




Stroke & Vascular Disorders
Fusiform and dolichoectatic aneurysms
May. 03, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Neurologic complications following diagnostic cardiac catheterization and percutaneous coronary interventions occur infrequently but are likely to be encountered by the practicing neurologist. In this article, the authors review the incidence and mechanisms of various procedure-related nervous system injuries, with an emphasis on stroke. Various coronary stent types and requirements for antithrombotic therapy to maintain stent patency have a significant implication on bleeding risk, especially intracranially. This risk is further magnified when the patient requires both anticoagulant therapy and dual antiplatelet therapy. The effects of acute kidney injury, which may be caused by radiographic contrast, as well as the potential impact of chronic renal failure on procedural stroke, are discussed. Catheter arterial access locations, their risks, and potential benefits as well as peripheral nervous system complications of such are reviewed.
|
• Cardiac catheterization is successfully performed in large numbers of patients worldwide for both diagnostic and therapeutic purposes. | |
|
• Neurologic complications involving both the central and peripheral nervous systems, although infrequent, are important causes of neurologic consultations given the high volume of patients evaluated and treated with these techniques. | |
|
• Stroke (most ischemic and hemorrhagic), the most dreaded complication, can occur by a variety of mechanisms following cardiac catheterization. | |
|
• Treatment strategies of stroke following cardiac catheterization need to be based on the type of intervention and concurrent medications used during the cardiac procedure. | |
|
• Medications required to avoid stent thrombosis may produce hemorrhagic complications. | |
|
• Specific peripheral nerve injuries can occur as a consequence of cardiac catheterization (eg, compression, traction, laceration). |
The first coronary angiogram was performed by Mason Sones in the 1950s. Since then, there has been rapid expansion and evolution of the catheterization procedure. More than 1 million cardiac catheterizations are performed in the Unites States annually (06). Cardiac catheterization can be diagnostic or therapeutic. When interventions are conducted, they are characterized as percutaneous coronary interventions and can include balloon angioplasty, atherectomy, and intracoronary stents.
Neurologic complications range from minor events that may or may not lead to any permanent sequelae (such as transient compression of the femoral nerve by subcutaneous hematoma) to catastrophic events (cerebrovascular arterial occlusion or dissection). The major focus of this article is to describe cerebrovascular complications of diagnostic and therapeutic cardiac catheterization. We also review some of the more common peripheral nervous system complications that are neurologically related.
Neurologic complications can be divided into central nervous system and peripheral nervous system complications (Table 1). CNS complications of cardiac catheterization include cerebrovascular (eg, transient ischemic attack, ischemic stroke, intracerebral hemorrhage), infectious events (eg, embolization of infected material to the brain), retinopathy, and myelopathy. In addition, contrast agent use may provoke seizures and encephalopathy. PNS complications include mononeuropathy (eg, femoral nerve compression), plexopathy (eg, due to retroperitoneal hematoma formation), and radiculopathy.
Major non-neurologic complications of cardiac catheterization include myocardial infarction perforation of the heart or great vessels, and death. Local arterial puncture-related complications include local hematoma formation, retroperitoneal hemorrhage, arteriovenous fistulas, pseudoaneurysm formation, and arterial thrombosis. Cardiac arrhythmias, atheroembolism, acute renal failure, infection, and radiation-related adverse effects may also occur.
