

Stroke & Vascular Disorders
Cardiovascular intervention: neurologic complications
Apr. 25, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author reviews the risk of stroke in children with sickle cell anemia (HbSS). Stroke occurs in 11% of children with the disease by 20 years of age. The author reviews the pathophysiology of stroke in sickle cell disease and discusses ways to identify those at high risk for stroke. Transcranial Doppler measurement of the time-averaged mean of the maximum (TAMM) blood flow velocities in the distal internal carotid and proximal middle cerebral artery has proven to be the best predictor of stroke risk in this population. The author discusses the transcranial Doppler technique used in the examination of children with sickle cell disease for both initial examination as well as follow-up examinations. He also reviews the effectiveness of transfusion therapy for prevention of stroke in this population and discusses possible alternative therapies, including hydroxyurea and bone marrow transplantation, for stroke prevention in this high-risk population. Finally, the author reviews publications on the risk associated with elevated anterior cerebral artery velocities, reports on encephalo-arterio-duro-synangiosis (EDAS) in patients with homozygous sickle cell anemia with moyamoya, and reviews the parameters that affect transcranial Doppler velocity and potentially impact stroke risk in this population. He reviews recent trials in HbSS, including SWITCH, TWITCH, and a controlled trial of transfusions for silent cerebral infarcts in sickle cell anemia. He cites the development of different gene therapies that can silence BCL11a, resulting in increased HbF levels.
|
• Children with sickle cell disease have an 11% risk of developing stroke by age 20 years. Of these strokes, 75% are ischemic and occur in patients with severe stenosis of the terminal internal carotid artery or proximal middle and anterior carotid arteries. | |
|
• Transcranial Doppler can identify those children at highest risk of developing stroke. | |
|
• Prophylactic chronic transfusion to maintain HbS levels of less than 30% decreases stroke risk by 90%. | |
|
• Because of the potential complications of long-term transfusion (risk of infection, alloimmunization, and iron overload), other therapies, including hydroxyurea and bone marrow transplantation, are currently being evaluated, but to date none have been as effective as transfusion. |
In this article, the term “sickle cell anemia” will refer to those cases homozygous for hemoglobin S. Other sickle hemoglobinopathies will be referred to by specifying the abnormality as appropriate (eg, HbSA [sickle cell trait], HbSC, HbSD, HbSE, etc.).
Sickle cell disease was first reported in 1910 by Herrick (95). In 1923, a young patient with sickle cell disease who suffered a stroke was reported by Sydenstricker and colleagues (213). Since those early observations, much has been learned about sickle cell disease through laboratory and clinical studies. These studies have established it as a genetic disease with autosomal dominant inheritance in which the abnormal gene product is an altered beta chain in the structure of hemoglobin (196). Most of the hemoglobin in the red cells in adults exists as a tetramer of two alpha and two beta chains. A change in the amino acid sequence of one of the globin chains gives rise to hemoglobinopathies, whereas decrease in quantity of globin chains causes the thalassemias. The major sickle hemoglobinopathies are categorized as sickle cell trait (Hb SA) (one normal beta-globin and the other a sickle beta-globin), sickle cell (Hb SS) (both beta-globins are sickle beta-globins), and sickle C hemoglobin (Hb SC) (one sickle beta-globin and the other C beta-globin).
In their 1949 article entitled “Sickle Cell Anemia, a Molecular Disease,” Pauling and colleagues demonstrated the significant differences in the electrophoretic mobility between sickle cell hemoglobin and normal hemoglobin, which was an observation that was important in the development of the concept of the molecular basis of disease (165). In 1956, Ingram demonstrated that patients with HbSS had a substitution of glutamic acid for valine at position six of the beta globin chain (110). This was found to be the result of an A to T transversion in the codon for amino acid 6 in the Beat-hemoglobin gene (Ingram). Deoxygenation of HbS may cause a transformation from a soluble compound to a densely packed polymer; this polymer is a series of parallel bundles of long fibers that align with other fibers, distorting the red cell shape from a biconcave disc to the crescentic or sickle shape. Depolymerization usually occurs with reoxygenation (51). Patients with HbSS have an ongoing hemolytic anemia, with average red blood cell life span of 10 to 20 days. Most patients maintain a hematocrit of 20 to 25.
Stroke was recognized early on as an important complication of sickle cell disease (104). The series of Greer and Scotland, as well as that of Portnoy and Herion, were the first to emphasize the high prevalence of cerebrovascular disease in sickle cell disease (83; 174). The most comprehensive study of stroke comes from the Cooperative Study of Sickle Cell Disease (CSSCD), which reported the prevalence of stroke in children to be 0.5% to 1% per year, for a total of 11% by 20 years of age (160). Other studies have confirmed this high incidence of stroke in children with sickle cell (181). This rate of stroke is extremely high, particularly when compared to the 2.5/100,000 yearly incidence of stroke in children without sickle cell disease (69), and is comparable to that of moderately high-risk elderly adults.
It has been estimated that in 2005 the United States HbSS population was over 89,000 people, with a total estimate of 89,079 (95% CI: 88,494 - 89,664) people with sickle cell anemia in the United States, of which 80,151 were black and 8928 Hispanic (32). Sickle cell disease has a high morbidity and mortality. There has been a significant increase in life expectancy for patients with HbSS over the last 50 years. Platt and colleagues reported that based on Cooperative Study of Sickle Cell Disease (CSSCD) data for 1313 females and 1229 males with HbSS followed from 1978 to 1988, the average life expectancy for males was 42 years, and for females 48 years (173). They cited Diggs, who estimated, based on an autopsy review, that patients with HbSS had a median survival of 14.3 years, with 20% of deaths occurring in the first two years of life, one third before the fifth year of life, half between 5 to 30 years, and one sixth after 30 years of age (48). A review of Medicare and Medicaid beneficiaries reported a current life expectancy of 52.6 years for patients with HbSS in the United States (111).
It has been reported that during the study period from 1999 to 2009, the greatest decline in sickle cell disease-related mortality rates occurred in children in the 1 to 4 year age group when compared to years 1979 to 1998 (decrease of 67% from 1.3/100,000 in 1979-1998 to 0.4/100,000 in 1999-2009). Significant declines in sickle cell-related mortality occurred in all pediatric groups up to age 19, with decreases of 61% for children age 0 to 1 year, 35% for children age 5 to 9 years, 33%for children age 10 to 14 years, and 22%for those age 15 to 19 years. This improved survival has been attributed to neonatal screening, early initiation of penicillin prophylaxis, and pneumococcal vaccinations, especially the current ones for invasive pneumococci. Transcranial Doppler screening was also thought to have perhaps contributed to the decline (85). Quinn and colleagues have reported similar findings for the Dallas Newborn Cohort, where 93.4% of children with HbSS survived to 18 years of age (182).
Sickle cell disease. Although the clinical manifestations are highly variable, typically, sickle cell disease presents early in life as a severe hemolytic anemia punctuated by painful episodes involving the extremities and bones ("vaso-occlusive crises"), bacterial infections, and cumulative organ damage due to infarction. It can present as an acute chest syndrome resembling pneumonia, which can be lethal according to the severity and etiology of the event (80; 225). In addition, systemic effects include retardation of cognitive and physical development (211; 196; 40; 156; 229; 203). Some of this clinical variability may be related to specific haplotypes. There are three major different haplotypes (Benin, Senegal, and Bantu), with Bantu tending to have more severe clinical manifestation, and Senegal the least severe (176).
Ischemic cerebrovascular disease. Cerebral infarction accounts for 75% to 80% of strokes in sickle cell disease. It typically presents with the sudden onset of symptoms of acute hemispheric dysfunction including hemiparesis, altered speech or aphasia, and hemisensory and visual deficits without alteration of consciousness (104; 177; 10; 166). Seizures, which are frequently focal at onset, occur in approximately 20% of cases and should alert the clinician to the possibility of cerebrovascular disease. Most strokes are not preceded by recognizable transient ischemic attacks; it should be recognized that transient ischemic attacks may be underidentified in young children because recognition and reporting of symptoms may be incomplete. Stroke and other neurologic problems may follow acute chest syndrome. Vichinsky reported in a series of 671 hospitalizations of 538 patients for acute chest syndrome that 11% of patients presenting with acute chest syndrome developed stroke or other neurologic complications while hospitalized (225). Of this 11%, 53% (59 cases) were nonspecific altered mental status. Eleven percent (6) was for seizures, and 8% (5) was for neuromuscular abnormalities. There were three cases of intracerebral hemorrhage, three cases of infarction, and three cases of diffuse anoxic ischemic injury. Publications have identified that bone marrow necrosis may result in fat embolism to the lungs, as well as to the brain, and bone marrow might be the cause of at least some of the cases of “altered mental status” in the acute chest syndrome population.
Almost all of the ischemic strokes occur in the anterior circulation, in the territory of the internal carotid artery and its branches. There are only rare reports of infarction in the posterior circulation territory. Clinically overt stroke is usually caused by stenosis or occlusion of the distal internal carotid artery and/or the proximal middle cerebral and anterior cerebral arteries (ACA). The pattern of stenosis is similar to that seen in moyamoya. These stenoses are typically distal to the posterior communicating artery so that the posterior communicating artery cannot provide collateral flow from the posterior cerebral artery (PCA) into the distal internal artery. The stenoses in the proximal ACA or middle cerebral artery usually prevent effective collateral flow from the opposite internal carotid artery through the ACA and the anterior communicating artery. As a result, most of the collateral flow is provided via leptomeningeal collaterals. There are potential leptomeningeal collateral connections at the borderzone between the MCA/ACA, MCA/PCA, and ACA/PCA. The collateral flow is through the PCA to its termination at the borderzone with the ACA or middle cerebral artery; the flow is then into the terminal middle cerebral or ACA, with retrograde flow across the cortical branches of the MCA and ACA. Infarction may occur when the decrease in flow from the stenosis proceeds at a rate faster than the rate of development of increased flow through the leptomeningeal collaterals. This progression could be secondary to rapid progression of the underlying pathology or to thrombus formation at the site of the stenosis. Worsened anemia or hypotension may trigger stroke in patients with severe stenosis as a result of worsening hemodynamic failure. Moyamoya vessels may develop in association with the intracranial stenoses and may be the site of hemorrhage later in the course of this disease.
Although most of the ischemic strokes in sickle cell disease occur in patients with stenosis of the distal internal carotid artery, proximal middle cerebral artery, or proximal posterior cerebral artery, there are some reports of stenosis in other locations. Gorman and colleagues reported four cases identified by submandibular transcranial Doppler (82). Two of the cases were cavernous internal carotid artery stenosis found on MRA TCD (so it is not clear how they were identified by extracranial TCD), and two were extracranial internal carotid artery stenosis. It is not clear from this report whether the stenosis seen in the extracranial internal carotid artery, approximately 4 cm distal to the ICA bulb (a site typical for carotid artery dissection), could have been the result of internal carotid artery dissections and not related to the homozygous sickle cell anemia (HbSS). Sharma reported on a single case of a web-like obstruction in both ICA bulbs. The patient had a left-sided weakness and moyamoya changes in the right ICA. The web in the left internal carotid artery was asymptomatic and presumably congenital. Verlhac and colleagues studied the extracranial internal carotid of 435 stroke-free children with HbSS, average age 7.8 years, with a 2 MHz ultrasound probe (221). Extracranial arterial tortuosity was seen frequently and was found in 33% of the boys and 18% of the girls. TAMM of greater than 160 cm/sec was found in at least one internal carotid artery of 45 of 435 patients. Five of these 45 had abnormal TCD exams, whereas 40 had normal TCDs. Low hemoglobin concentration and tortuous arteries were strongly associated with the velocities of greater than 160 cm/sec. Time of flight MRA was performed on 104 of 435 patients. The authors state the MRAs were performed routinely every two years on all children older than 5, as well as on all children found to have tortuous arteries. They reported that there were 63 extracranial stenosis patients, of whom 38 had less than 50% stenosis, 18 had 50% to 69% stenosis, and seven had 70% to 99% stenosis. They reported that the mild stenosis were associated with lower TAMM velocities than the severe stenosis. Time of flight MRA tends to overestimate stenosis, especially where there is turbulent flow, which may be caused by tortuous vessels. Therefore, it is difficult to know if the MRA stenosis measurements are accurate. The authors did not provide comparison data from their lab on the prevalence of tortuosity in normal children. Weibel and Fields reported on 2453 angiograms in 1407 patients ranging in age from 6 weeks to 81 years (235). They noted unilateral tortuosity in 223 cases and unilateral tortuosity in 105 cases. They noted that tortuosity was most prevalent in children, and their discussion suggested this was developmental in origin.
