







Neuro-Oncology
Turcot syndrome
May. 27, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Preoperative embolization of vascular tumors of the head, neck, and spine is considered an important adjunct to the surgical treatment of these lesions, primarily by minimizing the operative blood loss. In this article, the authors outline the fundamentals of preoperative embolization for highly vascularized tumors of the head, neck, and spine. The authors discuss the indications and anatomical and physiological considerations and illustrate technical details concerning the various embolic agents used to treat these complex lesions.
• Preoperative embolization is used for select cases of highly vascularized brain, head and neck, and spinal tumors to minimize intraoperative blood loss. | |
• The primary route for tumor embolization is transarterial. Direct percutaneous puncture is an alternative for select cases. | |
• Commonly used materials available for embolization include liquid embolics, particle embolics, and detachable coils. |
The term “embole” has historically held multiple connotations (48). In 1849, Virchow coined the use of “embolus” for the dislodgement of fragments of venous clots into circulation, generating arterial obstruction (48). Today, “embolus” refers to a liquid, solid, or gaseous substance that migrates intravascularly and might occlude the distal arterial bed or capillaries. Tumor embolization is the intentional mechanical blockage of vascular supply to a tumor via the injection of liquid or particulate agents. This can be performed either intra-arterially through a catheter-based endovascular or via direct percutaneous puncture (46). Since the first reports of preoperative embolization of juvenile nasopharyngeal angiofibroma and glomus jugulare tumors in the 1970s, the practice has become a mainstream adjunct in the management of hypervascularized tumors (46; 29).
A comprehensive preoperative angiographic evaluation should precede tumor embolization to delineate all possible arterial feeders and relevant collateral anastomoses. This evaluation may also include a balloon test occlusion or other provocative testing if sacrifice of a large vessel (such as the internal carotid artery or vertebral artery) is being considered. Evaluating the venous anatomy can be useful for surgical planning for tumors involving the venous sinuses.
The goal of preoperative tumor embolization is to attempt superselective mechanical blockage of tumor vasculature. Ideally, intratumoral vessel devascularization is achieved at the arteriolar or capillary level (03; 28; 22; 12). Embolization of tumor parenchyma with preservation of the parent artery avoids ischemic injury to adjacent tissues. Although embolization of a feeder artery proximal to the tumor bed may appear to devascularize the tumor, collaterals to the tumor capillary bed may still contribute to tumor vascularization and, therefore, to bleeding at the time of surgery. Proximal feeder artery occlusion may also prevent future arterial access to the tumor if embolization is required (28). Once superselective catheterization of a tumor-feeding arteriole is achieved, slow and careful injection of embolic material is performed under fluoroscopic guidance with care taken to avoid significant reflux or embolization into normal vascular territories. Once the capillaries from a given feeding pedicle are saturated with embolic material, additional embolization can be performed through other feeding pedicles.
Direct tumor puncture is another potential access route for tumor embolization and was originally described for juvenile nasopharyngeal angiofibroma in 1994 (06; 45). Direct tumor puncture is used for cases where the transarterial route is technically challenging because of small feeder size or where direct branches of the internal carotid artery or vertebral arteries are involved to avoid reflux of embolization material into intracranial circulation or the retina. To avoid adverse events, careful angiographic evaluation of a tumor should be performed to assess potential dangerous collaterals. Direct tumor puncture is most commonly used for head and neck or extra-axial spine tumors where percutaneous access is readily achievable. An advantage of direct tumor puncture is that the potential challenges of transarterial access are not applicable as the needle is inserted directly into the tumor (22).
The ideal timing of tumor embolization remains controversial due to limited data. Proponents of early surgery (within 1 to 3 days of embolization) anticipate symptomatic tumor swelling and aim to prevent revascularization of the tumor parenchyma via collateralization or dissipation of the embolic agent (22; 49). The latter is more common with particle embolics than with liquid embolics. On the other hand, longer wait times after embolization may allow for necrotic liquefaction of the tumor, which can further facilitate tumor resection (35; 36).
Various agents with different basic physical properties are available for tumor embolization, each with individual specific handling characteristics, delivery techniques, and side-effect profiles.
