






































General Neurology
Dysphagia
Mar. 18, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
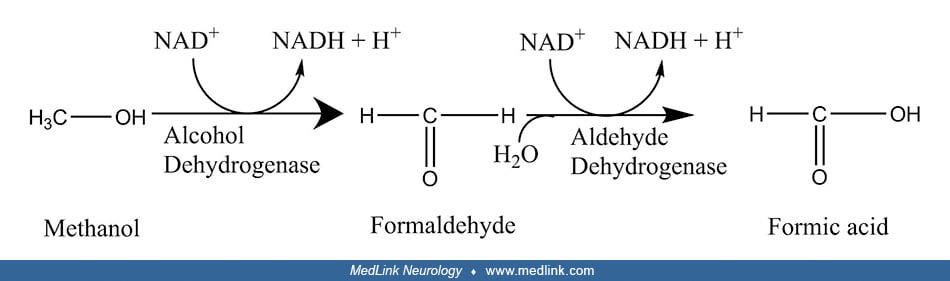
Methanol poisoning first became a clinical problem at the end of the 19th century when changes in manufacturing markedly increased the availability of methanol. By the early 20th century, methanol was recognized as an increasingly common cause of permanent blindness, metabolic acidosis, and death. The number of cases increased dramatically with Prohibition in the United States from 1920 to 1933. Methanol poisoning is now recognized as a cause of high-anion-gap metabolic acidosis, toxic blindness due to apoptosis of retinal ganglion cells and retrobulbar demyelination of the optic nerve, coma, seizures, and death. The toxicity of methanol is due to the toxicity of its metabolites, particularly formic acid. Morbidity and mortality can often be averted by blocking the metabolism of methanol by inhibiting alcohol dehydrogenase with ethanol or fomepizole and by facilitating the elimination of methanol and its toxic metabolites with hemodialysis.
|
• Methanol poisoning first became a clinical problem at the end of the 19th century when changes in manufacturing markedly increased the availability of methanol. | |
|
• By the early 20th century, methanol was recognized as an increasingly common cause of permanent blindness, metabolic acidosis, and death. | |
|
• The number of cases of methanol poisoning increased dramatically with Prohibition in the United States from 1920 to 1933. | |
|
• Methanol poisoning is now recognized as a cause of high-anion-gap metabolic acidosis, toxic blindness due to apoptosis of retinal ganglion cells and retrobulbar demyelination of the optic nerve, coma, seizures, and death. | |
|
• The toxicity of methanol is due to the toxicity of its metabolites, particularly formic acid. | |
|
• Morbidity and mortality can often be averted by blocking the metabolism of methanol by inhibiting alcohol dehydrogenase with ethanol or fomepizole and by facilitating the elimination of methanol and its toxic metabolites with hemodialysis. |
Poisoning with methanol was very rare in the United States before around 1890, at which period cheap methods of producing pure methanol were discovered (133). Through a process called "destructive distillation," wood chips and slabs of wood were put into a closed container and heated to at least 400° F (204° C). The natural liquids in the wood vaporized as the wood cooked into charcoal. The vapor was then distilled into a murky and unpleasant-smelling soup containing methyl alcohol, acetone, acetic acid, and various impurities. A second distillation could separate the pure methanol as a clear liquid. Methanol naturally became known as "wood alcohol" because of its source as a distillate from wood chips.
As early as 1904, Canadian-American ophthalmologist Casey Albert Wood (1856-1942) and Canadian ophthalmologist Frank Buller (1844-1905) collected 275 cases of methanol poisoning, including 153 cases of blindness and 122 deaths due to the consumption of methanol (wood alcohol) or the inhalation of its vapor (25; 25). As they then recognized, methanol was untaxed and retailed for 50 cents a gallon compared to ethanol, which was taxed and had a retail price of $2.60 a gallon, more than five times as much as methanol.