In an article addressing some of the issues of MRA TOF overestimation of stenosis, Strumph and colleagues, using a standardized MRA protocol with shorter echo times, higher field strengths, and increased voxel size, reported that of 10 patients initially classified as severe stenosis, five were reclassified to less stenosis (209). Ten patients with cerebral vasculopathy were scanned with both the older and newer protocol. They reclassified five of 10 patients to lower severity stenosis and found decreased severity of stenosis on MRA in six of 10 patients. The authors noted:
|
“One disadvantage of non-contrast MRA is the potential loss of flow related signal in regions of arterial tortuosity and/or branching, which are commonly present in patients with SCA, and the possibility for this artifact to simulate arterial stenosis. The possibility of artifactual stenosis is especially problematic in SCA, as the regions typically affected by artifact on non-contrast MRA overlap with the regions typically affected by sickle cell-related vasculopathy. Use of short-TEMRA techniques (ideally less than 5 ms) can be implemented to limit the artifactual loss of flow-related signal, and thereby more accurately assess the true patency of intracerebral arterial vessels. Increasing voxel size can increase SNR and improve the clarity of the images in order to better visualize vessels. Additionally, higher field strength also increases the SNR leading to less noise; however, it has the disadvantage of worsening dephasing flow artifact.” |
Deane and colleagues used 6 to 9 MHz ultrasound to examine the extracranial ICAs of 236 children with HbSS (43). They reported that 14 children had tortuous arteries, an additional nine had stenosis, and four had occlusion. They reported that most of their patients with extracranial stenosis also had intracranial stenosis.
Verlhac and colleagues has reported on extracranial carotid findings in a series of 54 HbSS patients who had had a clinically indicated MRI with MRA of head and neck during childhood or adolescence, with a follow-up scan after the 18 years of age (222). To be included in this retrospective review, patients also had to have undergone Doppler examination of the extracranial internal carotid (via a submandibular approach with a 2 MHz probe with color imaging) and transcranial Doppler of the intracranial arteries, and they had an averaged mean time of the maximum velocities of greater than 160 cm/sec. Verlac and colleagues stated that kinking (defined as a sharp bend of the internal carotid pathway with an acute angle less than 90 degrees between the two segments of the kink) was found in 72% of those studied. By velocity criteria they stated that a stenosis was noted in 48 of 54 children. They stated that at follow-up kinking was still present in 39 patients, with a decrease in the angulation of the kink in 24 patients, no change in 18, and worsening in 12. It should be noted that tortuosity of the extracranial carotids is very common. Weibel and colleagues reported that on angiography, six of 15 (40%) children who underwent bilateral carotid angiography, and 10 of 23 (43%) who underwent unilateral angiography, had tortuosity, coiling, or kinking; therefore, tortuosity is common in young patients (235). These authors also reported that in this group there were three cases of carotid web.
An article describes 167 children and young adults with HbSS who had MRA of the head and neck (193). They report 20 with intracranial stenosis. Nine of these were reported to have concurrent extracranial stenosis. The images demonstrate “compensatory narrowing” (vascular remodeling due to low volume flow proximal to the internal carotid artery, severe stenosis, or occlusion, and not actual stenosis) (76). It has been difficult to determine if the reported extracranial stenosis are focal stenosis, or if they represent similar “compensatory narrowing” to the internal carotid artery due to a chronically reduced flow secondary to severe stenosis or occlusion of the distal internal carotid artery.
There are a few case reports of posterior reversible encephalopathy (PRES) (also referred to as reversible posterior leukoencephalopathy syndrome, RPLS) developing in patients with HbSS (98; 94; 67; 124). PRES/RPLS is thought to represent the imaging characteristics of hypertensive encephalopathy, with increased water content (edema) seen mostly symmetrically in the posterior (parieto-occipital) parts of the brain and involving both gray and white matter. Further, it is thought to represent a process in which the blood pressure exceeds the arteriole’s ability to autoregulate blood flow, and flow into the vascular bed is unrestrained, with leakage of fluids out of the arterial system into the parenchyma (edema). With severe hypertension, the abnormalities may spread more anteriorly. The clinical presentation is variable and may include headache; depressed level of consciousness; visual disturbances, including cortical blindness; seizures; and, occasionally, focal weakness. As the name suggests, this is usually a reversible process, although more severe cases may develop infarction or hemorrhage. There is no specific level of hypertension at which this phenomenon develops; its development seems to be related to a marked rise from the patient’s baseline blood pressure. Treatment of the hypertension is usually effective in reversing this phenomenon. A report of children with HbSS who underwent hematopoietic cell transplantation found that 22% of those treated with calcineurin inhibitors developed PRES; all of these cases had hypertension (73). Those cases who developed PRES had a lower survival rate (74% vs. 94%) and lower disease-free survival (67% vs. 94%) than those who did not develop PRES.
Children presenting with cerebral infarction often show CT or MRI evidence of previously undetected brain lesions. Neurologic exam of those children clinically recognized as having a stroke usually shows some degree of hemiparesis. Although motor symptoms typically improve, patients (especially children) are left with significant cognitive deficits (90; 40; 17). Bilateral infarctions may be devastating, leaving patients with pseudobulbar palsy. The vast majority of strokes occur in the internal carotid artery distribution. Posterior circulation syndromes are unusual but have been reported. Death after cerebral infarction is rare.
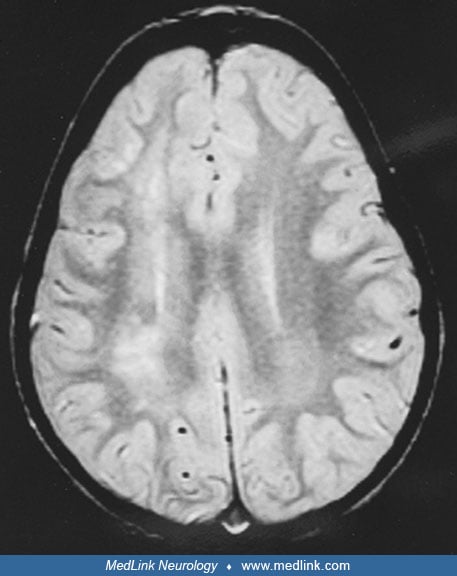
MRI detected abnormalities, referred to as silent or hyposymptomatic brain infarction, have been detected in 10% to 20% of sickle cell disease patients (52; 167). The CSSCD performed MRI screening on 312 patients above the age of 6 years and found that 17% of patients without a history of stroke had MRI lesions thought to be consistent with ischemic injury (150). These lesions have been referred to as "silent infarcts" (150). These “silent infarctions" were defined as small (less than 0.5 cm, accounting for 28% of silent infarcts), medium (0.5 to 1.5 cm, accounting for 61% of silent infarcts), and large (greater than 1.5 cm, accounting for 11% of silent infarcts). The majority of these small lesions occurred in the frontal and parietal lobes. Previous studies that relied on a focal neurologic abnormality or a history of a neurologic complaint or event probably underestimated the frequency of cerebral infarction. Special testing reveals abnormalities not evident on routine neurologic examination (146; 27). The CSSCD performed neuropsychological testing on 135 children ages 6 to 12 years along with MRI imaging of the brain (17). The nine children (6.6%) who had a history of stroke all had abnormal MRI and neuropsychological testing. The 21 children (15.6%) who had no stroke history but did have silent infarcts found on MRI had scores that were lower than normal but higher than the scores of children with clinical strokes. One hundred and five children (77.8%) had normal MRI. In a subsequent report by Pegelow, 286 children with HbSS had initial MRIs at 6 years of age or older, with 229 having follow-up MRIs (170). In this report, 21% of females had silent infarcts (with most found on initial exam), and 25% of males had silent infarcts (with some continuing to develop between the ages of 6 and 10 years). Some of the increased prevalence appeared to be related to improved imaging. It should be noted that the actual pathology of the silent infarctions has not been fully defined nor has the natural history of children with silent infarcts been fully defined. Wang and colleagues reported on MRI findings of 23 children enrolled in the multicenter, randomized, double-blinded Pediatric Hydroxyurea Phase III Clinical Trial, BABY HUG, who had MRI of the brain between the ages of 10 and 18 months (231). Three children were reported to have “silent infarcts,” two in the right frontal lobe and one bilaterally in the frontal lobes. All of these were very small punctate lesions.
As a result of the concerns about these “silent infarcts,” a multicenter trial, The Silent Cerebral Infarct Multicenter Transfusion (SIT) Trial, was initiated (220). The results of this trial were reported in the New England Journal of Medicine (46). This was an interventional trial in which children with HbSS who were found to have silent cerebral infarcts on MRI were randomized to receive either blood transfusion therapy or observation (standard care) for 36 months. Inclusion criteria were age 5 to 15 years, confirmed HbSS or HbS-Beta zero Thalassemia, and at least one infarct like lesions on MRI. Patients were excluded if they had a history of clinical stroke or TCD TAMM velocities that were considered abnormal by STOP criteria, if they were on hydroxyurea, or if they were receiving regular transfusions. Per the design paper, the primary end point was to “determine whether blood transfusion therapy will limit overt clinical strokes, or new or progressive silent cerebral infarctions in children with sickle cell anemia” (36). Recruitment occurred from 2004 to 2010. One thousand seventy-four children were screened with MRI. Three hundred seventy-nine had stroke-like lesions. One hundred ninety six were enrolled (99 in transfusion group, 97 in the observation group). Exit MRIs were obtained on 185 of 196 patients. They were followed for three years. The primary endpoint was reported for 6 of 99 transfused and 14 of 97 observed. Three of the events in the observation group were transient ischemic attacks. There was no difference in the development of silent cerebral infarctions (five in the transfusion group, seven in the observation group); there was one stroke in the transfusion arm and seven in the observation arm. The specific data for the strokes have not been published; the supplementary data reported that the patents who had end points had some differences at baseline than those who did not have events: they were younger (7.8 vs. 10.2 years of age), had slightly higher TCD velocities at baseline (153 cm/sec vs. 145 cm/sec), and had slightly higher WBC count (13.1 vs. 12.1). It is not clear from this study if the patients who suffered stroke were ones at high risk (younger patients with higher TCD velocities who converted to abnormal TCD velocities and higher risk during the trial), or if the presence of silent cerebral infarction by itself identified a group at slightly higher risk of future stroke, which would not have been identified by standard measures. The authors did not report what the TCD velocities were near the time of stroke. As reported by Adams and colleagues, children with TCD velocities greater than 170 cm/sec had about a 25% risk of stroke (09). It may be that the beneficial effect of transfusion in this trial represents the beneficial effects of transfusion in children with high velocity found on TCD.
The SIT trial also reported that of the 771 MRIs with DWI performed to screen for the presence of DWI lesions, 10 had abnormal DWI, with small volume high signal lesion consistent with an acute stroke-like event. Only two had a follow-up MRI; one of these patients had an abnormality at the same site on T2 FLAIR (180).
Ford and colleagues reviewed the MRIs of 286 children in the Silent Infarct Transfusion Trial and co-registered the identified silent infarct to a brain atlas (60). They reported that 90% of the silent infarcts were found in a region in the deep white matter of the frontal and parietal lobes, in the deep border zone area. They noted that this area is only 5.6% of total brain volume and that based on their arterial spin-labeling data, this was the area of lowest cerebral blood flow. It is not clear why these patients with no large artery stenosis would have low cerebral blood flow in this region. In response to their anemia, an elevated cerebral blood flow would be expected. Alternative possibilities such as more severe anemia or altered P50 with resultant lower oxygen delivery could potentially explain these findings. In response to the anemia, the cerebral arterioles (the resistance vessels) would be expected to be dilated so that there would be less reserve to respond to worsened hypoxia or hypotension, either of which could result in inadequate oxygen delivery to this border zone territory.
Several articles have reported increased oxygen extraction in the “borderzone” between anterior cerebral and middle cerebral artery in the deep white matter. However, a publication has reported significant differences in oxygen extraction fraction based on the assumptions used in the specific model (139). This article demonstrates that although MRI can be used to estimate oxygen extraction fraction, there are a number of issues that have yet to be resolved. In a small study of 21 HbSS patients and seven controls, it was found that patients with HbSS had higher cerebral blood flow than controls and a normal oxygen delivery rate. They used four different models to estimate oxygen extraction fraction. Using sickle specific calibrations they found a decreased oxygen extraction fraction and CMRO2 in HbSS patients, when using a different model they found opposite results with higher oxygen extraction fraction and lower CMRO2. They noted that it was not possible to definitively identify which model measured the actual physiology. It appears that the MRI-based oxygen extraction fractions will need to be validated by other measurement technology, such as PET.
An article on the effect of chronic transfusion in symptomatic patients reported on 40 children with HbSS who had clinical strokes and who had been enrolled in chronic transfusion protocols (105). Forty patients were studied. The median age at stroke was 5.4 years, with median follow-up from stroke of 5.5 years (range 2 to 15 years of age). Thirty-seven had serial MRIs. Seven had clinical strokes during follow-up. Eight developed silent infarcts during follow-up. At baseline, 25 of 40 (63%) had MRA-detected vasculopathy. During follow-up, five patients developed vasculopathy who did not have it at baseline, and 10 others had progression of their stenosis.
Pegelow reported that children with abnormal transcranial Doppler who had silent infarcts but did not receive transfusion had a higher risk of future stroke than those who were transfused (171).
In a retrospective study of 37 children with HbSS who had undergone MRI of the brain between 7 and 48 months of age, and who had been followed for an average of 14 years, 22 of 37 were found to have silent infarctions during follow-up (35). Ten patients were under the age of five years when they were first found to have silent infarctions. Three of the 10 developed stroke, two had transient ischemic attacks, and one died of splenic sequestration. Six of nine developed MRA stenosis or progressive MRI abnormalities. Of the 12 whose first silent infarction first developed after the age of 5, one had a stroke and one had a transient ischemic attack. Four developed MRA stenosis, and two had progressive MRI abnormalities. It was the authors’ suggestion that children with HbSS have a screening MRI/MRA examination prior to the age of 6. The authors recognized that there is currently no recognized effective therapy for silent infarcts.