Liquid embolics. Liquid embolics include n-butylcyanoacrylate (nBCA), ethylene vinyl alcohol, and ethanol. Liquid embolics can penetrate tumoral capillary beds but may generate angionecrosis, injury to normal structures, or cytotoxic edema (28).
nBCA, commonly referred to as glue, is an acrylic adhesive agent. It is mixed with ethiodized oil and a radio-opaque powder to increase polymerization time and confer opacity. To avoid inadvertent polymerization, the process must be performed without contamination from ionic material (blood, contrast, or saline). The microcatheter is first flushed with 5% dextrose in water, followed by the nBCA mixture (31). Once in contact with blood, nBCA polymerizes, becomes adhesive, and forms an acrylic cast. Prolonged injections are often not possible, and occasionally only a small portion of the nidus can be occluded with a single injection (34). At the end of the injection, the microcatheter is briskly but carefully withdrawn to prevent adhesion of the microcatheter within the nBCA cast. nBCA is thought to be one of the most permanent embolic agents (34).
Ethylene vinyl alcohol copolymer, Onyx (Medtronic), is a mechanically occlusive agent that is nonadhesive to the arterial wall. It is dissolved in dimethyl sulfoxide (DMSO) and polymerizes by desiccation once DMSO diffuses out of the compound. Two concentrations are available, 6% (Onyx 18) or 8% (Onyx 34). The “18” and “34” refer to centistokes, a unit of kinematic viscosity. Onyx 34, therefore, has a higher viscosity than Onyx 18 (34). Lower viscosity is desirable when there is a slow flow pattern or if distal penetration into a vascular bed is required. The non-adhesive properties of Onyx permit a prolonged and controlled injection with reduced risks of early polymerization (34; 31). During injection, reflux of embolic material is typically observed. A pause of 1 to 2 minutes is, therefore, commonly performed after the initial injection to allow the agent to solidify around the catheter tip before resuming injection. Reflux around the microcatheter generates a plug that allows the agent to take the path of least resistance, penetrating the nonembolized portions of the tumor (22). Additional pauses may be performed to promote penetration of new territories if needed. As with nBCA, catheter retention is a risk, and careful retraction is recommended.
Ethanol is a highly cytotoxic substance that causes endothelial injury and necrosis with consequent tumor blockage by thrombosis. Its low viscosity allows deep penetration. Vessel obliteration is considered permanent. The main risk relates to the development of cardiopulmonary collapse from pulmonary precapillary spasm (11; 31). In situations where preoperative embolization may not be possible or desirable, direct intratumoral ethanol injection has also been shown to be safe for the devascularization of hypervascular intracranial tumors (51).
Particulate embolics. Particulate embolics induce thrombosis within the embolized vessels by physically obstructing blood flow. Commonly used particulate embolics include polyvinyl alcohol, microspheres, gelatin sponge (Gelfoam), and microfibrillar collagen. PVA and microspheres in particular are available in various sizes that can be matched to the target arterial bed. Even the smallest sizes (45 to 100 µm for PVA and 50 to 150 µm for microspheres) are too large to fully penetrate capillary beds, making these less likely than liquid embolics to embolize critical non-target capillaries, such as the vasa nervorum of cranial nerves. Additionally, particulate embolics are more likely than liquid embolics to travel with the normal flow of blood and, therefore, are less likely to embolize branches to non-target tissue or enter collateral anastomoses where there is an opposing blood flow. However, embolization with particulate agents is considered more temporary than with liquid embolics because the induced thrombus can be absorbed, and the particles can dissipate over time (15). These properties make particulates well-suited for pre-operative embolization.
Particulate embolics are typically suspended in contrast to allow for visualization. They are commonly injected in a gentle pulsatile fashion to match the flow through the target artery. Injection can be performed proximal to a non-target branch if there is opposing flow through that branch. In such cases, however, careful attention must be paid to reflux into that branch, especially as the target branch begins to thrombose and flow into the non-target branches increases. Although the smallest particles provide the best tumor penetration, larger sizes may be chosen to minimize the risk of embolization of the vasa nervorum of cranial nerves.
PVA particles are micro-particles with uneven surfaces. These particles are adhesive to the endothelium and generate necrosis once they accumulate within the tumor vasculature. If not sufficiently diluted in solution, PVA particles are susceptible to aggregation that may occlude proximal vessels or clog the microcatheter.
Microspheres can be composed of tris-acryl gelatin, dextran, or copolymer. They are precisely calibrated, with consistent shape and size, translating to reliability in the caliber of the vessels blocked. Because they do not aggregate, there is superior tumor penetration and smaller chances of catheter clumping compared to PVA particles (31).