Wood and Buller categorized poisoning cases into three levels of severity:
|
1. Mild intoxication, with variable dizziness, nausea, and mild gastrointestinal disturbance, which resolved within a few days but was occasionally followed by visual impairment. | |
|
2. Moderate poisoning, with conspicuous dizziness, nausea, vomiting, gastroenteritis, and headache associated with dimness of vision, often increasing to total blindness. | |
|
3. Severe poisoning, with "an overwhelming prostration, which terminates in coma and death" (25). |
Wood and Buller recognized that in many cases there was a lag or delay of 24 hours or longer before the onset of the neurotoxic manifestations. In the more severe cases, patients often developed sudden blindness or near blindness, with widely dilated, reactionless pupils, typically in association with slow respiration, weak pulse, diaphoresis, or delirium and often passing into coma and death. Patients who became comatose rarely, if ever, recovered.
In non-fatal cases of severe poisoning, the course of visual symptoms was multiphasic. Within a few hours to several days of methanol exposure, patients developed bilateral, total blindness followed by a partial restoration of vision and then over a few days to weeks developed into complete and permanent blindness with optic atrophy (25). "It is a picture which methyl alcohol [methanol] alone can create" (25).
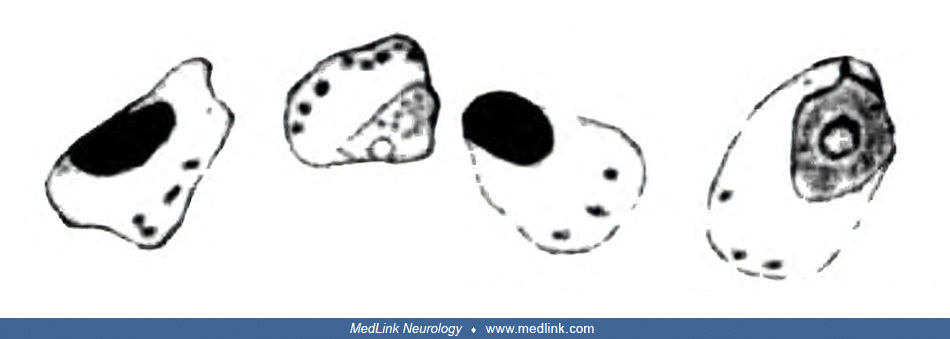
In 1912, German neuropathologists Ludwig Pick (1868-1944) and German Max Bielschowsky (1869-1940) were the first to report considerable pathological changes in the retinal ganglion cells and the optic nerve (125).
Retinal ganglion cells showed pathological changes that would now be recognized as those of chromatolysis, characterized by the loss or dispersion of the Nissl bodies starting near the nucleus and displacement of the nucleus towards the periphery of the perikaryon.
Sketches of a normal large retinal ganglion cell (left) and one undergoing chromatolysis in association with methanol poisoning (right). (From: Pick L, Bielschowsky M. Über histologische Befunde im Auge und im Zentralnervensyst...
Sketch of a group of severely altered retinal ganglion cells of the small type that are undergoing chromatolysis in association with methanol poisoning. Nissl stain. (From: Pick L, Bielschowsky M. Über histologische Befunde im ...
Sketch of a longitudinal section from the retrobulbar part of the optic nerve following methanol poisoning showing accumulations of "granular detritus between two blood vessels." Bielschowsky silver stain. (From: Pick L, Bielsc...
In 1913, Charles Baskerville (1870-1922), Professor of Chemistry and Director of the Laboratory in the College of the City of New York, published a detailed study: “Wood Alcohol: A Report on the Chemistry, Technology, and Pharmacology of and the Legislation Pertaining to Methyl Alcohol” (13).
