








































































Infectious Disorders
Arboviral encephalitis
May. 15, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author explains the clinical presentation, pathophysiology, prevention, diagnostic work-up, and management of anthrax meningoencephalitis. Anthrax meningoencephalitis generally presents with fever, headache, vomiting, and confusion or agitation, but there may also be symptoms related to the source of infection (eg, cutaneous, gastrointestinal, or inhalational). Hemorrhagic meningitis should raise a strong suspicion of anthrax infection. Anthrax meningoencephalitis is usually rapidly fatal, with roughly two thirds of affected patients dying within 24 hours of presentation; however, there are now at least eight reported survivals following anthrax meningoencephalitis. Unfortunately, most physicians and hospitals are not adequately prepared to diagnose and manage potential bioterrorism agents, including anthrax, and not much has changed since the U.S. bioterrorism outbreak in 2001. Guidelines suggest that empiric treatment for anthrax in which anthrax meningitis is suspected, or cannot be ruled out, should include at least three antimicrobial drugs. The preferred regimen includes a fluoroquinolone (ciprofloxacin), a carbapenem (meropenem), and a protein-synthesis inhibitor (linezolid).
|
• Anthrax has been developed as a biological warfare agent by at least seven countries. It remains a significant bioweapons threat and is considered the most likely biological warfare agent. | |
|
• Meningoencephalitis may develop with any clinical type of anthrax, including cutaneous, gastrointestinal, mixed gastrointestinal and cutaneous, inhalational, and injectional. | |
|
• Injectional anthrax has emerged since 2009 among heroin users in Europe. | |
|
• Anthrax meningoencephalitis generally presents with fever, headache, vomiting, and confusion or agitation, but there may also be symptoms related to the source of infection (eg, cutaneous, gastrointestinal, or inhalational). | |
|
• Hemorrhagic meningitis should raise a strong suspicion of anthrax infection. | |
|
• Anthrax meningoencephalitis is usually rapidly fatal, with roughly two thirds of affected patients dying within 24 hours of presentation; however, there are at least eight reported survivals following anthrax meningoencephalitis. | |
|
• Guidelines suggest that empiric treatment for anthrax in which anthrax meningitis is suspected, or cannot be ruled out, should include at least three antimicrobial drugs. The preferred regimen includes a fluoroquinolone (ciprofloxacin), a carbapenem (meropenem), and a protein-synthesis inhibitor (linezolid). | |
|
• Most physicians and hospitals are not adequately prepared to diagnose and manage potential bioterrorism agents, including anthrax, and not much has changed since the U.S. bioterrorism outbreak in 2001. | |
|
• Anthrax is now classified as a category A biological warfare agent, a category of microorganisms or toxins that can be easily spread, leading to intoxication with high death rates. |
Anthrax derives its name from the Greek word for coal (anthrakis) because the disease is commonly associated with black, coal-like, cutaneous eschars.
Occupational anthrax (eg, woolsorters’ disease). In the 19th century and early 20th century, occupational anthrax was a common problem in the United States and Great Britain, affecting workers in agriculture and industries involving direct contact with animals or animal products (132; 06). Workers in industries processing wool, other animal hair and bristles, leather, and horn and bone were all at risk.
Hides and skins were usually imported in a raw state and had to be tanned before they could be used in manufacture. At the tannery, the skins were sorted and then soaked, which brought the “dry” hides to a moist flexible state ...
(Source: Andrews JB. Anthrax as an occupational disease. Bulletin of the United States Bureau of Labor Statistics No. 205. Industrial accidents and hygiene series. Washington, DC: U.S. Government Printing Office, 1917. Andrews ...
In the 19th and early 20th century, cutaneous anthrax was the most common form of occupational anthrax (as it is now).
Treatment, though, was limited, and about one in four affected workers died. Even in the early 20th century, treatment was limited to washing the wound and applying tincture of iodine. Internal administration of iodine, tonics, and stimulants (quinine, alcohol, coffee), inhalation of oxygen, and experimental serotherapy were also advocated. The Italian physician Achille Sclavo (1861-1930) produced in 1895 a serum therapy for anthrax that he initially used for experiments on animals, but by 1897 was using this serum in human patients with unprecedented success (141; 194).
It consisted of the injection, usually intravenously, of fluids from an immunized animal. After 6 years, he had only 10 deaths among 164 cases (6.1%), a marked improvement over the case fatality rate of 24.1% in Italy at the time (06; 07). Sclavo's anti-anthrax serum was introduced to Britain in 1904 by the enterprising British physician and first medical inspector of factories Sir Thomas Morison Legge (1863–1932) (194). Within months, the serum became regarded by medical practitioners as an effective treatment for cutaneous anthrax, though access to “fresh” serum and the necessary speedy diagnosis remained problematic.
In the early 20th century, another form of serotherapy was developed by Austrian pathologist and immunologist Rudolf Kraus, then working in Buenos Aires; Kraus and colleagues reported only one death among 140 cases using intravenous injection of normal ox serum heated for 30 minutes to 1324 °F (06; 07).
The U.S. government published the common appearance of anthrax on the skin at different stages as a guide to clinicians to facilitate recognition of the disease and similarly prepared diagrams of anthrax bacilli and spores.
(Source: Andrews JB. Anthrax as an occupational disease. Bulletin of the United States Bureau of Labor Statistics No. 205. Industrial accidents and hygiene series. Washington, DC: U.S. Government Printing Office, 1917. Andrews ...
(Source: Andrews JB. Anthrax as an occupational disease. Bulletin of the United States Bureau of Labor Statistics No. 205. Industrial accidents and hygiene series. Washington, DC: U.S. Government Printing Office, 1917. Andrews ...
Anthrax as an impetus to the development of microbiology and immunology. Because the burden of occupational anthrax was costly and threatened multiple industries, there were strong incentives to identify the cause of the disorder and to find potential preventive measures and treatments. Among these was German physician Robert Koch (1843-1910), who had been working in a rural general medical practice (120; 121; 122; 123; 124; 125; 31; 129; 22).
Halftone photomechanical print by German photographer Josef Albert (1825-1886). (Source: Bibliothèque interuniversitaire de Santé. https://www.biusante.parisdescartes.fr/histoire/images/index.php?refphot=CIPB0672. Licence Ouv...
Koch organized his own small microbiological laboratory, and with great discipline, he developed novel techniques and pursued innovative experiments.
By 1876, Koch had proven the microbiological nature of anthrax and worked out much of the biology of the responsible organism, Bacillus anthracis.
Koch sent a letter announcing his discoveries to the preeminent German biologist and bacteriologist Ferdinand Cohn (1828-1898), who invited Koch to Breslau to demonstrate his findings.
Koch's 3-day-long series of demonstrations was a resounding success, and his work was published in Cohn's Beitrage zur Biologie der Pflanzen (“Contributions to the biology of plants”) in July 1876, an event later considered to represent "the birth of modern bacteriology" (120; 22). German-Jewish pathologist Julius Friedrich Cohnheim (1839-1884), who was present at Koch's demonstrations, said, "I consider this to be the greatest discovery in the field of microorganisms and I believe that Koch will surprise and shame us all once again with further discoveries” (127).
To support his conclusions, Koch began photographing his findings and published his first photographs of Bacillus anthracis from cultures in 1877 (121). By 1881, he was able to demonstrate Bacillus anthracis in diseased tissue (122).
(x700) Section of liver from rabbit dying of anthrax. All capillaries are more or less filled with anthrax bacilli. Individual anthrax bacilli appear in the capillary network surrounding the liver cells. (Source: Koch R. Zur Un...
(x500) Section from the kidney of a rabbit with anthrax. The glomerulus, partially densely filled with bacilli. (Source: Koch R. Zur Untersuchung von pathogen Organism. Mitheilungen aus dem Kaiserlichen Gesundhetisamte 1881a;1:...
In 1880, French veterinary surgeon Jean Joseph Henri Toussaint (1847-1890) developed an early anthrax vaccine, and because Toussaint was not a member of the French Academy of Sciences, his paper describing his accomplishment was presented before the academy by French veterinarian and pathologist Henri Bouley (1814-1885) on July 12, 1880. Toussaint had tested his attenuated vaccine on eight dogs and 11 sheep, half of which died after inoculation, a result that was not particularly compelling.
However, almost all of the credit for the creation of an anthrax vaccine went to French microbiologist Louis Pasteur (1822-1895) (55).
Pasteur gave a celebrated demonstration of anthrax vaccination on sheep at Pouilly-le-Fort in May 1881, using a vaccine that he portrayed as having been developed like his prior vaccine for chicken cholera, ie, by attenuating the microbe with prolonged exposure to atmospheric oxygen. He also commanded that his assistants publish nothing about this during his lifetime.
In the demonstration, 24 sheep, one goat, and six cows were inoculated twice with an anthrax vaccine on May 5 and 17, 1881, whereas a control group of 24 sheep, one goat, and four cows remained unvaccinated.
On May 31, all the animals were inoculated with anthrax bacilli, and the results were examined on June 2. All but one of the vaccinated animals remained healthy, whereas the unvaccinated sheep and goats had all died by the end of the day, and the unvaccinated cows were all manifesting symptoms of anthrax. Pasteur accepted the accolades he received and publicly attributed his success to his preparatory experiments.
However, 40 years after Pasteur's death, new facts emerged from Pasteur's nephew that Pasteur had instead used a method similar to that employed by Toussaint, killing the microbe with potassium bichromate. Pasteur's laboratory notebooks became available for study only in the 1970s, and careful analysis proved that Pasteur was guilty of scientific misconduct, and, as some have alleged, fraud. As American historian Gerald L. Geison (1943-2001) concluded in his award-winning The Private Science of Louis Pasteur (1995), "Pasteur deliberately deceived the public and the scientific community about the nature of the vaccine actually used at Pouilly-le-Fort." Instead of an oxygen-attenuated live vaccine, Pasteur had in fact used a potassium dichromate-killed vaccine, employing a process very much like Toussaint's. Pasteur subsequently developed an oxygen-attenuated anthrax vaccine (that nevertheless lost potency over time), but at the time of the Pouilly-le-Fort demonstration, Pasteur's own approach to vaccine development had not progressed to a satisfactory state. Pasteur never gave proper credit to Toussaint for his discovery, nor did he acknowledge having used Toussaint's method for the celebrated demonstration (183; 83; 192; 193; 56).
Use of anthrax as a biological warfare agent. Anthrax has so far been used on a limited basis as either a biological warfare or bioterrorism agent. In World War I, German agents reportedly tried to infect Allied horses as they were being shipped to the European front (58; 222), although other accounts discount this claim (191). Japan reportedly first developed anthrax as a bioweapon in the 1930s and used anthrax against China during World War II (191; 58; 208; 90; 222). In 1993, the Japanese terrorist group Aum Shinrikyo dispersed aerosols of anthrax and botulism throughout Tokyo on at least eight occasions (104), but these attacks failed to produce illness, apparently in part because the terrorists mistakenly used a harmless anthrax strain developed for vaccines (174). In 2001, anthrax was used as a bioterrorism agent in the United States, with several deaths, more than 20 cases, and over 32,000 individuals receiving postexposure prophylaxis because of anthrax delivered through the United States mail system (42).
