






Behavioral & Cognitive Disorders
Academic underachievement
Apr. 18, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Cryptococcal meningitis is the most common form of meningitis observed in AIDS, affecting 1% to 10% of patients; conversely, HIV is the greatest risk factor for cryptococcal infection. Other immunosuppressive conditions also predispose to its development, such as corticosteroid administration; however, it may also be seen in immunologically normal persons. Cryptococcal meningitis may be difficult to diagnose as its clinical features are often subtle. Headache is the most common symptom, but it is not universally present, and papilledema occurs in less than one third of persons. On occasion, cryptococcal infection of the CNS presents as mass lesion in the brain (cyst, granuloma, or abscess) or as encephalitis. The toxicity of the antifungal drugs, particularly amphotericin, may render treatment difficult. In the AIDS population, long-term prophylaxis may be required.
|
• Cryptococcal meningitis is the most common fungal meningitis and needs to be considered in the differential diagnosis of anyone with unexplained meningitis. | |
|
• Although meningitis is the most common neurologic manifestation of cryptococcal infection, CNS mass lesions and vascular insults may also occur. | |
|
• Cranial imaging studies either with CT scan or MRI in patients with cryptococcal meningitis may be unrevealing. | |
|
• CSF cryptococcal antigen studies are typically, but not invariably, positive in cryptococcal meningitis. |
Human cryptococcal infection was first described during the last decade of the 19th century. Busse, a pathologist, and Buschke, a surgeon, separately reported the isolation of yeast from the tibia of a young woman (18; 17). In 1905 the yeast was identified as a CNS pathogen when von Hansemann described the first case of cryptococcal meningitis (69).
Several different terms have been applied to the fungus currently referred to as Cryptococcus neoformans. Familiarity with these terms is helpful in reading the older literature. Busse employed the term “Saccharomyces hominis” because of the sarcoma-like appearance of the patient’s lesions (18). The fungus was transferred to the genus Cryptococcus by Vuillemin because of the absence of ascospores (175). Subsequently, the term “neoformans” was included to indicate “cancer or tumor-causing” in light of an association between the isolation of the organism and cancers. In 1916 Stoddard and Cutler distinguished between cryptococcus, blastomyces, and other mycoses (161). They named Cryptococcus “Torula histolytica” because of the mistaken belief that the cysts observed in tissues were the consequence of digestive actions of the organism. However, this term is no longer in use.
|
• Cryptococcal meningitis typically evolves in a subacute fashion. | |
|
• Headache and fever are the most common manifestations but are not invariable. | |
|
• Altered mental status and transient visual loss may occur. | |
|
• Features suggesting meningeal irritation are observed in only a minority of patients. |
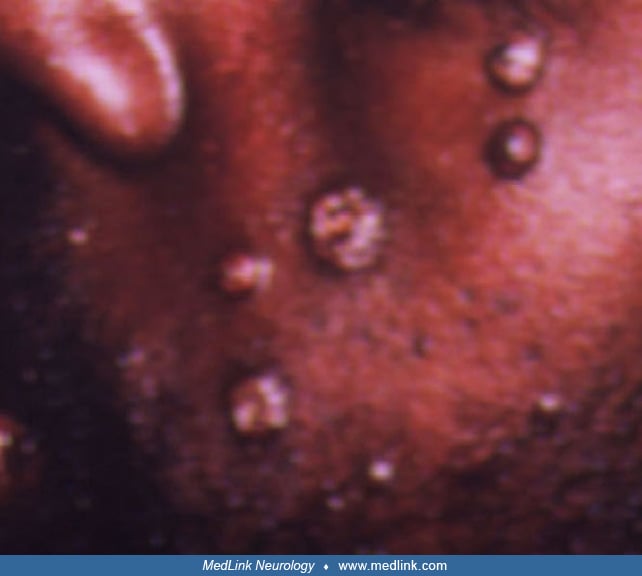
Cryptococcus may present with several different clinical patterns. Often, the infection is subclinical. It appears that exposure to C neoformans and subsequent sensitization without the appearance of clinical illness is not uncommon. Organs that may be sites of clinically apparent infection most commonly include the lung, CNS, skin, bone, and prostate, but others may be affected as well. Simultaneous dissemination to multiple sites may be observed. For instance, AIDS patients with overwhelming immunosuppression and cryptococcal meningitis have been described with skin lesions due to C neoformans (103). Some of these lesions may mimic molluscum contagiosum (103).
Cryptococcal meningitis is estimated to account for 40% to 86% of the estimated cases of symptomatic cryptococcal infection. The frequency of disseminated infection in the setting of cryptococcal meningitis is highlighted by the occurrence of abnormal chest radiograph opacities compatible with cryptococcal lung infections in 25% of patients with cryptococcal meningitis (70) and by the relatively high frequency with which the organism can be isolated from blood. The clinical presentation of cryptococcal meningitis appears similar in both immunocompetent and immunocompromised persons (86).
Cryptococcal meningitis generally progresses slowly; it is seldom explosive in onset. Patients with cryptococcal meningitis most commonly complain of headache, usually frontal or temporal in location. Headache is not invariable, and the combination of headache and fever occur together in only 67% to 82% of some large series of AIDS patients with cryptococcal meningitis. However, a study of nearly 300 HIV-infected persons with cryptococcal meningitis found that headache occurred in 99% (44). Neck stiffness was observed in approximately 70%. Mental status changes and alterations of level of consciousness are frequent. Nausea or emesis is present in about 45% of cases, whereas photophobia and features of meningeal irritation are remarkably uncommon for meningitis in general, occurring in less than a third of cases. Seizures occur in 4% to 18%, and cognitive impairment or alterations in sensorium occur in 17% to 24%. Episodes of transient loss of consciousness may be the heralding symptom (181). Cranial neuropathies are seen in up to 15%. Focal neurologic deficits occur in 5% to 15% of cases. Dizziness, cerebellar ataxia, and syncope have also been noted as presenting features (87; 191; 34; 35; 138). Mesencephalic abscesses complicating cryptococcal meningitis have resulted in a clinical presentation mimicking Parkinson disease (14). Myelopathy with an acute flaccid paraplegia and polyneuroradiculopathy may also complicate cryptococcal meningitis on rare occasion (39).
