





















Infectious Disorders
Arboviral encephalitis
May. 15, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author explains the clinical presentation, pathophysiology, prevention, diagnostic work-up, and management of West Nile virus infection.
|
• Most people who have been bitten by West Nile virus-infected mosquitoes have no symptoms or only mild ones. | |
|
• Approximately 20% to 30% of infected individuals develop a mild illness resembling the flu. Mild illness is referred to as West Nile fever. Symptoms of mild illness can include sudden onset of fever with malaise, anorexia, nausea, vomiting, diarrhea, headache, photophobia, neck pain and stiffness, myalgias, maculopapular rash, and lymphadenopathy. | |
|
• Only one person out of every 150 to 250 infected individuals develops severe disease. Severe neurologic illness may include encephalitis, meningoencephalitis, or poliomyelitis. Symptoms of severe disease can include high fever; nuchal rigidity; confusion, disorientation, obtundation, and memory loss; severe muscle weakness; or paralysis, tremors, and seizures. | |
|
• Cases of poliomyelitis in patients with West Nile virus infection have been identified since July 2002. In most cases, limb weakness is associated with signs and symptoms of encephalitis or meningitis. Cases were typically admitted with a 1- to 4-day history of symptoms, including fever, chills, vomiting, headache, fatigue, lethargy, confusion, myalgias, and facial and acute asymmetric painless limb weakness. Physical examination demonstrated asymmetric hyporeflexic or areflexic weakness of various extremities, generally with intact sensation. Several patients developed acute respiratory distress requiring ventilatory support. | |
|
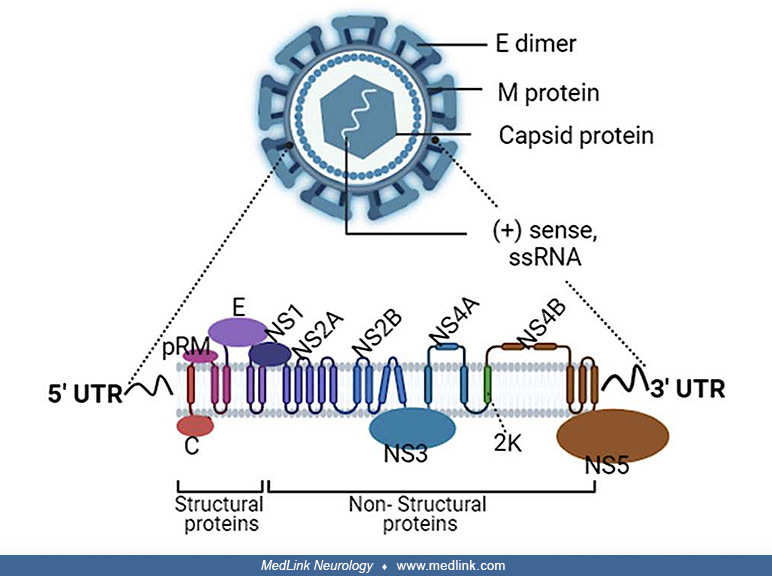
• West Nile virus is a flavivirus belonging to the Japanese encephalitis subgroup. This subgroup also includes the serologically closely related St. Louis encephalitis virus. Flaviviruses are small single-stranded RNA viruses, with a spherical envelope between 40 and 50 nm. | |
|
• West Nile virus is usually transmitted by Culex mosquitoes from infected birds. | |
|
• West Nile virus (as with other arboviruses) is typically inoculated by mosquitoes directly into the bloodstream or subcutaneous tissue. Initial West Nile virus replication occurs in the skin and regional limb nodes, followed by a primary viremia that seeds the reticuloendothelial system, and then a secondary viremia following replication in the reticuloendothelial system. Depending on a number of host factors, including the integrity of the blood-brain barrier, the central nervous system may be seeded during the secondary viremia. | |
|
• Penetration of West Nile virus into the central nervous system depends heavily on the degree and persistence of viremia but is also facilitated by altered blood-brain barrier permeability (eg, from hypercarbia, hyperosmotic agents, and mechanical disruption). | |
|
• About half of people who develop West Nile virus encephalitis or meningitis have persistent symptoms at 6 months, and only about one third are fully recovered after 12 months. | |
|
• Other than mosquito-borne transmission, mechanisms of documented transmission of West Nile virus include blood transfusion, organ transplantation, breast-feeding, transplacental, dialysis-related, and occupational (eg, laboratory workers infected by percutaneous inoculation and possibly through aerosol exposure). | |
|
• West Nile virus or another arbovirus (eg, St. Louis encephalitis virus) should be strongly considered in patients with unexplained encephalitis or meningitis in late summer or early fall. | |
|
• Serologic testing for West Nile virus can be problematic because samples obtained within 8 days of infection may be falsely negative due to cross-reactivity between West Nile virus and other flaviviruses and because of persistence of IgM antibodies. Also, West Nile virus IgM antibodies can persist for more than a year after initial infection, potentially producing confusion over whether the antibodies are a marker of current or previous infection. | |
|
• Although no specific treatment is approved for West Nile virus infection, intensive supportive care is sometimes needed, including hospitalization and ventilator support. |
West Nile virus was first isolated in 1937 in a febrile woman from the West Nile district of Uganda (120; 161). The virus was recognized as an arbovirus after it was isolated from mosquitoes, birds, and humans. In the 1950s outbreaks of the disease occurred in the Middle East, with identification of a nonfatal encephalitic form (161). The first major urban outbreaks occurred in Romania in 1996, where there were 17 deaths among 800 cases (33; 65; 297; 116; 161), and in Russia in 1999, where there were 40 deaths among more than 800 cases (241; 161).
By the 1990s West Nile virus was recognized in Africa, Europe, the Middle East, and Asia, but it was not identified in the Western Hemisphere until it was identified in the United States in 1999 (161). In 1999 an outbreak was identified in New York City, with seven deaths among 62 human cases (34; 35; 271; 84; 205; 210; 121; 161). The epidemic coincided with the deaths from West Nile virus of several thousand crows and the deaths of exotic birds at the Bronx and Queens zoos. The viral genome in the 1999 New York City outbreak was almost identical to that of a West Nile virus strain identified in Israel in 1998, suggesting that it originated in the Middle East (160; 97). The virus was found to overwinter in mosquitoes (37; 157).
Since 1999, the virus spread along the East Coast and then progressively westward to include almost the entire continental United States by the end of 2002 (69; 183; 298; 316; 38; 133; 235; 233; 121). The 2002 and 2003 West Nile virus epidemics in the United States were the largest arboviral meningoencephalitis epidemics ever documented in the western hemisphere and the largest West Nile virus meningoencephalitis epidemics ever recorded (216; 122). In the first 5 years after its introduction in the United States, West Nile virus spread to the 48 contiguous states and caused 667 reported deaths (111). Through 2013, there were approximately 39,500 confirmed and probable cases of symptomatic West Nile virus-related disease in the United States reported to the Centers for Disease Control and Prevention, including 17,319 cases (44%) with neuroinvasive disease and 1663 deaths. About 9% of neuroinvasive disease cases are fatal compared to 0.5% of non-neuroinvasive cases (177). It is likely that substantially more than 1 million people have been infected by the West Nile virus in the United States (24; 73); however, because many infected people do not develop serious symptoms and because surveillance systems are still developing, the true cumulative incidence is unknown. These epidemics have had tremendous economic impact across the country (326).
• Most people who have been bitten by West Nile virus-infected mosquitoes have no symptoms or only mild ones. | |
• Approximately 20% to 30% of infected individuals develop a mild illness resembling the flu--West Nile fever. | |
• Severe illness can occur in individuals of all ages, but only about one person out of every 150 to 250 infected individuals develops severe disease. | |
• Most cases of West Nile virus encephalitis are actually cases of meningoencephalitis with cerebrospinal fluid abnormalities similar to those of meningitis cases. | |
• A wide range of neuroinvasive disease is recognized, including encephalitis, meningoencephalitis, poliomyelitis, various movement disorders, cochlear-vestibular impairment, brachial plexopathy, subacute brachial diplegia, stroke associated with central nervous system vasculitis, and a clinical constellation of fever, altered mental status, and seizures resembling herpes simplex encephalitis. |
Most people who have been bitten by West Nile virus-infected mosquitoes have no symptoms or only mild ones. Approximately 20% to 30% of infected individuals develop a mild illness resembling the flu. Mild illness is referred to as West Nile fever. Symptoms of mild illness can include sudden onset of fever with malaise, anorexia, nausea, vomiting, diarrhea, headache, photophobia, neck pain and stiffness, myalgias, maculopapular rash, and lymphadenopathy (226; 85; 33; 144; 234; 186; 294).
Severe illness can occur in individuals of all ages, but only about one person out of every 150 to 250 infected individuals develops severe disease (205; 24; 32). Severe neurologic illness may include encephalitis, meningoencephalitis, or poliomyelitis. Of the 1425 neuroinvasive disease patients in the United States in 2017, 714 (50%) had encephalitis, 530 (37%) had meningitis, 86 (6%) had acute flaccid paralysis, and 92 (6%) had other neurologic illnesses (71). Acute flaccid paralysis may occur in isolation or in conjunction with other nervous system involvement; indeed, of those with acute flaccid paralysis, in 2011 93% also had encephalitis or meningitis whereas in 2017 only 38% also had encephalitis or meningitis (63; 71). Common symptoms and signs in the collective group with neuroinvasive disease include fever, headache, anorexia, nausea or vomiting, focal muscle weakness, walking instability, memory impairment, difficulty concentrating, confusion, depression, tremor, diplopia, nystagmus, dizziness, and fatigue (09; 290; 224; 149; 213; 251).
Most cases of West Nile virus encephalitis are actually cases of meningoencephalitis with cerebrospinal fluid abnormalities similar to those of meningitis cases (299; 300; 195). Symptoms of severe disease can include high fever; nuchal rigidity; confusion, disorientation, obtundation, and memory loss; severe muscle weakness; or paralysis, tremors, and seizures (33; 210; 234; 125; 235; 268; 269; 103; 259; 224). Some patients may develop cerebral edema; coma; aphasia; ataxia; tremor; myoclonus; parkinsonism; acute demyelinating polyneuropathy; multifocal neuropathies, brachial plexopathy, or polyradiculitis; hyperreflexia; oculomotor abnormalities; cranial neuropathies (especially peripheral facial paresis, which may be bilateral like with Lyme neuroborreliosis); multifocal chorioretinitis; dysarthria; breathing difficulties; myositis; rhabdomyolysis; autonomic instability; and myocarditis, pancreatitis, or hepatitis (210; 282; 304; 268; 299; 02; 07; 187; 246; 284; 294; 107; 244; 287; 163; 212; 289). Tremor (either postural or kinetic) and myoclonus are common; such hyperkinetic movement disorders in association with aseptic meningitis should suggest West Nile virus infection (299; 294).
Falcinella and colleagues reported an 85-year-old woman who was admitted with a 4-day history of fever and dysuria and treated at home with azithromycin (83). She had briefly been disoriented. On initial evaluation she was afebrile and eupneic but hypoxic in ambient air, with no other evident salient abnormalities on physical examination. Shortly after, the patient became agitated, febrile, and oliguric. Her condition deteriorated with persistence of high-grade fever and worsening mental status, and she ultimately became comatose with persistent involuntary movements. Neurologic exam revealed nuchal rigidity with cervical pain on neck flexion, poorly comprehensible speech, impaired execution of simple tasks, and diffuse limb tremors but no focal neurologic signs. Laboratory studies showed increased CRP (68.3 mg/L) and neutrophilic leukocytosis. CSF examination showed slight xanthochromia, 1000 RBC/mm3, 760 WBC/mm3 (polymorphonuclear), protein 430 mg/dl, glucose 46 mg/dl, and a CSF/serum glucose ratio of 0.46. She was treated with vancomycin, meropenem, and antiepileptic medications. All microbiological studies on blood, urine, and CSF were negative. EEG showed bilateral slow-waves from central-anterior leads. Brain MRI showed irregular, nonspecific lobar white matter hyperintensities on T2-weighted sequences. Her level of consciousness gradually started improving. On the twelfth day of hospitalization, PCR for West Nile virus from blood and urine specimens was positive, whereas serology was positive only for IgM. She was discharged to rehabilitation with residual cognitive and motor impairment.
