




















































































































General Child Neurology
Congenital heart disease: neurologic complications
Jun. 24, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Congenital syphilis, one of the transplacentally acquired preventable infections, can produce long-lasting morbidities in neonates. In this article, the author describes the epidemiology of congenital syphilis in the United States and developing countries as well as the clinical spectrum of the disease. Also discussed are issues pertaining to the prevention and diagnosis of congenital syphilis in the United States, as well as globally, and the treatment of presumed and proven congenital syphilis.
Syphilis has been recognized as an infection since the beginning of the 16th century, when Ferdinand Columbus (Hernando Colon; 1488-1539), the second son of Christopher Columbus (1451-1506), described its skin manifestations among the sailors returning from the first voyage to the New World in 1493; it was termed mal de la Hispaniola. The disease spread to the Spanish soldiers who fought at the side of the King of Naples and was then renamed morbo Napolitano. The disease reached the French Troops of Charles VIII (1470-1498) during their 3-week siege of the city of Naples in 1495. When this army returned to the north, the Italian Peninsula was invaded by syphilis, and the disease became known as morbo Gallico or the “French malady.”
Girolamo Fracastoro (1478-1553) of Verona became famous for his poem “Syphilis sive Morbus Gallicus” (37), in which the main character, the shepherd Syphilus, is afflicted by this disease as punishment for cursing the Gods (Frascatoro 1530; 89). This poem not only baptized the French malady with its present name, but it also hinted at its venereal origin. From Spain, the disease spread throughout Europe, and there exists exact documentation of its appearance in Asia, India (1498), China (1505), and Japan (1569) (85).
Hieronymus Fracastorius (Girolamo Fracastoro) shows the shepherd Syphilus and the hunter Ilceus a statue of Venus to warn them against the danger of infection with syphilis. Engraving by Jan Sadeler I, 1588/1595, after Christop...
Congenital syphilis was first described in an English 17th-century pediatric textbook, although Paracelsus (Aureolus Theophrastus Bombastus von Hohenheim; 1493-1541) first suggested in utero transmission (89). As a result of this knowledge, newborns with syphilis were abandoned by their mothers because of fear of contagion. English surgeon and venereologist Sir Jonathan Hutchinson (1828-1913) described the triad of notched incisors, interstitial keratitis, and deafness as criteria for congenital syphilis diagnosis (52).
In 1905, at the Charite Clinic in Berlin, German zoologist Fritz Schaudinn (1871-1906), with the dermatologist Erich Hoffmann (1868-1959), identified the spirochete Spirochaeta pallida later called Treponema pallidum as the causative organism of syphilis (96; 86). Shortly afterward, in 1910, German physician-scientist Paul Ehrlich (1854-1915) introduced a synthetic arsenical, salvarsan, as the main line of therapy. Although toxic, it had more efficacy than previous medications, such as mercury salts and guaiac.
The natural history of untreated syphilis is well-known because of an epidemiologic study initiated in 1891 in Oslo, Norway by Norwegian dermatologist Carl Wilhelm Boeck (1808-1873/1875?). This study documented the course of the untreated disease in 1978 patients and included many autopsies.
The “Tuskegee Study of Untreated Syphilis in the Negro Male” was started in 1932 by the United States Public Health Service to study the natural history of syphilis in hopes of justifying treatment programs for Blacks (20). It was a notorious example of human research carried out without informed consent and with actions that were intentionally deleterious to the subjects studied.
The Tuskegee Syphilis Study is a notorious example of human research carried out without informed consent and with actions that were intentionally deleterious to the subjects studied. (Source: US National Archives. Atlanta, Geo...
Because of the protean manifestations in humans, syphilis has been called the “Great Mimicker” (82).
Syphilis is transmitted mainly during sexual activity by direct contact with the mucocutaneous lesions of the primary or secondary stages of the disease. Vertical transmission can occur transplacentally at any time during gestation because of maternal spirochetemia but can also occur through contact with a genital lesion at the time of delivery.
Transplacental transmission rates vary depending on the stage of maternal infection: they are nearly 100% during the secondary phase, 70% to 100% during the primary phase, and 30% during the latent phase. The risk of fetal infection increases as the stage of pregnancy advances (45). Fetal syphilis is only detected on prenatal ultrasound after 18 weeks, when the immunocompetent fetus can generate the immunologic response necessary to cause abnormalities on ultrasound (91).
Congenitally infected subjects can present with either early congenital syphilis or late congenital syphilis.
Early congenital syphilis. Clinical manifestations may begin in the first 24 months of life but are usually evident at birth or in the first few months. The longer the interval between maternal infection and pregnancy, the more benign the outcome in the infant (Kassowitz law) (34). Between 30% and 40% of infected fetuses are stillborn (16). Infants can present with intrauterine growth retardation, failure to thrive, fever, hepatosplenomegaly, ascites, jaundice, and generalized lymphadenopathy, particularly with the involvement of the epitrochlear nodes.
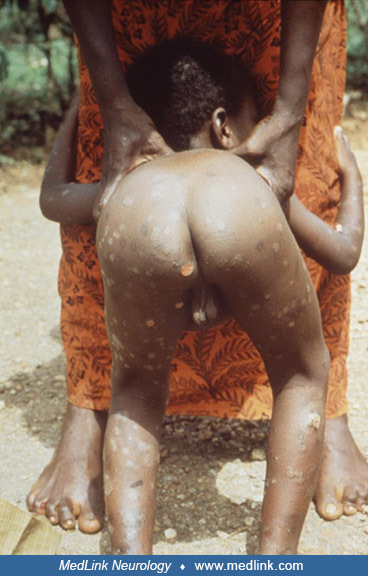
About half have mucocutaneous lesions with purulent or bloody rhinitis or “snuffles,” mucous patches and ulcers on the tongue, maculopapular or vesiculobullous rash often involving the palms and soles, and mucous patches and condyloma lata around the anus and external genitalia. Collectively, these can be called "syphilids," a term that includes any of the cutaneous and mucous membrane lesions characteristic of secondary and tertiary syphilis.
The 16-month-old girl’s mother had syphilitic sores on both nipples. Illustration by Surgeon Leonard Portal Mark (1855-1930), pathological artist at St. Bartholomew's Hospital, London. (Source: St. Bartholomew's Hospital Archiv...
Cutaneous manifestations may appear as erythematous macules (“roseola syphilitica”), erythematous to hyperpigmented oval or circular papules and plaques covered with scales, or a maculopapular eruption.
This female infant was born with congenital syphilis because while pregnant, her mother had been infected with the spirochete microorganism, Treponema pallidum. Note the papular rash on her chin and lips and the darkly pigmente...
This male infant was born with a condition known as congenital syphilis because his mother had been infected with the spirochete microorganism, Treponema pallidum, while pregnant and transferred the infection to her child by wa...
This photograph depicts a lateral view of a 7-months pregnant woman’s torso. Note the maculopapular eruptions on her abdomen, which were determined to be due to a secondary syphilis infection caused by the bacterial spirochete,...
Watercolor drawing of 6-week-old child. Both legs exhibit raised red areas of a ham-colored eruption, scaly in places. The feet are raw and red. Drawing presented to the Museum by Wilmot Parker Herringham, physician to St Barth...