Steen and colleagues from Memphis published a number of articles on MRI in sickle cell disease, suggesting that with the use of newer imaging techniques, the incidence of MRI abnormalities may be even higher than previously reported. They reported that up to 46% of patients with sickle cell disease had “brain injury” (cystic infarction, encephalomalacia, atrophy, or leukoencephalopathy). Some of the abnormalities that were reported by this group, such as arterial tortuosity and differences in T1 from those found in an age-matched population, are of unknown significance (202; 205; 204). Many subsequent publications have continued to label arterial tortuosity as abnormal, but there are no data to support any pathologic consequence of this tortuosity. Additionally, Steen reported on detailed MRI and neuropsychological testing of 54 children with HbSS, compared to age, race, and gender-matched controls (203). There were 30 children with normal MRI and MRA; when they were tested with the Wechsler Intelligence Scale for Children III, they performed more poorly on all tests than the controls, with an average score of 12 less than the controls for full-scale IQ, verbal IQ, performance IQ, verbal comprehension, perceptual comprehension, freedom from distraction, and processing speed. Interestingly, he did not find any difference in scores of children with HbSS who had normal MRI and MRA and those with what he described as abnormal MRI and MRA. There are many potential reasons for these children to score lower on IQ tests, including parental educational level, socioeconomic status, missed days of school, and nonrepresentative sample. Berkelhammer reviewed most of the published series on neuropsychological assessment in children with stroke (23). A review and meta-analysis of IQ in children with sickle cell documented, again, that children with sickle cell and no apparent brain abnormality on MRI had significantly lower IQ than age-matched healthy controls (121). Prussein and colleagues reviewed literature on variables that may affect cognitive function and identified hemoglobin and hematocrit, transcranial Doppler velocities, and socioeconomic status; he concluded that “the findings provide evidence for biological, environmental and psychosocial correlates across multiple domains of cognitive function in sickle cell disease” (178).
Chen and colleagues identified yet another potential contributor to the issue of IQ in children with HbSS (38). The authors studied 31 children with HbSS who had no evidence by MRI of signal intensity abnormalities and who had transcranial Doppler time-averaged mean maximum (TAMM) velocities of less than 170 cm/sec. Based on the results of the Kauffman Brief Intelligence Test the children were split into two groups, high and low IQ. All of the children underwent T1 MRI, which was analyzed using Graphical-Model-Based Multivariate Analysis (GAMMA) to assess the likelihood of association between IQ score and regional gray matter volume. The authors reported that children in the low-IQ group had smaller regional gray matter volume in both frontal lobes, both temporal lobes, and both parietal lobes. This finding suggests that some variance in intellectual ability in children with sickle cell disease is accounted for by regional variability of gray matter volume, which is independent of neuroradiological evidence of infarct.
Vichinsky and colleagues reported neuropsychological assessment of 160 neurologically asymptomatic, medically healthy African-American adults with sickle cell disease compared to 52 African Americans with hemoglobin AA, matched for age, gender, education, and benign medical history (226). The mean WAIS-III performance IQ was 86.69 for those with sickle cell and 95.19 for the control population; 33% of the sickle cell group versus 15% of controls had IQ scores less than 85. As part of this study, MRIs were performed with detailed measurements of intracranial volume, cortical gray matter, and white matter hippocampal volume. There was no difference in MRI measurements of cortical gray matter or hippocampal volume between the sickle cell patients and the controls. The study defined lacunes as lesions at least 5 mm in diameter and reported that they were present in 33% of sickle cell patients and 2% of controls. After adjustment for age, there was no relationship between WAIS IQ and the presence of these lacunes. Anemia and age were related to performance IQ, particularly for those over 40 years of age. Another publication documenting the effect of hemoglobin on executive function studied 37 children with HbSS, ages 6 to 18, and found that there was no association between transcranial Doppler velocities, or the presence of “silent infarcts,” and neurocognitive functioning (97). The authors did report that the more severe the anemia, the worse the patients performed on memory testing. Hood and colleagues compared three groups of children and young adults: two groups with HbSS (27 on chronic transfusion, 34 on hydroxyurea) and a group of 41 non-sickle cell demographically matched controls (99). Each group was tested twice 3 to 7 weeks apart. The patients on transfusion were tested 3 days after transfusion, then 3 to 7 weeks later. There was significant improvement in executive function following transfusion, correlating with the rise in hemoglobin concentration. When retested at 3 to 7 weeks posttransfusion, the executive function had declined to that of the HbSS cases on hydroxyurea.
Two articles have raised the possibility that there are causes other than silent infarct that could explain cognitive impairment in patients with HbSS. A study from the Neuropsychological Dysfunction and Neuroimaging Adult Sickle Cell Anemia Study Group reported on the MRI findings in 120 neurologically asymptomatic adults with HbSS with no history of neurologic dysfunction and compared them to the MRI findings in 33 healthy controls (HCs) who underwent MRI scanning using 1.5-tesla scanners on various platforms across the 12 sites. The imaging sequence used for volumetric analyses was a 3-dimensional T1-weighted image magnetization-prepared rapid acquisition gradient echo (MP-RAGE) or spoiled gradient recalled echo. The image processing was performed using FreeSurfer version 4.5, a fully automated image-processing suite that can provide measurements of cortical thickness and tissue volume in 116 total cortical and subcortical regions of the brain. The primary regions of interest for this study included volumetric measurement of the basal ganglia and thalamus, thickness of the frontal lobe cortex, volume of white matter hypointensities, and the presence of lacunes. After adjustment for age, sex, education level, and intracranial volume (ICV), comparison of the MRI regions of interest between participants with HbSS and the HCs found that participants with HbSS exhibited thinner cortex of the frontal lobe and smaller basal ganglia and thalamus volumes; these smaller volumes were present in the caudate, pallidum, putamen, and thalamus. When compared to HCs, patients with HbSS also had thinner cortex in the temporal lobe and parietal lobes. The two groups did not differ on occipital lobe thickness. There was no significant difference between patients with HbSS and the HCs on presence of lacunes or volume of white matter hypointensities. When patients with lacunes were removed from the analysis, white matter hypointensity volumes were not found to differ between the two groups (neither group had a greater burden of white matter changes based on volume measurements or visual rating of white matter changes). Based on these findings, it was the authors’ opinion that the observed abnormalities in cortical and subcortical gray matter structures were not primarily the result of cerebrovascular disease. Their conclusion suggested that (1) patients with HbSS who were neurologically asymptomatic had evidence of cognitive dysfunction; (2) there did not appear to be any difference in age effect on performance between HbSS patients and HCs; and (3) the cognitive dysfunction seen in this study population of patients with HbSS could not be explained by cerebrovascular lesions. It was their interpretation that the study’s findings indicated that the MRI detected structural brain differences that potentially contributed to cognitive dysfunction in sickle cell anemia (141).
Another group has reported a retrospective study on MRI volumetric measurements of cortical thickness and deep gray matter (122). They studied 26 patients with HbSS (13 with strokes) compared to 20 controls. They used a 3-dimensional fast low angle shot (FLASH) sequence to acquire their images. They also reported somewhat different findings than reported in Mackin’s article. They did report smaller volumes for total subcortical gray matter, but no difference in thalamic volumes. They also found smaller volumes in the hippocampus, amygdala, and cerebellar cortex. This study had a small number of patients. It was not clear how the inclusion of the patients with a history of stroke affected all of the measurements. However, this study also found structural differences between patients with HbSS and controls (122).
Intracranial hemorrhage. Less common than infarction, intracranial hemorrhage tends to occur in older patients and is usually manifested by sudden severe headache with alteration of consciousness, with or without focal findings (177). Hemorrhage is more likely than infarction to be fatal. In the CSSCD, nine of the 11 fatal strokes were hemorrhages, and the other two were undetermined; there was a 26% risk of death from intracranial hemorrhage (160). The clinical presentation depends on whether bleeding is subarachnoid, intraparenchymal, or intraventricular. Convulsions and coma suggest massive subarachnoid or intraventricular bleeding. Parenchymal bleeding is usually subcortical and presents with depressed alertness or stupor and focal findings (03).
Meningitis. Patients with sickle cell disease are prone to meningitis especially due to pneumococcus (190). Although the presentation is usually different from stroke, meningitis should be considered when acute central nervous system abnormalities are present in this population.
The prognosis for survival after stroke in sickle cell disease depends on the lesion. Cerebral infarction has a low mortality rate, whereas intracranial hemorrhage causes death in more than 50% of cases. Patients with infarctions, especially children, tend to recover motor function but have cognitive sequelae (90; 159). Other complications of ischemic stroke include seizures, spasticity, and delayed hemorrhage (176). Morbidity associated with intracranial hemorrhage depends on location and is similar to what may be expected in such cases in the absence of sickle cell disease. Intraventricular hemorrhage with clot in the third ventricle is an especially important condition to recognize because these patients may initially have a relatively normal neurologic examination but rapidly deteriorate due to the development of acute hydrocephalus. Cortical venous and sinus thrombosis have also been reported (158); in patients with clinical suspicion, a magnetic resonance venogram is recommended.
Case 1 (pediatric). MD was a girl of African descent who was found to have sickle cell anemia on newborn screening. She was neurologically well until she was 8 years old, when she awoke with weakness in her left leg. Her physical examination and vital signs were unremarkable. Her neurologic examination revealed a flattened left nasolabial fold and a moderate left hemiparesis. Reflexes were normal, and there was a Babinski sign on the left. A cranial CT scan revealed small infarcts adjacent to the right frontal horn. Although her baseline hemoglobin and hematocrit were typical for a child with sickle cell disease (Hemoglobin=7 to 8 grams/dl, hematocrit 22% to 24%), her admission hemoglobin was 4.9 gm/dl, and hematocrit was 14%. She received a transfusion, which brought the hematocrit to 32%. She had been screened with transcranial Doppler as part of a research study three months prior to her stroke (this was prior to the STOP trial). Transcranial Doppler showed a normal velocity for her age and hematocrit on the left but an elevated velocity in the internal carotid artery on the right (246 cm/sec time averaged mean of the maximum velocity). The patient had a brain MRI and a cerebral angiogram showing infarction in the right middle cerebral artery territory and a high-grade internal carotid artery stenosis on the right.
The patient’s strength improved considerably, and she was entered on a chronic transfusion program receiving 10 to 15 cc/kg packed red blood cells every 3 to 4 weeks. Chelation with deferoxamine was initiated three years later. At 15 years of age, she had had no further clinical stroke symptoms and no new brain lesions on MRI.
This case illustrates several typical features of pediatric sickle cell disease stroke including a typical age of onset and presentation, abnormal large arteries as indicated by transcranial Doppler before and angiogram after stroke, and a relatively good course after being started on transfusion. Her low hemoglobin and hematocrit on presentation, although not typical, has preceded stroke in some cases. If a child with HbSS has preexisting intracranial stenosis, a drop in hemoglobin, which often occurs in association with infection, could trigger symptomatic brain ischemia.
Case 2 (adult). SB was a woman of African descent who was diagnosed with sickle cell anemia at 5 years of age. She had no history of neurologic illness until she was admitted for one of her frequent pain episodes at the age of 20 years when she was noted to have difficulty with speech and right-sided weakness. A CT scan showed a subacute left temporal lobe infarction. She received transfusion and was treated with aspirin. Her transcranial Doppler revealed elevated velocities in the middle cerebral arteries, especially on the left side. She had an MRI that showed a large left temporal infarct.
Her symptoms improved in 15 days with some mild residual expressive aphasia and right hemiparesis.
She had recurrence of right hemiparesis and expressive aphasia one month later. A workup for hypercoagulable state, elevated homocysteine, and antiphospholipid antibodies was negative. A cerebral angiogram showed narrowing of the middle cerebral artery without moyamoya.
She received transfusions and was placed on warfarin, but compliance was poor. She became pregnant, and her anticoagulation was changed to low molecular weight heparin. After an uneventful delivery, she was switched back to warfarin but had another recurrent stroke one year later. She received an encephaloduroarteriosynangiosis (EDAS) in which the left superficial temporal artery was laid over the exposed cerebral cortex. The patient had a relatively uncomplicated hospital course and was discharged on low molecular weight heparin. She returned three months later with a small recurrent infarct on the left.
This adult case is unusual in several respects. It is unusual to have an adult with no prior history of stroke present with a new stroke. Adults with sickle cell disease have intracranial hemorrhage as often as infarction. This patient also had recurrent strokes despite receiving transfusion and treatment with two other therapies. There is little experience with warfarin in these cases, but it was chosen because of its possible benefit on intracranial stenosis. When this did not work, a surgical procedure was tried based on its use in moyamoya disease.
The two cases illustrate that although prevention of stroke in children with sickle cell disease is now well established from primary prevention with transcranial Doppler screening and prophylactic transfusion to effective secondary prevention, the prevention of stroke in adults is much less well established.
The majority of clinical ischemic strokes in sickle cell anemia are caused by progressive stenosis of the distal internal carotid artery and/or the proximal middle cerebral and anterior cerebral artery. The exact cause of the stenosis has not been determined. A number of factors potentially play a role, including high flow vasculopathy, severity of anemia, cellular adhesion molecules, presence of dense red blood cells, nitric oxide depletion, and a number of other factors that may contribute to the development and progression of this stenosis. To date, there have been no pathological correlations with the small high-signal lesions that are identified as silent infarcts. The actual cause of these high-signal lesions is unknown. They are postulated to be small infarctions. Children who develop moyamoya have ischemic strokes early and may begin to have hemorrhages later.