Gelfoam (Pfizer) is a water-insoluble, porous, and pliable agent. Gelfoam matrix facilitates temporary thrombus formation, completely resorbing within 4 to 6 weeks. It has the advantage of being able to reach distal vessels for occlusion due to its small particle size, but this also increases the possibility of reflux into off-target vessels (38). Gelfoam can be used for preoperative tumor embolization in both sponge and powder forms, and Gelfoam strips can be rolled into a cylinder and advanced through a catheter (40).
Detachable coils. Detachable coils may be used to sacrifice feeding arterial pedicles after liquid or particulate embolization. The purpose is to eliminate the feeding pedicle perfusion pressure, which could lead to recanalization (28). Coils may also be used to occlude a critical anastomosis that may be observed intraprocedurally, allowing for a safer continuation of the injection with less chance of embolizing non-target tissue (28; 22). Fibered coils are covered in dense polyester fibers and increase thrombogenicity to improve occlusive potential (31).
The incidence of major complications for preoperative embolization of brain, head and neck, and spinal tumors is generally reported to range from 3% to 6% (04; 05; 12). Because embolization precedes surgery, it is important to minimize the possibility of complications in the interest of patient outcomes.
Vessel injury and tumor hemorrhage. Microwire perforations of distal arterial branches and high injection pressures of embolic material or contrast agent can result in the rupture of fragile tumor vasculature and represent the primary preventable causes of intratumoral, peritumoral, and subarachnoid hemorrhage following endovascular tumor devascularization. Fortunately, periprocedural vascular injuries are usually clinically irrelevant or limited to transient headaches, focal seizures, or focal neurologic deficits (12).
Tumor swelling. Hypoxic swelling of the devascularized tumor begins immediately post-embolization and reaches its maximum after approximately 4 days (22). Steroids are, therefore, commonly administered at a bolus dose at the beginning of the embolization procedure and continued until after surgery. Patients should undergo close monitoring post-embolization, and urgent surgical intervention may be required if significant symptoms from mass effect develop.
Embolic material reflux. Inadvertent embolization of non-target tissue can occur when embolic material enters non-target arteries. This can occur during embolization of parenchymal arteries via reflux or during embolization of extracranial arteries via anastomoses with intracranial arteries (12). Thus, it is best to inject embolic material under biplane live subtraction angiography. Careful mapping of collateral anastomoses before embolization is important for safe embolization. However, potential anastomoses may not be well-visualized until the target vessels are partially embolized, so knowledge of potential collaterals is critical. For particle embolization, synchronizing the injection with the heartbeat also allows for the systolic pulse to carry particles in an anterograde fashion.
Cranial nerve injury. Terminal branches of the external carotid artery supply the transcranial and extracranial portions of most cranial nerves. Using liquid embolics or particulates smaller than 150 to 250 μm may result in cranial nerve palsy. Special care should be taken when working with the ascending pharyngeal artery (CN IX-XII), accessory meningeal artery (CN IV-VI), middle meningeal artery (CN VII), and the posterior auricular artery (CN VII) to protect their associated cranial nerves.
Meningiomas, paragangliomas, and juvenile nasopharyngeal angiofibromas are the most common tumors that warrant pre-operative embolization. Other tumors that may benefit from this treatment include hemangioblastomas, hemangiopericytomas, schwannomas, hemangiomas, primary spine tumors, and spinal metastases.
Meningiomas. Meningiomas are the most common primary central nervous system neoplasm (41). Meningiomas arise from connective tissue that surrounds the brain and encases an extensive capillary network, providing the opportunity for hypervascularized tumors to develop. Meningiomas are graded as WHO grade 1, 2, and 3 based on histopathological features, mitotic activity, and infiltration of the underlying brain. Recent advances uncovering molecular differences between meningiomas suggest that molecular profiling should be integrated into the grading process (08; 47).
Progressive neurologic symptoms may suggest a diagnosis of meningioma, but meningiomas are often found incidentally. CT or MRI reveals homogenous enhancement due to high vascularity. Digital subtraction angiogram may show a characteristic extra-axial delayed tumor blush.
Due to their meningeal origin, these tumors are usually supplied by dural arteries originating primarily from the external carotid artery. Meningiomas of the skull base or posterior fossa may be fed by dural branches from the internal carotid artery or the vertebral artery as well. Indications for treatment include progressive symptomatology, such as headaches, seizures, diplopia, or neurologic deficits due to infiltration or mass effect, and a concern for a higher grade (WHO grade 2 or 3).