Some patients have bony abnormalities, including periostitis and osteochondritis, that are self-limited but lead to painful pseudoparalysis of Parrot or pathologic fractures. The metaphysitis with metaphysical destruction, the classic Wimberger sign, and other bony changes can be seen on x-ray. Besides pseudoparalysis, the painful swellings of the extremities may be mistaken for nonaccidental trauma (60; 58; 95).
Other organ involvement includes pneumonitis; glomerulonephritis or nephrotic syndrome with hypertension, hematuria, proteinuria, hypoproteinemia, hypercholesterolemia, and hypocomplementemia; leptomeningitis; and ophthalmologic abnormalities, including interstitial keratitis, uveitis, optic atrophy, and papilledema.
|
General | |
|
• Intrauterine growth retardation | |
|
Skin | |
|
• Cutaneous maculopapular or vesiculobullous rash | |
|
Bone | |
|
• Periostitis | |
|
Mucosa | |
|
• Purulent or bloody rhinitis | |
|
Kidney | |
|
• Glomerulonephritis | |
|
Eyes | |
|
• Uveitis | |
|
CNS | |
|
• Leptomeningitis | |
|
Lungs | |
|
• Pneumonia | |
|
Laboratory | |
|
• Leukocytosis | |
Early congenital syphilis may present with life-threatening manifestations (See Table 2) secondary to liver failure, severe anemia, leukemoid reaction, thrombocytopenia, disseminated intravascular coagulation, hypoglycemia, acidosis, meningoencephalitis, respiratory failure secondary to pneumonia alba, or diaphragmatic compromise from ascites or hepatosplenomegaly. Pancreatitis, necrotizing enterocolitis, nephrotic syndrome with anasarca, and failure to thrive (114) are other severe presentations.
|
• Nonimmune hydrops |
Laboratory abnormalities include leukocytosis or leukopenia, Coombs-negative hemolytic anemia, thrombocytopenia, and increased liver enzymes. The CSF may show an increased protein concentration or a mainly lymphocytic pleocytosis. Premature infants born with early congenital syphilis have a greater tendency to have positive CSF findings (63).
Early congenital syphilis has been associated with persistent hypoglycemia and hypopituitarism (29).
Coinfection with HIV is associated with accelerated progression to early neurosyphilis with optic neuritis, meningitis, or cerebrovascular accidents; neurosyphilis may be the first sign of HIV infection (34).
Late congenital syphilis. The late manifestations of congenital syphilis result from either scarring from early untreated systemic disease or a hypersensitivity reaction. Approximately 40% of surviving infants develop late manifestations if untreated (44).
Sir Jonathan Hutchinson (1828-1913) established the fact that interstitial keratitis is almost always due to congenital syphilis and described a triad consisting of notched incisors (Hutchinson’s teeth), interstitial keratitis, and sensorineural deafness, which is sudden and usually occurs around 8 to 10 years of age.
Other signs include frontal bossing, short maxilla, saddle nose and other nasal deformities, protruding mandible, high-arched palate, palatal perforations, mulberry molars (Moon’s molars), perioral fissures (rhagades), bilateral knee effusions (Clutton’s joints), sternoclavicular thickening, saber shins, gummas, flaring scapulas, intellectual disability, and hydrocephalus (10).
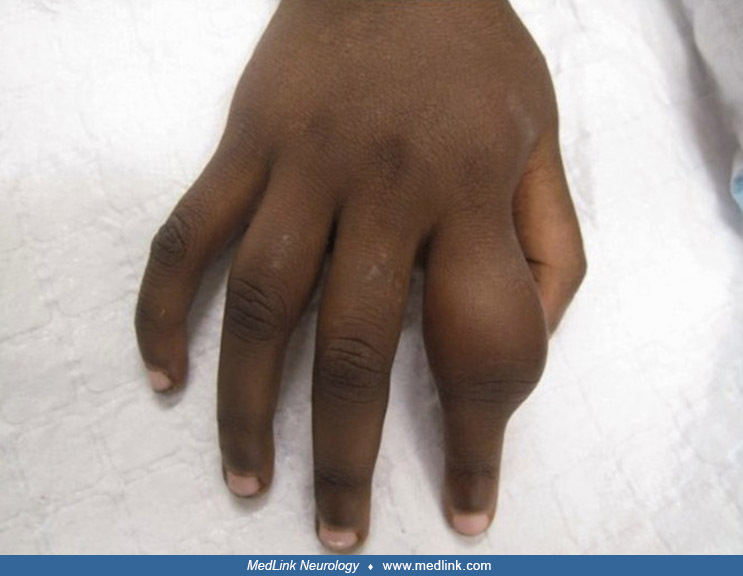
The du Bois sign, a shortened fifth finger (brachymesophalangia) in congenital syphilis, was recognized by the Swiss dermatologist Charles du Bois (1874-1947), director of the Dermatological Syphiligraphic Clinic of the Medical Faculty in Geneva (and not the French gynecologist Paul Dubois (1795-1871) as has often been misattributed) (110; 02; 03; 94; 54). The du Bois sign is not specific to congenital syphilis as it can be seen in Down syndrome and some other disorders.
This image depicts a dorsal view of a patient’s hands, which exhibited signs found in late congenital syphilis due to syphilitic bone disease that included osteoperiostitis, ulnar deviation of the middle fingers, and du Bois si...
Drawing in oil of a 16-year-old girl showing some of the effects of congenital syphilis. The teeth are “pegged” (Hutchinson teeth), and the bridge of the nose is flattened (saddle nose). Both eyes are affected with interstitial...
This man presented with complex symptomatology, subsequently diagnosed as complications of congenital syphilis. Note the stigmata indicative of this disease, including frontal bossing, mulberry molars, Hutchinson teeth, saddle ...
Watercolor drawing of the face of a young girl, aged 11 years, showing ulceration in the nose as a result of congenital syphilis. Illustration by surgeon and Anatomist Thomas Godart (active 1852-1861), pathological artist at St...
Gummas are nonspecific granulomas found in tertiary syphilis. They may occur in any organ and may be single or multiple. Gummas cause local destruction and typically occur in the palate, liver, or brain (34).
• Hutchinson triad | ||
- notched incisors (Hutchinson’s teeth) | ||
• Frontal bossing | ||
Congenital syphilis is associated with premature birth, low birth weight, stillbirth, neonatal death, and congenital abnormalities (eg, deformed bones, anemia, hepatosplenomegaly, jaundice, permanent vision or hearing loss, and meningitis) (108).
Late congenital syphilis should be considered an avoidable complication of congenital syphilis because it is almost completely prevented when early congenital syphilis, asymptomatic or symptomatic, is treated appropriately with careful serologic monitoring. Approximately 40% of surviving infants develop late manifestations if untreated (44).
Interstitial keratitis is the most common late finding, appearing close to puberty and even occurring with appropriate therapy (101). Because of the risk of developing sensorineural hearing loss, repeat audiologic testing is recommended at 24 to 30 months of age in an infant with congenital syphilis. In a systematic review of sensorineural hearing loss in congenital syphilis, no cases of progressive or delayed hearing loss due to congenital syphilis were found among children with previously normal testing (25).
Lanata and associates describe an infant with a delayed diagnosis of congenital syphilis in Ohio, USA (59).
A 7-week-old term Black boy born via uncomplicated vaginal delivery presented for evaluation of fever (102 degrees F), 2 days of increased irritability, and decreased left leg movement. He had experienced nasal congestion since birth. He had also developed a rash with discrete “sores” on his face and extremities that had peeled 1 week before presentation. There was no known trauma. Maternal prenatal care had been adequate, including treatment for bacterial vaginosis and Candida vaginitis during the first trimester. Laboratory work and serologies were negative.
