

Sleep Disorders
Sudden infant death syndrome
Jul. 05, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Epilepsy with generalized tonic-clonic seizures alone (GTCA) is likely a syndrome of idiopathic/genetic generalized epilepsy of uncertain boundaries. Onset usually occurs in late adolescence, and genetic predisposition is common. Generalized tonic-clonic seizures (GTCS) occur at any time, but mainly on awakening, and particularly after sleep deprivation and excessive alcohol consumption. By definition, other types of generalized seizure, such as absences or myoclonic jerks (characteristic mainly of juvenile myoclonic epilepsy), are not part of this syndrome, though this is debated. The EEG usually shows asymptomatic 3 to 4 Hz generalized spike/polyspike discharges, but often video-EEG after partial sleep deprivation with recording in sleep and awakening is needed. Differential diagnosis is demanding for the exclusion of nonepileptic attacks and focal onset tonic-clonic seizures. Prognosis is markedly variable, from excellent in mild cases to severe with continuing GTCS becoming more frequent and less dependent on the sleep-waking cycle and precipitating factors. Patients usually violate the precipitating factors and do not comply with medication because of certain personality traits. Prophylactic treatment, mainly with sodium valproate, levetiracetam, or lamotrigine, is effective.
• Epilepsy with generalized tonic-clonic seizures alone is likely a syndrome of idiopathic/genetic generalized epilepsy but of uncertain boundaries. | |
• Generalized onset tonic-clonic seizures may occur at any time, though those happening after awakening are more characteristic and better studied. | |
• Precipitating factors such as sleep deprivation and overconsumption of alcohol are significant; some patients may never have GTCS in the absence of these triggers. | |
• Other types of generalized seizures, such as absences or myoclonic jerks, are not part of this syndrome, but this is debated. | |
• Differential diagnosis is often difficult without an appropriately performed and assessed video-EEG. | |
• Prognosis varies from excellent to severe with lifelong continuing GTCS. | |
• Response to antiepileptic drugs, usually monotherapy with sodium valproate, levetiracetam, or lamotrigine, is commonly excellent. | |
• Avoidance of precipitating factors is the most significant part of management, but this is often violated because of certain personality traits. |
The manifestations of generalized tonic-clonic seizures (GTCS) are so dramatic that their accurate descriptions can be found as early as 1050 BC in the twenty-fifth Babylonian cuneiform tablet devoted to miqtu (a disease in which the person loses consciousness and foams at the mouth) (09). A realistic depiction of GTCS, including marked cyanosis, can be seen in the painting of Saint Ignatius of Loyola exorcising (1617) by Peter Paul Rubens (1577-1640) (76).
That seizures can be related to sleep was already known to Aristotle:
Hence, also they are subject to epileptic seizures; for sleep is like epilepsy, and, in a sense, actually is a seizure of this sort. Accordingly, the beginning of this malady takes place with many during sleep, and their subsequent habitual seizures occur in sleep, not in waking hours. (Aristotle: On Sleep and Sleeplessness 350 BC; http://classics.mit.edu/Aristotle/sleep.html). |
From the mid-nineteenth century, when all epilepsies were recognized as originating in the brain, GTCS (grand mal) were considered the cardinal manifestation of genuine or idiopathic epilepsy due to a predisposition to have seizures. This predisposition was believed to be associated only with generalized convulsions (24).
Gowers first mentioned that in 5% of his patients, attacks occurred only in the early morning (28). Langdon-Down and Brain divided their patients into those with diurnal, nocturnal, and diffused seizures. For the diurnal group, the most important peak was shortly after awakening (41). Hopkins found that seizures of 302 outpatients occurred in two main peaks: during sleep (about half of all patients) and in the period of awakening (defined as the first hour after arousal from sleep; about two thirds of all patients). The remaining patients had diurnal seizures any time “from the end of the awakening period to the resumption of sleep” (32). Griffiths and Fox found that of 104 institutionalized patients, 38.5% were “night-fitters,” 37.5% “day-fitters,” 10.5% “rising-fitters,” and 13.5% “diffused” (30; 33; 45; 50; 74; 75).
The most thorough and systematic study of the relation of GTCS to the sleep-waking cycle is by Janz (Janz 1953; 33). In his classical report, he makes an exhaustive review of the literature and masterfully analyzes his own data, concluding that:
Under this aspect, three types of course may be described: (1) grand mal epilepsies with attacks predominantly following waking and during the period of relaxation following work ("Feierabend"), the so-called awakening epilepsies; (2) grand mal epilepsies with attacks mainly after falling asleep or before waking, the so-called sleep epilepsies; (3) grand mal epilepsies with irregular dispersed attacks, the so-called diffuse epilepsies. As a rule these types remain constant even in cases of considerable duration. Transitions occur from awakening epilepsy to sleep epilepsy or to diffuse epilepsy and from sleep epilepsy to diffuse epilepsy, but not vice versa” (33). |
Of 1051 patients with “pure grand mal seizures only (no other types of seizure),” 30% occurred on awakening, 50% occurred in sleep, and 20% were random (33). His report examines all types of GTCS in their relation to awakening, sleep, or no particular circadian distribution, though it is better known and cited for “epilepsy with grand mal on awakening” to which he also devoted subsequent papers (35; 36). The most elaborate sleep investigations were made on this syndrome by Billiard (08).