The United States began research on offensive bioweapons in 1943 at Camp Detrick (now Fort Detrick) in Frederick, Maryland. To assess the risk of covert biological attacks in the 1960s, the army conducted large-scale covert tests at various civilian sites (eg, National Airport and Greyhound Terminal in Washington, D.C., and the New York City subway) using the anthrax simulant Bacillus globigii (191). The United States bioweapons program, which included the development of weaponized anthrax, was terminated in 1969 following an Executive Order by President Richard Nixon. All stockpiles of biological agents were destroyed by May 1972 (208). There is no evidence that these U.S. weapons were ever deployed.
In 1972, the United States, the United Kingdom, and the U.S.S.R. signed the Convention on the Prohibition of the Development, Production, and Stockpiling of Bacteriological (Biological) and Toxin Weapons and on Their Destruction ("The Biological Weapons Convention") (208). This treaty prohibits research, development, and stockpiling of biological agents for offensive military purposes. Although this biological weapons treaty has since been ratified by more than 140 countries, biological warfare research and the development of biological weapons continued in many countries (208).
The Soviet bioweapons program began before World War II under the auspices of Biopreparat, their bioweapons agency. This program continued until the 1990s, despite the Biological Weapons Convention. By the 1980s, Biopreparat could produce thousands of tons of weaponized anthrax annually. Biopreparat also developed antibiotic-resistant anthrax using recombinant DNA techniques.
In April 1979 accidental release of anthrax spores occurred at a military bioweapons factory (Military Compound 19) in Sverdlovsk in the former Soviet Union (now Yekaterinburg, Russia) (02; 144; 106; 58; 208; 218). This incident resulted in at least 66 human deaths (among the 77 patients identified) in a narrow zone up to 4 kilometers downwind from the facility, as well as outbreaks of anthrax in livestock up to 50 kilometers downwind (144). Although the Soviet Ministry of Health initially blamed the deaths on cutaneous and gastrointestinal anthrax occurring from consumption of contaminated meat, this scenario was doubted by military sources in the West (64; 162; 02; 144; 106; 58; 208). In 1992, Russian President Boris Yeltsin confirmed that this outbreak was a result of "military developments" (144), and clinical and epidemiologic studies documented inhalational anthrax from a mixture of different Bacillus anthracis strains as the cause (02; 144; 106).
In the aftermath of the Gulf War, Iraq acknowledged to the United Nations Special Commission Team 7 that it had conducted biological weapons research on a number of agents, including Bacillus anthracis (208). Further details were uncovered in 1995. Iraq had extensive research facilities at multiple sites, including Salman Park on the Tigris River. Iraq conducted field trials with Bacillus subtilis (an anthrax simulant) and various biowarfare agents using various delivery systems, including rockets, aerial bombs, sprayers attached to helicopters, and possibly unmanned drones (208). To reduce particle size in order to maximize the delivered dose of anthrax, Iraq used sequential filters in an arrangement reportedly similar to that used at Camp Detrick in the 1950s. Iraq produced 8500 liters of concentrated anthrax, of which 6500 liters were placed into R400 bombs, Al Hussein warheads, and other devices (208).
Anthrax has been developed as a biological warfare agent by at least seven countries. It remains a significant bioweapons threat and is considered the most likely biological warfare agent, as it is stable in spore form and can be stored for prolonged periods (63). It is easy and cheap to produce; there is no natural immunity in industrialized nations; it can be dispersed in the air; the inhalational form is highly lethal; and the agent is difficult to detect (209). Nevertheless, aerosolized anthrax has not yet been used on the battlefield, possibly in part because of "moral repugnance" of biological weapons, potential retaliation in kind, delayed manifestations following use, and uncertain effects depending on weather conditions (175). Indeed, the uncertainties of such weapons are demonstrated by the Sverdlovsk incident in the U.S.S.R. in 1979, which involved the accidental release of an estimated 10 kilograms of weapons-grade anthrax spores: this accident produced a total of 66 fatalities among a potentially exposed population of 1.2 million people (175).
Offensive anthrax bioweapons were initially manufactured as slurries of highly concentrated bacteria. Although easy and safe to manufacture, such slurries had to be refrigerated for storage and were difficult to disseminate (58). Later, freeze-dried powder formulations of anthrax spores were developed as bioweapons that, although technically difficult and dangerous to manufacture, were thermally stable without refrigeration and were easily disseminated (58). Bioweapon anthrax may also be modified to be multidrug-resistant and may be stabilized with other substances (eg, silica) to decrease electrostatic charges imparted by the milling process and thereby keep the particles from clumping. The latter issue is critical because biowarfare agents are most effectively delivered as an aerosol of particles from 1 to 5 microns in size (58). Particulates in this size range behave similarly to a gas and are taken into bronchioles and alveoli during respiration, whereas larger particles are much more difficult to disperse, rapidly fall to the ground, or become trapped in the upper airway (58). Anthrax aerosols are invisible, odorless, colorless, and tasteless.
Use of anthrax in bioterrorism. In late 2001, an anthrax outbreak attributed to bioterrorism occurred in the United States. Anthrax was spread through the mail (47; 39). Twenty-two cases were identified, 11 with inhalational anthrax and 11 with cutaneous anthrax (45; 43; 46; 47; 108; 105; 86). Five of the inhalational cases died. Only one of these cases had documented anthrax meningoencephalitis (108).
The FBI alleges that the 2001 anthrax bioterrorism outbreak in the United States was conducted by U.S. Army biodefense scientist Bruce Ivins, who worked at the U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID) in Fort Detrick, Maryland (146; 33). In 2008, shortly before these allegations were made public, Ivins committed suicide. The FBI employed a complex strategy to identify the source of the anthrax: (1) spores from the mailed envelopes were cultured, yielding thousands of colonies, one from each spore; (2) a small number of colonies with unusual features (“minority phenotypes”) were identified, and the genomes of these colonies were completely sequenced to identify the corresponding mutations; (3) tests were developed to screen anthrax samples for four of these mutations, using a polymerase chain reaction-based strategy; these molecular tests were applied to more than 1000 isolates from labs in the United States and other countries (75). In only eight of the study’s samples were all four mutations identified, and all were directly related to spores Ivins had created in 1997 (75). However, in February 2011, a scientific panel of the U.S. National Academy of Sciences independently evaluated the genetic evidence and concluded that it was insufficient to prove that Ivins was responsible. In addition, Ivins's laboratory did not contain the equipment needed to manufacture the refined powder of spores that were implicated in the 2001 bioterrorism attacks (33).
Anthrax is now classified as a category A biological warfare agent, a category of microorganisms or toxins that can be easily spread, leading to intoxication with high death rates (12). Other biological warfare agents in this category include botulism, plague, smallpox, tularemia, and viral hemorrhagic fevers (12; 14).
|
• There are three principal clinical forms of anthrax, which are categorized by the route of exposure: (1) cutaneous, (2) gastrointestinal, and (3) inhalational. | |
|
• A new form of anthrax, injectional anthrax, has emerged among heroin users in Europe. | |
|
• Systemic anthrax is typically fatal. | |
|
• Cutaneous anthrax is the predominant clinical form in naturally acquired anthrax, accounting for more than 95% of naturally occurring B. anthracis infections. | |
|
• Gastrointestinal anthrax occurs from 1 to 7 days following ingestion of large numbers of anthrax endospores, usually associated with eating undercooked contaminated meat. | |
|
• Inhalational anthrax typically develops from 2 to 10 days of respiratory exposure to aerosolized anthrax endospores, but cases may present up to 6 or 7 weeks after exposure. | |
|
• Meningoencephalitis may develop with any clinical type of anthrax, including cutaneous. | |
|
• Anthrax meningoencephalitis generally presents with fever, headache, vomiting, and confusion or agitation, but there may also be symptoms related to the source of infection (eg, cutaneous, gastrointestinal, or inhalational). |
There are three principal clinical forms of anthrax, which are categorized by the route of exposure: (1) cutaneous, (2) gastrointestinal, and (3) inhalational. A new form of anthrax, injectional anthrax, has emerged among heroin users in Europe (18; 66; 114). Regardless of the route of exposure, B. anthracis can spread through the bloodstream, causing systemic disease, septic shock, and death. Systemic anthrax is typically fatal.
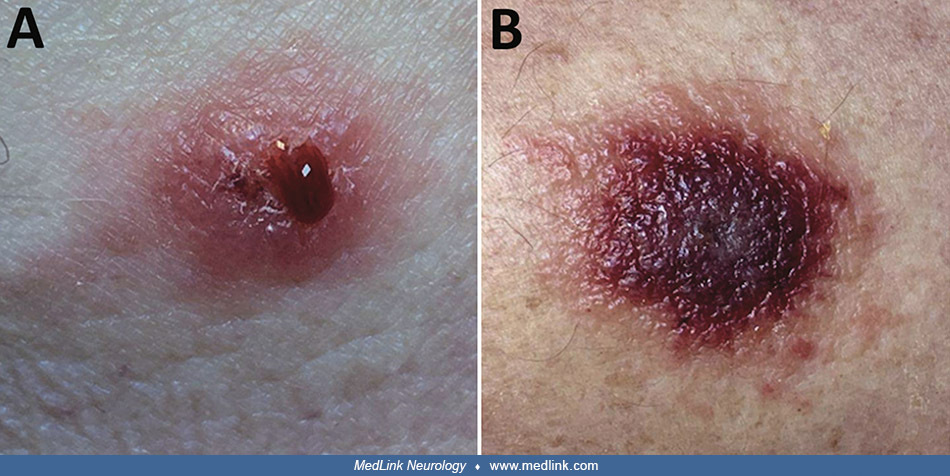
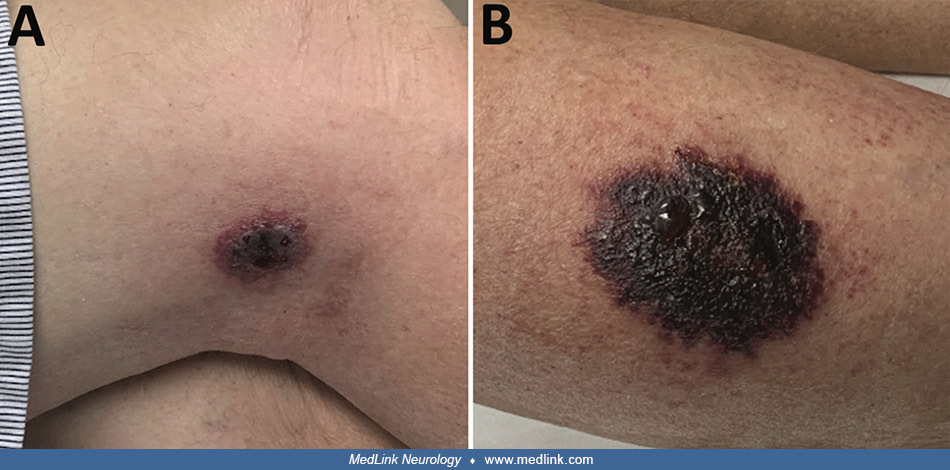
Cutaneous anthrax. Cutaneous anthrax is the predominant clinical form in naturally acquired anthrax, accounting for more than 95% of naturally occurring B. anthracis infections (14). Cutaneous anthrax is associated with handling infected animals or animal products (eg, meat, wool, hides, leather, or hair products) (149; 101; 154; 164; 118; 133; 03; 79; 139; 156; 08; 91; 163) and can sometimes be acquired by contamination of preexisting skin lesions with B. anthracis spores from the soil (71). Cutaneous anthrax typically develops in exposed skin areas (eg, face, neck, arms, hands) from 2 to 12 days after endospores are introduced into minor skin abrasions, but the incubation period can range from one to over 19 days (144; 68; 222; 149; 164; 163). Pruritic, erythematous papules from 1 to 2 cm in size progress to a vesicle or vesicles containing serosanguineous fluid and then evolve to a painless necrotic ulcer with a black eschar, associated with progressive regional edema and lymphadenitis (72; 77; 80; 180; 105; 52; 149).
