves the patient with a very small central window of vision may give a picture of someone who has 20/20 acuity but cannot recognize objects. Patients with simultanagnosia can be misdiagnosed as having general visual agnosia, as there can be confusion between being aware of the presence of an object and being able to identify it. Anomia or word-finding problems can be confused with visual agnosia. Two observations are important to avoid this error: (1) anomia is usually not just a visual problem, and (2) patients with anomia, unlike patients with agnosia, can often describe or show recognition with gestures even if they cannot name an object.
Prosopagnosia should refer to impaired recognition of the identity of faces in the absence of a more general ophthalmologic or neurologic disorder. Patients with macular degeneration can have impaired face recognition (93) but should have decreased acuity as well. Impaired face recognition has been described as part of many neurodegenerative conditions, including Parkinson disease (34) and Alzheimer disease (95) and autism spectrum disorders (27; 11).
Most patients with pure alexia also have a right hemifield defect. The latter on its own can affect reading if it encroaches on the central 5 degrees. This deficit is called “hemianopic dyslexia” (139; 123). A macula-involving right hemianopia slows reading more than a left hemianopia in languages read from left to right because it limits a preview of the material coming after fixation. Hemianopic dyslexia has a modest word-length effect of at most 120 ms per letter, whereas it may reach 1 second or more per letter in pure alexia (111). Careful perimetry of the central 10 degrees can be critical to exclude a small homonymous paracentral scotoma from an infarct of the occipital pole when the rest of the visual field seems intact. This situation is sometimes inadvisedly called amblyopic dyslexia (66).
The visuospatial problems of Balint syndrome and hemineglect can cause afflicted patients to get lost. Careful assessment of visuospatial functions and spatial attention is needed to avoid confusing these conditions with topographic disorientation.
Disorders of object recognition often group into syndromes. The acquired forms cluster with other deficits based on anatomic proximity. Even if different objects and visual functions have different networks, they are located close to each other in the brain. This proximity is the basis of Balint syndrome, which can be considered a “dorsal visual syndrome,” comprising simultanagnosia, ocular motor apraxia, and optic ataxia. However, not all patients have the complete triad, and some have additional deficits in spatial or temporal aspects of visual processing (91).
A classic “ventral visual syndrome” is the association of an apperceptive variant of prosopagnosia with superior field deficits (94; 36), dyschromatopsia (99), and topographic disorientation from both place agnosia and impaired cognitive map formation (31). This combination is seen with either right or bilateral inferior occipitotemporal damage. When bilateral, there may also be an element of alexia.
Left inferior occipitotemporal lesions can cause pure alexia and impaired lip reading (03), with or without right hemianopia.
The anterior temporal lobe is a point where information from multiple sensory modalities converges. Bilateral or right-sided lesions here can cause an amnestic variant of prosopagnosia with phonagnosia, which is impaired recognition of the identity of voices, and amusia, also known as tone-deafness (88; 33).
As with all anatomic syndromes, patients need not have full manifestations of the syndrome, as this will depend on the extent of the damage.
Examination begins by first ensuring that the patient has adequate basic visual, cognitive, and memory functions.
Object recognition generally relies on central vision, so measures of visual acuity and the central 10 to 15 degrees of the visual field are needed. Snellen acuity may be confounding, as severe object recognition difficulties may affect the ability to recognize letters and numbers. If the patient cannot read the Snellen chart, one can resort to testing with the tumbling “E’s” or the orientation of gratings used to measure contrast sensitivity. Large central scotomas in both eyes will make object recognition difficult, as in patients with macular degeneration. These subjects may still be able to make coarse object identifications (“is this a horse or a car?”) using their peripheral vision but not finer ones (“whose face is this?”).
The Mini-Mental State Examination and Montreal Cognitive Assessment are helpful for assessing the patient’s cognition, but one may need a more detailed neuropsychological review. Patients with more general disorders of semantic knowledge may also have problems with identifying objects, but this deficit should not be limited to visual input. Hence, patients should be tested with auditory or other nonvisual material. General problems with memory can affect object recognition tasks that depend on the recall of previous encounters with a specific item (“do you know whose face this is?”).
