













Neuroimmunology
Balo concentric sclerosis
Jul. 02, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Optical coherence tomography is a high-resolution, noninvasive imaging technique. In clinical settings, this infrared technology is used to measure retinal nerve fiber layer thickness and macular volume. The retinal nerve fiber layer is the inner-most layer of the retina and is derived from unmyelinated axons. The axons arise from ganglion cell neurons located in the ganglion cell layer, which is directly below the retinal nerve fiber layer. The layers of the retina ultimately form the optic nerves and become myelinated. Optical coherence tomography takes advantage of the accessibility of the retina to study the CNS. The retina is unique in the CNS in that it contains axons and glia but no myelin. Thus, it is potentially an ideal structure to study neurodegeneration, neuroprotection, and possibly even neurorestoration in multiple sclerosis and neurodegenerative disorders.
Optical coherence tomography is a commonly used retinal imaging technique employed to diagnose and monitor eye disease. Because the technology is capable of rapid and reproducible measurements of the retina, which is a direct projection of the CNS, it can quantitate certain neurodegenerative pathologies. It is emerging as a valuable technique for characterizing neurologic diseases and has already been studied extensively as a biomarker for multiple sclerosis. Optical coherence tomography provides a low-risk technology that can greatly improve clinical acumen for both clinically oriented and research-based neurologists.
|
• Currently, optical coherence tomography (OCT) is utilized as an ancillary test to assist with the diagnosis of multiple sclerosis and to distinguish multiple sclerosis from other demyelinating diseases, such as neuromyelitis optica (29). | |
|
• OCT has also been used to follow demyelinating disorders over time in individuals. | |
|
• OCT is an excellent tool for monitoring therapeutic benefits of multiple sclerosis treatments in individuals and has become a standard metric or “biomarker” for multiple sclerosis clinical trials. | |
|
• OCT correlates with other biomarkers, such as low-contrast vision, visual evoked potentials, color vision, and brain diffusion tensor imaging (25). | |
|
• Using multiple sclerosis as the initial model, OCT has demonstrated its potential as a biomarker for neurologic diseases. With the ongoing development of new technology and the growth of neurologic OCT research, more applications for OCT are constantly being discovered. It is now possible to achieve more precise layer analysis in the macula with the advent of automated segmentation of the retina and extended depth imaging of the choroid. |
Optical coherence tomography (OCT) as applied to retinal imaging is emerging as an important tool for characterizing neurologic disease. OCT retina scanning is a noninvasive technique that utilizes the reflection of near-infrared light to quantitatively image individual layers of the retina (43). Spectral domain OCT (SD-OCT), the modern generation of OCT technology, performs axial scans using optical frequency data instead of mechanical movement. It executes A-scans up to 100 times faster than time domain OCT (TD-OCT), which allows for an enhanced resolution down to several microns (83). Because the retina is an extension of the CNS, SD-OCT can provide a direct, high resolution, and real-time window into structural changes associated with neurodegeneration. Some new SD-OCT devices can automatically track eye position and movement and can be used to automatically track patients over time.
OCT is widely used by ophthalmologists for confirming diagnosis, tracking disease, and monitoring treatment. It has proven useful in monitoring the progression of diseases such as wet age-related macular degeneration, macular edema, and glaucoma (02). It also can help ophthalmologists characterize macular holes prior to surgery and in evaluating the vitreoretinal interface (02). OCT has proven useful beyond ophthalmology. It has emerging applications in diagnosis and in tracking progression of neurologic diseases and may prove a useful tool for neurologists.
OCT is a high-resolution, noninvasive imaging technique using infrared technology to measure retinal nerve fiber layer thickness and macular volume. The retinal nerve fiber layer is the inner-most layer of the retina and is derived from unmyelinated axons. The axons arise from ganglion cell neurons located in the ganglion cell layer, which is directly below the retinal nerve fiber layer. The layers of the retina ultimately form the optic nerves and become myelinated. OCT takes advantage of the accessibility of the retina to study the CNS (07). The retina is unique in the CNS in that it contains axons and glia but no myelin, thus, potentially an ideal structure to study neurodegeneration, neuroprotection, and possibly even neurorestoration in multiple sclerosis and neurodegenerative disorders.
This review will describe studies that have linked neurodegenerative disease to retinal changes visible on OCT. Characteristic patterns of change have emerged for several neurodegenerative diseases, but they have thus far lacked diagnostic specificity and are affected by glaucoma and other ocular disease processes. Traditionally, OCT studies have focused on two diagnostic parameters: retinal nerve fiber layer thickness and macular volume. New automated segmentation software now allows for accurate measurement of 10 retinal layers: inner glial limiting membrane, retinal nerve fiber layer, ganglion cell layer, inner plexiform layer, inner nuclear layer, outer plexiform layer, outer nuclear layer, outer glial limiting membrane, photoreceptors, and retinal pigment epithelium. In addition, current OCT instruments can measure choroid thickness using extended depth imaging (60). These technical innovations are beginning to be employed to characterize specific retinal changes associated with neurologic disease.