|
Neurologic complication |
Etiology |
Neurologic findings |
|
Ischemic stroke |
Proximal embolization, hypoperfusion, postoperative atrial fibrillation (POAF), and general hypercoagulable state |
Variable depending on the site of the lesion |
|
Hemorrhagic stroke |
Related to high-dose antithrombotic medications in the periprocedural period, hemorrhagic conversion of ischemic stroke |
Variable depending on the site of the lesion |
|
Seizures |
Could be secondary to acute stroke, medications, contrast-induced, or hypoxic brain injury |
Variable depending on the part of the cerebral cortex affected; can be motor, sensory, aphasic, etc. In rare cases, can proceed to nonconvulsive status epilepticus. |
|
Contrast-induced encephalopathy |
Secondary to endothelial dysfunction and failure of autoregulation, with predilection for posterior circulation |
Typically manifests as headache, encephalopathy, cortical blindness, or other focal cortical symptoms. Has estimated incidence of 0.3% to 1%. |
|
Cognitive dysfunction |
Could be due to multifocal embolism, systemic inflammation, toxic-metabolic encephalopathy, and ICU delirium |
Patients can have impairments of neurocognitive tasks |
|
Brachial plexopathy |
Brachial plexus injury with axillary artery approach |
Abnormal motor and sensory function in one arm; may have associated pain |
|
Lumbar plexopathy |
Lumbar plexus compressed by retroperitoneal hematoma |
Pain in the groin, flank, or abdomen with radiation to the anterior thigh; numbness of the anterior thigh and medial calf with reduced or absent patellar reflex |
|
Lateral femoral cutaneous nerve (LFCN) injury and femoral neuropathy |
Due to femoral artery approach (direct injury or compression by an arteriovenous fistula or pseudoaneurysm) |
LFCN: Meralgia paresthetica with paresthesia of the upper lateral thigh |
|
Median neuropathy |
Median nerve injury with brachial artery catheterization |
Paralysis of flexor pollicis longus and flexor digitorum profundus of the second digit |
|
Peripheral nerve |
Lateral femoral cutaneous nerve injury |
Meralgia paresthetica with paresthesia of the upper lateral thigh |
|
Peripheral nerve |
Femoral nerve (direct injury or compression by an arteriovenous fistula or pseudoaneurysm) | |
|
Peripheral nerve |
Median nerve injury with brachial artery catheterization |
Paralysis of flexor pollicis longus and flexor digitorum profundus of the second digit |
Adapted from (08; 18; 22; 30)
The incidence of stroke (both ischemic and hemorrhagic) related to percutaneous coronary intervention is rare. Incidence has varied in studies and typically ranges from 0.08% to 0.56%. These strokes are either ischemic (due to dislodgement of debris after manipulation from the catheters) or hemorrhagic (due to antithrombotic use in the periprocedural period) (15). It has also been found that more than half of these cases occur in the vertebrobasilar circulation despite only one third of the blood flow passing through it, on average. This has been postulated to be due to anatomy favoring emboli entering the posterior circulation as opposed to the anterior circulation (25). Spinal cord infarction is also a rare but known risk of percutaneous coronary intervention. Often, this is due to disturbances in blood flow caused by the balloon catheter entering the femoral artery to the common iliac artery. This reduces the blood supply to the spinal cord (34). The common mechanisms for ischemic stroke events are depicted in Table 2.
|
• General hypercoagulable state given immobility, anesthesia, and perioperative holding of baseline antithrombotic medications | |
|
• Embolization of atherosclerotic plaque material (could dislodge calcified plaques around the aortic valve in retrograde catheterization and while traversing the aortic arch) | |
|
• Air embolism from vascular access | |
|
• Iatrogenic aortic dissection with extension into the common carotid arteries | |
|
Adapted from (25) and (22) |
However, unlike the spontaneously occurring stroke, the literature regarding treatment of stroke that occurs in the context of cardiac catheterization has been largely described in retrospective reports with relatively small patient sample sizes. The current understanding and limitations in treatment of strokes occurring in this circumstance are described below. Complications of other cardiac catheter-delivered therapies such as patent foramen ovale closure, transcatheter aortic valvular replacement, and atrial fibrillation ablation procedures are beyond the scope of this article but have been addressed elsewhere (09).
Studies have demonstrated an in-hospital mortality of approximately 30% for patients who develop stroke (inclusive of both ischemic and hemorrhagic). This is in stark contrast to 1% for those who do not develop stroke. This is dependent on the clinical presentation and the degree of neurologic deficits. Hemorrhagic strokes have a higher impact on prognosis (particularly the 30-day mortality) compared to ischemic stroke. This grim effect is present even for long-term survival in which the 5-year mortality is higher for those who experience stroke during the percutaneous coronary intervention compared to those who do not (45.7% vs. 11.1%) (20).
Stroke is considered periprocedural if it occurs within 30 days of the procedure. Typically, there is an early peak in the incidence of stroke in the first few weeks after a percutaneous coronary intervention. Some studies have shown that the relative risk is highest within the first 48 hours (20). The risk of stroke (both ischemic and hemorrhagic) varies depending on whether a procedure is conducted. One large-center retrospective study demonstrated a periprocedural incidence of 0.09% for diagnostic cardiac catheterization versus 0.23% when percutaneous coronary intervention is performed (22). Most strokes related to diagnostic and therapeutic catheterization are ischemic. Risk factors are denoted below in Table 3.