Lateral view of a patient’s right forearm and hand, showing a large cluster of boils, or carbuncles, located primarily on the hand and wrist, which had manifested during a cutaneous anthrax infection caused by the bacterium,
View of a man's left forearm, showing a large cutaneous lesion, which had been diagnosed as a case of cutaneous anthrax caused by the bacterium, Bacillus anthracis. Note the characteristic dark-brown to black-colored e...
Clinical features in severe cases typically include fever, headache, malaise, hemorrhagic bullous lesions surrounded by an extensive erythema and edema, and leukocytosis; in occasional cases, patients develop septic shock (68).
Predictors of developing meningitis or dying include the following: fever or chills; diastolic hypotension; headache; anxiety; nausea or vomiting; abdominal pain; malignant pustule edema; thoracic edema; lymphadenopathy; leukocytosis; bacteremia; and coagulopathy (205).
Gastrointestinal anthrax. Gastrointestinal anthrax occurs from 1 to 7 days following ingestion of large numbers of anthrax endospores, usually associated with eating undercooked contaminated meat (36; 11; 222; 118; 151; 153; 21; 08; 89; 163). Infection may be associated with preexisting lesions in the alimentary tract, especially in the oropharynx (222). Initial symptoms may include fever, anorexia, nausea, vomiting, hematemesis, abdominal pain, bloody diarrhea, and hemorrhagic ascites (58; 36; 105; 222). In a review of the clinical features of hospitalized patients with anthrax, more than half with ingestion of anthrax developed ascites (91). Toxins destroy the mesenteric lymph nodes and the blood supply to the small bowel, producing bowel ischemia, peritonitis, and septicemia.
Inhalational anthrax. Naturally acquired inhalational anthrax is rare in the United States; only 19 cases were identified over the last century, with most occurring in special occupational risk groups (29; 51). Inhalational anthrax typically develops from 2 to 10 days of respiratory exposure to aerosolized anthrax endospores, but cases may present up to 6 or 7 weeks after exposure (144; 222). The mediastinal lymph nodes are the nidus of bacterial proliferation. Initial symptoms usually resemble a viral respiratory illness and may include fever, chills, diaphoresis, headache, myalgias, dyspnea, sore throat, cough (usually nonproductive), a feeling of heaviness in the chest, pleuritic pain, malaise, and weakness (144; 58; 44; 42; 38; 51; 105; 10). Some may present with symptoms suggestive of a gastroenteritis or cholecystitis, with nausea, vomiting, diarrhea, and abdominal pain before developing more serious respiratory symptoms (169; 42; 38; 105). Some may present with chest pain of sufficient acuteness and severity to suggest myocardial infarction (02). Chest radiography often reveals a widened mediastinum but does not show pneumonia (10). In a review of the clinical features of hospitalized patients with anthrax, most patients with inhalation of anthrax developed pleural effusions (91). Apparent clinical improvement over several days may be followed by abrupt worsening, with severe respiratory distress, septic shock, and death within 36 hours (58). About half of the cases ultimately develop hemorrhagic meningitis (02). Physical findings are usually nonspecific. Based on animal studies using nonhuman primates, the lethal dose is estimated to range from 2500 to 760,000 spores (222).
Injectional anthrax. Since 2009, injectional anthrax has emerged among heroin users in Europe (18; 66; 114). More than 70 cases have been reported from Denmark, France, Germany, and the United Kingdom. Many of these cases presented as a severe soft tissue infection, without a history of animal contact. The unfamiliar characteristics of injectional anthrax have led to diagnostic delays, inadequate treatment, and high case fatality rates (18). Cases of injectional anthrax commonly require surgical debridement (18).
Genome-based characterization of injectional anthrax isolates has identified two tight clusters that imply at least two separate disease events spanning more than 12 years, with one group exclusively associated with the 2009 to 2010 outbreak and located primarily in Scotland, and the second comprised of later (2012 to 2013) cases but also including a single Norwegian case from 2000 (114). Because of the genomic similarity of the two clusters, they were both probably caused by separate contamination events originating from the same geographic region (114).
Anthrax meningoencephalitis. Meningoencephalitis may develop with any clinical type of anthrax, including cutaneous (201; 173; 170; 69; 81; 117; 130; 138; 225; 164; 171), gastrointestinal (200; 130), mixed gastrointestinal and cutaneous (117; 130), injectional (95), and inhalational (05; 169; 02; 32; 130). Meningitis is most common among cases of inhalational anthrax, where it may occur in up to half of cases (05; 169; 28; 29; 02; 58; 130); however, among the 10 cases of confirmed or suspected inhalational anthrax related to the bioterrorist outbreak of anthrax in the United States in 2001, only the index case had documented meningitis (32; 41; 44; 42; 108; 130). Meningitis develops in 5% or fewer of cases of cutaneous anthrax (186; 138); however, most cases of anthrax meningitis develop from cutaneous anthrax, as the vast majority of naturally acquired cases of anthrax are cutaneous (130). Meningitis may occur rarely without a clinically apparent primary focus (70; 173; 170; 77; 130; 11; 82).
Anthrax meningoencephalitis generally presents with fever, headache, vomiting, and confusion or agitation, but there may also be symptoms related to the source of infection (eg, cutaneous, gastrointestinal, or inhalational) (05; 169; 70; 201; 173; 170; 200; 69; 81; 117; 226; 04; 110; 130; 203; 19; 34). Many patients present in extremis following a prodromal period of 1 to 6 days, and two thirds die within 24 hours of admission. Clinical signs on presentation frequently include fever (39.5°C to 41°C), malaise, meningeal signs, hyperreflexia often with bilateral Babinski signs, and delirium or stupor. Other clinical findings may include focal or generalized seizures, myoclonus, fasciculations, generalized rigidity possibly progressing to trismus and opisthotonos, lateralizing signs including unilateral fixed and dilated pupil with contralateral hemiplegia, and decerebrate posturing. Pathologic findings include hemorrhagic meningitis, with extensive edema, inflammatory infiltrates, and numerous gram-positive rods (67; 130; 145). The extensive hemorrhage of the leptomeninges gives them a dark red appearance on gross examination at autopsy, a finding referred to as a "cardinal's cap" (02). Uncommonly, there may be multiple intraparenchymal heterogeneous lesions or areas of ring contrast enhancement and a central diffusion restriction, compatible with abscesses (171).
Atypical anthrax presentations. Atypical presentations of anthrax can occur in patients without known cutaneous, gastrointestinal, or inhalational ports of entry (99). Patients with atypical presentations are less likely to have cough, chest pain, or abnormal lung examination findings (99). Rarely, atypical presentations of anthrax can manifest as meningoencephalitis, so-called “primary anthrax meningitis” (19; 82).
Untreated, the case fatality from cutaneous anthrax is about 20% to 30%, compared to 25% to 60% with gastrointestinal anthrax, and nearly 100% with inhalational anthrax. With treatment, mortality is less than 1% with cutaneous anthrax (58; 222; 92), whereas mortality remains high, even with aggressive treatment, with gastrointestinal or inhalational anthrax (98; 92). Inhalational anthrax was generally thought to be fatal in 80% to over 90% of cases (169; 29; 02; 222), but the mortality in the 2001 U.S. outbreak has been much better than anticipated (five of 11 cases or 45%) with the use of aggressive treatment and intensive care unit support, including mechanical ventilation and dialysis as necessary (42; 222). Since 2001, eight of 15 (53%) known patients with inhalation anthrax have survived with early diagnosis, combination antimicrobial drug treatment to eradicate the bacteria and inhibit toxin production, and aggressive pleural effusion management (92). Initiation of antibiotic or anthrax antiserum therapy during the prodromal phase of inhalational anthrax is associated with markedly improved survival compared with initiation of treatment of fulminant cases (98). Nevertheless, anthrax survivors report significant health problems and poor life adjustment one year after the onset of bioterrorism-related anthrax (176).
Anthrax meningoencephalitis is usually rapidly fatal, with roughly two-thirds of affected patients dying within 24 hours of presentation (130; 165), although there is a small number of reported survivals following anthrax meningoencephalitis (62; 186; 215; 201; 204; 116; 200; 130; 19). In a systematic review, survival of anthrax meningitis was predicted by treatment with a bactericidal agent and the use of multiple antimicrobials (112). There is limited information on long-term outcomes among the few survivors, but several cases were reported to have fully recovered (201; 200; 130; 19).
A 63-year-old man presented with a 4-day history of fever, myalgias, malaise, nausea, vomiting, and confusion (32; 108). He was treated with intravenous cefotaxime and vancomycin for presumed bacterial meningitis. Examination revealed a temperature of 39°C, no nuchal rigidity, absent Kernig and Brudzinski signs, and no cranial neuropathies or focal neurologic findings. The white blood cell count was 9400 with 77% neutrophils. Chest x-ray showed a widened mediastinum and basilar infiltrates. A computed tomography scan of the head without intravenous contrast was normal. A lumbar puncture showed cloudy CSF. Gram stain of CSF showed many polymorphonuclear leukocytes and numerous large gram-positive rods, singly and in chains. CSF laboratory studies disclosed relative hypoglycorrhachia (with CSF glucose 57 mg/dl and blood glucose 174 mg/dl), increased protein (666 mg/dl), red cells (1375 per cubic ml), and a polymorphonuclear pleocytosis (4750 white cells with 81% polymorphonuclear). A diagnosis of anthrax meningoencephalitis was considered based on the CSF results, and high-dose intravenous penicillin therapy was added. Within 6 hours, CSF cultures grew colonies of gram-positive rods, which were presumptively identified as Bacillus anthracis within 18 hours and confirmed as such within 36 hours. His hospital course was complicated by coma, generalized convulsive seizures, hypotension, azotemia, hyperkalemia, and acidosis. Cultures of blood and CSF grew Bacillus anthracis. Autopsy was performed and was consistent with inhalational anthrax; the central nervous system was not included in the autopsy. Subsequent investigation identified the probable source of exposure as an anthrax-contaminated letter, sent as part of an outbreak of anthrax bioterrorism in the United States. This was the index case of that outbreak.