West Nile virus retinopathy occurs in one fourth of patients with a history of West Nile virus infection and is more frequently observed in those with apparent severe neurologic sequelae (eg, West Nile virus encephalitis) (117; 151). Multifocal chorioretinitis has been reported in 75% of patients who present with West Nile virus meningoencephalitis (02; 305).
(A) In the right eye, fluorescein angiography showed hyperfluorescent lesions with a linear distribution, corresponding to the hypocyanescent lesions in indocyanine green angiography (ICGA). (B) In the left eye, fundus autofluo...
Optical coherence tomography angiography at the level of the lesions in the right eye in multifocal chorioretinitis due to acute West Nile virus infection. (A) OCT en face. (B) OCTA showed diffuse capillary network attenuation ...
(A) In the right eye, OCT at the level of the lesions showed recovery of the retinal pigmented epithelium and the ellipsoid zone. (B) In the left eye, OCT showed a reduction in the hyperreflective oval deposit on the retinal su...
West Nile virus retinopathy is characterized by multifocal chorioretinitis (with or without vitreous inflammatory changes), typically with linear clustering of chorioretinal scars that sometimes follow the course of retinal nerve fibers (117). West Nile virus retinopathy is also associated with abnormal reflexes on neurologic examination, poorer learning, greater dependence in activities of daily living, and a lower quality of life (117).
Other ocular manifestations described in West Nile virus infections include uveitis, retinitis, retinal hemorrhages, vascular leakage, vasculitis, macular edema, and optic disc swelling (117). Various neuropathalmologic manifestations have also been described, including optic neuritis, oculomotor palsies, opsoclonus-myoclonus, downbeat nystagmus, ocular flutter, and ocular dysmetria (246; 07; 244).
Cases of poliomyelitis in patients with West Nile virus infection have been identified since July 2002 (mean age is 55 years) (40; 98; 164; 132; 30; 296; 113; 159; 10). In most cases, acute flaccid limb weakness is associated with signs and symptoms of encephalitis or meningitis. Cases were typically admitted to the hospital with a 1- to 4-day history of symptoms, including fever, chills, vomiting, headache, fatigue, lethargy, confusion, myalgias, and facial and acute asymmetric painless limb weakness. Cases of West Nile virus-related poliomyelitis can present with an atypical temporal pattern of limb weakness, including onset several weeks after illness onset, and relapsing or recurrent limb weakness following a period of clinical plateauing or improvement (267). Physical examination demonstrated asymmetric hyporeflexic or areflexic weakness of various extremities, generally with intact sensation. Several patients developed bowel or bladder dysfunction and acute respiratory distress requiring ventilatory support.
A wide spectrum of movement disorders occurs with neuroinvasive West Nile virus infections, including opsoclonus-myoclonus, opsoclonus-myoclonus-ataxia syndrome (OMAS), myoclonus, ataxia, chorea, tremor, parkinsonism, and stiff-person syndrome (118; 167; 272). West Nile virus-associated movement disorders typically have an indolent course and resolve within a period of weeks to months. The most common type of tremor is an action tremor of the upper extremities, which is usually bilateral. Tremor in patients with meningitis subsides earlier than that in patients with encephalitis or acute flaccid paralysis. Opsoclonus-myoclonus responds well to intravenous immunoglobulins. Other neurologic presentations of West Nile virus infection include cochlear-vestibular impairment (223; 245); brachial plexopathy (66); postinfective brachial plexopathy consistent with Parsonage-Turner syndrome (260); subacute brachial diplegia (324); stroke associated with CNS vasculitis (04); altered mental status and fever of unknown origin (136); and a clinical constellation of fever, altered mental status, and seizures resembling herpes simplex encephalitis (250). Cases of myasthenia gravis have also presented within several months of West Nile virus infection, but whether this is simply incidental is not clear (165); a case control study found no significant association of myasthenia gravis with West Nile virus infection (08). A pattern of severe persistent chills mimicking malaria has also been reported (70).
Post-infection fatigue is common after West Nile virus infection, particularly among females, those younger than 50 years of age, and those with symptomatic clinical West Nile virus disease (91). Proinflammatory and antiviral cytokines are significantly elevated in those reporting fatigue after Went Nile virus infection compared to those not reporting fatigue (91).
Symptoms of mild illness generally last from several days to a week. Symptoms of severe disease can last for weeks, and in some cases, neurologic effects can be permanent (214). Risk factors for developing West Nile encephalitis or other neuroinvasive disease include diabetes, hypertension, cardiovascular disease, alcoholism, immunosuppression, male sex, older age, and posttransplant status (18; 206; 58; 131; 109; 323; 77; 01).
Among patients hospitalized for West Nile virus disease, 30% to 40% are discharged to long-term care facilities, and more than 50% have long-term sequelae (104). Physical and mental functions seem to improve or normalize within about a year (178), but about half of affected individuals have persistent symptoms at 6 months (68), and only about one third of people who develop West Nile virus encephalitis or meningitis are fully recovered after 12 months (143; 300; 312). Younger age at infection is a significant predictor of recovery (143). Most survivors regain independence, although residual neuropsychiatric problems and weakness are common (132; 277; 68; 213).
In a long-term follow-up study of 30 cases referred for neuromuscular and electrodiagnostic evaluation based on abnormal findings after West Nile virus infection, a third showed abnormalities on nerve conduction or needle electromyography due to primary or secondary outcomes of West Nile virus infection (10); the most common electrodiagnostic findings and causes of long-term disability were related to West Nile virus poliomyelitis, and the electrodiagnostic findings in these cases were similar to those observed in chronic poliomyelitis (10).
Motor recovery following West Nile virus-associated flaccid paralysis may continue over 18 months or more (182), but residual weakness is common (266). Recovery time is longer in patients with preexisting comorbid conditions (178; 68), and hypertension and diabetes have been linked to persistent symptoms (68).
In a systematic review and meta-analysis, subjective neurocognitive impairment, most notably fatigue (37%–75%), memory concerns (11%–57%), concentration deficits (17%–48%), and depression (17%–38%), were common at post-hospitalization follow-up (251).
Between 3% and 20% of patients who develop a severe illness ultimately die of their illness (218; 177); most deaths are reported in people older than 50 years of age. Increasing age, particularly age over 70 years, is a major risk factor for both severe meningoencephalitis and death (94; 18; 206). Other risk factors for death associated with West Nile neuroinvasive disease include absence of pleocytosis in the cerebrospinal fluid, presence of myoclonus or tremors, loss of consciousness, history of stroke, need for intubation and mechanical ventilation, chronic renal failure, hepatitis C infection, diabetes, hypertension, immunosuppression, and black race (18; 206; 266; 207; 251).
New neurologic abnormalities may develop over the first decade after West Nile virus infection regardless of initial clinical infection (313). In the Houston West Nile Cohort Study, the majority of patients (86%) with encephalitis (n=35) had abnormal neurologic exam findings at the time of the first assessment 1 to 3 years after West Nile virus infection, compared with uncomplicated fever (27%) and meningitis (36%) cases. At the time of the second assessment 8 to 11 years after West Nile virus infection, 57% of West Nile fever (n=7), 33% of West Nile meningitis (n=6), and 36% of West Nile encephalitis (n=14) cases had developed new neurologic complications. The most common abnormalities noted were impaired tandem gait, hearing loss, abnormal reflexes, and muscle weakness. Long-term neurologic abnormalities were most commonly found in patients with West Nile virus encephalitis.
|
• West Nile virus is a flavivirus belonging to the Japanese encephalitis subgroup. | |
|
• West Nile virus (as with other arboviruses) is typically inoculated by mosquitoes directly into the bloodstream or subcutaneous tissue. | |
|
• Flaviviruses (including West Nile virus) bind to a specific cell surface protein and then enter target cells by a vesicle-mediated process (ie, so-called receptor-mediated endocytosis). | |
|
• Penetration of West Nile virus into the central nervous system depends heavily on the degree and persistence of viremia but is also facilitated by altered blood-brain barrier permeability (eg, from hypercarbia, hyperosmotic agents, and mechanical disruption). | |
|
• The clinical, laboratory, and electrophysiologic abnormalities in most patients with asymmetric flaccid paralysis result from a polio-like syndrome with involvement of spinal cord anterior horn cells and motor nerve axons |
West Nile virus. West Nile virus is a flavivirus belonging to the Japanese encephalitis subgroup. This subgroup also includes the serologically closely related St. Louis encephalitis virus. Flaviviruses are small single-stranded RNA viruses, with a spherical envelope between 40 and 50 nm.
Flavivirus structural proteins are now designated E (envelope), C (core), and M (membrane-like), replacing older terminology of V3, V2, and V1, respectively (161). The E protein is the major constituent of the viral surface and is oriented parallel to the viral surface. The E protein is a class II viral fusion protein that mediates both the binding of West Nile virus to target cell receptors and the entry of West Nile virus into the target cells. The E protein differs structurally from the spikey projections of class I viral fusion proteins seen in other viruses (eg, orthomyxoviruses, paramyxoviruses, retroviruses, and filoviruses). Also, unlike class I viral fusion proteins, the E protein itself is not proteolytically cleaved for activation but instead requires cleavage of an accessory protein. Fusion in West Nile virus is faster and less temperature-dependent than fusion in viruses with class I fusion proteins.
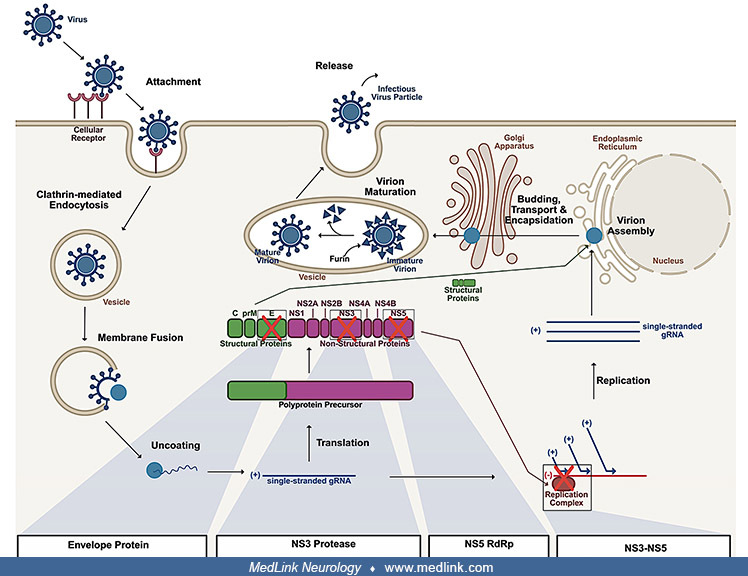
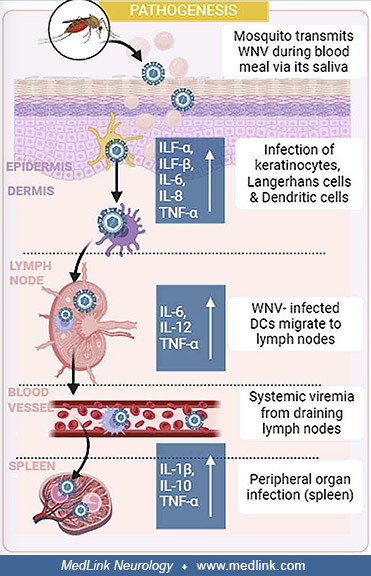
Pathogenesis of human infection with West Nile virus. West Nile virus (as with other arboviruses) is typically inoculated by mosquitoes directly into the bloodstream or subcutaneous tissue. Initial West Nile virus replication occurs in the skin and regional limb nodes, followed by a primary viremia that seeds the reticuloendothelial system, and then a secondary viremia following replication in the reticuloendothelial system (161). Depending on various host factors, including the integrity of the blood-brain barrier, the central nervous system may be seeded during the secondary viremia (161).
Flaviviruses (including West Nile virus) bind to a specific cell surface protein and then enter target cells by a vesicle-mediated process (ie, so-called receptor-mediated endocytosis) (161). Because of the wide host range of natural West Nile virus transmission, the cell surface protein target is likely to be highly conserved across different species. This target cell receptor molecule is a 105-kDa plasma membrane-associated glycoprotein.
