Stroke & Vascular Disorders
Medical complications of stroke
May. 03, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The number of cardiac procedures has increased rapidly. Neurologists are often called for consultation before or after cardiac procedures. Ischemic stroke, diffuse encephalopathy, and altered cognitive status are the most important neurologic complications of cardiac procedures.
• Most neurologic complications of cardiovascular procedures are due to embolism, hypoperfusion, seizures, infections, metabolic disturbances, or medication side effects. | |
• Ischemic stroke rate in the postoperative period is as high or even higher than intraoperatively. | |
• Brain MRI is more sensitive than head CT for detecting ischemic stroke. | |
• Peripheral nerve injury is mostly due to compression from a local hematoma and is usually transient. |
The number of cardiac procedures and, along with them, perioperative neurologic complications, has been steadily increasing. Neurologists are often consulted for both their prevention and management.
This review covers the neurologic complications of cardiovascular procedures, including coronary artery bypass graft surgery, cardiac valve procedures, cardiac catheterization for percutaneous coronary interventions, radiofrequency ablative procedures, closure of the patent foramen ovale, and cardiac transplantation.
Neurologic complications of heart transplantation. The main neurologic complications of cardiac transplantation are:
• Ischemic stroke |
Cerebrovascular events occurring soon after transplantation resemble those seen after valvular or coronary revascularization surgery. The risk factors include hypotension, cardioembolism, seizures, metabolic disturbances, and medication side effects. In a series of 322 patients, preexisting valvular heart disease was associated with ischemic stroke, whereas diabetes and renal failure were associated with seizures (132).
During cardiac transplantation, circulation is supported by a left ventricular assist device or an artificial heart. These devices may generate emboli that can cause a stroke (172). In a study of 382 patients of whom 140 received a left ventricular assist device, the predictors of ischemic stroke were 81 mg or less of aspirin and atrial fibrillation. For hemorrhagic stroke, the predictors were a mean arterial pressure of greater than 90 mm Hg, 81 mg or less of aspirin, and an INR of greater than 3.0 (171).
Another study combining data from the ENDURANCE destination therapy (DT) and ENDURANCE Supplemental (DT2) trials found that out of 604 patients who received a left ventricular assist device over 2 years, 29.5% had at least one stroke or transient ischemic attack; 7.3% had a hemorrhagic stroke, and 19.2% an ischemic stroke. The perioperative stroke rate was 5%. More than 2 weeks after a left ventricular assist device implant, supra- and sub-therapeutic INR values were associated with all stroke subtypes. Mean arterial pressure was higher among those with ischemic stroke but not with hemorrhagic stroke (33).
Any time a transplant patient experiences a delayed awakening following the procedure, one should consider ischemic stroke as a potential etiology, especially if there are prolonged cross-clamping times, hypotension during the procedure, or increased need for transfusion. In comparison to other cardiac surgeries, those who undergo heart transplant have a higher ischemic stroke rate, with incidence being 5% to 11%, and 20% of those patients experiencing their event within the first 2 weeks. Factors that increase the risk of stroke include older age, history of stroke, longer duration of mechanical ventilation, increased need for blood transfusion, and longer time on a transplant waitlist (41).
After cardiac transplantation, the aortic arch and the cervical vessels may also serve as embolic sources. Weeks to months later, the neurologic complications are caused by opportunistic infections, immunosuppression side effects, and lymphoproliferative disorders.
Neurologic complications of coronary artery bypass graft surgery.
• Central nervous system complications | ||
- Ischemic stroke and transient ischemic attack | ||
• Peripheral nervous system complications | ||
- Brachial plexus injury | ||
Ischemic stroke. The perioperative stroke rate at a single center, including 45,432 patients who underwent coronary artery bypass graft, revealed that perioperative stroke rate has declined over the last 30 years. Ischemic stroke occurs postoperatively more often than intraoperatively. Intraoperative stroke rates were lowest with off-pump coronary artery bypass graft (0.14%) and on-pump beating-heart coronary artery bypass graft (0%) and highest with on-pump coronary artery bypass graft with hypothermic circulatory arrest (5.3%) (169). Overall, rates of postoperative stroke have been estimated to be between 0.8% and 5.2% (62).
Brain MRI detects more ischemic lesions than head CT. The most common neuroimaging pattern is of multiple embolic punctate infarcts in the cerebral and cerebellar cortex, including in patients with encephalopathy without focal neurologic findings (185). Interestingly, a small case series that examined patients who completed MRI with DWI after coronary artery bypass graft surgery regardless of neurologic deficit found that between 18% and 26% had some form of ischemia if they were classified as “low-risk” patients, and 45% to 62% had ischemia present if they were considered “high-risk” patients. Lesions noted were often small and multifocal and often were not associated with focal deficits (62).
Microembolic perioperative stroke occurs especially in the border zones, but also in subcortical regions resembling lacunar lesions (78; 104; 99).
Involvement of the border zone between the middle and posterior cerebral arteries causes visual field defects and transcortical sensory aphasia. Lesions located between the middle and anterior cerebral arteries result in proximal-dominant extremities weakness (man in the barrel syndrome) and transcortical motor aphasia. Infarctions between superficial and deep branches of the middle cerebral arteries may present as mutism and rigidity. Watershed infarct of the cerebellum can present as dizziness, vertigo, and ataxia (77; 71).
Border zone infarction in the spinal cord often occurs at the midthoracic level between the spinal arteries and the artery of Adamkiewicz. This may result in acute urinary retention, flaccid paraparesis, and sensory loss with level (71).
Of interest is the timing of surgery in patients with both carotid artery stenosis and coronary artery disease. In simultaneous surgery, the rate of strokes was higher, but mortality was similar compared to surgery for carotid artery stenosis, followed by coronary artery bypass graft. However, there were no significant differences in 1-year mortality, and rates of myocardial infarction and transient ischemic attacks (31).
Depressed level of alertness. Decreased consciousness suggests diffuse encephalopathy. Somnolence occurs when the patient is fully attentive to surroundings while aroused, but alertness decreases rapidly to a sleep-like state. Brief arousal associated with decreased awareness or interest in surroundings is called obtundation. Decreased alertness associated with grimacing or withdrawal from painful stimuli characterizes stupor.