|
• Anthrax is caused by a large, encapsulated, gram-positive, aerobic, nonmotile, spore-forming bacillus, Bacillus anthracis. | |
|
• The spore is the infectious form commonly found in the environment. | |
|
• Anthrax has been developed as a biological warfare agent by at least seven countries. It remains a significant bioweapons threat and is considered the most likely biological warfare agent, as it is stable in spore form and can be stored for prolonged periods, it is easy and cheap to produce, there is no natural immunity in industrialized nations, it can be dispersed in air, the inhalational form is highly lethal, and the agent is difficult to detect. | |
|
• Following inhalation, anthrax spores are phagocytized by alveolar macrophages and transported to tracheobronchial lymph nodes, causing some to label the alveolar macrophages as “Trojan horse cells.” | |
|
• By the time that clinical symptoms appear, deadly toxins have already been produced, and it may be too late for antibiotics to alter the outcome. | |
|
• Full virulence of Bacillus anthracis requires an antiphagocytic capsule and the tripartite anthrax toxin, which is comprised of three proteins: (1) protective antigen, (2) edema factor, and (3) lethal factor. |
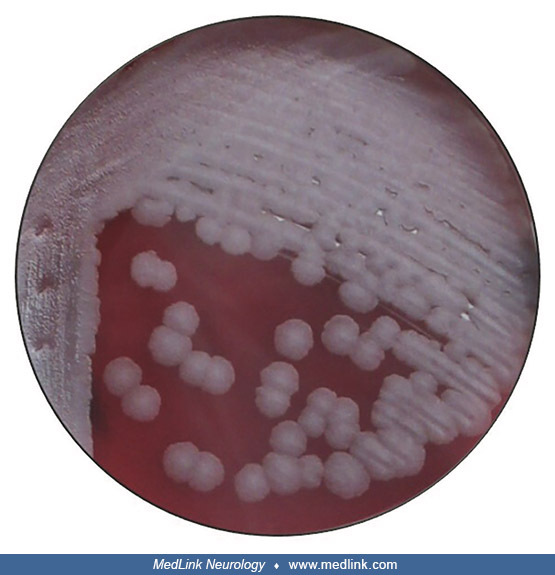
The Bacillus anthracis bacterium. Anthrax is caused by a large, encapsulated, gram-positive, aerobic, nonmotile, spore-forming bacillus, Bacillus anthracis. The spore is the infectious form commonly found in the environment (222).
Cultured colonies of Bacillus anthracis typically exhibit a roughly textured surface and irregular edges and may also exhibit a classic "medusa-head" or "judge's wig" morphology, a term given to colonies whose edges resemble a tangled mass of curly hair.
Colonies also exhibit a characteristic "tenacity," such that a small spire of colonial matter remained standing on its own support without toppling.
Viewed from the side, this low-magnification view of a Petri dish culture plate, shows two Bacillus anthracis bacterial colonies. The colony on the left was untouched, whereas the colony on the right was teased, thereb...
Bacillus anthracis may have different morphologic characteristics exhibited by the same microorganism when grown on different growth media, a phenomenon that is applied in the "encapsulation test.”
This image depicts a view of a Petri dish culture plate, which was partitioned down its center to perform an encapsulation test. On the left is a bicarbonate agar growth medium, and on the right is a blood agar growth medium. E...
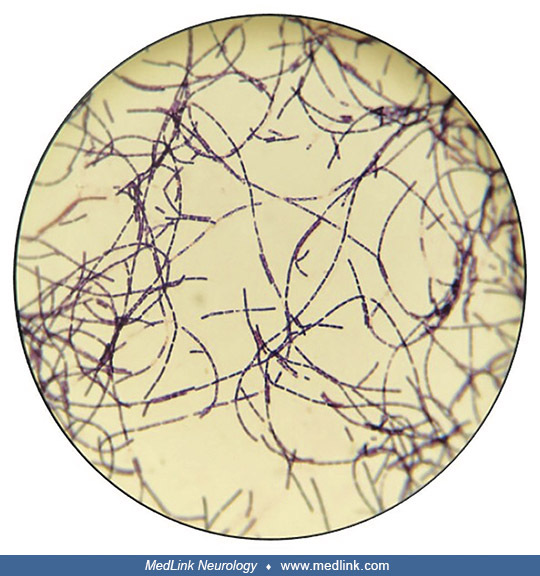
Bacillus anthracis tends to grow in long filamentous strands, which have a characteristic appearance on Gram-stained specimens.
Other stains may bring out additional features. For example, using the malachite green spore-staining technique can highlight green-stained endospores among red-colored, Bacillus anthracis bacteria.
Under a magnification of 1000X and using the malachite green spore staining technique, this photomicrograph highlights the green-stained endospores seen amongst these red-colored, Bacillus anthracis bacteria. (Photomic...
Some additional ultrastructural morphology of Bacillus anthracis bacteria can be visualized with light microscopy using special stains and growth media.
This photomicrograph reveals some of the ultrastructural morphology of Bacillus anthracis bacteria, which had been processed using M'Fadyean capsule stain and grown at 35°C on a growth medium of defibrinated horse bloo...
Greater ultrastructural detail is obtained using transmission electron microscopy.
Transmission electron microscopic image of Bacillus anthracis bacteria from an anthrax culture, showing cell division (A) and an endospore (B). (Image taken by CDC Pathologist Sherif R Zaki [1955-2021] and Elizabeth Wh...
Anthrax meningitis. Anthrax meningitis is histologically characterized by an influx of neutrophils and monocytic cells, hemorrhage, edema, vascular congestion, and the presence of B. anthracis bacteria in the cerebrospinal fluid. There may be associated focal intracerebral hemorrhage, subarachnoid hemorrhage, intraventricular hemorrhage, and diffuse cerebral edema.
Photomicrograph showing histopathologic details in a fatal human case of hemorrhagic meningitis due to anthrax. Note the rod-shaped, darkly stained Bacillus anthracis bacteria. (Source: CDC. Photograph by Dr. Marshall ...
Photomicrograph of a meningeal tissue sample demonstrating darkly stained, rod-shaped Bacillus anthracis bacteria from a fatal human case of inhalation anthrax. (Source: CDC. Photograph by Dr. LaForce, 1967. Public Hea...
Inhalation anthrax. Following inhalation, anthrax spores are phagocytized by alveolar macrophages and transported to tracheobronchial lymph nodes, causing some to label the alveolar macrophages as “Trojan horse cells” (182; 58; 88; 14). The spores germinate beyond the lungs in the lymphatics. At the tracheobronchial lymph nodes, local toxin production causes a necrotizing edematous lymphadenitis, progressing to mediastinitis and pulmonary edema, possibly with a bloody pleural effusion (182; 84; 78; 58).
Photomicrograph of a lymph node tissue sample (H&E), harvested at autopsy, from a 33-year-old patient with inhalation anthrax. Histopathologic findings of tissue necrosis. (Source: CDC. Photograph by S Benesky, 1966. Public...
Photomicrograph of a tissue specimen harvested from the bronchus of a deceased 60-year-old man, showing cytoarchitectural changes of inhalation anthrax (H&E). (Source: CDC. Photograph by Sidney J Brodsky, 1966. Public Healt...
Phagocytic dendritic cells (CD11c+ cells) probably serve as conduits of B. anthracis spores from the lung to the draining lymph nodes (187). The bacteria escape the lymphatic system and enter the bloodstream (bacteremia). About half of the cases of inhalational anthrax develop a concurrent hemorrhagic meningoencephalitis with bloody, purulent spinal fluid (84; 02; 78; 58). Septicemia, toxic shock, and death rapidly follow in less than 48 hours (182; 58). Bacillus anthracis efficiently invades human brain microvascular endothelial cells, comprising the blood-brain barrier (210).
Clinically similar presentations, particularly fatal pneumonia, can occur with inhalation exposure to Bacillus cereus containing Bacillus anthracis toxin genes, particularly in immunocompromised hosts (97; 96; 159; 09). Bacillus cereus (a soil organism that is also an opportunistic pathogen) is closely related to Bacillus anthracis.
Gastrointestinal anthrax. Grazing animals can acquire anthrax by ingesting anthrax spores that persist in soil. Spores germinate in the gastrointestinal tract and precipitate disease in a dose-dependent manner (158). Inoculation of vegetative bacilli also results in gastrointestinal anthrax. Exposure of anthrax-infected carcasses to oxygen triggers sporulation and further contamination of the surrounding soil. Virulence is severely affected by the loss of capsule (pXO2-encoded) but only moderately in the absence of toxins (pXO1-encoded), although the lack of toxins leads to reduced bacterial replication in infected hosts.
Pathological examination of infected tissue reveals edema, necrosis, and bacilli in the lymphatics with lymphadenitis.
“The jail-break model” in cutaneous and gastrointestinal anthrax. An alternate model, the so-called “jail-break model,” has been proposed for initial growth and dissemination of anthrax in cutaneous and gastrointestinal anthrax, and possibly for inhalational anthrax. In this model, (1) spores germinate at the site of initial entry into capsulated bacteria and start producing toxins; (2) bacterial growth and toxins cause epithelial/endothelial lining disruption; (3) bacteria pass through the damaged barrier, enter the lymphatics, and then reach the blood stream without requiring phagocytic transport (85; 214; 14).
Bacterial toxins and virulence factors. Bacterial toxins have long been felt to play a major role in clinical anthrax, because many effects of Bacillus anthracis cannot be attributed to microscopically evident tissue changes (23; 72). By the time that clinical symptoms appear, deadly toxins have already been produced, and it may be too late for antibiotics to alter the outcome.
Full virulence of Bacillus anthracis requires an antiphagocytic (poly-γ-D-glutamic acid) capsule and the tripartite anthrax toxin, which is comprised of three proteins: (1) protective antigen, (2) edema factor, and (3) lethal factor (107; 25). These toxins are thought to be responsible for the primary clinical manifestations of hemorrhage, edema, necrosis, and death. Protective antigen serves as an essential carrier molecule for edema factor and lethal factor (in binary combinations) and enables penetration of the toxins into cells by a complex process involving actin-dependent endocytosis (01; 181; 224).
Protective antigen is activated proteolytically in the blood and tissues and, once activated, binds to anthrax toxin receptors on cell surfaces (25). Specifically, to reach the endosomes, the anthrax toxin hijacks the endocytic pathway of CMG2 and TEM8, the two anthrax toxin receptors (76; 197). The pore-forming subunit of the toxin then inserts itself into endosomal membranes, preferentially into intraluminal vesicles (rather than the limiting membrane of the endosome), leading to the translocation of the enzymatic subunits into the lumen of these vesicles (76; 197). Then the enzymatic subunits reach the cytoplasm either by direct translocation or by back-fusion of intraluminal vesicles of late endosomes. In the cytoplasm, lethal factor cleaves members of the mitogen-activated protein (MAP)/extracellular signal-regulated kinase (ERK) family (or MEK) to inhibit nuclear protein synthesis (219; 76). This disables downstream ERK, p38, and JNK pathway signaling, leading to tissue damage and mortality (136). ERK pathway reactivation prevents anthrax toxin lethality in mice (136). The enzymatic subunits can also be released from the cell in exosomes.