Irreversible conformational changes in the E protein and viral uncoating occur at acidic pH within the endocytic vacuoles after which the viral genome is released into the cytoplasm for replication (161). Virus assembly takes place in the endoplasmic reticulum. Initially, the E protein forms a stable heterodimeric complex with the precursor of the M protein. The precursor M protein is cleaved by a protease in the Golgi system to generate fusion-competent mature infectious virions.
Following peripheral inoculation by the bite of a mosquito, initial West Nile virus replication is believed to occur in skin Langerhans dendritic cells, which migrate to draining lymph nodes where further replication ensues, leading to primary viremia and resulting infection of peripheral tissues (258). West Nile virus is cleared from the serum and peripheral tissues by the end of the first week. Detection of and recovery from West Nile virus infection depend on the ability of class I HLA molecules to reveal conserved West Nile virus epitopes to the cellular immune system that recognizes infected cells (196).
Loss-of-function mutations in the chemokine receptor CCR5 (including homozygosity for CCR5Delta32, a common mutant allele) has been associated with severe symptomatic West Nile virus infection in patients who present with clinical disease (99; 100; 76; 169; 170; 171). CCR5 normally mediates leukocyte chemotactic responses in antimicrobial host defense but was identified in 1996 as a crucial host factor exploited by HIV for cell entry (169). In West Nile virus infections, CCR5 acts by regulating trafficking of leukocytes to the infected brain (99). CCR5 deficiency is not a risk factor for West Nile virus infection per se, but it is a risk factor for both early and late clinical manifestations after infection (171). Thus, CCR5 may function normally to limit disease due to West Nile virus infection in humans.
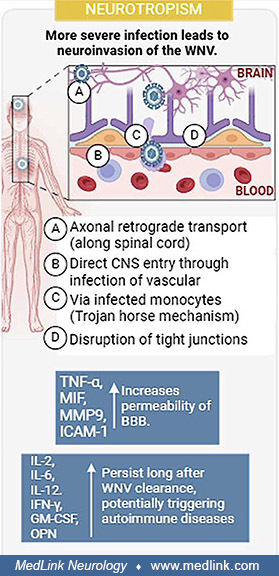
Central nervous system infection with West Nile virus. Penetration of West Nile virus into the central nervous system depends heavily on the degree and persistence of viremia but is also facilitated by altered blood-brain barrier permeability (eg, from hypercarbia, hyperosmotic agents, and mechanical disruption) (161). Animal studies suggest that coincident gram-negative bacterial infections can induce invasion of the central nervous system by West Nile virus, leading to markedly increased rates of encephalitis and death (161). This effect is apparently caused by endotoxin-stimulated release of various cytokines and secondary changes in the integrity of the blood-brain barrier (180). Infection of astrocytes by West Nile virus contributes to neuronal death by downregulation of an astrocyte-specific protective stress gene regulator, induction of neuroinflammatory genes, and release of neurotoxic substances (306). Expression of multiple matrix metalloproteinases is induced in West Nile virus-infected cortical astrocytes, and this contributes to blood-brain barrier disruption (309). West Nile virus entry into cells requires cholesterol-rich membrane microdomains, and it appears that West Nile virus utilizes lipid rafts during the initial stages of internalization of the virus (197).
A variety of innate and adaptive immune responses help modulate West Nile virus levels in blood, peripheral tissues, and the central nervous system. Interferon-alpha and beta help limit viral translation and replication soon after infection, in part by upregulating genes with direct and indirect antiviral functions, by stimulating maturation of dendritic cells, and by direct activation of B and T cells (258). Genetic variation in the interferon response pathway is associated with risk for symptomatic West Nile virus infection and with West Nile virus disease progression (16). Complement is also needed to prime humoral and cellular immune responses, and lack of a functioning complement system in animal models is associated with significantly increased mortality following West Nile virus infection (258). Virus-specific antibodies and cytotoxic T-cells are important for the clearance of flaviviruses (19; 28; 161; 258; 274). Humoral immunity (in particular, virus-specific IgM antibody) protects against West Nile virus infection and severe virus-related disease, partly by limiting viral levels in serum and by helping to prevent seeding of the central nervous system (310; 311; 161; 258). Preliminary studies suggest that patients with West Nile virus encephalitis may benefit from intravenous immunoglobulin from donors with a high frequency of West Nile virus exposure (161). West-Nile-virus-specific antibody in the CSF may decrease viral replication by interfering with viral attachment to receptors on the cell surface or by preventing endosomal fusion (161). T lymphocytes are also essential for protection against West Nile virus. CD4+ and CD8+ T cells are also involved in viral clearance from both peripheral tissues and the central nervous system, and individuals with impaired T-cell function (eg, those with hematologic malignancies or HIV infection) have an increased risk of neuroinvasive disease (258; 274). The chemokine CXCL12 at the blood-brain barrier normally binds to the CXCR4 receptors on leukocytes, limits entry of mononuclear cells into the CNS parenchyma, and instead keeps these cells localized to the perivascular spaces of the CNS microvasculature; in murine models, administering a specific CXCR4 antagonist promotes intraparenchymal migration of West Nile virus-specific lymphocytes, enhances viral clearance, reduces immunopathology within the central nervous system, and results in significant improvement in survival (188).
West Nile virus employs a multifaceted immune evasion strategy, encompassing the suppression of interferon (IFN) production and signaling through (1) targeting of STAT proteins, IRF3, and RNA sensors; (2) the modulation of antigen presentation via downregulation of MHC molecules and impairment of proteasome function; and (3) the manipulation of cytokine and chemokine responses to dysregulate inflammation and promote viral persistence (05). West Nile virus gains access to the CNS across the blood-brain barrier, both by disrupting barrier integrity and utilizing "Trojan horse" mechanisms.
Neurologic disease presentations of West Nile virus infection. West Nile virus may be asymptomatic, or it may produce a febrile flu-like illness or may cause more serious diseases including meningitis, meningoencephalitis (128), or poliomyelitis. The epidemiological characteristics of West Nile virus disease in children are similar to adult case subjects; however, West Nile neuroinvasive disease is more likely to manifest as meningitis in children than in older adults (172).
With West Nile virus encephalitis, the brain may be grossly normal (257). Histological findings are typical of a viral meningoencephalitis and include (1) variable neuronal necrosis in the grey matter with neuronal degeneration and neuronophagia, and microglial and polymorphonuclear leukocytic infiltration; (2) microglial nodules composed primarily of lymphocytes and histiocytes and present predominantly in the grey matter; (3) variable mononuclear perivascular inflammation (perivascular cuffing); (4) scattered mononuclear leptomeningeal infiltrates; and (5) focal mononuclear inflammation of the cranial nerve roots, especially in the medulla (271; 257; 141; 109; 264).
Immunohistochemistry performed on human central nervous tissue showing West Nile virus antigen (red) in the cytoplasm of neurons and cell processes. (Source: Schwarz ER, Long MT. Comparison of West Nile virus disease in humans ...
West Nile virus may also trigger autoimmune encephalitis (138).
Several studies have suggested that West Nile virus may produce persistent infection in the central nervous system in animals (242; 321; 150) or people (229; 208). Individuals with chronic symptoms after West Nile virus infection may have persistent renal infection over several years, although attempts to grow the virus from urine in the original study were not successful (208), and a later study failed to replicate the earlier findings (96; 163). West Nile virus can be isolated from the urine during acute infections (13; 220). West Nile virus may persist in whole blood for months after clearance in plasma (162).
Early case reports and case series have generally attributed the flaccid paralysis accompanying West Nile virus infection to an inflammatory neuropathy like Guillain-Barre syndrome (03; 256). Most of these initial reports did not have supporting electrophysiologic studies, and none reported spinal cord pathology. Guillain-Barre syndrome cannot explain the clinical, laboratory, and electrophysiologic abnormalities in most of these cases. Guillain-Barre syndrome generally presents with symmetric weakness, is frequently accompanied by sensory abnormalities or paresthesia, is associated with elevated CSF protein but is without CSF pleocytosis, and has electrophysiologic studies consistent with a predominantly demyelinating neuropathy.
The clinical, laboratory, and electrophysiologic abnormalities in most patients with asymmetric flaccid paralysis result from a polio-like syndrome with involvement of spinal cord anterior horn cells and motor nerve axons. Cases of poliomyelitis in patients with West Nile virus infection have been identified since July 2002 in the United States (40; 98; 164; 141; 168; 222; 268; 269; 30). Two previous reports also suggested that the acute flaccid paralysis of West Nile virus infection resulted from myelitis, with electrophysiologic support in one case, but without pathological support in either (87; 215). Subsequent reports have supported these findings (132; 141; 30) and documented an overlapping spectrum of meningitis, encephalitis, and myeloradiculitis. In addition, a polio-like syndrome has been previously reported with Japanese encephalitis virus, a flavivirus closely related to West Nile virus (278; 276), with dengue flavivirus virus (158), and with tick-borne flavivirus infections in continental Europe, including Far Eastern tick-borne encephalitis and Central European encephalitis (262). Moreover, pathologic studies in animals have demonstrated lesions of the ventral spinal cord grey matter and the spinal motor neurons, with an absence of peripheral nerve lesions, in birds, horses, and nonhuman primates infected with West Nile virus (181; 283; 29).
The basis of the spinal cord damage caused by West Nile virus is not entirely clear and may be multifactorial, including direct viral damage to neurons, secondary excitotoxic injury (17), and autoimmune-mediated transverse myelitis (184). Local immune activation within the spinal cord causes a failure of astrocyte glutamate reuptake even though the number of astrocytes increases (17); as a result, the rising extracellular glutamate levels may cause excitotoxic injury of both infected and uninfected anterior horn cells.
A few studies have suggested an alternative (or possibly concomitant) explanation for some cases of acute flaccid paralysis associated with West Nile virus (ie, acute anterior radiculitis) (168; 222; 221). These authors point out that previous electrophysiologic studies have, in fact, localized the abnormality to either the anterior horn or the ventral nerve roots. MRI studies of cases of polio-virus poliomyelitis have shown signal changes in the anterior horn, findings that have been absent from most recent cases of West Nile virus-associated flaccid paralysis. Instead, some cases of West Nile virus-associated flaccid paralysis have demonstrated intradural nerve root enhancement (222; 221). One case of West Nile virus-associated encephalomyelitis with flaccid paralysis was found at autopsy to have apparently asymptomatic neuronal loss, gliosis, and neurofibrillary tangle formation in the substantia nigra at a young age (261).
A case of stiff-person syndrome has also been reported following West Nile fever (118). Stiff-person syndrome is characterized by progressive muscle stiffness, rigidity, and spasms, involving especially axial muscles. These manifestations result from antibodies to glutamic acid decarboxylase, which interfere with central gamma-aminobutyric (GABA-ergic) synaptic transmission. Hassin-Baer and colleagues found a high degree of homology between a West Nile virus protein and an isoform of glutamic acid decarboxylase and suggested that antibody cross-reactivity was responsible for development of stiff-person syndrome in their case (118).
|
• West Nile virus is usually transmitted by Culex mosquitoes from infected birds. | |
|
• Mosquito and bird surveillance has become an important component of monitoring for West Nile virus. | |
|
• West Nile virus encephalitis occurs in temperate regions primarily in the late summer and early autumn, with approximately 90% of cases occurring in August and early September. | |
|
• In Africa, India, Australia, and most temperate regions of North America, West Nile virus now exists in an endemic cycle, whereas it remains epidemic in Europe, being reintroduced regularly directly from Africa in Western Europe or indirectly via the Middle East in Eastern Europe. | |
|
• Season is a strong risk factor for human infection because infection is typically strongly linked to exposure to mosquitoes; more than 90% of reported cases in the United States have onset of illness between July and September, with a peak in late August. | |
|
• Only about 0.4% to 0.7% of West Nile virus infections result in West Nile neuroinvasive disease. | |
|
• Mortality occurs mostly in older and immunocompromised individuals with neuroinvasive disease. | |
|
• Other mechanisms of documented transmission include blood transfusion, platelet transfusion, organ transplantation, breastfeeding, and transplacental. | |
|
• Universal blood donor screening has since nearly eliminated the risk of West Nile virus transfusion transmission but at an enormous cost. | |
|
• Intrauterine infections are apparently infrequent and may not adversely affect the health of infants at birth. | |
|
• Organ-derived West Nile virus infection is associated with a high incidence of neuroinvasive disease (70%) and with severe morbidity and mortality (30%). |
Animals. West Nile virus is usually transmitted by Culex mosquitoes from infected birds, which serve as amplifying hosts (275). Birds are the main reservoirs of West Nile virus, and on infection, the virus replicates to levels allowing for transmission to mosquito vectors. In human and other mammal infections (eg, horses), the viremia is too low for transmission to mosquito vectors; thus, mammals are considered to be dead-end hosts (264)
The various species of mosquitoes that can transmit West Nile virus (there are at least 36 such species) have variable life cycles and habit requirements, are collectively more common and less localized, and have less specific breeding requirements than species that transmit La Crosse encephalitis. They may also bite at different times of the day and often move into homes. These factors make West Nile virus difficult to control with mosquito management plans. Although ticks can become infected with West Nile virus, they do not play a substantial role in West Nile virus transmission (121). West Nile virus can be transmitted within mosquito populations by vertical transmission and possibly through infectious mosquito excreta, mechanisms contributing to viral maintenance in mosquito reservoirs (115).