Classification and nomenclature. The 1989 ILAE proposal recognized an epileptic syndrome of “Epilepsy with generalized tonic-clonic seizures on awakening” (or “epilepsy with grand mal on awakening”); they classified it amongst the idiopathic generalized epilepsies and defined it as follows:
Epilepsy with generalized tonic-clonic seizures on awakening is a syndrome with onset occurring mostly in the second decade of life. The GTCS occur exclusively or predominantly (more than 90% of the time) shortly after awakening regardless of the time of day or in a second seizure peak in the evening period of relaxation. If other seizures occur, they are mostly absence or myoclonic, as in juvenile myoclonic epilepsy. Seizures may be precipitated by sleep deprivation and other external factors. Genetic predisposition is relatively frequent. The EEG shows one of the patterns of idiopathic generalized epilepsy. There is a significant correlation with photosensitivity (15). |
The ILAE Task Force in 2001, based on a review by Andermann and Berkovic (04), abandoned the term “epilepsy with GTCS on awakening” and instead proposed a syndrome of “epilepsy with generalized tonic-clonic seizures only” (with GTCS only irrespective of circadian distribution) and classified it amongst “idiopathic generalized epilepsies with variable phenotypes”:
• Juvenile absence epilepsy |
“Epilepsy with GTCS only” included:
- Seizures on awakening |
Later, the ILAE Core Group revised its position and did not recognize it as a separate syndrome:
Epilepsy with GTCS only is not a syndrome, and the Core Group was unable to agree on any syndrome with this feature; the consistent diurnal pattern of seizures in some patients needs further investigation. Whether epilepsy with GTCS on awakening exists as a distinct entity is unclear (21). |
“Epilepsy with generalized tonic-clonic seizures alone” is the modified name used by the latest reports of the ILAE Commission, and it is listed amongst electroclinical syndromes of “adolescence – adult onset” together with juvenile absence epilepsy, juvenile myoclonic epilepsy, progressive myoclonus epilepsies, autosomal dominant epilepsy with auditory features, and other familial temporal lobe epilepsies (07). The current epilepsy manual of the ILAE Commission clarifies that “epilepsy with GTCS alone” means that seizures other than GTCS types of seizure are not allowed in this syndrome. If seizures other than GTCS types of seizure are allowed to be present, then the “epilepsy with GTCS alone” should be renamed to “epilepsy with predominant GTCS” (40). Such broadening of seizure types would cause significant overlapping with other syndromes of idiopathic generalized epilepsies and mainly with juvenile myoclonic epilepsy or idiopathic epilepsy with phantom absences (53). However, it is not clarified whether the proposal of Janz that six GTCS are required for making the diagnosis of epilepsy with GTCS on awakening (35) is practical, considering that most patients may have fewer than six seizures (in their lifetime) with appropriate treatment and avoidance of triggering factors (04) (see clinical vignette). Furthermore, there are some reports indicating that epilepsy with GTCS on awakening may be different from that with GTCS occurring randomly (29; 19; 67). Thus, the recognition and boundaries of epilepsy with GTCS alone may still be far from final dissolution.
In the 2014 ILAE epilepsy diagnosis manual, epilepsy with generalized tonic-clonic seizures alone is classified as a genetic epilepsy syndrome of adolescents/adults (14). The complete description of epilepsy with generalized tonic-clonic seizures alone is as follows:
This syndrome (previously known as epilepsy with grand mal seizures on awakening) is a common genetic generalized epilepsy. Individuals have infrequent generalized convulsive seizures from the second decade of life, typically provoked by sleep deprivation.
Note. A genetic generalized epilepsy is an epilepsy with generalized seizures associated with generalized epileptiform EEG patterns, such as generalized spike wave activity. |
Clinical context. This syndrome is characterized by the onset of generalized convulsive seizures between the ages of 5 and 40 years (peak 11 to 23 years, 80% of cases have their first convulsion in the second decade). Seizures may be frequent, with one fifth of cases having more than one seizure per month prior to treatment. Treatment is required for life. Sleep deprivation, fatigue, and alcohol lower the threshold for seizures. Antecedent and birth history are normal, although there are patients with a previous history of childhood absence epilepsy. Neurologic examination and head size are normal. Development and cognition are typically normal.
Mandatory seizures. Generalized convulsive seizures are mandatory for this epilepsy syndrome, predominantly/exclusively occurring on awakening (within 1 to 2 hours, although also seen from awake or sleep states).
Exclusionary. All other seizure types. |
EEG Background. The EEG background is normal.
Caution. Generalized slowing is not seen. | |
Caution. If focal slowing is seen consistently over one area, consider a structural brain abnormality. |
Interictal. Generalized spike-and-wave or polyspike-and-wave is seen in the interictal EEG. Half of the patients have these abnormalities only in sleep.
Caution. Although focal spike-and-wave can occur, if seen consistently in one area, consider a structural brain abnormality. | |
Caution. If slow spike-and-wave (< 2.5 Hz) is not seen, consider other epilepsy syndromes. |
Activation. An intermittent photoparoxysmal response to photic stimulation may be seen.
EEG abnormality is enhanced by sleep deprivation and during sleep. Generalized spike-and-wave often becomes fragmented with sleep deprivation or during sleep. Fragmented generalized spike-and-wave can appear focal or multifocal but is usually not consistently seen in one area. The morphology of the focal spike-and-wave typically appears similar to the generalized spike-and-wave.
Ictal. With generalized convulsive seizures, the ictal EEG is often obscured by artifact. Generalized fast rhythmic spikes are seen in the tonic stage. Bursts of spikes and after-coming slow waves are synchronous with clonic jerks. A postictal period of irregular slow activity follows.
Imaging. Neuroimaging is normal.
Genetics. It has a complex inheritance. Known genes linked to this syndrome include CLCN2 and others.
Family history of seizures/epilepsy. A family history of epilepsy is common (in 20%, commonly the same epilepsy syndrome). A family history of febrile seizures is reported in around 10% of cases.
• Genetic epilepsy with febrile seizures plus |
Note on nomenclature. The 2010 ILAE report has recommended that some terms used in this article, such as idiopathic, symptomatic, and cryptogenic, should be replaced with the terms genetic, structural-metabolic, and unknown, respectively (07). However, healthcare professionals are still more familiar with the “older” terms. Furthermore, the updated terminologies have not been widely accepted; idiopathic is not equated with genetic, and cryptogenic is more specific than unknown (53). A striking example of these difficulties is “idiopathic generalized epilepsies,” which cannot be replaced with the term “genetic generalized epilepsies.” It is for this reason that the 2017 position paper of the ILAE Commission for Classification and Terminology (60) stated that:
There has been, however, considerable desire to retain the term idiopathic generalized epilepsy. The Task Force has therefore decided that the term idiopathic generalized epilepsy will be acceptable specifically for the group of four epilepsy syndromes: Childhood Absence Epilepsy, Juvenile Absence Epilepsy, Juvenile Myoclonic Epilepsy, and Generalized Tonic-Clonic Seizures Alone. In individual cases, the term Genetic Generalized Epilepsy may be used where the clinician is comfortable with invoking a genetic etiology. |
The 2022 position paper of the ILAE Task Force on Nosology and Definitions groups GTCS within Idiopathic Generalized epilepsies, but separately from the others that also contain absence seizures and myoclonic seizures (31).
Epilepsy with GTCS alone, by definition, occurs in people with a normal neurocognitive state and manifests only with GTCS that stand alone without any other types of seizure. These are generalized onset tonic-clonic seizures.
Their true prevalence of epilepsy with GTCS alone, according to the circadian distribution of GTCS, may be higher on awakening than in sleep or randomly occurring (67; 39). However, the classical report of Janz described that of 1051 patients with “pure grand mal seizures only (no other types of seizure),” 30% occurred on awakening, 50% occurred in sleep, and 20% were random GTCS (33).
