


Infectious Disorders
Arboviral encephalitis
May. 15, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Infective endocarditis is a potentially lethal condition associated with a myriad of neurologic consequences, including stroke, mycotic aneurysms, vasculitis, discitis, meningoencephalitis, myelitis, and mononeuritis. Despite therapeutic advances, the incidence of infective endocarditis is rising on a global scale. Rapid identification and treatment via medical and surgical techniques in a multidisciplinary and collaborative fashion are necessary to achieve good functional outcomes.
|
• The neurologic complications of infective endocarditis are due to septic embolism to cerebral arteries. This may result in embolic stroke, infection of vessel walls with mycotic aneurysm or vascular rupture, and extension outside the affected vessel to cause meningitis or brain abscess. | |
|
• Although infective endocarditis typically develops on previously damaged cardiac valves, endocarditis in individuals abusing drugs intravenously may develop on valves that are normal. In both cases, infection results in valvular vegetations. | |
|
• Diagnosis of infective endocarditis requires a high index of clinical suspicion, careful cardiac and neurologic examination, and identification of the causative agent from blood cultures. Patient evaluation includes echoencephalography and other methods to detect valvular vegetations and injury as well as imaging of the brain and its supplying vessels, electroencephalography if seizures are suspected, and cerebrospinal fluid analysis. | |
|
• Rapid diagnosis and early antibiotic intervention remain the mainstays to avoid neurologic complications. Valvular surgery is indicated in many patients. | |
|
• Cardiac surgery should be performed as soon as possible (< 48 hours) where indicated. However, if ischemic or hemorrhagic stroke is present, delaying 1 to 2 weeks or 4 weeks, respectively, may be of benefit. | |
|
• The use of an antithrombotic while being treated for infective endocarditis should be approached with caution. |
Although infective endocarditis was probably recognized as a specific entity in 1646 by Riviere, its manifestations were not fully described until the 19th century (76). In 1846, Virchow was the first to recognize the occurrence of embolic events with infective endocarditis (76). In 1852, a little-known English doctor, William Senhouse Kirkes (1822–1864), demonstrated that embolic events in infective endocarditis arose from cardiac vegetations (16). In a series of three Gulstonian lectures at the Royal College of Physicians in London in 1885, Sir William Osler drew on his enormous experience in both medicine and pathology to provide the first truly comprehensive account in the English language of what he termed “malignant endocarditis” (94; 102). In his lectures, Osler pointed out that the disorder resulted in meningeal or other central nervous system complications in 12% of patients. Thayer proposed the term “infective endocarditis” to replace the older term “bacterial endocarditis” as it became clear that a wide range of pathogens, including bacteria, rickettsiae, and fungi, could be responsible for the disease (122; 123).
Prior to the advent of antibiotics, infective endocarditis was invariably fatal. Treatment became possible as penicillin and subsequent agents became available. Initially, infective endocarditis was heavily associated with rheumatic heart disease, and the viridans group of streptococci were the agents most encountered (46). With the relative conquest of acute rheumatic fever in developed countries, however, Staphylococcus aureus has become the agent most associated with infective endocarditis within Western populations (87; 14). However, streptococci remain a significant cause of infective endocarditis in developing countries (87; 14; 97).
|
• Infective endocarditis is a multisystem disease, and the neurologic complications of infective endocarditis must be considered in the context of the overall illness. | |
|
• Neurologic complications of infective endocarditis may include cerebrovascular consequences, such as stroke or mycotic aneurysm, direct infection of meninges or brain parenchyma, and encephalopathies. |
Systemic features of infective endocarditis. The clinical diagnosis of infective endocarditis remains difficult, though the two cardinal features are fever (present in approximately 90% of individuals) and heart murmur (present in approximately 75% of individuals) (87; 14). However, fever and other systemic signs may be absent in elderly or immunocompromised patients (50). Presentations vary from a fulminant or acute semiology with congestive heart failure and septic shock to an insidious course with low-grade fevers of unclear source (87). With this variability in mind, the interval between symptom onset and diagnosis tends to be in the range of 5 weeks and may be considerably longer, though the history of an inciting event such as a dental procedure or intravenous drug abuse may be helpful in diagnosis (17; 92). Cardiac murmurs may not be easily auscultated and may be absent in right-sided endocarditis. Changing cardiac murmur or de novo appearance of a regurgitant murmur indicating valvular destruction have been considered classic signs of endocarditis. These signs are now infrequent, occurring in under 10% of patients. Septic embolization may occur systemically and result in a myriad of end-organ symptoms, such as splenic abscesses, intracranial large-vessel occlusions, myocardial infarction, or ischemic limbs (91).
Classic peripheral clinical findings of infection endocarditis include digital clubbing, splinter hemorrhages of finger or toenails, conjunctival hemorrhage, Roth spots (retinal hemorrhagic lesions), Osler nodes (painful subcutaneous nodules related to immune complex deposition of the palms or soles), and Janeway lesions (painless vasculitic lesions of the palms or soles) (22). However, these findings are relatively less common, occurring in 10% to 15% of individuals (22).
Neurologic manifestations of infective endocarditis. The most common neurologic complication of infective endocarditis is cerebrovascular disease. This may manifest as ischemic stroke, hemorrhagic stroke, vasculitis, or myotic aneurysms. Additional complications include CNS infection resulting in meningitis or brain abscess, encephalopathy, or peripheral neuropathy.