For convexity meningiomas, the dural vascular supply is readily accessible during surgery and typically encountered prior to tumor resection. However, blood loss can still be significant, especially if intratumoral resection is performed (as opposed to en-bloc resection). Meningiomas may also have a fibrous or calcified consistency that hinders easy resection. In addition to decreasing intraoperative blood loss, embolization facilitates resection by causing necrosis, which can soften the tumor and make it more amenable to aspiration. A recent retrospective study revealed that preoperative embolization of meningiomas did not improve the Simpson grade of resection but was associated with prolonged recurrence-free survival (01).
Paragangliomas. Paragangliomas, also known as glomus tumors, are tumors arising from neuroendocrine cells of the autonomic neural system in the paravertebral sympathetic and parasympathetic chains. Although typically noninvasive, they do have the potential to metastasize. Paragangliomas are typically sporadic, affect adults, and present as a palpable mass or cranial nerve palsy due to mass effect. Clinical manifestations depend on the location, size, and neuroendocrine function.
The nomenclature of these neck tumors is based on their origin. Carotid body paragangliomas (glomus caroticum) are the most common and often present as a painless mass at the carotid bifurcation. Tympanic paragangliomas (glomus tympanicum) develop in the middle ear along the temporal bone and may cause hearing loss, pulsatile tinnitus, and a retrotympanic vascular mass due to tympanic nerve involvement. Glomus jugulare tumors may present with hoarseness due to lower cranial nerve palsy related to tumor presence in the jugular fossa. Vagal paragangliomas are often diagnosed as a mass at the angle of the mandible that grows near the vagus nerve, causing vagal and hypoglossal nerve dysfunction.
Like meningiomas, the vascularity of paragangliomas makes them apparent on CT or MRI with homogenous contrast enhancement. Uptake of radiolabeled octreotide can corroborate the diagnosis preoperatively. On angiography, enlarged arterial feeders with intense tumor blush can often be appreciated alongside rapid venous drainage. Characteristically, carotid body tumors will splay the external and internal carotid arteries further apart. In contrast, glomus vagale tumors will displace the internal and external carotid arteries anteriorly and the internal jugular vein posteriorly (22). The ascending pharyngeal artery, a branch of the external carotid artery, is a common feeding branch, but other external carotid artery branches may be involved. Preoperative embolization of paragangliomas is generally indicated due to the potential for surgical blood loss, particularly in lesions larger than 3 cm (50). However, although most studies report preoperative embolization to be safe and effective in these tumors (50; 53; 33; 30), some studies have shown no significant impact on surgical outcomes (55; 26). As with embolization of any external carotid artery branch, anastomoses to the intracranial arterial supply or to arteries that supply cranial nerves must be identified prior to embolization. In particular, embolization of glomus tumors risks cranial nerve palsies from embolization of ascending pharyngeal branches supplying the vasa nervorum of several cranial nerves (21).
Juvenile nasopharyngeal angiofibroma. Although rare, juvenile nasopharyngeal angiofibroma is the most common tumor of the nasopharynx (52). It usually presents in male patients during adolescence as nasal obstruction and recurrent epistaxis. According to tumor size and the direction of growth, patients might develop sinusitis, facial swelling, and proptosis. A reddish-gray sessile, lobulated, and encapsulated mass might be observed on endoscopic examination. Juvenile nasopharyngeal angiofibromas are benign tumors that might be locally aggressive, with rare malignant conversion (52).
Histologically, these tumors are mainly formed of a thin-walled vascular tissue with fibrous stroma and rare muscular fibers. Grading is based on tumor extent and invasion of adjacent spaces as seen on noninvasive imaging. Lower-grade tumors are confined to the nasopharynx, with higher grades assigned on extension into sinuses, pterygopalatine fossa, infratemporal fossa, and intracranial skull base (02). Although bone invasion is rare, remodeling and erosion are common.