Epilepsy with GTCS on awakening. By definition, these patients suffer exclusively from GTCS, which happen within the first 2 hours after awakening while the patient is in bed, in the bathroom, during or after breakfast, at home, or on the way to work (33); this is regardless of the time of the day, provided that it occurs on awakening. Most of the patients may also have GTCS in a second peak during the evening when relaxing (leisure time). According to Janz, a definite diagnosis of pure epilepsy with GTCS on awakening requires that at least six seizures have occurred predominantly during awakening or during relaxation (35). In some cases, seizures during sleep may develop over time and may even be predominant in the later course (37).
|
Either right from the outset or in the course of time a second attack peak develops, which is situated in the late afternoon or early evening according to the time of day, but from the point of view of its biological nature it is better termed the evening peak ("Feierabend-Gipfel") -- that is, a peak occurring after cessation of labour. Rising as such, and therefore the disturbance of postural reflexes, cannot be held responsible for the tendency of attacks to occur after waking, since patients can have attacks just as well while they are still in bed shortly after waking -- although less frequently -- as one to two hours after rising. In many cases an attack which does not begin until several hours after waking still has to be taken as an attack on awakening if the time between awakening and the beginning of a major attack is bridged by a series of minor attacks. The fact that waking up is decisive and not the time of day is underlined by the tendency of such patients to have attacks also after an afternoon nap. An attack not occurring in the late afternoon must also be interpreted as an evening attack if the situation immediately preceding it has the appearance of relaxation after activity (33). |
GTCS during sleep. Epilepsy with GTCS alone may manifest with GTCS occurring predominantly or exclusively during night or day sleep. They are more common within the first or second hour after going off to sleep (early nocturnal seizures) and 1 to 2 hours before the usual time of awakening (early morning seizures).
|
In sleep epilepsies not all the time spent in sleeping shows the same propensity for attacks. When the times are analyzed, two peaks become apparent…. The first peak occurs soon after falling asleep and the second in the early morning period of sleep… A single peak is unusual in the course of the disease. In individual cases the attacks usually occur on both occasions, even if not with equal frequency. Sleep epilepsy cases with one accentuated peak in the morning sleep are more common than cases where attacks occur mainly after falling asleep. The ratio which we determined from a small series of 76 sleep epilepsy patients is about 83% - 18% … patterns with a major peak after falling asleep more frequently tend also to have attacks during the afternoon nap than patterns with a late peak (33). |
GTCS occurring randomly without any particular circadian distribution. GTCS occur randomly any time of day or night, awake or asleep. In a study of 30 patients with random GTCS compared to 90 patients with GTCS on awakening, statistically significant differences occurred in relation to (a) the median duration of epilepsy, which was found shorter (2.0 vs. 9.5 years, p = 0.012) in epilepsy with random GTCS and (b) precipitating factors, which were found only in 10% (p=0.001) of patients with random GTCS (67).
Other than GTCS epileptic seizures. By name, in “epilepsy with GTCS alone,” GTCS should be the only type of seizures (14). However, in most reports of epilepsy with GTCS, either on awakening, in sleep, or randomly, patients who have absences or myoclonic jerks that usually occur immediately prior to a GTCS are included.
The incidence of preceding febrile seizures is 6% to 13% (67), or 10% according to the ILAE Commission.
Of 18 patients with epilepsy with GTCS alone, convulsive status epilepticus happened in one and absence status epilepticus in four patients (though none of these four patients had documented absence seizures) (39).
Precipitating factors. Precipitating factors, similar to those found in juvenile myoclonic epilepsy, occur exclusively in patients with GTCS on awakening. They are inconsistent or not found in the majority of patients with GTCS in sleep or those that occur randomly (33; 67).
Typically, GTCS on awakening happens after sleep deprivation, excessive alcohol consumption, stress, fatigue, and untimely sudden awakening. Shift work, changes in sleep habits (particularly during holidays), examinations, and celebrations predispose to GTCS on awakening.
|
Deprivation of sleep, especially combined with consumption of alcohol, and sudden awakening can therefore be considered as specifically provocative of attacks in epilepsies on awakening …We have described in detail elsewhere how the time of the attacks in the course of epilepsies on awakening is often determined for years only by such impulses and how the rhythm of the so-called Monday or holiday attacks (New Year, Carnival, birthdays and public holidays) is solely dependent on such occasions for excesses, or on emergencies during wartime (air raids), or on excessive examination preparations until well into the night (33). |
EEG photosensitivity is found in 13% (73) to 28% of patients (39) with epilepsy with generalized tonic-clonic seizures alone. Some of these patients also have clinical photosensitivity as a main precipitating factor (49; 69).
Age at onset and sex. The age of onset varies widely for “epilepsy with generalized tonic seizure alone” (33):
|
• Epilepsy with GTCS on awakening starts between the ages of 12 and 18 years, and in over three quarters (77%), starts between 10 and 25 years of age; only 11% begin in those over the age of 30 years (33). | |
|
• Epilepsy with GTCS in sleep probably does not have a particular age at onset; it starts between 12 and 18 years of age in one fifth of patients, between 10 and 25 years in less than half, and after 30 years of age in one third of patients. | |
|
• Also, epilepsy with random GTCS may not have a particular age at onset. | |
|
• Overall, it is assessed that epilepsy with GTCS alone starts 2 years later than juvenile myoclonic epilepsy (06; 70). |
In one report, the mean age at seizure onset was 16.6 years (±6.3 S.D., range: 5-41) for 68 patients with GTCS on awakening and 16.7 years for 30 patients with random GTCS (±7.5 S.D., range: 4-42) (67). In a report, the onset of GTCS was at a median of 18 years, ranging from 14.5 to 27 years (70).
Caraballo and associates reported epilepsy with generalized tonic-clonic seizures alone during childhood and discussed its validity as a separate syndrome of childhood (11). These were children with at least two unprovoked GTCS between 3 and 11 years of age, no other seizure types at diagnosis, normal psychomotor development, and neurologic examination, an EEG with normal background, paroxysms of generalized spikes and waves with a frequency of 2.5 Hz or above, and an unknown cause for epilepsy. Over a 12-year period (2005 to 2017), 26 patients met the inclusion criteria of epilepsy with GTCS only. Mean age at onset was 5 years. The seizures occurred while awake in 16 patients, on awakening in two, and during sleep in eight patients. The duration of seizures was around 3 minutes. Generalized spike-and-wave discharges were observed in all patients when awake and during sleep in eight and 26 patients, respectively. Nineteen responded well to valproic acid or levetiracetam. Antiepileptic treatment was discontinued in 16 patients who remained seizure-free over a period of 2 to 9 years of follow-up (11). Men (55%) are slightly more affected than women (45%). The male-to-female ratio amongst 88 cases with pure epilepsy with GTCS on awakening was 1.8 (35). Also, 1.6 was the male-to-female ratio amongst 57 patients with epilepsy with GTCS alone, including randomly occurring GTCS (70). This male prominence may be attributed to differences in alcohol exposure and sleep habits (37).