Ischemic stroke. Most neurologic events are related to cerebral embolization of septic material (61). Several factors that may predispose to embolization include larger vegetation size above 10 mm, mitral valve involvement, mobility of the vegetation, and Staphylococcus aureus infection (115; 10). Emboli may result in large or small vessel occlusions and may be either symptomatic related to index vessel occlusion or asymptomatic (37; 17). The American Heart Association does not recommend treatment of ischemic stroke by intravenous alteplase in those with known or suspected infective endocarditis due to risk of hemorrhagic transformation (100). Mechanical thrombectomy is the mainstay treatment for large-vessel occlusions and, barring other exclusion criteria, should be reasonably performed. Recanalization rates appear high, though further outcome and safety data are needed. Clear recommendations should be discussed on a case-by-case basis (31; 40).
Hemorrhagic stroke. Hemorrhage can result from hemorrhagic conversion of infarcts or from the rupture of infected vessels with or without mycotic aneurysm. One study found that of those with intracranial hemorrhage and infective endocarditis, nearly 25% were attributed to mycotic aneurysmal development (57). The resultant hemorrhage may be parenchymal, subarachnoid, or, in rare cases, subdural (44; 55; 11; 117; 28). Resolved infective endocarditis does not appear to increase the risk of long-term hemorrhagic stroke when accounting for valvular replacement and anticoagulation comorbidities (63).
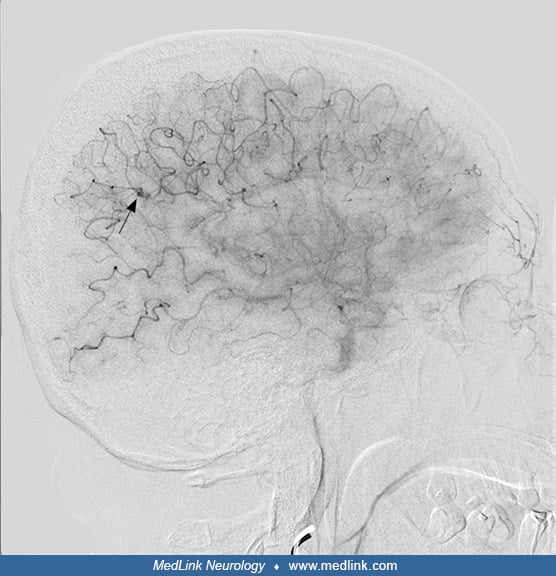
Mycotic aneurysms. As a consequence of a septic embolus within the intraluminal space, a localized inflammatory response develops, as does physical impediment of flow through vasa vasorum leading to aneurysmal dilation (55; 61). Mycotic aneurysms tend to have a predilection for distal middle cerebral artery branches with a fusiform shape and occur between 2% to 4% of individuals with infective endocarditis (57). However, the aneurysms themselves tend to be asymptomatic due to intrinsic mural fragility. Rupture may occur and leads to a high mortality rate (up to 80%) with intraparenchymal, intraventricular, or extra-axial hemorrhage, such as subarachnoid hemorrhage (36; 13). Infective endocarditis related to Staphylococcus aureus with mycotic aneurysms may be at a higher risk of aneurysmal rupture (13). As such, onset of severe headache, meningismus, seizures, and focal deficits such as cranial neuropathies in a patient with known endocarditis should all prompt immediate investigation. Modern CT and MRI vessel imaging of the brain have reasonable sensitivities and specificities for detecting mycotic aneurysms; however, conventional cerebral angiography remains the gold standard for diagnosis due to the inherent small size of the aneurysms (54; 127). Treatment is focused on a combination of aggressive antimicrobial therapeutics, endovascular strategies (eg, coiling, stenting, embolizing), and open surgical procedures (98). Conservative strategies with antibiotic therapy and surveillance imaging are reasonable; however, rupture requires immediate endovascular or surgical approaches. With antibiotic therapy, mycotic aneurysms may reduce in size, remain the same, or progressively enlarge. Documented enlargement of a mycotic aneurysm is an indication for urgent endovascular or neurosurgical intervention (89). Of note, mycotic aneurysms may be associated with increased risk of postoperative intracranial hemorrhage following valve replacement surgery (68).
Cerebral microbleeds. Cerebral microbleeds are a radiographic finding on hemosiderin-sensitive sequences and are classically associated as a radiographic variant of cerebral small-vessel disease (128). Of those with infective endocarditis, cerebral microbleeds are more frequent, with six times greater odds of having one to three cerebral microbleeds and 20 times greater odds of having three or more (64). Cerebral microbleeds may increase the risk of intracranial hemorrhage and tend to be more within a cortical distribution and associated with antiplatelet therapy, staphylococcal infection, and prosthetic valve infections (93; 53; 86). Presently, there are no data available to support altering treatment strategies based on the presence of cerebral microbleeds (23). It is reasonable to continue with aggressive antimicrobial therapies and careful monitoring of arterial hypertension.
Vasculitis. Vasculitis of the central nervous system may occur as either a primary (triggered) process or as a secondary (infectious) response (52; 125). Clinically, vasculitis may present with recurrent ischemic or hemorrhagic infarcts despite aggressive therapy. On pathologic and autopsy evaluations, findings between those with infective endocarditis and those with primary angiitis of the central nervous system appear to have similarities (09). Management should be focused on treating underlying infection, though immunomodulating therapies may be needed if persistent.
