Sleep Disorders
Sleep-related leg cramps
Jul. 03, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The concept that movement disorders may develop following trauma to the central and peripheral nervous systems has been widely accepted. It has both medical and legal implications for clinicians and their patients. The author of this clinical article reviews and provides updates on the pathogenesis, diagnosis, and management of posttraumatic movement disorders.
|
• Movement disorders can occur following central and peripheral nervous system trauma. | |
|
• Tremors and dystonia are the two most common abnormal movements following nervous system injury. | |
|
• The pathophysiology of posttraumatic movement disorders is complex and may include, but is not limited to, functional reorganization and alteration of neurotransmitters. | |
|
• Treatments for posttraumatic movement disorders are similar to those of nontraumatic movement disorders; however, the response is variable. | |
|
• A multidisciplinary approach is recommended in patients with comorbid psychological conditions and when there is pending litigation. |
Tremor, dystonia, and parkinsonism are the movement disorders that have been most often reported following trauma to both the central and peripheral nervous systems (35). Other movement disorders have been reported following trauma including chorea, hemiballism (58), ballism, paroxysmal dyskinesia, tics (23), progressive supranuclear palsy (60), painful legs and moving toes (104), cortical reflex myoclonus (38), palatal myoclonus (45), hemifacial spasm, hemimasticatory spasm, Meige syndrome (46), segmental myoclonus (51; 10), jumping postamputation stump, and other postamputation dyskinesia (50).
Although a direct causal link between a neurologic injury and the subsequent development of a movement disorder is not always clear with CNS trauma, a causal linkage is often even less apparent in cases of movement disorders following trauma to the peripheral nervous system. Some authors argue against the existence of “peripherally induced” movement disorders (119; 41), whereas others have argued that tremor, dystonia, and segmental myoclonus do occur following peripheral trauma (49; 50; 112).
Some authors suggest the term “posttraumatic syndrome” instead of “posttraumatic dystonia” in patients who have developed abnormal posturing of body parts following peripheral injury (65).
In addition, anecdotal reports suggest that trauma to both central and peripheral nervous systems may trigger or accelerate the progression of preexisting movement disorders.
Posttraumatic movement disorders have important medical and sometimes legal consequences. To establish the causal relationship between trauma and movement disorder, the severity of the injury, time course, and anatomical relationship must be taken into consideration. All types of movement disorders have been reported following CNS injury, but kinetic tremors and dystonia are the most common movement disorders to develop after severe head injury.
Although diagnostic criteria for peripherally induced movement disorders remain controversial, some criteria have been proposed: (1) trauma severe enough to cause local symptoms for at least two weeks or require medical evaluation within two weeks after trauma; (2) the initial manifestation of the movement disorder is anatomically consistent with the side of injury; and (3) the onset of the movement disorder occurs within one year after the injury (12).
Abnormal movements such as dystonia, tremor, and myoclonus can be a presenting symptom of complex regional pain syndrome (CRPS) in children following minor trauma to the affected limb (02), but a causal connection can only be suspected because of recall bias and the post hoc, ergo propter hoc fallacy.
Dystonia. A systematic review found that fixed dystonia, often associated with pain and sensory symptoms, was the most common movement disorder among 713 patients with a peripherally induced movement disorder (115); 26% of patients with peripherally induced movement disorder had an identifiable nerve injury, and more than one third of patients with a peripherally induced movement disorder developed CRPS. A study of 58 patients with CRPS type 1 (reflex sympathetic dystrophy) showed that 60% had muscle spasms leading to dystonic posture, 15% had coarse postural or action tremor, 9% had irregular jerks, 9% had dystonic spasms and irregular jerks, 5% had dystonic spasms and postural tremor, and 2% had episodic generalized choreiform movements (117).
Progressive delayed hemidystonia following seemingly mild traumatic brain injury has been reported (83). Following what was thought to be a mild traumatic brain injury, a 16-year-old boy developed progressive left hemidystonia over three years. Imaging revealed a traumatic scar involving the right basifrontal region and extending to the anterior, centromedian, and dorsomedial nuclei of the thalamus due to a blowout fracture of the roof of the orbit.
