Sleep Disorders
Sudden infant death syndrome
Jul. 05, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Cerebral sinovenous thrombosis is often unrecognized in neonates and children due to nonspecific clinical features and challenges in radiographic diagnosis. Risk factors for cerebral sinovenous thrombosis in neonates are different from those in older children. Treatment with anticoagulants, a well-established practice in adults, is offered in children and, to some extent, in neonates. The safety of anticoagulants and recanalization outcomes in cerebral sinovenous thrombosis has been established in children as well as in carefully selected neonates based on consecutive cohort studies; however, its benefit on neurologic outcome, particularly in neonates, has not been proven. The clinical outcome from cerebral sinovenous thrombosis remains worse in neonates than in children.
|
• The clinical and radiographic diagnosis of cerebral sinovenous thrombosis is challenging in neonates and children. | |
|
• Cerebral sinovenous thrombosis should be considered in any child with unexplained seizures or encephalopathy. | |
|
• Anticoagulant therapy is safe in the absence of significant intracranial hemorrhage in neonates and children. It is probably safe in the presence of intracranial hemorrhage as well, at least in older children. | |
|
• Anticoagulant therapy prevents worsening of thrombosis in both neonates and children. | |
|
• Clinical outcomes are poor in most neonates with cerebral sinovenous thrombosis. |
Early literature on cerebral sinovenous thrombosis is mainly based on autopsy studies by French physicians. In 1873, Parrot recognized sagittal sinus thrombosis in neonates. In 1884, Bouchut observed cerebral sinovenous thrombosis in infants who had seizures during febrile or debilitating illnesses. The same year, Rilliet and Barthez reported infection as a predisposing factor in young children. Lhermitte described the association of cerebral sinovenous thrombosis with congenital heart disease. Several years later, Symonds described “otitic hydrocephalus” referring to hydrocephalus and raised intracranial pressure in children with chronic otitis media and mastoiditis (83). This probably represents the first description of childhood cerebral sinovenous thrombosis in modern English literature. Because the condition was considered infrequent and difficult to diagnose, systematic literature was rare before the advent of modern neuroimaging techniques.
The clinical features of cerebral sinovenous thrombosis can be subtle and diffuse. They are dependent on the child’s age, extent, and location of thrombosis, along with presence/absence of associated venous infarction. In young children, coexisting neurologic diseases produce neurologic signs that overshadow or are impossible to differentiate from those of cerebral sinovenous thrombosis. Seizures and encephalopathy of varying degrees remain the major presenting feature in both neonates (72% and 60%, respectively) and children (50% and 25%, respectively) (19; 72; 59; 56; 36). A 15-year retrospective study on pediatric cerebral venous sinus thrombosis revealed that the most common presentation was diffuse neurologic symptoms, such as headaches and vomiting, occurring in 77.7% of cases (04). Seizures were noted in 22.2% of patients. All patients had at least one identifiable risk factor, with chronic systemic conditions (63%) and infections (44%) being the most prevalent.
Raised intracranial pressure develops gradually over hours, days, and sometimes weeks. In neonates and infants, a tense anterior fontanelle, separation of skull sutures, and dilated scalp veins may be seen. Focal neurologic deficits are rare in neonates (19; 59). In older infants and children, signs of raised intracranial pressure-like headache and papilledema with false localizing sixth cranial nerve palsy predominate with associated varying levels of altered consciousness. Seizures are present in about 50% of children (19) and are more frequently reported in patients with thrombosis of cortical veins (68). Headache and papilledema secondary to cerebral sinovenous thrombosis usually cannot be differentiated from that due to idiopathic intracranial hypertension. Visual disturbances are reported in about 20% of children and consist chiefly of diplopia due to false localizing sixth nerve palsy and visual field abnormalities.
A systematic review analyzed 75 reported cases of deep medullary vein thrombosis in neonates, encompassing both preterm and full-term infants (64). Clinical presentations frequently included seizures (48%), apnea (36%), and lethargy or irritability (35%), with 45% of cases requiring respiratory resuscitation or inotropic support.
The main complications of cerebral sinovenous thrombosis in children are intracranial hemorrhage and raised intracranial pressure that influence short-term mortality and long-term morbidity. A major difficulty in studying predictors of recanalization or long-term clinical outcomes is the influence of coexisting neurologic conditions that are present in a large number of children, especially neonates, with cerebral sinovenous thrombosis. Mortality in children is comparable to adults with cerebral sinovenous thrombosis ranging from 10% to 20%. Children in general tend to do better than neonates (56). The frequency of adverse neurologic outcomes in older children ranges from 10% to 20% (32; 56) whereas in neonates it ranges from 40% to 80% (28; 05; 56; 55; 41). Epilepsy is reported in 10% to 25% in survivors (56; 53). The range of neurologic abnormalities includes deficits in sensorimotor, language, and cognitive and behavioral domains. Recanalization rates and outcomes in neonates and children have now been documented (56). Neonates recanalize their thrombus faster (by 3 months) than older children (by 6 months). The findings in older children are similar to adults (06). The influence of recanalization on clinical outcome is less clear in all age groups, because in adults the data are conflicting (82; 81), and in the pediatric age group, neonates who recanalize earlier and more completely than older children still have a worse clinical outcome (56). We speculate that perhaps it is the rate of recanalization rather than the final outcome of recanalization that might matter. Recurrence of cerebral sinovenous thrombosis has not been reported in neonates and appears to be rare. In older children, recurrence rates, mainly determined by the presence of a prothrombotic state, range from 10% to 15% (39).