|
Patient demographics | |
|
Older age | |
|
Female sex | |
|
Chronic obstructive pulmonary disease | |
|
Medical history | |
|
Previous stroke or transient ischemic attack | |
|
Systolic dysfunction | |
|
Moderate to severe renal disease | |
|
Known high-grade carotid stenosis | |
|
Chronic carotid occlusion | |
|
Characteristics of the procedure | |
|
Non-elective case due to acute coronary syndrome | |
|
Blood transfusion | |
|
Triple vessel disease | |
|
Multipurpose guiding wires | |
|
Requirement of intra-aortic balloon pump | |
|
Percutaneous coronary intervention of an existing bypass graft | |
|
Hemodynamic instability | |
|
Presence of coronary arterial thrombus | |
|
Valvular disease | |
|
Left mainstem coronary disease | |
|
Post-operative characteristics | |
|
Post-operative atrial fibrillation | |
|
| |
A study published in 2019 demonstrated a higher incidence of post–percutaneous coronary intervention ischemic stroke than previously identified (03). The 0.56% incidence contrasts with the previously reported 0.10% of post–percutaneous coronary intervention ischemic strokes from the British Cardiovascular Intervention Society database, 2007 to 2012, and 0.22% of both post percutaneous coronary intervention ischemic and hemorrhagic strokes from the National Cardiovascular Data Registry, 2004 to 2007. It is possible that this observed increase could be secondary to higher risk profiles of patients (01). Use of an intra-aortic balloon pump and thrombus aspiration is commonly performed in patients with acute coronary syndrome and has been shown to significantly increase the rate of periprocedural strokes (41).
Aortic atheroma. Transesophageal echocardiography has demonstrated that complex plaque (ulcerated or mobile plaque) rather than plaque thickness alone (less than 4 mm vs. more than 4 mm) is associated with increased embolic stroke risk in the elderly, which is consistent across multiple ethnic groups (17). In addition to spontaneous embolization, aortic plaque is susceptible to mechanical disruption during cardiac catheterization procedures. Catheterization performed under emergent circumstances may increase the risk of contacting the vessel wall rather than maintaining the catheter closer to the center of the aortic lumen. Larger (greater than 6 French) and less flexible catheters have a greater likelihood of dislodging atheroma and producing major adverse events, including stroke (04).
Crossing the aortic valve. Crossing and manipulating across a diseased, calcified aortic valve is a step at high risk for cerebral embolism. The largest number of embolic signals typically occur during positioning across/manipulation of the aortic valve, with additional contributions from passage across the valve (24).
Catheter tip and guidewire atheroma. Fibrin formation at the catheter tip and along the guidewire can represent a source of embolization. Periodic catheter flushing, especially during catheter changes, can mitigate this phenomenon. Additionally, aortic atheroma can adhere to the guidewire and sheath, representing a source of embolization.
Antithrombotic therapy coronary interventions generate thrombin through endothelial damage and plaque disruption (42). AHA/ASA guidelines state that patients are typically treated with a loading antiplatelet dose, and parenteral anticoagulation (typically with unfractionated heparin and bivalirudin, though sometimes enoxaparin is used as well) is utilized during the procedure. Antithrombotic use increases the risk of hemorrhage, which can include intracranial hemorrhages. After the intervention, prolonged dual antiplatelet therapy is utilized in all patients for a duration of time (sometimes as short as 1 month, sometimes prolonged beyond 12 months). This helps reduce the risk of stent thrombosis and myocardial infarction (42). Sometimes, patients have other characteristics, such as atrial fibrillation requiring long-term anticoagulation. Studies have examined double versus triple therapy for these patients after a percutaneous coronary intervention. The presence of atrial fibrillation, mural cardiac thrombus, mechanical cardiac valves, etc, often necessitate therapeutic anticoagulation to minimize the risk of cardiogenic embolization. Therapeutic anticoagulation alone is insufficient to prevent coronary stent thrombosis, which requires initial dual antiplatelet therapy. The P2Y12 inhibitor modestly increases the risk of stent thrombosis compared to triple therapy, but at the benefit of having decreased bleeding risk, including intracranial hemorrhage. It is important to note that some patients require triple therapy, thus, significantly increasing their risk of intracranial hemorrhage (37). Additional risk factors for the development of hemorrhagic stroke include hypertension, aneurysms, arteriovenous malformations, and cocaine use. The management of these patients is very difficult as suspension of antithrombotic therapy can lead to stent thrombosis (10).
Emboli causing ischemic stroke during cardiac catheterization can be of different properties. There can be calcific emboli from atheromatous plaques, cholesterol emboli from ulcerated plaques, thrombi that form in situ on the catheter tips, and gaseous emboli that form during injection of contrast or saline (25). These emboli can cause neurologic deterioration or be asymptomatic (thus classified as a silent stroke). The exact manifestation of the neurologic deterioration is dependent on the area of cerebral involvement. There can also be ophthalmologic involvement. The ophthalmic artery is the first major branch of the internal carotid artery; therefore, emboli proximal to the carotid tend to go directly to the eye. The rate of retinal emboli after cardiac catheterization is controversial, approaching 6.3% in some studies. Although these are mostly clinically silent, a central retinal artery occlusion (CRAO) can be particularly damaging as meaningful recovery of vision occurs in less than 10% of patients with CRAO (02).