Cardoso Vale and colleagues reported a 52-year-old man who developed paroxysmal autonomic instability with dystonia syndrome after a severe traumatic brain injury (13). The traumatic brain injury required neurosurgical intervention and ventricular drainage. Postsurgical brain imaging disclosed extensive residua of his brain injury, as well as evidence of bilateral neurosurgical interventions, including an extensive left parietal craniotomy, trepanation in the right coronal suture, and an external ventricular drain in the frontal horn of the right lateral ventricle. He was left with spastic quadriparesis and cognitive impairment. During his intensive care unit stay and rehabilitation period, he presented with paroxysmal episodes of dystonic posturing accompanied by dysautonomia.
Imaging in a 52-year-old man with paroxysmal autonomic instability with dystonia after severe traumatic brain injury. (A, B) Cranial CT scan showing an extensive left parietal craniotomy, trepanation in the right coronal suture...
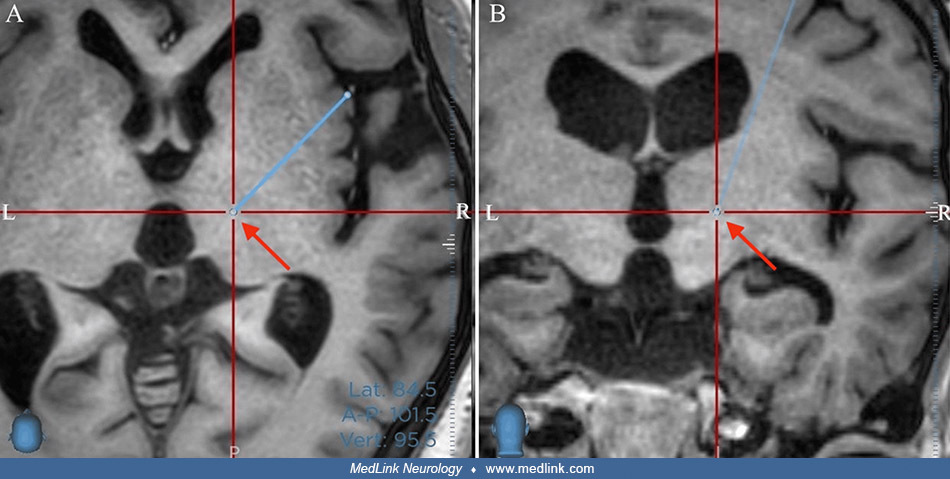
Kuramoto and colleagues reported a middle-aged woman with peripheral posttraumatic dystonia and complex regional pain syndrome following a scissors injury to her left hand 20 years previously (66). Initially, she experienced severe pain and tingling in her hand. A month after the injury, she developed an abnormal posture in her left hand, which gradually spread to other body parts. Botulinum toxin injections were inconsistent and did not improve muscle tone or correct limb position abnormalities. Various medications for neuropathic pain were either ineffective or caused intolerable adverse effects. On examination, she had a left claw hand deformity, and her left foot showed a rotated ankle joint with restricted motion. Abnormal positions of the opposite limb appeared when her pain increased. Muscle stretch reflexes were normal. A right ventro-oral thalamotomy was performed to improve her involuntary movements. After surgery, her abnormal limb posture disappeared when standing and walking, and she showed sustained improvement 3 months later.
Preoperative MRI in a middle-aged woman with peripheral posttraumatic dystonia with complex regional pain syndrome showing the planned targeting for a unilateral ventro-oral (Vo) thalamotomy. The preoperative target is in the r...
Postoperative coronal T2-weighted MRI following unilateral ventro-oral (Vo) thalamotomy in a middle-aged woman with peripheral posttraumatic dystonia with complex regional pain syndrome. As in a normal MRI, the left side of the...
Parkinsonism.
Central. A causal relationship between trauma and parkinsonism is supported by some but not by other studies. Parkinsonism is rarely a complication of a single head injury but may occur with penetrating injury to the brainstem or with an injury severe enough to result in a coma or vegetative state.