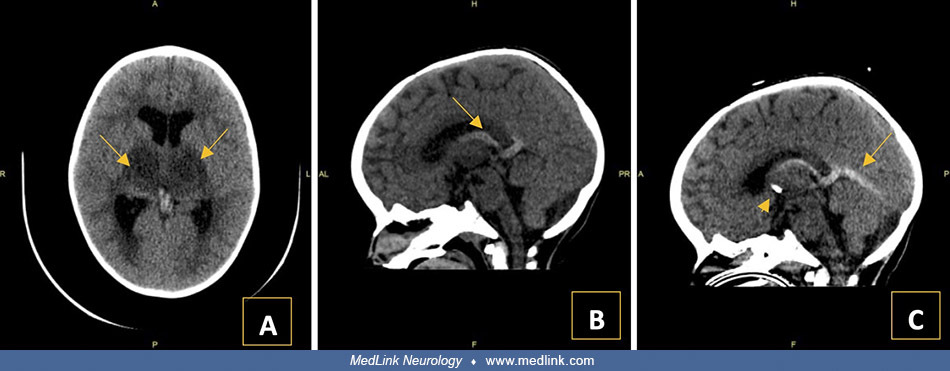
A 2.5-year-old girl with a history of severe iron deficiency anemia attributed to severe egg allergies and dietary habits was admitted to the pediatric intensive care unit (PICU) with symptoms indicative of an upper respiratory tract infection, irritability, and alarming stiffening movements. Initial imaging included CT, and CT venography revealed extensive cerebral sinovenous thrombosis in the bilateral internal cerebral veins, vein of Galen, and straight sinus, sparing the torcula. This was associated with acute hydrocephalus and secondary infarction in the bilateral thalami. Consequently, bilateral external ventricular drains were placed to manage the hydrocephalus.
Following her bilateral external ventricular drain insertion, unfractionated heparin was initiated as treatment for her cerebral sinovenous thrombosis.
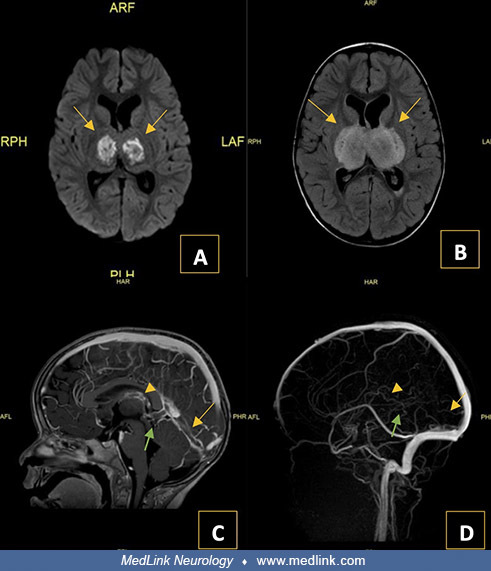
Throughout her 6-day PICU stay, she experienced fluctuations in her level of consciousness and irritability, which was managed with intubation and a regimen of sedatives, transitioning to maintenance therapy involving clonidine and diazepam. Continuous EEG monitoring for 3 days revealed no seizure activity. An MRI and MRV performed initially and subsequently showed stable thrombosis with no new infarction or clot propagation.
The underlying cause, microcytic anemia due to her vegetarian diet and excessive milk intake, was addressed with iron supplementation following confirmation of critically low hemoglobin levels.
Following stabilization, she was transferred to the neurology ward, and her treatment shifted from heparin to enoxaparin (low molecular weight heparin), with careful monitoring due to the risks posed by her external ventricular drains. Throughout this period, her neurologic examinations showed modest improvements in alertness and responsiveness, though her motor functions remained significantly compromised.
This case highlights the complexity of managing pediatric cerebral sinovenous thrombosis with significant neurologic implications. It underscores the importance of a multidisciplinary approach in handling both the immediate complications and the long-term management of cerebral sinovenous thrombosis, involving vigilant monitoring and adjustments in therapeutic strategies based on dynamic imaging results and clinical assessments.