Personality characteristics. Janz described patients with epilepsy with GTCS on awakening as unreliable, unstable, and prone to neglect (33; 35), a notion supported by a psychological evaluation (42).
|
They are distinguished rather by a tendency towards instability and thoughtlessness, by being easily influenced and led astray, by a lack of endurance and ambition, by grandiosity, laziness, sometimes also by megalomania and boastfulness which can lead to pseudologia in extreme cases. They are violent in their emotions, tend towards transient capricious bad moods, but can be easily pacified again. Realizing that they are at a disadvantage with ordinary, hard-working people, they often react with distrust, jealousy and obstinacy, so that their behavior may often seem infantile. Their moments of despair never last very long, and neither does their remorse. We only know of one patient with epilepsy on awakening who committed suicide in a moment of real despair. They are indifferent to themselves and their health and so there is no hypochondria amongst them, but this indifference often makes therapy, which must be intent on regularizing their way of life, difficult (33). |
Epilepsy with GTCS on awakening is largely influenced by external factors, alcohol, and sleep deprivation, which may be avoidable or self-inflicted. There are patients who remain seizure-free after adjusting their lifestyles and their jobs.
Sleep patterns. The sleep patterns of patients with epilepsy with GTCS on awakening are particularly unstable and modifiable by external factors (ie, antiepileptic drugs), and the patients may suffer from chronic sleep deficit (74; 35; 36).
Prognosis is uncertain in this syndrome as a whole. There are significant variations from very mild to very severe forms. In mild forms, patients have one or a few GTCS, probably under extreme precipitating factors. See, for example, the “mild form of idiopathic generalized epilepsy characterized by infrequent GTCS and generalized interictal EEG discharges of spike wave” (57). In severe forms, GTCS are frequent and lifelong. Characteristically, the interval between seizures becomes shorter with time and the precipitating factors less obvious. The GTCS may become more obvious and random and may also occur during sleep (35; 37). However, even in relatively severe cases, GTCS control improves with age, and seizure remission is achieved after the fourth decade of life, even after antiepileptic drug withdrawal (70).
In a report on epilepsy with GTCS alone, only half of the patients had more than six GTCS (10% had a single GTCS) during the observed life span (67). In another report, the lifetime number of GTCS ranged from 1 to 50 (mean 13) with an annual GTCS frequency ranging from 0.1 to 4 (mean 1/year) (39). In a Canadian study of 40 children with “idiopathic generalized epilepsy with only generalized tonic-clonic seizures,” all were neurologically and intellectually normal with generalized spike-wave on EEG. Follow-up averaged 22.2±7.6 years. Twenty-seven (75%) had a complete terminal remission (seizure-free, off medication) for 16.1±8.6 years. There were no deaths or intractable seizures. For those older than 21 years of age at follow up (N=30), major adverse social outcomes were psychiatric diagnosis for eight (27%), no high school graduation for 12 (40%), pregnancy outside a stable relationship for 11 (38%), living alone for seven (23%), unemployment for 10 (33%), and criminal conviction for two (7%). Satisfaction with their lives, friendships, and social activities were reported by 55% to 65% (10). The authors concluded that this syndrome “is a recognizable, relatively benign epilepsy syndrome with complete remission in 75%. Learning problems and unsatisfactory social outcomes are unfortunately common” (10).
A retrospective study aimed to compare long-term seizure outcomes in juvenile absence epilepsy, juvenile myoclonic epilepsy, and epilepsy with generalized tonic-clonic seizures alone (70). Charts of 870 outpatients with epilepsy from the Epilepsy-Center Berlin-Brandenburg in Germany were reviewed, among whom 176 had adolescent-onset idiopathic generalized epilepsy (53 juvenile absence epilepsy, 66 juvenile myoclonic epilepsy, and 57 epilepsy with generalized tonic-clonic seizures alone). Median patient age at investigation was 60 years; median follow-up time was 42.5 years. If possible, patients were additionally interviewed on psychosocial and clinical variables. Age at first seizure was significantly higher in patients with epilepsy with generalized tonic-clonic seizures alone (median 18 years) than in patients with juvenile absence or juvenile myoclonic epilepsy (14 years each). Long-term seizure outcomes hardly differed among the three subsyndromes. At the end of follow-up, 60% of all patients were in 5-year terminal seizure remission, and in 14%, epilepsy had resolved—that is, these patients were more than 10 years without seizures and more than 5 years without pharmacotherapy. Twenty percent of all patients had persistent seizures of any type and 11% had GTCS during the last year of follow-up. Across all patients, 23% reported a psychiatric comorbidity, 87% had married, and 57% had achieved university entrance qualification. Thus, long-term outcome is highly similar across all subsyndromes of adolescent-onset idiopathic generalized epilepsy (70).
Gomez-Ibanez and colleagues aimed to identify prognostic factors for drug resistance in patients with idiopathic generalized epilepsy of adult onset (27). Drug-resistant epilepsy was defined as a failure of adequate trials of two tolerated and appropriately chosen and used antiepileptic drug schedules. Patients were classified as either drug-resistant or drug-responsive. Of 279 patients, 122 were drug-resistant, 105 drug-responsive, and 52 were undefined and excluded from the analysis. After multivariate analysis, early seizure onset (age < 13 years), long-time epilepsy, several generalized seizure types, status epilepticus, EEG with generalized epileptiform activity, mainly polyspikes, and side effects with antiepileptic drugs were assessed as poor outcome factors. Additionally, 50.6% identified modifiable seizure triggers. Regarding syndromes, epilepsy with generalized tonic-clonic seizures alone had the same factors as other syndromes, except several seizure types; presence of additional GTCS, polyspikes, history of antiepileptic drugs side effects, and psychiatric disorder were poor factors for absence epilepsy; only psychiatric comorbidity revealed significance in juvenile myoclonic epilepsy.