In one study before the advent of brain imaging, only two of 86 cases of parkinsonism following trauma were deemed to be true posttraumatic parkinsonism (37); these two cases had severe head injuries, and parkinsonism developed in conjunction with other extensive neurologic deficits. In 1934, Grimberg proposed that the diagnosis of posttraumatic parkinsonism could be made only if (1) a trauma was of sufficient severity to produce definite damage to the brain, (2) the trauma was direct to the head, and (3) there was a clear and definite developmental connection between trauma and disease (37). Hemiparkinsonism can develop from direct penetrating injury to the contralateral substantia nigra (16; 107), as a delayed effect of remote traumatic hemorrhage in the substantia nigra (39; 20), and with mass effects on the basal ganglia due to mass lesions affecting the corresponding cerebral hemisphere (eg, subdural hematoma) (85; 88). Although parkinsonism is accepted almost as dogma as a complication of repeated head trauma in boxers, case descriptions are not widely available, and available reports are generally by authors with no personal contact with these subjects. Given that only a minority of boxers develop cognitive or motor disability and that these data have rarely, if ever, been controlled by other high-risk hobbies or occupations, contact sports, or other activities, physicians should use more caution before concluding that there is a causal connection. A questionnaire study of 704 retired Thai kickboxers found that a high number of professional bouts (more than 100) was a risk factor for Parkinson disease, which was diagnosed in only five of the boxers (73). Other environmental factors like paraquat exposure and genetic predisposition, such as ApoE gene mutation and alpha-synuclein Rep1 expansion, may play an important role in the development of Parkinson disease following head injury (53; 33; 70; 57).
Peripheral. A wide range of movement disorders has been attributed to peripheral trauma (71).
(Source: Lenka A, Jankovic J. Peripherally-induced movement disorders: an update. Tremor Other Hyperkinet Mov [N Y] 2023;13:8. Creative Commons Attribution 4.0 International [CC-BY 4.0] license, creativecommons.org/licenses/by/...
However, the role of peripheral trauma leading to parkinsonism with severe bradykinesia, rigidity, and postural instability is controversial, and every effort must be made to determine whether the patient may have exhibited symptoms before the reported injury. Typically, reports of parkinsonism attributed to peripheral nerve injury describe the development of rest or postural tremor within days or weeks after an injury to the affected limb, followed by progressive rigidity and bradykinesia that gradually spreads beyond the original injury site. In a report of 28 patients with peripherally induced movement disorders, severe local injury preceded the onset of movement disorders by 60 days. The mean age at onset of movement disorders was 46.5 years. Tremor was present in all 28 patients, 11 of whom exhibited additional parkinsonian features. In 20 patients, the movement disorders spread beyond the original site. Possible predisposing factors were identified in 13 patients; nine had essential tremor or a family history of essential tremor. In addition, complex regional pain syndrome was present in six patients (12).
Hemiatrophy-hemiparkinsonism/hemidystonia. The main clinical features of hemiatrophy-hemiparkinsonism include atrophy of one side of the body (face, trunk, limbs), ipsilateral hemiparkinsonism (bradykinesia, rigidity, tremor), and, in many cases, dystonia (21).
Some separate hemiatrophy-hemiparkinsonism/hemidystonia as separate syndromes, but given the frequent clinical combination of both hemiparkinsonism and hemidystonia, there seems to be a clinical spectrum rather than two separate conditions. Furthermore, the condition is often referred to as hemiparkinsonism-hemiatrophy syndrome" or "hemidystonia-hemiatrophy syndrome," but, by all accounts, each of these presents the components in the wrong temporal sequence.
The mean age of parkinsonism onset is earlier than in idiopathic Parkinson disease, often in the 3rd, 4th, or 5th decade. MRI abnormalities (cortical, basal ganglia atrophy contralaterally to the side of clinical presentation) are reported in about one third of patients.
In one case, positron emission tomography with 18F-fluorodeoxyglucose and 18F-dihydroxyphenylalanine showed bilaterally symmetrical uptake with no significant increase or decrease in the cerebral hemispheres, including the striatum, but exhibited a significant reduction in the uptake of 18F-DOPA in the contralateral posterior striatum (42).
(A) Hemiatrophy of the left-sided lower limb. (B) The right lower limb is significantly shorter and smaller than the left lower limb, and the right foot was in an abducted posture. (C) Compared to the right calf, the left calf ...
(Source: He C, Zhang P, Li Y, et al. Hemiparkinsonism or hemidystonia with hemiatrophy syndrome: a case series with follow-up. Front Neurosci 2020;14:64. Creative Commons Attribution [CC BY] license, creativecommons.org/license...
In many cases, a history of prenatal injuries was reported (59; 67; 21). Levodopa treatment is often ineffective (21; 42).
Tremor.