An asymptomatic cerebral infarction occurs when there is brain infarction seen on imaging without clinically overt symptoms. The incidence of these asymptomatic cerebral infarctions is around 10% (40). MRI of the patient before and after the procedure will show diffusion restriction (ischemic causes of restriction of free movement of water molecules). These diffusion restriction lesions are likely infarctions with permanent tissue loss. Although the long-term prognosis of patients who have these asymptomatic cerebral infarctions has not been reported, several studies have demonstrated the likely influence of asymptomatic cerebral infarction in the development of dementia and depression (40).
Although radial access has appeared in meta-analyses to lower the risk of major adverse events and mortality compared to femoral access, there is no consistent demonstration in lowering the risk of percutaneous coronary intervention–associated ischemic stroke. It is possible that radial access is more so a surrogate for operator expertise (28). Effective anticoagulation can reduce the risk of thrombus formation. Typically, a 70 to 100 U/kg intravenous bolus of unfractionated heparin is utilized when no glycoprotein IIb/IIIa inhibitor is combined for an ACT target of 250 to 350 seconds, and a 50 to 70 U/kg intravenous bolus is utilized when a glycoprotein IIb/IIIa inhibitor is planned. Fondaparinux is associated with a higher risk of catheter thrombosis, so it should be avoided, particularly in patients with STEMI (05). Previously, glycoprotein IIb/IIIa inhibitors (GPIs) were routinely used with intraprocedural administration of unfractionated heparin (UFH) to disrupt the platelet aggregation pathway. Now, with the development of quicker-onset P2Y12 inhibitors and advances in stent design, GPIs are more selectively utilized in situations where there is high thrombotic burden, when there is lack of timely P2Y12 administration, or as a bailout strategy (07). Post-procedurally, patients are on a set duration of at least dual antiplatelet therapy, most commonly with aspirin and clopidogrel. Given the genetic variations in the ability to activate clopidogrel, testing for adequate antiplatelet effect is important. In certain patients, clopidogrel may need to be switched to prasugrel or ticagrelor. Prasugrel has been demonstrated to increase the risk of fatal and intracranial hemorrhage in patients with prior stroke or transient ischemic attack, so clinical judgment is needed as to when clopidogrel may need to be switched (20).
The low incidence of stroke during cardiac catheterization makes randomized, prospective trials difficult to perform. The 2026 AHA/ASA Guideline for the Management of Patients with Acute Ischemic Stroke stated that use of IV thrombolysis (IVT) during or immediately post-angiography should be considered as benefit likely outweighs risk (32). However, real-world implications of offering IVT when patients have received antithrombotic therapy with cardiac catheterization need to be considered.
As patients who undergo cardiac catheterization typically receive unfractionated heparin within the last 48 hours, the aPTT may still be elevated, leading to IVT being contraindicated (29). If the aPTT has normalized, IVT can be considered “off label” after a thorough consideration of the potential risks and benefits. Another consideration if the aPTT has not normalized is to reverse the coagulopathy with protamine. However, there is a lack of data on its efficacy and safety in acute ischemic stroke. There are also some anecdotal reports of stent thrombosis after administration of protamine, though this overall trend is not reflected in meta-analyses (14). In addition, after IVT is given, antithrombotic therapy is typically held afterwards for 24 hours. This may have significant impact if percutaneous coronary intervention was conducted as that can markedly increase the risk of stent thrombosis and major adverse cardiac events.
With regards to glycoprotein IIb/IIIa inhibitors (GPIs), abciximab is considered contraindicated for concurrent administration with intravenous alteplase (31). Drawing from meta-analyses regarding intracerebral hemorrhage risks for the 3 GPIs, the pooled relative risk for symptomatic intracerebral hemorrhage was 1.16 in all studies, suggesting that GPI usage can induce symptomatic intracerebral hemorrhage, most significantly seen with abciximab (43). However, routine use of GPIs in cardiac catheterization has fallen in recent years.