Diagnostic angiography usually demonstrates an early and intense blush persisting into the venous phase (02). These tumors are fed by distal branches of the internal maxillary artery. As the tumor enlarges, other vascular territories may be recruited, such as the ophthalmic artery (22). Since their blood supply can be bilateral, it is important to perform angiograms of both carotids. Preoperative embolization may be useful in larger tumors and in those that extend intracranially. Preliminary studies have suggested that embolization of juvenile nasopharyngeal angiofibromas with Onyx may offer a greater degree of devascularization than other embolic agents (23). Their nasopharyngeal location makes them suitable for embolization by direct puncture as an alternative to transarterial therapy. In small studies, direct puncture has been associated with decreased intraoperative blood loss and greater tumor devascularization compared to transarterial therapy (13; 14).
Spinal tumors. Bony vertebral metastases from breast, lung, prostate, kidney, and thyroid cancers are common and have been found in as high as 70% of terminal cancer patients (18). Spinal metastases are associated with devastatingly high morbidity and are generally an end-stage development in cancer progression (10). Surgical interventions have historically been palliative in nature. Recent advances in spine surgery, such as the development and popularization of minimally invasive spine surgery and stereotactic radiosurgery, have improved outcomes in the management of spinal metastases (10). In particular, renal cell, breast, and thyroid metastases can be hypervascular, posing challenges to surgical resection.
Although rare, several hypervascular primary spinal tumors also exist, including giant cell tumors, multiple myelomas or plasmacytomas, hemangiomas, aneurysmal bone cysts, meningiomas, and hemangioblastomas (41).
Preoperative embolization is increasingly recognized as a viable option for reducing intraoperative surgical complications, primarily blood loss (37; 24). Its efficacy has been explicitly demonstrated in a variety of tumors, including giant cell tumors of the sacrum and spine (56). A 2016 systematic review and meta-analysis involving 1305 patients and 37 studies found that preoperative embolization of spinal tumors is safe and effective (27). However, a more recent systematic review published in 2020 involving 11 studies and 839 patients uncovered that only tumors specifically identified as hypervascular on angiography benefit from decreased intraoperative blood loss (25). This finding has been corroborated by a second meta-analysis involving 12 studies and 744 patients (19). Furthermore, a retrospective review of 62 patients undergoing preoperative embolization of spinal tumors found that subsequent estimated intraoperative blood loss was associated with tumor volume, surgical approach, and invasiveness of the surgery but not tumor vascularity or degree of embolization (39). Given these findings, it is worth noting that transarterial chemoembolization is an effective alternative strategy for pain relief in hypervascular spinal metastatic tumors (07). Hypervascularity may not be restricted to classically vascular tumors, such as renal cell carcinoma, and has been reported in patients with breast and prostate cancers (37). Preoperative embolization may, therefore, be considered for any patients undergoing surgical resection of spinal metastasis.
Contraindications to preoperative embolization of brain, head and neck, and spinal cord tumors include patient and anatomical factors. Given that embolization is typically performed under general anesthesia and can last several hours, patient comorbidities that increase the risk of general anesthesia may alter the risk/benefit profile of embolization. Therefore, the potential for significant intraoperative blood loss must be carefully considered. More important are anatomic factors that increase the risk of embolization, including anastomoses to arteries supplying the brain, cranial nerves, or spinal cord that can be put at risk during embolization. Careful angiography evaluation is, therefore, necessary to identify or exclude such potential anastomoses prior to embolization. The presence of such anastomoses does not necessarily preclude safe embolization but may alter the choice of embolic agent and the extent of embolization. Importantly, the overall risks and benefits of embolization must be carefully weighed in the context of the potential surgical risks.
Head and neck tumors can be embolized with liquid agents (such as NBCA, Onyx, or ethanol) or particles (such as polyvinyl alcohol, embolic spheres, and Gelfoam). The capillary bed of head and neck tumors is approximately 200 μm; therefore, 150 to 250 μm particles are most appropriate (28; 42). Smaller particles should be avoided to preserve vasculature distal to tumor beds (42). Liquid agents, such as ethanol, NBCA, and Onyx, may be used by experienced operations with high diffusion capacity and potential for complications in mind (34; 15; 13; 14; 21; 24; 27). Thus, operator experience, tumor characteristics, and the properties of the embolic agent must be considered when choosing the agent used. An advantage to particles is that they can be used in patients under conscious sedation, which facilitates intraoperative neurologic monitoring. The use of DMSO with Onyx and the use of NBCA may cause significant pain, so these agents may require the administration of steroids or utilization of general anesthesia.