Physical examination revealed a fussy but consolable infant, mild congestion without rhinorrhea, a hoarse cry, oral thrush, and hepatomegaly. Small, discrete, hypochromic macular lesions with fine desquamation of the borders were noted on his cheeks, chin, arms, and legs. Ophthalmologic examination was normal. The left hip and knee were held in a flexed position; movement of the contralateral hip caused discomfort.
Radiograph of his right femur showed a nondisplaced fracture of the distal metaphysis. Skeletal survey revealed additional fractures of the bilateral tibia, scattered areas of cortical destruction, and diffuse periostitis of long bones. Computed tomography scan of the head was normal. Laboratory results were as follows: white blood cell count 8.9 x 109/L; hemoglobin 6.9 g/dL; hematocrit 22.6%; platelets 528 x 109/L; and reticulocyte count 8.5%. The direct Coombs testing, uric acid, lactate dehydrogenase, serum electrolytes, parathyroid hormone, and urinalysis were unremarkable. Aspartate aminotransferase was normal (37 U/L), but alanine aminotransferase (74 U/L) and alkaline phosphatase (905 U/L) were elevated. Respiratory viral testing was positive for coronavirus.
Child abuse consultants reviewed the findings and became concerned about congenital syphilis based on the cutaneous lesions found on the palms and soles. Rapid plasma reagin (RPR) testing was performed, and infectious disease specialists were consulted. The patient’s serum RPR titer was 1:512, and the Treponema pallidum particle agglutination (TP-PA) test was reactive, confirming the diagnosis of congenital syphilis. CSF collected to evaluate for possible neurosyphilis revealed one red blood cell/mm3, six white blood cells/mm3 (45% polymorphonuclear neutrophils; 35% lymphocytes; 20% monocytes), normal glucose (45 mg/dL), elevated protein (61 mg/dL), and nonreactive VDRL. Ophthalmologic examination was normal. After establishing the diagnosis, his mother recalled that she had first noticed his left lower extremity pseudoparalysis on his fourth day of life but was reassured after evaluation by his pediatrician.
He received 10 days of intravenous aqueous penicillin G (50,000 units/kg/dose every 6 hours). Four hours after the first dose, he developed a Jarisch-Herxheimer reaction characterized by transient fever and tachycardia. His pseudoparalysis and pain resolved before discharge. On follow-up, he achieved normal growth parameters and developmental milestones. At age 7 months, the serum RPR titer had decreased to 1:4.
The parents were referred to the health department for confirmatory testing. The mother’s RPR titer was 1:32 with a reactive fluorescent treponemal antibody absorption (FTA-ABS) test. She was found to have hyperpigmented lesions on the palms and soles and was ultimately diagnosed with secondary syphilis. The father’s RPR test was nonreactive. Both parents received a single intramuscular injection of benzathine penicillin G (2.4 mU).
The bacterium Treponema pallidum is a human pathogen and has never been cultured with certainty in artificial media, fertilized eggs, or tissue cultures. The organism can remain viable in stored blood or plasma at 4 degrees C for up to 24 hours (55).
Morphologically, T pallidum is a thin spiral-shaped bacterium that measures about 0.2 µm in width and 5 to 15 µm in length; the organism is tightly wound, and sequent turns around its spiral are separated by 1µm. They are actively motile, corkscrewing constantly along their major axes. In addition, three sheathed flagella are located at each end. The spirals are so thin that dark-field illumination or immunofluorescence is necessary for visual detection of T pallidum.
The treponeme has a glycosaminoglycan layer (that may have an antiphagocytic capacity), six major proteins in the outer membrane, and a double wall that contains cardiolipin (some of which may be incorporated from damaged host tissues). Antibodies to the cardiolipin form the basis for the nontreponemal serologic tests (34). The T pallidum genome has been sequenced (38).
Only two bacterial species are commonly found to cross the placenta and infect the fetus: Treponema pallidum subspecies pallidum and Listeria monocytogenes (33). The treponemes can cross the placenta at any stage of the disease and at any time of pregnancy. T pallidum enters the fetus either by hematogenous or transplacental spread or by contamination with active vaginal or vulvar lesions during passage through the birth canal. Fetal infection causes increased production of inflammatory cytokines IL2, IFN-gamma, TNF-alfa, and prostaglandins. This and the intense fetal inflammatory response elicited by the activation of macrophages by treponemal lipoproteins may cause fetal death, preterm birth, intrauterine growth retardation, and other manifestations of congenital syphilis (82). In a study of 215 patients with treponemal infection, chronic villitis (94%), acute chorioamnionitis (92%), and villous immaturity (66%) were the most common abnormalities (67). HIV co-infection and penicillin treatment were associated with reduced frequencies of inflammatory lesions (67).
Controversy exists regarding the association with first-trimester loss. Some believe that passage of treponemes in the first 20 weeks is associated with only a mild inflammatory reaction in the placenta (111), whereas others found spirochetes in fetal tissue from spontaneous abortions at 9 to 10 weeks of gestation (45). Although antibodies are formed in response to this infection, the disease progresses. Likewise, acquired syphilis may occur in individuals who have had the congenital form of the disease (34).
Among a cohort of 2,566,246 women in California between 2007 and 2011, 991 pregnancies were complicated by maternal infection with syphilis (0.04%). Syphilis infection was significantly associated with preterm delivery (aOR: 1.27, 95% CI: 1.05-1.54), NICU admission longer than 24 hours (aOR: 2.54, 95% CI: 2.13-3.04), and stillbirth (aOR: 5.01, 95% CI: 3.16-7.92) after adjusting for potential confounders, including maternal age, race and ethnicity, education, parity, prenatal visits, body mass index, smoking, and insurance status (97).
In a perinatal autopsy study of 21 stillborn fetuses, common findings included chronic stress of the thymus, hydrops fetalis, and hepatosplenomegaly (57); common placental findings included placentomegaly and amniotic fluid infection. The infected placenta is thick and enlarged with prominent vascular proliferations, villous immaturity and hypercellularity, chronic villitis, and foci of acute villitis (90).
In another perinatal autopsy study of 11 feto-placental examinations of untreated congenital syphilis, the most consistent autopsy findings included hydrops, long bone metaphyseal bands on x-ray, and hepatic lesions (51). The combination of chronic and acute villitis/intervillitis is a common placental feature in these cases with mixed inflammatory populations.
Following incubation, the classic findings of obliterative endarteritis occur, which include endothelial and fibroblastic proliferation and thickening and infiltration with plasma cells, lymphocytes, and histiocytes.
Extramedullary hematopoiesis is seen in the liver and may be observed in the spleen, stomach, intestine, pancreas, and lung.
Inflammatory reactions are seen in the liver, spleen, stomach, intestine, and pancreas. The “pneumonia alba” consists of an obliterative fibrosis, with increased connective tissue in the septa and interstitium and, on gross inspection, large, firm yellow-white lungs. Immune complex deposition occurs in the renal glomeruli and may or may not include complement.
Widespread involvement of long bones and ribs is prevalent, with osteochondritis, osteomyelitis, and periostitis. The trabeculae are eroded, and fibrosis occurs (34).
Neurosyphilis can be either meningovascular or parenchymatous. In both forms, the infectious process begins in the meninges as a widespread diffuse arachnoiditis with inflammation concentrated around the meningeal vessels and the branches that penetrate the cortex. Small meningeal arterioles can show thickening and infiltration of the adventitia as well as intimal proliferation; syphilitic phlebitis is less common, though both arteritis and phlebitis can result in infarction with localized lesions of the brain or spinal cord.
Obstructive or communicating hydrocephalus can result from meningeal fibrosis and obliteration of the subarachnoid spaces.