Visual symptoms may occur in up to 21% of cases and neuro-ophthalmic findings in up to 33% (72; 138). Impaired visual acuity may be the presenting manifestation in some patients (117). Visual symptoms may include transient, abrupt, or progressive loss of visual acuity in one or both eyes due to increased intracranial pressure (49), necrotizing optic neuropathy from cryptococcal infiltration (116; 36), or compression of the optic nerve with vascular compromise (98). Diplopia may be intermittent or persistent and may be associated with cranial neuropathies, skew deviation, internuclear ophthalmoplegia, and nystagmus (60; 83; 84; 58; 141). Papilledema occurs in 1.5% to 12% of cases (72; 138). Visual field deficits may be homonymous, bitemporal, or altitudinal (60; 66; 63). Visual symptoms may be the first indication of recurrent cryptococcal meningitis in AIDS patients on maintenance antibiotic therapy (66). Involvement of vestibulocochlear nerve may result in vertigo and hearing loss (132).
Psychiatric symptoms may also be presenting features of cryptococcal meningitis. Psychosis (35) and behavioral changes (139) have been noted. Mania as an isolated presenting symptom has been described in two patients, one of whom responded to successful therapy of his meningitis with complete resolution of the manic syndrome (78). In some cases, no signs of neurologic disease are present, and diagnosis arises during the evaluation of systemic symptoms (191; 138).
Analogous to the immune reconstitution inflammatory syndrome (IRIS) that occurs following the administration of highly active antiretroviral therapy in HIV-infected patients with tuberculosis and progressive multifocal leukoencephalopathy, a similar disorder may be observed in cryptococcal infection (76). IRIS typically occurs within three months of the initiation of highly active antiretroviral therapy (16). IRIS takes two forms, “paradoxical” cryptococcal IRIS is a worsening of symptoms that occurs in individuals with established disease, and “unmasking” cryptococcal IRIS is the unexpected development of de novo cryptococcal meningitis following the initiation of antiretroviral therapy (115). Distinguishing IRIS from recurrent disease may be difficult (115). In a review of the disorder, 13% of 101 AIDS patients with cryptococcal meningitis receiving HAART developed IRIS (163); an increased baseline serum cryptococcal antigen was a risk factor. In another review, the median CD4 count at the time of diagnosis of cryptococcal meningitis was 25 cell/ml and at the time of IRIS 197 cells/ml (153). The underlying illness, eg, cryptococcal meningitis, may be inapparent until brought to light by the restoration of an effective immune response (16). The development of increased intracranial pressure in HIV-infected patients being treated for cryptococcal meningitis may be the consequence of IRIS (76; 184). Death ensues in up to one third of all patients with cryptococcal meningitis IRIS (149). A disorder characterized by clinical worsening following the initiation of treatment in immunologically young individuals has also been reported and referred to as postinfectious inflammatory response syndrome (PIIRS) (157). In one study, it was observed in 29% of immunocompetent individuals less than 50 years of age with cryptococcal meningitis (157).
|
• A worse prognosis is associated with extremes of age, underlying disease (particularly HIV infection), extracerebral cryptococcosis, and high CSF pressure among other factors. |
Factors associated with relapse are difficult to distinguish from those associated with poor survival. In general, the relapse rate and prognosis with cryptococcal meningitis appears to be variable. Survival has been reported in the range of days to more than 20 years in untreated cases. Among the factors that have been associated with relapse of cryptococcal meningitis following treatment are immunosuppression, neurologic manifestations at presentation, CSF leukocyte counts less than 20 cells/cu mm, CSF antigen titers greater than 1:32, positive CSF India ink studies following four weeks of treatment, and CSF antigen titers that exceed 1:8 after four weeks of treatment (166). These factors should be considered general rules as considerable disparity exists between the studies exploring prognosis in cryptococcal meningitis. Often confounding factors were not addressed. In a study in which potential confounds were examined, only the initial level of consciousness and CSF antigen titer were strongly associated with therapeutic failure (100).
Factors associated with a poor prognosis vary from study to study. An overall poor prognosis in cryptococcal meningitis has been associated with the following factors: young age (30); advanced age (170); abrupt onset (30); seizures (185); coma (185; 81); prolonged course over six weeks (30); extracerebral cryptococcosis (30); cryptococcemia (04; 146; 81); underlying illnesses (30), including HIV infection (170); corticosteroid administration (30); Cushing syndrome (48; 88); long-term antibiotics (30); high CSF pressure (30); and low CSF cells count (often neutrophilic leukocytes) (30). A study of mortality in cryptococcal meningitis unassociated with AIDS found lymphoma, semi-coma, leukocytosis, and initial high titers of cryptococcal antigen in cerebrospinal fluid (especially greater than or equal to 1:512) to be the best correlates and, on multivariate analysis, determined that lymphoma and initial high cryptococcal antigen titers were independent predictors of mortality (150). In HIV infection, significant prognostic factors include low CSF glucose; CSF with less than 20 cells/cu mm (139); high CSF lactate; high CSF cryptococcal antigen titer (greater than or equal to 1:1024) (191; 139); positive cultures of extrameningeal specimens (34); initial level of consciousness; the presence of seizure, hydrocephalus, and central nervous system vasculitis (100); neurologic impairment on initiation of therapy (35; 139); abnormal CT scan (35); and hyponatremia. A study of 501 HIV-infected patients with cryptococcal meningitis from four resource-poor countries demonstrated that CSF fungal burden, altered mental status, and rate of clearing of the infection were good predictors of acute mortality (73). In an HIV-infected cohort, measurement of CSF cytokines, chemokines, and macrophage activation markers demonstrated that interleukin (IL)-6 and interferon-gamma were most predictive of prognosis, although others, such as, IL4, IL-10, and IL-17, also contributed modestly (74). Three-year mortality in cryptococcal meningitis in one study correlated, after multivariate adjustment, with severe hyperglycemia (≥ 200 mg/dL) (170).