Central. Tremors not related to parkinsonism or cerebellar dysfunction are the most common movement disorders following head injury (63). Posttraumatic tremors usually affect the arms and often exhibit a combination of rest, postural, and kinetic components, likely due to extensive lesions involving the thalamus, midbrain, red nucleus, cerebral peduncle, and cerebellum. In patients with tremor after severe head injury, tremor usually begins 1 to 18 months post-injury, often as an associated hemiparesis is resolving (03). Posttraumatic tremor is often associated with other movement disorders (eg, dystonia, athetosis, and myoclonus) and may be disabling, particularly with high-amplitude (> 10 cm) postural and kinetic (2.5 to 4 Hz) tremors.
A case of Holmes tremor has also been reported after a stabbing lesion in the midbrain: a 31-year-old man had been stabbed in the right eye, and he presented with a rest and action tremor in the left arm associated with left hemiparesis and corresponding post-contrast volumetric T1-weighted MRI with sagittal oblique reformation showing the knife trajectory reaching the right midbrain (18).
Peripheral. Approximately two thirds of patients who developed tremor and dystonia after peripheral trauma had predisposing factors such as a family history of essential tremor or dystonia, perinatal injury, or prior exposure to dopamine receptor blocking agents (52). In most patients with tremors following peripheral trauma, the tremor spreads beyond the side of original injury. Tremor may occur as an isolated symptom (17), but in some cases, it is associated with dystonia and parkinsonism. CRPS type I (reflex sympathetic dystrophy) may be seen in the affected limb, as it was in one of five cases of posttraumatic tremor developing within nine months after a peripheral injury (52).
Dystonia.
Central. Dystonia is characterized by involuntary, sustained, and patterned muscle contractions of opposing muscles that result in repetitive or sustained twisting movements or abnormal postures. Lesions in the striatum, particularly in the putamen, thalamus, and pontomesencephalic region, can cause dystonia (77; 72). Perinatal injury, closed head injury, encephalitis, and thalamotomy have been reported to cause hemidystonia (95). The onset of dystonia can be as early as 20 minutes after the injury (94), but it may be delayed by several months or years after trauma. In addition to limb dystonia, axial (neck and trunk) dystonia can also develop 6 months after a closed head injury associated with a caudate lesion. Most adult patients with dystonia following trauma have a history of head injury during the first two decades of life (69). Among nine patients with dystonia following severe head injury, hemidystonia was the most common, and seven patients with hemidystonia had contralateral caudate-putamen lesions (62).
Peripheral. It is often difficult to distinguish posttraumatic, peripherally induced dystonias from primary (idiopathic) dystonia, and some patients with idiopathic torsion dystonia give a history suggesting that dystonic movements had been precipitated or exacerbated by trauma or some repetitive, intense movement (eg, exercise or practicing a musical instrument) (55). In subjects with dystonia attributed to peripheral injury, dystonia appeared first in the injured part of the body within days or up to 12 months after the trauma, although delayed onset following injury of up to 3 years has been reported (116). Posttraumatic, peripherally induced dystonias are often characterized by (1) a fixed posture that is present at rest and often occurs in conjunction with underlying contracture; (2) limitation of range of motion; (3) absence of sensory tricks (geste antagonistique); and (4) presence of CRPS (about 20% of patients). In fact, CRPS may represent a variant of posttraumatic cervical dystonia that may develop over time (27). About 10% to 20% of patients presenting with cervical dystonia have a history of significant neck trauma, such as whiplash injury (25; 110). Posttraumatic cervical dystonia can be classified into two groups according to the latency between injury and onset of dystonia. Acute-onset cervical dystonia usually begins immediately or within days after trauma and is often associated with (1) significantly increased frequency of laterocollis with prominent shoulder elevation and trapezius hypertrophy; (2) pain; (3) marked limitation of range of motion; (4) abnormal postures without phasic movements; (5) lack of effect of sensory tricks; (6) no increase with activation; and (7) variable response to botulinum toxin (87). Many patients with acute-onset cervical dystonia are involved in litigation.
The other type of posttraumatic cervical dystonia is delayed-onset cervical dystonia, usually occurring between 3 and 12 months after neck trauma; the clinical picture is similar to idiopathic cervical dystonia. In task-specific dystonias such as writer’s cramp, only about 10% of patients report a history of hand or forearm trauma (78). Other posttraumatic focal dystonias include blepharospasm following ocular trauma and oromandibular dystonia following trauma to the face, mouth, or jaw (including trauma from oral surgery) (36; 105).