Diffuse meningeal inflammation of the secondary stage can be carried over into the tertiary stage with increased fibrosis of the meninges and the formation of small, often miliary gummas.
In parenchymatous congenital neurosyphilis, as in juvenile paresis, diffuse degeneration occurs with cerebral and cerebellar atrophy. Microscopic changes include round-cell meningeal and perivascular infiltration, loss and degenerative changes in the nerve cells with an increase in microglia and astroglia, a disturbance of normal cytoarchitecture, deposition of iron pigment, and the presence of spirochetes (111).
Risk factors (analytic epidemiology). Congenital syphilis is contracted from an infected mother via transplacental transmission of T pallidum any time during the pregnancy or at birth from contact with maternal lesions. Among women with untreated early syphilis, up to 40% of pregnancies result in spontaneous abortion, stillbirth, or perinatal death. The rate of transmission is 60% to 100% during primary and secondary syphilis and decreases with later stages of maternal infection – 40% with early latent and 8% with late latent infection.
Prevention of congenital syphilis relies on identifying and adequately treating pregnant women with syphilis. All women should be screened serologically early in pregnancy. In areas where syphilis is prevalent and women are at high risk for infection, serologic testing should also be performed at 28 to 32 weeks’ gestation and at delivery, given the fact that false-negative test results are possible in recent infection and that syphilis can be acquired later in pregnancy after initial testing (04).
Changes in the population incidence of primary and secondary syphilis among women are usually followed by similar changes in the incidence of congenital syphilis (19). Syphilis is rare in much of the industrialized world but persists in the United States as well as in resource-limited countries (04).
A study of linked maternal and congenital syphilis data from the Georgia Department of Public Health, in the period from 2008 to 2015, found that of 505 women with syphilis infection, 23% had an infant with congenital syphilis (56). After adjusting for race and ethnicity, factors associated with a congenital syphilis outcome were age greater than 35 years (adjusted odds ratio 3.9), hospital or emergency department diagnosis of syphilis (adjusted odds ratio 3.4), and high-risk behaviors such as exchanging sex for money or drugs (adjusted odds ratio 3.3).
A review of maternal and perinatal risk factors associated with congenital syphilis found that inadequate prenatal care, as well as inadequate or late treatment of maternal syphilis, were significant risk factors for congenital syphilis (81). Women with recent syphilis with high VDRL titers had a higher rate of vertical transmission (81). A prior history of syphilis with adequate treatment was identified as a protective factor, resulting in lower rates of congenital syphilis (81). Among the epidemiological and demographic aspects surveyed, young age, lower schooling, unemployment, low family income, and no fixed residence were associated with a higher risk of congenital syphilis (81).
In a retrospective analysis of the CDC's Natality Live Birth database for the years 2016 to 2019, of the more than 15 million births included, 0.11% were complicated by maternal infection with syphilis (43). Concurrent infection with gonorrhea was associated with the highest risk of syphilis in pregnancy (adjusted odds ratio, 7.2). Low educational attainment, Black race, and Medicaid insurance were also associated with a significantly increased risk of syphilis. Syphilis infection was associated with an increased risk of preterm birth, low birth weight, congenital malformations, low 5-minute Apgar scores, neonatal intensive care unit admission, immediate ventilation, and prolonged ventilation.
Pregnant women who engage in high-risk behaviors, including sex work, having multiple sexual partners, or substance use, are at a higher risk of syphilis exposure and infection (08; 109).
United States descriptive epidemiology. The incidence of congenital syphilis decreased dramatically in the United States from the 1940s to the 1980s due to the availability of penicillin and an emphasis on maternal and infant case findings (22). This was followed by a short period of increased rates at the beginning of the 1990s and then again since 2012 in all race and ethnicity groups (22; 08; 61).
The rate of congenital syphilis decreased in the United States from 1991 to 2005 but increased slightly from 2005 to 2008 (21). The congenital syphilis rate among infants less than 1 year of age increased 23%, from 8.2 cases per 100,000 live births in 2005 to 10.1 in 2008. This increase followed a 38% increase in the primary and secondary syphilis rate among females from 2004 to 2007. From 2005 to 2008, the congenital syphilis rate among infants born to Hispanic, white, and black mothers increased; most of the increase in congenital syphilis cases and rate occurred in infants born to black mothers. This increase was observed in infants born to black mothers, primarily in the South. The increases in primary and secondary syphilis among black women in the South were linked to crack cocaine use and commercial sex work (19).
From 2008 to 2012, the number of congenital syphilis cases declined in the United States from 10.5 to 8.4 cases per 100,000 live births, reflecting declining trends in rates of primary and secondary syphilis among women, from 1.5 to 0.9 cases per 100,000 women. During this period, all regions of the United States have experienced a decrease in congenital syphilis rates except for the Midwest, where the rate increased from 4.2 to 6.8 cases per 100,000 live births, attributed primarily to increases in Illinois and Ohio. The increased congenital syphilis rates were seen 1 to 2 years after observed increases in primary and secondary syphilis among women in these states. Racial disparities between non-Hispanic black and non-Hispanic white congenital syphilis rates increased from 2008 to 2012; relative decreases in rates of congenital syphilis were higher among whites (21%) than blacks (11%) (21).
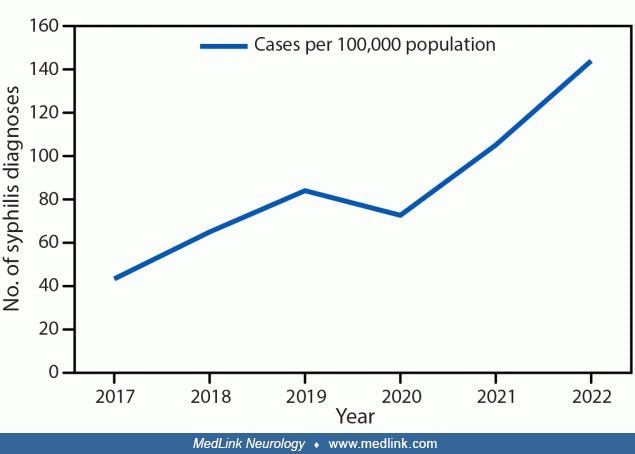
Since 2012, the rate of reported congenital syphilis has subsequently increased each year (21; 18; 22; 35; 69; 11; 28; 31; 65; 78; 93; 08; 70). Penicillin shortages, lack of screening, and lack of adequate treatment have all contributed to global disease burden (01). Rising stillbirth rates are related to rising congenital syphilis rates in the United States from 2016 to 2022 (65). By 2017, the national rate was 23.3 cases per 100,000 live births, with a total of 918 reported cases, including 64 syphilitic stillbirths and 13 infant deaths. Following historic trends, this increase in congenital syphilis incidence has paralleled increases in primary and secondary syphilis among all women and reproductive-aged women from 2013 to 2017 (155.6% and 142.8% increases, respectively) (22).
Reported number of cases of congenital syphilis among infants, by year of birth, and rates of reported cases of primary and secondary syphilis among females aged 15-44 years, by year--United States, 2012 to 2022. Cases per 100,...
Rates of maternal syphilis increased markedly from 2016 to 2022, with increases in maternal syphilis in all racial groups but especially for American Indians or Alaska Natives (40; 78). Maternal syphilis rates increased for all maternal age groups, but especially for those younger than 20 years and those 20 to 24 years (40). Maternal syphilis rates increase with increasing delays in prenatal care, with the lowest levels for women who received prenatal care in the first trimester and the highest for women who did not receive prenatal care (40; 109). There is considerable geographic variation by state in maternal syphilis rates and the rate of change from 2016 to 2017 through 2021 to 2022 (40).