The persistence of the sleep-wake cycle characterizes the vegetative state. Chewing, teeth grinding, or scratching movements can occur. The persistent vegetative state lasts more than 4 weeks, and it becomes permanent after 3 months. The comatose patient is not arousable, but the brainstem reflexes are preserved. Brain death is characterized by the absence of alertness to external stimuli and all brainstem reflexes.
Nonconvulsive status epilepticus must be excluded in patients with altered alertness. Electrolyte imbalance, acute liver or renal dysfunctions, hypoxia, or hypotension should also be considered. Stroke does not usually affect alertness unless it involves the reticular activating system. Large hemorrhagic or ischemic strokes can decrease alertness by increasing intracranial pressure.
Altered awareness. Confusion is characterized by normal alertness but decreased awareness, orientation, or memory. Restlessness or agitation are typical for delirium. Together, they cause cognitive impairment.
Approximately half of the coronary artery bypass graft procedures result in early cognitive impairment. Improvement usually occurs within 6 months, but in one third of cases, the deficits persist up to 12 months (122). Two thirds of patients have complete resolution of neurologic deficits during long-term follow-up (96). However, delayed cognitive impairment may occur after 5 years (123). Prolonged cognitive complaints have been reported in up to 42% of patients 5 years after cardiac surgery.
Prior stroke is a risk factor for delirium after coronary artery bypass graft (144). MRI imaging in patients with cognitive impairment can reveal multiple small brain lesions (92).
Cognitive impairment may be related to cerebral microembolism, hypoperfusion, edema, inflammation, or metabolic derangements.
The levels of tau protein and neurofilament light protein, specific markers for neuronal injury, may help predict the risk of delirium (146; 29). Tau protein level improves with the clinical status of the patient (08). The serum level of neuroserpin, a highly neuron-specific and extremely sensitive protein, is another promising marker for neuroregeneration after off-pump coronary artery bypass graft (166).
Seizure. The incidence of seizures after coronary artery bypass graft is about 0.5% (62). Seizure etiology is multifactorial; stroke, atherosclerotic or air embolism, inflammatory mediators released during surgery, and epileptogenic medications (antifibrinolytics and cephalosporins).
Asymptomatic embolism. Asymptomatic embolism occurs frequently during coronary artery bypass graft and endovascular procedures (63).
Brachial plexus injury and mononeuropathies. Brachial plexus injury and mononeuropathy may occur after compression or stretching during surgery, often occurring due to chest wall retraction utilized with harvesting of the left internal mammary artery (62). The lower trunk of the brachial plexus is more vulnerable than the upper trunk. Injury to the phrenic nerves with unilateral or bilateral diaphragmatic paralysis may result from direct manipulation of the nerve, ischemia, or cold cardioplegia (45; 84).
Neurologic complications of left heart catheterization.
• Central nervous system complications | ||
- Ischemic stroke and transient ischemic attack | ||
• Peripheral nervous system complications | ||
- Lumbosacral plexopathy | ||
CNS complications after left heart catheterization are rare. Ischemic stroke is the most common (55%), followed by transient ischemic attack (26%), contrast reaction (15%), and neurologic symptoms of unknown etiology (4%). The most common symptom is visual disturbances, including diplopia and visual loss. Hemiparesis or aphasia, facial weakness with or without aphasia or dysarthria, and paresis in the face and arm were also described. Transient unresponsiveness, transient global amnesia, seizures, delirium, and migraine may also follow left heart catheterization.
Ischemic stroke caused by large vessel occlusion has a worse outcome compared with small vessel occlusion (149). Cerebral embolism usually originates from the atheromatous aortic arch or the clots forming at the catheter tip.
Femoral nerve injury. Femoral artery puncture can rarely cause pseudoaneurysm, hematoma, arteriovenous fistula, and femoral artery occlusion. Femoral nerve compression incidence is 0.2%. The severity ranges from mild transient sensory neuropathy to disabling paralysis. The average delay from catheterization to recognition of symptoms is 37 hours; severe pain precedes the diagnosis of neuropathy in about half of patients. Although initially disabling, neuropathy usually resolves completely; surgery is only recommended if there are coexisting complications (87).
Lumbosacral plexopathy. Retroperitoneal hematomas can cause lumbosacral plexopathy, with the femoral and obturator nerves being primarily involved. The size of the hematoma does not correlate with the severity of the sensory or motor deficits.
Neurologic complications of other cardiac procedures.
Aortic aneurysm repair. Aneurysms of the aortic arch are often treated by surgery. In a series of 284 patients undergoing aortic aneurysm repair, death or stroke occurred in 6.6% (165). Transient neurologic dysfunction occurred in 9.2%. Two patients developed brachial plexus injury from axillary artery cannulation. In another report of 103 patients undergoing total aortic arch replacement, about 9% developed stroke, and approximately 7% had transient neurologic deficits. Four percent also had paraparesis or paraplegia (176).
Hypothermic circulatory arrest and selective cerebral perfusion are used to minimize these complications. In a series of 39 consecutive patients undergoing aortic arch replacement surgery with selective brain perfusion by axillary artery cannulation, only one patient had a permanent postoperative neurologic deficit, and two patients had temporary deficits (156).
Endovascular repair of the aortic arch with a branched endograft is an alternative to open surgical repair. Of 147 (99.3%) procedures that were successful, disabling stroke occurred in six (4.1%) patients, and nondisabling stroke in eight (5.4%) (168).
The risk factors for spinal cord ischemic during aortic aneurysm repair are age greater than 65 years; history of neurologic disease, hyperlipidemia, diabetes, coronary artery disease, heart failure, and renal insufficiency; less than 6 months since last aortic repair; chronic anticoagulant use; preoperational hemoglobin less than 9; coagulopathy; hypotension (mean arterial pressure < 70 mm Hg); longer operations (> 100 min); aneurysms longer than 5 cm; and anatomic location of aneurysm caudal to T-11 (12).
Aortic dissection repair. Aortic dissection classification aids in standardizing the management. The American cardiothoracic surgeon DeBakey classified aortic dissection into type I when both ascending and descending segments are involved, type II involves the ascending aorta, and type III involves the descending aorta after the origin of the subclavian artery. Stanford type A dissection includes the segment before the left subclavian artery, and Stanford type B dissection includes the aorta beyond the left subclavian artery. Aortic dissection surgery is lifesaving but can be very complex and associated with severe neurologic symptoms.
Aortic dissection DeBakey type I, which involves both the ascending and descending aorta, remains a severe condition whose repair may result in stroke in 8% and cerebral edema in 1% of patients (47).