In an animal model of peripherally induced dystonia in Tor1a+/- mice that express 50% torsinA, a nerve crush injury was followed by abnormal posturing in the lesioned hindlimb of both mutant and wild-type mice, but the phenotypic abnormalities were increased by about 40% (p < 0.05) in the mutant mice (43). This was exacerbated by treatment with L-Dopa. The investigators suggested that peripheral nerve injury coupled with environmental stressors reduced torsinA concentration, resulting in central motor network dysfunction leading to dystonia.
The long-term prognosis for posttraumatic movement disorders has not been well studied. Complete, spontaneous recovery is, however, rare except in patients with tremors following mild head injury. In the rare cases of dystonia associated with subdural hematoma, the prognosis is favorable after hematoma removal. Fixed contractures often develop in posttraumatic dystonias following severe head injury if treatment and physical therapy are delayed.
Perinatal injury and closed head injuries have been associated with various movement disorders. In peripherally-induced movement disorders, several mechanisms of injury have been reported, including striking the neck against the floor, whiplash injury, traction injury of the neck or shoulder, twisting the back while lifting, pulling the starter cord of a mowing machine, heavy objects dropping on a limb, ankle sprain fall during active military duty (14), surgery (eg, laminectomy or corpectomy) (109), fracture of a long bone or rib (90), dental procedures (in oromandibular dystonia), electrocution, and burn injury (52; 103).
Prolonged immobilization following a peripheral insult seems to be an important risk factor because many movement disorders manifest after removal of a cast or splint. In one study, cortical thickness and white matter fractional anisotropy were examined in 10 patients with right-arm injury requiring at least 14 days of limb immobilization (68). The patients underwent two MRI examinations: the first within 48 hours postinjury and the second after an average time interval of 16 days of immobilization. Immobilization was associated with decreased cortical thickness in the left primary motor and somatosensory areas as well as decreased fractional anisotropy in the left corticospinal tract, providing evidence that immobilization induces rapid reorganization of the sensorimotor system. Using diffusion tensor imaging, another study showed cortical reorganization in response to cervical injury (28).
Unknown genetic predisposition and environmental factors may contribute to the pathogenesis of movement disorders following trauma, given the rarity of posttraumatic movement disorders after nervous system injury.
Movement disorders after central trauma. Traumatic cerebrocortical lesions may alter basal ganglia function indirectly and influence the development of movement disorders (32). CNS alterations following trauma include an inflammatory response, oxidative stress injury, axonal sprouting, demyelination, remyelination, central synaptic reorganization, diaschisis, and changes in neurotransmitter sensitivity (28). Several movement disorders (eg, dystonia) may develop several months or years after head trauma; the mechanism of such variable latency is unclear (48). Dystonia may be masked by the persistent severe hemiparesis following head injury (77). When both pyramidal and extrapyramidal systems are affected by trauma, the subsequent movement disorder may consist of a combination of dystonia and spasticity. In a rat model of traumatic brain injury, alpha-synuclein expression was increased in the pars compacta of the substantia nigra, which may pathologically support the link between head injury and Parkinson disease (01).
Movement disorders after peripheral trauma. A causal relationship between peripheral trauma and subsequent movement disorder is widely, but not universally, accepted (49; 119; 114; 113; 71). Several factors play important roles, including genetic susceptibility, preexisting brain dysfunction, and prior exposure to certain drugs or toxins.
(Source: Lenka A, Jankovic J. Peripherally-induced movement disorders: an update. Tremor Other Hyperkinet Mov [N Y] 2023;13:8. Creative Commons Attribution 4.0 International [CC-BY 4.0] license, creativecommons.org/licenses/by/...