(1) Significant increasing trend from 2016 to 2022 (p < 0.05). (2) Significant difference from other race and Hispanic-origin groups for 2022 (p < 0.05). (3) Significant difference from other race and Hispanic-origin grou...
(1) Significant increasing trend from 2016 to 2022 (p < 0.05). (2) Significant decreasing trend by timing of prenatal care for each year 2016 to 2022 (p < 0.05). Note: In 2022, 2.2% (77,228) of mothers did not receive pre...
Each state and the District of Columbia. Note: Maternal syphilis rate is the number of live births to women with syphilis per 100,000 live births. (Source: National Center for Health Statistics, National Vital Statistics System...
Rates of congenital syphilis similarly vary by race and are highest among American Indians or Alaska Natives, native Hawaiians or Pacific Islanders, and blacks, although all racial groups except Asians have seen progressive increases in rates since 2017 (22).
There is considerable geographic variation in congenital syphilis rates within the United States, with the highest-rated states concentrated in the West (22). However, since 2012, most states have experienced increases in case counts and rates (22).
In 2020, a Centers for Disease Control and Prevention study showed that half of the U.S. congenital syphilis cases in 2018 occurred due to gaps in testing and treatment during prenatal care (24). The most frequently missed opportunities for preventing congenital syphilis cases occurred in mothers who were diagnosed but inadequately treated (31% of cases) or mothers who did not have timely prenatal care (28% of cases). Prevention gaps varied by region; nearly nine in 10 congenital syphilis cases were in the South and West. In the South (34% of cases), lack of adequate treatment was the most common missed prevention opportunity, whereas in the West, lack of timely prenatal care was most common (41% of cases) (24d).
An analysis by the CDC in 2023 identified the lack of timely prenatal care and the consequent lack of timely syphilis testing as the most important missed preventive opportunity among mothers delivering children with congenital syphilis, followed closely by the lack of adequate maternal treatment despite receipt of a timely syphilis diagnosis (23).
In 2022, there were 3,761 cases of congenital syphilis in the United States, including 6% that were stillborn and 1% that died in infancy (69). A lack of timely testing and adequate treatment during pregnancy contributed to 88% of cases of congenital syphilis (69). Testing and treatment gaps were present in most cases across all races, ethnicities, and U.S. Census Bureau regions (69).
Timely testing is performed 30 or more days before delivery. Late identification of seroconversion is a new reactive syphilis test fewer than 30 days before delivery after a nonreactive test earlier in pregnancy. Adequate treat...
In Mississippi, the number of infants hospitalized with congenital syphilis spiked 11-fold from 10 in 2016 to 110 in 2022 (100). There was a corresponding 12-fold rise in hospitalization rates for congenital syphilis in this interval. Of the 367 infants hospitalized with congenital syphilis from 2016 to 2022, 98% were newborns, 93% were covered by Medicaid, 71% were African American, and 58% were nonurban residents. Newborns with congenital syphilis had higher odds of being affected by maternal illicit drug use, being born prematurely (less than 37 weeks), and having very low birth weight (less than 1,500 g) than those without congenital syphilis.
Numbers above bars are rates for each year. Rates were obtained by dividing the number of infants hospitalized with congenital syphilis by the total number of delivery hospitalizations per year. (Source: Staneva M, Hobbs CV, Do...
The increases in maternal infections have also produced an increase in stillbirths and infant deaths due to congenital syphilis (22; 65). In 2023, there were 3882 cases of congenital syphilis in the United States, including 279 congenital syphilis–related stillbirths and neonatal/infant deaths (108).
Stillbirths with congenital syphilis are not identified well by existing surveillance systems. In a prospective, single-site cohort study of all cases of syphilis among mothers and their infants from 1984 to 2002, 191 cases of congenital syphilis were identified, of whom 59 died, for a case-fatality ratio of 31% (113). Of the 59 deaths, 90% were stillborn, and 10% died in the neonatal period. Most (74%) stillbirths occurred in the third trimester. The CDC surveillance case definition correctly identified all infants with congenital syphilis, but the CDC case-fatality ratio was only 10%.
Global descriptive epidemiology. Worldwide, syphilis is a leading cause of adverse pregnancy outcomes (ie, stillbirth and neonatal death) (105). Screening and treatment for syphilis during pregnancy remain suboptimal in low- and middle-income countries despite feasible and cost-effective diagnosis and prevention of maternal-to-child transmission (107).
In 2007, the World Health Organization (WHO) launched a global initiative to eliminate congenital syphilis. This was followed by the Global Guidance on Criteria and Processes for Validation of Elimination of Mother-to-Child Transmission of HIV and Syphilis, launched in 2014. To be considered for elimination of maternal-to-child transmission of syphilis, countries must have met WHO criteria for 2 years for process indicators and 1 year for the impact indicator before review by regional and global validation committees to confirm elimination. The impact indicator was a case rate of congenital syphilis less than or equal to 50 cases per 100,000 live births. Process indicators included (1) antenatal care coverage of at least one visit greater than or equal to 95%; (2) coverage of syphilis testing of pregnant women greater than or equal to 95%; and (3) treatment of syphilis-seropositive pregnant women greater than or equal to 95%.
In June 2017, a global meeting of experts convened by the WHO Department of Reproductive Health and Research and the Bill and Melinda Gates Foundation reviewed the progress made to eliminate congenital syphilis since the 2007 initiative. Only 9% of Global Aid Monitoring (GAM)-reporting countries achieved the milestone of greater than or equal to 95% testing of women who received antenatal care and greater than or equal to 95% treatment of pregnant women who test positive. These data fall short of the 2020 milestone of 70% of countries. Meeting participants felt that this limited progress could be attributed to challenges such as limited access to and performance of syphilis testing in antenatal care clinics and limited availability and use of benzathine benzylpenicillin (only recommended treatment for pregnant women with syphilis) (112).
Unfortunately, many countries have experienced a reemergence of congenital syphilis and syphilis among women of childbearing age over the past 10 to 20 years (13; 73; 12; 30; 46; 66; 75; 77; 87). Case rates are rising in many high-income countries but remain relatively low compared with those in low- and middle-income settings (74). There continue to be large variations in case rates by region, with the highest numbers of cases in the African and Eastern Mediterranean regions (39). There are also pockets of high-incidence areas within the other regions.
In Brazil, rates for syphilis in pregnant women and rates of congenital syphilis have been rising for the past decade (73; 30; 79; 98). An increasing proportion of these women have been prescribed penicillin over this interval, but significant gaps remain.
HIV and syphilis cases reported on the Brazilian National Notifiable Diseases Information System (SINAN) by 06/30/2022. HBV cases reported on SINAN by 12/31/2021. (Source: Health Surveillance Secretary of the Ministry of Health...
HIV and syphilis cases reported on the Brazilian National Notifiable Diseases Information System (SINAN) by 06/30/2022. HBV cases reported on SINAN by 12/31/2021. (Source: Health Surveillance Secretary of the Ministry of Health...
Maternal syphilis cases reported on the Brazilian National Notifiable Diseases Information System (SINAN) by 06/30/2022. Prescribed treatment was with at least one dose of benzathine penicillin, regardless of the clinical form....
United States. Prevention and detection of congenital syphilis lies in identifying and treating syphilis in pregnant women, which requires that all pregnant women receive adequate prenatal care.
This is accomplished through routine serologic screening of pregnant women (22). The CDC advises rescreening high-risk women at 28 weeks’ gestation and again at delivery (62). To manage pregnant women who have syphilis, the CDC recommends obtaining information concerning ongoing risk behaviors and treatment of sex partners to assess the risk for reinfection. The CDC also recommends that no mother or newborn infant leave the hospital after birth without maternal serologic status being documented at least once during pregnancy and preferably again at delivery in at-risk women (22).