More than 300 species of birds have been infected, including robins, crows and jays, Canadian geese, mallards, ring-necked pheasants, and various birds of prey (21). The American robin (Turdus migratorius) represented the ecologically most important bird viral reservoir (21). Unlike corvids (eg, crows and jays), robins may serve as hosts without succumbing to illness. Shifts in mosquito feeding behavior, especially during periods of robin dispersal and migration, may plan an important role in amplifying the number of human infections (142). Birds of prey are thought to have acquired the virus most often from other birds rather than through a mosquito vector.
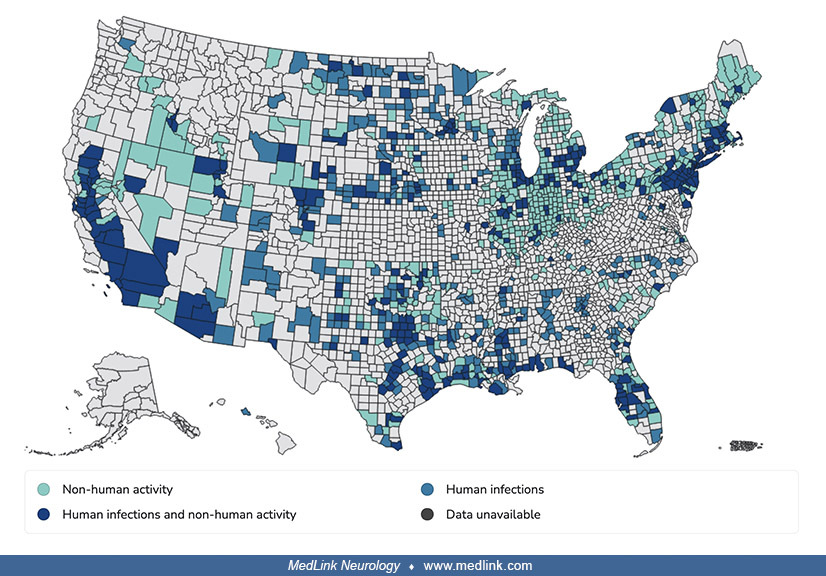
Mosquito and bird surveillance has become an important component of monitoring for West Nile virus. Counts of infected mosquitoes and dead birds are indicators of risk for human infections (36; 69; 157; 20; 225; 111). Dead bird counts typically increase prior to the identification of human cases (225). Indeed, the first indicator of West Nile virus activity in almost all U.S. counties reporting such activity was a West Nile virus-infected dead bird; an index human case occurred in only 4% of affected counties. Of counties reporting human cases, the first human illness was preceded by reports of infected animals (including mosquitoes) by a median of 1 month.
The relative utility of different surveillance approaches is not clear, with some studies suggesting that mosquito surveillance is a more accurate predictor of human risk than monitoring dead and infected wild birds (20) and other studies suggesting the opposite (225). Because bird surveillance depends on public cooperation and active involvement in bringing in dead birds for testing, bird surveillance is much more effective at predicting human illness in urban areas with high human population densities (225). Horse and other mammal deaths are less useful for surveillance because they are much less common, and they precede identification of human cases less often (225). Dogs and cats are readily infected with West Nile virus (11), and the high efficiency of oral transmission in cats suggests that prey animals may be a significant source of infection for mammalian carnivores (as it is in birds of prey) (11). Neither dogs nor cats are thought to function as an epidemiologically important amplifying host (11), but alligators can serve as epidemiologically important amplifying hosts in areas with high population densities of juvenile alligators (148). Sentinel chicken surveillance is a poor predictor of subsequent human infections (225).
Unfortunately, because of budget considerations, since the first national assessment of the capacity for surveillance, prevention, and control of West Nile virus in 2005, 22% of jurisdictions have stopped active human surveillance, 13% have stopped mosquito surveillance, 70% have reduced mosquito trapping and testing, and 64% have eliminated avian mortality surveillance (111).
To help obviate the monitoring cost, time, and difficulty of using mosquito pool testing and bird surveillance, wastewater-based epidemiology is being explored (156; 327). Pilot studies have been encouraging. West Nile virus RNA has been detected in wastewater samples during periods of known viral circulation, and detections in wastewater solids correspond to the occurrence of cases in the season and location of sampling (156; 327).
Dissemination of West Nile virus in the United States. Complete transcontinental movement of the virus occurred within 3 years of the initial recognition of human cases in New York City in 1999. Compared to 2001, the number of human and animal cases and the geographic range of West Nile virus infection increased dramatically in the United States in 2002 and 2003 (47; 233; 121; 74; 254). The geographic range expanded to include almost the entire contiguous United States except four mountainous states in the West (233; 121; 110; 152; 254). According to extrapolations from screening the United States blood supply for West Nile virus, by 2003 an estimated 0.5% of the U.S. population had been infected with West Nile virus, and by 2008 approximately 1% of the U.S. population had been infected with the virus (24; 240).
Neuroinvasive disease. Based on seroprevalence surveys, approximately 75% to 80% of human West Nile virus infections are asymptomatic, about 20% cause a febrile illness (West Nile fever), and only about 0.4% to 0.7% of West Nile virus infections result in West Nile neuroinvasive disease (205; 24; 60; 32; 104). The virus is most likely to produce encephalitis or death in those over age 50 years and in those with weakened immune systems, but people of any age can develop severe neurologic disease from West Nile virus infection (315; 316; 129). The risk of West Nile neuroinvasive disease appears to be highest in areas where the primary vectors are Culex tarsalis and Culex quinquefasciatus mosquitoes (173). Chronic renal disease, history of cancer, history of alcohol abuse, diabetes, and hypertension are independently associated with encephalitis in multivariable analyses, but only hypertension is associated with meningitis, and only immune suppression is an independent predictor of death in multivariable analyses (176).
In a population-based cohort study in Ontario, Canada, from 2002 through 2012, 345 individuals developed West Nile neuroinvasive disease (18.3%) out of 1884 West Nile virus infections (288). Immunocompromised [adjusted rate ratio 2.61 (95% CI 1.23-4.53)] and male sex [adjusted rate ratio 1.32 (95% CI 1.00-1.76)] were risk factors for encephalitis, in addition to age, for which each 1-year increase was associated with a 2% [adjusted rate ratio 1.02 (95% CI 1.02-1.03)] relative increase in risk.
Among 18,266 West Nile virus neuroinvasive cases reported to the Centers for Disease Control and Prevention over the interval from 2010 to 2024, approximately half (56%) were West Nile virus encephalitis, a third (35%) were West Nile virus meningitis, 6% were acute flaccid paralysis, and 4% were unspecified (based on tabulations of annual data by Douglas J Lanska MD MS MSPH). The situation is somewhat more complicated because some present with more than one form of West Nile virus neuroinvasive disease (eg, West Nile virus encephalitis and acute flaccid paralysis). In addition, the number of unspecified cases was zero from 2010 to 2013, and since 2017 the number of unspecified cases has exceeded the number with acute flaccid paralysis.
The number of hospitalizations for West Nile virus infections from 2010 to 2024 was 20,336 (mean hospitalizations per year = 1453). This exceeds the number of neuroinvasive cases (n=18266) over this interval and represents about two thirds (69%) of total cases (based on tabulations of annual data by Douglas J Lanska MD MS MSPH).
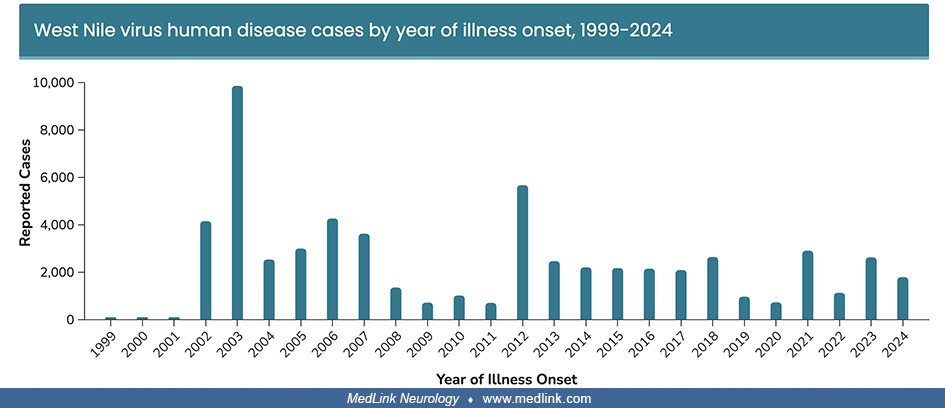
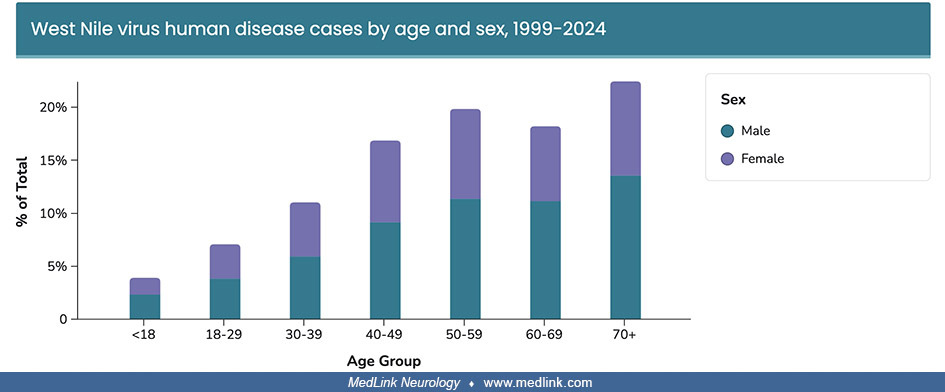
Incidence in the United States. From 1999 to 2021, there were 55,444 cases of human West Nile virus infection, including 27,776 neuroinvasive cases. Reported cases varied markedly by year, with the most reported cases in 2003 and a second lesser peak in 2012. The number of reported cases increases with age and is greater in males than in females.
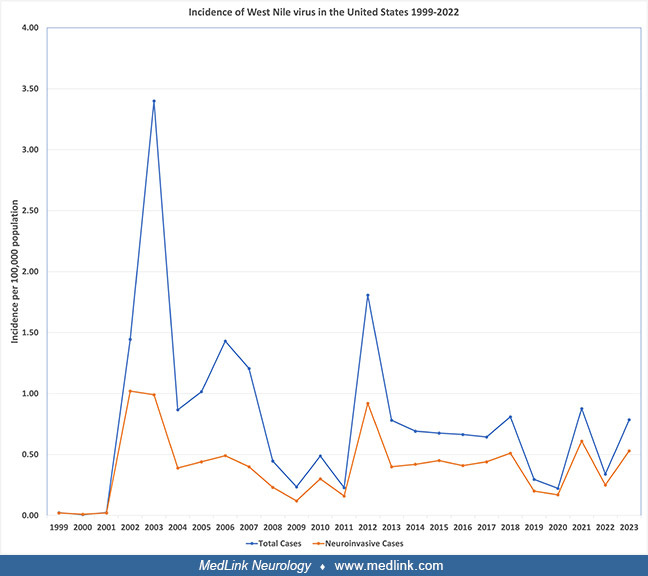
The national incidence rates of West Nile virus infections peaked in 2003 at 3.4 cases per 100,000 population with close to 9,900 cases reported to the Centers for Disease Control and Prevention in the United States (121). Indeed, the 2003 West Nile virus epidemic in the United States was the largest arboviral meningoencephalitis epidemic ever documented in the western hemisphere and the largest West Nile virus meningoencephalitis epidemic ever recorded. Incidence rates then declined sharply and were less than 0.5 per 100,000 population from 2008 to 2011, before again abruptly increasing to a peak of 1.8 per 100,000 population in 2012, with a large percentage of incident cases in Texas in 2012 (232; 146; 22; 71; 189; 190). Since 2013, they have remained below 1.0 per 100,000 population (303; 279; 82).