Sudden unexpected death in epilepsy (SUDEP) has not been studied in this syndrome, but considering that GTCS is the most common seizure type associated with SUDEP (22), the risk of SUDEP may be a realistic possibility and should be assessed carefully in order to prevent it (71).
The following clinical vignettes show the marked variability of epilepsy with GTCS alone.
Case 1: a typical case with GTCS on awakening without EEG spike-wave discharges. A 20-year-old technician presented to the accident and emergency department following a mild head injury caused by a GTCS. This occurred at 9 am as he was getting ready for work. He had been at a wedding the previous night, had become intoxicated, and had slept for only 2 hours. Six previous GTCS had occurred since the age of 16 years; five of them happened within half an hour of awakening, when he was sleep-deprived and intoxicated. The remaining GTCS occurred late in the afternoon while he was relaxing, watching television after a successful job interview.
His EEG, including a video-EEG during sleep and awakening, showed some non-specific brief bursts of theta activity without spikes. He complied poorly with his medication, phenytoin and sodium valproate, was a heavy drinker, and frequently stayed out late. His maternal half-sister had an interesting form of occipital lobe epilepsy with occipital photosensitivity and infrequent visual seizures with secondary generalization occurring mainly during sleep (01). His father had epileptic seizures, but no more details were known.
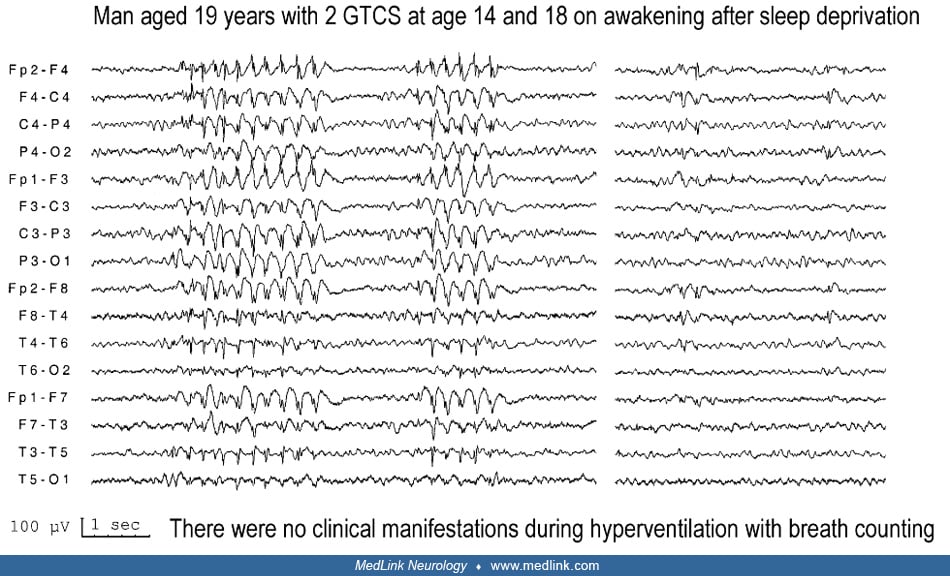
Case 2: a typical case with GTCS on awakening with asymptomatic spike-wave EEG discharges. A Cambridge University graduate celebrated his 23rd birthday with an all-night party and many alcoholic drinks. He woke up after 2 hours of sleep, and within half an hour, had a GTCS. A reliable witness described no absences or jerks preceding the GTCS. In the previous 4 years, he had experienced two GTCS on awakening under similar conditions of sleep deprivation and alcohol drinking. He considered these episodes to be self-inflicted and did not want regular medication but accepted our advice to take sodium valproate 2000 mg if he felt at risk.
His video-EEG after partial sleep deprivation showed brief, up to 3 seconds, high amplitude discharges of 3 to 4 Hz small spikes and slow wave on awakening. There were no clinical manifestations during these discharges, and breath-counting failed to detect any overt cognitive impairment.
Case 3: a case of midday GTCS after strong precipitating factors. A 21-year-old first-year student in Oxford University had two GTCS (September 2010 and March 2011) that occurred under identical precipitating factors. Both GTCS occurred at around lunch time, 4 to 5 hours after awakening. On both occasions, she went to bed late at night after an excessive consumption of alcohol, and she had only a few hours of sleep. There was no evidence of myoclonic jerks or absences. There was no family history of epilepsy or any significant illnesses. An EEG after partial sleep deprivation showed brief bursts of generalized irregular sharp-slow wave complexes with anterior dominance and sometimes with a mild right-side emphasis. The diagnosis of epilepsy with GTCS alone was made. She was strongly advised regarding precipitating factors; she declined prophylactic medication. However, she had another GTCS in October 2011 that again was precipitated by sleep deprivation. She was out with friends, had three pints of beer, and went to sleep at around 4 am. She woke up at 8 am to participate in team athletic activities. The GTCS occurred in the changing room at around 2 pm. Treatment with levetiracetam was initiated, but this induced depression, which she never had before, and which resolved 2 weeks after discontinuation of medication. No further seizures occurred in the following 8 months.
Case 4: a case with nocturnal GTCS only. A 19-year-old student and rugby player had three GTCS during sleep at age 15 years, within 1 month. There were no specific precipitating factors. He had normal neurocognitive development without a history of febrile convulsions or other seizures. A maternal uncle had epilepsy. EEG showed high-amplitude bifrontal slow waves and occasional nonlocalizing spike transients superimposed on the slow waves during sleep. No further seizures occurred in the next 4 years while on sodium valproate 500 mg twice daily, and he was driving.
Case 5: a case with diurnal GTCS of late onset and generalized spike-wave EEG discharges. A 62-year-old otherwise healthy gentleman had two diurnal GTCS at age 59 and 62 years of age at his workplace. There were no specific precipitating factors. Brain MRI was normal, but EEG showed several bursts of generalized, irregular spike and slow wave activity without clinical manifestations.
Case 6: a typical case of epilepsy with phantom absences and GTCS. A 25-year-old woman reported that she’d experienced a single brief and uncomplicated febrile convulsion at age 3 years. At 17 years of age, she had a GTCS in the afternoon while talking to her teacher. There were no preceding symptoms or apparent precipitating factors. On appropriate questioning, she was adamantly clear that she was not aware of myoclonic jerks or absences. A video-EEG 10 days later documented phantom absences.
Treatment with sodium valproate1000 mg daily was initiated, but she had another GTCS again in the afternoon hours 5 days after stopping her medication. She was well and free of seizures for the next 7 years of follow-up on treatment with sodium valproate. Video-EEGs showed brief asymptomatic discharges of spike or multiple spike-wave.