Central nervous system infection. Central nervous system invasion by bacteria in infective endocarditis may result in meningitis, brain abscess, or, less commonly, discitis, myelitis, or brain and epidural abscesses. These are most common in endocarditis due to Staphylococcus aureus but may also occur with a variety of organisms (74; 83; 33; 116). Presentation of these infectious conditions in the setting of endocarditis does not differ from that seen in individuals without cardiac valve infection. Meningitis is now unusual in most clinical cases due to recognition and prompt treatment and occurs in only 3% to 5% of patients (83; 116). Although infrequent, Streptococcus pneumoniae endocarditis can occur in a clinical triad of pneumonia, aortic valve endocarditis, and meningitis (Austrian syndrome), with rapid destruction of the aortic valve and frequent adverse outcome (33; 104). Mild encephalitis/encephalopathy and a reversible splenial lesion (MERS) is a rare neurologic finding in children and adults (51). Back pain and autonomic dysfunction may be present in those with discitis or myelitis (30). Interventional approaches may be desirous for abscesses and discitis.
Encephalopathy. As with other systemic infections, encephalopathy may develop, especially in those with a severe infectious burden. A myriad of etiologies exists, including toxic-metabolic, iatrogenic (medication-related), cardiac encephalopathy, direct central nervous system infection, seizures, or stroke (117). In rare instances, infective endocarditis may present as severe depression without other changes in cognition (46; 101). A comprehensive evaluation of reversible and emergent causes should be undertaken.
Neuropathy. Mononeuropathy or mononeuropathy multiplex are rare features of infective endocarditis that arise from extrinsic compression by peripheral mycotic aneurysms or embolization to nerva vasorum (96; 04; 95).
Other neurologic syndromes. Headache (25% to 42% of patients with neurologic complications), seizures (1% to 15%), myelopathy, and ocular involvement may all develop in patients with endocarditis (83). Ophthalmic changes include the appearance of conjunctival petechiae, conjunctival hemorrhages, and Roth spots (112). Ocular involvement may also manifest as unilateral visual loss from central retinal artery occlusion or retinal hemorrhage; hemianopia may result from ischemia in the optic radiations or occipital cortex. Diplopia can arise secondary to brainstem or specific cranial nerve involvement (46). Occasionally, infective endocarditis can result in spondylodiscitis, with or without epidural abscess. For this reason, the possibility of underlying endocarditis should always be kept in mind in patients with unexplained spinal disc space infections or with epidural abscess (85; 30; 08).
All-cause 30-day mortality in infective endocarditis is roughly 20%, and a variety of studies indicate a persistently elevated mortality rate in the months and years following (84). Patients with neurologic involvement do less well, with a mortality rate of approximately 45%, particularly with left-sided heart infection (44; 19). Adverse prognostic factors include age over 70 years, congestive heart failure, cerebrovascular events, Staphylococcus aureus infection, prosthetic valve endocarditis, and infective endocarditis acquired in a healthcare setting (07; 87; 44). There does not appear to be a specific neuroimaging pattern that predicts outcomes from a neurologic perspective (47). Mortality in intravenous drug abusers with infective endocarditis – even with surgery – may approach 50%, in part because of poor patient compliance with treatment (14; 45).
|
• Staphylococci, streptococcal organisms, and enterococci account for 80% to 90% of cases of infective endocarditis (14). | |
|
• Staphylococcus aureus is the most common organism to cause infective endocarditis, though a high index of suspicion should be kept for alternative species. |
Causative organisms. Staphylococci, streptococcal organisms, and enterococci account for 80% to 90% of cases of infective endocarditis (14). In a series of 497 patients with infective endocarditis, Selton-Suty and colleagues detected the following isolates (110):
|
Organism |
% of isolates | |
|
Staphylococci |
36.3% | |
|
Staphylococcus aureus |
26.6% | |
|
Coagulase-negative staphylococci |
9.7% | |
|
Streptococci and Enterococci |
48.3% | |
|
Oral streptococci |
18.7% | |
|
Nonoral streptococci |
17.5% | |
|
Enterococci |
10.5% | |
|
Other |
1.6% | |
|
HACEK organisms* |
1.2% | |
|
Candida species |
1.2% | |
|
Other |
6.0% | |
|
Two or more organisms |
1.8% | |
|
No organisms detected |
5.2% | |
|
| ||
Staphylococcus aureus remains the most common organism in much of the world, though regional variations exist. If the most common organisms have been ruled out, special consideration should be focused on unique aspects of the patient’s history, for example:
|
• Culture negative |
Coxiella burnetti and Bartonella species are the most common, though screening for HACEK organisms and fungal sources are worthwhile (41). |
|
• Immunosuppressed individuals |
Fungal (Candida species and Aspergillus) (03; 59) |
|
• Farming activities |
Coxiella burnetti (129) |
|
• Unpasteurized milk / endemic areas |
Brucella species (34) |
|
• High-risk sexual behaviors |
Neisseria gonorrhea, rare in the current antimicrobial era (Jackman and Glamann 1991) |
|
• Cat contact |
Bartonella henslae; cats are classically associated, though this may occur in homeless persons with alcoholism (119; 105; 124) |
|
• Prosthetic valve endocarditis |
Corynebacterium species; additionally with intravenous drug users and immunocompromised patients (131) |
|
• Intravenous drug use |
Polymicrobial infections are more common in intravenous drug users than in nonusers (118; 29). |
|
• SARS-CoV-2 co-infection |
Staphylococcus aureus remains the most common organism, followed by Enterococcus (103). |