Preoperative embolization therapy is technically successful in most cases. A prominent decrease in tumor blush on angiography is generally accepted (12; 37; 32). However, most studies report nonmatched samples in a retrospective fashion, making it difficult to quantify the clinical benefit. In the few controlled trials conducted, results have been mixed, and it is unclear whether the benefits outweigh the risks (37; 09; 32). Although extensive tumor devascularization can be achieved, Iacobucci and colleagues found that increased radiation exposure, extended duration of procedures, and related complications may not necessarily justify the technique (32). The incidence of cranial nerve injury is particularly concerning and has at least been reported in embolization of glomus jugulare and carotid body tumors (17; 20; 21; 43; 44). In a retrospective study by Gaynor and colleagues, devascularization of glomus jugulare tumors resulted in permanent cranial nerve palsies in 2 of 11 patients, one of the facial nerve (CN VII) and one of the lower cranial nerves (CN IX – XII) (21). Others have also reported facial nerve palsies in the preoperative embolization of jugular paragangliomas with both particulate and liquid embolic agents (20; 43). Fernandez-Torron and colleagues reported a case of Brown-Sequard syndrome in a patient undergoing embolization of a vertebral hemangioma (17). Thus, careful patient selection is critical.
Direct tumor puncture has been established as an alternative to the transarterial route for treatment of paragangliomas and juvenile nasopharyngeal angiofibromas (13; 14; 16). Elhammady and colleagues reviewed vascular tumor embolization for various head, neck, and spinal lesions with Onyx in 43 patients (13; 14). In their series, the intraparenchymal penetration of Onyx was greater in the tumor puncture cases than the transarterial cases, but the mean percentage of tumor devascularization estimated by change in tumor blush was similar. Still, the mean intraoperative blood loss was lower in tumors with intraparenchymal penetration (459 ml) than transarterial (2689 ml) (13). In a review by Felbaum and colleagues, direct puncture embolization of carotid body tumors was also shown to be safe and efficacious in reducing intraoperative bleeding (16). However, at least one case has been reported of the development of Horner syndrome 10 hours after direct carotid body tumor embolization with Onyx (54).
Given the potential of anastomotic arterial connections and the possibility for embolic material to diffuse into unintended vasculature, the choice of embolic agent is extremely important. As previously noted, smaller particles and less viscous agents might migrate from the external carotid artery toward the internal carotid or vertebral arteries during the tumor embolization procedure. This could generate inadvertent ischemia of the retina (through the ophthalmic artery), the cranial nerves (through embolization of the vasa nervorum), or the brain parenchyma. The embolization of external carotid artery branches may also lead to mucosal and tongue necrosis as well as damage to the larynx (22). Devascularization of glomus jugulare tumors with Onyx can also result in a high incidence of irreversible cranial palsies (21). However, nearly all studies published to date have been in relatively few patients, and larger sample sizes are needed to gain a more accurate estimate of cranial nerve palsies following preoperative embolization of cranial, head and neck, and spinal tumors.
In spinal cases, particles may dislodge through intersegmental anastomoses and generate spinal cord ischemia. Thus, small-sized particles should be avoided because they may block arterial flow to the spinal carotid at levels with inadequate or absent collateral supply. Likewise, embolization in cervical tumors requires careful attention due to potential anastomoses between the carotid, vertebral, and subclavian arteries. Direct tumor puncture may be considered for cervical vertebral body lesions if feeders are too small for safe catheterization.
With an estimated complication rate ranging from 3% to 6% (04; 05; 12; 27), preoperative embolization of cranial, head and neck, and spinal tumors is generally safe for the vast majority of patients. Newer meta-analyses suggest that complication rates in patients undergoing preoperative embolization may be equal to those not undergoing preoperative embolization (19). However, as previously discussed, numerous complications have been reported in the literature, and extreme caution is warranted to prevent damage to nearby structures.
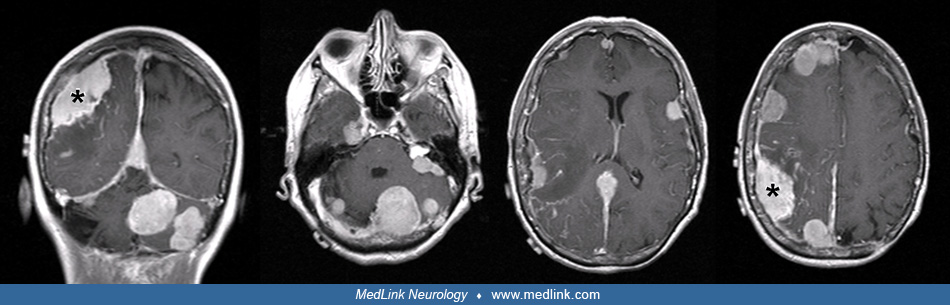
Case 1. A 67-year-old female with neurofibromatosis type 2, bilateral acoustic schwannomas, and multiple meningiomas was found to have a rapidly enlarging right parietal meningioma causing mass effect. The meningioma was targeted for presurgical embolization.
