



Epilepsy & Seizures
Febrile seizures
Jun. 02, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Generalized onset clonic seizures are a relatively rare type of motor (convulsive) seizure mainly affecting infants and very young children. They also occur in patients with metabolic and electrolyte derangements. Clinically, they manifest with bilateral, rhythmic clonic convulsions, with each clonic event lasting fewer than 100 ms at a repetitive rate of 1 to 3 Hz. Consciousness is usually lost or impaired. There is significant misperception in terminology and definition and particularly in their differentiation from myoclonus. In this article, the author details the clinical manifestations, pathophysiology, EEG, differential diagnosis, and management of patients with generalized onset clonic seizures.
|
• Generalized onset clonic seizures are rare and mainly affect infants and very young children. | |
|
• Generalized onset clonic seizures manifest with bilateral clonic convulsions, each lasting fewer than 100 ms at a repetition rate of 1 to 3 Hz. | |
|
• The distinction between myoclonic seizures and clonic seizures is not clear. Classically, clonic seizures are rapid rhythmically recurrent events, whereas myoclonic seizures are single or irregularly recurrent events. | |
|
• Mechanisms are different from those of the clonic phase of generalized tonic-clonic seizures. | |
|
• There is a need for better characterization of generalized onset clonic seizures with video-EEG correlations. |
Generalized onset clonic seizures were mainly investigated by Henri Gastaut and his school in Marseilles (13).
Clonic seizures. Perhaps because they occur almost exclusively in early childhood, clonic generalized epileptic seizures are recognized even less frequently than tonic generalized epileptic seizures. They are encountered most often by family practitioners and pediatricians rather than specialists in neurology or epileptology. Clonic seizures occur more frequently than often recognized.
Clinical description. The attacks begin with loss of consciousness associated either with sudden hypotonia or, conversely, with a brief generalized tonic spasm, sometimes so abbreviated that it could be considered as massive bilateral myoclonus. Both will cause falling. The child then remains on the floor for 1 or more minutes and is seized by a series of bilateral myoclonus, usually generalized, although often asymmetrical and predominating on one side or in one limb. Subsequently, the variability of amplitude, frequency, and spatial distribution of these jerks from one moment to the next may become extraordinary. The most unlikely combinations are observed. Rapid low-amplitude twitching of facial muscles, for instance, may be associated with infrequent but very intense jerks of the upper limbs and with such rapid myoclonus of the lower limbs that virtual tetanic contraction results. Certain authors believe that in some attacks the entire body can jerk at such a high frequency that they could be described as “vibratory generalized epileptic seizures.” In our experience, the existence of such seizures is very doubtful, and they would have to be distinguished from the vibratory periods of the generalized tonic-clonic seizures and from certain rare tremors that may occur during epileptic automatisms.
In some children, particularly those aged 1 to 3 years, the myoclonus remains bilaterally synchronous and massive throughout the attack, rather than showing such complex and unstable patterns.
The autonomic changes are relatively important during prolonged seizures in which accumulated bronchial secretions may cause respiratory distress. Regaining of consciousness is rapid after brief seizures. Those of long duration, however, may be followed by a confusional or even comatose state with generalized muscular hypotonia and areflexia.
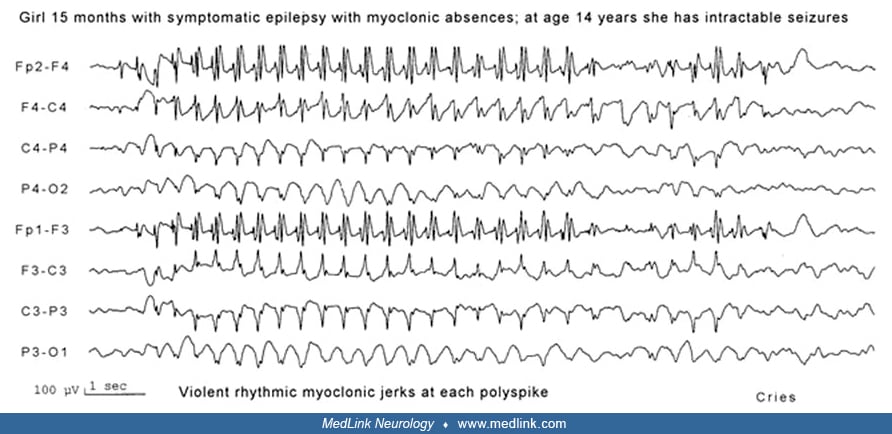
Other forms of clonic seizures, which are seen in older subjects, are more properly considered as absence status with marked myoclonus, often rhythmic, or prolonged myoclonic absences with the jerks repeated at 3/sec.
NREM sleep is frequently accompanied by bilaterally synchronous polyspike discharges sometimes associated with myoclonus and leading at times to a hypnic clonic generalized epileptic seizure. However, both discharges and seizures are absent from REM sleep (13).