Pathogenesis. Although transient bacteremia is relatively common in normal individuals, normal cardiac valves are typically resistant to infection, and infective endocarditis is an infrequent event (55); its development requires underlying valvular abnormality or injury. An important exception to this is S aureus, which can infiltrate normal valves. In developing countries, rheumatic carditis remains a major risk factor for infective endocarditis, and the mitral valve is most affected. In developed countries, rheumatic heart disease is the underlying condition in less than 5% of patients, and important underlying conditions include the presence of prosthetic valves or cardiac devices such as permanent pacemakers or cardioverter-defibrillators, or congenital heart disease (55). Injectable drug use, with valvular damage caused by repeated injections of particulate matter, remains an important cause and is particularly associated with right-sided endocarditis. Valvular injury from any of these causes can result in interstitial valvular edema and valvular deposition of fibrin and platelets, a condition termed “nonbacterial thrombotic endocarditis,” which can provide a substrate for subsequent infection following bacteremia and development of valvular vegetations (14; 55). Additionally, cholesterol crystals themselves, which are found in atherosclerotic plaques and sclerotic cardiac valves, may promote bacterial adhesion, which may then contribute to the development of endocarditis (12). The major neurologic sequelae of infective endocarditis are the result of emboli from these vegetations.
|
• Infective endocarditis is a relatively rare condition, though predisposing risk factors may increase the risk. |
Infective endocarditis is an infrequent condition, with an incidence of 1.5 to 11.6 cases per 100,000 person-years (14; 55). The condition is predominantly associated with four groups of conditions: (1) congenital or acquired valvular disease; (2) prosthetic valves; (3) indwelling cardiac devices, including pacemakers and extracorporeal membrane oxygenation; and (4) intravenous drug abuse. The EURO-ENDO registry, which involved a prospective cohort of 3116 adult patients, recorded native valve endocarditis in 1764 (56.6%) patients, prosthetic in 939 (30.1%), and device-related in 308 (9.9%) (49). In that study, infective endocarditis was community-acquired in 2046 (65.66%) patients and involved native valves in 56.6% of patients, prosthetic valves in 30.2%, and device-related infections in 9.9%. Additional risk factors include human immunodeficiency virus infection and prolonged exposure to healthcare settings (87; 55). In the prospective cohort study by Murdoch and colleagues, the most common underlying condition was degenerative (predominantly mitral or aortic) valvular disease (43% of cases) followed by the presence of a prosthetic valve (23% of cases) (87). Adults with sequelae of congenital heart disease appear to have a higher association with developing infective endocarditis (78). Intravenous drug abuse accounted for 10% of cases, with an equal number associated with infections resulting from chronic intravenous access. Only 3% of their patients had rheumatic valvular disease. Significant underlying conditions included diabetes (16% of patients in Murdoch’s series) and hemodialysis. Although left-sided endocarditis is much more common in general, the distribution of valvular involvement differs strikingly in intravenous drug users: in this population, 79% of cases have been reported to involve right-sided valves (as opposed to 13% in non-intravenous drug abusers), with 16% of cases involving left-sided valves and 5% involving valves on both sides of the heart (118; 29). However, left-sided valvular involvement has been reported to be higher in intravenous drug users who develop neurologic complications (79).
|
• A scientific statement from The American Heart Association recommends antibiotic prophylaxis for high-risk individuals undergoing dental procedures. |
Identifying patients with conditions that predispose to the development of infective endocarditis is considered an important means of preventing disease. Procedures that may cause transient bacteremia (eg, dental procedures) have traditionally been premedicated with antibiotics, though this is not based on randomized controlled data. For those with a high risk of developing infective endocarditis from bacteremia (eg, prosthetic cardiac valves, congenital heart disease, prior infective endocarditis, cardiac transplants), prophylaxis may be of highest benefit (13). Of note, a scientific statement from The American Heart Association recommends antibiotic prophylaxis for high-risk individuals undergoing dental procedures together with good oral hygiene (130). Antibiotic choice depends on local resistances and type of procedure being completed.
The classical clinical indicators of infective endocarditis should suggest the diagnosis. These include cardiac murmur, fever, and elevated C-reactive protein and erythrocyte sedimentation rate, which may reach levels over 100 mm/hr. However, the systemic and neurologic consequences of infective endocarditis are protean, and these classical symptoms, including murmur, are not present in all patients. For example, single or multiple cerebral or brainstem infarcts, which may be the presenting manifestations of endocarditis, are more commonly due to atrial fibrillation or, less often, aortic atheroma. Furthermore, many symptoms and signs found in infective endocarditis, including elevated C-reactive protein and erythrocyte sedimentation rate, can be duplicated by other conditions. These include vasculitides accompanying collagen-vascular diseases, such as polyarteritis nodosa; the hypercoagulable state seen with anticardiolipin antibody syndrome occurring alone or with other collagen vascular diseases; Libman-Sachs endocarditis, seen with systemic lupus erythematosus or anticardiolipin antibody syndrome; Loeffler endocarditis, a rare consequence of hypereosinophilic syndrome with cardiac involvement (Churg-Strauss syndrome); marantic (nonbacterial) endocarditis accompanying malignancy (01; 58; 108), Behcet syndrome (35); or conditions such as hepatitis B antigenemia (43). Clinical and MRI changes resembling CNS infarcts, at times with an accompanying rise in erythrocyte sedimentation rate, can also be seen in intravascular lymphomatosis (15; 73; 111).