In a meta-analysis of 3000 patients who underwent the frozen elephant trunk technique for type A aortic dissection repair, the pooled rates of adverse events were 4.7% for spinal cord stroke, 7.6% for cerebral stroke, and 8.8% for perioperative mortality. The left subclavian artery may occasionally be sacrificed, causing exertion-induced weakness. This may be treated with carotid-subclavian bypass (58).
Retrograde type A acute aortic dissection may benefit from endovascular repair. A retrospective study of 19 patients from one medical center who underwent endovascular repair found no in-hospital or neurologic complications (93).
Type A aortic dissection surgical repair may also cause hemorrhagic stroke, especially if preoperative antithrombotic medication is used. Hemorrhagic stroke was associated with higher complexity of surgery and longer cardiopulmonary bypass and aortic clamping time compared to ischemic stroke. Inpatient mortality, degree of disability, and 5-year mortality were higher in the hemorrhage group (100).
Type B aortic dissection, beyond the left subclavian artery, can lead to life-threatening complications, from rupture to stroke and paraplegia. There is insufficient information regarding the effectiveness and safety of open surgical repair compared to the endovascular approach (80). During thoracic endovascular aortic repair (TEVAR) of type B aortic dissection, the origin of the left subclavian artery is covered in approximately half the cases. The main complications are arm claudication, stroke, and paraplegia (182).
A meta-analysis of left subclavian artery coverage revascularization did not reduce the risk of stroke or mortality (68). However, those who had revascularization before or during TEVAR were less likely to develop neurologic complications (118).
Spinal cord ischemia was significantly higher when the length of the graft exceeded 15 cm or extended beyond T8 (136).
Although unrepaired acute aortic dissection is usually fatal, some unoperated patients survive the acute phase. Out of 205 patients operated after a median duration of dissection of approximately 7 months, 3% had a stroke and 7% had a fatal outcome (187).
Placement of a lumbar drain preoperatively is indicated for the prevention of spinal cord ischemia during TEVAR (54). A study of prophylactic lumbar drain that included 309 procedures performed in 268 patients for 307 endovascular aortic repairs found a complication of 8.1% (4.2 major and 3.9 minor). The complications included paraplegia, intracranial hemorrhage, meningitis, arachnoiditis, CSF leak, bloody tap, and a retained catheter tip (134).
Other methods to prevent ischemia during surgery include the use of cerebral oximetry, intraoperative EEG, bispectral index to measure cerebral perfusion during the procedure, and the use of transcranial Doppler to monitor blood flow (188).
Cardiac valve surgery.
• Ischemic stroke or transient ischemic attack | |
• Seizure | |
• Vasovagal syncope |
Heart valve repair and replacement have been performed for several decades. The incidence of neurologic complications after heart valve surgery is less documented in the literature compared to the complications after coronary artery bypass graft. The incidence of ischemic events has been estimated to be about 2% to 5%, with rates of other neurologic events ranging from 8% to 20%. When DWI MRI was utilized post-procedure, up to 41% of patients had new infarctions, with 35% of patients being noted to have persistent neurocognitive deficits up to 6 weeks out (62).
Balloon valvuloplasty. Balloon valvuloplasty of the aortic and mitral valves is effective and safe. Of 674 patients enrolled in the National Heart, Lung, and Blood Institute (NHLBI) registry who underwent percutaneous aortic balloon valvuloplasty, 2% had strokes, 5% had seizures, 2% had vasovagal syncope, and 0.6% developed transient neurologic deficits in the peri-procedural period (124). A more recent study completed in 2017 reported a stroke rate of 1.8%, indicating stability over time (03).
Aortic valve replacement. Severe symptomatic aortic stenosis is treated by surgical aortic valve replacement (SAVR). In a single-center retrospective analysis of 132 patients who underwent aortic valve replacement, there were no recorded strokes (34).
Transcatheter aortic valve replacement (TAVR) is less invasive and used for symptomatic aortic stenosis with high surgical risk. In a study of 1660 patients with severe, symptomatic aortic stenosis of intermediate surgical risk, the rate of stroke was lower with TAVR than with SAVR. Moreover, those with strokes after TAVR recovered earlier. However, at 12 months, stroke rates and quality of life were similar in both study groups (48). Another study of 1204 pairs of patients treated for severe aortic stenosis found that SAVR was associated with more frequent early major strokes than TAVR (83).
In a meta-analysis and systematic review, in patients with low and intermediate risk, TAVR was associated with a similar rate of neurologic complications and mortality but a higher risk of arterial complications compared to surgical aortic valve replacement (177). Similarly, in another meta-analysis and systematic review of patients at low risk, transcatheter aortic valve replacement and surgical aortic valve replacement had similar neurologic complications (145). DWI lesions were seen on MRI after aortic valve replacement in 38% of patients, related to the preoperative T2 white matter lesion volume (164).
Several characteristics are associated with a higher risk of cerebrovascular events, including advanced age at the time of surgery, history of atrial fibrillation, and history of chronic kidney disease. In addition, bleeding can be associated with a higher risk of further cerebrovascular events, as this often leads to a cessation of antithrombotic agents and, thus, increased risk of thromboembolic events while those agents are being held post-surgery (07).
Mitral valve repair or replacement. Repair or replacement of a nonfunctional mitral valve is often indicated. In a database of 1250 patients, the incidence of stroke after mitral valve surgery was 4.2% to 5% (60; 173). Mitral valve repair offers excellent short- and long-term outcomes. In the elderly, valve repair was less often, but not statistically significantly associated with neurologic complications (46).
Balloon mitral valvuloplasty is an alternative to open surgery for mitral stenosis. In a study of 45 patients, only one patient had a postprocedural stroke (174). Of 201 consecutive patients undergoing this procedure, three developed “thromboembolism.” It is not clear whether these patients developed strokes (186).
Combined procedures. Combined procedures such as double-valve replacements or valve replacement with coronary artery bypass graft increase the risk of neurologic complications. In a review of 2008 patients undergoing valve surgery, the overall risk of stroke was 2.2%, whereas with combined procedures, it was 5.4%. The risk factors were calcified ascending aortic atherosclerosis, advanced age, diabetes, and an ejection fraction of less than 30%. Stroke increased hospital mortality from 4.6% to 24% (52).
In a study, the subcortical lesions seen on brain MRI after valve replacement surgery were associated with impaired memory, attention, and information processing speed. All these cognitive impairments resolved after 4 months (92).