Epilepsy with GTCS alone is probably genetically determined of complex inheritance associated with CLCN2 and other genes; a family history of epilepsy is common and in 20%, the same epilepsy syndrome (14).
Epilepsy with GTCS on awakening. Approximately 12.5% of cases have a family history of epilepsy (37). In a study of 10 patients in whom the diagnosis of the affected relatives could be ascertained, the diagnoses were: epilepsy with GTCS seizures on awakening in one, absence or juvenile myoclonic epilepsy in four, and only isolated seizures (ie, a mild manifestation of risk, possibly idiopathic generalized) in another four. Only one relative had a diagnosis of neonatal seizures, which did not belong to the idiopathic generalized epilepsies (37).
One family with photosensitivity and epilepsy with GTCS on awakening has been reported (49).
There is a genetic relationship between epilepsy with GTCS on awakening and other idiopathic generalized epilepsies, such as juvenile myoclonic epilepsy or childhood or juvenile absence epilepsy, as more than one phenotype may occur in the same family (17).
Epilepsy with GTCS alone. In one study, GTCS were detected in 32% of the affected first-degree relatives (67). Other syndromes of idiopathic generalized epilepsy (childhood absence epilepsy, juvenile absence epilepsy, and juvenile myoclonic epilepsy) were less frequent (14%). A considerable number of affected relatives of patients had febrile seizures (45%), but only one of them developed epilepsy with GTCS alone.
In another study, a family history of epilepsy was detected in 28% of first-degree relatives amongst 18 patients with epilepsy with GTCS alone (39).
Molecular genetic studies. Durner and associates found evidence for linkage to chromosome 8 in adolescent-onset idiopathic generalized epilepsy families with either “pure grand mal epilepsy (random or on awakening)” or juvenile absence, but not for juvenile myoclonic epilepsy (19). The same group of authors had previously reported that:
|
… pure adolescent-onset grand mal epilepsy on awakening is linked to the EJM-1 locus and may be genetically the same as juvenile myoclonic epilepsy... No such link to EJM-1 locus was found for adolescent-onset grand mal epilepsy in which the seizures occur at any time during waking (29). |
Other pathogenetic considerations. Meencke and Janz found marked microdysgenesis with varying regional distribution in the brains of seven of eight people with epilepsy with GTCS on awakening who came to autopsy (48). Observations included increased nerve cell density in the stratum moleculare, indistinct boundary between lamina 2 and stratum moleculare, protrusion of nerve cells into the pia mater, increased number of nerve cells in white matter, disorganized columnar cortical neuronal architecture, and Purkinje cell dystopia. Because migration of nerve cells and layer organization occur between the seventh embryonic month and the neonatal period, disturbance in that period may be implicated in the pathogenesis. Microdysgenesias of this type are also seen in other forms of epilepsy and may be a nonspecific marker for epileptogenic predisposition.
Yang and colleagues examined the resting state of functional connectivity between the two hemispheres and its relationships with clinical characteristics in idiopathic generalized epilepsy with generalized tonic-clonic seizures using a technique called "voxel-mirrored homotopic connectivity (VMHC)" (77). Compared to the controls, the patients with IGE-GTCS showed significant increases in VMHC in the bilateral anterior cingulate and medial prefrontal gyrus. No areas showed decreased VMHC in patients. Moreover, the VMHC in the bilateral thalamus, orbital frontal cortex, and cerebellum showed significant negative correlations with the illness duration. The authors concluded that their findings provide preliminary evidence of increased interhemispheric resting state functional connectivity in patients with IGE-GTCS during the interictal period. The VMHC deficits in these regions and the inverse relations between VMHC and clinical characteristics may play an important role in the pathophysiology of IGE-GTCS (77).
Callosal morphology was studied with T1-weighted data on a 3T MRI scanner in a well-matched sample of 22 patients with juvenile myoclonic epilepsy—15 patients with generalized tonic clonic seizures, and 42 controls (03). Significant differences between patients with juvenile myoclonic epilepsy and controls were observed within the callosal genu, anterior midbody, and isthmus, with thinner regions in patients with juvenile myoclonic epilepsy. There were no significant differences between patients with generalized tonic clonic seizures and controls.
In one study, Liu and colleagues reported state-specific functional network connectivity disruptions in patients with idiopathic epilepsy with generalized tonic clonic seizures, and the majority of aberrant functional connectivity manifested itself in the default mode network (43). In addition, temporal metrics derived from state transition vectors were altered in patients, including the total number of transitions across states and the mean dwell time, the fraction of time spent, and the number of subjects in a specific functional network connectivity-state. Furthermore, the alterations were significantly correlated with disease duration and seizure frequency. It was also found that dynamic functional network connectivity could distinguish patients from controls with an accuracy of 77.91% (P< 0.001) (43).
A study found abnormalities in spontaneous activity in the gray and white matter tracts as documented with diffusional kurtosis imaging and regional homogeneity in patients with genetic/idiopathic generalized epilepsy with generalized tonic-clonic seizures (44). Compared with healthy controls, patients exhibited markedly increased regional homogeneity in the bilateral putamen, the thalamus, right pallidum, right supplementary motor area, and the bilateral paracentral lobules; they also exhibited markedly decreased regional homogeneity in the posterior cingulate/precuneus, left angular gyrus, and dorsolateral prefrontal cortex. Diffusional kurtosis imaging revealed lower fractional anisotropy in the left anterior/superior corona radiata, left superior longitudinal fasciculus, and genu/body of the corpus callosum. Higher mean diffusivity was detected in the bilateral anterior corona radiata, left superior corona radiata, left cingulum, and genu/body/splenium of the corpus callosum. Furthermore, reduced mean kurtosis values were identified over the bilateral superior/posterior corona radiata, left anterior corona radiata, right superior longitudinal fasciculus, left posterior thalamic radiation, and the genu/body/splenium of the corpus callosum (44).
The pathophysiology of “generalized onset tonic-clonic seizures” is detailed in the relevant clinical summary.
Prevalence of epilepsy with GTCS alone varies significantly according to the criteria used and investigative procedures. The reported prevalence of epilepsy with GTCS on awakening is from 0% (47) to as high as 17% of patients with epileptic seizures (34).