Historical note and nomenclature. Definition of terms may be useful here for the neurologist new to retinal physiology:
Retinal ganglion cells. These cells transmit the information from the other layers of the retina to the brain. The axons of these cells make up the optic nerve. Retinal ganglion cells comprise the most superficial cell layer in retina and are susceptible to damage in a number of disease entities, including glaucoma and non-glaucomatous optic neuropathies.
Macula. The macula is the central portion of the retina that is responsible for central vision. An insult to the macula can cause loss of central vision and a significant decrease in visual acuity.
Papillomacular bundle. A collection of retinal ganglion cells that carries the information from the macula (the central retina) to the optic nerve and on to the brain. If damaged, central visual field defects occur. The clinical impact of damage to the papillomacular bundle is impaired central vision (centrocecal scotoma). OCT scan centers on the optic disc in order to analyze the peripapillary area and produce a cross-sectional image.
|
• The retinal nerve fiber layer is composed of the axons of the retinal ganglion cells, so OCT provides a measurement of axonal damage in the CNS. | |
|
• The macula is composed of 34% neuronal (ganglion) cells, so OCT provides a measurement of neuronal degeneration. |
The histology of the retinal layers correlates with findings on the OCT scan.
See www.mdsupport.org for more information.
Time versus spectral domain optical coherence tomography (OCT). OCT was initially developed as a tool for studying glaucoma. First iterations of OCT were time-dependent instruments, or time-domain OCT. Spectral-domain OCT uses Fourier transformation to generate even higher resolution imaging and is especially useful for evaluating the macula. Fourier transformation is an important image processing tool used to decompose an image into its sine and cosine components. The output of the transformation represents the image in the Fourier or frequency domain whereas the input image is the spatial domain equivalent. In the Fourier domain image, each point represents a particular frequency contained in the spatial domain image.
Both time-domain and spectral-domain OCT use light interference patterns to produce a tomogram, or cross-section, through the layers of the retina. From this information, the OCT is able to construct a 2-dimensional (time-domain or TD-OCT) or 3-dimensional (spectral-domain or SD-OCT) in individual segment boundary algorithms.
|
• The newest versions of OCT use spectral domain technology. | |
|
• SD-OCT has improved image quality and acquisition by collecting a larger set of actual data points, allowing for accurate spatial correlations and mapping of individual retinal layers over a larger area in a shorter period of time (28). |
Usefulness of OCT in demyelinating disease. OCT is currently utilized as an ancillary test to assist with the diagnosis of multiple sclerosis and to distinguish multiple sclerosis from other demyelinating diseases such as neuromyelitis optica (29). OCT has also been used to follow demyelinating disorders over time. OCT is an excellent tool for monitoring therapeutic benefits of multiple sclerosis treatments in individuals and has become a standard metric or “biomarker” for multiple sclerosis clinical trials. OCT correlates with other biomarkers such as low contrast vision, visual evoked potential, color vision, and brain diffusion tensor imaging (25).
Optic neuritis. Optic neuritis is an inflammatory injury to the optic nerve and is often the first manifestation of multiple sclerosis. Retinal nerve fiber layer thinning develops in the majority of optic neuritis patients after 3 to 6 months. Patients with multiple sclerosis and optic neuritis have a higher average thinning than those with multiple sclerosis alone. Following an initial episode of optic neuritis, OCT can detect axonal loss reflected as thinning in the retinal nerve fiber layer as early as 3 months after the episode. Acute edema may be detected even earlier in cases of anterior optic neuritis, appearing as a thickening of the retinal nerve fiber layer. Axonal loss may affect the whole peripapillary retinal nerve fiber layer, although the temporal quadrant is often the most affected. This may be due to the predominant involvement of the papillomacular bundle, which conveys the fibers from the fovea (the central macular structure responsible for detailed color and visual functions). As a result, macular function is reduced in eyes that have been affected by optic neuritis. More severe retinal nerve fiber layer thinning is seen in optic neuritis associated with neuromyelitis optica compared to optic neuritis seen in patients with multiple sclerosis (74).
Multiple sclerosis. In multiple sclerosis, peripapillary retinal nerve fiber layer thinning occurs and is associated with reduced macular volumes, especially with patients with history of optic neuritis. Visual function deteriorates with this thinning. The retinal nerve fiber layer thinning seen in multiple sclerosis typically affects temporal quadrants.
The retinal nerve fiber layer can be abnormal in asymptomatic patients or those without any prior history of optic neuritis; thus, OCT can show evidence of retinal thinning even before the patient is aware of any visual deficits. OCT can be abnormal even in individuals with so-called “benign multiple sclerosis.”
Retinal nerve fiber layer thinning observed by OCT has been shown to correlate with a variety of clinical measures, such as brain atrophy, disease subtype, disease activity, and disability status by Symbol Digit Modality Test and MRI measures of optic nerve atrophy.