(Source: Data from the U.S. Centers for Disease Control and Prevention, Atlanta, Georgia, and U.S. Census Bureau population estimates for July 1 of each year of the reporting period. Plot by Dr. Douglas J Lanska.)
In an approximation of the pattern seen with overall West Nile virus infections, the national incidence of West Nile virus neuroinvasive disease peaked in 2002 and 2003 (1.0 cases per 100,000 population) and was much less from 2004 to 2011 before again transiently increasing in 2012 (0.9 cases per 100,000 population) (14; 64; 174; 175; 155; 189; 190).
Neuroinvasive disease incidence increases with increasing age, with the highest incidence (1.4 cases per 100,000 population) occurring among persons aged 70 years and older (62; 191; 192).
A total of 12,835 neuroinvasive cases were reported in the United States from 2009 to 2018. Incidence is expressed as cases per 100,000 population. Incidence calculated using U.S. Census Bureau population estimates for July 1 o...
Anomalies in temperature and precipitation are associated with above average West Nile virus neuroinvasive disease incidence (112). Above average annual temperature is associated with an increased likelihood of higher-than-normal West Nile virus neuroinvasive disease incidence nationally and in most regions (112; 139).
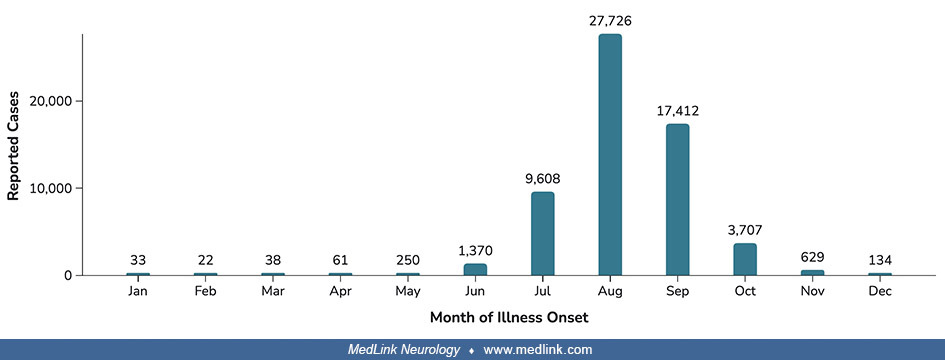
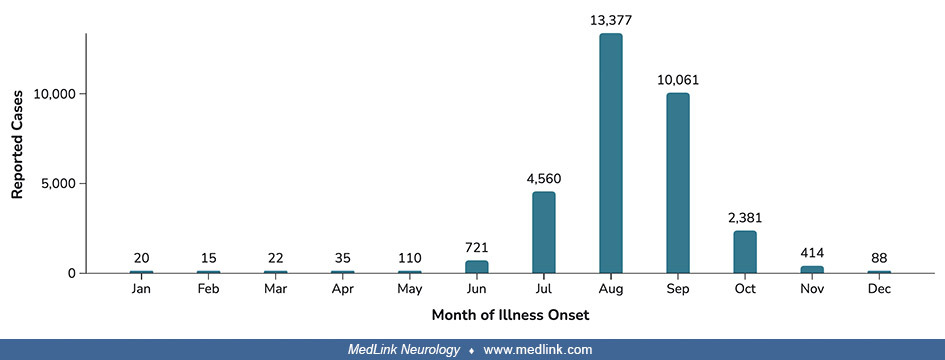
Seasonal patterns. West Nile virus infections and cases of West Nile virus neuroinvasive disease occur in temperate regions primarily in the late summer and early autumn, with approximately 90% of cases occurring in August and early September in the United States. In South Africa (in the southern hemisphere), the period between January and June covers the South African mid-summer to autumn months, when the availability of mosquito breeding sites and vectorial capacity increases due to the warmer and wetter weather conditions (193).
(Source: MacIntyre C, Lourens C, Mendes A, et al. West Nile virus, an underdiagnosed cause of acute fever of unknown origin and neurological disease among hospitalized patients in South Africa. Viruses 2023;15[11]:2207. Creativ...
Incidence peaks in the late summer and early autumn. A total of 21,869 cases were reported in the United States from 2009 to 2018. (Source: McDonald E, Mathis S, Martin SW, Staples JE, Fischer M, Lindsey NP. Surveillance for We...
In part, this seasonal pattern is due to a shift in mosquito feeding behavior from birds to humans, greatly amplifying the number of human infections: Culex pipiens, the dominant bird-to-bird (enzootic) and bird-to-human (bridge) vector in the northeast and north-central United States, shifts its feeding preferences from birds to humans at this time because of dispersal and migration of its preferred host, the American robin (Turus migratorius) (142). Warmer and less rainy conditions enhance West Nile virus circulation and cause virus spillover from the sylvatic cycle (ie, the cycle of West Nile virus infection in animals) (26). In West Nile virus epidemics, the number of human cases decreases with the onset of cooler weather in fall as the mosquitoes die. In warmer climates, West Nile virus can be transmitted year-round. The overwintering period is an important climatic constraint on the dynamics of West Nile virus in cold-temperate regions of North America and Europe (318; 137); even in warmer areas of the United States, environmental conditions during overwintering appear to be critical for West Nile virus amplification during summer outbreaks (243; 139). Transmission of West Nile virus involves so many vectors and hosts within different landscapes and regions that multiple overwintering pathways are possible (248). In southern states of the United States, warmer winters are associated with an increase in the average number of West Nile virus-infected mosquitoes per trap-night and development of large human West Nile virus epidemics (67; 318).
The largest recorded West Nile virus outbreak in a U.S. county occurred from May to December, 2021, in Maricopa County, Arizona, and included 1487 cases, 1014 (68%) hospitalizations, and 101 (7%) deaths (154). The reason for the unprecedented outbreak is unknown but is likely multifactorial, related to increased rain, recent population growth and housing development, and changes in healthcare-seeking behavior during the COVID-19 pandemic. Of the 1487 cases, 956 (64%) were neuroinvasive: 618 (65%) encephalitis, 319 (33%) meningitis, 1 (< 1%) Guillain-Barre syndrome, 1 (< 1%) acute flaccid paralysis, and 17 (2%) not specified (154).
Number of West Nile virus cases (N = 1487), vector indices, and public health responses, by epidemiologic week start date--Maricopa County, Arizona, 2021. Neuroinvasive and non-neuroinvasive cases are shown. The vector index is...
In Africa, India, Australia, most temperate regions of North America, and parts of Europe, West Nile virus now exists in an endemic cycle, whereas it remains epidemic in Europe, being reintroduced regularly directly from Africa in Western Europe or indirectly via the Middle East in Eastern Europe. Only one endemic genotype is present in India, and another single genotype is present in Australia, apparently because West Nile virus was successfully introduced into these locations only once; genetic studies suggest these introductions occurred many centuries ago (185).
Season is a strong risk factor for human infection because infection is typically strongly linked to exposure to mosquitoes. The vast majority of reported cases in the United States (more than 90%) have onset of illness between July and September, with a peak in late August (172; 177). Human cases in the southern states precede cases in northern states by about 1 month. Other risk factors for human infection include situations that support or promote mosquito propagation, including standing water (eg, flooded basements) that can support in-home mosquito breeding (116; 139). Similarly, irrigation has been linked to a greater incidence of human and veterinary West Nile virus cases in the United States from 2004 to 2006 (93; 79). In urban Atlanta, West Nile virus infection in mosquitoes, corvids, and humans is spatially clustered and significantly associated with streams affected by combined sewer overflow (307). Storms can also significantly increase the number of mosquito-breeding sites: after Hurricane Katrina in 2005, there was a greater than 2-fold increase in the incidence of West Nile neuroinvasive disease in hurricane-affected areas in 2006 compared with previous years (25). From 2001 to 2005, warmer temperatures, elevated humidity, and heavy precipitation each increased the rate of human West Nile virus infection in the United States independent of season (281).
Other risk factors for West Nile virus infection include having a water-holding container in one's yard and not working or attending school outside of the home (95). These factors are obviously related to conditions that either foster the growth of mosquitoes or that increase human exposure to mosquitoes.
Mortality and case fatality in the United States. Mortality occurs mostly in older and immunocompromised individuals with neuroinvasive disease (301; 146). Mortality of patients with neuroinvasive disease is approximately 10% overall but 20% in individuals 70 years or older and 30% to 40% in patients with hematologic malignancies, solid organ transplants, and those receiving B-cell-depleting monoclonal antibodies (104).
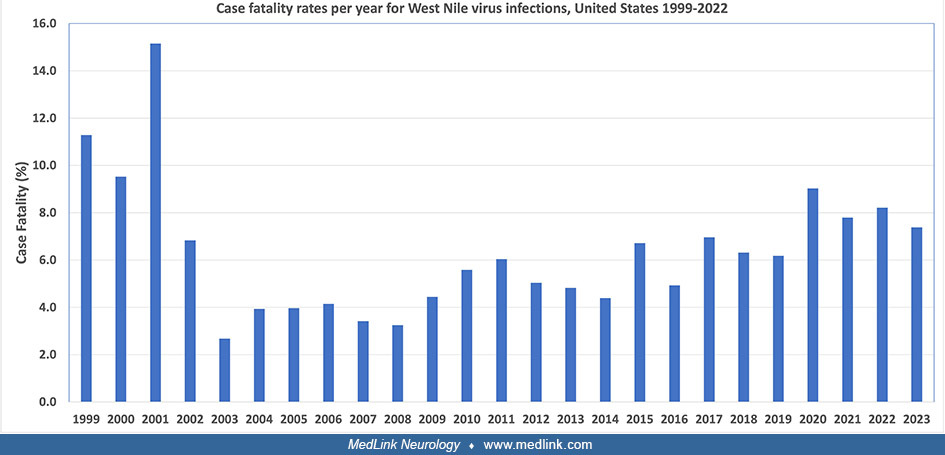
The apparent case-fatality rate among recognized cases of West Nile virus infection has decreased significantly since 1999, probably at least in part because of greater detection of milder cases rather than a changing virulence of the virus (52; 54; 55; 56; 60; 121; 175; 189; 190). From 1999 to 2024, there have been 2970 deaths attributed to West Nile virus infection, most among those with neuroinvasive disease. Over this period, case fatality ratios have varied on a yearly basis by more than a factor of 2, from a low of 2.7% in 2003 to a high of 15.2% in 2001, with an average case fatality of 5.0%.
However, these estimates are somewhat misleading because mild cases are still largely underreported (205; 60). Mostashari and colleagues used an estimate of the frequency of neuroinvasive disease (0.7% of all West Nile virus infections) (205) and the observed number of neuroinvasive cases for 2007 (1227) (60) to estimate that there were approximately 175,000 individuals with West Nile virus infection in 2007, of whom 117 died, giving a corrected estimate of case fatality of 0.07%. Using a range of estimates of the frequency of neuroinvasive disease (0.4% to 0.7% of all West Nile virus infections) (205; 24; 32) and the observed number of cases since 1999, there were approximately 3.6 million to 6.3 million individuals with West Nile virus infection over this interval, of whom 2450 died, giving a corrected estimated range of overall case fatality of 0.04% to 0.07% (Lanska unpublished data). According to more sophisticated calculations using reported case data from ArboNET and previous seroprevalence data stratified by age and sex, an estimated 7 million persons in the United States have been infected with West Nile virus since its introduction in 1999, which gives an estimated overall case fatality of 0.03% (253).