Cerebral sinovenous thrombosis results from a combination of intravascular and extravascular risk factors. Prothrombotic states may predispose directly to thrombosis whereas acute and chronic illnesses or prothrombotic medications act as triggers. Idiopathic cerebral sinovenous thrombosis is reported in less than 10% to 15% of children (56). Neonates are vulnerable to cerebral sinovenous thrombosis due to many physiological risk factors. These are pregnancy- and perinatal period-related maternal hypercoagulable state (03), molding of skull bones during labor causing mechanical damage to underlying dural sinuses, a relatively high hematocrit, venous flow that is dependent on head positioning (16), and lower than normal levels of fibrinolytic factors like protein C, protein S, and antithrombin III (02). Physiological compression of the superior sagittal sinus by the occipital bone in supine position has been implicated as a potential mechanism for cerebral sinovenous thrombosis in neonates (84). Prenatal or perinatal disorders have been reported in approximately 51% of neonates with cerebral sinovenous thrombosis. These include maternal infections, gestational diabetes, premature rupture of membranes, abruptio placentae, and birth asphyxia (93). Preterm birth and complicated delivery are also risk factors for cerebral sinovenous thrombosis. Hypoxia in the preterm is an independent risk factor associated with neonatal cerebral sinovenous thrombosis (79). Other acquired insults include dehydration, bacterial sepsis, and meningitis. Hypernatremic dehydration in exclusively breastfed neonates has been associated with neonatal cerebral sinovenous thrombosis (78). A 27% (10 out of 37) incidence of cerebral sinovenous thrombosis secondary to post therapeutic hypothermia for asphyxia has been shown (65). Post cardiac surgery, there was found to be a 28% (11 out of 40) incidence of neonatal cerebral sinovenous thrombosis (15). Associated risk factors included younger age, lower weight, and the use of central venous catheter. Prothrombotic abnormalities have been reported in 15% to 20% of neonates with cerebral sinovenous thrombosis (09). Risk factors of deep medullary vein thrombosis in neonates were found to be similar to other types of neonatal cerebral sinovenous thrombosis, including complicated deliveries (38%), prematurity (40%), congenital heart disease (48%), and neonatal infections (40%). Seizures were the most common presenting symptom, occurring in 52% of cases. Hemorrhagic infarction was significantly more frequent in isolated deep medullary vein thrombosis (77%) compared to cerebral sinovenous thrombosis without deep medullary vein thrombosis (p = 0.013) (14). In older infants, iron deficiency anemia is occasionally associated with cerebral sinovenous thrombosis (72). Head and neck infections, especially otitis media and mastoiditis, resulting in septic cerebral sinovenous thrombosis are present in 25% of older infants and children (19; 36). In older children, head trauma or cranial surgery can mechanically damage dural sinuses and cause cerebral sinovenous thrombosis (69; 95). Chronic systemic diseases that result in an acquired prothrombotic state are present in about 60%. These include systemic lupus erythematosus, nephrotic syndrome, inflammatory bowel disease, hematologic disorders, cardiac disease, and others (19; 67). Acute illnesses with accompanying element of dehydration are present in nearly one third of children with cerebral sinovenous thrombosis. Acquired and congenital prothrombotic abnormalities put together have been reported in 33% to 96% of children with cerebral sinovenous thrombosis (09). Congenital prothrombotic disorders include factor V Leiden; prothrombin gene G20210A; dysfibrinogenemia; deficiencies of protein C, protein S, and antithrombin III; factor VIII, factor IX, and factor XI excess; factor XII deficiency; and thrombomodulin mutation (18; 09; 45). Acquired prothrombotic states include anticardiolipin antibody; lupus anticoagulant; acquired activated protein C resistance; acquired deficiencies of protein C, protein S, and antithrombin III; and hyperhomocystinemia. Although patients with COVID-19 are hypercoagulable, there is no evidence at present to demonstrate an association between the SARS-CoV-2 virus and cerebral venous sinus thrombosis in children (01; 08). The Johnson & Johnson COVID-19 vaccine (Ad26.COV2.S) has been linked to rare cases of venous thrombosis, particularly cerebral sinovenous thrombosis with thrombocytopenia syndrome (73). A JAMA case series reported 12 cerebral sinovenous thrombosis cases during March and April 2021, and another study in the Annals of Internal Medicine noted 57 thrombocytopenia syndrome cases primarily linked to this vaccine, an estimated rate of 3.83 per million doses. In response, the CDC and FDA temporarily paused its use in April 2021, later resuming it with a warning about the low but serious risk, especially in women of childbearing age (74). Notably, no pediatric cases were reported.
Genetic causes of cerebral sinovenous thrombosis include a novel mutation in Serpin C1 gene, which presents as unprovoked neonatal cerebral sinovenous thrombosis. This mutation causes a type 1 antithrombin (AT) deficiency and presents within the first week of life. Mutations in the A1 gene (Serpin C1) are associated with an 18-fold increase risk of cerebral sinovenous thrombosis (45).
JAK2 (Janus Kinase 2) V617F mutation causes cerebral sinovenous thrombosis without an underlying hematological abnormality diagnostic for myeloproliferative neoplasms (29).
El-Khoury and colleagues have reported that children undergoing therapy for acute lymphoblastic leukemia (ALL) had 10.5% incidence of cerebral sinovenous thrombosis if the following are present: intermediate/high risk disease, triglyceride levels greater than 615 mg/dl, mediastinal mass, and larger body surface (24).
Cerebral sinovenous thrombosis due to gain of function pathogenic variants in PIK3CA associated with megalencephaly-capillary malformation-polymicrogyria (MCAP) syndrome has been reported (30).