Retinal nerve fiber layer thinning observed by OCT does not correlate with acute optic neuritis. Typically, retinal nerve fiber layer atrophy is seen 3 months after optic neuritis in multiple sclerosis. Early in the disease, OCT may be less sensitive than visual evoked potentials. One study of 65 subjects with 96 clinically affected optic nerves diagnosed at least 6 months prior found the sensitivity of OCT was 60% whereas sensitivity of visual evoked potentials was 80%. The OCT identified less than 20% of all subclinically affected eyes, and visual evoked potentials identified 75% (64).
Multiple sclerosis as a model of neurodegenerative disease. Multiple sclerosis and neuromyelitis optica serve as models for the use of OCT to define biomarkers in neurodegenerative disease (10). The literature on OCT in multiple sclerosis has been reviewed in full elsewhere and will only be summarized here. The thickness of the retinal nerve fiber, the combined thickness of the ganglion cell layer and inner plexiform layer (GC-IPL), and overall macular thickness are affected by multiple sclerosis (04). The timing of retinal nerve fiber layer loss can help in determining whether or not neuroprotective agents would be helpful in an episode of optic neuritis (04). Additionally, reductions in GCL-IPL thickness mirror reductions in gray matter in the CNS and correlate with increased disability (04). As a result of these findings, OCT is routinely used in multiple sclerosis clinical trials to track changes in retinal structure. The usefulness of OCT in multiple sclerosis suggests its applicability to other neurodegenerative diseases.
Additionally, OCT is useful in distinguishing between multiple sclerosis and neuromyelitis optica as the cause of optic neuritis (10). A review suggested that all patients presenting with optic neuritis should receive SD-OCT in the form of a peripapillary ring scan and a macular scan. Retinal nerve fiber layer thinning and ganglion cell layer thinning are both characteristic signs of optic neuritis, but the thinning tends to be more severe in neuromyelitis optica than in multiple sclerosis optic neuritis (06). Finally, macular scans can detect microcystic macular edema, which occurs more frequently in neuromyelitis optica than in multiple sclerosis optic neuritis (10). A 20% or greater retinal nerve fiber layer reduction in one eye can alert clinicians to a past episode of optic neuritis that went unnoticed (06).
|
• Several studies show neuromyelitis optica has more severe retinal nerve fiber layer thinning than multiple sclerosis, especially after optic neuritis in multiple sclerosis and particularly in superior and inferior quadrants (46). | |
|
• Ratchford and colleagues estimated that a first episode of optic neuritis caused 24 micron more loss of retinal nerve fiber layer thickness in neuromyelitis optica than in relapsing-remitting multiple sclerosis and that retinal nerve fiber layer loss greater than 15 micron after optic neuritis should prompt consideration of the neuromyelitis optica spectrum disease (74). | |
|
• Retinal nerve fiber layer thickness correlates well with visual field defects. | |
|
• Retinal nerve fiber layer and macular thickness also correlate with disability and EDSS score. | |
|
• OCT helps track axonal loss in neuromyelitis optica and discriminates between neuromyelitis optica and multiple sclerosis because of dramatic retinal nerve fiber layer thinning in neuromyelitis optica. |
Primary progressive multiple sclerosis. Progressive forms of multiple sclerosis have significant decreases in retinal nerve fiber layer thickness and macular volume. Time domain OCT has been shown to have limited use for monitoring ongoing loss of retinal axons late in this disease. A trend toward decreased macular thickness in primary progressive multiple sclerosis compared to relapsing-remitting multiple sclerosis has been described (27).
Clinically isolated syndrome. One study of 56 consecutive patients showed that the mean retinal nerve fiber layer and macular volumes were not significantly different compared with controls (68). There was no correlation between retinal nerve fiber layer atrophy or macula and conversion to multiple sclerosis at 6 months. In that study, OCT did not reveal subclinical axonal loss at the earliest clinical stage of multiple sclerosis and did not predict conversion to multiple sclerosis at 6 months.
Optical coherence tomography in multiple sclerosis clinical trials and treatment. Now OCT is recommended as useful technology for documenting outcomes in multiple sclerosis clinical trials (37). OCT is useful to monitor adverse events, specifically the macular holes seen in the fingolimod trial. These adverse events were seen 0.4% of patients on the 0.5 mg dose, and slightly more were seen in patients on the 1.25 mg dose. This was typically noted around 3 months after therapy was initiated and presented as painless visual loss. One group reported early bilateral onset at 10 days after initiation of therapy (22).
Optical coherence tomography and other neurologic disorders. OCT is currently being applied to the understanding of several other areas of neurologic disorders, including spinocerebellar ataxia, Parkinson disease, hereditary spastic paraparesis, and Alzheimer disease.
Ataxia. Pula and colleagues studied a heterogeneous group of patients with spinocerebellar ataxia and found abnormalities, particularly in spinocerebellar ataxia types 1, 2, and 3 (73).