Under general anesthesia, a load of intravenous heparin was given and ACT checked hourly to levels between 250 to 300 seconds. A 6F Envoy catheter was navigated over a 0.038-inch glidewire across the aortic arch and maneuvered in to the RICA artery. Under magnified roadmap guidance, a Marathon microcatheter was advanced over a shaped Mirage microwire into the right middle carotid artery. A moderate tumor blush from the distal parietal middle carotid artery branches was observed. The microcatheter was then carefully navigated distally into each of the 2 feeding pedicles, one at a time.
After a microinjection through the microcatheter, DMSO was infused at a rate of 0.1cc/ min (0.3cc total) through the microcatheter in each pedicle, which were then embolized with Onyx-18 until there was reflux back toward the catheter (0.2cc). The microcatheter was removed, and final AP/lateral angiograms were obtained, demonstrating substantial decrement in the tumoral capillary blush.
Case 2. A 61-year-old male with hepatocellular carcinoma developed cord compression and progressive lower extremity weakness related to metastatic disease to the spine. Because a previous resection attempt had been aborted due to excessive tumor bleeding, presurgical embolization was performed.
A 5-French Cobra catheter was advanced over a 0.038 inch Glidewire, and a selective segmental artery angiogram was done from T5 to T12 bilaterally, revealing tumor blush from the right T9, T10, T11, and left T9 and T10 radicular arteries. An Echelon 14 microcatheter was advanced over a shaped Synchro micro-wire into the radicular branch of right T9 where a microangiogram was performed. Concentric microspheres of 100 to 300 µ were prepared in a contrast-saline mixture and titrated to a uniform and diffuse suspension. They were then injected under subtracted roadmap guidance until stagnation was seen in the radicular artery. The Echelon catheter was removed, and a Prowler select catheter was navigated over the microwire into the radicular branch and flushed with 5% dextrose solution; nBCA glue (proportion of 3:1) was injected to occlude the proximal radicular artery and branches.
Of note, the dilution ratio of Ethiodol to N-butyl cyanoacrylic acid determines the depth to which penetration of glue is desired. A ratio of one part Ethiodol to one part NBCA (1:1) polymerizes very rapidly after entering in contact with blood, whereas a ratio of (3:1) allows more penetration. The same process was done at the level of right T10 and left T9. The right T11 was only injected with nBCA.
Although tumor blush was observed during left T10 radicular artery injection, embolization was not performed as this branch also gave rise to the artery of Adamkiewicz. After treatment, no tumor blush could be appreciated.
Preoperative embolization of hypervascularized tumors, such as meningiomas, paragangliomas, juvenile nasopharyngeal angiofibromas, and spinal metastases, has been shown to reduce intraoperative blood loss and operative time (53; 12; 37; 24; 27; 32; 55; 10; 19; 25; 26). Although the goal of embolization is to aid surgical resection and is theorized to reduce surgical complications and improve patient outcomes, embolization may also be used as a direct route for chemotherapeutic agent delivery (03; 07).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Matthew Potts MD
Dr. Potts of Northwestern University Feinberg School of Medicine has no relevant financial relationships to disclose.
See ProfileKhizar Nandoliya
Mr. Nandoliya of Northwestern University Feinberg School of Medicine has no relevant financial relationships to disclose.
See Profile
Rimas V Lukas MD
Dr. Lukas of Northwestern University Feinberg School of Medicine received honorariums from Jazz Therapeutics, Novocure, and Servier for speaking engagements, honorariums from Cardinal Health, Catalyx, Merck, and Novocure for advisory board membership, research support from BMS as principal investigator, and an honorarium from GT Medical Technologies for DSMB membership.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
May. 27, 2026
Neuro-Oncology
May. 27, 2026
Neuro-Oncology
May. 23, 2026
Neuropharmacology & Neurotherapeutics
May. 11, 2026
Stroke & Vascular Disorders
May. 03, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026