Re-exposure to prothrombotic agents, such as asparaginase, has been shown to be generally safe when managed with appropriate anticoagulation (76). Evidence suggests a low recurrence rate of cerebral sinovenous thrombosis and no significant long-term neurologic sequelae. At a median follow-up of 4.5 years, 61% of patients had normal neurologic status, and 57% achieved complete recanalization, with no significant differences observed between those re-exposed to asparaginase and those who were not.
The brain’s venous drainage consists of a network of dural sinuses, cerebral veins, and cortical veins, which are divided into the superficial and deep systems. The superficial venous system consists of cortical veins and the superior sagittal sinus that drains into the torcular and then predominantly into right transverse (lateral) sinus, and right internal jugular vein. The deep system consists of inferior sagittal sinus, basal vein of Rosenthal, and paired internal cerebral veins that empty into the vein of Galen and then the straight sinus, which finally drains into the torcular. The deep system drains predominantly into the smaller-caliber left transverse (lateral) sinus and left internal jugular vein. Anteriorly, the paired cavernous sinuses are connected to the jugular system by the petrosal sinuses.
The cerebral venous system is a valveless system functioning at a low pressure and slow velocity. The venous sinuses encased in the rigid dura are non-collapsible. This results in a passive drainage of blood flow from the brain to the heart (13). The flow in the sinuses is gravity- and respiration-dependent and can be bi-directional depending on the venous pressure gradient. Reduction in systemic blood pressure can result in stasis or reversal of blood flow within dural sinuses. A relative reduction of thrombomodulin in the lining of cerebral sinuses further increases the propensity to thrombus formation (49). Dural sinuses play an important role in cerebrospinal fluid (CSF) dynamics due to the presence of arachnoid granulations.
In cerebral sinovenous thrombosis, the mechanism for venous infarction is obstruction of venous drainage with increasing venous pressure in the region of brain drained by that vein or venous sinus, in the absence of venous collaterals. Venous congestion results in extravasation of fluid into the brain, producing focal or diffuse cerebral edema and hemorrhage due to diapedesis of red blood cells through capillaries. The edema may be transient if venous flow is re-established, or it may be associated with permanent tissue infarction if the increased venous blood pressure exceeds the arterial perfusion pressure. In the latter situation, there is inadequate delivery of arterial blood and regional ischemic “venous” infarction results (10; 51). Once the initial thrombus has formed, the ensuing obstruction and venous stasis can promote propagation of the initial thrombus. Relief of obstruction, even if delayed, can ease the venous congestion in cerebral sinovenous thrombosis completely. Occlusion of superior sagittal sinus or dominant transverse sinus impairs the function of arachnoid granulations, which interferes with CSF absorption and increases venous congestion and may result in communicating hydrocephalus (51). If the raised intracranial pressure is severe, pressure on the optic nerves causes papilledema, which if unrelieved over time can progress to optic atrophy and visual impairment.
Emerging evidence underscores the pivotal role of inflammation in the pathophysiology of severe cerebral sinovenous thrombosis. Hu and colleagues shed light on the contribution of neuroinflammatory processes—particularly involving microglia, astrocytes, and neutrophils—in driving complications, such as disruption of the blood-brain barrier, cerebral edema, and venous infarction (35). These cellular interactions appear to play a central role in shaping both the progression and clinical severity of cerebral sinovenous thrombosis. Complementing this, Zhou and colleagues offered a contemporary reinterpretation of the Virchow triad, focusing on the effects of cerebral venous congestion at the molecular level (96). Their findings, derived from an animal model, revealed that venous congestion triggers endothelial damage, promoting a prothrombotic environment through activation of platelets, the complement system, and coagulation pathways. This work emphasizes the mechanistic link between endothelial injury and thrombosis risk in the context of cerebral venous disorders.
The incidence of childhood cerebral sinovenous thrombosis has been estimated at 0.67 per 100,000 children per year (19). Neonates comprised nearly 50% of that study. Subsequent data suggest much higher frequency in neonates at 2.6 to 12 per 100,000 term neonates per year (34; 05). Still, these figures are underestimates, as the incidence is probably increasing due to better awareness, improved neuroimaging, and increased numbers of children at risk for cerebral sinovenous thrombosis, resulting from increased survival in predisposing disorders like prematurity, leukemia, and congenital heart disease. Cerebral sinovenous thrombosis might also occur during fetal life, although this possibility is seldom considered, and the available literature is extremely scarce in this regard (46; 48; 62). The frequency of preterm cerebral sinovenous thrombosis is unknown. A German study has shown that although the incidence of both term and preterm cerebral sinovenous thrombosis is 6.6 per 100,000, 10% to 27% of those were preterm. Asymptomatic preterm infants had 4.4% incidence (66; 80).