General visual agnosia. A diagnostic impression for general visual agnosia can begin by showing the patient various items in the room and asking them to name the items, describe what they are, or mime how they are used. Identifying objects in line drawings may be more sensitive because they provide fewer visual cues than real objects. Difficulties on these tests should be compared to their ability to identify the same objects by hearing or touch. If the latter function is also impaired, patients have a multimodal problem rather than visual agnosia.
The type of general visual agnosia can be probed by first determining if patients can copy or identify simple shapes like squares, triangles, and circles. If not, they have a form agnosia (46; 98). Some patients with form agnosia can identify objects in drawings if they are allowed to trace their outline, translating a visual percept into a kinesthetic one (01; 85).
If patients can identify simple shapes, one then assesses whether they can identify the objects in an overlapping figures test, which is a good method of detecting integrative agnosia (73; 65). Patients with this type of visual agnosia also have trouble recognizing the impossibility of images like Escher drawings. To do so requires an appreciation that the local elements do not integrate into a correct three-dimensional structure (44).
To test for their knowledge of object structure, ask patients to describe what objects look like or to draw them from memory. Their visual access to semantic stores of object knowledge can be probed by showing them several objects and asking them which ones are related and which ones are not (“which is the odd one out?” of hammer, wrench, and egg-beater). In order to ensure that the problem is specific to vision, this performance should be compared to the ability to do the same task with the names of objects rather than pictures.
These bedside tests can be supplemented by other available neuropsychological batteries, which can also help with the distinction between associative and apperceptive types. The Visual Object and Space Perception Battery (VOSP) assesses various elements of object recognition and visuospatial perception (131). In contrast, the Birmingham Object Recognition Battery (BORB) assesses low-level, intermediate, and high-level processes in object recognition (107). Other useful tests include the Cortical Vision Screening Test (CORVIST) (104; 103) and the Leuven Perceptual Organization Screening Test (L-POST) (122).
Most of the processing used in general object perception should be relatively intact in patients with selective visual agnosias. One or more of the above tests should be done to establish that point before assessing more specific types of object recognition.
Prosopagnosia. Prosopagnosia can be assessed in the clinic by using the photo albums available on smartphones to assess whether faces appear familiar. Use of a friend or family member’s telephone is even better because the patient will be less familiar with those images, and there are likely to be more faces that they do not know. The friend or family member can confirm the accuracy of the patient’s response.
More formal testing can include the use of a Famous Faces test, with the proviso that the patient has seen the celebrities before. Poor familiarity with famous faces is contrasted with good recognition of famous names.
Otherwise, short-term familiarity for faces is often probed by tests that show the patients some faces in a learning phase and then ask them in a recall phase to indicate which of a larger set of faces are ones they had learned and which are not. This function can be probed with the Cambridge Face Memory Test (45) and the Warrington Recognition Memory Test (129). With the latter, poor performance on the face half of the test can be contrasted with better performance on the word half of the test. Ideally, the diagnosis of prosopagnosia should also require a demonstration of good familiarity for voices, but in most of us, voice recognition is not as accurate as face recognition, and we lack clinical tests for voice recognition.
With developmental prosopagnosia, it is also important to consider whether the subject has an autism spectrum disorder, as face processing can be impaired in this condition (128; 11; 78; 120).
Pure alexia. Pure alexia can be assessed at the bedside by reading single words and paragraphs in a magazine or book. One can get an impression of whether the patient takes longer with words that have more letters. An increased word-length effect is the diagnostic hallmark in those with retained but inefficient reading (14). If they cannot read words, assessing their reading of numbers and single letters can help determine the severity of the deficit (116).
Patients with pure alexia can write much better than they can read. However, some will have a “surface dysgraphia,” in that their ability to spell and write words with irregular spelling (eg, yacht, colonel) is impaired, implying a problem with accessing an internal lexicon (112). Patients with severe problems with both reading and writing have alexia with agraphia, which is a linguistic rather than a perceptual deficit. Speech and auditory comprehension should be tested to ensure that poor reading is not simply part of an aphasia.