Edema factor and lethal factor actively suppress chemokine production and neutrophil recruitment during infection, which allows the anthrax bacillus to reproduce and spread unimpeded (210).
Edema factor is a calmodulin-dependent adenylate cyclase that combines with protective antigen to form edema toxin; edema toxin increases cyclic AMP and produces local edema and impairs neutrophil function (77; 67; 198; 25; 136). Although it had been postulated that the in vivo toxicity of edema toxin is mediated by cAMP-dependent events, this is not the case; instead, edema toxin-induced ATP depletion plays an important role in the toxin's pathogenesis (134).
Lethal factor is a zinc metalloprotein that combines with protective antigen to form lethal toxin, a protein kinase; lethal toxin stimulates macrophages to release large quantities of pro-inflammatory cytokine molecules (ie, tumor necrosis factor alpha and interleukin-1 beta), resulting in shock (77; 67; 198; 223; 136). Lethal toxin is critical to bacterial penetration of the blood-brain barrier and development of meningoencephalitis because it disrupts brain microvascular endothelial monolayer integrity and endothelial tight junction protein zone occludens-1 (ZO-1) (74). Lethal toxin also attacks host immunity through multiple mechanisms, including attenuation of macrophage pro-inflammatory responses, suppression of dendritic cell function, and blocking actions of T- and B-lymphocytes, such as antigen-receptor dependent lymphocyte proliferation, cytokine production, and immunoglobulin production (13; 223).
Among other actions, these toxins collectively depress cerebral cortical electrical activity (119; 211), depress central respiratory center activity (119; 177; 211), cause bleeding and destruction of the brain and vital organs in the chest (02), and induce cardiovascular collapse (119). Toxin-induced vascular dysfunction is mediated in part by disruption of the endothelial cell barrier (87).
Progression of anthrax after infection is largely mediated by two native virulence plasmids, pXO1 and pXO2 (73). The genes for lethal toxin and edema toxin are located on pXO1, and genes for the anti-phagocytic poly-Υ-D-glutamic acid capsule are located on pXO2. Attachment to (adhesion) and invasion of brain microvascular endothelial cells by blood-borne B. anthracis is also mediated by the pXO1 plasmid-encoded envelope protein, BslA. BslA is necessary and sufficient to promote adherence to the brain endothelium and also contributes to blood-brain barrier breakdown by disrupting the tight junction protein ZO-1.
Additional virulence factors are secreted as well, including two zinc metalloproteases: neutral protease 599 and immune inhibitor A. Immune inhibitor A contributes to blood-brain barrier disruption associated with anthrax meningitis, by additional proteolytic attack on ZO-1 (152). The increase in blood-brain barrier permeability begins with internalization of immune inhibitor A into human brain microvascular endothelial cells, followed by degradation of ZO-1. The expression of Immune inhibitor A contributes to hemorrhagic brain damage associated with fatal meningoencephalitis.
|
• Anthrax is endemic in sheep, cattle, goats, and horses, particularly in Africa, Asia, and the Middle East. | |
|
• Spores can remain dormant in some types of soil for many decades, serving as a potential source of infection for grazing livestock. | |
|
• Humans may become infected by contact with, ingestion, or inhalation of spores from infected animals or their products (eg, wool or hides). | |
|
• Cutaneous anthrax most commonly results when spores from contaminated animal products enter breaks in the skin, whereas "woolsorter disease" is an occupational inhalational anthrax infection acquired by wool mill workers. | |
|
• Naturally occurring cases outside of agricultural or industrial settings have resulted from exposure to products from anthrax-infected animals, eg, anthrax-contaminated bristle shaving brushes, animal hair or yarn, bone meal, and drums made from contaminated hides. | |
|
• Since 2000, cases of cutaneous and systemic anthrax have occurred in Scotland due to injection of heroin contaminated with anthrax. | |
|
• Anthrax is rarely found in most developed countries because of vaccines for animals and at-risk people. | |
|
• Epidemiologic clues to bioweapon use include (1) an outbreak or multiple, simultaneous outbreaks with large numbers of patients complaining of respiratory symptoms; (2) high case fatality; (3) sick or dead animals of different species; or (4) multidrug-resistant pathogens. | |
|
• In patients with anthrax meningoencephalitis, males outnumber females by 3 to 1, due in part to differences in occupational exposure (many affected individuals have been wool mill workers or farmers). |
Anthrax in animals. Anthrax is endemic in sheep, cattle, goats, and horses in multiple countries, particularly in Africa, Asia, and the Middle East. Spores can remain dormant in some types of soil for many decades, serving as a potential source of infection for grazing livestock (67; 147; 222; 155; 199; 227; 160; 220). Animals acquire spores through direct contact with contaminated soil (147).
Human anthrax. Humans may become infected by contact with, ingestion, or inhalation of spores from infected animals or their products (eg, wool or hides) (51; 155; 199; 227; 160; 163; 220).
Cutaneous anthrax most commonly results when spores from contaminated animal products enter breaks in the skin, whereas "woolsorter disease" is an occupational inhalational anthrax infection acquired by wool mill workers (05; 30; 169; 16).
Posteroanterior chest x-ray taken 4 months after onset of anthrax in a 46-year-old man. Note the widened mediastinum and bilateral pulmonary effusion. The patient had worked for 2 years as a card tender in a goat hair processin...
Naturally occurring cases outside of agricultural or industrial settings have resulted from exposure to products from anthrax-infected animals (eg, anthrax-contaminated bristle shaving brushes, animal hair or yarn, bone meal, and drums made from contaminated hides) (53; 222). Two Turkish boys developed cutaneous anthrax after contaminated cow's blood was smeared on their foreheads as part of a traditional ritual (79). Laboratory-acquired cases have been reported and may be fatal (49; 50; 190). Human-to-human transmission of clinical anthrax has not been clearly documented (35), although historically in Gambia, antibodies to B. anthracis were found in people living in close contact with patients, and B. anthracis was isolated from communal loofahs (94).
Since 2000, cases of cutaneous and systemic anthrax have occurred in Scotland due to injection of heroin contaminated with anthrax (179; 24; 57; 172).
Anthrax is rarely found in most developed countries because of vaccines for animals and at-risk people. There has been a dramatic reduction in livestock and human cases of anthrax in the United States since 1900, in part due to livestock and at-risk human immunization, proper disposal of infected animals, and restriction of imported wool, hides, and other products (28; 29).
Since 1960, adult anthrax mortality has ranged from 31% for cutaneous to 90% for primary meningitis (91). Median incubation periods ranged from 1 day (interquartile range [IQR]: 0–4) for injection anthrax to 7 days (IQR: 4–9) for inhalation anthrax (91).
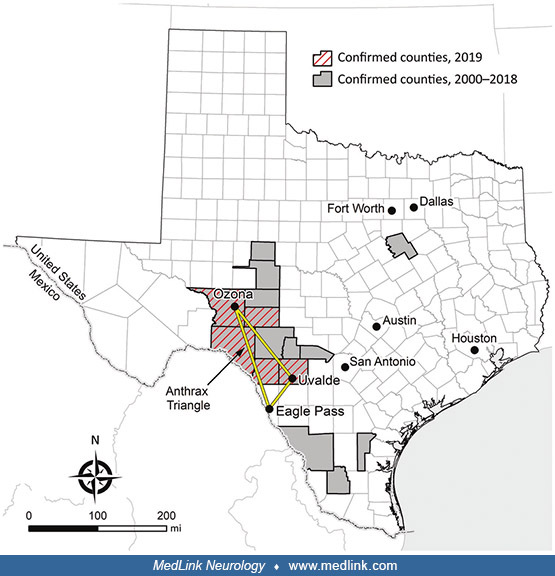
In 2019, an outbreak of animal anthrax in the so-called "Anthrax Triangle" of Texas resulted in cutaneous anthrax in one person (189). The “Anthrax Triangle” represents the geographic region of Texas where laboratory-confirmed animal anthrax cases are most frequent and is bounded by the towns of Eagle Pass, Ozona, and Uvalde (206); counties represented in this region include Crockett, Edwards, Kinney, Maverick, Sutton, Uvalde, Val Verde, and Zavala counties.
The first confirmed 2019 animal case occurred in an exotic antelope, and ultimately, the Texas Veterinary Medical Diagnostic Laboratory reported 25 culture-positive animals, including cattle, horses, white-tailed deer, antelope, and a goat, from Crockett, Kinney, Sutton, Uvalde, and Val Verde counties. Unconfirmed estimates suggest that more than 1,000 animal losses might be attributed to the 2019 outbreak. On July 23, 2019, a non-Hispanic White man in his 70s from the anthrax-affected area was evaluated by his physician for two lesions near his right knee. Before lesion onset 4 days earlier, he had moved two deer carcasses from beneath his porch and scraped his leg on the velvet-covered antlers. Examination showed (1) an indurated, raised, erythematous 5-cm lesion with small ulcerations that oozed serosanguinous fluid and was surrounded by a blanched halo, and (2) a nonindurated erythematous macule.
He had no popliteal or inguinal adenopathy. Two swab specimens were obtained from the larger lesion. The patient was treated with a cephalosporin intramuscularly and given a prescription for ciprofloxacin. The specimen was PCR-positive for B. anthracis, and this result was confirmed by culture.
On July 26, after having taken four doses of ciprofloxacin, he was feeling worse and was evaluated in the emergency room of a hospital. He reported pain, difficulty walking, and nausea, along with intermittent spontaneous drainage of a dark, jelly-like material from the larger wound. He was afebrile and had a nondraining, nonerythematous eschar on the lateral aspect of the right calf as well a painless, nondraining, nonerythematous eschar on the lateral aspect of the right knee.
His leukocyte count was 12,000 (103 cells/µL). His antibiotic was switched to intravenous doxycycline (100 mg every 12 hours). He was ultimately discharged on hospital day 13.
Another human case of cutaneous anthrax occurred in the same area (in a county adjacent to the Texas "Anthrax Triangle") in January 2024, affecting a male rancher aged 50 to 59 years on a sheep farm (206).
A large outbreak of cutaneous and gastrointestinal anthrax occurred from April to May 2023 in the Koraput district of Odisha, India (163). During the outbreak, 47 clinically suspected anthrax cases were identified in five villages. The epidemic curve indicated multiple point-source exposures starting from April 13, 2023. Exposures from handling dead animals were associated with cutaneous anthrax, and eating uncooked meat of dead sheep was associated with gastrointestinal anthrax. "About 10 cases" were confirmed as cases of anthrax by RT-PCR testing. No deaths were recorded in the outbreak. The most common clinical manifestation was a skin eschar (70%), followed by skin swelling, reddening, and pruritis, and, finally, abdominal pain, lymphadenopathy, skin vesicles, vomiting, and diarrhea, all in 30% or less of the cases.
Anthrax meningoencephalitis. Among patients with anthrax meningoencephalitis, males outnumber females by 3 to 1 (130). This represents, in part, differences in occupational exposure because many affected individuals have been wool mill workers or farmers (05; 169; 170; 81; 117).