A variety of conditions may predispose to infective endocarditis, including the following:
|
• Rheumatic heart disease |
• The diagnostic evaluation of an individual with neurologic complications of infective endocarditis involves two separate processes: (1) diagnosis of the endocarditis itself and identification of the infectious organism; and (2) delineation of the nature and extent of neurologic involvement. |
The diagnosis of infective endocarditis requires a combination of clinical, laboratory, and echocardiographic data. The most accepted criterion for the diagnosis of infective endocarditis is the modified Duke criteria, which categorizes individuals into definite, possible, and rejected infective endocarditis was first published in 2000, then revised in 2023 (72; 42). The diagnosis of definite infective endocarditis entails meeting either pathologic criteria or having two major clinical criteria, or one major and three minor criteria, or five minor criteria. Possible infective endocarditis requires one major and one minor criterion or the presence of three minor criteria. Rejected infective endocarditis criteria are met when a firm alternative diagnosis is made, lack of recurrence despite antibiotic therapy duration less than 4 days, no pathologic or macroscopic evidence of infective endocarditis at surgery or autopsy with antibiotic therapy given less than 4 days, or does not meet criteria for possible infective endocarditis.
Pathologic criteria: | ||||
• Clinical signs of active endocarditis with microorganisms identified from: a vegetation, cardiac tissue, an explanted prosthetic valve or sewing ring, an ascending aortic graft (with coexistent valve involvement), an endovascular intracardiac implantable electronic device, or from an arterial embolus. | ||||
• Active endocarditis (acute, subacute, or chronic) identified on one of the aforementioned biologic samples. | ||||
Major criteria: | ||||
1. Microbiologic criteria | ||||
a. Positive blood cultures | ||||
i. Typical: Microorganisms that commonly cause infective endocarditis isolated from 2 or more separate blood culture sets | ||||
ii. Atypical: Microorganisms that occasionally or rarely cause infective endocarditis isolated from 3 or more separate blood culture sets | ||||
b. Positive laboratory tests | ||||
i. Positive polymerase chain reaction or other nucleic acid-based technique for Coxiella burnetii, Bartonella species, Tropheryma whipplei from blood | ||||
ii. Coxiella burnetti antiphase I immunoglobulin G antibody titer > 1:800 or isolated from a single blood culture | ||||
iii. Indirect immunofluorescence assays (IFA) for detection of IgM and IgG antibodies to Bartonella henselae or Bartonella quintana with immunoglobulin G titer ≥1:800 | ||||
2. Imaging criteria | ||||
a. Echocardiography and cardiac CT imaging | ||||
i. Echocardiography and/or cardiac CT showing vegetation, valvular or leaflet perforation, valvular or leaflet aneurysm, abscess, pseudoaneurysm, or intracardiac fistula | ||||
ii. Significant new valvular regurgitation on echocardiography as compared with previous imaging. Worsening or changing of preexisting regurgitation is not sufficient. | ||||
iii. New partial dehiscence of prosthetic valve as compared with previous imaging | ||||
3. Surgical criteria | ||||
a. Evidence of infective endocarditis documented by direct inspection during heart surgery if cardiac imaging, microbiologic, or histopathology is not available. | ||||
Minor criteria: | ||||
1. Predisposition | ||||
a. Previous history of infective endocarditis | ||||
b. Prosthetic valve | ||||
c. Previous valve repair | ||||
d. Congenital heart disease | ||||
e. More than mild regurgitation or stenosis of any etiology | ||||
f. Endovascular intracardiac implantable electronic device | ||||
g. Hypertrophic obstructive cardiomyopathy | ||||
h. Injection drug use | ||||
2. Fever | ||||
a. > 38.0 degrees Celsius or 100.4 degrees Fahrenheit | ||||
3. Vascular phenomenon | ||||
a. Clinical or radiological evidence of arterial emboli, septic pulmonary infarcts, cerebral or splenic abscess, mycotic aneurysm, intracranial hemorrhage, conjunctival hemorrhages, Janeway lesions, purulent purpura | ||||
4. Immunologic phenomenon | ||||
a. Positive rheumatoid factor, Osler nodes, Roth spots, or immune complex-mediated glomerulonephritis | ||||
5. Microbiologic evidence falling short of a major criterion (one of either) | ||||
a. Positive blood cultures for a microorganism consistent with infective endocarditis but not meeting the requirements for major criterion | ||||
b. Positive culture, PCR, or other nucleic acid-based test for an organism consistent with infective endocarditis from a sterile body site other than cardiac tissue, cardiac prosthesis, or arterial embolus; or a single finding of a skin bacterium by PCR on a valve or wire without additional clinical or microbiological supporting evidence | ||||
6. Imaging abnormality | ||||
a. Abnormal metabolic activity as detected by radiotracer (as above) within 3 months of implantation of prosthetic valve, ascending aortic graft (with concomitant evidence of valve involvement), intracardiac device leads, or other prosthetic material | ||||
7. Physical examination | ||||
a. New valvular regurgitation identified on auscultation if echocardiography is not available. Worsening or changing of preexisting murmur, however, is not sufficient. | ||||
| ||||
Updates to the modified Duke Criteria for 2023.
