
Epilepsy & Seizures
Ambiguous paroxysmal events
Mar. 22, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Hemiclonic seizures (non-Jacksonian) are a type of unilateral convulsive seizure, mainly affecting infants and young children. Their most typical presentation is in hemiconvulsion-hemiplegia-epilepsy where hemiclonic status epilepticus is followed by permanent hemiplegia. They also occur in Dravet syndrome, metabolic and electrolyte derangements, age-related benign childhood epilepsies, and, more rarely, in idiopathic generalized epilepsy. They manifest with entirely one-sided, unilateral, clonic convulsions from onset without the focal elements and without the marching of Jacksonian seizures. Hemiclonic status epilepticus is common. Ictal EEG shows discharges that are mainly generalized from the start, but have significant emphasis over one hemisphere. Hemiclonic seizures have not been considered in the updated ILAE classifications and need re-assessment with video-EEG documentation and other modern brain imaging technologies. In this article, the author reviews historical aspects, clinical manifestations, pathophysiology, EEG, differential diagnosis, and management of patients with hemiclonic (non-Jacksonian) seizures.
• Non-Jacksonian hemiclonic seizures mainly affect infants and very young children. | |
• Clinically, non-Jacksonian hemiclonic seizures are unilateral from onset or at least lack the typical focal onset and marching of typical Jacksonian hemiclonic seizures. | |
• Hemiclonic status epilepticus is common. | |
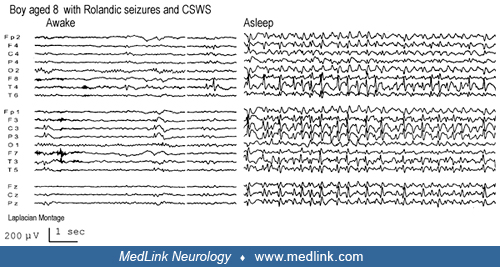
• Interictal EEG mainly shows generalized or unilateral spike-and-wave or polyspike-and-wave discharges that occur either spontaneously or following overbreathing or photic stimulation. | |
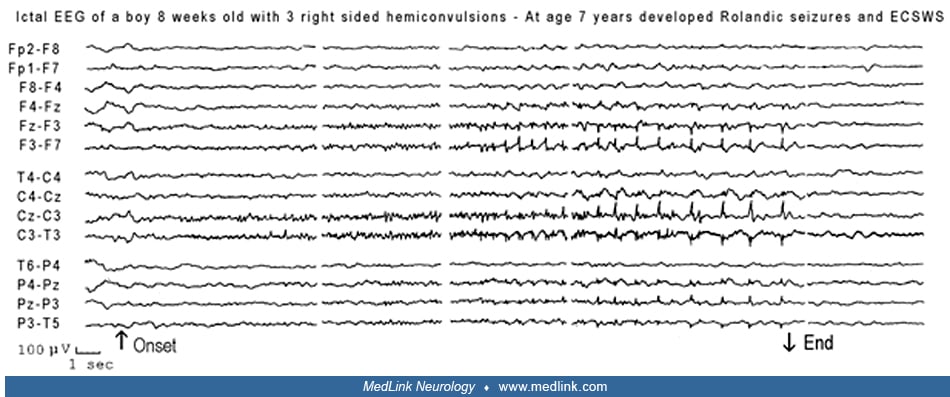
• Ictal EEG does not show focal rolandic discharges, but spike or spike-and-wave discharges, identical to those seen in typical generalized epilepsies, appear on the contralateral hemisphere. | |
• The underlying mechanisms of non-Jacksonian hemiclonic seizures are assumed to be similar to those of generalized epilepsies but are limited to one hemisphere as opposed to a focal mechanism. | |
• There is a need for better characterization of hemiclonic (non-Jacksonian) seizures with video-EEG correlations and newer imaging technologies. | |
• Termination of prolonged hemiclonic seizures is a medical emergency because of the risk for permanent hemiplegia and subsequent epilepsy. |
Historical note. The first account of focal clonic seizures progressing to hemiclonic seizures can be found as early as 1050 BC in the twenty-fifth Babylonian cuneiform tablet devoted to miqtu (a disease in which the person loses consciousness and foams at the mouth) (75; 09):
In the time of his possession, while he is sitting down, his (left) eye moves to the side, a lip puckers, saliva flows from his mouth, and his hand, leg and trunk on the left side jerk (or, twitch) like a (newly)-slaughtered sheep, it is miqtu. If at the time of the possession his mind is consciously aware, (the demon) can be driven out; if at the time of the possession his mind is not so aware, (the demon) cannot be driven out. |
Every student of neurology is familiar with “Bravais-Jackson seizures” or “Jacksonian seizures” and postictal hemiparesis (Todd hemiparesis). Bravais was the first to describe focal clonic evolving to hemiclonic seizures and postictal hemiparesis, which he called "hemiplegic epilepsy” (10). Jackson, who described the same phenomena of “convulsions beginning unilaterally,” reasoned that there must be localized movement representation in the cerebral cortex, and provided a new concept of epileptogenesis (38). Furthermore, Jackson accepted that the initially unilateral convulsive phenomena could spread to involve both sides of the body, whereas Bravais believed that this was incompatible with his entity, unless the generalization was a very rare event in the sufferer (25). Todd described "epileptic hemiplegia" of what is today known as Todd paralysis (70).