Pathophysiologic changes in patients with movement disorders following trauma to the peripheral nervous system may resemble those in CRPS type I (reflex sympathetic dystrophy). Axonal density in a CRPS-affected limb is decreased compared to unaffected ipsilateral and normal contralateral limb controls, whereas symptom-matched control subjects did not have decreased axonal density in the painful site (86); thus, it appears that CRPS type I is specifically associated with posttraumatic distal nerve injury. However, it is yet unclear whether distal axonal injury has direct implications in the pathogenesis of posttraumatic movement disorders. Centrally, functional changes in afferent neuronal input to the spinal cord and central cortical-subcortical reorganization are probably involved (05). That peripheral injury can affect reorganization in the basal ganglia is suggested by the observation that thermal injury to a rat hind limb causes bilateral reduction in neuronal activity in the basal ganglia (19). Peripheral nerve deafferentation can also cause expansion of the receptive fields of sensory neurons in the thalamus. Central reorganization probably explains why peripherally induced movement disorders tend to spread beyond the original site of injury. A functional MRI study in patients with CRPS demonstrated activation of contralateral primary somatosensory, motor, and parietal association cortices; activation of bilateral secondary somatosensory, insular, and cingulate cortices; and deactivation in the visual, vestibular, and temporal cortices (75). A study using transcranial magnetic stimulation demonstrated abnormal excitability of the motor cortex in peripherally induced dystonia (07). Taken together, these findings suggest that peripheral trauma may be associated with functional reorganization in the brain and a shift of activation from tonically active sensory systems, such as visual and vestibular cortices, to somatosensory-related brain areas in CRPS patients (05; 91).
The actual prevalence of posttraumatic movement disorders is unknown. There are few epidemiological studies on the prevalence of posttraumatic movement disorders with variability in methodology and population among studies, yielding a frequency ranging from 13% to 66% (61).
In a study of 221 surviving patients with head injury admitted to a trauma unit with Glasgow Coma Scale scores of 8 or less, 22% developed posttraumatic movement disorders, which were transient in 10% and persistent in 12% (63); tremor was the most common movement disorder found in this series. In a follow-up study of 519 patients with mild-to-moderate head injury (Glasgow Coma Scale score between 9 and 15 on admission to the hospital), movement disorders were found in 10%, which were transient in 7% and persistent in 3% (64).
In general, it is difficult to establish a causal connection between trauma and the subsequent development of a posttraumatic movement disorder because of recall bias and the post hoc, ergo propter hoc fallacy. Cases are recognized in which a posttraumatic movement disorder was diagnosed, but later events showed that to be erroneous (08); such cases are likely underreported because many find it difficult to report clinical mistakes and because of medicolegal concerns.
Tremor. A population-based study in Spain demonstrated that serious head injury was significantly more common in patients with essential tremor than in controls (06).
In a questionnaire study of 195 patients with essential tremor, a history of head trauma and family history of tremor were associated with early age of onset (74).
Posttraumatic dystonia. Lee and colleagues found only 10 cases with dystonia after head trauma among 133 patients with symptomatic dystonia and either hemiparesis or demonstrated MRI/CT lesions (69). A case-control study of task-specific focal dystonias identified a significant association between head trauma with loss of consciousness and development of writer’s cramp (100), but several other studies demonstrated no association between head trauma and late-onset primary cranial dystonias, such as hemifacial spasm (79) or blepharospasm (92).
Posttraumatic parkinsonism. The role of head trauma as a risk factor for Parkinson disease is controversial. In several retrospective case-control studies, a history of trauma dates back 20 or 30 years before the onset of parkinsonism, augmenting difficulties with recall bias and confounding efforts to establish a causal relationship. A survey study in England found a positive correlation between head trauma and Parkinson disease (31).
In a case-control study in Olmsted County, Minnesota, the frequency of head trauma overall was significantly higher in patients with Parkinson disease than in controls (odds ratio=4.3; 95% CI=1.2 to 15.2) (09). Another case-control study in British Columbia, Canada, found that head injury, particularly at work, is associated with an increased risk for Parkinson disease (40). A third multicenter case-control study in Italy involving 492 Parkinson disease cases found a significant positive association between Parkinson and head trauma preceding disease onset (adjusted odds ratio=1.5; 95% CI 1.0-2.1) (84). However, in two population-based, case-control studies in Denmark and Sweden, hospital contact for head injury was probably a consequence of developing Parkinson disease rather than its cause, as the head injuries usually occurred within 3 to 12 months before diagnosis of Parkinson disease (101; 24). Another interview-based case-control study in Denmark failed to demonstrate that head injury increases the risk of Parkinson disease (56).
A systematic review and meta-analysis of 22 studies demonstrated a pooled odds ratio for the association of head injury and Parkinson disease of 1.57 (95% CI, 1.35-1.83), with a higher risk in subjects with a history of concussion (47). However, another systematic review from the International Collaboration on Mild Traumatic Brain Injury Prognosis Group did not find evidence to support the causal association between mild traumatic brain injury and Parkinson disease (76).