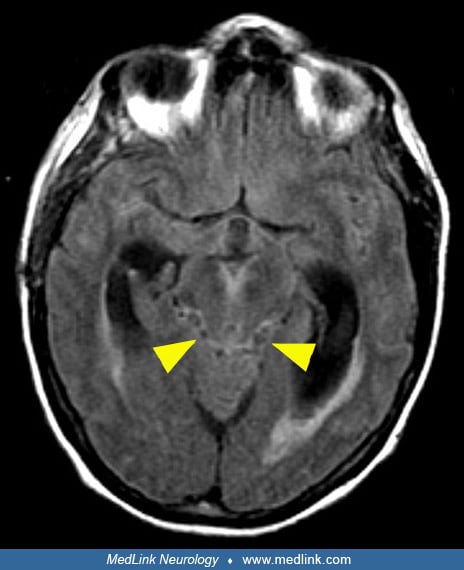
A 52-year-old woman presented to the emergency department with altered mental status. She had been diagnosed with AIDS nine months earlier when she presented with oral thrush, weight loss, and wasting. At that time her CD4 count was 4 cells/cu mm. She was started on combined antiretroviral therapy but stopped it three months before presentation. On examination, she was afebrile with a supple neck. She was unable to follow simple commands or answer questions. She withdrew all limbs to pain and exhibited normal limb strength and tone. Muscle stretch reflexes were symmetric and 1+ and bilateral Babinskis were noted. Laboratory studies showed a slight leukocytosis at 12,100 cells/cu mm with normal differential. Serum sodium was 124 mEq/L. Drug screen was negative, and she failed to respond to D50 or naloxone. A CT scan was negative, but cranial MRI revealed hyperintense signal abnormalities on T2-weighted image and FLAIR in the midbrain, thalamus, and left internal capsule.
Leptomeningeal enhancement that predominated around the brainstem was observed. Diffusion-weighted imaging and apparent diffusion coefficient mapping in these regions was consistent with acute infarction.
CSF examination showed 58 WBCs/cu mm (79% lymphocytes, 4% monocytes, and 17% polymorphonuclear cells), CSF/serum glucose of 19/82 mg/dL, protein 98 mg/dL, negative cultures, strongly positive India ink, and positive Cryptococcal antigen. This patient illustrates the potential for basilar meningitis, in particular cryptococcal meningitis and tuberculosis, to be associated with cerebral infarction. In a study of stroke and TIAs in AIDS, 40% of infarcts and 8% of TIAs were associated with cryptococcal meningitis (57).
|
• Two varieties of cryptococcus account for most human infections: C neoformans var neoformans and C neoformans var gattii. | |
|
• C neoformans var neoformans causes most human infections. | |
|
• C neoformans var gattii is seen more often in immunocompetent persons. |
Cryptococcus neoformans, an encapsulated yeast, is a common soil fungus found throughout the world. Areas contaminated by pigeon droppings are particularly likely to contain this organism. It is often the predominant organism in desiccated alkaline environments with high nitrogen and high salt contents. It cannot compete successfully when soil mixing and irrigation foster the growth of other fungi and amoeba. C neoformans can remain viable after 2 or more years in moist or desiccated pigeon excreta. Antigenic variations in the polysaccharide capsule are used to define four serotypes, of which A and D most commonly cause human infections (09). Two varieties are distinguished: C neoformans var neoformans (serotypes A and D) and C neoformans var gattii (serotypes B and D). Both are members of the phylum Basidiomycota and are readily distinguished from other pathogenic yeasts by the presence of a polysaccharide capsule, formation of melanin, and urease activity; all function as virulence determinants (89). C neoformans is typically observed in the immunosuppressed population, such as in AIDS, whereas C gattii is reported more often in immunocompetent patients (89). C gattii is typically limited to subtropical and tropical zones and accounts for less than 20% of cryptococcal cases (89). However, in a review of immunocompetent persons less than 50 years of age, 63% of the identified strains were C neoformans, and only 17% were due to C gattii (157). C neoformans need not infect a vertebrate to complete its life cycle. In the animal model of disease, strain differences with respect to total capsule volume and rate of accumulation are correlated with neurovirulence (126). The differences in pathogenicity of the various strains of Cryptococcus has been proposed to be the consequence of immunogenic proteins secreted by each strain (19).
Human infection is usually acquired by inhalation of spores. The initial pulmonary infection is generally asymptomatic, although a self-limited pneumonia resolving over several weeks to months in the absence of treatment may be seen. Containment of the infection to the lungs is the consequence of both cell-mediated and humoral immunity (54). Pulmonary cryptococcosis includes the constellation of fever, cough, pleuritic pain, malaise, and weight loss. Occasionally, the cough is productive of blood-tinged sputum. The disease often affects both lungs and examination reveals diminished breath sounds, dullness to percussion, and, on occasion, a friction rub. Pulmonary infection generally resolves in its entirety, although the infection may persist as a mediastinal mass (134). Chest radiographs show variable patterns depending on the severity of the disease, the duration of the infection, and the host response.
Typically, the spread of C neoformans is limited to the lung and lymph nodes, but hematogenous dissemination may result in the seeding of other organs. The latter is particularly likely in the setting of immunosuppression. Alternatively, the organism may become reactivated from the sites of initial infection years later. Factors influencing dissemination include the polysaccharide capsule and secreted enzymes including laccase, phospholipase B, and urease (54). Resistance to infection is primarily dependent on cell-mediated immunity, although clinical infection occurs in both apparently normal and immunocompromised individuals (50). Most cases of cryptococcal meningitis are observed in individuals with underlying impairment in cell-mediated immunity (145), chiefly, in the setting of AIDS, lymphoreticular malignancies, sarcoidosis, connective tissue diseases, bone marrow and organ transplantation, and corticosteroid therapy. Humoral responses are generated by cryptococcal infection and may play a role in control of infection. Anti-cryptococcal immunoglobulins may be detected in the CSF of patients with cryptococcal meningitis (128); however, the absence of cryptococcal infection in persons with congenital or acquired humoral abnormalities indicates that this is of limited importance (68).