In neonates, cerebral sinovenous thrombosis may be overlooked as the cause of seizures or obtundation, particularly in the context of hypoxic-ischemic encephalopathy, metabolic acidosis, or sepsis. Poor feeding, irritability, and hyper- or hypotonia are also symptoms and signs to consider in the neonatal presentation of cerebral sinovenous thrombosis (19; 80). Cerebral sinovenous thrombosis, like intracranial hemorrhage, should be considered as a cause of neurologic deterioration in sick patients. Cerebral sinovenous thrombosis should be distinguished from arterial ischemic stroke, post-asphyxial parasagittal injury, and contusion following trauma (44). In older children, early or mild cases of cerebral sinovenous thrombosis may be difficult to distinguish from idiopathic intracranial hypertension or other causes of raised intracranial pressure. Clinical diagnosis may be difficult in the context of infections that may themselves precipitate thrombosis. A high suspicion of cerebral sinovenous thrombosis should be maintained in a child or neonate with (1) unexplained seizures or encephalopathy and (2) new onset/worsening of preexisting seizures or encephalopathy in the presence of coexisting neurologic or systemic disorders. Furthermore, when assessing a suspected intravenous filling defect on neuroimaging, the clinician must consider a differential diagnosis in mind including, most commonly, (1) asymmetry of the transverse sinuses; (2) extraaxial fluid collections; and (3) arachnoid granulations (11; 43; 42). The appearance of the thrombus at various ages and on different MRI pulse sequences is helpful in differentiating a thrombus from these mimics and preventing unnecessary treatment.
Investigations performed in cerebral sinovenous thrombosis should be aimed at (1) confirmation of the diagnosis and delineating the extent of brain injury, (2) screening for prothrombotic disorders, and (3) correctly identifying associated risk factors.
The diagnosis of cerebral sinovenous thrombosis is not possible only clinically. Neuroimaging with dedicated sequences of the intracranial venous system is mandatory. Knowledge of the normal variations in the venous anatomy as well as advantages and limitations of available imaging techniques is important (25; 75; 91). Computed tomography (CT) is frequently performed in most children due to ease of availability, short procedure time, and capacity to detect acute hemorrhage. Plain or unenhanced CT can miss cerebral sinovenous thrombosis; hence, contrast study is essential. CT can also yield false positive results in neonates. Signs indicative of cerebral sinovenous thrombosis on a non-contrast CT are the ‘‘filled triangle’’ or ‘‘dense triangle’’ sign or the ‘‘cord sign,’’ which describe the increased density of an intraluminal thrombus in sinovenous channels. On contrast-enhanced CT, ‘‘empty triangle’’ or ‘‘empty delta’’ sign refers to a non-contrast enhancing thrombus surrounded by the dural walls of the sinus, which enhance with contrast. CT venography using a multi-slice technique has been reported to be better than routine CT and a good substitute for MRI and MR venography in adults (61). However, the radiation risk needs to be duly considered in the pediatric age group. MRI is the preferred modality in most instances because of its ability to demonstrate flow, thrombus, edema, infarction, and concurrent abnormalities. On conventional MR images, acute thrombus (1-3 days) within a cerebral vein or dural sinus is isointense on T1-weighted images and hypointense on T2-weighted images. In the subacute stage (7-14 days), thrombus is hyperintense on T1-weighted images as well as T2-weighted images. In addition to conventional MRI, dedicated MR venography is essential to document flow disturbance in the affected sinovenous channel. Several techniques such as time-of-flight, phase contrast, and contrast-enhanced MR venography are helpful. Sensitivity and lack of radiation are major advantages of MRI over CT, but the need for sedation and the availability of urgent/emergent time are the main limitations. There is limited experience with diffusion-weighted imaging in neonates and children with cerebral sinovenous thrombosis as opposed to that with adults (21). Diffusion-weighted imaging, in addition to shedding light on mechanisms of brain injury in cerebral sinovenous thrombosis, has been reported to be useful in predicting recanalization in adults (26) and perhaps might be useful in children, although there are conflicting data for the pediatric population (54; 87). There is limited experience with imaging modalities other than CT and MRI. Cranial ultrasound is helpful for diagnosing centrally located venous infarcts or hemorrhages in infants with an open fontanelle. The technique, however, is highly operator-dependent; hence, diagnosis is tricky based on ultrasound alone. Its major advantage is the bedside availability and noninvasive nature. Doppler ultrasound can define absent/reduced flow in the sinovenous channels in cerebral sinovenous thrombosis, but mainly in the superior sagittal sinus (52; 66). Catheter cerebral angiography is rarely required nowadays for cerebral sinovenous thrombosis diagnosis due to the advent of CT and MRI. Although MR may be preferred for its lack of radiation, CT venogram is at least equivalent in sensitivity for cerebral venous sinus thrombosis diagnosis. There continues to be variability in employment of imaging modalities for pediatric cerebral venous sinus thrombosis. Importance of standardization of imaging pathways for pediatric cerebral venous sinus thrombosis have been reviewed (47). Adopting specific imaging protocols for cerebral venous sinus thrombosis aids in diagnostic precision and targeting management, which impacts outcome.