The presence of retinal changes has also been investigated in other forms of ataxia, leading to better characterization of the pathology underlying certain members of this disease group. Studies have shed light on whether hypermyelination or hypertrophy of retinal fibers occurs in patients with autosomal recessive spastic ataxia of Charlevoix-Saguenay (ARSACS). Traditionally, myelinated retinal fibers were considered a hallmark of ARSACS and were used as diagnostic criteria (92). Studies have applied OCT to investigate whether this could be corroborated by thickening of the retina (69). Although multiple studies have detected an increase in retinal thickness, they support hypertrophy rather than hypermyelination. Myelination as detected by OCT is characterized by not only increased thickness but also hyper-reflectivity and posterior shadowing. These studies detected a significant increase in peripapillary retinal nerve fiber layer thickness but no classical findings of myelinated fibers emanating from the optic disc. It is now being increasingly accepted that retinal nerve fiber layer thickening can lead to striations that may have been confused with hypermyelination by ophthalmologic fundus examination (97). Imaging with OCT has demonstrated its potential to elucidate more about the subclinical characterization of ARSACS and should now be considered an important diagnostic tool for the disease.
Friedreich ataxia. Friedreich ataxia has also been explored with OCT, as patients sometimes present with visual impairment in addition to cerebellar ataxia and progressive sensory neuropathy. The disease is caused by a GAA repeat mutation, leading to loss of the mitochondrial protein, frataxin. Although mitochondrial disorders often present with optic neuropathy, ophthalmic manifestations had been less well understood in Friedreich ataxia until studied with OCT. Four independent studies determined that mean retinal nerve fiber layer is consistently decreased in patients with Friedreich ataxia (65; 84; 24). Retinal nerve fiber layer thickness correlated with age of onset, disease duration, and International Cooperative Ataxia Rating Scale (ICARS) score. However, only a minor subset of these patients had clinical visual impairment or defects detectable by fundoscopy (65). This indicates there is common subclinical optic neuropathy that could become a valuable metric for evaluating disease. Seyer and colleagues found retinal nerve fiber layer thinning correlated with GAA repeat length, which encourages inquiry about whether retinal nerve fiber layer could mark prognosis as well (84). Longitudinal clinical trials are necessary to confirm the utility of this subclinical optic neuropathy as a biomarker for Friedreich ataxia.
Spinocerebellar ataxia. With the exception of SCA7, these conditions are not typically characterized by ophthalmic involvement. However, visual impairment and clinical optic disc atrophy have been noted in some SCA1 patients, inspiring two studies to investigate whether this is related to a more common subclinical pathology detectable by OCT (73; 88). Pula and colleagues detected significant macular thinning in SCA1 and Stricker and associates, using a peripapillary retinal nerve fiber layer scan, found selective retinal nerve fiber layer thinning in the temporal region, which may indicative of pathology in the papillomacular bundle. This resembles pathology in mitochondrial diseases such as Leber hereditary optic neuropathy and dominant optic atrophy. Two case reports used OCT to detect maculopathy in association with SCA1 patients (91). However, the pathogenesis of SCA1 and mechanisms of visual involvement are still unclear.
Parkinson disease. Retinal nerve fiber layer thinning has been reported in Parkinson disease, particularly in superior and temporal areas (32).
Numerous studies document retinal nerve fiber layer thinning in Parkinson disease (14). Although temporal region thinning is most often reported, this result has been inconsistent. A review of several OCT studies of patients with Parkinson disease suggests that thinning of the macular IRL, which contains dopaminergic neurons, may be more diagnostically predictive than retinal nerve fiber layer thinning (14). Both macula and retinal nerve fiber layer thinning are worse contralateral to the patient’s dominant tremor side, suggesting that these retinal changes are indeed directly disease related (23; 51). Photoreceptor thinning in Parkinson disease has also been documented using OCT (63; 79). Two large studies of patients with Parkinson disease and healthy controls implemented the new OCT automated segmentation program (33; 21). Both studies found decreased thickness of the ganglion cell layer and inner plexiform layer in Parkinson disease patients, although they disagreed on changes in the inner nuclear layer, outer nuclear layer, outer plexiform layer, and retinal nerve fiber layer. These differences may have stemmed from discrepancies in how thinning was measured. Intriguingly, the degree of ganglion cell layer thinning correlated with severity and duration of Parkinson disease, as measured by the Hoehn and Yahr scale (42). These findings suggest the power of the new automated segmentation method and the relevance of applying it to neurodegenerative disease.
OCT continues to provide useful evidence of neurodegeneration in Parkinson disease, including patients with Parkinson disease associated with rapid eye movement disorder (95).
Hereditary spastic paraparesis. A French group found OCT correlations with SPG7 mutations responsible for autosomal recessive hereditary spasticity, suggesting relevance of OCT as a biomarker for this mutation (47; 94).
Alzheimer disease. A depletion of optic nerve ganglion cells and their axons has been histologically observed in patients with Alzheimer disease (41).