Mechanical thrombectomy is a reasonable treatment option for those patients with large vessel occlusion secondary to cardiac catheterization. One issue is the availability of neurointerventionalists to perform these procedures, especially in the community hospital setting. Despite the low frequency of ischemic stroke secondary to cardiac catheterization, the sheer number of procedures performed annually does make this an important issue. Individualized programs have been developed in community hospitals without neurointerventionalists to perform mechanical thrombectomy. Although individual programs seemed to have similar efficacy compared to mechanical thrombectomy trials performed around the same time, there were higher rates of subarachnoid hemorrhage (21). Typically, patients are transferred to comprehensive stroke centers who have mechanical thrombectomy capabilities, but that transfer could cause significant delays. Although data are sparse on the use of mechanical thrombectomy for stroke after cardiac intervention, it seems that hospitalized patients with cardiac interventions and ischemic stroke may be less than half as likely to receive mechanical thrombectomy as patients with ischemic stroke without cardiac intervention (16). These lower rates could be due to a multitude of factors, including diagnosis delays (including prolonged anesthetic effects) and perceived higher procedural risk.
Cardiac catheterization may be achieved via access from the femoral or radial arteries. Table 4 provides a more detailed summary of the most common femoral arterial access-related complications, their pathophysiology, and potential neurologic complications. Nerves distal to the site of hematoma formation may be compromised by ischemic monomelic neuropathy (36; 27; 08).
Radial approach was first introduced in 1989. Given that it's more superficial, earlier recognition of bleeding complications and easy or rapid compressibility may cause lower risk of death and reduction in major adverse clinical events (19). Although European and American cohorts do not demonstrate a lower risk of periprocedural stroke with the transradial approach, a Japanese registry reported lower risks (28). However, despite the rising utilization of the transradial approach, the transfemoral approach is necessary for complex percutaneous coronary intervention procedures.
|
Complication |
Pathophysiology |
Potential neurologic complication |
|
Thigh ecchymosis |
Subcutaneous or groin hematoma |
Femoral neuropathy |
|
Retroperitoneal hemorrhage |
Femoral artery puncture above inguinal ligament |
Femoral neuropathy |
|
Pseudoaneurysm formation |
Puncture of a femoral artery branch |
Femoral neuropathy |
|
Arteriovenous fistula |
Concomitant femoral artery and venous puncture |
Femoral neuropathy |
|
Arterial thrombosis |
Either due to arterial dissection or embolic material from catheter lumen |
Ischemic monomelic neuropathy |
Local hematoma formation. A large area of thigh ecchymosis around the femoral artery puncture site is not rare. Subcutaneous hematoma may compress the femoral nerve. Femoral nerve compression may last weeks to months to resolve. Most patients only have sensory discomfort, including paresthesias, dysesthesias, and pain. Decreased strength of femoral nerve-innervated muscles may occur. Avoiding strenuous activity may prevent expansion of hematoma formation and, hence, femoral nerve compression.
Retroperitoneal hematoma. Femoral artery puncture above the inguinal ligament may result in hematoma extension into the retroperitoneal space. The retroperitoneum is divided into the perirenal space and anterior and posterior pararenal spaces. Direct hemorrhage within the psoas muscle may also occur. The lumbar plexus and its branches lay anterior to the psoas muscles. A retroperitoneal hematoma may compress the lumbar plexus, particularly the lower lumbar plexus, the sacral plexus, and the femoral or obturator nerves (11). Fascial tracking of blood in the femoral nerve sheath may result in femoral neuropathy in the absence of visible retroperitoneal blood.
Arteriovenous fistula. Concomitant puncture of the femoral vein may lead to a fistulous communication between the femoral artery and the femoral vein.
Pseudoaneurysm formation. Femoral pseudoaneurysm occurs when a periarterial hematoma remains continuous with the arterial lumen. The incidence of femoral neuropathy was 2.5% in a prospective study of 79 patients treated for femoral pseudoaneurysm following cardiac catheterization (35).
Effects of renal disease. Acute kidney injury following percutaneous coronary intervention is a known phenomenon. It occurs in 3.3% to 14.5% of patients. This can be due to the use of intravenous contrast media, hemodynamic instability, and cholesterol embolization. Patients who develop acute kidney injury after percutaneous coronary intervention are more likely to have worse outcomes. In particular, cholesterol embolization is associated with a higher likelihood of long-term renal replacement therapy (12).
Studies have demonstrated that chronic kidney disease is associated with both higher risk and worse outcomes after ischemic stroke. There is also a causal association between chronic kidney disease and intracranial hemorrhage (38). Although the potential of hemorrhage in the presence of chronic kidney disease does not represent a contraindication to IVT and studies have shown the 90-day efficacy of IVT is not affected, safety outcomes like symptomatic intracranial hemorrhage rates and all-cause mortality can be affected (39).