Janz found "pure" epilepsy with GTCS on awakening (ie, GTCS only) in 10% and mixed GTCS with absences or myoclonic jerks or other seizures in 17% of 4816 patients (34). Schmitz and Wolf reported a prevalence of 4.6% in 699 hospital patients (61). Loiseau and associates found a prevalence of 2.1% in 570 patients of his private practice but none amongst 263 patients seen in the hospital (46). Roger and associates found that of 253 patients with idiopathic generalized epilepsy, 30 (12%) had epilepsy with GTCS on awakening, and 39 (15%) had “a mild form of idiopathic generalized epilepsy characterised by infrequent GTCS and generalized interictal EEG discharges of spike wave.” The authors considered that this latter group probably belongs to a mild form of idiopathic generalized epilepsy that they called “non-syndromic grand mal” (57). Oller-Daurella and Oller found that of 1033 patients with idiopathic generalized epilepsy, 138 (13%) had GTCS only with onset from 3 to after 18 years of life (Oller-Daurella and Oller 1994). Shian and Chi found a prevalence of epilepsy with GTCS on awakening of 20% amongst 71 Chinese children with idiopathic generalized epilepsy (62). Genton and associates reported that amongst 253 consecutive cases of idiopathic generalized epilepsy, 32 (15.4%) patients had rare GTCS with generalized spike-wave discharges in the interictal EEG (25). Onset of GTCS was from childhood to adulthood, and there was no particular circadian distribution of the GTCS on awakening. In a large survey of 8570 patients from 14 epilepsy centers in Lombardy, 1494 (17.4%) had an unequivocal diagnosis of idiopathic generalized epilepsy, and in 176 of these (11.8%, or 2.1% of all patients) the diagnosis was epilepsy with grand mal on awakening (52). Delgado-Escueta and associates stated that 22% to 37% of patients with idiopathic generalized epilepsies have "pure grand mal on awakening" (18). In their study of 101 patients with idiopathic generalized epilepsy beginning in adolescence, Reutens and Berkovic found that only 10 patients had GTCS alone--but neither on awakening nor in the evening period of relaxation (56). Unterberger and colleagues found a prevalence of 2.9% for epilepsy with GTCS alone amongst adult outpatients with epilepsy (67). Koutroumanidis and colleagues, in a study of mainly adult patients with epilepsy seen in St. Thomas’ hospital over 23 years, found 18 patients with epilepsy with GTCS alone (in 16 patients, GTCS were on awakening). In the same period, 15 patients with “idiopathic generalized epilepsy with phantom absences” all had GTCS (39). Conversely, in the Nova Scotia Childhood Epilepsy population-based cohort of 692 children, 40 (5.8%) had “idiopathic generalized epilepsy with generalized tonic-clonic seizures alone” (10).
Epilepsy with GTCS on awakening was not found in a community study where underdiagnosis may have occurred (47). In a genetic study of 88 families identified through a proband with adolescent-onset idiopathic generalized epilepsy, 20 probands had “GTCS as the sole seizure type” (epilepsy with GTCS alone); in 15 of these probands, GTCS were randomly occurring during the day, and in the other five probands, GTCS occurred predominantly after awakening (19).
Epilepsy with GTCS alone was most common after juvenile myoclonic epilepsy syndrome in two studies from Iran (05) and India (65).
GTCS are severe and potentially dangerous epileptic seizures. Proper advice in regard to precipitating factors, circadian distribution, and antiepileptic treatment may significantly reduce their occurrence or render the patient seizure-free. Assessing the risks and implementing the necessary safety procedures are important steps in preventing trauma and fatal accidents. The possibility of SUDEP should be discussed and considered.
The differential diagnosis should distinguish generalized onset tonic-clonic seizures of this syndrome from (1) nonepileptic paroxysmal events (functional seizures) and (2) focal onset tonic-clonic seizures (53). Subsequently, syndromic diagnosis includes differentiation mainly from other idiopathic generalized epilepsies.
The differentiation of GTCS from nonepileptic paroxysmal events is detailed in the relevant MedLink Neurology articles.
Syncope (including the long QT syndrome) and psychogenic nonepileptic attacks (functional episodes) are often the main reasons for misdiagnosis.
Generalized tonic-clonic seizures are a common feature of many idiopathic and structural or metabolic (symptomatic), focal, and generalized epilepsies. Some of these, irrespective of etiology, have a particular consistent circadian distribution. Whether GTCS are of generalized or focal onset is equally demanding and significant. The focal onset of secondarily generalized tonic-clonic seizures is not always easily recognized. Secondarily generalized tonic-clonic seizures usually manifest with preceding auras or other objective focal symptoms, but these are not always apparent, particularly if they occur in sleep or generalize rapidly. Inquiring about the existence of other minor seizures, such as absences, myoclonic jerks, or simple or complex focal seizures, is significant for diagnosis and management.
The syndromic diagnosis may be impossible for a patient with one or two GTCS irrespective of circadian distribution. However, if these are of generalized onset, a syndrome of idiopathic generalized epilepsy should be considered. Myoclonic jerks on awakening are characteristic and prominent in juvenile myoclonic epilepsy, whereas they may not exist or are minor in epilepsy with GTCS alone; precipitating factors are common in both. Typical absence seizures with severe impairment of consciousness, as in juvenile absence epilepsy, do not feature in epilepsy with GTCS alone. Idiopathic epilepsy with phantom absences is a syndrome to consider, and this appears to be different from epilepsy with GTCS alone (54; 39). See clinical vignette, case 6.
In all the above circumstances, EEG and particularly video-EEG may give the answer. Generalized discharges of spike-wave indicate generalized epilepsy though some focal abnormalities may be present. Unequivocal focal spikes indicate focal epilepsy. A routine normal EEG does not exclude a diagnosis of epileptic seizures. EEG after partial sleep deprivation with recording during sleep and awakening states may be needed (53). Brain MRI may reveal abnormalities in focal epilepsies. ECG is becoming part of a routine practice in the investigation of patients with suspected GTCS.
A detailed history is pivotal for the correct diagnosis. By definition criteria, patients are otherwise normal and all investigations other than EEG are unremarkable. However, considering the broad spectrum of differential diagnoses, ECG and brain imaging should be performed.
The EEG in epileptic syndromes, including epilepsy with GTCS alone, has been masterfully detailed in a publication by the ILAE Neurophysiology Task Force (40).
Interictal EEG. Background EEG is normal. In epilepsy with GTCS on awakening, discharges of 3 to 4 Hz spike/polyspike and wave are reported in approximately 50% of those without and 70% of those with additional absences or myoclonic jerks (74; 35). These discharges mainly consist of generalized 3 to 4 Hz spike/polyspike-wave of usually brief duration (3 to 8 seconds) without associated clinical manifestations (such as phantom absences). These are exaggerated or occur exclusively during hyperventilation. Breath-counting during hyperventilation is important in order to detect whether the discharges are associated or not with mild impairment of cognition (absence).