Using 2018 national congenital syphilis surveillance data and a previously developed framework, the CDC identified missed opportunities for congenital syphilis prevention based on an increase in reported congenital syphilis cases in the United States from 2013 to 2018. Nationally, the most missed prevention opportunities were (1) a lack of adequate maternal treatment despite the timely diagnosis of syphilis (31%) and (2) a lack of timely prenatal care (28%) (24).
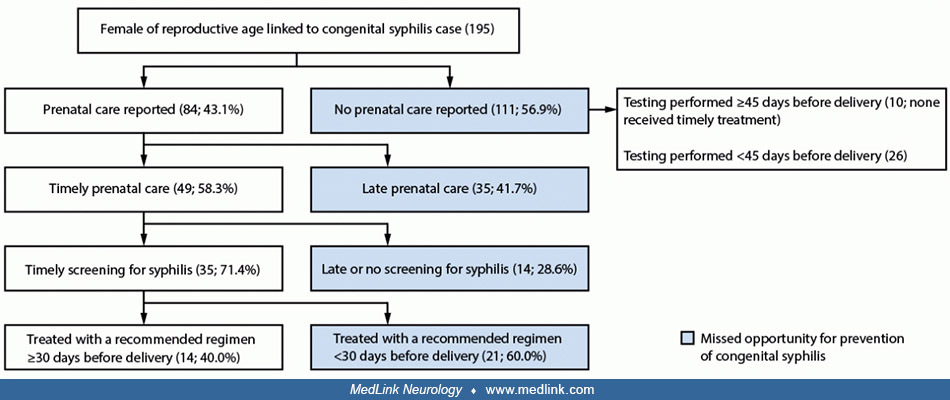
Southern Nevada Health District (Clark County) emergency department visit data by pregnant women were reviewed for 2017 to 2022 to assess whether there were missed opportunities to screen pregnant females for syphilis (84). Among 195 pregnant women identified, only 43% received prenatal care during pregnancy. Over one half (57) had at least one emergency department encounter 30 or more days before delivery and had not yet received testing for syphilis at the time of the encounter; syphilis testing was performed at only 68% of these encounters. Lack of prenatal care was a considerable barrier to timely testing and treatment in Clark County, Nevada, but emergency department visits are an opportunity for syphilis screening of pregnant females who do not access prenatal care. Syphilis testing should be part of the standard process for emergency department visits of pregnant women who have not received prenatal care or who have not yet received testing for syphilis.
Clark County, Nevada, 2017 to 2022. Notes: (1) Timely is defined as 45 or more days before delivery for prenatal care and screening and 30 or more days before delivery for initiation of appropriate treatment. (2) Testing among ...
Globally. For global elimination of congenital syphilis, the World Health Organization identified four pillars for action in 2007: (1) ensure sustained advocacy and political commitment for successful health initiatives; (2) increase access to and quality of maternal and newborn health services; (3) screen and treat all pregnant women and partners; and (4) establish surveillance, monitoring, and evaluation systems (48). These pillars will not only impact congenital syphilis but also improve maternal health and decrease infant mortality, HIV/AIDS, and other diseases. Hossain and colleagues analyzed the implementation of this plan (countries with low-to-mid prevalence rates of congenital syphilis versus countries with high prevalence rates) and found that implementation was variable in the 14 countries analyzed (48). Financial resources, though a limiting factor, were not an insurmountable barrier to improvement.
Congenital syphilis is now part of a group of congenital infections that, since 1971, has been known as TORCH, an acronym for Toxoplasmosis, Other, Rubella, Cytomegalovirus, and Herpes (76). The acronym was devised to focus attention on a group of microbial agents that cause such clinically similar manifestations in newborns that testing for one should mean testing for all (76). The emergence of human immunodeficiency virus infection and the reemergence of congenital syphilis have led to modifications of the TORCH acronym, for example, STORCH (Syphilis, Toxoplasmosis, Other, Rubella, Cytomegalovirus, and Herpesvirus) and STARCH (Syphilis, Toxoplasmosis, Acquired immunodeficiency syndrome, Rubella, Cytomegalovirus, and Herpesvirus), which more appropriately reflect current pathogens (09).
Yaws. Many clinical signs of congenital syphilis are also present in yaws, a chronic bacterial infection that affects the skin, bone, and cartilage. Yaws is caused by the bacterium Treponema pallidum subspecies pertenue, which belongs to the same group of bacteria that causes venereal syphilis; consequently, another term for yaws is non-venereal endemic syphilis (42; 64). The clinical similarities between congenital syphilis and yaws include skin rashes and saber shins, although yaws has a greater tendency to form papillomas and ulcers. Yaws typically affects children under 15 years who live in poor communities in warm, humid, and tropical forested areas of Africa, Asia, Latin America, and the Pacific Islands. Affected populations typically live in rural areas with little access to modern health services. Poverty and poor personal hygiene are risk factors for the spread of yaws, which spreads through direct contact.
The first sign of yaws is the appearance of a painless papule on the skin, which grows into a papilloma. These large, early granulomatous lesions are highly infectious and display a yellow, crusty surface. Without treatment, sores begin to spread.
These lesions were diagnosed as old, juxta-articular nodules due to yaws. The patient was treated with an intramuscular injection of 2.4 mega units of benzathine benzylpenicillin. (Source: Photography by Dr. Peter Perine, Cente...
(Source: Dofitas BL, Kalim SP, Toledo CB, Richardus JH. Yaws in the Philippines: first reported cases since the 1970s. Infect Dis Poverty 2020;9[1]:1. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creative...
Treatment for this patient consisted of intramuscular injections of 600 units of procaine benzylpenicillin in oil with aluminium monostearate (PAM). (Source: Photography by Dr. Peter Perine, Centers for Disease Control and Prev...
(Source: Photography by Dr. Peter Perine, Centers for Disease Control and Prevention, 1979. Public Health Image Library [PHIL] ID# 3833, Centers for Disease Control and Prevention, Atlanta, Georgia. Public domain.)
The first sign of yaws is the appearance of a painless papule that grows into a papilloma. These early granulomatous lesions are characterized by a yellow-crusted appearance and are highly infectious. (Source: Photography by Dr...
The first sign of yaws is the appearance of a painless papule that grows into a papilloma. These early granulomatous lesions are characterized by a yellow-crusted appearance and are highly infectious. (Source: Photography by K....
The skin lesions were of an undetermined duration and were pruritic. Skin findings included (1) numerous small, whitish, scaly macules on the shoulders and arms; (2) a single, black-crusted erosion on the right elbow area; and ...
(Source: Dofitas BL, Kalim SP, Toledo CB, Richardus JH. Yaws in the Philippines: first reported cases since the 1970s. Infect Dis Poverty 2020;9[1]:1. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creative...
In late yaws, individuals may develop so-called "crab yaws," characterized by hyperkeratosis with fissuring, ulceration of the soles of the feet, and, less commonly, by hyperkeratosis involving the palms of the hands.
Note the soft, tumor-like masses on the sole of his foot, which when both feet are affected, cause the patient to walk in a characteristic but odd fashion, on the sides of his feet, hence the nickname "crab yaws". (Source: Phot...
Note the soft, tumor-like masses on the sole of his foot, which when both feet are affected, cause the patient to walk in a characteristic but odd fashion, on the sides of his feet, hence the nickname "crab yaws". (Source: Phot...