Anthrax bioweapon or bioterrorism. Because of the complexities of development and dispersal of an anthrax bioweapon, it had been anticipated that small-scale sabotage or attempts at personal murder were more likely than large-scale attempts at inflicting mass casualties with anthrax, and that crude dispersal in a close area was the most likely mode of attack. In the 2001 U.S. outbreak of anthrax acquired through intentional contamination of mail, most cases involved media, government, and postal service employees; several civilian cases remain unexplained (44).
Epidemiologic clues to bioweapon use include (1) an outbreak or multiple, simultaneous outbreaks with large numbers of patients complaining of respiratory symptoms; (2) high case fatality; (3) sick or dead animals of different species; (4) multidrug-resistant pathogens (58). A World Health Organization report estimated that the release of 50 kg of anthrax spores upwind of a city of 500,000 population would result in 125,000 infections and nearly 95,000 deaths (221). A report by the United States Congressional Office of Technology Assessment estimated between 130,000 and 3 million deaths following aerosolized release of 100 kg of anthrax spores upwind of Washington, D.C. (157).
|
• Vaccination of livestock in endemic areas is the most effective method of preventing naturally acquired anthrax in animals and humans. | |
|
• Prevention of anthrax in civilians as a result of bioterrorist activity is limited to prevention of exposure and postexposure prophylaxis (postexposure prophylaxis is considered under management), whereas in military personnel and selected at-risk populations, prevention has also included vaccination. | |
|
• Anthrax Vaccine Adsorbed (AVA), a cell-free, noninfectious anthrax vaccine prepared from a noncapsulating, nonproteolytic anthrax strain, was licensed by the Food and Drug Administration in 1970 for soldiers, at-risk scientists and laboratory workers (ie, those working with anthrax), at-risk veterinarians and livestock handlers, and at-risk wool mill workers. |
Vaccination of livestock in endemic areas is the most effective method of preventing naturally acquired anthrax in animals and humans (36; 199; 220). Management of anthrax in livestock includes quarantine of the herd, removal of the herd from contaminated pastures, vaccination of livestock, treatment of affected livestock, and incineration and, later, burial of infected carcasses, bedding, and other material found around the carcasses (36). Other factors that contributed to the control of naturally occurring human anthrax in the United States include improved industrial hygiene, strict importation guidelines for animals, and regulations that minimized the importation and use of contaminated animal products.
In anthrax endemic areas, livestock are seldom presented for vaccination, and unsafe handling of diseased animals and carcasses can greatly augment the frequency and lethality of human cases. Knowledge remains inadequate to prevent unnecessary livestock and human cases in many endemic areas, including African countries and India (150; 166). In a cross-section study of community knowledge, attitudes, and practices toward anthrax in Kenya, 23% reported that they would slaughter and sell potentially contaminated beef to neighbors, whereas 63% would bury or burn the carcass (150); in addition, although 94% believed vaccination prevents anthrax, only 55% would present livestock for vaccination.
Prevention of anthrax in civilians as a result of bioterrorist activity is limited to prevention of exposure and postexposure prophylaxis (postexposure prophylaxis is considered under management). In military personnel and selected at-risk populations, prevention has also included vaccination (48); however, legal challenges resulted in a temporary halt of military vaccinations as of December 2003. Although previous Centers for Disease Control guidance (35) indicated that anthrax vaccine could be requested through the Centers for Disease Control, such a vaccine was not provided to civilians during the 2001 outbreak in the United States (44; 130). Subsequently, civilians deemed at high risk of exposure who had completed a 60-day course of antibiotics were offered postexposure anthrax vaccination (37; 105).
Anthrax Vaccine Adsorbed (AVA), a cell-free, noninfectious anthrax vaccine prepared from a noncapsulating, nonproteolytic anthrax strain, was licensed by the FDA in 1970 for soldiers, at-risk scientists and laboratory workers (ie, those working with anthrax), at-risk veterinarians and livestock handlers, and at-risk wool mill workers (209). AVA was reapproved for licensure by the Food and Drug Administration in 1985 and remains the only licensed human anthrax vaccine in the United States (222). AVA, now marketed as BioThrax (Emergent BioSolutions, Lansing, Michigan), is licensed for use in non-pregnant adults aged 18 to 65 years who are at high risk of exposure.
AVA is a considerable improvement over previously available vaccines, including the uncharacterized whole-cell vaccines developed initially in 1881 (185). Originally, it was administered as a series of six subcutaneous exposures over 18 months, followed by annual boosters for persons with continuing potential exposure risk (58; 209). In 2008, the Centers for Disease Control and Prevention published the results of a 4-arm randomized controlled trial comparing the original regimen administered by subcutaneous administration with the original regimen administered by intramuscular injection, a reduced dose schedule administered by intramuscular injection, and a placebo that received saline injections at the same intervals; intramuscular injection significantly reduced the occurrence of injection-side reactions, and immunological priming of reduced-dose regimens proved noninferior to the original licensed regimen (140). For pre-event or preexposure prophylaxis, the United States Advisory Committee on Immunization Practices now recommends five 0.5-ml doses of AVA administered intramuscularly at 0 and 4 weeks and 6, 12, and 18 months, followed by annual 0.5-ml booster injections after the 18-month dose (222). A booster dose of AVA for preexposure prophylaxis can be given every 3 years instead of annually to persons not at high risk for exposure to Bacillus anthracis who have previously received the initial AVA 3-dose priming and 2-dose booster series and want to maintain protection (26). People with contraindications to intramuscular injections (eg, coagulopathies) may continue to receive AVA by subcutaneous administration (222). In contrast to the revised vaccine administration schedule and route for pre-event or preexposure prophylaxis, the FDA decided in June 2009 to continue the preexisting postexposure prophylaxis protocol until new data become available; therefore, for postexposure prophylaxis, AVA should only be administered under an Investigative New Drug protocol or Emergency Use Authorization in a 3-dose series (at 0, 2, and 4 weeks) by the subcutaneous route in conjunction with antimicrobial therapy for a minimum of 60 days (222).
The Department of Defense Anthrax Vaccine Immunization Program, announced in 1997 and instituted in 1998, administered 8.4 million doses to approximately 2.1 million military personnel from March 1998 through December 2008 (222). Although previously mandatory for military servicemen and women, a United States District Court ruled on October 27, 2004, that the Department of Defense can no longer inoculate troops without their consent. The vaccine is associated with frequent local reactions but only rare serious side effects sufficient to require hospitalization (approximately once per 200,000 doses) (209). In fact, in a study employing a historical cohort before the inception of the Department of Defense Anthrax Vaccine Immunization Program in 1998, hospitalization following anthrax vaccination was significantly less likely from any cause, diseases of the blood and blood-forming organs, and diseases of the respiratory system among 170,723 active duty U.S. service members who were vaccinated with the anthrax vaccine (216).
The Vaccine Adverse Event Reporting System has monitored adverse events reported following vaccination with AVA. The most common adverse events that occurred after AVA administration (either alone or concurrently with other vaccines) were arthralgia (17%), headache (16%), pruritus (15%), pain (14%), injection-site erythema (13%), fever (11%), erythema (10%), pain at the injection site (10%), rash (10%), and myalgia (10%) (222). There is no convincing evidence of long-term adverse health effects associated with AVA administration (222). Vaccine postmarketing surveillance has identified no association between optic neuritis and receipt of the anthrax vaccine by members of the U.S. military (167).
AVA is neither recommended nor licensed for use during pregnancy, and the Department of Defense continues a policy of avoiding anthrax vaccination in pregnant women (48). AVA is now available under an investigational new drug application in combination with extended antibiotic treatment for civilians exposed to inhalational anthrax who have completed a 60-day course of antibiotics (37; 105).
Other vaccines are used in people and animals in other countries with diverse adaptive immune responses to different anthrax antigens (131). Britain and China have vaccines derived from toxins filtered from a bacterial culture (188; 104). The United Kingdom uses the Anthrax Vaccine Precipitated (AVP) vaccine, an alum-precipitated cell-free filtrate of culture supernatant from a nonencapsulated strain of B. anthracis (from which bacterial cells and some LF and EF are removed by downstream filtering) (131; 148). Russia's vaccine involves inoculation of live spores of a weakened strain of anthrax originally developed for livestock vaccines in the 1930s (188; 104); this vaccine, referred to as a live anthrax vaccine (LAV) or live attenuated anthrax vaccine (LAAV), uses live attenuated STI strain B. anthracis spores that lack an essential virulence factor (ie, the plasmid that encodes the capsule), and consequently the vaccine is “attenuated” (131). At least a dozen countries manufacture anthrax vaccines for livestock, which are similar to the Russian vaccine for people.
New vaccines are in development, including at least one based on a highly purified, genetically engineered protective factor administered with a modern adjuvant (184; 142). The AV7909 anthrax vaccine being developed for postexposure prophylaxis may require fewer vaccinations and a reduced amount of antigen to achieve an accelerated immune response compared with the AVA (BioThrax®) vaccine (100).
Much work needs to be done internationally to develop capabilities to manage victims of biological or chemical terrorism (115). At present, most physicians and hospital emergency departments in the United States are ill-prepared to treat victims of such terrorism (113; 217; 195).
A high index of suspicion is essential for prompt diagnosis of inhalational anthrax, especially in identified or likely at-risk groups (ie, employees of public figures, media employees, mail handlers, and those with known or likely exposure). Inhalational anthrax does not typically cause nasal congestion, rhinorrhea, or sore throat like the common cold or most other influenza-like respiratory viruses (38; 103), although it can (169; 38). Clinical features suggestive of inhalational anthrax, as opposed to viral respiratory tract infection, include the presence of nonheadache neurologic symptoms, dyspnea, nausea or vomiting, and any abnormality on lung auscultation (103). Early cases of inhalational anthrax may resemble viral respiratory illness or, in some cases, gastroenteritis. In the only 20th-century outbreak of inhalational anthrax in the United States, which occurred in a textile mill in 1957, clinical diagnoses among the four (of five) listed cases included (1) influenza, (2) a severe cold or (3) possible bronchitis, and (4) possible cholecystitis. In the Sverdlovsk outbreak in 1979, cases of inhalational anthrax were most commonly felt to be cases of pneumonia; in some cases, though, severe chest pain resulting from hemorrhagic thoracic lymphadenitis and mediastinitis resulted in a clinical diagnosis of myocardial infarction. Other possible considerations in the differential diagnosis of inhalational anthrax include viral pneumonia, mycoplasma pneumonia, Legionnaire’s disease, histoplasmosis, coccidioidomycosis, psittacosis, tularemia, and Q fever. Both tularemia and anthrax may produce similar mediastinal lymphadenopathy (198).
Cutaneous anthrax has been confused with a brown recluse spider bite; it may also be confused with staphylococcal or streptococcal furuncles, ecthyma gangrenosum, cutaneous tuberculosis, ulceroglandular tularemia, plague, and other skin infections (67; 180; 198).
Gastrointestinal anthrax must be differentiated from other causes of acute abdomen, including peritonitis, acute gastroenteritis, mechanical obstruction, peptic or duodenal ulcer, typhoid fever, and tularemia (67).