Several changes were made in the latest iteration of the modified Duke criteria. Most noticeably, the requirement for timing and separate venipunctures was removed for blood cultures. The authors added definitions for “typical” organisms and modernized the laboratory testing to include PCR and immunofixation assays. The use of cardiac CT and PET imaging was additionally added. The use of a surgical major criterion was added when the other major criteria are not able to be assessed for, such as in resource limited situations. Minor criteria were added to incorporate cardiac implanted devices, splenic and cerebral abscesses, immune medicated processes, and the use of PET within 3 months of cardiac surgery.
Clinical manifestations of infective endocarditis include fever in up to 90% of patients, chills, anorexia, and weight loss. Symptoms can be subacute and insidious, adding to difficulty and delay in diagnosis. Other symptoms include malaise, headache, myalgias and arthralgias, and night sweats. Cardiac murmur occurs in up to 85% of patients but may not be detected by auscultation. Most significant is appearance of a new regurgitant murmur indicating developing valvular insufficiency. Splenomegaly and cutaneous manifestations are hallmarks of infective endocarditis. These include splinter hemorrhages; petechiae of the skin, mucous membranes, palate, and conjunctivae; Janeway lesions, which are nonerythematous papules on palms and soles; Osler nodes, which are tender subcutaneous nodules on palms, fingers, and toes; and Roth spots, exudative hemorrhagic lesions of the retina with pale centers.
These include complete blood counts, erythrocyte sedimentation rate, and C-reactive protein. Patients may exhibit a normochromic normocytic anemia. Urinalysis can show proteinemia and, importantly, microscopic hematuria or red blood cell casts (14; 55). Infective endocarditis may be accompanied by several inflammatory markers, including positive rheumatoid factor, hypoglobulinemia, cryoglobulinemia, circulating immune complexes, lupus anticoagulant, anticardiolipin antibodies, and false positive test for syphilis. Lupus anticoagulant and anticardiolipin antibodies may improve or resolve with antibiotic therapy (75). Of note, not all patients with infective endocarditis show signs of inflammation or inflammatory markers: in a retrospective review of 469 patients with left-sided endocarditis, Ribeyrolles and colleagues identified 13 patients (2.3%) with C-reactive protein values between 4.7 and 14.2 mg/L (106). The main presentations were apyretic heart failure and stroke. Eighty-five percent of these patients were without fever, and all patients had normal white blood cell and neutrophil counts. Sixty-two percent of these patients had severe valvular lesions on transesophageal echocardiography, including severe valvular regurgitation, valvular perforations, and paravalvular abscess (106). Modern testing including polymerase chain reaction, indirect immunofluorescence assays, and other nucleic acid-based techniques are now being used as denoted in the updated modified Duke Criteria from 2023.
These represent the essential diagnostic test for infective endocarditis. The prior time requirement was removed from the current Duke criteria, now noting samples must be isolated from separate blood culture sets as above.
This is most common where blood has been sterilized by previous antibiotic treatment. Cultures may also be initially negative in cases of endocarditis due to fastidious organisms, such as HACEK bacteria, defective streptococci-Gemelia, Granulicatella, Abiotrophia sp, Propionibacterium acnes, or Candida species: in these cases, prolonged incubation will usually allow identifying the causative pathogen in a few days. A minority of cases are due to intracellular bacteria that cannot be routinely cultured in blood with currently available techniques. Examples include Bartonella sp or Coxiella burnetti, which may be diagnosed serologically, by PCR, or by culture of excised heart valve tissue (121; 90). Tropheryma whipplei, a rare cause of culture-negative endocarditis, may be diagnosed by histological or PCR examination of intestine or excised heart valve, or by serum PCR (69; 80; 88). The newer technique, metagenomic next-generation sequencing, which isolates nonhost species of nucleic acids and compares them to a database of infectious organism nucleic acid sequences, may provide a powerful additional tool in the diagnosis of culture-negative endocarditis (24; 26; 27; 65).
These studies are second in importance only to blood cultures and are crucial in identifying valvular lesions.
Transthoracic echocardiography. Transthoracic echocardiography has a sensitivity of only about 70% for detecting vegetations on native valves and 50% for detecting vegetations on prosthetic valves (48). Transesophageal echocardiography is complementary to transthoracic echocardiography where transthoracic echocardiography is negative for vegetations (32). Separately, it may also provide insight to intracardiac abscesses and preoperative planning. False-negative findings are likelier in patients who have preexisting severe valvular lesions, prosthetic valves, cardiac implanted electronic devices, small vegetations, or abscesses or if a vegetation has already broken free and embolized (06; 14; 55; 67; 126). Distinguishing between vegetations and thrombi, cardiac tumors, and myxomatous changes may be difficult.