In both neonates and children, multiple sites are often involved in cerebral sinovenous thrombosis. The superficial system, including the superior sagittal and transverse sinuses, is involved in the majority. In severe cases, both superficial and deep systems may be thrombosed. Between 50% and 90% of neonates and children with cerebral sinovenous thrombosis have venous infarcts (59; 32; 56). In neonates, over three-quarters of infarcts are hemorrhagic (05), whereas in older infants and children a third are hemorrhagic (56). With thrombosis of the superficial system, infarcts are located in the cortex and white matter and may be bilateral (85). With thrombosis of the deep system, the infarcts are usually located in one or both thalami or the cerebellum (85; 05). In term newborns with intraventricular or thalamic hemorrhage, cerebral sinovenous thrombosis involving the deep system may be the underlying cause and should be sought (94). There probably are differences in the pattern of brain injury due to cerebral sinovenous thrombosis between term and preterm newborns (40). Isolated cortical venous thrombosis in absence of dural sinus involvement is also possible (68). In a systemic review by Pin and colleagues describing imaging regarding deep medullary vein thrombosis, MRI consistently revealed fan-shaped linear T2 hypointense lesions, predominantly affecting the frontal (84%) and parietal (76%) lobes, with hemorrhagic infarctions observed in 98% of cases (64).
Testing for prothrombotic risk factors typically includes activated partial thromboplastin time, INR, antithrombin III, protein C and protein S levels, plasma fibrinogen, anticardiolipin antibodies, lupus anticoagulant, Factor V Leiden mutation, MTHFR mutation, prothrombin gene (G20210A) mutation, plasminogen, lipoprotein-a, Factor VIII, and plasma homocysteine. The results of these should be interpreted based on local laboratory standards, and age should be taken into consideration when interpreting values. The presence of prothrombotic abnormalities varies widely across studies (09; 93), and whether they are true causal associations with cerebral sinovenous thrombosis is not clear, as many seem to be transient and most are negative on repeat testing (56).
Lastly, a thorough screening for risk factors is helpful to determine the condition predisposing to cerebral sinovenous thrombosis, based on the individual case scenario. This may include but is not limited to investigations like blood counts, electrolytes, inflammatory work-up, iron studies, CSF, and microbial cultures, as per the clinical indication.
The mainstays of management of childhood cerebral sinovenous thrombosis are (1) targeting the risk factor, (2) neuroprotection, and (3) careful consideration for antithrombotic therapy.
Removal and/or avoidance and/or treatment of the associated risk factor are important, as alleviation of the underlying “hypercoagulable state” predisposing to thrombosis is critical. Prompt attention to perinatal risk factors, intracranial infections, and hematological/heart/liver/kidney disease is suggested. Dehydration and iron deficiency anemia are important targets. Neuroprotective measures are aimed at preventing and limiting the extent of venous infarction and brain injury. Maintenance of temperature, blood pressure, glucose, blood volume, and treatment of seizures and raised intracranial pressure are essential. The role of prophylactic anticonvulsants is controversial, but a low threshold for EEG is helpful. Seizures can increase infarct volume and resultant brain injury. The role of anti-edema measures is relatively better defined in adults than in children. Mannitol and acetazolamide can be considered on an individual case basis, although it is important to remember that both induce diuresis, which can cause volume depletion that in turn could theoretically worsen thrombosis. Positive pressure ventilation and decompressive craniectomy are other therapies for life-threatening raised intracranial pressure, although these should be considered on the merit of individual situations.
Specific antithrombotic therapy includes anticoagulant therapy, antiplatelet therapy, and thrombolytic therapy. In childhood cerebral sinovenous thrombosis, unfractionated heparin, low-molecular-weight heparin, and vitamin K antagonists (warfarin) are the main anticoagulants. The rationale of anticoagulant therapy is to prevent propagation and thereby enable the unopposed dissolution (recanalization) of the existing thrombus, by the fibrinolytic system. Safety of anticoagulant therapy has been established in adults even in the presence of intracranial hemorrhage and is the standard practice (22; 17; 23; 70). Older children are increasingly treated based on adult data, but many neonates are still not treated (37; 36). Data have confirmed the safety of anticoagulant therapy with low hemorrhagic complication (non-fatal) rate (5%) in cerebral sinovenous thrombosis (05; 56) in both neonates and older children. It has also been shown that in the absence of anticoagulant therapy, worsening/propagation of thrombosis occurs in over one third of neonates and children (56; 55; 63). Propagation can be accompanied by new venous infarction in 10% to 40% of cases (56; 55). Thus, there could be some risk in not giving anticoagulant therapy to neonates and children with cerebral sinovenous thrombosis. However, the effect of anticoagulant therapy on the long-term clinical outcome, particularly neonates, who generally tend to have worse outcomes, is not yet known.
The 2024 American Heart Association guidelines for the diagnosis and management of cerebral venous thrombosis in pediatric patients provide updated recommendations that closely align with previous guidelines from the American College of Chest Physicians (ACCP) and the American Heart Association (71). For older children with cerebral sinovenous thrombosis without significant intracranial hemorrhage, the American Heart Association continues to recommend anticoagulation therapy, typically with low molecular weight heparin or standard heparin, as a class IIa recommendation with level of evidence C. This is consistent with the ACCP's grade 1B recommendation. For cases in which significant intracranial hemorrhage is present, the American Heart Association suggests a more cautious approach. Anticoagulation may be initiated or deferred with close radiographic monitoring at 5 to 7 days, and anticoagulation should be considered if there is evidence of thrombus propagation on serial imaging. This mirrors the ACCP's grade 2C recommendation. For neonates, the American Heart Association guidelines also recommend considering anticoagulation with low molecular weight heparin or standard heparin, especially if there is clinical deterioration or evidence of thrombus extension on serial imaging. Serial imaging at 5 to 7 days is advised to exclude propagation if anticoagulation is not initially pursued. This is in line with the ACCP's grade 2C recommendation for anticoagulation in the absence of significant hemorrhage and the option of supportive care with serial imaging if hemorrhage is present. Overall, the 2024 American Heart Association guidelines reaffirm the importance of individualized treatment plans based on the presence of hemorrhage and the risk of thrombus propagation, maintaining a similar stance to the previous ACCP and American Heart Association guidelines.