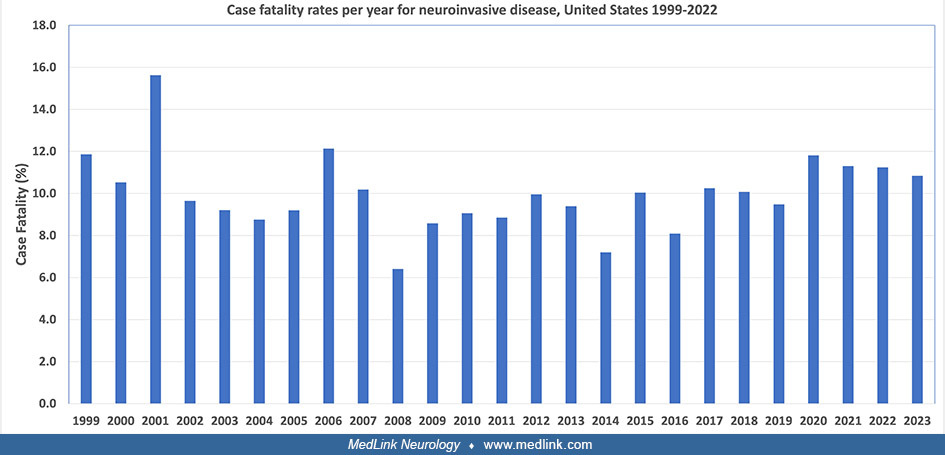
Cases of neuroinvasive disease are likely to be more completely reported, and almost all deaths occur among these cases. From 1999 to 2024, there have been 30,392 neuroinvasive cases among 59,204 total cases, indicating that neuroinvasive cases represent about half (51%) of all reported cases. Case fatality ratios for neuroinvasive disease over this period have varied on a yearly basis by more than a factor of 2, from a low of 6.4% in 2008 to a high of 15.6% in 2001. Over the interval from 1999 to 2024, case fatality for neuroinvasive disease has averaged about 9.8% (Lanska unpublished data).
Similarly, case fatality for the subgroup of West Nile virus neuroinvasive disease cases with encephalitis has been estimated to be between 4% and 16% (277; 258). The case-fatality ratio progressively increases with increasing age among persons with neuroinvasive disease, as is particularly evident in the decade from 2009 to 2018 (62; 191; 192).
In Texas, over the period from 2002 to 2012, there were similar numbers of “acute-phase” (within 90 days of symptom onset) and “convalescent-phase” (more than 90 days after symptom onset) deaths (238). Ninety-two percent of acute-phase and 78% of convalescent-phase deaths occurred among cases of West Nile neuroinvasive disease. Convalescent-phase neuroinvasive disease cases showed excess deaths from infectious and renal causes; cases younger than 60 years of age had increased risks for all-cause death, specifically from renal, infectious, digestive, and circulatory causes.
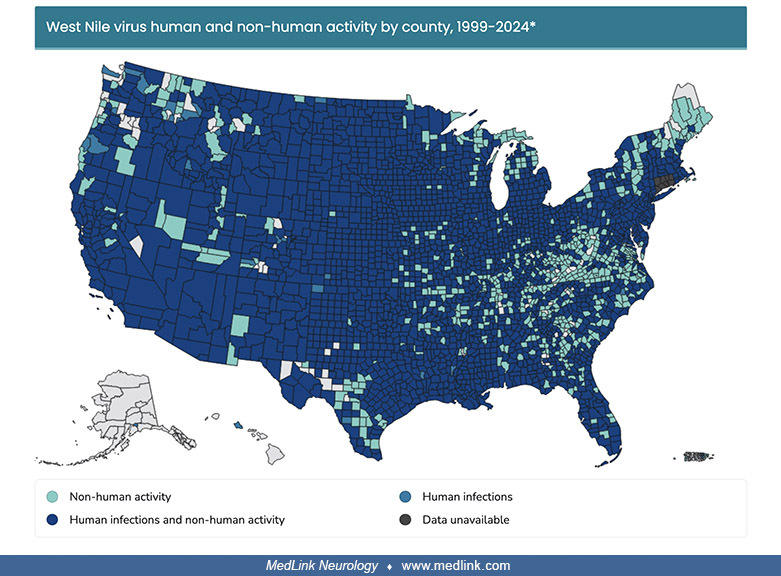
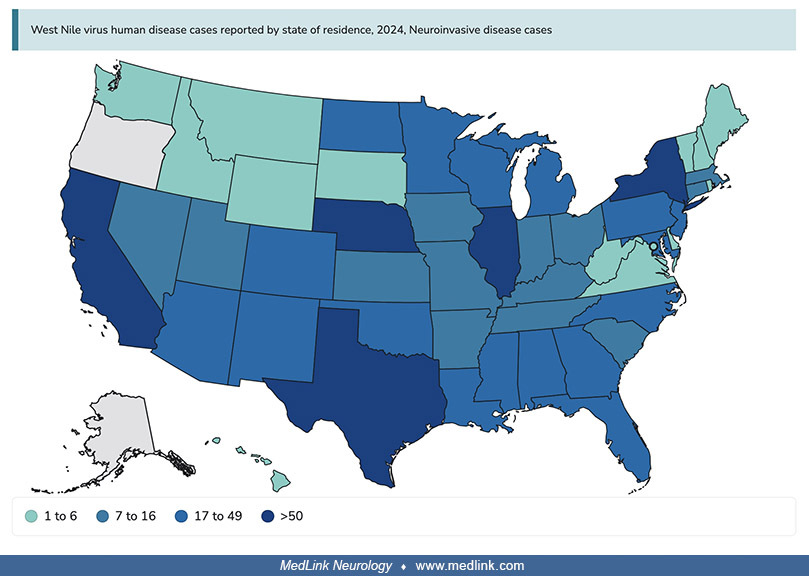
Geographic distribution in the United States. In the interval from 1999 to 2024, most counties of the contiguous United States were affected by both non-human West Nile virus activity and human activity. In 2023 and 2024, involvement was somewhat scattered.
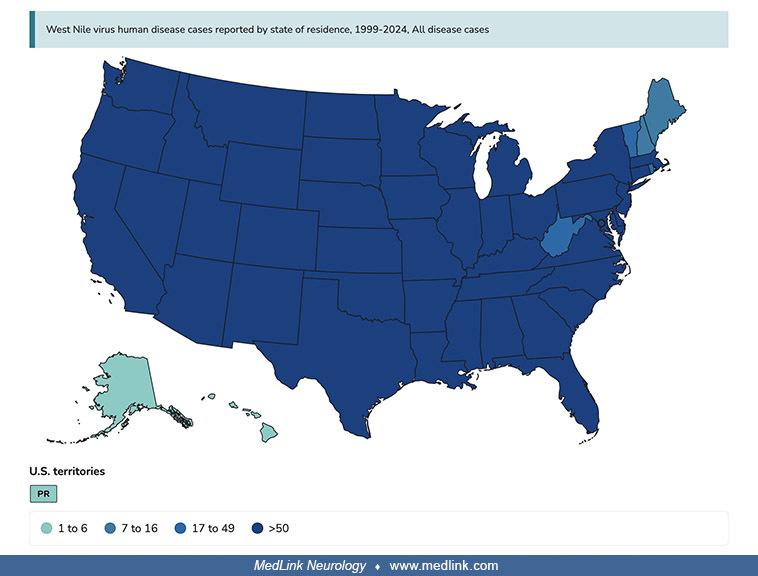
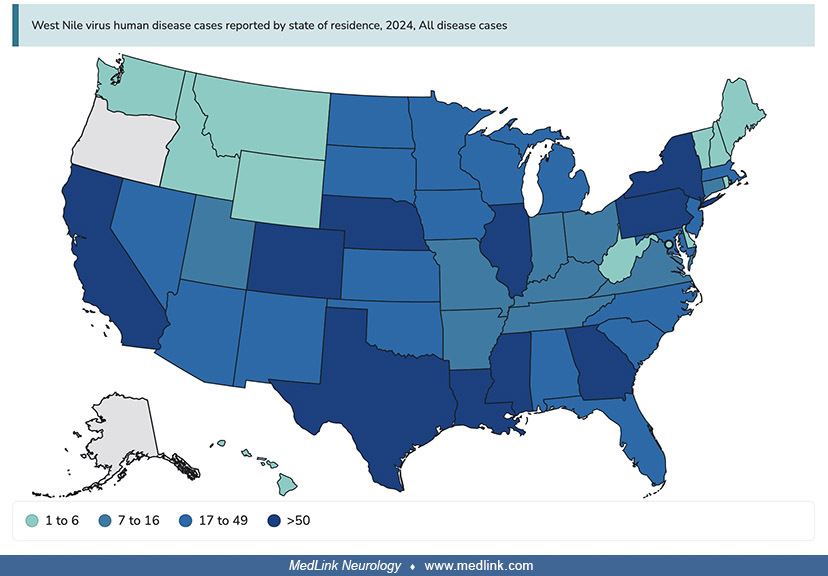
From 1999 to 2024, all but seven states had more than 50 cases of human West Nile virus infection: Alaska, Hawaii, Maine, New Hampshire, Rhode Island, Vermont, and West Virginia. In 2024, 10 states had 50 or more cases: New York, Pennsylvania, Illinois, Nebraska, Colorado, California, Texas, Louisiana, Mississippi, and Georgia.
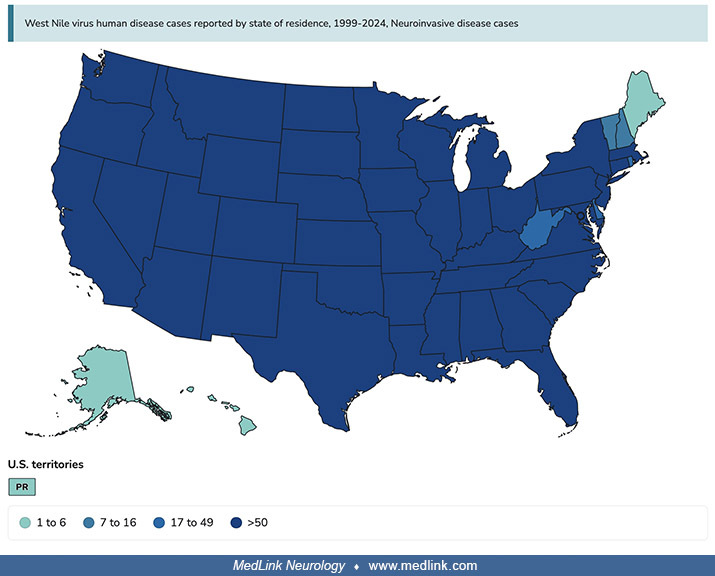
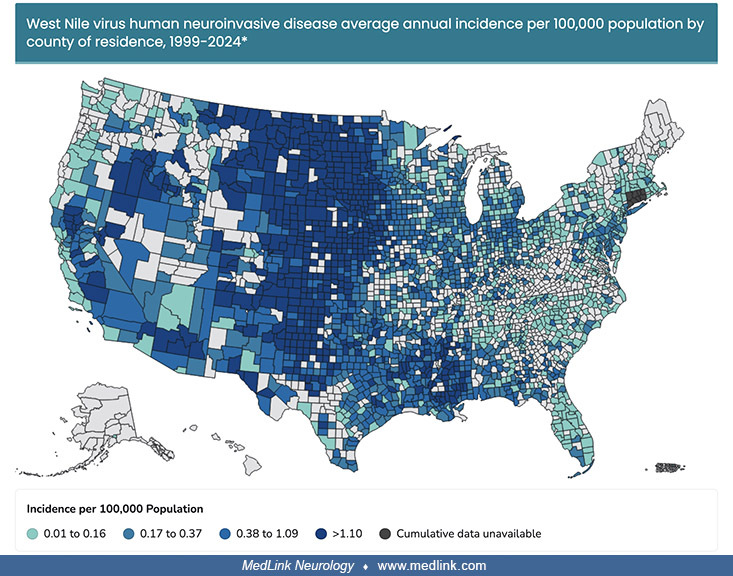
From 1999 to 2024, all but eight states had more than 50 cases of neuroinvasive human West Nile virus infection: Alaska, Delaware, Hawaii, Maine, New Hampshire, Rhode Island, Vermont, and West Virginia. At a county level, the highest incidence rates from 1999 to 2024 were seen in the West North Central, West South Central, and Mountain census divisions. In 2025, five states had 50 or more cases: New York, Illinois, Nebraska, Texas, and California.