Focal abnormalities may be similar and as common as in juvenile myoclonic epilepsy (02) and other idiopathic generalized epilepsies (53).
Photoparoxysmal responses are reported in 13% (17% of females and 9% of males) of patients with epilepsy with GTCS on awakening (73) and 28% of patients with GTCS alone (39).
The first routine EEG may be normal in approximately 12% of patients (67), but the yield of abnormalities increases with repeat EEG and partial sleep deprivation EEG with recordings during both sleep and awakening states. There is no point in doing a sleep-deprived EEG with the recording ending before awakening (which is the more sensitive period for these patients).
Some authors consider EEG generalized discharges as a mandatory diagnostic criterion for epilepsy with GTCS only (39), but this may not apply to patients with a single routine EEG, which may be normal or show nonspecific abnormalities in nearly half of the patients.
Ictal EEG. Ictal EEG should be the same as that seen in any other generalized onset tonic-clonic seizure.
The question is whether other generalized seizures (absences or myoclonic jerks) or generalized discharges precede the onset of the GTCS. A published review includes an illustrated ictal EEG from a patient, who on long-term monitoring, had brief generalized discharges of spike and slow wave (phantom? asymptomatic?) prior to going to sleep (74). On awakening, frequent myoclonic jerks associated with generalized polyspikes preceded a GTCS by more than 30 minutes (a situation associated with juvenile myoclonic epilepsy in the so-called generalized clonic-tonic-clonic seizure).
One of the most important aspects of management is avoidance of precipitating factors. Patients should be firmly warned of the common seizure precipitants (sleep deprivation with early awakening and alcohol consumption) and, when possible, should avoid occupational night shifts. The avoidance of seizure triggers should also be stressed to friends and family members because patients may not comply with these recommendations. Therefore, patients as well as close friends and family should be seen, if possible, after every recurrence to clarify the presence of a potential trigger and re-emphasize the need for trigger avoidance. Safety measures should be strengthened in periods of increased susceptibility to GTCS, such as having a shower rather than a bath and keeping the door open when showering in the morning after awakening (68).
Prophylactic drug treatment. This is entirely empirical for this syndrome, though antiepileptic drugs effective in generalized onset tonic-clonic seizures should be used (53; 16; 64).
Older retrospective open studies suggest that phenobarbital is more effective than phenytoin or carbamazepine (74; 35). Even bromides have been found effective in pharmacoresistant cases (74). However, valproate should be avoided in persons with weight issues. In addition, bromides or phenobarbital are unlikely to be prescribed today, and carbamazepine may be contraindicated in patients with absences and myoclonic jerks, which may be exaggerated by this drug (66).
Therefore, based on its effectiveness in all types of generalized seizures, sodium valproate may be the drug of choice. A prophylactic high dose of sodium valproate in patients with GTCS alone may be effective if administered once at night when risk factors have been severely violated (53). However, sodium valproate should be firmly avoided in women of childbearing age because of the high risk of teratogenicity (see Pregnancy and epilepsy) and cognitive issues. European population-based studies have examined potential paternal effects of valproate use during spermatogenesis with conflicting results: one study reported a 1.5-fold increased risk of neurodevelopmental disorders, and another found no significant associations (12; 13). These findings are not reflected in current FDA labeling, which focuses solely on the well-established teratogenic risks of maternal valproate use during pregnancy.
Lamotrigine (26) and levetiracetam (59; 16) are probably viable options as a first choice. Add-on perampanel is effective in drug resistant cases (23; 58). Lacosamide should also be considered (16; 72). Carbamazepine add-on may be considered in cases refractory to valproate, levetiracetam, and lamotrigine (38).
However, a review of an evidence-based guide for the selection of antiepileptic drugs for patients with generalized onset tonic clonic seizures found class 1 evidence of the efficacy of only four antiepileptic drugs (lamotrigine, levetiracetam, perampanel, and topiramate) (63).
Reevaluating the need for drug therapy (in particular polytherapy), maintaining seizure control for a given period before pregnancy, and counseling about the importance of preventing GTCS might improve pregnancy outcome in women with this type of epilepsy (55).
An idea of trends in antiepileptic drug treatment for epilepsy with GTCS alone may be obtained from two relevant reports (67; 39). In the first report, 83 of 98 patients (85%) received prophylactic antiepileptic drug treatment, 59% sodium valproate either alone or in combination with other antiepileptic drugs (lamotrigine, phenobarbital, primidone, carbamazepine, phenytoin) (67). After 5 years of treatment, 65% (37 of 57) of the patients with GTCS on awakening were seizure-free compared with 77% (20 of 26) of those with random GTCS. Eleven patients (16%) with GTCS on awakening had a seizure relapse after discontinuation of drug treatment on medical advice. No treatment was initiated in 15% (15 of 98) of patients because the seizures were rare or single events (67). In the other study, five of 18 patients with epilepsy and GTCS alone declined prophylactic treatment (39). In the other 13 patients, antiepileptic drugs used were sodium valproate alone or in combination mainly with lamotrigine (eight patients); the other five patients were on carbamazepine, levetiracetam, clonazepam, clobazam, and topiramate, either alone or in combination of the two. At their last assessment after a follow-up period from 2 to 20 years (mean 9.4 years, median 8 years), seven patients were seizure-free, yielding a 60% chance for a fair outcome when patients with insufficient follow-up and those who declined treatment were excluded. EEG asymptomatic discharges of generalized discharges of spike and polyspike-wave persisted, including those who were seizure-free (39).
See Prognosis above. In epilepsy with GTCS on awakening, there is a high (83%) incidence of relapse on withdrawal of treatment (after a minimum of 2 years seizure-free). Long-term outcome does not differ between patients with GTCS on awakening or randomly (70).
Although no information is available that is specific to this syndrome and pregnancy, information is available on epilepsy and pregnancy in general.
No specific information is available. The continuity of antiepileptic drug treatment must not be interrupted by anesthesia. Parenteral administration is possible with the drugs of first choice.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Henry Hasson MD
Dr. Hasson of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See Profile
Solomon L Moshé MD
Dr. Moshé of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 05, 2026
General Child Neurology
Jun. 24, 2026
General Child Neurology
Jun. 10, 2026
Epilepsy & Seizures
Jun. 02, 2026
General Neurology
May. 13, 2026
General Child Neurology
May. 12, 2026
Neuropharmacology & Neurotherapeutics
May. 11, 2026
Epilepsy & Seizures
May. 08, 2026