In high-risk patients, endovascular valve replacement is preferred. However, this approach is associated with more frequent neurologic complications.
New, often multiple, ischemic lesions were observed on brain MRI of 27 (84%) patients (81). In another study of high-risk patients, although the 1-year mortality rate was similar in the endovascular and surgical groups, major stroke was more frequent in the endovascular group (5.1% vs. 2.4%) (159).
Patent foramen ovale closure. Recurrent neurologic events may result from paradoxical embolism through a patent foramen ovale. A clinical trial in patients with stroke attributable to patent foramen ovale presence that enrolled 980 patients between 18 and 60 years of age found that patent foramen ovale closure was not superior to medical treatment alone in intention-to-treat analysis but was superior in the prespecified per-protocol and as-treated analyses. The perioperative complications include groin and retroperitoneal hematoma, nerve injury, and atrial fibrillation. Serious adverse events occurred in 4.2% of the patients in the closure group (28).
A meta-analysis including five randomized trials totaling 1829 patent foramen ovale closure patients and 1611 medical therapy patients found that patent foramen ovale closure prevented cryptogenic ischemic stroke and neurovascular and mortality events but increased the risk of atrial fibrillation 4.6 times (183). A more recent study estimated that the risk of postoperative atrial fibrillation may be underestimated, with rates ranging from 20.9% to 37%. Factors that influence the rate of developing atrial fibrillation include age (older), male sex, and size or type of device used (155).
Radiofrequency ablation for atrial fibrillation. Atrial fibrillation is an important cause of stroke. Rhythm can be controlled by radiofrequency ablation (RFA) or long-term antiarrhythmic drugs (90). Although atrial fibrillation is more common in the elderly, radiofrequency ablation is less effective in this population. Those at medium to high risk should continue oral anticoagulant after the procedure (163). The transseptal puncture during ablation creates an interatrial shunt, which favors paradoxical embolism. Moreover, endothelial damage may activate coagulation. Additional studies have shown that radiofrequency ablation has a similar or lower risk of adverse cardiovascular outcomes compared with medical treatment alone, suggesting that perhaps the previously held view that medication should be a first-line therapy should be challenged (14). However, complications are still possible and should be considered.
Radiofrequency ablation was associated with 1.02% neurologic complications in a study of 93,801 procedures performed in the U.S. between 2000 and 2010 (42). Analysis of 3360 consecutive cases of radiofrequency ablation revealed 0.5% peri-interventional thromboembolic events within 1 month, of which 45% were strokes. Most events occurred within 48 hours. The risk factors for peri-procedural thromboembolism are peripheral vascular disease and previous stroke (94).
A rare, potentially fatal complication of radiofrequency ablation is the atrioesophageal fistula. A retrospective analysis of 28 cases of atrioesophageal fistula found that complications developed within 1 month of the procedure. They included fever, neurologic symptoms, and hematemesis. The neurologic symptoms are confusion, seizures, meningitis, stroke, and post-prandial transient ischemic attack. Blood tests, including cultures, were consistent with sepsis. Lumbar puncture may show pleocytosis, elevated protein, lactate, and bacteria. The fistula may be aggravated by the insertion of a nasogastric tube, endoscopy, or transesophageal echocardiography (162). CT of the chest is the preferred diagnostic test. Esophageal repair may be lifesaving (32).
Watchman left atrial appendage closure for atrial fibrillation. The Watchman left atrial closure device was not inferior to warfarin for the prevention of stroke due to nonvalvular atrial fibrillation (76). In a systematic review of thrombosis associated with 2118 devices (Watchman, Amplatzer cardiac plug, and Amulet), the incidence of thrombosis was 3.9%. The median time to diagnosis was 1.5 months (97). However, in a small pilot study of 21 patients who underwent brain MRI 48 hours before and 24 hours after the insertion of Watchman, Amplatzer, or Amulet devices, the rate of silent cerebral infarcts was not significantly increased (95). Recurrent neurologic symptoms may be caused by late device dislodgement, which requires device extraction (115).
Postoperatively, the prediction of early neurologic complications may accelerate diagnosis as well as early intervention (05). Less than one third of perioperative strokes cause severe disability at the time of discharge (154; 109; 99).
Several biomarkers were studied to predict perioperative neurologic complications. Preoperative serum NMDA receptor antibody levels correlate with neurologic complications in a study of 557 high-risk patients who underwent coronary artery bypass graft or valve replacement (17). Elevated preoperative serum C-reactive protein level correlated to higher mortality after coronary artery bypass graft (82).
Preoperative S100-β level did not correlate with perioperative neurologic complications (17). However, the persistent postoperative elevation of S100-β, a calcium-regulating astroglial protein released by brain injury, correlated with cardiopulmonary bypass time and decreased Mini-Mental State Examination score (50). Another study of 35 patients who underwent abdominal aorta repair failed to confirm a correlation between plasma or CSF S100-β level and cardiopulmonary bypass (143).
Analysis of 92 neurologic-related proteins in the serum and CSF of 23 patients, before and after aorta surgery, aimed to assess the risk of neurologic injury. Spinal cord injury was associated with IL-6, GFAP, CSPG4, delirium with TR4 and EZH2, and hallucinations with NF1 (101).
However, cognitive dysfunction after cardiac surgery does not correlate with global cortical beta-amyloid deposition (91). Research by the NIH has found that postoperative levels of GFAP, NFL, tau, and UCHL1 (all biomarkers) increase regardless of whether the patient experiences postoperative neurocognitive change. This suggests that cardiac surgery results in some form of neuroaxonal damage (as evidenced by increases in NFL, tau, and UCHL1) and glial activation (as evidenced by an increase in GFAP) (184).
The response to surgery is only partially explained by patients’ characteristics or procedure variables. Knowledge of genetic variability may improve short- and long-term outcome prediction. Neurologic complications range from subtle cognitive deficits (up to 69%) to stroke and coma (up to 6%). For example, the APOE genotype modulates the inflammatory response, atherosclerosis, and autoregulation. Genetic variants in platelet membrane glycoproteins modulate thrombosis, and along with the inflammatory mediators, the propensity for perioperative stroke. The intensity of neuroendocrine and metabolic response to surgical trauma, like antidiuretic and stress hormones, the renin-angiotensin system, depends on the severity of trauma or sepsis. Insulin resistance is related to perioperative adverse events after cardiac surgery (135).