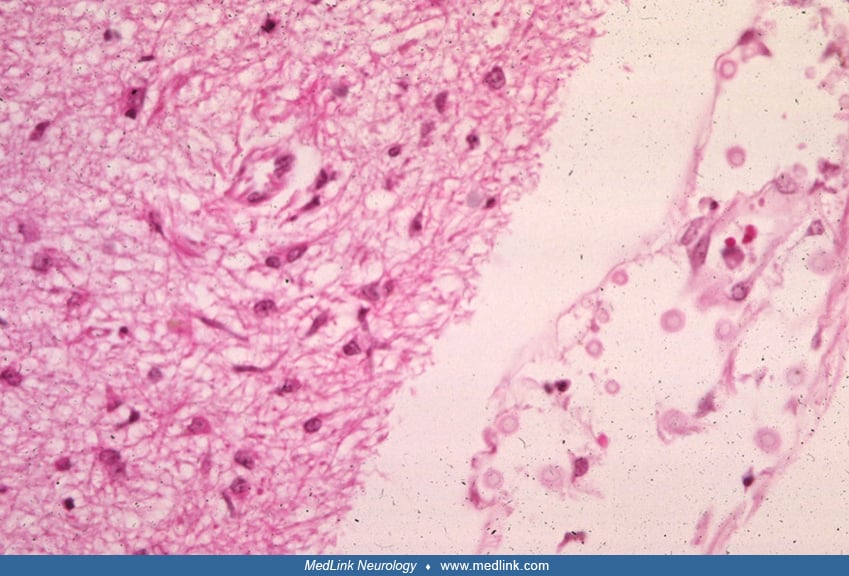
To a large degree, the tissue involved determines the nature of the pathological response to cryptococcal infection. In general, two types of histologic pattern occur with cryptococcal infection: (1) gelatinous and (2) granulomatous (06). Both types may coexist in the same lesion. The gelatinous lesions are characterized by masses of organisms and mucoid degeneration of the affected tissue. Granulomatous lesions are characterized by the presence of histiocytes, giant cells, lymphocytes, and variable degrees of a fibroblastic response.
Mouse studies indicate that Cryptococcus neoformans crosses the blood brain barrier by transcellular migration across brain endothelial cells (25) and then proliferates in the subarachnoid space resulting in leptomeningeal opacification with a gelatinous appearance. In HIV-infected individuals, the inflammatory response may be sparse and discrete, resulting in focal collections of macrophages and formation of giant cells. Focal granulomas composed of macrophages, lymphocytes, giant cells, and fungi may be seen. In cryptococcal meningitis, an exudate typically predominates at the base of the brain. This leptomeningeal exudate is usually gray-yellow in color and may extend over the surface of the cerebral and cerebellar hemispheres, although it predominates in the basal meninges. Extension into the ventricles and perivascular space is observed, and hydrocephalus may develop. Inflammation is usually, but not invariably, minimal.
The organisms extend along Virchow-Robin spaces where clusters of fungi may distend the perivascular space into adjacent parenchyma. This pathological process may also affect the spinal cord and nerve roots giving rise to myeloradiculitis (110). Intracerebral abscesses and cryptococcomas may be found in some cases. Mucicarmine staining demonstrates the capsule of the organism (93; 174). Tubercles averaging 2 to 3 mm in diameter may occur along blood vessels. A collection of yeast that distorts without destroying the brain and exhibits little or no surrounding inflammation or gliosis is referred to as a “gelatinous pseudocyst” (62).
Typically, these lesions have been present for a relatively short period of time. Localized granulomatous lesions are referred to as “cryptococcomas,” “torulomas,” or “cryptococcal granulomas” (147).
Although these lesions are chiefly observed in the cerebral hemispheres, they have also been reported in the cerebellum (82) and spinal cord (148). Persons with these lesions generally exhibit focal neurologic findings and have had the infection for a period of weeks or months.
Another cause of focal neurologic findings in the setting of cryptococcal meningitis is cerebrovascular disease (144; 186; 168; 65; 80; 92), which occurs as a consequence of perivascular granulomatous infiltration or from vascular occlusion at the time of brain herniation. Multiple ischemic insults can be observed, although this is distinctly unusual (136). Persons with AIDS have a higher incidence of parenchymal brain lesions and involvement of extracranial sites, as well as concomitant opportunistic infection (most often Pneumocystis carinii pneumonia) in 15% to 35% (166).
Cryptococcus is cleared by neutrophils and macrophages in a process that is mediated by complement, interferon, and T lymphocyte-derived lymphokines. Animal experiments reveal a critical role of interferon-γ for control of cryptococcal CNS infection and suggest that anti-CD40 and IL-2 therapy can be protective (189). The large polysaccharide capsule appears to be a virulence factor, inhibiting phagocytosis and leukocyte migration and activating the alternative complement pathway. One of the capsule’s defense mechanisms is the ability to produce a toxic polysaccharide that kills the engulfing macrophage (159). Survival in mammalian hosts is encouraged by the stimulation of capsular production by the physiologic concentrations of CO2 and by the low ferric iron concentrations found in the lung. Toll-like receptor 2 (TLR2) expression in patients with cryptococcal meningitis appears to be lower than in healthy controls and may contribute to the impaired host defense that naturally protects against development of the infection (188).
Cryptococcus has a particular affinity for the CNS, perhaps due to the absence of complement and soluble anticryptococcal factors present in serum and a diminished inflammatory response to the agent in brain tissue. A receptor on CNS cells for a ligand on the yeast has been proposed (77; 106) but has yet to be identified. Specific phenotypes of C neoformans appear to have a predilection for invasion of the nervous system. These include melanin production, the ability to thrive at body temperature, and the presence of a polysaccharide capsule (90; 24). In vitro experiments reveal that C neoformans causes marked alterations in the cytoskeleton of human brain endothelial cells resulting in swelling of mitochondria and endoplasmic reticulum, membrane ruffling, and irregular nuclear morphology with a resultant disruption of the blood-brain barrier (29). Elaboration of urease is also believed to be important in the disruption of the blood-brain barrier (54).
|
• An increasing incidence of cryptococcal meningitis predated the AIDS pandemic. | |
|
• HIV infection remains the greatest risk factor for cryptococcal meningitis. | |
|
• Cryptococcal meningitis is associated with a number of immunosuppressive drugs including some used in the treatment of multiple sclerosis, particularly, fingolimod. | |
|
• Cryptococcal meningitis is seen an increasing number of persons without an underlying immune deficiency. |
In the decades preceding the AIDS epidemic, the reported incidence of cryptococcal infection saw a dramatic increase (59). This increase was seen with other mycotic infections as well and was attributed to increasing numbers of persons with immunosuppressive conditions, migration of susceptible persons into hyperendemic areas, and aging of the population (59). With the advent of the AIDS epidemic in the 1980s, the incidence of cryptococcal infection, in particular cryptococcal meningitis, increased even more (87; 56; 107). Between 5% and 15% of untreated patients with AIDS in certain areas of the world will develop C neoformans disease during the course of their illness (164; 42). However, following the introduction of highly active antiretroviral therapeutic regimens, the incidence of cryptococcal meningitis has declined significantly in the HIV-infected population in western countries (140). However, this has not been a universal experience. For instance, in China, cryptococcal meningitis is the most common opportunistic infection in AIDS and is a significant cause of mortality (178). Cryptococcal meningitis may herald AIDS and occur in individuals not otherwise suspected to be HIV infected (11; 64). An epidemiological study from inpatient databases of 18 states in the United States identified 30,840 hospitalizations coded for cryptococcal meningitis (131). Only 21.6% of these cases occurred in HIV-uninfected persons. However, the incidence rates of cryptococcal meningitis have declined significantly during the antiretroviral therapy era, with rates of 3.7, 1.8, and 0.3 per 1000 person-years at risk in 1995 to 1996, 1997 to 1999, and 2000 to 2014, respectively (169). Despite declining incidence rates with HIV infection, monitoring cryptococcal antigenemia in HIV-infected persons with CD4 lymphocyte counts less than 200 cells/μL and treating those that are positive with fluconazole is recommended though there remains uncertainty as to whether this approach has reduced mortality (176). The potential magnitude of the problem has been illustrated by a study from India, a high burden country, in which cryptococcal antigenemia was detected in 60.8% of antiretroviral naïve patients and 39.2% of ART failures with CD4 lymphocyte counts less than 100 cells/μL (01).