Most early authors thought that sickled erythrocytes clogged smaller arteries or arterioles of the brain in a manner analogous to what was believed to occur in other organs (19). However, early observations by Bridgers showed obliteration of large and small cerebral arteries and infarction patterns involving a range of arterial territories (30). After Stockman and colleagues showed large vessel stenosis on angiography, more attention was paid to the contribution of large arterial disease causing most of the clinically evident cerebrovascular syndromes (208; 192). At least 80% of strokes can occur in association with stenosis of the distal internal carotid, proximal middle cerebral, or anterior cerebral artery.
It is difficult to relate the essential pathology of sickle cell disease (the formation of hemoglobin polymer strands within the erythrocyte, causing profound distortions of shape and deformability) to the development of vascular lesions causing stroke. Sickled cells do not pass well through the microcirculation, but the simplistic notion that this is the cause of stroke is inadequate because, typically, the stenosis develops in the large arteries which have diameters much larger than the erythrocyte. The cause of stroke is probably multifactorial. It may be that the high velocity flows in these children set the stage for the development of the vasculopathy and that the addition of other processes is required to trigger the actual development of the stenosis. Some work has focused attention on a possible key role for the coagulation system. In this view, the initiating event is injury to endothelium followed by loss of the thromboresistant properties of the endothelium and either gradual formation of clot or acute blockage of vessels by thrombus (62; 96). A possible coagulopathic state with significant decreased levels of both protein C and S activities has been reported (214). Liesner reported a reduction in protein C, protein S, and heparin cofactor II, and an increased production of thrombin-antithrombin complexes and fragment F1+2 levels in children with sickle cell disease, but he did not think that these abnormalities played a significant role in the development of cerebrovascular disease (138). Elevated homocystinemia in some cases may increase risk (102). However, two studies have not demonstrated any difference between stroke cases and controls in either serum homocysteine levels or for the methylene tetrahydrofolate reductase gene (20; 41). Endothelial dysfunction and stimulation of growth factors causing fibrosis may also add to the vessel stenosis associated with sickle cell disease (217). Anemia is associated with high flow rates (29; 12), which may predispose to vessel damage. However, this is unlikely to be the entire explanation because conditions such as thalassemia have significant anemia but are not known to be associated with these lesions (03). Abnormal adherence of red blood cells to vascular endothelium may also be involved (92). A number of factors may be at work to produce stroke in these patients.
A number of articles documenting elevated plasma free hemoglobin in sickle cell disease (as a result of the ongoing intravascular hemolysis) have been published (79; 149; 120). Research indicates that plasma free hemoglobin binds to nitric oxide, resulting in endothelial dysfunction and impaired vasoreactivity, and this is strongly associated with pulmonary hypertension. These authors proposed that this mechanism may also be involved in the production of cerebral vasculopathy in sickle cell disease. Several prominent sickle cell researchers have published detailed critiques of the free hemoglobin hypothesis (33; 93).
One publication would argue against pulmonary hypertension as a cause of the high-velocity tricuspid regurgitant jet (TRV) that has been the echocardiographic criteria for pulmonary hypertension (155). Niss and colleagues have attempted to address the issues of the reported high TRV on echo and pulmonary hypertension. They proposed a unique cardiomyopathy characterized by enlarged left atrial volume, evidence of enlargement of the left ventricle at end diastole with evidence of normal systolic function, but with end diastolic dysfunction consistent with restrictive physiology with superimposed hyperdynamic circulation (secondary to their anemia). They reported that only 53 of 173 (31%) patients with high TRV had pulmonary hypertension confirmed on right heart catheterization and that 40% had pulmonary artery hypertension on right heart catheterization. They proposed that this combination predisposes to sudden death from arrhythmia, as is seen in other causes of right heart cardiomyopathy. Manci and colleagues state that up to 40% of deaths in sickle cell have been reported to be unexpected or sudden and that arrhythmias could account for some of these (142).
There appears to be an increased risk of stroke in certain sibships. Driscoll reported on 207 families where more than one child had HbSS (50). There were 42 families where at least one child had a stroke; in 10 families a second child had a stroke, a frequency much higher than in the rest of the HbSS population, suggesting some genetic modifier on stroke occurrence in these families.
Kwiatkowski reported on transcranial Doppler findings in siblings with sickle cell disease (132). Of 249 children with HbSS screened over a 2-year period, there were 69 siblings from 29 families. All 42 children from 20 families had normal TCDs. Of the 21 children from nine families, with at least one child with TCD time-averaged mean of the maximum (TAMM) velocity in the distal internal carotid or middle cerebral artery of greater than 170 cm/sec, children from five families were concordant for elevated TCD velocities. The children from four of these five families were initially discordant and only became concordant on follow-up exams. The authors stated that this report supports the existence of a familial predisposition to cerebral vasculopathy in sickle cell disease. Based on their study of 230 children enrolled in CSSCD, Hoppe and colleagues suggested several candidate genes that may play a role in predisposition to specific stroke subtypes (100).
Kirkham screened 95 children with sickle cell disease with TCD and overnight pulse oximetry. They reported that 19 children (17 with Hemoglobin SS) developed strokes (seven), transient ischemic attacks (eight), and seizures (four). They suggested that nocturnal hypoxemia was an independent risk factor for stroke in this population (125). Subsequently, Setty and colleagues studied 28 children with HbSS, nine with HbSC, and 10 normal controls. They demonstrated that 15 of the 28 children with HbSS had nocturnal hypoxemia, but they found that all of the children with nocturnal hypoxemia had waking hypoxemia as well and that this hypoxia was a chronic ongoing phenomenon. The cause of this hypoxemia was not identified (197). A report from the United States did not find any relationship between sleep-disordered breathing and TCD velocities in 64 neurologically normal children with HbSS who underwent polysomnography because of a positive history of snoring (81). No data were provided about nocturnal oxygenation.
It is possible that the high TCD velocities are a marker for poor oxygen delivery to the tissue, and that in an effort to maintain adequate oxygenation, more blood volume must be delivered, resulting in higher flow velocities. The inadequate oxygenation could be secondary to hypoxia related to pulmonary dysfunction, to abnormal oxygen dissociation, or other processes. Quinn and colleagues looked at daytime oxygen saturation and its relationship to TCD velocities (183). Using a multivariate analysis controlling for patient age and hematocrit, the authors found an inverse relationship between daytime oxygen saturation and TCD velocity, and they attributed about 5% of the variability of TCD velocity to the hemoglobin saturation.
Quinn and Dowling reported on the use of near infrared spectroscopy (NIRS) to assess cerebral oxygenation. The investigators evaluated “the absolute oxygen saturation in cerebral tissue” “in the watershed zone between the anterior and middle cerebral arteries.” They studied 149 patients. One hundred and twelve were HbSS patients, or HbSS/Sβ(0). They demonstrated decreased cerebral oxygen saturation and also reported a trend for decreasing oxygen saturation with increasing age (179). It should be recognized that NIRS remains effectively unvalidated as to the exact site of measurement. In an accompanying editorial, Kato discussed these findings and attempted to put the findings into context in the complexities of oxygen saturation and oxygen tissue delivery. He noted that oxygen saturation was not necessarily the same as oxygen concentration, as the oxygen saturation of hemoglobin is not only a function of oxygen’s partial pressure, but is also affected by hemoglobin’s oxygen affinity. It is known that HbSS has low oxygen affinity. The high intracellular concentrations of 2,3-diphosphoglycerate in sickle red blood cells results in decreased oxygen affinity (increased P50), lowering oxygen saturation at any given oxygen tension. This makes it difficult to interpret whether the lower oxygen saturation in HbSS that is found not only in cerebral but also systemic measurements is partly secondary to the decreased oxygen affinity of erythrocytes (119).
Stehbens and Lie suggested that hemodynamic stresses associated with flow through curves in vessels result in localized arterial injury with intimal proliferation (206). The high sheer stress that results from the high-volume flow in sickle cell disease may set the stage for high-flow vasculopathy. Additional factors such as inflammation with release of cytokines, elevated plasma free hemoglobin, genetic predisposition, or other yet undefined factors could trigger arterial wall remodeling, resulting in stenosis.
A report identified what appeared to be two mutations that seemed to be protective against stroke. This report screened 677 children with HbSS (177 with documented stroke) with genome-wide association studies using genotype data single nucleotide polymorphisms arrays. Two mutations were identified that appeared to be associated with decreased stroke risk. This observation will need to be assessed in a larger population (59).
Hyacinth and colleagues reported that children with HbSS with abnormal TCDs had higher levels of brain derived neurotropic factor (BDNF) and platelet derived growth factor (PDGF) AA and –AA/BB than did children with HbSS who did not have abnormal TCD velocities (109). High levels of PDGF AA were associated with stroke. It is not clear if the high levels cause the increased stroke risk or if they are the result of the underlying cerebral ischemia. In a subsequent study, Hyacinth and colleagues reviewed data on blood samples from 80 children enrolled in the STOP trial (107). They compared 40 children with HbSS with abnormal TCD randomized to transfusion with 40 children with abnormal TCD on standard care. They measured biomarkers in samples from baseline, one year of followup, and study exit. There appeared to be an imbalance at baseline in many of the biomarkers, with the standard care group having higher levels of all biomarkers at baseline. There appeared to be a decline in the biomarkers in the transfusion group, but the data provided did not allow the reader to determine how much of a reduction there was, as only the comparison of values at the time of exit was presented for the nontransfused and transfused groups.
Cerebral infarction. Although the relationship to the sickled cells is obscure, symptomatic cerebral infarction is clearly related to the presence of large artery stenotic or occlusive lesions in the intracranial segments of the carotid system. On angiography, the most commonly affected sites are the supraclinoid internal carotid artery and the proximal middle and anterior cerebral arteries. The vertebrobasilar system and the posterior cerebral arteries are affected only rarely. Abnormalities may extend to medium and small arteries as well (75). At pathology, the proximal lesions show relatively normal media and adventitia but splitting and reduplication of the internal elastic lamina and the apparent accretion of fibrotic tissue on the lumen side (191; 129; 217). This material has been variously described as endothelial hyperplasia, fibroblasts, fibrin thrombi, and thrombus with sickle red cells incorporated into the lesion. Acute thrombus formation may occur in the presence of minimal preexisting intraluminal disease, but this is probably rare (96). There may also be abnormal red blood cell adhesion to the vascular endothelium and altered vasomotor tone regulation (64; 92).
The precise mechanism by which infarction is produced is unknown, but it is speculated that progressive narrowing of the large vessels restricts flow, leading to hemodynamic failure; this narrowing may also create a nidus for clot formation and artery-to-artery embolism. The importance of hemodynamic failure is supported by pathological (191) and neuroradiological (11; 166) studies showing a high incidence of so-called "border zone" infarctions between major arterial territories. Patients who have severe flow-limiting stenosis, and who have impaired distal cerebral perfusion, the development of hypotension, worsened anemia, or hypoxia, could precipitate symptomatic ischemia distal to the stenosis.
There have been a number of publications using MRI assessment of cerebral blood flow, oxygen extraction fraction, and cerebral metabolic rate for oxygen (CMRO2) in patients with sickle cell disease. The reader should be aware that the MRI methodology used in these reports may result in underestimation of both oxygen extraction fraction and cerebral metabolic rate for oxygen. Initial studies in sicklers assumed that sickle blood behaved the same as normal blood and reported elevated oxygen extraction fraction values (140). Li and colleagues subsequently found that the T2 values of sickle blood were shorter than the T2s based on normal hematocrit (137). They attributed this to two possible phenomena: deoxygenated HbS tends to aggregate, resulting in a shorter T2; also the irregular shape of sickled rbcs could result in a stronger magnetic field gradient around the rbc, with resultant faster dephasing and stronger T2 relaxation. They reported that T2 calibrations built from individual sickle blood yielded higher precision in estimation of venous oxygenation, oxygen extraction fraction, and cerebral metabolic rate for oxygen and did not result in the reported 13% to 17% underestimation of these measurements. It was noted that the measured oxygen extraction fraction and cerebral metabolic rate for oxygen did not differ significantly from those of healthy individuals (137).
Although patients with intracranial disease often have compensatory narrowing of the cervical carotid artery and dilatation of the vertebrobasilar system (in response to the increased volume flow), these abnormalities are believed to be secondary to intracranial disease (135). Patients with sickle cell disease often have cardiomyopathy, but cardiogenic embolism appears to be rare. The role of sickled cells themselves is unknown. Fat embolism, the result of bone marrow infarction, may result in the acute chest syndrome and could play a role in some cases of stroke. As documented by Gibbs, not only can fat embolism be associated with stroke, but it may also be a cause for the “silent infarcts” (77). These would be infarctions, but unrelated to primary local arterial disease.
Several publications have suggested that fat embolism may be a more frequent cause of stroke and “silent infarctions” than previously recognized. A typical scenario appears to be that a patient with HbSS presents to the emergency department with pain crisis and then develops sickle chest syndrome and unresponsiveness. If the patient undergoes CT head scanning, the scan appears normal. However, neuroimaging with MRI may reveal the “starfield” pattern on diffusion-weighted imaging and multiple small, low signal lesions representing microhemorrhages scattered throughout both hemispheres and the posterior fossa (164; 215; 117; 216; 74).