APOE4 genotype may be related to adverse cerebral events (170). Moreover, the APOE4 allele is associated with worse cognitive recovery 5 years after surgery (10). Genetic variants of the C-reactive protein and interleukin-6 genes are associated with stroke after cardiac surgery (65).
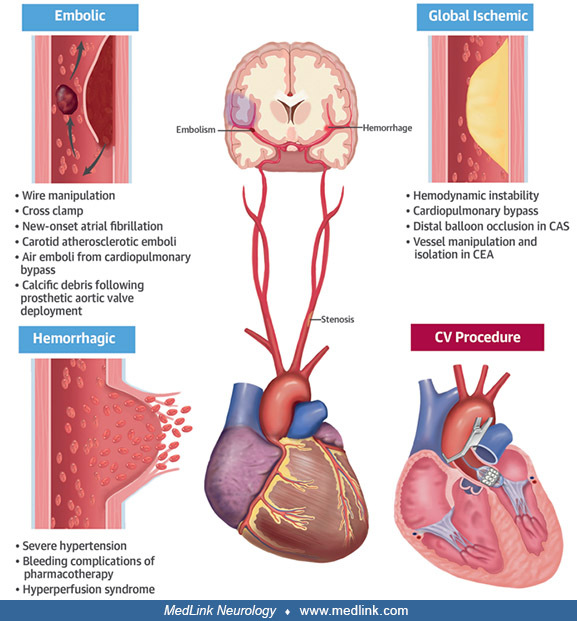
The main causes of neurologic complications of cardiac procedures are:
|
• Embolism of blood clots, atherosclerotic debris, or originating in the devices used to maintain circulation. | |
|
• Activation of coagulation on contact between blood and cardiopulmonary bypass circuit or left ventricular assist device. | |
|
• Alteration of the cerebral excitability by medication | |
|
• Compression of peripheral nervous fibers | |
|
• Infection | |
|
• Immunosuppression |
Ischemic stroke or transient ischemic attack after cardiac procedures. Cerebral dysfunction after cardiac surgery is attributed to embolism and intraoperative alterations in blood pressure (57). The mechanisms underlying postoperative neurologic dysfunction include microemboli and hypoperfusion during surgery and postoperative atrial fibrillation (111).
In a retrospective study of 16,184 patients, the risk factors for stroke after cardiac surgery were prior stroke, hypertension, diabetes, peripheral vascular disease, preoperative infection, and prolonged cardiopulmonary bypass (23). Additionally, older age (especially over 80 years), more severe cardiovascular disease, and cumulative vascular risk factors increase the risk for stroke after cardiac procedures (89).
The acute brain edema seen on the MRI FLAIR sequence shortly after surgery primarily affects the cortex. This correlates with the pathological finding of the cortex and deep gray matter arteriolar and capillary dilatations (70). The vascular dilatations noted after cardiopulmonary bypass are thought to be caused by emboli (114). Overall, the leading differential diagnosis for the cause of cerebral ischemia after cardiac procedures is of embolic origin, supported by the finding that ischemia is often found in multiple vascular territories (89).
Emboli are classified as macroemboli (if greater than or equal to 200 microns) and microemboli (16). Embolization can occur during aorta cannulation, decannulation, cross-clamping, or the use of an intraaortic balloon pump. Emboli may consist of cholesterol particles from the proximal aorta, air from the heart or open aorta, calcium particles from the aorta or mitral and aortic valves, and blood clots from the left atrium or ventricle (142). Other microemboli consist of gas bubbles from oxygenators, fat from cardiotomy cell clumps, and silicone particles from the bypass pump. The smallest emboli scatter widely and are more likely to cause generalized neuropsychological alterations than hypoxia (71). The number of fatty microemboli increases with the duration of the cardiopulmonary bypass (22). Large vessel occlusion can cause symptoms corresponding to its distribution and result in stroke or coma (18).
Coagulation pathway activation by the cardiopulmonary bypass circuit leads to platelets and coagulation factor consumption (02; 88). The release of tissue factor is the main trigger of coagulation during the cardiopulmonary bypass (44).
Impaired autoregulation may explain the increased risk of perioperative stroke in patients with a history of stroke and diabetes mellitus (142).
Cognitive impairment after cardiac procedures. The mechanism of the biphasic cognitive decline after coronary artery bypass graft surgery is unclear. Some early short-term cognitive changes may be multifactorial and reversible (150). Perioperative ischemic stroke is not always related to cognitive decline (36).
Risk factors associated with cognitive impairment after surgery can often be separated into factors present before surgery and those present intraoperatively. Preoperatively, factors include advanced age, pre-existing cognitive impairment, depression, diabetes, and lower education levels. Additionally, there is some evidence that the APOE4 genotype could play a role. Intraoperatively, surgical approach, need for bypass, surgery duration, blood pressure, and hemoglobin levels play a role (180).
The perioperative burden of hypertension or hypotension affects both short- and long-term outcomes in cardiac interventions, including stroke, delirium, and death (102).
Cerebral autoregulation in the spared brain is diminished perioperatively and may lead to cognitive dysfunction, worse clinical outcome, and even death (103).
The main complications of cardiac procedures are:
|
• Stroke | |
|
• Encephalopathy | |
|
• Cognitive impairment | |
|
• Headache | |
|
• Seizures | |
|
• Infections |
Percutaneous coronary intervention . Most coronary revascularization is achieved by percutaneous coronary intervention, an increasingly popular approach due to higher safety than coronary artery bypass graft (105). The incidence of stroke (ischemic and hemorrhagic) after cardiac catheterization ranges from is 0.07% to 7.0%(89). However, many perioperative embolic events are clinically silent. Approximately 15% of patients who underwent cardiac catheterization had asymptomatic ischemic cerebral lesions on MRI-DWI (25).
Coronary artery bypass graft. In a retrospective study of 2985 patients who underwent coronary artery bypass graft, the incidence of stroke was 1.6%, similar to conventional coronary artery bypass graft and off-pump coronary artery bypass graft. However, more recent studies have been compiled into the https://www.sts.org/research-data/registries/sts-national-database, which estimates the incidence of stroke after coronary artery bypass graft to be around 1.3%, an overall decreasing trend over the years (56). The mechanism is large artery embolism in 76% and watershed in 15% of cases. Previous stroke, extensive aortic calcification, female gender, and congestive heart failure were predictors of stroke. The in-hospital mortality and long-term survival rate were affected by perioperative stroke (53). In prospective studies, the incidence of stroke after coronary artery bypass graft was 1.5% to 5.2% (110; 152; 24).