Several studies have examined patients with mild cognitive impairment using OCT. Mild cognitive impairment can precede Alzheimer disease, so diagnosing it and characterizing it early could be of crucial importance in preventing further decline. Most studies have found decreased retinal nerve fiber layer thickness in patients with mild cognitive impairment relative to age-matched healthy controls (70; 45; 03; 20; 56; 67). Reductions in macular thickness (30) and GC-IPL thickness (20) have also been reported.
The retinal nerve fiber layer and IRL thin in Alzheimer disease. An early meta-analysis of SD-OCT in patients with Alzheimer disease confirmed a significant reduction in retinal nerve fiber layer thickness in all quadrants (40). Such crude measures of retinal nerve fiber layer thickness have failed to consistently correlate with MMSE scores. However, a new linear discriminant function using retinal nerve fiber layer thickness correlates with MMSE scores and has similar accuracy to CSF testing for tau protein (54). Newer studies have also looked at other OCT parameters. Gharbiya and colleagues demonstrated choroid thinning in a cohort of patients with Alzheimer disease (35). Macular volume and GC-IPL thickness are also reduced in patients with Alzheimer disease (09; 33; 20; 30). These latter findings are supported in a meta-analysis (19). This raises the question of whether implementing automated segmentation analysis in OCT scans of patients with Alzheimer disease could yield a biomarker with better correlation to cognitive function and greater prognostic value.
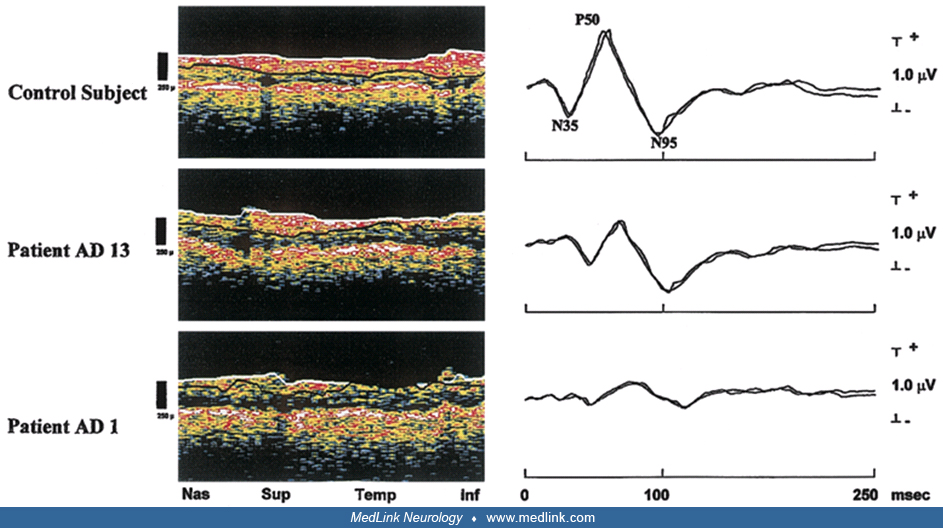
OCT-measured retinal nerve fiber layer thickness in Alzheimer disease reveals thinning superiorly and inferiorly. Parisi and colleagues correlated reduction in retinal nerve fiber layer thickness with abnormal pattern ERG responses (71).
The role of OCT in evaluating patients with early versus late Alzheimer disease is being assessed in ever more detail. Findings by Lad and colleagues controvert previous reports of thinner nerve fiber layer in moderate-to-severe Alzheimer disease (52). Cross-sectional GC-IPL measurements revealed areas of thinning adjacent to areas of thickening, suggesting that morphological changes are dynamic in Alzheimer disease.
Advanced OCT techniques have demonstrated additional structural changes in the Alzheimer retina, with one group reporting direct visualization of amyloid plaques (48) and another demonstrating decreased density of the macula’s microvasculature (96). The latter finding aligns with OCT evidence of reduced blood flow rates in the retinal arterioles and venules of those with mild cognitive impairment and Alzheimer disease, despite them having larger vessel diameters that matched healthy controls (44). With these microvascular changes, perhaps metabolite delivery and/or clearance is impaired early in the course of disease.
Huntington disease. Retinal layers, most significantly the retinal nerve fiber layer and ganglion cell layer, are strongly correlated with the disease progression in Huntington disease and are being evaluated as useful biomarkers for disease progression. They have potential for use in Huntington disease clinical trials, similar to use of OCT in multiple sclerosis therapeutic trials (38).