Although case reports of stroke occur in patients with hemoglobin SA, sickle cell hemoglobin C, and hemoglobin CC, these appear to be isolated or rare events. There is no evidence that risk of stroke is increased in these other hemoglobinopathies.
Intracranial hemorrhage. The hemorrhage may be subarachnoid, intraparenchymal, or intraventricular. Arteriographic and pathologic investigations of patients with intracranial hemorrhage suggest several mechanisms, including the following: (1) rupture of a saccular aneurysm, or less commonly, an arteriovenous malformation; (2) rupture of intraparenchymal or periventricular "moyamoya"-like small arteries, which have developed in response to the presence of large artery occlusive disease; or (3) no large artery disease except for dilatation, leaving small vessel rupture as the presumed source (218; 10). Aneurysm development in sickle cell disease appears to be different than in the general population in that it occurs at a younger age, multiple aneurysms are more common, and there appears to be an increased incidence of posterior circulation aneurysms (161; 16; 151). Hemodynamic stress related to the increased volume collateral flow though the posterior cerebral arteries is thought to explain the high incidence of top of the basilar aneurysms seen in sickle cell disease; top of the basilar aneurysms are reported to account for up to 50% of aneurysms in HbSS patients but only 5% in nonsickle cell disease aneurysm cases (162). Intraparenchymal and intraventricular hemorrhage likely occur because of rupture of the small, dilated, moyamoya vessels, similar to what is seen in moyamoya disease (210; 127).
Other considerations. The possibly deleterious effect of chronic anemia, producing profound vasodilation and limiting the "vascular reserve" available to compensate for a superimposed stress such as hypotension, hypoxemia, or worsening anemia (“aplastic crisis”), may be important as well. This may be especially significant in children with high cerebral blood flow demands. Acute reduction in hematocrit, in the presence of restrictive large vessel lesions (159), may result in the acute development of a cerebral infarct.
There is radiological and pathological support for the finding that small vessel or microinfarcts also occur in sickle cell disease and are due to a variety of factors including occlusion by sickled erythrocytes and narrowing of arterioles (96). There have been reports of cortical venous and sinus thrombosis that may be explained by a hypercoagulable state (158).
According to the National Heart Lung and Blood Institute, sickle cell anemia is the most common inherited blood disorder in the United States, affecting about 70,000 to 100,000 Americans or 1 in 500 African Americans. About two million Americans have the sickle cell trait.
Earlier estimates of the incidence of stroke in sickle cell disease of 10% to 20% were likely influenced by referral bias (83; 174). A population study from Jamaica indicated an incidence of 7.4% by 14 years of age (21). The best estimates are from the CSSCD (160). In that study, the risk of having a stroke by 20 years of age was 11%, by 30 years of age was 15%, and by 45 years of age was 24% (although the number of patients reaching this age was small) for sickle cell disease patients and 2%, 4% and 10% respectively for those with sickle cell hemoglobin C. In the CSSCD, data were collected from 4082 sickle cell disease patients enrolled from 1978 to 1988. This long-term observational study demonstrated the incidence of first-time stroke, either cerebral infarction or hemorrhage, to be highest in early childhood, 2 to 5 years of age (1.02 per 100 patient-years), followed by 6 to 9 years of age (0.79) and falling to 0.41 between 10 and 19 years of age (160). The Dallas Pediatric Sickle Cell Program looked at 448 children who were identified by newborn screening to have sickle cell disease; in these children, long-term follow-up (average of 7.9 years; range=0.1 to 17.7 years) revealed 30 clinically obvious strokes, 27 infarcts, and three hemorrhages. Stroke-free survival at 18 years of age was estimated to be 88.5%. This 11.5% risk of developing a stroke by 18 years of age is similar to that reported by the CSSCD (181).
Cerebral infarction accounts for most strokes (75%) and is the most common cause of stroke in sickle cell disease children (177). In the CSSCD, hemorrhage accounted for 33% of first strokes in adults. The risk of hemorrhage was fairly low in children younger than 20 years of age and was highest in young adults (160).
A report examined the etiologies of stroke in adults as well as in children with HbSS (34). Of 26 children (mean age 7.1 years) with HbSS and stroke, 24 had vasculopathy-associated stroke. Of the 29 adults (mean age 32.3 years), vasculopathy was present in 12; seven had cardiac source embolism, one antiphospholipid antibody syndrome, one cocaine use, and eight were undetermined.
Clearly established risk factors for cerebral infarction in sickle cell disease are homozygous state (hemoglobin SS), young age, prior stroke (177), and elevated blood flow velocities in basal brain arteries by transcranial Doppler (09; 07; 08). Two small studies suggested that silent lesions on MRI (130) and MRA abnormalities in children with abnormal transcranial Doppler indicate an elevated risk for stroke (195). In one study, elevated systolic blood pressure was associated with recurrence of stroke in sickle cell disease (169). Miller and colleagues reported on 392 children with hemoglobin SS followed prospectively, 70 of whom had adverse events (25 were stroke). They found that children with a history of an episode of dactylitis occurring prior to one year of age, steady-state hemoglobin of less than 7 gm/dl, and leukocytosis in the absence of infection were at increased risk of the subsequent development of adverse outcomes (148). Modification of risk by degree of anemia, presence of fetal hemoglobin, minor genetic variables called haplotypes, or coexistence of alpha chain thalassemia has been reported (03). Hsu reported that children with HbSS with alpha thalassemia are less likely to have stroke and more likely to have normal transcranial Dopplers (103). He noted that these children tended to have slightly higher hemoglobin and lower mean corpuscular volume, suggesting lower levels of hemolysis. Large vessel arterial lesions (10), older age (160), prior ischemic stroke (175), and arterial aneurysms predispose to hemorrhage.
A report that used ambulatory blood pressure monitoring in a population of HbSS patients has suggested that hypertension may be much more common than generally appreciated. Ambulatory blood pressure monitoring was performed on 38 children ages 11 to 16 years. Twenty-five had HbSS (13 were on chronic transfusion) and 13 had HbSC. Patients were studied while they were free from intercurrent pain crisis or disease. Blood pressure values were classified as abnormal (ie, in the hypertensive range if the mean value, systolic or diastolic, was ≥ 95th percentile for age, gender, and height). They were classified as being within the prehypertensive range if this value fell between the 90th and 95th percentiles. Each subject was categorized as a “dipper” (decrease in average systolic and diastolic BP ≥ 10% during sleep) or a “nondipper” (decrease < 10%). Eight of 12 HbSS patients on standard care had ambulatory hypertension, and five of 13 on chronic transfusion had ambulatory hypertension. Only one patient in each group had hypertension based on blood pressure measurements in clinic. In addition, there were a significant number of patients who were nondippers in both groups. These data need to be confirmed in a larger study. If this observation is correct, the identification of masked hypertension would be another target to help reduce the risk of stroke and other vascular disease in this population (198).
When transcranial Doppler has been used to screen nonstroke sickle cell patients, studies have shown a strong predictive value for the development of stroke, with approximately 40% going on to develop stroke when the intracranial blood flow velocity (time-averaged mean of the maximum) in the middle cerebral or distal internal carotid artery was 200 cm/sec or greater (09; 07; 08). This observation was the basis for the Stroke Prevention Trial in Sickle Cell Anemia (STOP) (08), which demonstrated the feasibility of primary prevention of stroke in patients with sickle cell disease. STOP used TCD to screen children with sickle cell anemia who were aged 2 to 16 years but who had no history of stroke. Children who had transcranial Doppler with TAMM velocity of greater than 200 cm/sec in the terminal internal carotid or the proximal middle cerebral artery were offered randomization to either standard care or regular blood transfusions. Exchange or simple transfusions were allowed. The goal of transfusion was to maintain the percent hemoglobin S at less than 30%; this required transfusions approximately every 3 to 4 weeks.
STOP was halted early when it was observed that the incidence of stroke (cerebral infarction or intracranial hemorrhage) was more than 90% lower in the transfusion group. When the study was halted, there were 11 strokes in the standard care arm and one in the transfusion arm. TAMM velocities of greater than 200 cm/sec as measured by TCD proved to be an effective predictor of stroke, with a risk of 10% per year in those receiving standard care. Because the trial was halted at two years, the duration of 10% per year risk of stroke beyond 24 months is not known. A long-term observational follow-up has been reported on the STOP participants (136). One hundred and twenty-seven of the 130 participants were followed from February 1995 through June 2000. At the end of the trial, 12 patients were on transfusion therapy for stroke indications. All other participants were offered transfusion therapy for stroke prophylaxis. Of the initial 63 randomized to transfusion therapy, there were 52 who were on continued transfusion at the end of the trial (one was ineligible; only one abnormal TCD), four were never transfused, one had suffered a stroke, and five had quit transfusion). Forty-seven of the 52 opted to continue transfusion, with 40 remaining on transfusion and stroke free throughout the follow-up period. Among the five who opted to not continue transfusion, one developed stroke and was placed on chronic transfusion. Of the original 67 allocated to standard care, 12 were on chronic transfusion: 11 for stroke and one for leg ulcers. One patient was lost to follow-up. Of the other 54, two developed stroke shortly after closure of STOP and were placed on chronic transfusion. Twenty-three of 52 patients opted to initiate transfusion therapy (two of whom subsequently had strokes). One of the 29 who remained on standard care developed a stroke. All of the six patients who developed stroke post-trial had at least one abnormal TCD prior to stroke, confirming the ability of TCD to identify children at high risk for stroke.
Determining the ongoing risk will be important as it will be helpful in making management decisions, not only in deciding whether to start or maintain transfusion, but in consideration of the use of alternative therapies such as hydroxyurea, gene therapy, or bone marrow transplantation. It is unclear how long the prophylactic transfusion should be continued. There have been reports that have documented a high risk of stroke recurrence after stopping transfusion when it was used for secondary prevention (230; 184). The decision to initiate transfusion in asymptomatic patients with elevated velocities on TCD exam should be made after careful consideration of the risks and benefits, and treatment should be given in a setting experienced with transfusion and its complications.
STOP II was an NIH funded trial to determine if transfusions could be safely discontinued in the high-risk population (05). In this trial, patients were identified by high-risk TCD and transfused for more than 30 months to maintain HbSS at less than 30%; those children whose TCD velocities returned to normal, who had normal MRA, and who were willing to participate were randomized to either continuation or discontinuation of transfusion. They were followed closely both clinically and with serial TCDs. Endpoints were stroke or reversion of TCD to high risk. Of the 79 children enrolled, 41 were randomized to discontinuation of transfusion. At an average of 4.5 months after discontinuing transfusion, 14 developed high risk TCD, and two others developed clinical stroke. None of the children in the continued transfusion arm suffered an end point. Based on these results, these children who have been found to have abnormal TCDs will either have to remain on transfusion with chelation to address the iron overload issue, or alternative therapies (such as bone marrow transplantation, conversion to hydroxyurea, or others) will have to be used for long-term management.
Bernaudin and associates reported similar results in a nonrandomized study of attempted discontinuation of chronic transfusion in children with abnormal TCD velocities (26).
TCD velocities are affected by a number of variables. The interested reader should pursue more details on TCD as performed in STOP and the various factors that may influence velocity (154). There are several points to be made about TCD. TCD is an assay of blood flow physiology, measuring the velocity of flow, not the volume of flow. It does not directly provide information as to the caliber of the artery being assessed by TCD. All TCD studies should be performed in a manner similar to that used in STOP: patients should be in “steady state,” as hypoxia, fever, hypoglycemia, altered C02, and changes in severity of anemia will all cause an increase in TCD velocities. Transfusion will increase oxygen delivery and reduce TCD velocities, so screening TCD should not be performed within 4 weeks of transfusion to allow patients to return to steady state hemoglobin levels.
The STOP trial demonstrated that the TCD velocities could be used in children with sickle cell disease to predict increased risk of stroke: the higher the velocity, the greater the risk of stroke (07; 08). The velocities used in STOP refer to the time-averaged mean of the maximum (TAMM) and not peak systolic velocities. It is important to be aware of this difference, as most vascular labs use peak systolic velocities for extracranial arterial assessment.
Adams and colleagues reviewed the TCDs performed for STOP and analyzed the risk of conversion to abnormal based on the results of the first TCD (06). Overall, the risk of conversion to abnormal on follow-up TCD exam was greatest for younger patients with high conditional (185 to 199 cm/sec) velocities. One thousand two hundred and fifteen children with normal or conditional TCD exam had more than one TCD exam. The average age at the time of initial screening was 7.8 years, and the average follow-up was 22 months. A total of 114 (9%) children developed abnormal TCD during follow-up. A two year old with a normal initial TCD had a 4% risk of conversion to abnormal TCD in 12 months; a two year old with a high conditional TCD had a 50% risk of conversion to abnormal in the next 12 months. Hankins and colleagues subsequently reported a similar rate of conversion for the Memphis group (87).
Several studies have directly compared TCD with Transcranial Color Doppler Imaging (TCDI) (113; 153). In general, TCDI velocities were slightly lower than those obtained with TCD. This difference may be secondary to technical issues related to probe design and manipulation. The older TCDI probes were larger and difficult to manipulate. The newest generation of TCDI probes have smaller probe surface and are more easily manipulated. Preliminary results suggest that the newer TCDI probes are obtaining velocities closer to those obtained by TCD.
The STOP trial reported on the use of peak systolic velocities in prediction of stroke risk. This report indicated that peak systolic velocities greater than 250 predicted increased stroke risk (112).