Yaws may eventually cause disfigurement and disability, especially because late or tertiary yaws causes degenerative changes in cartilage and bones, including those of the midface, resulting in a facial deformity known as rhinopharyngitis mutilans or gangosa. The condition is now readily treated with antibiotics.
(Source: Dofitas BL, Kalim SP, Toledo CB, Richardus JH. Yaws in the Philippines: first reported cases since the 1970s. Infect Dis Poverty 2020;9[1]:1. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creative...
The face of this woman showed the ravages of a disease known as yaws, a nonvenereal endemic syphilis, caused by the spirochete Treponema pallidum subspecies pertenue. The condition caused degenerative changes to the cartilage a...
The face of this 78-year-old man shows the ravages of chronic yaws, a nonvenereal endemic syphilis, caused by the spirochete Treponema pallidum, subspecies pertenue. The photograph shows degenerative changes to the cartilage an...
The effectiveness of treatment for yaws is shown in the case of a 30-year-old woman who developed yaws after breastfeeding her 13-month-old infant. The infection began on her left breast and spread to her back, chin, and neck. Treatment with an intramuscular injection of 2.4 mega (million) units of benzathine benzylpenicillin (benzathine penicillin G) produced dramatic improvement after only 1 week.
Most cases of early congenital syphilis occur without symptoms, hence, the need for maternal serologic screening during pregnancy and at the time of delivery. The U.S. Preventive Services Task Force (USPSTF) recommends screening at the first available opportunity (108).
A thorough evaluation of the newborn should occur if an infant meets the CDC case definition, including an infant whose mother had untreated or inadequately treated syphilis at delivery, regardless of signs in the infant.
CDC case definition of congenital syphilis. For public health surveillance purposes, the CDC published a case definition of congenital syphilis (Centers for Disease Control and Prevention 2018):
|
(1) An infant whose mother had untreated or inadequately treated syphilis at delivery, regardless of signs in the infant. Or (2) An infant or child who has a reactive nontreponemal test for syphilis (VDRL, RPR). Or (3) Equivalent serologic methods and any one of the following: | |
|
• Any evidence of congenital syphilis on physical examination (see clinical description). | |
|
• Any evidence of congenital syphilis on radiographs of long bones. | |
|
• A reactive CSF venereal disease research laboratory test (VDRL) test. | |
|
• In a nontraumatic lumbar puncture, an elevated CSF leukocyte (white blood cell, WBC) count or protein (without other cause). | |
|
Suggested parameters for abnormal CSF WBC and protein values: | |
|
• During the first 30 days of life, a CSF WBC count of >15 WBC/mm3 or a CSF protein concentration >120 mg/dl is abnormal. | |
|
• After the first 30 days of life, a CSF WBC count of >5 WBC/mm3 or a CSF protein concentration >40 mg/dl, regardless of CSF serology is abnormal (23). | |
|
• Physical examination | |
|
• Quantitative nontreponemal and a treponemal serologic test for syphilis on infant’s serum sample (not on cord blood because false positive and false negative results can occur) | |
|
• Determination of antitreponemal IgM antibody by a CDC-approved method, if available. | |
|
• CSF cell count, protein, and VDRL | |
|
• Long bone x-rays (unless the diagnosis has already been otherwise established) | |
|
• CBC, platelet count | |
|
• Other tests such as liver function tests, chest x-ray as indicated. | |
|
• If available, pathologic examinations of the placenta or umbilical cord using fluorescent antitreponemal antibody staining |
The physical examination of the infant should focus on the myriad manifestations of early syphilis, many of which will not be present in the immediate neonatal period. Long-bone radiographs show pathologic changes (eg, diaphyseal periostitis and osteochondritis) in 20% of asymptomatic patients and 90% of symptomatic patients (14). The diagnosis of congenital syphilis in symptomatic infants rarely poses a problem, but a problem frequently arises when the infant is asymptomatic at birth (approximately 60% of cases). Early identification and treatment of at-risk neonates are essential to preventing long-term consequences (92).
|
Nontreponemal (detect anticardiolipin antibody and are reported as a titer) | ||
|
Standard tests | ||
|
• VDRL | ||
|
Experimental tests | ||
|
• VDRL ELISA IgG AND IgM | ||
|
Treponemal (detect the immune response to antigens on the spirochete cell surface and are reported as positive and negative) | ||
|
Standard tests | ||
|
• fluorescent treponemal antibody | ||
|
Experimental tests | ||
|
• 19S-IgM fluorescent treponemal antibody-absorption | ||
As with adults, the serologic testing of newborns is neither entirely sensitive nor specific. Previous recommendations were to begin with nontreponemal tests for screening and to use the treponemal tests to confirm presumptive diagnoses (the “traditional algorithm”) (05; 80), but the U.S. Centers for Disease Control and Prevention has now proposed a “reverse sequence algorithm” that begins with a treponemal serologic test (eg, enzyme immunoassay or chemiluminescence immunoassay) (80). Quantitative nontreponemal tests help determine not only the adequacy of treatment but also the occurrence of reinfection and relapse (80).
Algorithms that can be applied to screening for syphilis with serologic tests. Abbreviations: CIA = chemiluminescence immunoassay; EIA = enzyme immunoassay; RPR = rapid plasma regain; TPPA = Treponoma pallidum particle agglutin...
(Source: Papp JR, Park IU, Fakile Y, Pereira L, Pillay A, Bolan GA. CDC Laboratory Recommendations for Syphilis Testing, United States, 2024. MMWR Recomm Rep 2024;73(1):1-32. Adapted from: Peeling RW, Mabey D, Kamb ML, Chen XS,...
Testing for HIV should be done in all cases of syphilis (05). The treponemal tests are cumbersome and expensive, and some are not widely available. Although the treponemal tests are highly specific, their sensitivity is only about 75% to 80% (41; 104; 71).
The prozone phenomenon, caused by an excess of antibodies that interferes with the regular screening tests, is a cause of false negative tests that contribute to late diagnosis of congenital syphilis (15; 80). With clinical findings suggestive of congenital syphilis but negative maternal syphilis tests, healthcare providers should consider the possibility of maternal false negative tests caused by the prozone phenomenon (15; 80).
In developing countries where the availability of on-site testing versus off-site testing is an important issue, tests such as the on-site treponemal immunochromatographic strip (ICS) test, though more expensive than the off-site RPR test, have been cost-effective because the prevalence of maternal syphilis is high (27).
CSF should be analyzed for all children suspected of congenital syphilis because neurosyphilis occurs in 40% to 60% of infants with congenital syphilis (88). This diagnosis is difficult to establish because of passive transfer of nontreponemal IgG antibodies from serum into CSF (106). The CSF abnormalities supporting the diagnosis include an increased protein concentration and leukocyte count and a positive VDRL. The interpretation of these results in neonates is difficult because their CSF protein can be normal up to 150 mg/dL, and their leukocyte count can reach 35 cells/mm3 in term neonates and 45 cells/mm3 in low-birthweight premature infants. Negative CSF VDRL or FTA-ABS does not exclude CNS involvement. Hence, if CSF test results cannot exclude infection in an infant evaluated for congenital syphilis, the infant should be treated (05). Using the CSF rabbit infectivity test to identify infants with CNS T pallidum infection, overall CNS infection was best predicted by IgM immunoblotting of serum or PCR assay of serum or blood (72). However, because such testing is not routinely available and because the risk of CNS involvement is high in congenital syphilis, infants diagnosed as having congenital syphilis by physical examination, conventional laboratory tests, and radiological examination should be treated with a 10-day course of aqueous penicillin G or penicillin G procaine for presumed CNS infection.