Direct antithrombin inhibitors such as bivalirudin have been anecdotally used in specific cases of apparent heparin resistance but no large cohort study has been performed to assess efficacy and safety (07). Data on direct oral anticoagulants are emerging in pediatric venous thromboembolism with a potential for future clinical trials in pediatric cerebral sinovenous thrombosis (12; 50). The Kids-DOTT Multinational Trial has studied 417 patients over a period of 13 years from 2008 to 2021 and suggests that a 6-week course was non-inferior to a 3-month course in terms of recurrence and bleeding events (92). The trial utilized dalteparin, a low molecular weight heparin, as anticoagulant therapy. It supports the use of a 6-week anticoagulation therapy regimen as a viable option for treating provoked acute cerebral sinovenous thrombosis in patients under 21 years old, with outcomes comparable to a 3-month regimen. The EINSTEIN Junior and DIVERSITY trials offer key evidence supporting the use of newer oral anticoagulants in children with venous thromboembolism. The EINSTEIN Junior Trial evaluated bodyweight-adjusted rivaroxaban in 335 children (0–17 years) with venous thromboembolism. The children were treated using bodyweight-adjusted doses of rivaroxaban. Drug levels were tested and were found to be similar to those seen in adults, and there was no pattern of increased bleeding or other adverse events, supporting the treatment’s safety and effectiveness (57). The DIVERSITY trial, a randomized open-label trial, compared dabigatran to standard anticoagulation in 267 children (33). Dabigatran was non-inferior in efficacy, with comparable rates of thrombus resolution, recurrent venous thromboembolism, and bleeding events. On the other hand, the S2k guideline on cerebral venous and dural sinus thrombosis, an adult-focused study, recommends low molecular weight heparin as the optimal initial anticoagulant over oral anticoagulants as the primary treatment choice (89). Following the acute phase, they recommend transitioning to oral anticoagulation with direct oral anticoagulants for 3 to 12 months to enhance recanalization and prevent recurrent cerebral sinovenous thrombosis. This approach aligns with the consensus that low molecular weight heparin is initially preferred due to its efficacy and safety profile in the acute management of cerebral sinovenous thrombosis.
Other therapies such as antiplatelet agents like aspirin do not seem to have a role in cerebral sinovenous thrombosis, as the coagulation system rather than platelets is the chief player in the thrombotic process, although aspirin has on rare occasions been administered in some patients when anticoagulant therapy has failed to halt the propagation of cerebral sinovenous thrombosis (authors’ personal communication). There are no clinical trials to inform the role of thrombocytic agents such as tissue plasminogen activator, urokinase, streptokinase, or mechanical thrombectomy, other than small case series (88; 60). In general, these should be perhaps reserved only for very aggressive cerebral sinovenous thrombosis that worsens despite adequate anticoagulant therapy. The safety in children is not clear; therefore, outside of clinical trials, use of these agents is not recommended. The ACCP recommends that thrombolysis, thrombectomy, or surgical decompression be performed only in children with severe cerebral sinovenous thrombosis in whom there is no improvement with initial unfractionated heparin therapy (grade 2C).
Endovascular techniques such as venous mechanical thrombectomy for treating refractory cerebral sinovenous thrombosis may be considered in carefully selected cases. Centers with experienced neurointerventionalists with neurovascular multidisciplinary team set up is key to implementing this practice. Evidence of clinical or radiographic progression despite anticoagulation may be candidates for venous thrombectomy. Mortimer and colleagues present a series of nine children in poor clinical condition who underwent endovascular therapies (58). Several methods were used including local tPA, microguidewire and catheter disruption, balloon angioplasty, and thromboaspiration using the Penumbra device. Eight children had good functional outcomes. A small case series of seven children described using mechanical thrombectomy for children in whom neurologic deterioration occurred despite optimal anticoagulation therapy—six out of seven had venous infarct preoperatively. In three out of seven children, intrasinus thrombolytic therapy (tPA) was used (31). Six out of seven children had favorable outcome with mRS 0 or one 90 days post procedure. Catheter directed thrombolytic (CDT) therapy has also been used as adjunctive therapy to venous thrombectomy. Torres and colleagues described a case series of five children where CDT therapy was used for 17 to 48 hours at a dose of 1 to 2 mg/hr. Unfractionated heparin was continued during this time (86). All children had partial resolution of clot burden, and one child had rapid reocclusion. Important complications of CDT that may occur and important during decision making include post-procedure bleeding, parenchymal/intraventricular hemorrhage, and petechial brain hemorrhage.