Kwiatkowski and colleagues analyzed the contribution of anterior cerebral artery velocities to stroke prediction in the STOP trial (131). The data on 1975 patients who underwent TCD exams were reviewed. There were 65 cases of ACA velocities greater than 200 cm/sec; 20 of these 65 were patients with normal or conditional MCA/ICA velocities, and two of these 20 suffered a stroke. Of the 45 cases with abnormal MCA/ICA velocities, eight of 45 (17.8%) with ACA velocities greater than 200 cm/sec had a stroke, as compared to 18 of 159 (11.3%) with ACA velocities less than 200 cm/sec. The authors then looked at stroke risk for ACA velocities greater than 170 cm/sec. They found ACA velocities greater than 170 cm/sec in 46 of 1442 patients with normal ICA/MCA velocities, in 59 of 329 with conditional ICA/MCA velocities, and in 101 of 204 with abnormal ICA/MCA velocities. When adjusted for the ICA/MCA risk classification, patients with ACA velocities greater than 170 cm/sec had a 2.9-fold increased risk of stroke compared to those with ACA velocities less than 170 cm/sec. There were 25 strokes that occurred in patients with ACA velocities greater than 170 cm/sec (out of a total of 54 in the entire cohort); only two of these strokes were in the ACA distribution.
In an analysis of 88 children followed as part of STOP 2, it has been reported that in those children with abnormal STOP TCD who started on transfusion, the median decrease in TCD velocity was 38 cm/sec, occurring by three months after initiation of chronic transfusion (134).
A publication on long-term follow up of patients in STOP has reported on the risk of hemorrhagic stroke during follow up. Follow-up data were collected from 2850 of 3835 STOP or STOP II participants (61). At the time of the last-known status, patients (51% male) were a median of 19.1 (interquartile range, 16.6 to 22.6) years of age. The overall hemorrhagic stroke incidence rate was 63 per 100,000 person-years (95% CI, 45-87). Stratified by age, the incidence rate per 100,000 person-years was 50 (95% CI, 34-75) for children and 134 (95% CI, 74-243) for adults greater than 18 years of age. Thirty-five cases of “hemorrhagic stroke” were identified. Twenty two were subarachnoid hemorrhage, 13 were intraventricular, and 11 were intraparenchymal. Ten cases had aneurysms. Seven had moyamoya. Ten occurred during hospitalization for sickle-related complications (bone marrow transplant, sickle chest, pain crisis, and sepsis). The incidence was 50.4 per 100,000 patients under 18 years of age, and 134 for those greater than 18 years of age. The authors suggested that all children with HbSS should have a screening MRA but did not recommend an age for screening (61).
The results of STOP led to recommendations for screening children with sickle cell disease. The most crucial part of the program is TCD. One article has provided details on the technique and interpretation of TCD in the sickle cell population (154). Transcranial color Doppler has also been used to identify patients at high risk of stroke (113; 153). To date, TCD is the only technique that has been demonstrated to be predictive of stroke risk. Although there are other noninvasive methods such as MRA, these may not give the same information as TCD. Many of the children who qualified for STOP with high-risk TCD velocities had normal MRAs and would not have been identified as high risk by MRA. Abboud and coworkers, reporting on MRA findings in STOP, noted that of the 31 MRAs obtained within 30 days of randomization, 24 of the 31 were normal (01). In these 24, the average TCD velocities were 216 cm/sec; the other seven were abnormal with average TCD velocities of 277 cm/sec. MRA has shown to have a sensitivity of 80.5% and a specificity of 94% for detecting stenosis or occlusion in carotid circulation when compared with conventional angiography in symptomatic patients (116). Although it seems reasonable that screening with MRA would give potentially comparable information, data are limited on this point, and the only prospective, validated data that predict future stroke risk come from high velocity TCD. TCD might detect early flow dysregulation, and high velocities may precede and promote the formation of stenotic lesions.
Several publications have attempted to identify children at high risk for stroke by using information other than TCD velocities. One group developed an index using age, AST, and hemoglobin level and compared the index to the TCD findings (157; 186). Although this index did demonstrate statistically significant correlation with TCD velocities, with high sensitivity, the specificity was poor. Potentially, in areas where TCD is not available, this index could be used to identify a group at higher risk who could be referred for TCD.
Transfusion has been the standard of care for secondary stroke prevention. Early estimates of the risk of recurrence without transfusions were as high as 90% (192), but the rate was 47% in the Jamaican cohort study (21). The recurrence rate in the CSSCD was only 14%, but this is misleading because many of these patients were given chronic transfusion after the first stroke (160). Dobson used angiography (primarily MRA) to identify the presence of moyamoya changes in 43 patients with first stroke before 18 years of age (49). Four of 19 patients with moyamoya followed for an average of eight years had recurrent stroke on transfusion, whereas only one of 23 without moyamoya followed for an average of 4 years had a stroke on transfusion.
Secondary prevention of stroke has been accomplished, at least for recurrent cerebral infarction, through the use of chronic regular blood transfusions (192), which reduce the recurrence to 10% to 20% or less (37; 03). The maintenance of hemoglobin S at a level less than 30% appears to be effective in reducing the rate of recurrent infarction but does not prevent transient neurologic events (168).
Although transfusion decreases the risk of stroke, it appears to have little effect on established stenosis, with long-term follow-up reports indicating that some of these patients have progressive stenosis despite continued chronic transfusion therapy. Russell and colleagues reported on 30 children with HbSS with focal neurologic events who underwent cerebral angiography on at least two occasions (192). Twenty-six of the 30 children had abnormal angiograms. There were four children with abnormal angiograms who did not have transfusion. All four of these cases demonstrated progression of the arterial abnormalities, and the authors commented that “irregular vessel walls were prevalent” on the second arteriogram. In 13 patients with chronic transfusion, there was stabilization of stenosis, and “most luminal surfaces became smooth.” The authors reported that “stenosis sometimes progressed even years after apparent initial stabilization.” There were two patients whose initial arteriograms were abnormal, then normalized on transfusion, but became abnormal again after transfusion was stopped. Other studies have also noted regression, stabilization, and/or progression of arterial stenosis in patients who had moyamoya at the time of initiation of transfusion therapy. Gyang and colleagues reported that six of nine patients on chronic transfusion for secondary stroke prevention demonstrated progressive stenosis, with progression noted after an average of eight years on transfusion. The authors did not define how they measured stenosis or change over time (18; 31; 84). Using a nonvalidated MRA rating scale, Bishop and colleagues evaluated MRA in 34 patients (22 with stroke, 12 with only abnormal TCD) on chronic transfusion for an average of 6.5 years (28). They reported that eight of 22 patients with stroke demonstrated worsening of stenosis on MRA, whereas only one of 12 with abnormal TCD had worsening MRA. Thirteen of 22 stroke patients had abnormal baseline MRAs; seven of the 13 worsened. None of the abnormal TCD cases had abnormal MRA at baseline; one of these worsened during follow-up. Another study has also reported worsening of stenosis in a subset of patients despite chronic transfusion therapy. This study reported on a series of 27 patients with HbSS who were placed on chronic transfusion for abnormal TCDs; 18 had follow-up MRI/MRA during an average follow-up of 34 months. Five had MRA evidence of new or worsening arterial stenosis (199). The best management for progressive stenosis is not known. Management of recognized risk factors such as hypertension is appropriate. Statins and ACE inhibitors have been proposed by some for their “vascular protective” effects. Based on her experience, Bernaudin has recommended bone marrow transplantation in cases of progressive stenosis (24). The surgical revascularization, encephaloduroarteriosynangiosis (EDAS), may be appropriate in these patients.
There are a number of reports that the incidence of stroke in HbSS has declined significantly since the introduction of transcranial doppler screening. One report reviewed the California-wide hospital discharge database to identify all first admissions for stroke in children with HbSS, comparing the time periods of 1991 through 1998 and 1999 through 2000 (69). They documented a first stroke rate of 0.88 of 100 person-years during 1991 through 1998, 0.50 in 1999, and 0.17 in 2000. It was their interpretation that the annual rates had significantly declined from a previously stable stroke rate, and that this decline had occurred since the publication of STOP, suggesting that decline was related to the implementation of prophylactic transfusions in the high-risk group. A 2010 publication from Children’s Hospital in Philadelphia reviewed the incidence of stroke in their pediatric sickle cell population for the “pre-TCD” era and the “post-TCD” era and reported that the incidence of stroke prior to TCD use was 0.67 per 100 patient years; they also reported that in the “post-TCD” era the incidence had dropped to 0.06 per 100 patient years (53). An article from the Creteil Pediatric Sickle Cell referral center reported that they began screening 12- to 18-month-old children with HbSS with TCD in 1992, and screening with biyearly MRI/MRA for patients older than 5 years in 1993 (25). Since 1998, they transfused all children with two TCDs with TAMM >200 cm/sec in the middle cerebral or distal internal carotid artery. Two hundred and seventeen children were screened. Over a mean follow-up of 7.7 years, there were only three strokes (1.9%). Of the 45 cases with abnormal TCD, there was only one who suffered a stroke. The authors concluded that early screening and intervention resulted in a reduction of stroke risk by the age of 18 from the 11% reported by the CSSCD to 1.9%. A report conducted a retrospective trend analysis of the 1993 to 2009 Nationwide Inpatient Sample and Kids Inpatient Database for hospitalizations for stroke in sickle cell patients. There was a decline from a rate of 0.51/100 patient years from 1993 to 1998, to 0.28/100 patient years for 1999 to 2009. This was attributed to TCD screening and introduction of chronic transfusion for patients at high risk (143).
Despite the publication of STOP and its recommendations about screening and management of HbSS children with high-velocity TCDs, there has been suboptimal implementation of both TCD screening as well as management as per the STOP protocol. There has been a publication on follow-up of participants in STOP (133). Data on 74% of the children screened for STOP were reviewed. For the 2808 patients who were stroke free at the end of STOP, mean duration of follow up was 9.1 years. A total of 60 strokes occurred. Most of the patients who suffered a stroke had not been managed according to STOP protocol due to either failure to obtain TCD screening or failure to appropriately treat those identified as high risk by TCD screening.
Hydroxyurea (HU) can increase fetal hemoglobin and improve the clinical course of patients (37). Potential benefits of hydroxyurea include increased hematocrit, increased percent F with decreased sickling, decreased red cell adhesion, improved red cell rheology, decreased hemolysis, and increased nitric oxide (144; 194). Another potential benefit was reported in a retrospective study of children with HbSS followed at two tertiary respiratory clinics who were subsequently started on hydroxyurea and seen in follow up (219). Of 21 cases who had sleep studies followed an average of 9 months before starting hydroxyurea and an average of 9 months after starting hydroxyurea, there was an increase in mean overnight oxygen saturations from 93.5% to 95.2%. Of the 32 cases that had spot daytime oxygen saturation checked pre- and post-hydroxyurea, the median SpO2 rose from 93.5% to 96.3%. There was an accompanying increase in hemoglobin from 7.6 to 8.3 g/L.
The Multicenter Study of Hydroxyurea has reported on the long-term safety of hydroxyurea. They enrolled 299 patients in the MSH trial. This trial started in 1992, with enrollment over about 15 months, and it ended in 2009. Forty-four patients never had hydroxyurea, 140 had hydroxyurea for less than five years, 55 had hydroxyurea for 5 to 10 years, 40 had hydroxyurea for 10 to 15 years, and 20 had hydroxyurea for greater than 15 years. Mortality appeared to be reduced in patients on long term hydroxyurea, with 87% of the death occurring in patients who had never taken hydroxyurea or had taken it for less than five years. The risk of developing malignancy appeared to be the same in all groups (207).
In 2014, an expert panel published a number of recommendations including the following on hydroxyurea: “The panel recommends that hydroxyurea therapy be offered in children beginning at 9 months of age, including those who are asymptomatic” (240). Karkoska and colleagues published their experience, comparing the time period prior to 2014 when 43% of their patients were on hydroxyurea to the post-2014 period when 95% were on hydroxyurea (118). They reported a decrease in sickle cell anemia-related admissions from 67 of 100 patient years for 2010 to 39 of 100 patient years for 2019.
In an effort to address the concerns about iron overload in those patients undergoing chronic transfusion, Ware organized the SWITCH trial (Stroke with Transfusion Changing to Hydroxyurea) (233), a phase III NHLBI-funded trial that randomized 133 children with sickle cell disease who had suffered a stroke and been on chronic transfusion therapy an average of 7 years to either continued transfusion with deferasirox or to hydroxyurea and monthly phlebotomy. The primary endpoint was secondary stroke and management of iron overload. The trial was stopped prematurely; there were no strokes in the 66 randomized to continued transfusion group and seven strokes in the 67 randomized to hydroxyurea. There did not appear to be any difference in the reduction in iron overload by phlebotomy compared to deferasirox (National Institutes of Health Press Release). Ali and colleagues published an observational study of 43 HbSS patients in Jamaica who suffered a first clinical stroke (14). Chronic transfusion therapy for secondary stroke prevention was not available. Hydroxyurea was offered to patients for secondary stroke prevention. Ten patients took hydroxyurea; 33 did not. During 111 person-years of follow-up, there were 20 strokes (60%) in the non-hydroxyurea group and one stroke (10%) in the hydroxyurea-treated group. The hydroxyurea-treated patient who had the recurrent stroke had moyamoya by MRA. The authors concluded that chronic transfusion should remain the treatment of choice for stroke prevention. They suggested that hydroxyurea at maximally tolerated doses should be considered for stroke prevention in settings where chronic transfusion programs are not possible or acceptable. It is likely that those patients with moyamoya pattern vasculopathy will require other therapies.