Other tests, as clinically indicated, include chest radiography for pneumonia alba, complete blood count for leukemoid reaction, blood smear and Coombs test for hemolytic anemia, platelet count, liver function tests for hepatitis, urinalysis for hematuria and proteinuria, and HIV/TORCH titers.
Identification and treatment of congenital syphilis at birth or within 3 months of life prevents late sequelae (91). Parenteral penicillin G remains the preferred drug for syphilis at any stage. Parenteral penicillin is the only documented effective therapy for patients with syphilis during pregnancy and for those with neurosyphilis and is strongly recommended whenever possible in HIV-infected patients. Higher CSF penicillin levels are reached with aqueous penicillin G than with procaine penicillin G (07).
Due to the diagnostic limitations of congenital syphilis, the CDC developed treatment recommendations based on clinical scenarios (91). Management decisions are based on the following: (1) identifying syphilis in the mother; (2) comparing the maternal (at delivery) and infant nontreponemal serologic titers by using the same test and preferably the same laboratory; (3) determining the adequacy of maternal treatment for syphilis; and (4) determining if the infant has clinical, laboratory, or radiological evidence of syphilis (18).
For management purposes, neonates can be divided into three groups (17; 05):
(1) Symptomatic infants with proven disease, as demonstrated by (A) evidence of active disease on physical, radiological, or laboratory examination, or (B) the placenta, umbilical cord, or body fluids are positive for treponemes using specific fluorescent treponemal antibody staining or darkfield examination.
(2) Asymptomatic infants born to untreated mothers, whose treatment was not documented, or who received inadequate treatment during pregnancy. (A) presumed disease in infants whose evaluation (serologic, radiologic, and CSF examination) is abnormal, or (B) no apparent disease in infants whose evaluation is normal.
(3) Asymptomatic infants born to mothers who received adequate treatment for syphilis; for example, a mother who was treated more than 4 weeks before delivery with an appropriate penicillin regimen and whose nontreponemal antibody titer in early syphilis decreased 4-fold, or the low titer remained stable and low in late syphilis and the mother has no evidence of reinfection or relapse.
If a neonate has proven or presumed congenital syphilis, aqueous crystalline penicillin G is preferred. The dosage should be based on chronological, not gestational, age. The recommended dosage is 100,000 to 150,000 U/kg per day (given as 50,000 U/kg/dose intravenously every 12 hours during the first 7 days and then every 8 hours thereafter for a total of 10 days). Alternately, some experts recommend aqueous procaine penicillin G (50,000 U/kg/dose once a day, intramuscularly) for 10 days. If more than 1 day of therapy is missed, the entire course should be restarted.
Asymptomatic infants born to mothers whose treatment for syphilis may have been inadequate should be fully evaluated and treated with aqueous crystalline or procaine penicillin G for 10 days. Some experts treat with a single dose of 50,000 U/kg of benzathine penicillin G intramuscularly if the clinical and laboratory evaluation, including CSF findings and x-rays (long bones and chest), was normal and the follow-up can be ensured.
Asymptomatic infants born to mothers whose treatment for syphilis was adequate should be examined and followed monthly until their serologic test results become negative. If adequate follow-up is not feasible, some experts recommend treating these infants with a single dose of benzathine penicillin.
Infants over 1 month of age with possible congenital syphilis or who have neurologic involvement should be treated with aqueous crystalline penicillin, 200,000 to 300,000 U/kg per day, intravenously (administered every 4-6 hours), for 10 days. This regimen should also be used to treat children older than 2 years of age who have late and previously untreated congenital syphilis. Further, some experts also suggest giving such patients a single dose of benzathine penicillin G, 50,000 U/kg, intramuscularly, after 10 days of intravenous aqueous penicillin. If the CSF examination and CSF-VDRL are negative, some experts recommend treating with three weekly doses of benzathine penicillin G 50,000 U/kg (05).
If there is a shortage of aqueous crystalline penicillin G, some or all doses may be substituted with daily doses of procaine penicillin. If both aqueous and procaine penicillin G are unavailable, ceftriaxone may be used in consultation with a specialist to treat congenital syphilis. Ceftriaxone must be used with caution in jaundiced infants, and because ceftriaxone has not been adequately studied in the treatment of congenital syphilis, infants will need clinical and serologic follow-up (18).
In cases of penicillin allergy, skin testing should be done and will be negative in most patients. Desensitization should be performed in the remaining patients. Administration of penicillin to “allergic” individuals with such precautions has been well tolerated.
The Jarisch-Herxheimer reaction, including fever, chills, hypotension, tachycardia, tachypnea, and leukocytosis, occurs in some newborns within a few hours after treatment. It can be treated with prednisone to mitigate symptoms if necessary. Treatment with penicillin should not be discontinued (34).
After appropriate therapy for congenital syphilis, follow-up should be performed on both symptomatic and asymptomatic neonates (103). A careful physical examination should be performed at 2, 4, 6, and 12 months of age. Nontreponemal serologic testing should be performed every 2 to 3 months until the test becomes negative or the titer has decreased by at least 4-fold. After successful treatment of congenital syphilis, titers should decline by 3 months and become nonreactive by 6 months. If titers increase, fail to decline, or are still present 6 to 12 months after initial treatment, the infant should be reevaluated, including CSF examination, and retreated with parenteral penicillin G for 10 days (05).
Because treponemal tests can remain positive despite effective treatment, they are not used to evaluate the response to therapy. After treatment, the infants usually seroconvert by 18 months of age. A reactive treponemal test at 18 months of age requires full reevaluation and treatment for congenital syphilis (05; 99).
If congenital syphilis is diagnosed and treated appropriately and timely, the prognosis for this disease is excellent. However, there is an increased risk for worse outcomes and possible death in (1) premature infants, (2) those who have a delay or do not receive proper treatment, (3) patients who display an extensive spread of the disease with multiple organ failure, (3) and infants with a severe Jarisch-Herxheimer reaction with treatment. Delayed diagnosis and treatment can lead to late and persistent clinical features of intellectual disability, skin gummas, scarring, hearing deficits, and skeletal abnormalities (49).
The American Academy of Pediatrics and the American College of Obstetricians and Gynecologists recommend universal screening of all women early in pregnancy, then at delivery and after exposure to an infected partner (06). Additionally, screening in the beginning of the third trimester is recommended for high-risk pregnant women, such as those who use illicit drugs, and for women in areas of high syphilis prevalence. Both the American Academy of Pediatrics and American College of Obstetricians and Gynecologists recommend the use of nontreponemal screening tests (VDRL or RPR) initially, followed by a confirmatory test using treponemal antibody test if the VDRL or RPR is positive. Repeat screening in the first and third trimester results in fewer maternal and neonatal adverse outcomes and is both cost-effective and results in improvement of outcomes (47). These data support updated screening guidelines, moving toward repeat screening as the standard of care.
Although rare, congenital syphilis should be considered in the differential diagnosis of nonimmune fetal hydrops (due to fetal anemia), which, in severe cases, can result in stillbirth or neonatal death. Doppler flow studies showing increased peak systolic velocity in the middle cerebral artery strongly suggest fetal anemia, the severity of which can then be confirmed by cordocentesis. Chen and colleagues reviewed the published cases of syphilitic nonimmune hydrops and reported a successful outcome with intrauterine transfusion in a case of nonimmune hydrops due to congenital syphilis (26).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Child Neurology
Jun. 24, 2026
General Child Neurology
Jun. 10, 2026
Epilepsy & Seizures
Jun. 02, 2026
General Child Neurology
May. 12, 2026
Epilepsy & Seizures
May. 08, 2026
General Child Neurology
Apr. 29, 2026
General Child Neurology
Apr. 29, 2026
General Child Neurology
Apr. 24, 2026