The differential diagnosis of anthrax meningoencephalitis includes subarachnoid and intracerebral hemorrhage, nonanthrax bacterial or aseptic meningitis, herpes simplex virus encephalitis, other forms of infectious meningoencephalitis in immunocompromised individuals, and cerebral malaria (05; 169; 70; 72; 201; 29; 67; 32; 117; 130). Listeria monocytogenes is the only common gram-positive rod causing meningitis; it does not produce hemorrhagic meningitis and is rarely seen on Gram stain.
|
• Treatment should not be delayed pending a diagnostic workup for possible anthrax. | |
|
• No rapid screening test is available to diagnose inhalational anthrax in the early stages. | |
|
• In a conventional (noncrisis) setting, patients with systemic anthrax should undergo a lumbar puncture to determine whether they have anthrax meningitis, provided that no contraindications exist. | |
|
• In a contingency setting (ie, when resource availability or other circumstances shift evaluation and management to nonpreferred methodologies, medications, and locations), patients with systemic anthrax who have two or more clinical features of meningitis (ie, severe headaches, altered mental status including confusion, meningeal signs, or other neurologic symptoms/signs) or a contraindication to a lumbar puncture should be presumed to have anthrax meningitis, whereas patients with fewer of the screening symptoms and signs should have lumbar punctures. | |
|
• Hemorrhagic meningitis should raise a strong suspicion of anthrax infection. | |
|
• Computed tomography or magnetic resonance imaging of the head in patients with anthrax meningoencephalitis may demonstrate focal intracerebral hemorrhage, subarachnoid hemorrhage, intraventricular hemorrhage, diffuse cerebral edema, and prominent leptomeningeal enhancement. |
|
Clinical criteria (A OR B) | |||
|
(A) Death of an unknown cause with organ involvement consistent with anthrax; | |||
|
(a) At least one of the following specific signs and symptoms: | |||
|
(1) Evidence of pleural effusion | |||
|
(b) At least two of the following nonspecific signs and symptoms: | |||
|
(1) Abdominal pain | |||
|
Laboratory criteria | |||
|
(A) Confirmatory laboratory evidence (a, b, c, d, OR e) | |||
|
(a) Culture and identification of B. anthracis or Bacillus spp. expressing anthrax toxins from clinical specimens by the Laboratory Response Network (LRN) | |||
|
(B) Presumptive laboratory evidence (a, b, OR c) | |||
|
(a) Demonstration of B. anthracis antigens in tissues by immunohistochemical staining | |||
|
Epidemiologic linkage (A OR B) | |||
|
(A) Exposure to an environment, food, animal, materials, or objects that is/are suspected or confirmed to be contaminated with B. anthracis or anthrax toxin-producing Bacillus spp | |||
|
Case classification | |||
|
(A) Probable (a, b, OR c) | |||
|
(a) Meets the clinical criteria AND meets presumptive laboratory evidence | |||
|
(B) Confirmed (a OR b) | |||
|
(a) Meets the clinical criteria AND meets confirmatory laboratory evidence | |||
|
| |||
Treatment should not be delayed pending a diagnostic workup for possible anthrax. Detailed interim guidelines for investigation of, and response to, Bacillus anthracis exposures have been published (38; 40).
No rapid screening test is available to diagnose inhalational anthrax in the early stages (38). Rapid tests to detect conditions with similar clinical presentations (eg, group A beta-hemolytic streptococcal infections, influenza infections, and respiratory syncytial virus infections in infants) have been encouraged (42; 38). White blood cell counts may be elevated with anthrax (42; 105) but are generally normal (or possibly low) with influenza and other respiratory viral infections. Gram stain and culture of blood, CSF, or pleural fluid can establish the diagnosis of anthrax, but these are late clinical findings. Sputum Gram stain is not often positive. Enzyme-linked immunosorbent assay, immunohistology, serum serology (with sequential blood samples at least a week apart), and polymerase chain reaction demonstration of Bacillus anthracis DNA can be used to confirm the diagnosis but are of little help clinically, as these typically must be performed at a reference laboratory, the results are generally not available in time to affect the clinical outcome (126). Nasal swabs can help establish exposure, but anthrax spores are rapidly cleared, which means that an exposed person may have a negative swab; nasal swabs are not indicated to diagnose anthrax, to determine risk of exposure and need for antimicrobial prophylaxis, or to determine when antimicrobial prophylaxis may be stopped (38; 40). With inhalational anthrax, a chest x-ray may demonstrate hilar or mediastinal adenopathy, a widened mediastinum, pleural effusions, or infiltrates (58; 42; 38).
Posteroanterior chest x-ray on the fourth day of illness from a fatal case of inhalation anthrax. Note the widened mediastinum and pleural effusion. (Source: CDC. Public Health Image Library, image number 1795. Public domain.)<...
Anthrax should be diagnosed if a chest x-ray demonstrates a widened mediastinum in the setting of fever and other constitutional symptoms, in the absence of another obvious cause (eg, severe blunt chest trauma or postsurgical infection).
Diagnostic recommendations for anthrax meningitis vary by setting (25). In a conventional (noncrisis) setting, patients with systemic anthrax should undergo a lumbar puncture to determine whether they have anthrax meningitis, provided that no contraindications exist. In a contingency setting (ie, when resource availability or other circumstances shift evaluation and management to nonpreferred methodologies, medications, and locations), patients with systemic anthrax who have two or more clinical features of meningitis (ie, severe headaches, altered mental status including confusion, meningeal signs, or other neurologic symptoms/signs) or a contraindication to a lumbar puncture should be presumed to have anthrax meningitis, whereas patients with fewer of the screening symptoms and signs should have lumbar punctures. Identification of Gram-positive rods, pleocytosis, visible turbidity, or visible hemorrhage in cerebrospinal fluid is sufficient for a diagnosis of probable anthrax meningitis. In a crisis setting (ie, when resource limitations require medical care prioritization, allocating care to those with the highest likelihood of survival or benefit) a clinical case definition (ie, without lumbar puncture) may be used to identify patients with probable anthrax meningitis: under these circumstances, patients with systemic anthrax and severe headache, altered mental status, meningeal signs, or other neurologic signs should be considered to have anthrax meningitis.
(Source: Bower WA, Hendricks K, Pillai S, Guarnizo J, Meaney-Delman D, Centers for Disease Control and Prevention (CDC). Clinical framework and medical countermeasure use during an anthrax mass-casualty incident. MMWR Recomm Re...
An evidence-based assessment tool has been developed for screening patients for meningitis during an anthrax mass casualty incident (112). Severe headache, altered mental status, meningeal signs, and other neurologic signs at presentation independently predicted meningitis in a derivation cohort. The presence of one of these signs and symptoms on admission had a sensitivity of 89% for finding anthrax meningitis in the adult validation cohort and 83% in the pediatric validation cohort. Anthrax meningitis was unlikely in the absence of any of these signs or symptoms, whereas anthrax meningitis was very likely in the presence of two or more of these signs or symptoms.
Quick and reliable assessment of patients for anthrax meningitis using clinical symptoms and signs is possible (20). If low-resource diagnostic testing is feasible for some patients, pairing algorithms improves specificity. Pairing algorithms with differing symptoms and signs minimizes the proportion of patients requiring additional diagnostics.
Hemorrhagic meningitis should raise a strong suspicion of anthrax infection (104; 110; 130; 203; 145; 82). In the index case in the 2001 bioterrorist outbreak in the United States, the initial diagnosis was made from CSF (32). Findings are fairly consistent across reported cases (70; 201; 173; 170; 200; 69; 81; 32; 130). CSF in anthrax may appear cloudy, with yellowish or pinkish coloration, or may be grossly bloody; evolution across this spectrum has been reported in serial lumbar punctures in an individual patient. The supernatant is frequently xanthochromic. Opening pressure may be normal or increased (300 to 500 mm of CSF). Hypoglycorrhachia is common, with CSF glucose frequently ranging from 20 to 40 mg/dl. CSF protein is generally elevated, with initial CSF protein values from 120 to 1150 mg/dl (median 400 mg/dl) and with maximum reported values of 1333 mg/dl. CSF is frequently hemorrhagic, but in the early stages, there may be no red cells; the range of red cell concentration on initial lumbar puncture is from 0 cells per cubic mm to 1375 cells per cubic mm (median 400), with maximum reported values as high as 1,800,000 cells per cubic mm. There is a polymorphonuclear CSF pleocytosis with a range of 560 to 4750 white cells per cubic mm on initial lumbar puncture (median 2500), with maximum reported values as high as 58,000 white cells per cubic mm; the percentage of polymorphonuclear cells ranges from 67% to 95% (median 81%). CSF cultures are usually positive, but CSF may be sterile after several days of antibiotics. Gram stain generally shows numerous polymorphonuclear leukocytes as well as many large gram-positive rods, either singly or in short or long chains; indeed, virtually all case reports of anthrax meningitis that give Gram stain results report these findings. Serial lumbar punctures may document an evolution from cloudy to grossly bloody CSF, with increasing protein concentration, numbers of red cells and polymorphonuclear leukocytes, and proportion of polymorphonuclear leukocytes among white cells.
Other laboratory findings in patients with anthrax meningoencephalitis include elevated white blood cell counts (up to 80,000) with a left shift, positive blood cultures in approximately 75% of patients, positive skin biopsy cultures in patients with skin lesions, and frequently abnormal chest x-rays in patients with respiratory symptoms.
Electroencephalogram results have rarely been reported, even though seizures are fairly common. In part, this reflects the moribund state of most of these patients. In one patient with reported myoclonus and fasciculations, EEG showed disorganized, low-amplitude, slow waves (1 to 7 Hz) (170).
Computed tomography or magnetic resonance imaging of the head in patients with anthrax meningoencephalitis may demonstrate focal intracerebral hemorrhage, subarachnoid hemorrhage, intraventricular hemorrhage, diffuse cerebral edema, and prominent leptomeningeal enhancement (69; 117; 82). Parenchymal cerebral enhancement has not been reported (117). Findings may progress rapidly on serial brain imaging studies (69).
|
• Naturally occurring Bacillus anthracis is generally susceptible to many antibiotics, including ciprofloxacin and other fluoroquinolones, doxycycline and other tetracyclines, penicillins, macrolides, rifampin, vancomycin, aminoglycosides, imipenem, clindamycin, chloramphenicol, cefazolin, and other first-generation cephalosporins. | |
|
• For postexposure prophylaxis of inhalational anthrax following intentional exposure to Bacillus anthracis, the Centers for Disease Control recommends initial treatment with ciprofloxacin or doxycycline until antibiotic susceptibility is determined, with total therapy for at least 60 days, in combination with a 3-dose series of anthrax vaccine adsorbed administered at time zero, at 2 weeks, and at 4 weeks. | |
|
• Very few cases of survival following anthrax meningoencephalitis have been reported. | |
|
• Steroids have been recommended for consideration as adjunctive agents without any age restriction in anthrax meningitis. |
Bioterrorism or bioweapons using anthrax. Bacillus anthracis is a Tier 1 biological select agent due to its potential to cause great harm (178; 111). Tier 1 agents present the greatest risk of deliberate misuse with significant potential for mass casualties or devastating effects to the economy, critical infrastructure, or public confidence and pose a severe threat to public health and safety.