Of 4140 patients who underwent isolated coronary artery bypass graft, 2.5% had early (less than 24 hours) and 0.9% late (more than 24 hours to discharge) stroke. To that end, the major etiologies of stroke during the intraoperative period remain thromboembolism and hypoperfusion, whereas the major etiologies of stroke in the early postoperative stage (first 7 days) include arrhythmias and hemodynamic instability. In later days (days 7 to 30), patient risk factors come into play, including older age, previous stroke, hypertension, hypercholesterolemia, diabetes, and peripheral vascular disease (56).
Combined surgery. In a single-center study of 4335 patients, in coronary artery bypass graft with or without aortic valve replacement, stroke was detected in 1.8%. The combination of coronary artery bypass graft with carotid endarterectomy increased the risk of perioperative stroke from 0% to 15.1% (98).
Percutaneous coronary intervention versus coronary artery bypass graft. Pooled data analysis of 11 randomized clinical trials, including 11,518 patients, found a reduced risk of stroke at 30 days and 5 years after the procedure. Patients who had a stroke within 30 days after the procedure had significantly higher mortality compared to those who did not have a stroke (72).
Heart transplantation. Experience from a single center, including 200 patients, revealed that 23% had neurologic complications: ischemic stroke, seizures, diffuse encephalopathy, headache, and cerebral infections. Preoperative mechanical circulatory support requirement was the most important predictor of poor neurologic outcome (189). The risk factors for ischemic stroke after cardiac transplant are prior stroke and dilated cardiomyopathy (79; 13).
Prevention of perioperative neurologic complications includes:
• Preoperative evaluation should include prior stroke, large vessel atherosclerosis, valvular disease, and atrial fibrillation. | |
• Treatment of hyperglycemia, hypotension, and hyperthermia is recommended. | |
• Dexmedetomidine administered perioperatively does not prevent perioperative delirium. | |
• Cerebral protection devices may be tested. |
Comprehensive preoperative evaluation of risk factors, including prior stroke, carotid stenosis, and aortic atherosclerotic plaques, may help prevent complications after coronary artery bypass graft surgery (27).
Hyperthermia after coronary artery bypass graft is associated with decreased cognitive function (64). Off-pump coronary artery bypass graft surgery patients experience less hyperthermia than on-pump patients. The reason may be a lower level of inflammation during off-pump coronary artery bypass graft. Measures to avoid hyperthermia are reasonable (35).
A systematic review and meta-analysis including 34,650 patients found that a glycosylated hemoglobin level lower than 7% is associated with a decreased risk of stroke and transient ischemic attack (risk ratio 0.53; 95% confidence interval, 0.39-0.70; P < .0001). This suggests that optimal glycemic control before cardiac surgery is reasonable (37).
Preoperative statins have been shown to reduce mortality from coronary artery bypass graft surgery but not the risk of stroke (128). In a retrospective study, beta-blockers and statins reduced the number of perioperative strokes (19). Ideally, an LDL of less than 55 should be targeted, and if not reached with high-dose statins, ezetimibe can be introduced to reach the target level (51).
Postoperative atrial fibrillation was associated with cognitive impairment (160). In a systematic review with meta-analysis of five studies of treatment with oral anticoagulation for atrial fibrillation after cardiac surgery, including 203,946 patients, the risk of thromboembolic complications was reduced, but the risk of hemorrhagic complications was higher than without anticoagulation. Further studies are needed to confirm this finding (121). Use of rate-control medications pre-operatively and postoperatively remains controversial, as evidence of the benefits of use is still lacking. If introduced, it should be done cautiously, with gradual dose adjustment and short-acting agents (51).
Cerebral embolism after transcatheter aortic valve replacement did not differ significantly between the groups receiving dual antiplatelet and anticoagulation with edoxaban (129).
In a systematic review and meta-analysis, including 6018 patients, mild hypothermia during surgery is associated with a lower risk of stroke compared with deep hypothermia (OR 0.50; 95% CI 0.28-0.89).
A systematic review found that dexmedetomidine does not decrease delirium as it was initially thought (130).
Neurologic complication risk factors associated with general cardiac surgery. Several studies have attempted to identify the subset of patients at high risk preoperatively.
A. Factors predicting postoperative neurologic complications (141) | |||
1. Preoperative factors | |||
a. Carotid stenosis greater than 50% | |||
2. Intraoperative factors | |||
a. Valve surgery | |||
B. Factors predicting higher postoperative mortality (99) | |||
1. Preoperative factors | |||
a. Carotid stenosis greater than 50% | |||
2. Intraoperative factors | |||
a. Longer cardiopulmonary bypass | |||
C. Factors predicting perioperative stroke (110) | |||
1. Preoperative factors | |||
a. Age | |||
2. Intraoperative factors | |||
a. Longer cardiopulmonary bypass | |||
D. Factors predicting postoperative delirium (23) | |||
1. Preoperative factors | |||
a. Prior cerebrovascular disease | |||
2. Intraoperative factors | |||
a. Need for massive blood transfusion | |||
E. Factors predicting postoperative neurologic complications (151) | |||
1. Preoperative factors | |||
a. Hypertension | |||
2. Intraoperative factors | |||
a. Severe hypotension | |||
3. Postoperative factors | |||
a. Occurrence of atrial fibrillation | |||
F. Factors predicting postoperative seizure (107) | |||
1. Preoperative factors | |||
a. Renal dysfunction | |||
2. Intraoperative factors | |||
a. Open heart surgery | |||
Age. Advanced age is a major predictor of stroke and cognitive dysfunction following cardiac surgery (61). In a study of 2000 patients who underwent cardiopulmonary bypass, the neurologic deficits occurred nine times more often in those 75 years or older compared to those younger than 65 years of age. The mortality rate was nine times higher (35.7% vs. 4.0%) in patients with perioperative neurologic deficits than in those without deficits (113). Fortunately, new surgical techniques have improved the outcome in elderly patients (140).
Sex. Women have an increased risk of perioperative neurologic complications and mortality (74).
Previous stroke. A history of stroke predicts perioperative complications or stroke. Awakening from anesthesia is prolonged, and the likelihood of confusion or reintubation is higher. The risk of focal neurologic deficits, new strokes, and reappearance or worsening of previous stroke symptoms is increased (138; 75).