Not unexpectedly, cryptococcal meningitis also occurs with increased frequency in a variety of other immunosuppressive conditions. For instance, it is a significant cause of morbidity and mortality in organ transplant recipients. In a study from the University of Pittsburgh, a major organ transplant center, the incidence of cryptococcal meningitis among transplant recipients was 0.5% (28/5521) (182). The greatest risk for development was among heart transplant recipients at 2.1% (8/372); however, the greatest mortality with the disease was in liver transplant recipients (182). Sarcoidosis (137) and idiopathic CD4 lymphopenia (143) are other risk factors for cryptococcal meningitis. Cryptococcal meningitis has been reported in multiple sclerosis patients treated with natalizumab (172) as well as with fingolimod (123; 31). Diabetes mellitus and liver cirrhosis are also risk factors for the disease. In a review of 28 published studies of cryptococcal meningitis with diabetes, all-cause mortality was 38.3% and mortality with meningitis was 36.2% (114). The 90-day mortality rate for cryptococcal meningitis with liver cirrhosis was 20% in one study (190).
Individuals without any recognized immunological deficiency continue to account for a substantial proportion of CNS cryptococcosis. In a study, immunocompetent persons comprised 43.5% of all the cases (101). In comparison to the immunocompromised group, immunocompetent individuals had a higher incidence of cryptococcal meningitis, lower rates of fungemia, and lower mortality (101). Among immunocompetent individuals, immunogenetics may contribute to the risk of cryptococcal meningitis. A study from China found an association with the HLA loci DQB1*05:02 and susceptibility to cryptococcal meningitis (99).
|
• The high risk of cryptococcal meningitis in AIDS patients with CD4 counts less than 100 warrants either prophylactic therapy or careful serial monitoring of serum cryptococcal antigen levels. |
Prevention is only relevant in the AIDS population. Two forms of prevention are possible. As the risk of cryptococcal meningitis is considerable in HIV-infected persons with CD4 T lymphocyte counts below 100 cells/cu mm, primary prophylaxis is considered in this population. An alternative to primary prophylaxis is screening for serum cryptococcal antigen positivity in those with CD4 T cells below 100 cells/cu mm as it correlates with an increased risk of cryptococcal meningitis and mortality in this population (13). Relapse is common in the patient with AIDS who has already suffered from cryptococcal meningitis. Prevention in that population is regarded as secondary prophylaxis.
Primary prophylaxis. The safety and efficacy of triazole antibiotics has raised the possibility of primary prevention in susceptible immunosuppressed HIV-infected individuals. An open label trial showed a reduced rate of cryptococcal meningitis in patients with CD4 levels less than 68/mm3 given 100 mg/day fluconazole compared to controls from the previous two years seen in the same site (113). One review suggested that primary prophylaxis be considered for patients with CD4 counts less than 50/mm3 but noted that the impact of such therapy on survival or on the susceptibility of various fungi to current agents is uncertain (125). A Cochrane Database review supported either fluconazole or itraconazole to reduce the incidence of cryptococcal disease in adults with advanced HIV infection (23).
Prevention of relapse. Early series of AIDS patients with cryptococcal meningitis treated only with acute therapy were associated with relapse rates of 50% to 60% (87; 191; 35). Open label trials of fluconazole (162) and itraconazole (45; 49) and a retrospective series in which some patients were given amphotericin B or ketoconazole (34) suggested survival benefit for maintenance therapy. A large placebo-controlled trial documented a 19% persistence of positive CSF cultures following six weeks of primary therapy with amphotericin alone or in combination with flucytosine and a significant benefit for fluconazole 100 to 200 mg/day in preventing relapse in patients with sterile CSF (15). Subsequently, a study comparing fluconazole 200 mg/day to amphotericin B 1.0 mg/kg per week found the former agent to be more effective with less toxicity (130).
Despite maintenance therapy, recurrent cryptococcal meningitis occurs in 2% to 16% of AIDS patients (34; 35; 15; 130). Serum cryptococcal antigen is not a reliable marker for CNS infection (56; 15). CSF cryptococcal antigen titers decline with successful therapy, but subsequent rises with recurrence are apparently acute and not predicted by routine monitoring of CSF (15). Persistence of cryptococcus in the prostate despite sterilization of CSF has been shown (94). Molecular genetic studies have revealed clonal identity of serial isolates obtained from three AIDS patients with recurrent meningitis (155). Although prospective studies have yet to be done on the natural history of persistently positive cultures in patients with suppression of clinical disease, it seems likely that recurrence results from sequestered organisms in CSF or elsewhere.
Failures of primary or secondary prophylactic therapy might potentially be due to resistant fungi. A case in which resistance to fluconazole appeared to evolve during therapy has been reported (118), and another in which resistance of a Cryptococcus neoformans var gattii species to fluconazole was noted (119). In a small series, no change in sensitivity of serial isolates to either fluconazole or amphotericin was detected, but there was a wide variation in the dose sensitivity to fluconazole among different isolates (21). Higher doses of fluconazole to 800 mg/day have been reported to be effective salvage therapy in patients failing conventional therapy with either fluconazole or amphotericin (12), and response may be observed in those resistant to amphotericin B (130).