The role of decompressive craniectomy for cerebral sinovenous thrombosis in children is lacking in the literature, although adult data are available. It is performed when clinical deterioration includes hemorrhagic venous infarct, raised intracranial pressure, and risk of imminent cerebral herniation as a life-saving procedure. Theoretically, decompression alleviates pressure on the sinuses due to edema from the brain and may help in restoring venous flow. This, however, requires pausing unfractionated heparin; consensus opinion on timing of recommencement of unfractionated heparin is not available, and variability in practice continues. Therapy with unfractionated heparin remains vital for ongoing management postoperatively. Published guidelines and recommendations for surgical and interventional management are lacking at present; future studies are required.
Neurologic deficits are often present at the time of discharge. Motor and cognitive sequelae may require long-term rehabilitation regimens (20). Some of the neurologic symptoms that children may suffer after cerebral venous sinus thrombosis include (but not restricted to) headache, visual impairment, and cranial nerve VI palsy secondary to intracranial pressure. Deficits that may be present due to venous infarction range from developmental delay, learning disabilities, hemiparesis, and hemisensory loss. Children who have been anticoagulated are more likely to have good cognitive outcome (72). Statistically significant association with death in those with a Glasgow coma score of less than 12. The neurologic sequelae is dependent on whether the cerebral venous sinus thrombosis results in parenchymal injury that either leads to venous infarct (cortical or subcortical), deep nuclei (basal ganglia and thalamus), or primary hemorrhage, resulting in intra or extra parenchymal injury with intraventricular hemorrhage, subdural, or subarachnoid hemorrhage.
Slim and colleagues studied the neurocognitive outcome following cerebral venous sinus thrombosis with a prospective observational study (77). Most children with cerebral venous sinus thrombosis exhibited emerging cognitive deficits. The domains tested included intellectual disability, executive function, attention, language, or behavior. Slim and colleagues looked at 50 children with a median age of 2 years 10 months, with a median follow-up time of 4 years (77). When compared with normative children, those who had suffered cerebral venous sinus thrombosis had a lower mean full-scale IQ, with lower working memory and processing speed scores. Executive function, attention, and language domains were also affected with lower scores. Interestingly, the verbal comprehension index did not differ. Spearing of verbal ability after cortical lesions was a consistent finding across multiple studies irrespective of the type of lesion, laterality, and age (90; 77). Children with cerebral venous sinus thrombosis demonstrated difficulty with verbal learning and memory. Children with behavioral problems were also those who had refractory seizures at presentation. Females are less likely than males to experience difficulties with processing speed.
It is important to note that this study showed that no differences in cognitive outcomes were associated with age at cerebral venous sinus thrombosis presentation (neonate vs. non-neonate), neurologic comorbidity, presence of seizure disorder, number of dural vessels involved (except for adaptive skills), and presence of parenchymal injury (infarct or hemorrhage). Neurologic deficits are reported in 17% to 46% of cases, with cognitive and behavioral deficits being more prevalent than motor deficits. Seizures and epilepsy are also notable long-term outcomes, with acute seizures at presentation being a predictor for the development of epilepsy. In neonates, long-term follow-up is crucial as deficits may only become evident with brain maturation over many years. Factors associated with worse outcomes include the presence of venous infarcts, seizures at presentation, and incomplete recanalization (38).
Mineyko and colleagues offer prospective data on seizure outcomes following pediatric cerebral sinovenous thrombosis (53). Among 24 children, 25% developed epilepsy by 1 year, whereas 37.5% experienced acute symptomatic seizures at diagnosis. Notably, half of those with epilepsy had no infarcts, hemorrhage, or seizures during the acute phase, underscoring that epilepsy may emerge even in the absence of early parenchymal injury. Despite this, 71% achieved favorable functional outcomes at 1 year, per the King's Outcome Scale and modified Rankin scores.
Despite a low mortality rate of 2.6% in cases of deep medullary vein thrombosis in neonates, a significant proportion of survivors experienced long-term neurologic sequelae, including intellectual disability (37%) and epilepsy (18%) (64).
The use of anticoagulation and association with neurologic outcomes has been reported (27). Treatment and outcomes in 410 children from the International Pediatric Stroke Study (IPSS) were studied using the Pediatric Stroke Outcome Measure (PSOM). Eighty two percent of children received anticoagulation; a multivariate analysis showed that anticoagulation was significantly associated with favorable outcomes and had a lower odds of severe neurologic impairment or death at hospital discharge. Further randomized control trials are, however, required to fully validate this.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Mahendranath D Moharir MD MSc FRACP
Dr. Moharir of the University of Toronto has no relevant financial relationships to disclose.
See ProfileYara Al-Salloum MD
Dr. Salloum of The Hospital for Sick Children has no relevant financial relationships to disclose.
See Profile
Bernard L Maria MD
Dr. Maria of Thomas Jefferson University has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 05, 2026
General Child Neurology
Jun. 24, 2026
General Child Neurology
Jun. 10, 2026
Epilepsy & Seizures
Jun. 02, 2026
General Neurology
May. 13, 2026
General Child Neurology
May. 12, 2026
Epilepsy & Seizures
May. 08, 2026
Stroke & Vascular Disorders
May. 03, 2026