The TWITCH trial results were published in 2016 (232). This trial used TCD TAMM as a surrogate marker for stroke risk. This trial studied 121 patients with HbSS, aged 4 to 16 years old, who had been found to have abnormal TCD velocities and had been maintained on chronic transfusion for at least one year. Exclusion criteria were clinical stroke or transient ischemic attack, inadequate TCD examination, or severe vasculopathy on MRA. Patients were randomized to continued chronic transfusion to maintain HbS levels less than 30% or to oral hydroxyurea. The hydroxyurea was initiated at 20 mg/kg/day and titrated to the maximal tolerated dose (MTD), defined as moderate marrow suppression of neutrophils and reticulocytes. Patients were continued on transfusion during the titration phase, averaging 27 weeks (range 24-32) to MTD. The primary study endpoint was maximum TCD TAMM on the index side (hemisphere with highest TAMM at baseline) at 24 months after trial entry; secondary endpoints were TCD velocity on on-index side, new stroke, and new brain MRI/MRA lesions. The average duration of transfusion prior to enrollment was 3.8 in the transfusion arm and 4.5 in the hydroxyurea arm. Average age on entry was 9.5 years. The trial was stopped based on noninferiority analysis after 67% of patients had completed the study. Average TAMM at exit was 143 cm/sec for the transfusion arm and 138 cm/sec for the hydroxyurea group. No child reverted to abnormal TCD velocities. Exit MRI did not detect any new lesions in either treatment group. There were 23 serious adverse events in the hydroxyurea group and 10 serious adverse events in the transfusion arm. This study suggests that in a similar selected population of patients with HbSS, hydroxyurea may be effective for stroke prevention. It should be noted that the trial was short and that the average bridging transfusion was 6 to 8 months of the 24-month trial duration.
The SCRIPP study reported that in patients placed on hydroxyurea, for every 1 gm/L increase in hemoglobin there was a 15.0 cm/sec decline in TAMM (55).
Similarly, Rankine-Mullings reported on 43 children with HbSS and TAMM greater than 170 cm/sec (11 were greater than 200 cm/sec). On the maximal tolerated dose of hydroxyurea there was a reduction of TAMM by 24 + 30 cm/sec compared to baseline; 28 returned to normal TAMMs (185).
The similarity of the arterial pathology in sickle cell disease with that seen in moyamoya has prompted a few to try surgical revascularization. Vernet and colleagues first reported a patient with sickle cell anemia and moyamoya who underwent encephalo-duro-arterio-synangiosis (EDAS) with impressive demonstration of neovascularization (223). There are a number of subsequent reports on the use of EDAS in patients with sickle cell disease with intracranial vasculopathy. Fryer reported 10 EDASs performed in six children with sickle cell disease with moyamoya who were being maintained on chronic transfusion. He reported stroke-free survival in five of the six at an average follow-up of 33 months. There was one stroke two weeks after an EDAS procedure. Follow-up imaging was available for four patients, documenting patency of graft vessels and growth of collateral connections (68). Hankinson and associates reported their experience with encephaloduroarteriosynangiosis in 12 children (10 of whom had a history of stroke with sickle cell disease and moyamoya) (89). The average age was 12 years at the time of surgery. Seven patients had bilateral encephaloduroarteriosynangiosis, and five had unilateral encephaloduroarteriosynangiosis. The mean follow-up was 46.8 months. During this time, one had a stroke (3 weeks postoperatively) and another had a transient ischemic attack 18 months postop and made full recovery. Seven patients had follow-up angiography demonstrating evidence of revascularization. Smith and colleagues reported EDAS on 12 patients with sickle cell disease and moyamoya, with an average follow-up of 49 months postsurgery (201). There was a perioperative stroke, but no other strokes during follow-up. On follow-up imaging there were “new surgical collaterals in 17 of 19 hemispheres.” The authors also reported that there was “progression of the moyamoya in 13 of 19 hemispheres.” Kennedy and colleagues reported on 17 cases of moyamoya in HbSS treated with EDAS (some of whom had probably been reported by Hankinson in 2008), and they reviewed the other reported cases (123). Their interpretation was that the EDAS appeared to be safe and effective. Yang and colleagues reported the Hopkins experience in 15 cases of HbSS with moyamoya; seven patients (12 hemispheres) had EDAS; none of the cases with EDAS had a stroke over an average followup of 11.6 years, whereas four of the eight patients who did not have EDAS had a stroke during this time (239). Similarly, Alarmi and associates reported EDAS on eight patients with HbSS and moyamoya, reporting no complications, and a return to normal school activities (13). Not all articles have reported positive outcomes from EDAS. Winstead and colleagues reported on 11 patients with HbSS and moyamoya; seven had EDAS at an average age of 19 (237). Three had no evidence of flow in their grafts at followup, and one had a late hemorrhagic stroke. There was no difference in the occurrence of stroke between the EDAS group and the nonoperative group, prompting the authors to suggest a prospective controlled trial to evaluate the effectiveness of EDAS in this condition.
Although there is pathological evidence of thrombus formation at the site of the large artery narrowing, making the use of antithrombotic agents attractive, there is little experience with antiplatelet agents or anticoagulants for either primary or secondary prevention of sickle cell disease-related stroke. Anticoagulation may be especially hazardous if moyamoya vessels are present. The use of aspirin cannot be casually recommended because those at highest risk are children in whom aspirin use has been curtailed due to an association with Reye syndrome. However, it is reasonable to consider the use of aspirin in those children who have had a stroke, as well as those with moyamoya, as the risk benefit ratio should favor aspirin reducing future stroke. Similarly, experience with ticlopidine or clopidogrel in children or adults with sickle cell disease is limited. Warfarin has been tried in adults with stroke; however, there is no systematic experience, and the bleeding risk of moyamoya would dictate caution in patients with this finding. To date, there are no reports of the use of balloon angioplasty to dilate the narrowed arterial segments in these patients.
Patients with sickle cell disease who suffer a subarachnoid hemorrhage due to aneurysm should undergo an evaluation for the cause of the hemorrhage. If an aneurysm is found, then obliteration of the aneurysm by either endovascular therapy (coiling) or surgical therapy (clipping) is appropriate. The appropriate management of incidentally discovered intracranial aneurysms is not clear. In adults, asymptomatic aneurysms less than 7 mm are observed, whereas intervention is recommended for those larger than 10 mm. If there are associated arterial changes of either stenosis or moyamoya, chronic transfusion therapy is probably appropriate.
Although there is little support in the literature, transfusion for intracranial hemorrhage not associated with aneurysm seems reasonable. In some cases, the angiogram may show no aneurysm or obstructive vasculopathy. In such cases, we recommend short-term transfusion (for 1 to 2 years) only.
Sickle cell disease encompasses a long list of hemoglobinopathies that have two things in common: the presence of some amount of hemoglobin S and demonstration of sickling under some conditions. The majority of sickle cell disease patients with stroke have homozygous SS or S thalassemia. When hemoglobin S is combined with other hemoglobins, such as A (SS trait) or C (hemoglobin sickle cell disease), sickling is greatly retarded and generally all symptoms, including those secondary to cerebrovascular events, are mitigated. Patients with hemoglobin S variants and trait should not be assumed to have the typical sickle cell disease-related vascular disease until other causes of stroke have been eliminated (108).
The differential diagnosis of ischemic stroke in sickle cell children includes the differential for ischemic stroke in the young. This includes (but is not limited to) dissection of the carotid or vertebral arteries, embolic disease (cardiac or transcardiac), hypercoagulable states (including lupus anticoagulant, anticardiolipin antibodies, Sneddon syndrome, deficiencies of protein S, protein C, antithrombin), Fabry disease, intracranial venous thrombosis, and vasculitis. There are a few qualifications: (1) patients are often children and unable to give a detailed history; (2) trauma, drug use, hypoglycemia, or accidental intoxication may be confounding factors; (3) patients with sickle cell disease are at risk for bacterial meningitis, and this diagnosis should be considered when a decreased level of consciousness or seizures are part of the presentation. Other causes of fever and focal neurologic exam would include brain abscess, herpes encephalitis, septic embolism, or vasculitis; (4) the relatively high prevalence of cerebrovascular disorders in sickle cell disease may lead to the erroneous assumption that any CNS syndrome is due to stroke in these patients. For example, sickle cell disease patients with myelopathic symptoms may not have spinal cord infarction, but compression due to extramedullary hematopoiesis (an unusual but reported complication of sickle cell disease), transverse myelitis, or multiple sclerosis, conditions for which transfusion is not indicated, should also be considered; (5) nonfocal symptoms such as dizziness (196) are more likely due to acute vestibulopathy than brainstem ischemia; (6) isolated neuropathies or ataxia are also unusual manifestations of stroke in sickle cell disease; and (7) aggressive treatment of pain with narcotics, especially meperidine, has been associated with seizures in sickle cell disease due to normeperidine, a metabolite of meperidine (22). Sickle cell disease patients with seizures should be evaluated for cerebral ischemia, but meperidine-associated seizures should be considered in the differential diagnosis of such patients who present during or after treatment of episodes of pain.
Patients with suspected stroke should receive a noncontrast cranial CT promptly (to evaluate for hemorrhage or mass lesions) followed in selected cases by MRI and MRA. Catheter cerebral angiography is usually recommended for cases of intracranial hemorrhage. Angiography can be performed safely if patients are prepared by reduction of hemoglobin S to less than 30% of the total hemoglobin and if vigorous hydration is added. The initial evaluation of acutely symptomatic patients should also consider other causes of brain dysfunction including trauma, meningitis, encephalitis, brain abscess, drugs, or metabolic factors. Still, a lumbar puncture usually is not needed in the absence of meningismus, fever, or other evidence of infection, unless subarachnoid hemorrhage is suspected and not confirmed by CT. Spinal cord infarction is rare in sickle cell disease, and, in cases of myelopathy, a thorough search for other etiologies should be undertaken before assuming the lesion is an infarction related to sickle cell disease.
An EKG, complete blood count, and chemistries should also be obtained; special tests for coagulopathies or cardiac sources of stroke may be appropriate in some patients, especially those with recurrent stroke despite transfusion. If the CT does not show stroke or another lesion responsible for the patient's symptoms, MRI should be performed. The CT or MRI typically shows cortical and subcortical areas of ischemic damage in either territorial or "border zone" patterns and often old lesions in asymptomatic areas (242). Once the patient is stabilized, transcranial Doppler can be used to examine the intracranial vessels. Unlike patients at risk before onset of stroke, transcranial Doppler may not show high velocity in patients who already have had stroke and who have advanced arterial disease leading to symptoms (04). In addition, the indication for chronic transfusion, at least in children, is ischemic stroke as documented by clinical and radiographic methods. Even if the patient has no demonstrable vasculopathy, most specialists would recommend transfusion at least for a few years.
Cerebral angiography is clearly indicated in all cases of intracranial hemorrhage (except epidural and subdural) to detect surgically correctable aneurysm or arteriovenous malformations. Angiography also is useful in patients presenting with transient symptoms whose imaging studies are negative. In this situation, angiography is used to determine the extent of large vessel disease, which, if present, strengthens the case for treating the patient with repeated transfusions (159).
"Border zone" lesions in the territory shared by the anterior and middle cerebral arteries and middle and posterior cerebral arteries as well as between the deep and superficial circulations are especially common findings on MRI. The scans also may show punctate lesions in the deep white matter (167). In our experience, little information is added by MRI contrast in sickle cell disease unless tumor or brain abscess are strong alternate diagnoses. MRI and neuropsychological testing often are helpful in assessing cognitive deficits for special education and rehabilitation planning. Focal and generalized atrophy are sometimes present. Patients can have enlarged intracranial vessels, presumably as a response to increased flow. Although focal vessel enlargement may be mistaken for aneurysm, an asymptomatic aneurysm can be discovered by MRI. A few centers perform MRI and angiography or other tests such as positron emission tomography on symptomatic patients. In most centers, however, patients are committed to recurrent transfusions on the basis of cerebrovascular symptoms combined with CT or MRI confirmation of parenchymal damage or angiographic or other evidence of severe large vessel disease.
In all neurologically asymptomatic patients with sickle cell disease, we recommend screening with transcranial Doppler. It can predict risk and could lead to prophylactic transfusion for the prevention of stroke (08).
Although pre- and postnatal identification of the beta-globin gene is possible, its impact on future advances in sickle cell disease therapy is limited due to the heterogeneous clinical presentations caused by the beta-globin gene mutations (65).