A case-control study in 93 twin pairs from the National Academy of Sciences/National Research Council World War II Veteran Twins Cohort demonstrated an association between a prior head injury with amnesia or loss of consciousness and an increased risk for Parkinson disease (odds ratio, 3.8; 95% confidence interval, 1.3-11; p = 0.014). Risk increased further with a subsequent head injury and with head injuries requiring hospitalization (34).
A population-based analysis quantified the risk for developing Parkinson disease after traumatic brain injury compared to nontraumatic brain injury trauma in California: among patients aged 55 and older, traumatic brain injury was associated with a 44% increased risk of developing Parkinson disease over 5 to 7 years that was not likely from confounding factors or reverse causation (30).
A systematic review of 26 case reports or case series of posttraumatic parkinsonism identified 36 patients, of whom about half (47%) had 1 to 6 months of latency to symptom onset, and 83% were male (99). The authors concluded that (1) posttraumatic parkinsonism can occur with or without evident brain lesions on neuroimaging, (2) the most common types of injuries that cause posttraumatic parkinsonism are motor vehicle accidents followed by falls, and (3) posttraumatic parkinsonism is responsive to medication or surgical treatments (99).
There are no known preventive strategies following trauma that may decrease the occurrence of posttraumatic movement disorders. Obviously, efforts should continue to minimize the occurrence of trauma.
Nondystonic torticollis. It is important to differentiate nondystonic torticollis that may occur following trauma from “true” dystonic torticollis. Nondystonic torticollis may result from atlantoaxial subluxation or fixation, fourth nerve palsy, and hemianopsia, causing head posturing, nasopharyngeal infection, and psychogenic dystonia. Acute posttraumatic dystonic torticollis begins 1 to 4 days after the neck injury and differs clinically from idiopathic torticollis by marked limitation of range of motion, lack of improvement after sleep ("honeymoon period"), and absence of geste antagonistique. Pain onset immediately after trauma and marked spasms of the paracervical muscles are other predominant features. Anticholinergic therapy is without benefit; however, some improvement may occur with botulinum toxin injection (111).
Primary (idiopathic torsion) dystonia. In contrast to action dystonia and mobile dystonic posture, seen in patients with primary dystonia, the posttraumatic, peripherally induced dystonias are often characterized by a fixed posture that is present at rest, often with underlying contractures, limitation of range of motion, absence of sensory tricks, and the presence of CRPS.
Psychogenic movement disorders. Many authors argue that the relationship between trauma and movement disorder is coincidental. This is often reinforced by the perception that patients with posttraumatic movement disorders have a psychological component to their disorder and that the development, persistence, and severity of the disorder are influenced by pending litigation. Moreover, the clinical phenomena develop after variable (and often extremely long) intervals remote from the putative inciting event, and the supposed traumatic triggers are often minor traumatic events without evidence of significant, persistent, structural brain damage (29). Most abnormal movements with a psychogenic cause are classified in the dyskinesia categories. A psychogenic movement disorder is suggested by (1) a sudden onset; (2) spontaneous remissions; (3) fluctuating frequency, amplitude, and pattern; (4) paroxysmal occurrence; (5) distractibility; and (5) an atypical character of the movement outside of the spectrum of typical movement disorders (82; 29). In addition, other features such as false (“give-way”) weakness, false sensory symptoms, and pseudoseizures may be present. A dramatic improvement after suggestion, physical therapy, and psychotherapy argues against an organic etiology. Finally, clinicians should consider the possible combination of an existing movement disorder with a psychogenic dyskinesia or the exaggeration of a posttraumatic movement disorder on a psychological basis.
Posttraumatic shoulder movement disorders provide an example of the difficulty of distinguishing organic and functional posttraumatic movement disorders. In a report by Pandey and colleagues of three cases of shoulder movement disorders subsequent to trauma to the shoulder region (89), there were some clinical features suggesting a functional etiology in two cases, but physiological studies failed to produce objective evidence of a functional nature in all three cases (89). A later report by Vial and colleagues documented a functional etiology for posttraumatic jerky movements of the scapula and neck (118). A 22-year-old right-handed man presented with a 1-year history of abnormal movements of his neck and upper back that developed gradually 2 weeks after a blunt impact in that region during martial arts training. He reported severe, focal, nonneuropathic pain. Examination disclosed non-rhythmic, jerky movements of the left side of the neck and upper back that diminished with muscle activation and on recumbency. Cervical and thoracic MRI studies were normal. During EEG recorded from the C3 electrode (reference to the contralateral mastoid), abnormal movements started once the subject was instructed that the study had begun. They were readily entrainable. EEG/EMG back-averaging revealed a Bereitschaftpotential preceding movement onset, confirming the functional nature of the movements (80).