Cardiac arrhythmias. Atrial fibrillation has been found to occur after percutaneous coronary intervention in certain studies, but incidence is quite rare at approximately 0.1% (23). However, when it occurs, it can be devastating as atrial fibrillation may lead to cardioembolism to the brain or spinal cord. Both tachyarrhythmias and bradyarrhythmias may produce hypotension and potential for ischemic brain injury.
Infection. The femoral arterial approach has a lower risk of infection (0.06%) compared to the brachial artery approach (0.6%) (13). Infrequently, if endocarditis ensues, a cerebral mycotic aneurysm may form.
Contrast- and medication-related complications. Seizures following cardiac catheterization may be due to stroke or contrast agents. Overall, contrast-induced seizures have mostly been reported in adults but may also occur in children. Despite the increased use of non-ionic, low-osmolar agents, there remains the risk of contrast-induced encephalopathy of 0.3% to 1%. Comparatively, the risk of contrast-induced encephalopathy in hyperosmolar iodinated contrast agents is around 4% (26).
The mechanism behind contrast-induced encephalopathy is not definitive. A prominent manifestation of contrast-induced encephalopathy is transient cortical blindness. This is likely due to the relatively higher permeability of the blood-brain barrier in the occipital cortex. Other symptoms include confusion, motor and sensory deficits, ophthalmoplegia, and aphasia, among others. Typically, the symptoms manifest within minutes to hours and fully resolve within 48 to 72 hours (33).
The clinical management of patients who suffer cerebrovascular complications during or following cardiac catheterization is unlike that applicable to any other clinical scenario. More often than not, the patients have received sedatives that obscured their neurologic assessment and are likely to have received antithrombotic agents that notably increase the risk of hemorrhagic stroke but limit the applicability of intravenous thrombolytic treatment.
In general, the approach to patients who suffer an acute neurologic change while still in the catheterization suite is materially different than that of patients whose neurologic symptoms are discovered after the cardiac procedure has been completed. However, they do share some common steps during the early treatment stages:
|
(1) CODE STROKE Alert. It is imperative that, on recognition of acute neurologic symptoms suggestive of the possibility of an acute stroke, the intramural predefined urgent treatment pathway for acute stroke is activated. This assures that management of the patient is based on clinical practice guidelines that the institution has already sanctioned, that all available resources (particularly clinical stroke experts) are brought to bear on behalf of the patient, and that an "all hands on deck" attitude leaves very little room for unnecessary delays in care. | |
|
(2) Sedative reversal. It seems reasonable that, for any patient who is known to have received moderate sedation for the index procedure, reversal agents are promptly administered to determine: (A) Are the neurologic symptoms the results of the sedation? Or (B) Do the neurologic symptoms seem to be, in fact, caused by an acute cerebrovascular derangement? Because most patients have received a combination of opiates (eg, fentanyl) and benzodiazepines (eg, midazolam), we recommend the administration of both naloxone and flumazenil, respectively, to these patients. Just as in any other clinical scenario, care must be exercised because of the possibility of triggering adverse reactions such as opiate withdrawal (former) or seizures (latter). |
Once these two steps are completed, the subsequent strategy will depend largely on the circumstances of the discovery of the acute neurologic symptoms.
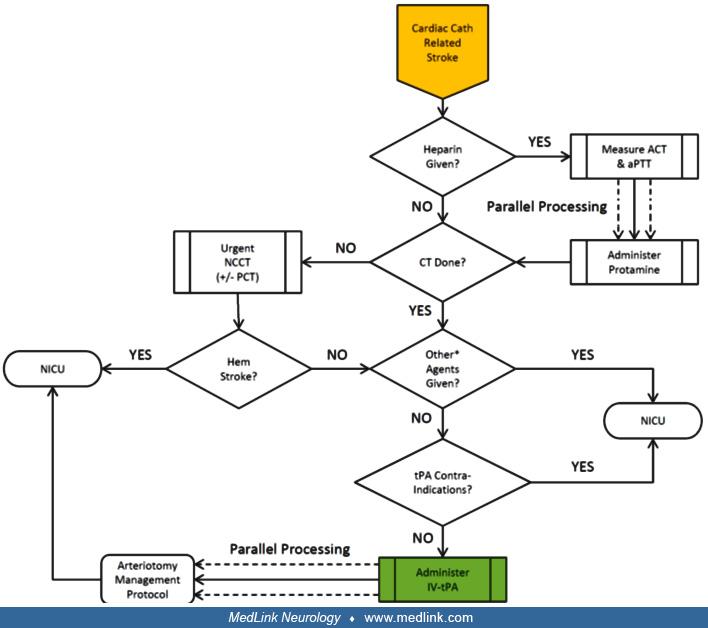
On recognition of acute neurologic changes during a heart procedure, and following the two common steps described above, if the patient is not back at his baseline following the administration of sedation reversing drugs, the next step depends on the availability in that particular catheterization suite of cone-beam CT. This modality, increasingly available in modern catheterization suites, allows rapid, "on the spot" image acquisition of the brain without having to move the patient. If this is carried out and a hemorrhagic stroke is diagnosed, the cardiac index procedure should be aborted and the patient moved to the neurointensive care unit for further care. If, on the other hand, there is no imaging evidence of an intracranial hemorrhage, urgent neuroangiography should be the next step because it can be carried out without moving the patient.