In the era of highly active antiretroviral therapy with which a significant return to normal immune function may be observed, the necessity of secondary prophylaxis remains an open question. One prospective study addressing that issue found no recurrence of cryptococcal meningitis during a median 48-month follow-up in a group of patients with CD4 cell counts greater than 100 cell/cu mm and an undetectable HIV RNA level that had been sustained over three months (173).
As cryptococcal meningitis may present in manifold fashions and is a treatable condition, it must be in the differential diagnosis of many clinical presentations including headache, encephalopathy, stroke, and seizure. The telltale features of meningitis, such as fever and signs of meningeal irritation, may be absent or relatively inapparent. On rare occasion, a cerebral cryptococcoma may even masquerade as a glioma (171).
Generally, the differential diagnosis of cryptococcal meningitis includes a broad range of other disorders that cause meningitis accompanied by a predominantly mononuclear CSF pleocytosis. Among the disorders that need to be considered are certain viral meningitides, some forms of bacterial meningitis (eg, tuberculous meningitis and partially treated bacterial meningitis), other fungal meningitides, parasitic meningitis (eg, amebic meningitis and trichinosis), carcinomatous and lymphomatous meningitis, drug-induced and chemical meningitis, and meningitis accompanying connective tissue diseases (eg, systemic lupus erythematosus and rheumatoid arthritis).
Radiology. CT imaging is insensitive to cryptococcal meningitis, revealing nonspecific atrophy or no abnormalities in most instances (129; 127; 167). On rare occasion, unusual manifestations may be observed, such as CT demonstration of large, ring-enhancing, intraparenchymal lesions with intralesional calcification (05).
MRI is more sensitive than CT. In a study of 62 HIV-seropositive patients with cryptococcal meningoencephalitis, baseline imaging was abnormal in 53% of CT scans but in 92% of MRIs (27). Despite its increased sensitivity, MRI may still substantially underestimate the lesion burden found on pathologic examination (105). In immunocompetent individuals, multiple cystic lesions in the basal ganglia with marked ring enhancement (in contradistinction to the typical absence of contrast enhancement in the immunosuppressed individual) has been described (142).
Contrast enhanced imaging with MRI may reveal meningeal enhancement but appears to do so less frequently than in non-HIV-infected patients with cryptococcal meningitis. In a study comparing cryptococcal meningitis in HIV and non-HIV populations, normal brain imaging was observed in 44% of the former versus 13% of the latter (97). Parenchymal cryptococcomas may appear as enhancing mass lesions within the parenchyma (191; 167; 03). On diffusion-weighted MR imaging, cryptococcomas show a hypointense central cavity, which on apparent diffusion coefficient maps is hyperintense; these features mimic necrotic brain tumors rather than pyogenic brain abscesses (71). Miliary nodular enhancing leptomeningeal lesions have been noted uncommonly (167). In the absence of pathological confirmation, it is difficult to exclude the possibility of concurrent opportunistic pathology accounting for enhancing mass lesions (105).
Nonenhancing foci (which may be numerous in the basal ganglia and midbrain, displaying signal intensities similar to CSF) represent dilated Virchow-Robin spaces. On pathologic examination these may be filled with clusters of cryptococci and mucinous secretions. These collections have been referred to as gelatinous pseudocysts by some authors (127; 167; 105; 03). Cerebral infarcts may also occur with cryptococcal meningitis. In a study, 13% of patients had infarcts on MRI, with most common site of involvement being the basal ganglia followed by the thalamus, frontal, temporal, and parieto-occipital regions (108).
Cerebrospinal fluid. Identification of cryptococcus in the CSF is the gold standard for establishing the diagnosis. In contrast to non-HIV-infected individuals with cryptococcal meningitis, CSF abnormalities may be subtle in AIDS patients. The opening pressure is elevated in about two thirds and may exceed 500 mm of water. Animal studies suggest that C neoformans strain differences, such as the expression of glucorunoxylomannan, influences the degree of inflammation and the elevation of intracranial pressure (61). The CSF is typically clear, although on occasion, may be cloudy. Pleocytosis is lacking or modest in most instances; however, occasionally vigorous mixed inflammatory responses are seen. Hypoglycorrhachia and elevated protein levels are found in up to three fourths of cases.
India ink stains will disclose cryptococci in 50% of non-AIDS patients and in as many as 80% of those with AIDS (121). The India ink is positive in 70% to 94% of patients with positive CSF cultures.
Cryptococcal antigen latex agglutination is a reliable test of the presence of the organism in the CSF as it is positive in more than 90% of patients with meningitis (87; 191; 34; Clark et a 1990; 139; 138) and is a valuable test while awaiting fungal cultures (154). Falsely negative cryptococcal antigen tests may occur. Although in most instances, false negative antigen tests do not appear to be due to a prozone phenomenon or interference from bound antibody or protein (43), occasionally a prozone phenomenon may be observed with spuriously negative studies (102). Like the India ink test, high titer CSF cryptococcal antigen (greater than 2:2034) is seen more commonly in the AIDS patient than the non-AIDS patient with cryptococcal meningitis. Cryptococci are cultured from CSF in virtually all patients with meningitis but less commonly with parenchymal cryptococcomas in the absence of meningitis (191); however, a study of first-episode HIV-associated cryptococcal meningitis in Uganda found that 10% had a sterile culture despite the presence of cryptococcal antigen in the CSF (133). The yield is improved when large volumes of CSF (10 to 30 mL) are removed and cultured. Neither India ink nor CSF cryptococcal antigen studies are reliable measures to assess the adequacy of therapy. CSF fungal cultures are definitive in this regard. Next-generation sequencing has also been demonstrated to be valuable in identifying cryptococcal meningitis (183).
As mentioned, other CSF parameters are frequently abnormal as well. The CSF leukocyte count varies considerably. With rare exception, lymphocytes predominate. White cell counts rarely exceed 800 cells/cu mm (134). Low numbers may occur in the setting of AIDS or corticosteroid administration. The number of cryptococci may exceed the number of leukocytes. A quantitative assessment of the number of viable yeast may yield between 103 and 107 colony-forming units of yeasts per mL of CSF (121). CSF protein levels are high and may exceed 1 g/dL, but are typically in the range of 40 to 600 mg/dL. In those instances where the protein is excessive, a subarachnoid block should be considered. Hypoglycorrhachia may also be seen.