Cardiac CT and MRI. 4D cardiac CT can detect local extensions of infection, including abscess, fistula, and pseudoaneurysm. It can also incidentally detect pulmonary emboli. It is useful in suspected infective endocarditis in patients with negative transthoracic echocardiography and contraindications to transesophageal echocardiography. 4D CT can be coupled with CT angiography for a noninvasive way to evaluate the coronary arteries perioperatively without the risks associated with catheterization (66; 67; 81). Cardiac MRI is less well studied. It is potentially more sensitive than echocardiography for detecting vegetations, especially in patients with poor echocardiography images.
FDG-PET and leukocyte scintigraphy. PET imaging may be of use for native valve infective endocarditis. The utility of FDG-PET is founded on the uptake of 18F-fluorodeoxyglucose by cells, with higher uptake taking place in cells with higher metabolic activity, including as in areas of inflammation. Similarly, leukocyte scintigraphy relies on the use of radiolabeled leukocytes (ie, leukocytes previously extracted from the patient, labelled, and reintroduced into the patient) to allow for localization of inflamed tissue. The most significant contribution of FDG-PET may be the ability to detect infective endocarditis early when echocardiography is initially negative. When abnormal FDG uptake was included in the modified Duke criteria, it increased the sensitivity to 97% for detecting infective endocarditis on admission (107; 81). Both FDG-PET and leukocyte scintigraphy have a high sensitivity, specificity, and negative predictive value for cardiac implanted electronic device infection. They may help to differentiate thrombus from infected vegetation.
Brain imaging. As with stroke, CT scan is often initially done to rule out hemorrhage or hemorrhagic stroke. Beyond this, however, contrast-enhanced MRI is preferred to detect parenchymal lesions. Both CT angiography and MR angiography can be used for initial evaluation of intracranial vasculature but may miss mycotic aneurysms seen on catheter angiography (57). For this reason, 4-vessel catheter angiography remains the gold standard for the diagnosis of mycotic aneurysms given their frequent distal location within the cerebral arterial tree (57). Vessel wall imaging may provide an additional noninvasive means of detecting areas of actual vascular infection. Although it is common practice to evaluate for mycotic aneurysms in the setting of hemorrhagic lesions or high suspicion, routine screening has not been proven to improve outcome: in a study of preoperative MRI findings, there was not an association of findings with postoperative outcomes regardless of timing of valvular surgery (21; 20).
Spinal imaging. If clinical concern develops regarding discitis or spinal infection pathology, MRI of the cervical, thoracic, or lumbar spine with and without contrast may be helpful.
Transcranial Doppler ultrasound. Transcranial Doppler ultrasound provides a noninvasive method of detecting emboli within the cerebral circulation. It has been widely used in the study of stroke patients and can be an important tool in predicting patients at risk for neurologic complications in infective endocarditis. A study by Huang and colleagues suggested that transcranial Doppler may be useful for the noninvasive detection of intracranial embolic events and for monitoring the effect of antibiotic treatment (56). The study may also provide valuable data regarding the timing of valve replacement surgery (71).
Lumbar puncture. Lumbar puncture should be performed if meningitis is suspected and should be considered is indicated in patients with disorientation, altered level of consciousness, or significant headache. The study has little value in stroke and is relatively contraindicated as an initial study if brain abscess, other space-occupying lesions, or severe cerebral edema are suspected. A specific CSF formula, however, does not exist to differentiate endocarditis from other infectious etiologies. Lumbar puncture should be approached with caution if myelitis or epidural abscess are suspected and, if considered indicated, should be carried out at a spinal level well away from the suspected site of infection.
Treatment of infective endocarditis with neurologic complications requires consideration of four separate areas: antibiotic treatment, surgical repair or replacement of infected valves, treatment of the neurovascular complications of endocarditis including stroke, mycotic aneurysm, and hemorrhage, and treatment of meningitis or brain abscess.
A closely collaborative team approach consisting of neurologists, infectious disease specialists, interventional radiologists, and cardiothoracic surgeons is essential in providing effective care (38; 39).
Antimicrobials are the mainstay of treatment for infective endocarditis. Neurologic manifestations mainly occur before antimicrobial treatment is initiated, and rapid diagnosis and administration of antimicrobial therapy is still the most effective means to prevent neurologic complications. The risk of stroke after antibiotic initiation decreases 0.5% to 0.3% per day (52).
Empiric antibiotic treatment is generally not recommended, though it may be initiated while awaiting culture results if clinically warranted after three sets of blood cultures have been obtained, separated by venipuncture site and time. Specific antibiotic treatment is eventually determined by antibiotic sensitivities following blood culture.
|
Empiric Therapy for Infective Endocarditis Pending Culture Results* | |||
|
Condition |
Empiric antibiotics |
Remarks | |
|
Native valve endocarditis with indolent presentation |
IV amoxicillin + optional use of IV gentamicin OR IV vancomycin plus cefotaxime or ceftriaxone |
The use of gentamicin is controversial | |
|
Native valve endocarditis with severe sepsis |
IV vancomycin plus cefotaxime or ceftriaxone OR IV vancomycin + IV meropenem |
Some workers recommend concomitant use of gentamicin but this is controversial | |
|
Prosthetic valve endocarditis |
IV vancomycin + IV gentamicin + IV or oral rifampin | ||
|
*Consultation with Infectious Disease is strongly recommended before selecting treatment | |||
Consultation with an infectious diseases’ specialist is highly recommended to guide therapy. Therapy is typically continued for 2 to 6 weeks depending on the specific organism and valvular status, and it is timed from the last negative blood culture (06). Fungal endocarditis, though rare, has high mortality and demands a high index of suspicion, especially in patients with predisposing host conditions. Candida endocarditis should be immediately treated with liposomal amphotericin B or caspofungin, with optional addition of flucytosine (06; 59; 109). Voriconazole has also been used as treatment. Treatment of Aspergillus endocarditis is difficult. Amphotericin has been used in combination with voriconazole (85; 59; 109).