Non-Jacksonian hemiclonic seizures were first mentioned by Gibbs (34) and Lennox (46) with no particular details. However, it was Henri Gastaut and his associates in Marseilles who provided superb descriptions of the clinical and EEG manifestations of non-Jacksonian unilateral and hemiclonic seizures (hemi grand mal and hemiclonic seizures) (32; 30; 58; 59; 23).
Hemiconvulsive seizures, or one-sided convulsions, include all, tonic or clonic, epileptic phenomena that involve all or part of the skeletal musculature of one side of the body only (thereby excluding "adversive" seizures, which result from the contraction of bilateral synergetic muscles). Clinical observation and simultaneous cinematographic, electroencephalographic and electromyographic recording of thousands of spontaneous and induced seizures have convinced us of the existence of at least two major types of non-Jacksonian hemiconvulsive epilepsy: | |||
• One-sided or "hemi-grand mal” | |||
• Hemiclonic seizures. | |||
The "hemiconvulsive seizures" concern all epileptic convulsions--tonic or clonic--interesting only one side of the body. The "Jacksonian epilepsy" is one of the aspects of this type of epilepsy, the others being: | |||
• "Hemi grand mal": typical grand mal seizures, but strictly localized to one side of the body and, electroencephalographically, to the contralateral hemisphere. | |||
• "Hemiclonic seizures": clonic phenomena often beginning with an "oculoclonic crisis,” spreading to the whole ipsilateral half of the body. On the EEG, on the contralateral hemisphere, two to three c/s slow waves and eight to 10 waves predominating in the posterior region are observed. | |||
The hemiclonic seizures occur specifically in children and in two main groups of epileptics: | |||
• Those with neurologic, radiological or electroencephalographical signs of focalization (among whom are found some with " hemiconvulsion-hemiplegia-epilepsy syndrome"). | |||
• Those without any sign of cerebral focalization, but suffering from petit mal or grand mal (32). | |||
Nomenclature and classification. Hemiclonic seizures are profoundly featured in the 1970 ILAE classification as influenced by Gastaut (29):
111. Unilateral or predominantly unilateral seizures: Seizures in which the clinical and electrographic aspects are analogous to those of the preceding group (generalized bilateral symmetrical seizures), except that the clinical signs are restricted principally, if not exclusively, to one side of the body, and the electroencephalographic discharges are recorded over the contralateral hemisphere. Such seizures apparently depend upon a generalized or at least very diffuse neuronal discharge that predominates in, or is restricted to, a single hemisphere and its subcortical connections. They are characterized by clonic, tonic or tonic-clonic convulsions, with or without an impairment of consciousness, expressed only or predominantly in one side. Such seizures sometimes shift from one side to the other but usually do not become symmetrical. | ||
Ictal EEG may show: | ||
(i) partial discharge very rapidly spreading over only one hemisphere (corresponding with only contralateral seizures) | ||
(ii) discharges generalized from the start but considerably predominant over one hemisphere, susceptible to change from one side to the other at different moments (corresponding to alternating seizures) | ||
(iii) partial discharge, susceptible to change, from time to time, in morphology and topography (from area to area and, sometimes, from one side to the other) | ||
Interictal EEG may show: | ||
(i) focal contralateral discharges | ||
(ii) bilateral and synchronous symmetrical or asymmetrical discharges of spike and wave or polyspike and waves | ||
(iii) focal discharges, susceptible to change, from time to time in morphology and topography. | ||
Hemiclonic and unilateral seizures have been detailed by Oller-Daurella and Dravet and also by Roget in the first edition of the “blue guide” (59; 53).
Subsequent ILAE classifications and proposals do not consider unilateral seizures other than hemiclonic seizures from ipsilateral propagation of focal clonic seizures to neocortical areas (26). A related “hemiconvulsion-hemiplegia-epilepsy syndrome” is recognized as an epileptic syndrome (08; 18).
According to the latest 2014 ILAE epilepsy diagnosis manual, hemiclonic seizures are focal, and they are classified among those with elementary motor features that involve a stereotyped contraction of a muscle or group of muscles (18). Such motor features may be predominantly convulsive (rhythmic jerking (clonic activity)) and may occur alone or in combination with tonic activity (eg, hemiclonic that is rhythmic jerking (clonic activity) involving only one side of the body). Conversely, generalized convulsive seizures are typically bilateral and symmetric although variants with asymmetry including head and eye deviation can be seen (18). According to Dravet and Seino, “these variations reflect our lack of knowledge of the true physiopathology of generalized and unilateral seizures…. In practice, no clear-cut borderline exists between generalized and unilateral clonic seizures, in many cases, making it difficult if not impossible to classify them” (23).
Hemiclonic seizures are not mentioned in the updated ILAE positional paper on the classification of seizure types (28) and epilepsies (63). Also, hemiclonic status epilepticus is not considered in the latest ILAE definition and classification of status epilepticus (71).
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125