Of the 720 cases of methanol poisoning due to ingestion that were identified in the report, 390 (54%) died, 90 became totally blind, 85 were left with visual impairment, 6 to 10 had temporary blindness, 31 recovered, and about 114 did not have associated outcome data. If the cases lacking outcome data are excluded, approximately two of every three cases died (64%), and most of the remainder were left blind or with some degree of visual impairment (29%). Another 64 cases of methanol poisoning were identified to be due to inhalation exposure, of which six died, 14 became and remained totally blind, 30 had partial blindness (some of which were totally blind but then recovered some vision), two had temporary visual impairment that resolved, seven had eye irritation, and four had other or unknown reactions. The better outcomes from inhalation exposures likely reflect the smaller doses received.
In the late 19th and early 20th centuries, some methanol was present in patent medicines, including Lash’s Bitters (168). In 1905, American journalist and muckraker Samuel Hopkins Adams (1871-1958) published an 11-part exposé of the patent medicine fraud, "The Great American Fraud," in Collier's magazine. An advertisement for this exposé shows Death titrating a mixture of wood alcohol (methanol) and laudanum (tincture of opium).
December 1905 advertisement for Collier's magazine's exposé of the patent medicine fraud, culminating in Samuel Hopkins Adams' 11-part series, "The Great American Fraud." (Illustration by American illustrator Edward Wi...
One famous patent medicine peddler from that era was Lydia Pinkham, who sold an herbal-alcoholic "women's tonic" containing 18% alcohol (36 proof) for menstrual and menopausal problems. Cartoons of the era showing Mrs. Pinkham serving her concoction also show signs for the product juxtaposed with bottles of wood alcohol (methanol).
Lydia Pinkham (1819-1883) was born into a prominent Quaker family in Lynn, Massachusetts. The economic recession of the 1870s forced Lydia to be enterprising, and she and her family made and marketed an herbal-alcoholic "women'...
Enlarged detail. To the left of the sign for "Lydia Blinkham's on draught - October brew" (on the right end of the second shelf) is a bottle of wood alcohol (methanol). It is unclear if Pinkham used some methanol in "Lydia E. P...
Starting in 1906, the United States government started adding toxic chemicals to industrial alcohol so it could be used for industrial purposes without the associated tax applied to ethanolic beverages meant for human consumption. During Prohibition in the United States--the period of the nationwide constitutional ban on the production, importation, transportation, and sale of alcoholic beverages from 1920 to 1933--the U.S. government intentionally adulterated industrial ethanol with methanol and other toxic chemicals as a deterrent to its misdirection for alcohol consumption. Given the continued high public demand for alcohol, speakeasies (illicit establishments selling alcoholic beverages) and organized crime syndicates flourished with bootleg liquor, and patrons invented novel ways of hiding bootleg liquor on their person (eg, hiding hip flasks in their garters or boots).
Photo taken in Washington DC on January 21, 1922. The significance of the swastikas in the floor tiles is unclear but was probably unrelated to German "National Socialism." Long before swastikas were misappropriated by Adolf Hi...
Some of the bootleg liquor was smuggled from the Caribbean (eg, rum runners) and other countries by ship, along the border with Canada by motorized vehicles, or by individual sailors, including U.S. military personnel.
Prohibition agents amid cases of scotch whiskey in hold of "rum runner" captured by the Coast Guard cutter USS Seneca, circa 1924. (Courtesy of the Library of Congress Prints and Photographs Division, Washington, DC. Image edit...
The nurses were photographed with their two attorneys at the Washington Navy Yard on June 17, 1925. (Courtesy of the Library of Congress Prints and Photographs Division, Washington, DC. Image edited by Dr. Douglas J Lanska.)
Some bootleg liquor was manufactured illegally (moonshine), but most--comprising tens of millions of gallons--was distilled from denatured industrial alcohol that had been stolen and diverted from its original purpose. Unfortunately, distillation generally failed to remove the much more poisonous methanol from the ethanol.
Both federal and local governments struggled to enforce Prohibition; enforcement was initially assigned to the Internal Revenue Service but was later transferred to the Justice Department and the Prohibition Bureau.