Amyotrophic lateral sclerosis. OCT has been preliminarily explored in amyotrophic lateral sclerosis patients, as it has the potential to provide insight about nonmotor involvement in amyotrophic lateral sclerosis. Although the disease is traditionally characterized as a motor neuron disease, growing evidence supports that amyotrophic lateral sclerosis is a complex neurologic disease on the same disease spectrum as fronto-temporal dementia. Roth and colleagues did not find significant retinal changes; however, Ringelstein and associates detected marked thinning of the inner nuclear layer (INL) and a subtle decrease in the average retinal nerve fiber layer thickness and macular volume as compared with age-matched controls (78; 75). Additionally, an autopsy in an amyotrophic lateral sclerosis patient with a C9orf72 mutation detected histopathological retinal involvement in the inner nuclear layer (26). The two OCT studies differed in the number and characterization of patients enrolled as well as in the type of OCT used. Roth and associates studied substantially more patients but elected to eliminate severe patients with progressive muscle atrophy and those with familial amyotrophic lateral sclerosis, whereas Ringelstein and colleagues included any patients who met the clinical diagnosis without other neuroophthalmic complications. A notable difference in analysis is that Ringelstein and associates did not apply a post hoc correction for multiple comparisons due to the exploratory nature of the study, whereas Roth and colleagues used a Bonferroni correction. Due to the mixed results of these OCT studies and differences in their study design, it would be valuable for future studies to investigate the potential of OCT imaging with amyotrophic lateral sclerosis, particularly with examination of the inner nuclear layer. One subsequent study did find evidence of subclinical retinal degeneration using OCT but primarily involving ganglion cell bodies and axons (77). This pattern implicates retrograde degeneration as a possible mechanism for retinal changes, which may vary in amyotrophic lateral sclerosis depending on the degree of brain involvement.
Idiopathic intracranial hypertension. OCT has emerged as a diagnostic tool in pediatric and adult idiopathic intracranial hypertension (50). Idiopathic intracranial hypertension, also known as pseudotumor cerebri, is characterized by increased intracranial pressure leading to headache, nausea, and ophthalmologic symptoms. A small but significant positive correlation has been demonstrated between CSF opening pressure and retinal nerve fiber layer thickness, ONH volume, and total retinal thickness (34). Moreover, SD-OCT is a reliable tool for monitoring papilledema secondary to idiopathic intracranial hypertension (66). Indeed, retinal nerve fiber layer thickness and retinal pigment epithelium-basement membrane conformation, both measured by OCT, respond to shunt surgery for idiopathic intracranial hypertension (85; 76). Furthermore, after the resolution of papilledema, OCT can detect macular atrophy (36). OCT with automated segmentation technologies will probably prove more useful to distinguish axonal loss from resolving optic disc edema (08).
Nutritional disorders. OCT findings in Wernicke encephalopathy include severe macular edema and hemorrhage (59).
Cuban epidemic optic neuritis. A presentation at the NeuroCuba conference showed that patients suffering from epidemic optic neuritis in Cuba showed findings similar to changes seen in multiple sclerosis and nutritional disorders, with thinning of temporal retinal nerve fiber layer, and distinct from severe diffuse changes, such as those seen in Leber optic atrophy (81; 82).
Susac syndrome. Susac syndrome is an autoimmune endotheliopathy with predilection for brain, retina, and cochlea. This classically presents with branch retinal artery occlusions, corpus callosal lesions, and hearing loss as well as encephalopathy. Susac syndrome can be confused with demyelinating disorders such as multiple sclerosis or neuromyelitis optica because of demyelinating-appearing lesions presenting in young women. We have found OCT to be very helpful as an adjunctive diagnostic metric and for clinically following these cases. In patients with Susac syndrome, OCT demonstrates global thinning and loss of foveal contour that is very specific and not seen in multiple sclerosis. OCT taken together with the unusual MRI findings and clinical findings is extremely helpful in directing clinicians toward the correct diagnosis and prompt treatment in these patients (12).
Sleep disorders. OCT has been studied in patients with obstructive sleep apnea hypopnea syndrome. Nasal parapapillary retinal nerve fiber layer thickness was significantly lower in severe obstructive sleep apnea hypopnea syndrome than in controls and mild to moderate cases (18).
Other disorders. OCT is useful for finding ophthalmologic disorders in neurology patients.
Future uses of OCT in multiple sclerosis and neurologic disease. Microcystic macular edema of the retinal inner nuclear layer has been identified in patients with multiple sclerosis by use of OCT (80). Increased inner nuclear layer thickness on OCT is also associated with disease activity in multiple sclerosis. If this finding is confirmed, inner nuclear layer thickness could be a useful predictor of disease progression in patients with multiple sclerosis. Reviews of OCT support the use of OCT in multiple sclerosis clinical trials (02; 05; 31; 72; 49).
OCT with automated segmentation has been used to characterize a growing set of disorders from autoantibodies such as GAD65 (16) and CASPR-2 (12).
Activity-dependent changes in infrared reflectivity at the photoreceptors were documented over a decade ago in humans and animal models (86; 87; 90). In ongoing studies, these intrinsic optical signals were readily detectable with a commercially available SD-OCT. This phenomenon has received renewed interest now that research-grade OCT systems have documented a small but related activity-dependent change in the space between the outer glial limiting membrane and the retinal pigment epithelium (55; 57; 98). This tentatively bridges reflectivity changes to activity-dependent changes in extracellular water content that, to-date, have only been studied in animal models with MRI (13) and other more invasive techniques (55). Retinal water and waste management is likely swayed by photoreceptor mitochondrial function (11) and retinal pigment epithelial function (01). A glial influence is plausible, especially for intrinsic optic signals found in other layers of the retina (89). This may represent a new way of studying function of non-neuronal support cells and may match changes in the central nervous system.