Diagnosis of posttraumatic movement disorders is based on clinical history and physical examination. Brain imaging may show contralateral basal ganglia (particularly caudate-putamen) or thalamic lesions in patients with hemidystonia following severe head injury. Functional studies such as SPECT, PET, or functional MRI are used for research purposes.
Parkinsonism. The treatment of posttraumatic parkinsonism is the same as for Parkinson disease, but the response to medications is less predictable. In patients with established substantia nigra lesions, the benefit from levodopa therapy may be dramatic; however, in some cases, it may be complicated by motor fluctuations and dyskinesia. In peripherally induced parkinsonism, levodopa is usually not effective due to postsynaptic damage from central reorganization associated with aberrant peripheral input. Emerging surgical therapies, such as functional stereotactic surgery or, preferably, deep brain stimulation in the thalamus, may be effective in selected cases (61; 102). The postsynaptic component of peripherally induced parkinsonism is supported by a poor response to bilateral stimulation of the subthalamic nucleus (04).
Tremor. The postural and intention tremor occurring after mild to moderate head injury usually do not require therapy and subside spontaneously. In contrast, only a small number of patients with tremor following severe head injury improve spontaneously within one year of onset. In these cases, posttraumatic tremor is difficult to treat. Beta-blockers such as propranolol may decrease kinetic tremor and improve motor control (22). Carbamazepine, primidone, levodopa/carbidopa, anticholinergics, benzodiazepines, and new antiepileptic drugs such as topiramate may be used as an initial therapy for postural and action tremors. Botulinum toxin injection into the affected limbs is helpful in some cases that fail oral therapy, but the high doses that must be administered to both proximal and distal arm muscles limit its use. In severe, medically refractory cases, surgical intervention (eg, deep brain stimulation or ablative stereotactic surgery with targets in the thalamus or the subthalamic nucleus) should be carefully considered. Despite the excellent efficacy of ablative stereotactic surgery, many patients develop permanent cognitive/language side effects and secondary dystonia. Therefore, deep brain stimulation to the ventral intermediate nucleus of thalamus, ventro-oralis posterior/zona incerta region, or globus pallidus internus is generally recommended, although it has been used in only a limited number of patients with posttraumatic tremor and the benefit is variable (96; 97; 44; 108; 98; 93); this approach should be considered no earlier than one year after the onset of tremor (61). It has been anecdotally reported to benefit pediatric patients with posttraumatic tremor and should be offered for drug-resistant pediatric or adult patients with posttraumatic tremor (93).
Dystonia. Medical therapy for posttraumatic dystonia is often ineffective: anticholinergic drugs produce only a minimal response. Botulinum toxin is the treatment of choice for posttraumatic torticollis and other focal dystonias. Functional stereotactic surgery targeting the thalamus, the subthalamic nucleus, or the internal globus pallidus is an alternative option for patients with disabling hemidystonia. Benefit is usually seen in the early postoperative period; however, the long-term outcome is still unknown. Outcome data for deep brain stimulation in posttraumatic hemidystonia or peripherally induced dystonia remain limited (11). Globus pallidus stimulation may have long-term efficacy in patients with posttraumatic hemidystonia and dystonic tremor (54; 15). In patients with generalized dystonia and posttraumatic hemiballism, chronic intrathecal administration of baclofen via an implanted pump may provide symptomatic relief (81; 26). Other surgical interventions (eg, local peripheral and central denervation) may be considered in refractory cases. In patients with significant psychiatric comorbidities and pending litigation, multidisciplinary treatment including physiotherapy and psychotherapy should be considered (106).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See Profile
Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 03, 2026
Movement Disorders
May. 24, 2026
Movement Disorders
May. 18, 2026
Movement Disorders
May. 18, 2026
Movement Disorders
May. 18, 2026
Movement Disorders
Apr. 02, 2026
Movement Disorders
Mar. 11, 2026
Movement Disorders
Mar. 11, 2026