New York City Deputy Police Commissioner John A Leach (second from right), watching agents pour liquor into a sewer following a raid during the height of Prohibition. New York World-Telegram and the Sun Newspaper Photograph Col...
Unfortunately, the high demand for black market alcohol also led to the distribution of the toxic bootleg liquor--denatured industrial alcohol. In addition, some saloonkeepers intentionally adulterated bootleg ethanol with much cheaper methanol. The result, predictably, was a sharp upturn in the number of deaths and cases of permanent blindness due to methanol.
In response to the problem of bootleg liquor, in 1926 President Calvin Coolidge (1872-1933) authorized a marked increase in the amount of methanol added to industrial alcohol, to the point where the methanol content was as high as 10% of the final product, knowing that this would significantly increase the number of cases of methanol poisoning. Predictably, this change resulted in an ongoing disaster of blindness and death caused by methanol poisoning throughout the Prohibition Era.
By 1926, 750 New Yorkers perished from such poisoning, and hundreds of thousands more suffered irreversible blindness and other neurologic impairment. Of the half a million gallons of liquor confiscated in New York in 1927, nearly all contained methanol and other poisons. Other people were poisoned by drinking straight industrial methanol, which was legal but extremely dangerous, though from newspaper reports at the time most of the victims had been unaware of the dangers. By the end of the Prohibition Era, an estimated 10,000 United States citizens were killed by methanol poisoning.
Beginning in the early 1920s, likely with the increase in case material, several investigators recognized the association of methanol poisoning with metabolic acidosis (61; 62; 127). In one case, successfully treated with sodium bicarbonate, there was a marked increase in the urinary excretion of lactic and formic acids (61).
Despite the reports from Wood and Buller (25; 25), and the subsequent flood of cases during the Prohibition Era, many others discounted the toxicity of methanol and attributed the observed adverse effects to impurities in the methanol rather than to methanol itself (07; 08; 133). Toxicity of pure methanol was not proven until a poisoning outbreak in Hamburg in 1922, when chemical-grade methanol (98.5% methanol, 1.4% water, 0.1% impurities, mostly formaldehyde) was shipped from New York for use in chemical manufacturing but was instead consumed by dockworkers (130).
In the 1940s, ethanol was found to be a competitive inhibitor of methanol oxidation by alcohol dehydrogenase, which led to ethanol as a therapy for acute methanol intoxication (178; 04). Early administration of ethanol could retard the oxidative metabolism of methanol and prevent the accumulation of toxic metabolites, particularly formate.
By 1960, experiments with dogs had shown that hemodialysis could quickly and effectively lower levels of methanol (104). Since then, there has been a back-and-forth debate about the relative merits and timing of inhibitors of alcohol dehydrogenase and dialysis, but it is clear that some combination of both is needed for severe methanol poisoning.
In 1963, Theorell and Yonetani found that pyrazole inhibits the action of horse liver alcohol dehydrogenase in vitro by forming a complex with alcohol dehydrogenase and NAD+ (158), a finding that was soon applied to various studies of the mechanisms of ethanol- and methanol-related toxicities (158; 91; 21; 19; 102; 126; 20). In1970, Blomstrand and Theorell reported the use of 4-methylpyrazole in studies of ethanol oxidation in humans. Blomstrand further suggested as early as 1970 that 4-methylpyrazole might be useful in treating methanol poisoning (19; 20). By 1979, Blomstrand and colleagues showed that 4-methylpyrazole produced a profound inhibition of methanol oxidation and, thus, prevented accumulation of the toxic metabolite formic acid in methanol-poisoned monkeys (20). 4-methylpyrazole was named fomepizole (trade name Antizole) and was ultimately approved by the U.S. Food and Drug Administration in 2000. The clinical trial that led to FDA approval of fomepizole for that indication was published in 2001 (23). Fomepizole is now on the World Health Organization List of Essential Medicines in category 4.2 Specific Antidotes and Other Substances Used in Poisonings (170).
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125