The ILAE Commission of 1981 classified generalized onset clonic seizures amongst generalized seizures together with generalized tonic-clonic seizures (GTCS), tonic seizures, myoclonic seizures, and absence seizures and defined them as follows:
|
• Clonic seizures: Generalized convulsive seizures occasionally lack a tonic component and are characterized by repetitive clonic jerks. As the frequency diminishes, the amplitude of the jerks does not. The postictal phase is usually short. Some generalized convulsive seizures commence with a clonic phase passing into a tonic phase leading to a “clonic-tonic-clonic” seizure. | |
|
• Ictal EEG consists of “Fast activity” (10 Hz or more) and slow waves, with an occasional spike-and-wave pattern. | |
|
• The EEG interictal expression is of “spike-and-wave or polyspike-and-wave discharges” (03). |
Clonic seizures are defined as follows in the ILAE glossary:
|
• “Clonic: Myoclonus that is regularly repetitive, involves the same muscle groups, at a frequency of approximately 2 to 3 c/s, and is prolonged. Synonym: rhythmic myoclonus” (02). |
The ILAE core group classified clonic seizures amongst self-limited epileptic seizures of generalized onset with tonic or clonic manifestations and explains:
|
Clonic seizures are fast rhythmic events (1 to 2 Hz), associated, or not, with impaired consciousness. Mechanisms are different from those of the clonic phase of GTCS. In the latter, the clonic phase represents the phasing in of seizure-suppressing mechanisms, whereas in clonic seizures, the repetitive discharges appear to be due primarily to rhythmic excitatory discharges. There may be several types of generalized clonic seizures…. The distinction between myoclonic seizures and clonic seizures is not clear. Classically, clonic seizures are rapid rhythmically recurrent events, whereas myoclonic seizures are single or irregularly recurrent events… Differential diagnosis between myoclonic and clonic seizures can be difficult because a single jerk can be a fragment of a clonic seizure (09). |
In the 2014 ILAE “epilepsy diagnosis” manual, generalized onset clonic seizures are categorized among generalized convulsive seizures. Generalized seizures are convulsive, absence, tonic, atonic, and myoclonic (04).
“Generalized convulsive seizures are typically bilateral and symmetric although variants with asymmetry including head and eye deviation can be seen. A tonic-clonic seizure is a seizure consisting of a tonic and a clonic phase, typically in this order, however, variations such as clonic-tonic-clonic are also seen. A clonic seizure is a seizure involving bilaterally rhythmic jerking and may occur alone or in combination with tonic activity where there is bilaterally increased tone of the limbs typically lasting seconds to a minute. The jerking in a clonic seizure is more sustained and rhythmic than seen in a myoclonic seizure” (04).
The most recent ILAE positional papers on the operational classification of seizure types retain the name “generalized onset clonic seizures” and classify them amongst “generalized onset motor seizures” (12; 11). Generalized onset seizures are motor (tonic-clonic, clonic, tonic, myoclonic, myoclonic-tonic-clonic, myoclonic-atonic, atonic, epileptic spasms) or nonmotor (absence) typical, atypical, myoclonic, eyelid myoclonia. Also, the authors explain that “Generalized clonic seizures begin, progress, and end with sustained rhythmic jerking of limbs on both sides of the body and often head, neck, face, and trunk. Generalized clonic seizures are much less common than are tonic-clonic seizures, usually occur in infants, and should be distinguished from jitteriness or shuddering attacks” and “Myoclonus differs from clonus by being briefer and not regularly repetitive” (11).
|
• Clonic: Jerking, either symmetric or asymmetric, which is regularly repetitive and involves the same muscle groups. | |
|
• Myoclonic: Sudden, brief (< 100 msec), involuntary single or multiple contraction(s) of muscle(s) or muscle groups of variable topography (axial, proximal limb, distal). Myoclonus is less regularly repetitive and less sustained than clonus. |
Dr. Panayiotopoulos’s clarifications. It is apparent that according to the various ILAE classifications and definitions, generalized onset clonic seizures are mainly distinguished from generalized myoclonic seizures by their rhythmicity.
This has created significant overlap in what to call clonic or myoclonic seizures, and often these terms are used interchangeably. An example of this is “myoclonic absence seizures,” which manifest with clonic rather than myoclonic motor manifestations.
Conversely, what is called “clonic-tonic-clonic” generalized seizure of juvenile myoclonic epilepsy (05) may indeed be myoclonic-tonic-clonic seizure because the preceding events are random and irregular myoclonic seizures (22). This view has now been substantiated with the introduction of this term in the ILAE operational classification of seizure types: “Generalized myoclonic-tonic-clonic seizures begin with a few myoclonic jerks followed by tonic-clonic activity. These seizures are commonly seen in patients with juvenile myoclonic epilepsy and occasionally with other generalized epilepsies. It is arguable whether the initial jerks are myoclonic or clonic, but they are rarely sufficiently sustained to be considered clonic” (11).
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125