Serologic studies. Cryptococcal antigen titers in serum are usually elevated in patients with cryptococcal meningitis, in some cases even when antigen titers in CSF (34) and CSF cultures for cryptococcal are negative (156). This observation underscores the importance of obtaining serum cryptococcal antigen in all patients suspected of having cryptococcal meningitis. The level of serum cryptococcal antigen and changes in response to therapy do not appear to reliably reflect CSF responses (56; 35; 130). Blood culture may be diagnostic and CSF negative for Cryptococcus in the presence of cryptococcal meningoencephalitis (152). Spuriously negative serum and CSF cryptococcal antigen assay may occur in the presence of high antigen levels (prozone phenomenon), and detection may require dilution (102).
Serum cryptococcal antigen titers may reflect disease disseminated to other organs; this occurs in conjunction with meningitis in up to one half of cases. Titers above 1:8 suggest disseminated cryptococcosis. Most common sites for extrameningeal infection are the lungs, blood, urine, and bone marrow, but virtually any organ may be involved (87; 94; 35; 138).
|
• The standard treatment of cryptococcal meningitis in nonpregnant adults is amphotericin B and flucytosine. | |
|
• The duration of induction therapy should be no less than 2 weeks. | |
|
• Following induction therapy, maintenance therapy with fluconazole for 8 weeks is recommended. | |
|
• Routine administration of corticosteroids with the antibiotic regimen is not recommended, though it is helpful in the treatment of IRIS or PIIRS. | |
|
• Increased intracranial pressure may mandate the placement of a shunt. |
Authorities have advanced various recommendations regarding the treatment of cryptococcal meningitis in HIV infection. Consensus is that the expectation from treatment is control rather than eradication of infection. Early series reported acute mortalities within six weeks of the completion of therapy of 18% to 37% and, generally, within the first two weeks (87; 34; 35; 139). A variety of treatment regimens were used both within and between studies. A large study from Vietnam of nearly 300 HIV-infected patients with cryptococcal meningitis randomized to amphotericin B alone, amphotericin B and flucytosine, and amphotericin B and fluconazole, convincingly demonstrated that combining high-dose amphotericin B at 1 mg/kg of body weight per day for four weeks with flucytosine 100 mg/kg per day for two weeks resulted in a significantly improved survival (44). There was no survival benefit with the coadministration of fluconazole. The addition of interferon-gamma immunotherapy to standard treatment has been demonstrated to increase clearance of Cryptococcus from the CSF (75).
The standard treatment for cryptococcal meningitis has been amphotericin B at doses of 0.7 to 1.0 kg/day intravenously. Dosages used, however, have ranged from 0.3 to 1.0 mg/kg per day, with higher doses given for shorter periods before reduction to a maintenance regimen (87; 191; 34; 94; 35; 139; 180; 47). The currently recommended doses are either liposomal amphotericin B 3 to 4 mg/kg intravenously per day or amphotericin B lipid complex 5 mg/kg per day (40). Amphotericin B is a polyene antibiotic that binds to ergosterol in the cryptococcal membrane, altering its permeability. Combined induction therapy of amphotericin B combined with flucytosine (02) is generally recommended as this combination has been associated with greater sterilization of the CSF at two weeks and fewer treatment failures (52; 51). The duration of treatment may be as little as two weeks provided that a lumbar puncture documents negative CSF fungal cultures and the intravenous treatment is followed by at least 10 weeks of high dose fluconazole (400 to 800 mg/day orally) as maintenance therapy (02). However, longer treatment durations may be dictated by serious neurologic complications and the response to therapy. In studies prior to AIDS, amphotericin B was found to be more effective in treating cryptococcal meningitis when administered with flucytosine, an oral antimycotic metabolized to 5-fluorouracil within fungal cells, which inhibits fungal DNA and RNA synthesis. Flucytosine may also inhibit purine and pyrimidine uptake by fungi. Myelosuppression from the usual doses of 100 to 150 mg/kg per day has been problematic in AIDS patients, however, limiting its use; gastrointestinal reactions and hepatotoxicity may also occur and cause problems (162; 130). Many large retrospective studies have failed to show survival benefit from combination therapy in AIDS patients, in part due to the impact of toxicity (34; 35). A comparative study of amphotericin B administered intravenously versus a similar group receiving the drug via Ommaya reservoir suggested that CSF cryptococcal clearance and recovery rates were better in the latter group (179). The placement of an Ommaya reservoir may be particularly helpful in the setting of refractory intracranial hypertension (177).
During therapy with amphotericin B, electrolytes and renal function need to be monitored carefully. Renal toxicity, which is related to the cumulative dose administered, is the major limiting adverse effect. During infusion, acute reactions commonly occur with fevers, chills, rigors, headache, and nausea, which may be mitigated by pretreatment with hydrocortisone, nonsteroidal antiinflammatory agents, anti-emetics, and antihistamines. Other potential adverse reactions include seizures, phlebitis, anemia, and edema (162). Amphotericin B is contraindicated in persons who are hypersensitive to the drug or who have significant renal insufficiency. In addition to its nephrotoxicity, other side effects include infusion-related erythema, fever, rigors, hypokalemia, and hypomagnesemia. Patients receiving other nephrotoxic agents should be treated with liposomal amphotericin B.
Attempts to mitigate toxicity from amphotericin B therapy have included incorporation into liposomes (37; 38) and infusion of amphotericin in a fat emulsion (96). Successful responses were obtained in a single patient in the latter instance and a dozen patients in the former. Both regimens were well tolerated. Liposomal amphotericin B is administered as 3 to 6 mg/kg per day intravenously. Doses of amphotericin lipid complex are 5 mg/kg per day. At least three weeks of induction is required when it is used without flucytosine in the setting of renal insufficiency. In general, this expensive preparation is used in the place of amphotericin B only when concomitant nephrotoxic agents are required, there is significant preexisting renal insufficiency (02), or patients have failed other therapies (53).
Flucytosine is administered as 100 mg/kg per day orally in four divided doses and must also be adjusted for renal insufficiency. It is typically administered for two weeks at the inception of therapy. Side effects include bone marrow suppression, azotemia, and hepatic dysfunction. Flucytosine cannot be used as monotherapy due to the rapid development of resistance by the organism.