Open heart surgery. Intracardiac air embolism may complicate open-heart surgery. Leaflet and annulus calcium deposits embolization during cardiac valve replacement, high-intensity transient signals (HITS). The number of high-intensity transient signals correlates with the neuropsychological outcome (137).
Ascending aorta atheroma. The presence of ascending aorta atheroma predicts neurologic events, stroke, prolonged hospitalization, and mortality after surgery (39; 40; 09; 139). Embolism is reduced by avoiding aortic manipulation during surgery (178).
Off-pump surgery lowers the incidence of stroke compared to the on-pump group (0.4% vs. 3.9%) (131). The off-pump, no-touch surgical technique avoids aortic manipulation and the effects of cardiopulmonary bypass (139; 26). Intraoperative ultrasound of the proximal aorta helps to avoid the area of plaque before clamp placement and prevent perioperative stroke (113; 126).
Cardiopulmonary bypass. Cardiopulmonary bypass provides circulatory support during cardiac surgery. However, the bypass circuit is thrombogenic. Coating the bypass circuits with phosphoryl-choline or heparin seems to reduce thromboembolic complications (43; 73). Longer duration of cardiopulmonary bypass increases the perioperative neurologic complications (113; 99).
In a small study, surgery performed without cardiopulmonary bypass, the off-pump technique, has reduced overall morbidity and mortality compared with on-pump surgery (04). However, another study, enrolling 2203 patients who underwent coronary artery bypass graft, did not find a significant difference in the composite outcome, stroke, or neuropsychological decline between the two groups at 30 days (157).
Perioperative mean arterial pressure. Cerebral blood flow remains constant to sustain the brain metabolism. Blood flow is defined as cerebral perfusion pressure divided by cerebrovascular resistance. Autoregulation maintains the cerebral blood flow relatively constant at cerebral perfusion pressure values between 50 and 130 mmHg.
Cerebral perfusion pressure is the difference between the mean arterial and intracranial pressure. As the intracranial pressure is constant, around 10 mmHg, it is suggested to maintain the mean arterial pressure between 60 and 140 mmHg during the procedure.
Initial studies suggested maintenance of mean arterial pressure at greater than 50 mmHg to prevent cerebral dysfunction. Subsequent studies did not confirm these findings (55; 113; 158).
Carotid artery stenosis. The incidence of hemodynamically significant carotid stenosis is 11% to 20% in patients undergoing cardiac operations (167).
In a retrospective review of 1022 coronary artery bypass surgery patients, the overall rate of perioperative stroke was 2.2%. The rate was increased with the severity of extracranial carotid stenosis, from 4.7% in less than 70% stenosis, 5% in 70% to 99% stenosis to 8% in total occlusion (38).
In patients with asymptomatic carotid stenosis undergoing coronary artery bypass graft, the risk of in-hospital stroke or death was similar regardless of the degree of carotid stenosis (148).
Summary. Common risk factors are advanced age, carotid artery stenosis, prior heart surgery, prior stroke, peripheral vascular disease, hypertension, diabetes mellitus, aortic atheroma, open heart surgery, and prolonged cardiopulmonary bypass time.
Risk factors associated with left heart catheterization.
Risk factors of CNS complications. Risk factors include female sex, peripheral vascular disease, left ventricular hypertrophy, severe coronary disease, poor left ventricular ejection fraction, concomitant peripheral vascular disease, percutaneous coronary intervention, longer fluoroscopy times, and protruding aortic atheroma (175; 96; 149). Aspirin administration before percutaneous coronary intervention has been associated with decreased risk of in-hospital mortality and stroke (86).
Risk factors of peripheral nervous system complications. Thrombocytopenia, female sex, and excessive anticoagulation (aPTT > 150 seconds) are strong predictors of retroperitoneal hemorrhage. However, there is no strong correlation between the hematoma size and the severity of neurologic deficits. Most patients are treated by transfusion alone (an average of 4 units). Urgent surgery is needed if hypotension is refractory to fluid administration (87). Neurologic complications during intra-aortic balloon pump include peripheral nerve injuries and, rarely, paraplegia related to spinal cord infarction (11).
Further risk factors for stroke during left heart catheterization include pre-existing atherosclerotic plaque in the aorta or aortic arch, complex anatomy, multiple catheter exchanges mid-procedure, and need for stiff or wide- or large-bore catheters (106).
Perioperative neurologic dysfunction following cardiac catheterization and surgery is generally due to surgical and catheter manipulations. However, other nonsurgical factors such as drugs, infection, lymphoproliferative disorders, and metabolic derangements may also play a role, particularly in cardiac transplantation patients.
The key tests used in patients who experience complications following cardiac procedures are:
|
• Head CT | |
|
• Brain MRI. There is increasing evidence of safety in patients with cardiac pacemakers and defibrillators. | |
|
• Coagulation profile | |
|
• Blood and fungal cultures | |
|
• Lumbar puncture | |
|
• EEG |
CT is the first-line imaging modality for acute stroke care. Diffusion-weighted MRI is more sensitive to ischemic lesions that are small or in unsuspected locations. However, MRI is not readily accessible in most emergency departments (25). Concern persists in patients with cardiac pacemakers and defibrillators (15). However, several studies have demonstrated the safety of cerebral MRI in these patients (127; 147; 116). Patients with pulmonary artery catheters that include pacing or thermistor wires should not undergo MRI (125). Coagulation intensity with heparin and Coumadin is monitored with APTT and PT/INR, respectively. Fever is an indication of blood cultures and, in some cases, lumbar puncture.
Electrographic seizures occur infrequently after cardiac surgery and are generally associated with a good prognosis. Hence, prophylactic continuous EEG monitoring is unlikely to be cost-effective in this population (59).