Cerebral infarction. Most of the treatment experience in sickle cell disease is in children. Acute cerebral infarction is treated emergently with blood transfusions using concentrated erythrocytes (03). The optimal method (simple transfusions vs. exchange), the extent, and the efficacy of acute transfusion are not established. In a small, retrospective, cohort study of children, Hulbert and associates reported that exchange transfusion was more effective than simple transfusion for the initial stroke treatment. The results also suggested that exchange transfusion may reduce the risk of future strokes more than simple transfusion (106). Patients should receive aggressive hydration, unless there is concern for massive cerebral edema, in order to decrease blood viscosity. Aspirin should be administered to adults. Our practice is to manage younger patients with exchange transfusion, avoiding hypotension during phlebotomy and attempting to reduce the hemoglobin S to less than 30% within 48 to 96 hours. Patients with altered sensorium, those with massive stroke, and those requiring central venous access are treated initially in an intensive care setting. In most cases, these patients enter programs of recurrent transfusions, in which they receive 10 to 15 cc/kg packed erythrocyte transfusions every 3 to 4 weeks for an indefinite period (37). Alloimmunization to human leukocyte antigens may be reduced by using extended cross matching, including the utilization of phenotypically matched red blood cell units for C, E, and K antigens. Iron overload, which is especially prevalent after 1.5 to 2 years of standard transfusion, is usually treated by chelation therapy, including desferrioxamine, which must be administered by IV or subcutaneous infusion. An FDA-approved iron chelator is Deferasirox, an oral agent that may improve compliance. If feasible, erythrocytapheresis (automated exchange transfusion) may be used as an alternative or as an adjunct treatment to minimize iron overload; while decreasing iron accumulation it increases the exposure to blood volume (114; 228).
Many pediatric hematologists initiate aspirin for secondary prevention therapy. If, as suggested by Shatat and colleagues, there is a significant prevalence of “masked hypertension”, then a more aggressive evaluation for the presence of ambulatory hypertension would seem warranted, as well as a blood pressure-lowering therapy instituted, for those individuals with evidence of hypertension. Statin therapy is being investigated for secondary stroke prevention.
Few data indicate when or if it is safe to stop transfusions after childhood stroke with imaging documented stenosis in sickle cell disease. Small series looking at recurrence rates after 1 to 2 years of treatment or longer have reported high stroke rates (236; 230). For this reason, treatment is usually continued until late adolescence or until iron overload or development of alloantibodies makes transfusion difficult or dangerous (234). There is less enthusiasm for recurrent transfusions among hematologists caring for the adult "graduates" of these pediatric treatment programs. Many patients stop transfusion for a variety of reasons. The rate of recurrent stroke among these adult patients is not known. It is plausible but unproven that the risk for recurrent stroke declines as blood flow needs diminish after childhood, making adults less vulnerable when transfusions are stopped.
One publication has reported the outcomes of 22 patients who had an ischemic stroke prior to the age of 18 years between 1993 and 2009 (145). These patients were managed with chronic exchange transfusion. At the age of 18, patients transitioned to adult hematology. Eight patients then refused to continue transfusion or were noncompliant with the transfusion regimen. All of these eight patients died between 1 and 5 years after transition. This article does not mention the use of hydroxyurea on these eight patients, but it does not appear to have been part of their regimen. It did report that the eight patients had higher levels of ferritin, suggesting poor compliance with chelation therapy. This article would argue for continued transfusion in this population, or at a minimum, hydroxyurea with close follow up with MRI and transcranial Doppler to monitor for the need to restart transfusion.
Adults with sickle cell disease should be considered for recombinant tissue-type plasminogen activator treatment of acute ischemic stroke if they present within three hours of onset of symptoms and have an appropriate CT scan.
Bone marrow transplant has the potential to cure sickle cell disease. Bone marrow transplant has been used successfully in a large number of patients with thalassemia but to date has been used in a much smaller number of patients with sickle cell disease. The efficacy of chronic transfusion versus matched sibling-related bone marrow transplant for the treatment of stroke in sickle cell disease remains widely debated. Opinions range from transplant being the only potentially curative treatment with no report of stroke recurrence (212) to there being no difference detected between bone marrow transplant and chronic transfusion (172). Numerous studies have demonstrated intermediate results with approximately 84% disease free and 94% survival rates after bone marrow transplant (163). There are a number of potential problems with bone marrow transplantation in children with sickle cell disease, including the paucity of children with siblings who are HLA identical and suitable donors, the morbidity and mortality associated with transplantation, failure of engraftment, graft-versus-host phenomenon, and the risk of infertility. Graft rejection rates between 10% (228) and 22% (163) have been reported. Mortality rates of 3% to 6% have been reported (228), and survival rates of 94% and 97% 5-year probability of overall survival have been cited (45; 163). Currently, researchers are evaluating nonmyeloablative regimens that may be less toxic (72). Neurologic complications after bone marrow transplantation occurred in seven of 21 patients, including three with intracranial hemorrhage (two of these fatal). Seizures and extension of previously silent infarct have also been reported (02). The latest review of transplantation has just been published and summarizes the risks and potential benefits of transplantation in patients with sickle cell disease (200).
Although stroke is considered an important indication for transplant, the relatively high risk of recurrent stroke after the procedure is discouraging and raises concerns that once the intracranial arterial disease has become established, transplantation may not be effective in preventing future strokes. A small study found the development of new brain lesions on serial MRIs following bone marrow transplant (238). Improvements in the conditioning regimen and posttransplant care may reduce the complication rate.
There has been a publication of a point-counterpoint on the potential benefits and risks of transplantation of HLA identical sibling hematopoietic stem cell transplantation in children with symptomatic sickle cell anemia (58), marshalling arguments for transplantation (despite recognizing the 5% to 10% short-term mortality) in paucisymptomatic cases of HbSS, as the successful transplants do not experience vaso-occlusive crisis nor progressive sickle-related progressive organ damage, and Debaun and Clayton argued against routine hematopoietic stem cell transplantation citing the ever increasing survival rates in HbSS and the low event rate for death or organ failure (44). They called for a clinical trial to compare regular blood transfusion with hematopoietic stem cell transplantation for secondary stroke prevention or for progressive organ dysfunction.
The FDA has approved hydroxyurea as a treatment for moderate or severe sickle cell disease (56). As noted earlier, the expert panel has recommended its use starting at age 9 months. It increases HbF, total hemoglobin, NO, and mean corpuscular volume (MCV). There is a decrease in white blood count, reticulocyte count, and lactate dehydrogenase (a marker for hemolysis) (240). Hydroxyurea appears to be relatively safe for long-term use (88; 47).
Voxelotor, a drug that prevents HbS polymerization by decreasing the partial pressure of oxygen at which hemoglobin is 50% saturated, has been approved by the FDA (224). A small phase 3 clinical trial demonstrated that its administration was associated with about a 1 g/dl increase in hemoglobin concentration; accompanying this was a decrease in biomarkers of hemolysis. It is not yet clear if this alteration in oxygen unloading will be associated with improved oxygen delivery to the brain.
Other HbF inducers, such as butyrate and decitabine, are currently under investigation. Because hydroxyurea, decitabine, and butyrate induce HbF by different mechanisms of action, it has been proposed that the use of two or more of these drugs may be more effective than single-agent therapy (56).
In a proof of concept article, Ribeil reported using a lentiviral transfer of a modified human beta-globin gene in a 13 year old with HbSS (187). This substitution results in inhibition of polymerization of HbS as well as an increase in the production of HbA. The patient underwent myeloablation with busulfan; two days after a washout period, he underwent infusion of transduced CD34+ cells. He was then supported by blood transfusion as needed. Neutrophil engraftment occurred by day 38 and platelet engraftment by day 91. There was a gradual increase in HbAT87Q, to a level of 5.5 g/dl at 9 months and 5.7 g/dl at 15 months. At 15 months after transplantation, he had not had any sickle cell disease-related events or hospitalizations.
Two trials, using different methodology (one used lentiviral insertion of a BCL11a suppressor and the other used CRISPR-Cas9 editing to reduce BCL11a expression), were published in New England Journal of Medicine in 2021 (54; 63). Both trials demonstrated that silencing the BCL11a transcription factor, which suppresses postnatal HbF production, resulted in high level of HbF production distributed in almost all red blood cells, as well as reduced HbS production. There was a reduction in hemolysis. There was a reduction in vasoocclusive events. There are potential concerns about potential long-term effects associated with the two techniques used to suppress BCL11a, as well as from the myeloablative conditioning, so long-term follow up will be important.
Lentiviral integration results in insertional mutations in the treated cells. The long-term consequences of integration of the viral vector into the genome are as yet unknown. The CRISPR-Cas9 modification causes a double stranded DNA break, with potential for off target DNA modifications.
There are also concerns about the toxicities of the conditioning regimens that must be administered prior to transplantation of genetically modified cells. Six percent of non-Hodgkins lymphoma who undergo autologous transplantation will develop acute leukemia secondary to the chemotherapy (78).
Endothelial injury and dysfunction is a recognized problem in sickle cell disease and has been postulated to be related to stroke risk. Statins are recognized to have a number of noncholesterol-lowering effects, including reduction of inflammatory markers and normalization of endothelial function, including upregulation of nitric oxide synthase. A pilot trial on the short-term use of simvastatin in 26 patients with sickle cell disease demonstrated it to be safe (101). In this population, simvastatin increased nitric oxide metabolites (NOx) by 23% in the 20 mg/day group and by 106% in the 40 mg/day group. They noted that patients on hydroxyurea had higher baseline NOx levels than those not on hydroxyurea, and that the increase in NOx was less in the group on hydroxyurea. The inflammatory marker CRP decreased by 68%, and IL-6 decreased by 50% to 70%. There was no effect on VEGF, VCAM, or tissue factor levels. The authors state that the results of this study should lead to larger randomized trials to assess the clinical and mechanistic effects of simvastatin on both endothelial function as well as vascular inflammation.
Lesions classified as “silent strokes” represent a heterogenous group. Some are clearly secondary to large artery disease. Others are identified by high signal on MRI but have had little pathological study. For “silent strokes,” the most efficacious therapy is still being explored. Refer back to the discussion on The Silent Infarct Transfusion Trial (SIT) for effects of transfusion on the risk of development of silent infarcts.
Intracranial hemorrhage. The most important immediate management steps for intracranial hemorrhage are to (1) treat increased intracranial pressure and prevent brain herniation in parenchymal bleeds; (2) prevent deterioration from acute hydrocephalus using ventriculostomy drainage in cases with intraventricular blood; (3) give nimodipine in patients with subarachnoid hemorrhage (a treatment protocol has been provided by Rinnert and colleagues) (189); (4) reduce hemoglobin S by exchange transfusion and hydration in an intensive care setting; and (5) perform cerebral angiography as soon as feasible.
If angiography shows an aneurysm or arteriovenous malformation, surgery or endovascular intervention should be considered. Intervention should be followed by recurrent transfusions in younger patients to decrease hemodynamic stress on vessels. If extensive occlusive disease or moyamoya is revealed, a patient should be treated with sequential transfusions until 21 years of age or offered the option to continue indefinitely after considering the risks of prolonged transfusion. In cases of intraventricular hemorrhage with hydrocephalus, emergency ventriculostomy may be combined with thrombolytic therapy to facilitate removal of clots (57). Long-term cerebrospinal fluid shunting may be required.
Other neurologic problems. Skull infarction, usually in the periorbital region, may result in local swelling, proptosis, and local hematoma formation either in the orbit or in the epidural space intracranially (71; 152; 115; 15; 70; 86).
Mental neuropathy, or numb chin syndrome, which may be the result of local mental or alveolar nerve compression from either dental disease (abscess, trauma, etc.) or from metastatic disease with mental nerve compression, has been reported in a number of patients with sickle cell disease in the absence of other causes of mental neuropathy (128; 126; 66; 147).
General considerations. Stroke patients should be evaluated for poststroke depression and should receive risk-factor counseling. Hyperactivity and other behavioral problems after stroke in children are common, and pharmacotherapy and special education may be appropriate. Neuropsychological evaluation and rehabilitation counseling are helpful in planning for the long-term needs of these patients.
“Silent cerebral infarcts” may be associated with neurocognitive dysfunction and poor school performance; however, reported interventions are extremely limited (228). One small series reported the potential benefit of “cognitive rehabilitation” that involved memory strategy training as well as academic tutoring (241).
Meningitis. The addition of vancomycin to the antibiotic regimen should be considered (39). Children, and probably adults, should also be treated with steroids in addition to antibiotics.
Pregnancy in sickle cell disease carries a relatively increased risk for intrauterine growth retardation, toxemia, thrombophlebitis, pyelonephritis, and spontaneous abortion. Preexisting renal disease and congestive heart failure may worsen during pregnancy. Hemodynamics of anemia and high cardiac output are accentuated during periods of uterine contractions (91; 42; 227).
Patients with sickle cell disease (particularly older patients, those with a history of pulmonary and CNS disease, and those with previous heavy transfusions) are at an increased risk of perioperative complications, especially acute chest syndrome and vaso-occlusive events. Patients requiring general anesthesia should receive maintenance fluids at least 12 hours before surgery. General anesthesia should aim for a mild respiratory alkalosis (pH about 7.45). Blood replacement for significant intraoperative blood loss is recommended. Postoperative parental hydration should keep the patient at 1 to 1.5 times the maintenance, and aggressive respiratory care is necessary to minimize pulmonary complications. Patients receiving neurosurgery, such as clipping of an aneurysm, should be transfused to reduce Hb S to less than 30% before angiography and surgery (188).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Fenwick T Nichols III MD
Dr. Nichols of the Medical College of Georgia has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
Apr. 25, 2024
Behavioral & Cognitive Disorders
Apr. 18, 2024
Behavioral & Cognitive Disorders
Apr. 17, 2024
General Child Neurology
Apr. 05, 2024
General Child Neurology
Apr. 01, 2024
General Child Neurology
Mar. 29, 2024
General Child Neurology
Mar. 29, 2024
General Child Neurology
Mar. 29, 2024