Average annual incidence data is unavailable for Connecticut at the county level. Connecticut changed from counties to a planning region in 2022. (Source: ArboNet, U.S. Centers for Disease Control and Prevention. Public domain....
Geographic distribution in Europe. West Nile virus is an emerging mosquito-borne pathogen in Europe, apparently due in part to climate changes (81; 179; 194): from 2006 to 2021, 2916 West Nile neuroinvasive disease cases were registered, of which 2081 (71%) and 383 (13%) resulted in the hospitalization and death of the patient, respectively (249). Warm winters are associated with more intense West Nile virus circulation in southern Spain (194).
The density of both “probable” and “confirmed” cases is shown for each administrative area for which there was at least one confirmed case before 2020. Specifically, the number of West Nile virus (WNV) cases by aggregating both...
To investigate the extent to which West Nile virus spatial expansion in Europe can be attributed to climate change while accounting for other direct human influences, such as land use and human population changes, ecological niche models were developed to predict the risk of local West Nile virus circulation leading to human cases to then unravel the isolated effect of climate change by comparing factual simulations to a counterfactual simulation based on the same environmental changes but a counterfactual climate where long-term trends have been removed (81). These models demonstrate a notable increase in the area ecologically suitable for West Nile virus circulation during the period 1901 to 2019, whereas this area remains largely unchanged in a no-climate-change counterfactual. Thus, the drastic increase in the human population at risk of exposure is partly due to historical changes in population density, but climate change has also been a critical driver behind the heightened risk of West Nile virus circulation in Europe.
Geographic distribution in Africa. An extensive review of 153 scientific papers published between 1940 and 2021, concerning West Nile virus infections in Africa, highlighted several important conclusions: (1) the co-circulation of West Nile virus lineages 1, 2, and 8 in the African continent; (2) evidence of circulation of West Nile virus among humans, animals, and vectors in at least 28 countries and the lack of knowledge on the epidemiological situation of West Nile virus for 19 countries; (3) the presence of diverse West Nile virus–competent vectors in Africa, mainly belonging to the Culex genus; and (4) the lack of vector competence studies for several other mosquito species found naturally infected with West Nile virus in Africa and the need for more competence studies on ticks (198).
(Source: Mencattelli G, Ndione MH, Rosà R, et al. Epidemiology of West Nile virus in Africa: an underestimated threat. PLoS Negl Trop Dis 2022;16[1]:e0010075. Creative Commons Attribution 4.0 International License [CC-BY 4.0], ...
Horizontal and vertical person-to-person transmission. Other mechanisms of documented transmission include horizontal transmission by blood transfusion (39; 40; 41; 42; 44; 45; 46; 51; 57; 61; 285; 204; 23; 27; 72; 80; 89; 121; 145; Petersen and 80b; 286; 200; 109; 92; 104), platelet transfusion (119), or organ transplantation (40; 42; 44; 53; 59; 60; 61; 130; 204; 147; 121; 209; 109; 201; 247; 319; 323; 106; 77; 01; 263; 280; 140; 104). Vertical transmission is also possible by breastfeeding (43; 104), and transplacentally (48; 121; 109; 104). Additional routes of person-to-person include percutaneous and conjunctival exposures (104).
Horizontal transmission via blood transfusion. Before universal screening of the United States blood supply, the high infection incidence (up to 2% of the population in some areas) and the high frequency of asymptomatic infections (approximately 75% to 80% of those infected remain asymptomatic) translated into a considerable risk of West Nile virus transfusion transmission despite the short duration of viremia following infection (230; 104). Universal blood donor screening has since nearly eliminated the risk of West Nile virus transfusion transmission, but at an enormous cost (230; 105). Rarely, cases of blood or platelet transfusion-associated West Nile virus infection can occur if the suspect unit was collected early in the viremic period when viral RNA was below the limit of detection of the assay (119). Also, because of cross-reactivity between viruses in the Japanese encephalitis group, receiving inactivated Japanese encephalitis virus vaccination may be associated with positive West Nile virus blood donor screening nucleic acid tests (78).
Fairly sensitive methods are now available for screening blood donors, but organ donors are not screened routinely (61; 314), and such screening is not required by national policy (211). Even with improved screening methods, occasional cases of blood transfusion transmission occur, for example, with donations immediately prior to conversion on individual-donation nucleic acid testing (106). West Nile virus transmission via transplanted organs carries extremely high morbidity and mortality (230).
Twenty-three cases of confirmed transfusion-related West Nile virus transmission were documented in the United States in 2002 before blood screening for West Nile virus was implemented, compared with just 14 cases in 2003 after screening was implemented (227; 200; 57; 104). Since July 2003, blood collection agencies in the United States have been using West Nile virus nucleic-acid amplification tests to screen all blood donations and have been quarantining and retrieving potentially infectious blood products. This approach has been successful in preventing most cases of West Nile virus transmission through transfusion of blood and blood products. In 2006, the two post-transfusion cases were immunosuppressed individuals who developed West Nile virus neuroinvasive disease after receiving blood products from a single infected donor despite a negative minipool nucleic acid amplification test at the time of blood donation (57). It is currently not feasible to test individually all blood donations in the United States, but individual donation testing has been used in areas with a high incidence of West Nile virus infection. Although screening of blood donors for West Nile virus is now extremely sensitive, current methods still do not detect all West Nile-infected blood donations: some residual transfusion risk remains due to donations with low levels of virus (200; 57; 61). Until more sensitive methods of testing are developed, clinicians should continue to investigate cases of West Nile virus infection in people who have received blood transfusions and report cases with suspected transfusion-associated illness.
West Nile virus RNA persists in the red cell fraction in whole blood, and the level of persistence in whole blood may reflect the initial viral burden in plasma (162). West Nile virus RNA persistence in blood also varies with blood group of the infected individuals: following West Nile virus RNA-positive blood donation, blood group A donors maintained higher West Nile virus viral load in whole blood than blood group O donors, which suggests that West Nile virus adherence to red cells may be mediated by molecules overrepresented at the surface of blood group A red cells (162).
Horizontal transmission via transplantation. West Nile virus transmission during solid organ transplantation was identified in 14 clusters in the U.S. and Italy from 2002 to 2023 (104). Organ-derived West Nile virus infection is associated with a high incidence of neuroinvasive disease (70%) and with severe morbidity and mortality (30%) (319). The median time for onset of symptomatic infection is 13 days after transplantation (range 5 to 37 days). In the most common presentation, an unexplained fever that is unresponsive to antibiotic therapy is followed by the rapid onset of neurologic deficits.
Vertical transmission. Transmission of West Nile virus by breastfeeding is possible but appears to be rare (43; 123). Transplacental transmission has been documented (48; 121; 109), but intrauterine infections are apparently infrequent and may not adversely affect the health of infants at birth (219).
Laboratory accidents. Laboratory workers have been occupationally infected by percutaneous inoculation and possibly through aerosol exposure (121; 109).
Other. Possible dialysis-related West Nile virus transmission has been reported (50). West Nile virus has also been detected in urine (295; 12; 13; 220), although no cases of transmission via contaminated urine have been reported.
Altered disease course with immunomodulatory therapies. Immunomodulatory therapies for other conditions may alter the disease course of West Nile virus infection and, in some cases, may increase the severity of clinical disease (127). One patient developed West Nile virus encephalitis and poliomyelitis 2 weeks following treatment with rituximab for B-cell lymphoma and subsequently developed delayed encephalitis with ascending demyelinating polyneuropathy 6 months later, possibly as a result of reactivation of the virus or, less likely, the development of a postinfectious autoimmune process (127). A retrospective cohort study of adults with neuroinvasive West Nile virus infection at the Mayo Clinic from 2006 to 2021 found that individuals who were immunosuppressed had a higher risk of disease complications and poorer outcomes than individuals who were not immunosuppressed (195).
|
• Prevention efforts are directed at limiting exposure to mosquitoes. | |
|
• Eradication of flaviviruses is extremely difficult because most flavivirus life cycles involve arthropod vectors and nonhuman amplifying/reservoir hosts. | |
|
• Cost-effectiveness analyses have suggested that unless disease incidence increases substantially, universal vaccination against West Nile virus would be unlikely to produce societal monetary savings. |
Prevention efforts are directed at limiting exposure to mosquitoes (36; 49). This can be done at a population level by eliminating mosquito breeding sites and by use of aerial mosquito adulticiding, which can be effective in reducing human illnesses related to West Nile virus infection (31; 255; 104).
To avoid mosquito bites, individual patients should do the following:
|
• Apply insect repellant containing no more than 35% of the active ingredient, diethyltoluamide. Children should use products containing no more than 10% N,N-diethyl-m-toluamide (called DEET). Follow the directions on the repellant container. | |
|
• Consider staying indoors at peak mosquito-biting times (dawn, dusk, and early evening). | |
|
• Wear long-sleeved shirts and long pants when outdoors. | |
|
• Consider applying repellants with permethrin or DEET to clothing when outdoors. | |
|
• Keep window and door screens in good repair. | |
|
• Eliminate stagnant or standing water around your home where mosquitoes can lay eggs. This includes water in flowerpots, buckets, old tires, clogged rain gutters, and birdbaths. |
Hunters are at risk both from mosquito bites and from cleaning or eating potentially infected birds. Hunters can minimize their risk by doing the following:
|
• Taking precautions to avoid mosquito bites. |
In some cases, insecticides have been increasingly used to control mosquito vectors of West Nile virus. Human health risks from residential exposure to mosquito insecticides are low and are significantly exceeded by the risks of West Nile virus-related disease (236).
Eradication of flaviviruses is extremely difficult because most flavivirus life cycles involve arthropod vectors and nonhuman amplifying/reservoir hosts. Flavivirus vaccines are currently available against yellow fever, Japanese encephalitis, and tick-borne encephalitis. Vaccines for West Nile virus are in development but are not expected to be available for several years (161; 239; 322; 135; 302; 320). Various West Nile virus immunization strategies have been investigated in animal models, including a formalin-inactivated (killed) virus veterinary vaccine, a live attenuated chimeric virus vaccine candidate, passive immunization with West Nile virus immune serum, and immunization with heterologous flavivirus vaccines (ie, Japanese encephalitis virus, St. Louis encephalitis virus, yellow fever virus) (291; 291b; 161; 199).
Unless disease incidence increases substantially, cost-effectiveness analyses have suggested that universal vaccination against West Nile virus would be unlikely to produce societal monetary savings (325). This does not, however, mean that high-risk groups for neuroinvasive or fatal disease would not benefit from a safe and effective vaccine, nor does it mean that application of such a vaccine in these individuals would not be cost-effective.
The differential diagnoses include stroke, Guillain-Barre syndrome, polyradiculitis, subacute polyneuropathy, meningoencephaloradiculitis, encephalitis (including other arboviral encephalitides), other encephalopathies, myelitis, poliomyelitis, meningitis, and postviral demyelination. Among children (less than 18 years of age) with neuroinvasive arboviral infection in the United States, the most common causes are La Crosse virus encephalitis and West Nile virus neuroinvasive disease, with La Crosse virus primarily affecting younger children, and West Nile virus more commonly affecting older children and adolescents (88). West Nile virus is now the most common cause of arbovirus encephalitis and meningoencephaloradiculitis in the United States, but it is not a common cause of Guillain-Barre syndrome, polyradiculitis, myelitis, meningitis, or postviral demyelination. Even in areas of recognized West Nile virus infection in animals, most human cases of aseptic meningitis are caused by enteroviruses and not West Nile virus (134). Other arboviral encephalitides, such as those from eastern equine encephalitis, can sometimes present diagnostic difficulties (124).
Because of cross-reactivity between viruses in the Japanese encephalitis group, receiving inactivated Japanese encephalitis virus vaccination may be associated with positive West Nile virus blood donor screening nucleic acid tests (78).