The reflectivity of certain retinal layers is influenced by the angle at which the OCT beam enters the eye (58). In general, SD-OCT reflectivity is highest when the beam is fully perpendicular to a bundle of well-aligned microstructures, like the axons of the retinal nerve fiber layer. Disease states that disrupt this alignment might be detected by measuring how reflectivity changes as a function of beam angle. Dedicated hardware (93) may facilitate these studies.
Use of OCT both in research and in clinical diagnostics has continued to expand in neurologic disorders. Further expansion is foreseeable as new techniques to study retinal function and structure in ever-finer detail come online. OCT is easy to use in the clinical setting, where its ability to characterize neurodegeneration remains a fertile area for investigation.
There are no absolute contraindications to use of OCT, although patients with thick cataracts or high diopter refractive error may present technical difficulties. Pregnancy is not considered a contraindication to this technology.
There are no known adverse effects to this technology.
Many neurodegenerative diseases have been characterized by nonspecific macular volume reduction and retinal nerve fiber layer thinning around the optic disc. However, studies have detected reduction of specific layers of the macula, particularly the ganglion cell layer and inner retinal layers in Parkinson disease and Alzheimer disease. There is also evidence for involvement of the inner nuclear layer in amyotrophic lateral sclerosis. Optical coherence tomography has proven effective in the characterization of retinal pathology in other diseases, including idiopathic intracranial hypertension, Susac syndrome, and ataxias, as well as the toxic effects of certain treatments.
Retinal pathology as detected by OCT may provide a valuable biomarker for aiding in diagnosis and monitoring disease progression and treatment. More precise layer analysis of the macula enabled by automated segmentation technology may offer substantial insight about further retinal pathology and will be valuable in future studies to investigate unobserved structural patterns. Functional OCT techniques may further enrich these structural assays.
Conclusion. OCT is a helpful ancillary clinical device for neurologists. Using multiple sclerosis as the initial model, OCT has demonstrated its potential as a biomarker for neurologic diseases. With the ongoing development of new technology and the growth of neurologic OCT research, more applications for OCT are constantly being discovered. It is now possible to achieve more precise layer analysis in the macula with the advent of automated segmentation of the retina and extended depth imaging of the choroid. Overall, retinal nerve fiber layer thinning has been noted in many neurodegenerative diseases, providing a potential metric for monitoring disease. Although reduced retinal nerve fiber layer thickness has been too nonspecific to aid in diagnosis, more accurate and in-depth analysis of additional retinal layers offers the possibility to unveil abnormal structural patterns. Automated segmentation has already been employed to detect retinal pathology in the ganglion cell layer and inner plexiform layer in Parkinson disease, showing that ganglion cell layer thinning correlates with disease severity. This not only urges the question of whether ganglion cell layer thickness can be a valuable biomarker for Parkinson disease but also offers promise for the use of automatic segmentation as an improved method for investigating unobserved retinal pathology. Additionally, studies have found ganglion cell layer-inner plexiform layer thinning in Alzheimer disease and mild cognitive impairment patients. Optical coherence tomography’s ability to noninvasively and longitudinally study neuronal and microvascular structure in these conditions may offer new insights into the progression of mild cognitive impairment in Alzheimer disease. Although initial OCT studies on amyotrophic lateral sclerosis disagreed about the presence of retinal pathology, additional investigation with automatic segmentation would be beneficial, as inner nuclear layer thinning is a possible pathologic marker in the retina. OCT is useful in characterizing other diseases like idiopathic intracranial hypertension as well as various forms of ataxia, including ARSACS, Friedreich ataxia, and SCA1. Further exploration will be necessary for a better understanding of how OCT can serve as an effective clinical tool for various neurologic diseases. With the continual advancement of OCT technology and constant discoveries from its applications, opportunities for future investigation using OCT will continue to emerge. Neurologists can use OCT to improve their clinical acumen with little risk to their patients.
Current normative OCT databases are limited in size and in terms of ethnic diversity. A study by Caldito and colleagues reported, “Relative to Caucasian Americans, African American patients with multiple sclerosis have been found to have greater retinal structural injury in the inner retinal layers. Increased thickness of the inner nuclear layer and the presence of microcystoid macular pathology at baseline predict clinical and radiological inflammatory activity, although whether race plays a role in these changes has not been investigated. Similarly, assessment of outer retinal changes according to race in multiple sclerosis remains incompletely characterized” (17).
These findings underscore the need to have larger, more diverse OCT databases that better represent the diversity of populations we care for in order to more completely understand variation in disease course, mechanisms of inflammation, and neurodegeneration, and to more accurately interpret findings in clinical trials that use OCT as a clinical endpoint.