Cardiac valve surgery may be of benefit in those with uncontrolled infection, high-risk embolism potential, or heart failure (14). Prosthetic valve endocarditis presents unique challenges, and cardiac surgeons should be involved as soon as the diagnosis of prosthetic valve endocarditis is made to determine the best treatment strategies in a multidisciplinary manner (05).
Neurologic complications impact the timing and risk of surgical correction, and ambiguity exists amongst consensus recommendations. Each instance should be discussed on a case-by-case basis in a multidisciplinary fashion. Data do note that early surgical correction (within 48 hours) reduces in-hospital death and risk of systemic embolism (62). Among patients with preoperative ischemic stroke, the American Association for Thoracic Surgery consensus guidelines recommend a delay in surgical intervention of 7 to 14 days from diagnosis for ischemic stroke and more than 21 days for those with preoperative hemorrhagic stroke if clinically stable; otherwise, early or emergent surgery is recommended (99).
Antithrombotic medications. The American Heart Association does not recommend adjunctive therapy of antiplatelet medications for those with infective endocarditis; however, those who were previously prescribed may continue if no hemorrhagic complications develop (06). Additionally, there is a recommendation to stop all forms of anticoagulation for those who have a mechanical valve–associated infective endocarditis and who have developed a central embolic event for 2 weeks; intravenous heparin may then be cautiously reintroduced and then transitioned to oral medications (06). However, for those who have intracardiac thrombus or other emergent thrombotic processes requiring emergent anticoagulation, it may be used after the risks and benefits have been weighed by a multidisciplinary team (such as heparin infusion). Those with intracranial hemorrhage should not be prescribed antithrombotics.
Intravenous thrombolytics. The American Heart Association and American Stroke Association recommended that intravenous alteplase should not be used for acute stroke associated with infective endocarditis (100).
Mechanical thrombectomy. Presently, there are not enough absolute data available to provide consensus statements. Of the case series reported, similar rates of recanalization and outcomes are provided and are comparable to the general population (117).
Mycotic aneurysmal treatment. Unruptured aneurysms can be treated medically and followed with serial angiography or can be treated endovascularly. Less often, surgical clipping may be employed in cases of aneurysms that have ruptured or are enlarging (18; 114; 02). If stenting is performed, antiplatelets should be used to prevent in-stent thrombosis.
Treatment of the underlying infectious etiology remains the mainstay of therapy for central nervous infections related to infective endocarditis. Discitis and central abscesses may require surgical intervention.
Overall in-hospital mortality in infective endocarditis is roughly 20%, and increases to 25% to 30% by 6 months (14; 25). Five-year mortality is as high as 40% and can approach 70% in patients requiring intensive care unit hospitalization (82). Patients with neurologic involvement have a mortality rate of approximately 45% (44). Altered mental status at infective endocarditis onset, which is indicative of brain injury, is a major determinant of short-term outcome (17). Other adverse prognostic factors include age over 70 years, congestive heart failure, cerebrovascular events, Staphylococcus aureus infection, prosthetic valve endocarditis, and infective endocarditis acquired in a healthcare setting (87; 110; 44; 07). Mortality in intravenous drug abusers with infective endocarditis—even with surgery—can approach 50%, in part because of poor patient compliance with treatment (14; 45). Mortality in Candida endocarditis approaches 40%, and mortality in Aspergillus endocarditis is 60% (59; 70).
Incidence, clinical symptomatology, and treatment of abscess in pregnancy do not differ from those seen in nonpregnant individuals, nor do the complications of infective endocarditis affect the fetus. All antibiotics cross the placenta to various degrees, but only tetracycline has been documented to affect fetal development (77). Although few solid data regarding the teratogenic potential of other antibiotics exist, experience suggests that the penicillins (except ticarcillin), cephalosporins, and aminoglycosides can all be safely used in pregnancy. Therapy for endocarditis should, therefore, continue during pregnancy with the understanding that higher drug levels may be required given the increased volume of distribution and rate of clearance that normally occur in pregnant women. A multidisciplinary team is proven to improve outcomes amongst this special patient population (113).
Patients with infective endocarditis who undergo cardiac surgery in the setting of a recent CNS complication may pose a significant perioperative risk from both a cardiac and a neurologic standpoint. No particular anesthetic agents are contraindicated, and antibiotics are continued through the perioperative period in their usual doses (120).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Eric Goldstein MD
Dr. Goldstein of Brown University has no relevant financial relationships to disclose.
See Profile
John E Greenlee MD
Dr. Greenlee of the University of Utah School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Infectious Disorders
May. 15, 2026
Infectious Disorders
May. 12, 2026
Infectious Disorders
May. 05, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Infectious Disorders
May. 01, 2026
Infectious Disorders
Apr. 30, 2026