• The United States Centers for Disease Control and Prevention has published a case definition for arboviral encephalitis or meningitis that is applicable to West Nile virus encephalitis and meningitis. | |
• West Nile virus or another arbovirus (eg, St. Louis encephalitis virus) should be strongly considered in patients with unexplained encephalitis or meningitis in late summer or early fall. | |
• Serologic testing for West Nile virus can be problematic because samples obtained within 8 days of infection may be falsely negative due to cross-reactivity between West Nile virus and other flaviviruses and also because of persistence of IgM antibodies. | |
• In patients with suspected West Nile virus neuroinvasive disease, serum and CSF should be obtained for assay of IgM and IgG antibodies to West Nile virus using enzyme-linked immunosorbent assays. | |
• Cerebrospinal fluid analysis of patients with West Nile virus neuroinvasive disease typically shows a moderate pleocytosis and an elevated protein level, with a normal glucose level. |
The United States Centers for Disease Control and Prevention has published a case definition for arboviral encephalitis or meningitis that is applicable to West Nile virus encephalitis and meningitis (49). There is presently no similar case definition for West Nile virus poliomyelitis. However, the criteria are easily modified to include poliomyelitis in the same line with encephalitis and meningitis.
IgM testing of serum or cerebrospinal fluid is recommended, followed by confirmatory neutralizing antibody testing in cases of possible exposure to cross-reacting flaviviruses, atypical presentation or death, or suspected unusual transmission modes, such as organ transplantation (104). Reverse transcription-polymerase chain reaction testing is often more sensitive than IgM testing in patients with severe immunocompromise.
Probable West Nile virus encephalitis or meningitis | ||
• Encephalitis or meningitis | ||
• Occurring when West Nile virus transmission is likely (late summer or early fall) | ||
- Single or stable (up to 2-fold change) elevated titer of West Nile virus-specific serum antibodies | ||
- Serum IgM antibodies detected by antibody-capture enzyme-linked immunosorbent assay, but with no available confirmatory results from West Nile virus-specific serum IgG antibodies | ||
Confirmed West Nile virus encephalitis or meningitis | ||
• Encephalitis or meningitis | ||
• Laboratory confirmation | ||
- Four-fold or greater increase in West Nile virus-specific serum antibody titer | ||
- Isolation of West Nile virus from, or demonstration of West Nile virus-specific antigen or genomic sequences in, tissue, blood, CSF, or other body fluid | ||
- West Nile virus-specific IgM antibodies demonstrated in CSF by enzyme-linked immunosorbent assay | ||
- West Nile virus-specific serum IgM antibodies (demonstrated by enzyme-linked immunosorbent assay) confirmed by West Nile virus-specific IgG antibodies (demonstrated by neutralization or hemagglutination inhibition) | ||
West Nile virus or another arbovirus (eg, St. Louis encephalitis virus) should be strongly considered in patients with unexplained encephalitis or meningitis in late summer or early fall (234).
Serologic testing for West Nile virus can be problematic because samples obtained within 8 days of infection may be falsely negative due to cross-reactivity between West Nile virus and other flaviviruses, and because of persistence of IgM antibodies (69; 234; 292; 73; 308; 90). False-positive results can occur with West Nile virus testing because of exposure to St. Louis encephalitis virus or dengue virus or because of previous vaccination for yellow fever or Japanese encephalitis (69; 234; 292; 308; 90). Cross-reactivity is particularly problematic when there are concurrent outbreaks of St. Louis encephalitis virus and West Nile virus infections (308). Also, West Nile virus IgM antibodies can persist for more than a year after initial infection, potentially producing confusion over whether the antibodies are a marker of current or previous infection (69; 234; 252; 73). In the latter case, a 4-fold increase in West Nile virus-specific neutralizing antibody titer between acute and convalescent serum drawn 7 to 14 days apart can confirm acute infection (234).
Due to antibody cross-reactivity, samples that are positive with premembrane/envelope-specific IgM antibody-capture enzyme-linked immunosorbent assays (MAC-ELISA) can be confirmed with a time-consuming plaque reduction neutralization test (PRNT) (90). A diagnostic algorithm combining the use of multi-antigen virus-like particle-specific and nonstructural-protein-1-specific MAC-ELISAs was developed. This approach can produce more specific and reliable results for the serodiagnosis of Japanese encephalitis virus and West Nile virus infections without the need for PRNT (90).
Nucleic acid amplification testing for West Nile virus (as has been used to screen minipool samples of blood donors) has been found to be diagnostically helpful in evaluating symptomatic patients as well, particularly in the first 8 days after onset of symptoms as viremia is common in early symptomatic West Nile virus infection (293). Nucleic acid amplification testing significantly improves diagnostic yield when combined with serology, and indeed the two approaches seem to be largely complementary (293).
In patients with suspected neuroinvasive disease, serum and CSF should be obtained for assay of IgM and IgG antibodies to West Nile virus using enzyme-linked immunosorbent assays (36; 69; 234; 102). Because IgM antibodies do not normally cross the blood-brain barrier, the presence of IgM antibody to West Nile virus in the CSF strongly suggests central nervous system infection. Positive ELISA results should be confirmed with the more specific plaque reduction neutralization test in cell culture, which may take 10 days to complete. This helps to eliminate false-positive results from cross-reactivity with other flaviviruses, especially St. Louis encephalitis virus.
Cerebrospinal fluid analysis of patients with neuroinvasive disease typically shows a moderate pleocytosis and an elevated protein level, with a normal glucose level (234; 73; 300). Mean cerebrospinal fluid white cell counts are about 200 cells/mm3 in those with either meningitis or encephalitis, although the range is fairly wide from less than five cells/mm3 to more than 500 cells/mm3 (300). Between one third and one half of initial cerebrospinal fluid samples have at least 50% neutrophils in their initial cerebrospinal fluid samples, with the remainder having a lymphocytic predominance (73; 300; 228). Encephalitis cases tend to have higher cerebrospinal fluid protein levels, but there is considerable overlap: approximately half of encephalitis cases and about 1/6 of meningitis cases have cerebrospinal fluid protein levels of 100mg/dl or greater (300). Cerebrospinal fluid studies are only a modest predictor of clinical outcome (300). Because IgM antibody does not cross the blood-brain barrier, West Nile virus-specific IgM antibody in CSF strongly suggests central nervous system infection (69; 234; 228), although some patients may have persistent West Nile virus IgM antibody responses (73). Repeat CSF testing may be necessary when initial serology is negative (108). CSF should also be cultured and analyzed by polymerase chain reaction techniques to detect West Nile virus nucleic acid. However, because isolation and PCR testing are relatively insensitive, negative results do not exclude West Nile virus infection (69; 234; 108).
CT of the brain is usually normal, and MRI is normal in up to 30% of cases (108). MRI may show enhancement of the leptomeninges, the periventricular areas, or both (234). Abnormalities identified on MRI typically involve the basal ganglia, thalamus, mesial temporal lobes, brainstem, and cerebellum (237; 108; 75; 202), but similar distributions of brain involvement are seen in other flavivirus infections, including Japanese encephalitis and St. Louis encephalitis (108). Hyperintensity on T2-weighted and FLAIR imaging with normal signal intensity on T1 is typical of West Nile virus encephalitis; diffusion restriction can be seen in up to half of cases (108; 75). Patients with West Nile virus-associated flaccid paralysis frequently have spinal cord or cauda equine abnormalities on magnetic resonance imaging (237).
In patients with West Nile virus poliomyelitis, laboratory findings included variable peripheral blood leukocytosis, normal cerebrospinal fluid glucose levels, elevated CSF protein levels, and variable degrees of lymphocytic CSF pleocytosis. Brain and cervical spinal cord imaging is generally either normal or shows incidental minor abnormalities that could not account for the presenting clinical manifestations (166), but some cases show T2 hyperintensities in the anterior horns of the spinal cord on magnetic resonance imaging, and others show evidence of meningitis or polyradiculitis (168; 06; 153; 265; 10). EMG and nerve conduction studies typically indicate a severe, asymmetric process affecting anterior horn cells, their axons, or both. Sensory amplitudes, motor distal latencies, conduction velocities, and F wave latencies are normal (in the absence of concomitant disease), whereas compound muscle action potentials are reduced (06). When electromyography is performed within 10 days of onset of weakness, fibrillations are absent, but recruitment is severely reduced with normal-appearing motor units in clinically weak muscles (06). After 2 weeks from the onset of illness, electromyography may show profuse spontaneous activity including fibrillation potentials in both strong and weak muscles (06).
IgM and neutralizing antibody tests confirm acute West Nile virus infections. Stool cultures and polymerase chain reaction studies for the presence of enterovirus are negative.
Increasingly, a spectrum of cord, nerve root, and peripheral nerve root pathology has been recognized in patients with West Nile virus infection (222; 221; 126; 270; 265). A small proportion of West-Nile-virus-associated flaccid paralysis have a more widespread myelitis, Guillain-Barre syndrome, lymphocytic infiltration of nerve roots, or axonal polyneuropathy, and rare cases develop isolated brachial neuritis (222; 221; 126; 270; 265; 30).
|
• There is no approved specific treatment for West Nile virus infection. | |
|
• Intensive supportive care is sometimes needed, including possible hospitalization, intravenous fluids, breathing support with a ventilator, and good nursing care. | |
|
• Neurologic rehabilitation may benefit those with prolonged functional decline after West Nile virus-associated meningoencephalomyelitis, but the outcomes remain highly variable. |
Although there is no approved specific treatment for West Nile virus infection, patients with symptoms such as high fever, confusion, headaches, or muscle weakness should seek medical attention immediately.
Intensive supportive care is sometimes needed, including possible hospitalization, intravenous fluids, breathing support with a ventilator, and good nursing care (102; 258; 109).
Some preliminary studies have suggested that patients with West Nile virus encephalitis may benefit from intravenous immunoglobulin from donors with a high frequency of West Nile virus exposure (273; 114; 259), but problems with loss of effectiveness over time and variability in production limit its use (217). A trial comparing an immunoglobulin product with high titers of anti-West Nile virus antibody, intravenous immunoglobulin, and normal saline found no significant differences between these groups for either the safety or efficacy endpoints (101).
In affected transplant recipients, treatment usually includes supportive care, reduction of immunosuppression, and frequent administration of intravenous immunoglobulin or in combination with interferon alfa-2b (319; 323; 140).
High-dose ribavirin and interferon alpha-2b also have some in vitro activity against West Nile virus, but there are no controlled trials of these drugs in people (122).
Humanized monoclonal antibodies with potent neutralizing activity are a potential treatment for patients, even after West Nile virus has infected central nervous system neurons (203).
Human monoclonal antibodies against West Nile virus nonstructural protein 1 (NS1) protect against lethal West Nile virus infection in mice, suggesting that antibodies targeting specific regions in the NS1 structure could serve as countermeasures that control West Nile virus infection in humans (317). NS1 is a 46 to 55 kDa glycoprotein that homodimerizes in the endoplasmic reticulum, where it functions as a scaffold to recruit viral and host factors necessary for replication (317). Infected cells also express dimeric NS1 on the plasma membrane and secrete a soluble, hexameric form, which can be detected in circulation in infected individuals (317). Extracellular forms of NS1 can bind to the surface of cells, can bind complement and Toll-like receptors to modulate or evade host immunity, and can interact with endothelial cells to regulate permeability across blood-tissue barriers (317). The West Nile virus NS1 dimer structure is comprised of three domains: (1) the b-roll; (2) the wing; and (3) the b-ladder or “b-platform”).
One monomer is gray, and one is color coded by domain (blue, b-roll; yellow, wing; red, b-ladder; and salmon, spaghetti loop). The disordered flexible loop is indicated by orange dashed lines. (Source: Wessel AW, Doyle MP, Engd...
One monomer is gray, and one is color coded by domain (blue, b-roll; yellow, wing; red, b-ladder; and salmon, spaghetti loop). The disordered flexible loop is indicated by orange dashed lines. (Source: Wessel AW, Doyle MP, Engd...
Neurologic rehabilitation may benefit those with prolonged functional decline after West Nile virus-associated meningoencephalomyelitis (15), but the outcomes remain highly variable (86).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Infectious Disorders
May. 15, 2026
General Neurology
May. 13, 2026
Infectious Disorders
May. 12, 2026
Infectious Disorders
May. 12, 2026
Infectious Disorders
May. 05, 2026
Infectious Disorders
May. 01, 2026
Infectious Disorders
Apr. 30, 2026
Headache & Pain
Apr. 10, 2026