OCT continues to have an important role in clinical trials of multiple sclerosis, particularly in remyelination and therapeutic neuroprotection studies. Evolving OCT technologies, such as OCTA (OCT angiography), which acquires high-resolution images of retinal vasculature, and SS-OCT (swept-source OCT) provide improved depth and range of imaging, along with simultaneous choroidal and vitreous imaging. OCTA may be particularly useful in longitudinal studies looking at cardiovascular comorbidities. OCT is being used in ongoing phase 2 and phase 3 clinical trials looking at neuroprotection using GCIPL atrophy as a surrogate for global disease processes and as an estimate of neurodegeneration (53; 61).
OCT may additionally have a potential role in how diagnostic criteria are applied in making the diagnosis of multiple sclerosis. The diagnosis of multiple sclerosis requires proof of dissemination in space (DIS) and dissemination in time (DIT), according to the 2017 McDonald criteria. In 2016, the MAGNIMS (Magnetic Resonance Imaging in MS) group had recommended inclusion of the optic nerve as an additional area for demonstrating DIS, established either clinically or paraclinically, by MRI, OCT, or by visual evoked potentials. Evidence was deemed insufficient, and the optic nerve was not incorporated into the 2017 McDonald criteria. A study by Bsteh and colleagues investigated whether adding the optic nerve as determined by OCT as a fifth DIS criterion to the 2017 McDonald criteria improved diagnostic criteria in a well-characterized cohort of patients with a first demyelinating event (15). This study found that the modified DIS-OCT criteria improved diagnostic accuracy (81% vs. 66%) by means of increasing sensitivity (84% vs. 78%) without compromising specificity (52% vs. 52%). This is in line with other studies using clinical, MRI, and visual evoked potentials definitions of optic nerve involvement. As OCT techniques and criteria for use are more refined, along with improved reproducibility of GCIPL measurements, it is possible that upcoming revisions of the McDonald criteria may be able to incorporate use of OCT as evidence of the optic nerve involvement and further burnish the role of OCT in diagnosis of multiple sclerosis.
At the 40th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) in 2024, revised criteria to the 2017 McDonald criteria were presented (62). The newly proposed 2024 McDonald criteria increase the relevance of OCT in facilitating the diagnosis of multiple sclerosis.
In addition to allowing new biomarkers to identify multiple sclerosis, the optic nerve is now allowed as a “fifth topography.” Lesions in the optic nerve can now be used as evidence of multiple sclerosis. This increases the relevance of OCT as a paraclinical test to confirm optic nerve disease.
The final publication of the new 2024 McDonald criteria is forthcoming, but a preliminary summary is as follows.
|
• New biomarkers that have excellent predictive accuracy can now be incorporated. | ||
|
-- Central vein sign (CVS): defined as a blood vessel within a multiple sclerosis plaque, seen on MRI | ||
|
-- Paramagnetic rim lesions (PRLs): defined as a rim of iron around the edge of a multiple sclerosis lesion, seen on MRI | ||
|
-- Kappa free light chains (kFLC): an inflammatory marker found in CSF may be used instead of oligoclonal bands | ||
|
• The optic nerve can now be included as a fifth topography, or anatomical location, to demonstrate dissemination in space (DIS) despite previous concerns about lack of specificity. Now, evidence of optic nerve disease can be defined by OCT, visual evoked potentials, or MRI. | ||
|
• The presence of a typical clinical syndrome is no longer necessary to make a diagnosis if other criteria are met. This will allow clinicians to diagnose and treat more promptly. | ||
|
• Dissemination in time is no longer required if lesions in four or five topographies support a diagnosis of multiple sclerosis: periventricular, juxtacortical, spinal cord, infratentorial, and the optic nerve. | ||
|
• MRI abnormalities in the brain and spine will be required, as multiple sclerosis will not be strictly a clinical diagnosis. | ||
|
• Patients with radiologically isolated syndrome (RIS) may be diagnosed with clinically definite multiple sclerosis if they meet dissemination in time (DIT) criteria, have CSF biomarkers, and have at least six CVS lesions. | ||
|
• The benefit of incorporating the optic nerve and the biomarkers described above is to facilitate more accurate and timely diagnosis so that appropriate treatment can be initiated earlier to prevent permanent neurologic deficits due to multiple sclerosis. | ||
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Jacqueline T Bernard MD
Dr. Bernard of Oregon Health & Sciences University received honorarium from TG Therapeutics, Genentech, and 2ndMD as a consultant.
See Profile
Anthony T Reder MD
Dr. Reder of the University of Chicago received honorariums from Genentech, Genzyme, and TG Therapeutics for service on advisory boards and as a consultant and stock options from NKMax America for advisory work and an unrestricted lab research grant from BMS.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuroimmunology
Jul. 02, 2026
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuromuscular Disorders
Jun. 16, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuro-Oncology
Apr. 30, 2026
General Child Neurology
Apr. 24, 2026
Neuromuscular Disorders
Apr. 23, 2026