Although in many hospitals cardiologists have been credentialed to perform "carotid angiograms," we must emphasize the need for an expert neuroangiographer to take over the care of the patient at this moment. A lot of the findings in the context of this clinical scenario may be sufficiently subtle to require experience that cardiologists do not generally have. In fact, a close look at the figure above shows that, if cone-beam CT is not available, we recommend proceeding with urgent neuroangiography anyway because it is likely to uncover the most important information relevant to the immediate care of the patient.
If a large arterial occlusion is diagnosed during the neuroangiographic study, the operator can then quickly proceed to thrombectomy. Moreover, irrespective of the presence of a large artery occlusion, at that moment the patient can be qualified for treatment with intravenous tPA.
Unlike the patients described in the previous section, the recognition of acute neurologic changes typically occurs after the cardiac index procedure has been concluded and the patient is in the recovery area or the coronary care unit shortly thereafter. Again, following the two common steps described earlier, if the patient is not back at his baseline following the administration of sedation-reversing drugs, the next step is to acquire urgent imaging of the brain and its vasculature by means of non-contrast CT and CTA studies. In addition, and although still controversial, some recommend adding perfusion CT studies to the urgent imaging protocol. In this context, two caveats are important to point out:
|
(1) The value of perfusion CT in cases of very early ischemia is not as well established as in those patients with protracted symptoms. | |
|
(2) The technical optimization of perfusion CT in a patient who has already received contrast during the cardiac index procedure may not be possible due to artifactual contamination from circulating contrast agent. |
Once again, if the urgent CT imaging demonstrates a hemorrhagic stroke, the patient should be immediately transferred to the neurointensive care unit for further care per clinical practice guidelines. Conversely, if the CTA demonstrates a large arterial occlusion, the patient should be immediately transferred back to the catheterization suite for urgent thrombectomy. In parallel, the patient can be qualified for treatment with intravenous tPA.
In general, qualifying and administering intravenous tPA to one of these patients is not materially different than in any other clinical scenario. However, there are some details that are worth mentioning, the first one regarding how to manage those patients who have received unfractionated heparin during the cardiac index procedure. Clearly, the general recommendations are that active anticoagulation (ie, aPTT > 40 sec) is a contraindication for treatment with intravenous tPA. However, there is an increasing number of reports in the literature of patients successfully treated with intravenous thrombolysis following reversal of the heparin-related anticoagulation. Therefore, we recommend prompt measurement of both activated clotting time and activated partial thromboplastin time in these patients, followed by intravenous administration of protamine sulfate in sufficient doses to normalize the coagulation parameters.
It is also important to note that imaging of the brain using non-contrast CT is a sine qua non criterion for treatment with intravenous thrombolysis. Therefore, those patients who have not had such tests should promptly undergo imaging, including the same modalities described above and with the same caveats. Once this is accomplished and the heparin has been reversed, the next major hurdle has to do with the patient having received other antithrombotic agents, namely glycoprotein IIb/IIIa inhibitors or bivalirudin. Presently, any of these agents represents a substantial increased risk for hemorrhagic complications following the administration of intravenous tPA and, therefore, one should probably avoid such treatment.
Otherwise, it should be possible to qualify the patient's benefits-to-risks profile using a standard approach for the use of intravenous tPA in patients with acute ischemic stroke. Those patients who otherwise qualify should be promptly treated with intravenous tPA, and the attention of the treatment team should then also include management of the arteriotomy site.
In our opinion, having an arterial access site for the cardiac index procedure should not necessarily preclude the use of intravenous tPA for the treatment of these patients because they all represent "compressible" sites.