More formal reading tests with normative values can be administered by neuropsychologists. Experimental word reading tests examine the word length effect (a perceptual variable, as the number of letters approximates how much visual processing is being done) while controlling for linguistic variables, such as the part of speech or how frequently the word is encountered in reading.
Landmark agnosia. Landmark agnosia is tested by assessing the patient’s ability to recognize scenes or buildings. A collection of scenic pictures in the clinic is handy. One can also upload images of famous landmarks (Taj Mahal, CN Tower, Eiffel tower, Niagara falls) from the internet, hoping that the patient has seen them before. Again, the photo library on a friend’s smartphone may be shown if they contain familiar places in their hometown.
Cognitive map formation. Testing cognitive map formation at the bedside is more challenging. One can ask patients to describe the route they took to the clinic from the front door of the hospital. If a family member is present to validate their answer, one can do the same for the route between two familiar places in their neighborhood. Ultimately, these impressions can be confirmed by formal testing, as with the online battery at www.gettinglost.ca. It can test place recognition, cognitive map formation in a virtual environment, and other navigational skills.
• Strategic adaptations to help the patient with impaired object recognition in daily life involve greater emphasis on tactile or auditory cues or visual cues that are not affected by their disorder. | |
• Various types of computer software can also augment the function of these patients by substituting for their deficient skills. |
In the absence of effective therapies, substitutive strategies may help patients with visual agnosia adapt to their deficit.
An occupational therapist with an interest in visual disorders can help patients learn strategies to live with general visual agnosia. They should be encouraged to use tactile and auditory cues about objects. The value of putting verbal labels on items in their environment depends on the extent to which reading is spared. Organizing the location of items in their world can help by making their search more predictable and limiting the number of possible answers to the question, “what objects could be in this place?”. Although there are no formal driving rules in most jurisdictions for this rare problem, afflicted patients should be advised not to drive.
Patients with prosopagnosia often benefit from knowing beforehand which individuals will be present in a room in order to narrow the choices. Many patients will learn to wait until the other person talks so that they can identify them by their voice. Explaining their deficit to others can help avoid unpleasant social misinterpretations. Nametags can be helpful in the right setting. Ultimately, mobile devices with face recognition software could prove handy.
The widespread availability of devices with GPS capability has made route-finding much easier for patients with topographic disorientation, although navigating inside buildings may still be difficult.
For alexia, substitutive strategies include audiobooks and free text-to-speech translators on the internet.
There is no clinical consensus on effective treatment of visual agnosias. For general visual agnosia, the efficacy of restorative approaches tried so far is limited (71).
There is a long history of case reports describing attempts to improve face recognition in prosopagnosia (15; 42; 38). More recently, studies involving small cohorts of patients with developmental or acquired prosopagnosia have shown that perceptual learning can lead to modest improvements in the perception of the shape of faces (41; 38; 32). Only anecdotal evidence supports the notion that this finding translates into benefit in daily life. One trial found benefit with oxytocin treatment (15).
None of the treatments used for pure alexia has been accepted as a standard of care. none of which have become standard of care. They include increasing the spacing between words or phrases (16; 90), oral articulation during reading (30), repetitive oral reading of text (16), and finger tracing of letters (90; 101).
Extremely little is known about therapies for topographic disorientation. Over-learning of familiar routes may help the navigation of some patients in daily life, although this ability may not generalize to new situations.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Jason J S Barton MD PhD FRCPC
Dr. Barton of the University of British Columbia has no relevant financial relationships to disclose.
See Profile
Jonathan D Trobe MD
Dr. Trobe of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Behavioral & Cognitive Disorders
Apr. 17, 2024
Neuroimmunology
Mar. 24, 2024
Infectious Disorders
Mar. 24, 2024
Stroke & Vascular Disorders
Mar. 21, 2024
General Neurology
Mar. 18, 2024
General Neurology
Mar. 14, 2024
Behavioral & Cognitive Disorders
Mar. 07, 2024
Behavioral & Cognitive Disorders
Mar. 07, 2024