The development of triazole agents, which inhibit cytochrome P450 enzyme activity by limiting fungal ergosterol synthesis (162), has had a major impact on control of cryptococcal infections in AIDS patients. Fluconazole has a higher CSF penetration than itraconazole, though both have shown efficacy in AIDS patients with cryptococcal meningitis (160; 162; 49; 113). Fluconazole is administered as 400 mg/day in acute therapy and 200 mg/day as suppressive therapy. Side effects include nausea, rash, and hepatitis. Itraconazole is administered as 200 to 400 mg twice daily. Its side effects include nausea, abdominal pain, rash, headache, edema, and hypokalemia. Posaconazole, another triazole antifungal agent, is active against Cryptococcus, but experience with neurologic infection is limited (111).
Comparisons of triazoles with amphotericin B for acute therapy of cryptococcal meningitis in AIDS patients have yielded mixed results to date. The largest trial found no significant difference in overall mortality between fluconazole and amphotericin B, although mortality with fluconazole was concentrated in the first two weeks of illness. Doses of the agents and combination therapy with flucytosine were not controlled (139). Amphotericin B 0.3 mg/kg per day plus flucytosine 150 mg/kg per day was superior to itraconazole 200 mg/day over six weeks in a series (46). Amphotericin B 0.7 mg/kg per day for a week followed by thrice weekly administration for nine weeks in combination with flucytosine 150 mg/day was superior to fluconazole 400 mg/day in another series (95). Variations in dosages, combinations of medications, severity of illness on entry, and definitions of successful outcome among studies limit direct comparisons (130). Fluconazole is administered as 200 to 800 mg/kg per day orally or intravenously. Because of its excellent bioavailability and affordability, the oral preparation is preferred to the parenteral preparation. Alspaugh and Perfect recommend 3 to 9 months of fluconazole maintenance therapy at doses of 200 mg/kg per day in patients without HIV infection and lifelong therapy in the HIV-infected person (02). The drug’s chief side effects are mild nausea and hair loss. A related drug, itraconazole, can be substituted at doses of 200 to 400 mg/kg per day orally or intravenously. Oral itraconazole is an effective prophylactic agent for Cryptococcus in AIDS (26).
Although not an approved therapy in the United States or Europe for cryptococcal infection, an increasing body of experience suggests that voriconazole is an effective antifungal agent (07; 20; 112). Granulocyte/macrophage colony-stimulating factor and interferon are being evaluated as adjunctive therapies. Other potential future therapies include azole antifungals and anticapsular monoclonal antibodies (02). Intrathecal amphotericin B is also an option in treating cryptococcal meningitis refractory to intravenous antifungal treatments (187).
The practice of administering dexamethasone with amphotericin B and fluconazole in HIV-associated cryptococcal meningitis is not supported by data. A double-blind, randomized, placebo-controlled trial comparing HIV-infected patients treated with or without dexamethasone in addition to standard antifungal therapy revealed that it did not reduce mortality and was associated with more adverse events and disability (08). However, in the setting of IRIS or PIIRS in which CNS inflammation is associated with increased intracranial pressure and severe symptoms, corticosteroid use may be warranted. To date, there is no widely recommended dosing regimen. Dexamethasone starting at 20 to 24 mg intravenously daily for one week with subsequent tapering over 4 to 6 weeks or prednisone 60 to 80 mg per day tapered over 4 to 6 weeks have been employed.
Elevated intracranial pressure is common in patients with cryptococcal meningitis and may result in hydrocephalus. It has been postulated that sustained elevations in intracranial pressure may contribute to early mortality by impairing cerebral circulation (49). Therapeutic modalities include drainage by serial lumbar punctures, ventricular drainage, and acetazolamide. The former has been recommended by some authorities when CSF opening pressures equal or exceed 250 mm water (67). Uncontrollable intracranial hypertension may occur in the absence of hydrocephalus, and ventriculoperitoneal shunting may be lifesaving (122). On rare occasion, however, cerebellar tonsillar herniation may occur in the setting of cryptococcal meningitis in the absence of mass lesion (10). Nonetheless, in those individuals with raised intracranial pressure, therapeutic lumbar punctures, particularly in resource poor settings, have been reported to be associated with a 69% relative survival protection (22).
Acute visual loss in patients with HIV-associated cryptococcal meningitis may be transient, abrupt, or progressive and may result from increased intracranial pressure (49), although other causes need to be considered--eg, necrotizing optic neuropathy due to cryptococcal invasion (36) and constrictive arachnoiditis (98). Visual loss in HIV-associated cryptococcal meningitis is independently associated with fungal burden and raised intracranial pressure (109). Patients with papilledema and severely impaired vision may respond to antibiotic therapy alone (66), ventricular shunting of CSF (165), or lysis of arachnoid adhesions (104). The performance of therapeutic lumbar punctures for individuals with high intracranial pressure (> 250 mm H2O) or new symptoms were associated with a significantly reduced mortality (18% vs. 7%), but therapeutic lumbar punctures should be undertaken cautiously (135). Optic nerve sheath fenestration resulted in visual recovery of two patients with cryptococcal meningitis who had persistent associated papilledema and visual loss despite antibiotic therapy (63).
Both cryptococcal pneumonia (55; 91) and meningitis (124; 151; 41; 79; 158; 85; 32; 33; 120; 28) have been reported during pregnancy. Dissemination of Cryptococcus to the placenta has been reported in the setting of AIDS (85). Whether there is an increased incidence of cryptococcal infection in this population remains unanswered, but a small increment is not unlikely. Although a potential risk of fetal drug toxicity exists, the reported cases to date indicate good survivals of both mother and infant and no lasting toxicity.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Joseph R Berger MD
Dr. Berger of the Perelman School of Medicine, University of Pennsylvania, received consultant honorariums from Celegene/BMS, Cellevolve, EMD Serono/Merck, Genentech, Genzyme, Janssen/J&J, Morphic, Novartis, Roche, Sanofi, Takeda, and TG Therapeutics. He received honorariums from MAPI and ExcisionBio as a scientific advisory or data safety monitoring board member. And he received research support from Biogen and Genentech/Roche.
See Profile
John E Greenlee MD
Dr. Greenlee of the University of Utah School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Behavioral & Cognitive Disorders
Apr. 18, 2024
Behavioral & Cognitive Disorders
Apr. 17, 2024
Infectious Disorders
Apr. 10, 2024
Infectious Disorders
Apr. 02, 2024
Neuroimmunology
Mar. 24, 2024
Neuroimmunology
Mar. 24, 2024
Infectious Disorders
Mar. 24, 2024
Infectious Disorders
Mar. 24, 2024