There is a slight difference in the management of femoral arteriotomies because of the size of the vessel as well as its potential for percutaneous closure. Along these lines, if the patient has a femoral sheath in place at the moment of the discovery of the acute neurologic changes, two options are available: (1) percutaneous closure, and (2) suturing the sheath with delayed removal. If the former path is chosen, we favor the use of closure devices to secure the arterial wall. Following closure, however, care of the arteriotomy site should be quite similar to that of a patient with a recently removed sheath due to the possibility of leakage following thrombolytic treatment.
Patients who have radial or brachial arteriotomies should always have their sheath removed because of the thrombotic complications associated with smaller arteries. Following removal of any arteriotomy sheath, pressure dressings must be available to control any thrombolytic-related bleeding. Femoral arteriotomies are best handled using a combination of femoral artery compression device with Doppler monitoring of distal pulses. The device should be inflated to a pressure sufficient to contain the bleeding, while producing minimal effect on the distal Doppler signal. Radial arteriotomies can be handled similarly by using the radial artery compression device; in most of these cases, Doppler monitoring is unnecessary due to the collateral circulation to the hand. Finally, the most threaded arteriotomies involve the brachial artery, which is an unforgiving vessel. No specific devices for bleeding control are available for this site; we recommend using a standard blood pressure cuff position proximal to the arteriotomy site and always in conjunction with Doppler monitoring of the distal circulation.
Case 1. A 64-year-old woman with past medical history of hepatitis C-induced cirrhosis necessitating liver transplant, hyperlipidemia, and diabetes mellitus presented to the emergency department with chest pain caused by an ST-elevated myocardial infarction. Emergent cardiac catheterization demonstrated left main coronary artery disease treated with percutaneous coronary intervention. Following the procedure, she demonstrated slurred speech, left hemiparesis, right gaze preference, left hemineglect, and an extensor left plantar response. Initial cerebral CT was unremarkable. Laboratory studies were notable only for a chronically elevated white count of 26,500. Potential thrombolytic therapy would preclude a loading dosage of clopidogrel, placing the stent at risk for thrombosis. After a detailed discussion with the family and the cardiologist, intravenous rt-PA was administered, without appreciable clinical benefit. Subsequent CTA of the intracranial vasculature demonstrated truncation of an M2 branch of the right middle cerebral artery consistent with acute occlusion.
An incidental large cavitary right upper lobe pulmonary lesion was discovered. Fungal elements were cultured from a bronchioalveolar lavage. Needle biopsy of the pulmonary apical lesion was deferred in view of necessity for dual antiplatelet therapy to maintain stent patency over the short-term. She was treated with empiric voriconazole and followed with surveillance chest CT imaging. Brain MRI demonstrated extensive restricted diffusion in the right frontotemporal region with borderline increased T2/FLAIR hyperintensity compatible with acute or early subacute infarct.
Case 2. Following a prolonged right and left heart catheterization, we were consulted to evaluate a 42-year-old man with bilateral upper extremity (R > L) weakness. Pertinent past medical history included dextrocardia with situs solitus, so-called “congenitally corrected” transposition of the great arteries (eg, ventricular inversion with left-anterior aortic malposition), multiple ventricular septal defects, and valvular pulmonic stenosis. He had prior ischemic strokes with old areas of left frontal and right striatal encephalomalacia on CT. In addition, he had evidence of abnormal segmentation of C5 and C6, with a 5 mm posterior subluxation of C5 with respect to C6 on cervical spine x-rays.
Pertinent findings on neurologic examination included a “waiter’s tip” posturing of the upper extremities. There was marked weakness (R > L) of shoulder abduction and elbow flexion with the supinated arm, weak flexion of the forearm with the forearm midway between pronation and supination, weak external rotation of the upper arm, and preservation of shoulder elevation. Biceps and brachioradialis reflexes were absent. Triceps reflexes were preserved. There were bilateral Hoffmann responses. He had bilateral patellar hyperreflexia with positive suprapatellar reflexes and bilateral crossed adductor responses. Ankle reflexes were brisk without clonus. Both plantar responses were extensor. There was minimal decreased sensation to pinprick on the medial aspect of the left hand.
A clinical diagnosis of bilateral Erb type of brachial plexopathies with superimposed upper motor neuron findings from prior stroke was made. EMG showed acute denervation in C5, C6 innervated muscles bilaterally. Motor axons were anatomically continuous to some degree. The patient received intensive physical therapy and had a complete recovery of his bilateral brachial plexopathies at 6-month follow-up.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Margaret Yu MD
Dr. Yu of the University of Illinois Chicago has no relevant financial relationships to disclose.
See ProfileJose Biller MD
Dr. Biller of the Stritch School of Medicine at Loyola University of Chicago has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026