• Intravenous thrombolysis may be contraindicated in patients who have undergone a recent surgical procedure. | |
• Intra-arterial thrombolysis has been used successfully in strokes following cardiac catheterization. | |
• Mechanical thrombectomy is an option if a large cerebral artery is occluded. | |
• Perfusion studies may help select patients with large arterial occlusion up to 24 hours from stroke onset. | |
• Permissive hypertension should be used cautiously in unstable cardiac patients. | |
• The risk of death or severe cardiovascular morbidity is high, but there is no significant difference between synchronous and staged carotid artery revascularization and coronary artery bypass graft surgery. |
Management of peri-procedural stroke. Treatment of periprocedural stroke is similar to that of ischemic stroke. Urgent head CT is needed to exclude intracerebral hemorrhage. Intravenous tissue plasminogen activator can be given within 4.5 hours from the stroke onset unless contraindicated by coagulopathy or recent surgical procedure. Large vessel occlusion with salvageable penumbra, less likely to respond to tPA, may be treated, within 24 hours in selected cases, with endovascular thrombectomy. Cerebral perfusion imaging by CT or MRI may help with the selection for mechanical thrombectomy of large vessel occlusion with a significant mismatch between the penumbra and infarct core (108). In a retrospective database of 5022 consecutive patients, 870 underwent endovascular thrombectomy and had excellent outcomes (67).
In the acute period, permissive hypertension should be avoided in certain cardiac conditions like pulmonary edema, aortic dissection, and acute myocardial infarction, or when organ injury is suspected.
During cardiac catheterization. There is anecdotal evidence of successful intra-arterial thrombolysis for ischemic stroke during or after cardiac catheterization (89).
After coronary artery bypass surgery. Recent surgery is a contraindication to intravenous tPA. There is anecdotal evidence of benefit from intra-arterial thrombolysis (85). Permissive hypertension may be used cautiously after surgery to prevent bleeding from an unhealed surgical site.
After cardiac transplantation. Patients waiting for cardiac transplantation require circulatory support from a left ventricular assist device. This device is thrombogenic and requires anticoagulation, a contraindication for intravenous tPA (117). Mechanical thrombectomy can be used for large vessel occlusion. Permissive hypertension should be cautiously used in patients with heart failure.
Management of potential stroke risk factors that are commonly found during preprocedural screening.
Patent foramen ovale. Patent foramen ovale allows an embolus to travel from the venous to the arterial systemic circulation. Larger right-to-left shunts are linked to higher rates of embolism. Patent foramen ovale closure reduces the risk of stroke in selected patients without other risk factors for stroke, which is not the case in most perioperative strokes (112).
Carotid artery stenosis. Carotid endarterectomy may benefit carefully selected patients with symptomatic and asymptomatic carotid stenosis (69). As coronary artery disease and carotid stenosis may coexist, optimal timing of carotid endarterectomy relative to coronary artery bypass graft surgery has been of interest. Carotid duplex ultrasound screening is reasonable before elective coronary artery bypass graft surgery in patients older than 65 years of age and those with left main coronary stenosis, peripheral arterial disease, a history of cigarette smoking, a history of stroke or transient ischemic attack, or carotid bruit.
A systematic review of 97 studies of combined carotid endarterectomy and coronary artery bypass graft surgery did not find a significant difference between the synchronous and staged procedures. The risk of stroke or major cardiovascular morbidity was 10% to 12% (119). In a meta-analysis of 12 studies including coronary artery bypass graft patients with asymptomatic unilateral carotid stenosis, the lowest risk of stroke or death was observed in the synchronous carotid endarterectomy and off-pump coronary artery bypass graft surgery group (2.2%), whereas the risk of the other groups was 7% to 8% (49).
Carotid artery stenting (CAS) is an alternative to carotid endarterectomy (21). A meta-analysis of 11 studies examined the overall operative risk of cardiovascular events in patients undergoing staged carotid artery stenting plus coronary artery bypass graft surgery. In a cohort of predominantly asymptomatic unilateral carotid disease patients, the 30-day risk of death/any stroke was 9.1% (120). Data from randomized controlled trials suggest that carotid artery stenting and carotid endarterectomy are similar when it comes to long-term benefits, but perioperative stroke risk and death rate are higher with carotid endarterectomy (01).
Additionally, carotid revascularization by endarterectomy or stenting with embolic protection before or concurrent with myocardial revascularization surgery is reasonable in symptomatic patients with stenosis of more than 80%. However, the safety and efficacy of carotid revascularization in patients with asymptomatic carotid stenosis, even if severe, are not well established (20).
General management of cardiac transplanted patients. Usually, opportunistic CNS infections occur 3 weeks after surgery. Post-transplantation lymphoproliferative disorder may be confined to the nervous system or disseminated. The response to treatment is poor (133).
Some antiepileptic drugs may reduce immunosuppressant levels in post-transplantation patients (30). Newer agents are not subject to this interaction.
Out of 100 patients who underwent heart valve procedures, 24 had focal deficits, of which 92% recovered completely at 5 months (158). Vocal cord dysfunction due to direct trauma or recurrent laryngeal nerve injury can lead to partial laryngeal obstruction and may require reintubation (153).
Cognitive decline after cardiac surgery may affect 7% to 49% of patients at 3 months and up to 33% after 1 year (179). Of concern was also the late decline of cognitive function after the cardiac procedures. However, this is most likely related to the progression of preexisting vascular disease, another neurodegenerative disease, or new neurologic events (111).
Analysis of the Veterans’ Affairs Quality Improvement Program database, including 1422 patients, found that the median survival time of patients with stroke after coronary artery bypass graft was 6.7 years. The mortality of patients with stroke compared to those without a stroke within the first 30 days postoperatively was 79% versus 96%, 58 versus 83%, and 36% versus 63% at 1, 5, and 10 years, respectively. Predictors of 1-year mortality were renal failure, prolonged ventilation, coma, and reoperation for bleeding (181).
The Prevention of Delirium and Complications Associated with Surgical Treatments (PODCAST), an international, multicenter, randomized, controlled trial, is ongoing to study the effects of a subanesthetic dose of intraoperative ketamine on postoperative delirium and other neurologic and psychiatric outcomes in cardiac and noncardiac surgeries. Smaller randomized controlled trials have shown a significant reduction in postoperative delirium from 31% to 3%; beneficial effects have been attributed to ketamine’s antiinflammatory and anti-excitotoxic actions (06).
Studies have shown the correlation between low cortical oxygen saturation and cognitive dysfunction, prolonged hospitalization, and perioperative cerebrovascular accidents in patients undergoing cardiopulmonary bypass. A randomized trial has demonstrated higher intraoperative cortical oxygen saturation during anesthesia with sevoflurane compared to total intravenous anesthesia with midazolam and fentanyl during cardiopulmonary bypass (66).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Elizabeth Anderson MD
Dr. Anderson of NYC Health and Hospitals/Kings County has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026