Most physicians are not adequately prepared to diagnose and manage potential bioterrorism agents, including anthrax (59), and not much has changed since the U.S. bioterrorism outbreak in 2001 (195). Factors that could potentially mitigate the consequences of an anthrax attack include the ability to promptly recognize and manage the illness and its public health consequences, limitation of secondary contamination through appropriate decontamination, and development and implementation of genotyping methods that can facilitate investigations and thereby influence the governmental response to an attack (63). In addition, though, the circumstances of a significant outbreak of anthrax (eg, as in an accidental or intentional release of anthrax spores) could easily overwhelm treatment resources, forcing triage protocols and the use of alternate treatment regimens.
Mathematical modeling indicates that vaccination used as postexposure prophylaxis in conjunction with antibiotics is the most effective mitigation strategy to reduce deaths after an aerosolized attack and is more effective when the response starts early (ie, within 2 days after release) and has high adherence, whereas it makes only a small difference when started late (ie, after 10 days) (60).
For bioterrorism-associated anthrax, the U.S. Food and Drug Administration has approved five antibiotics (doxycycline, penicillin-G, levofloxacin, moxifloxacin, and ciprofloxacin), two monoclonal antibodies (obiltoxaximab and raxibacumab), one polyclonal antitoxin (Anthrax Immune Globulin Intravenous), and two vaccines (Anthrax Vaccine Adsorbed and Anthrax Vaccine Adsorbed with an adjuvant) (17). A national stockpile system ensures that communities have ready access to these agents.
Anthrax meningoencephalitis. Survival is very low for patients with anthrax meningitis, regardless of treatment (130; 168). Very few cases of survival following anthrax meningoencephalitis have been reported (62; 186; 215; 201; 204; 116; 200; 130; 19). An 8-year-old boy was initially treated with sulfonamide, chloramphenicol, and penicillin until the organism was identified, at which time the patient was switched to intravenous penicillin and corticosteroids (201). A 25-year-old man treated with penicillin and corticosteroids survived, but with residual right arm weakness (116). In addition, a 6-year-old boy and a 12-year-old boy treated with intravenous penicillin plus intramuscular streptomycin (but without corticosteroids) survived (204; 200); however, his 2-year-old sister, who was treated with the same regimen, died (200).
In a review of treatment outcomes for patients hospitalized with naturally acquired and bioterrorism-related anthrax from 1880 to 2018, neither monotherapy nor combination therapy was particularly effective for anthrax meningitis, although the sample size was small (168); mannitol may have improved survival for meningitis patients, but steroids did not.
Naturally occurring Bacillus anthracis is generally susceptible to many antibiotics (130). However, although all B. anthracis strains from a naturally occurring source or an intentional release were thought to be susceptible to the recommended antimicrobial drugs (except for penicillins), antimicrobial-resistant B. anthracis strains can be created with relative ease through serial passaging on selective media (27). Because bioterrorists could mass-produce a multidrug-resistant B. anthracis strain capable of evading previously recommended first-line antimicrobial medical countermeasures, updated CDC guidelines provide postexposure prophylaxis and treatment recommendations that include numerous antimicrobial drugs from multiple classes (27). The antimicrobial drugs recommended as first-line agents are expected to address most scenarios, whereas the alternative antimicrobial drugs provide contingencies for contraindications, intolerances, unavailability, and natural or genetically engineered resistance (27). The latest CDC guidance should be consulted for specific details on antibiotic prescribing (27).
Postexposure prophylaxis. For empiric postexposure prophylaxis of inhalational anthrax following intentional exposure to Bacillus anthracis, the CDC recommends initial treatment with either ciprofloxacin, levofloxacin, doxycycline, or minocycline until antibiotic susceptibility is determined, with total therapy for at least 60 days, in combination with a three-dose series of anthrax vaccine adsorbed administered at time zero, 2 weeks, and 4 weeks (105; 196; 27). These drugs are considered equivalent first-line agents for postexposure prophylaxis and have similar susceptibility profiles for naturally occurring isolates, similar safety profiles, and a low rate of anaphylactic reactions (196; 27). Long-term use of these antibiotics appears to be relatively safe to treat a large-scale exposure to anthrax in a bioterrorism attack (143). Amoxicillin or penicillin VK can be used for penicillin-susceptible strains (27).
In a review of treatment outcomes for patients hospitalized with naturally acquired and bioterrorism-related anthrax from 1880 to 2018, antimicrobial postexposure prophylaxis reduced the risk of anthrax following exposure to B. anthracis (168).
Empiric treatment regimens for systemic anthrax, including anthrax meningitis. Empiric treatment regimens for systemic anthrax (defined as hyperthermia or hypothermia, tachycardia, tachypnea, hypotension, or neutrophilia or neutropenia) with or without meningitis are complex and include eight possible regimens with variations for adults, pregnant or lactating women, and children (27). CDC guidance should be consulted for definitive treatment protocols (27). Anthrax meningoencephalitis should be treated with a polydrug antibiotic regimen, using agents with good CNS penetration in meningitis and providing good antibacterial coverage for Bacillus anthracis for at least 2 to 3 weeks, or until the patient is clinically stable, whichever is longer. The preferred antibiotic regimen for anthrax meningitis ("Regimen 1") includes bactericidal drugs from different antimicrobial classes plus a protein synthesis inhibitor or an RNA synthesis inhibitor (eg, ciprofloxacin plus meropenem plus minocycline) (27). Fluoroquinolones have adequate CNS penetration and are not known to be susceptible to natural resistance. The carbapenem drugs are highly resistant to beta-lactamases and provide good CNS penetration. Because of the presence of constitutive or inducible beta-lactamases in Bacillus anthracis isolates from the 2001 U.S. outbreak, penicillin alone (eg, penicillin G or amoxicillin) is not recommended as initial therapy. Definitive therapy should be directed by antibiotic susceptibility test results, when available, and the clinical course. One or two oral antibiotics may be sufficient if the patient improves.
All recommended antibiotic agents for postexposure prophylaxis or treatment of anthrax may be associated with allergic reactions, and all are likely to cause side effects when administered for 60 days, although the penicillins are likely to be the best tolerated. Fluoroquinolones can cause various side effects (eg, nausea, vomiting, abdominal pain, diarrhea, anorexia, dizziness, headache, insomnia, mood changes, tremor, restlessness, confusion, and, rarely, psychosis, hallucinations, seizures, and Achilles tendon rupture); in children, they may cause permanent cartilage damage and arthropathy. Tetracyclines frequently cause gastrointestinal disturbances, can cause photosensitivity reactions, and may cause staining and deformity of the teeth in young children (up to age 8 years) or when administered in utero after the fourth month of pregnancy. In a small survey of 490 persons taking postexposure prophylaxis antibiotics in Florida, approximately 20% reported adverse events attributed to the antibiotics after only 1 to 2 weeks, including symptoms of itching, breathing problems, and swelling of the face, neck, or throat.
In a retrospective chart review of patients with cutaneous anthrax in the Kyrgyz Republic from 2005 through 2012, 37 of 230 patients with cutaneous anthrax were categorized as likely developing anthrax meningitis (128). All 37 likely meningitis patients survived receiving only mono- or dual-therapy antimicrobials. Underlying medical conditions (eg, obesity, hypertension, and chronic obstructive pulmonary disease) and tobacco and alcohol use were identified as potential risk factors for developing severe anthrax and anthrax meningitis in these patients with cutaneous anthrax. Therefore, treatment of anthrax meningitis may not require three antimicrobials, but further studies are needed to verify this.
Antitoxins. Antibiotics alone will not address toxin-mediated injury caused by Bacillus anthracis, and indeed, their utility is largely limited to the earliest stages of illness (202). Antitoxin therapy treats the toxemia component of anthrax infection that antibiotics cannot address and that is, in fact, responsible for most of the morbidity and mortality associated with anthrax infection.
Although anthrax antitoxin was utilized early in the 20th century in combination with penicillin to treat anthrax meningitis with reported success in a single case (186), with the advent of antibiotics, its use declined, and it ultimately became unavailable until concerns of anthrax being used as a bioweapon prompted development of novel anthrax antitoxins for treatment (102). Limited human and animal evidence suggests that adjunctive antitoxin treatment may improve survival from systemic anthrax infection (93). Furthermore, antitoxins may be an alternative to antimicrobials for treatment or postexposure prophylaxis during an intentional anthrax incident involving a multidrug-resistant B. anthracis strain (93).
An antitoxin should be administered in a single dose as an adjunct to antimicrobial drug therapy; options include either raxibacumab, obiltoxaximab (ETI-204), or AIGIV (anthrax immunoglobulin intravenous; Anthrasil) (27). All of these have been approved by the FDA as adjunctive therapies for inhalational anthrax (61). Antitoxin therapy treats the toxemia component of anthrax infection that antibiotics cannot address and that is, in fact, responsible for most of the morbidity and mortality associated with anthrax infection. Despite a lack of human data on these new antitoxins, limited experimental data from animal studies suggest that adjunctive antitoxin therapy may improve survival (102; 61).
Raxibacumab and obiltoxaximab are monoclonal antibodies or antitoxins that are administered intravenously for the treatment of adult and pediatric patients with systemic anthrax in combination with appropriate antibiotic drugs and for prophylaxis of inhalational anthrax when alternative therapies are not available or not appropriate (207; 202; 27; 109). Both are antiprotective antigen monoclonal antibodies that limit the deleterious effects of anthrax toxin until endogenous antibodies are produced and immunity acquired.
AIGIV was developed for the treatment of toxemia associated with inhalational anthrax. It is a plasma product collected from individuals vaccinated with the anthrax vaccine. It contains IgG antibodies against the Bacillus anthracis protective antigen. Based on simulations, the intravenous administration of 420 U AIGIV is expected to result in a greater than 80% probability of survival in more than 90% of the human population (15). Exposure levels are likely to be similar in healthy and obese adults, but exposure in children is expected to be up to seven-fold higher than in healthy adults, allowing for doses in pediatric populations that range from one to seven vials. The optimal human dose was estimated based on the pharmacokinetic and pharmacodynamic properties of AIGIV in animals and model-based translation to predict human exposure and efficacy.
Anthrax vaccine. Anthrax vaccine is now available under an investigational new drug application in combination with extended antibiotic treatment for civilians exposed to inhalational anthrax who have completed a 60-day course of antibiotics (105; 196). A short course of postexposure antibiotic prophylaxis combined with vaccination (ie, initiated simultaneously) has been shown to improve protection against inhalational anthrax in animal models and may shorten the duration of antibiotic prophylaxis needed to protect against inhalational anthrax (212). Three doses of the anthrax vaccine can be administered at 0, 2, and 4 weeks, and antibiotics should be continued throughout this period (58; 105).
Treatment of symptomatic cerebral edema. Corticosteroids have been recommended as an adjunct to the treatment of meningitis in children and are thought to reduce neurophil migration across the blood-CSF barrier, decrease neutrophil lysosome release in the subarachnoid space, and facilitate reconstitution of the blood-CSF barrier. Steroids had been recommended for consideration as adjunctive agents without any age restriction in anthrax meningitis (92). However, there is no clear clinical evidence of a benefit from corticosteroids in anthrax meningitis (27). In a review of treatment outcomes for patients hospitalized with naturally acquired and bioterrorism-related anthrax from 1880 to 2018, steroids did not appear to improve survival (168). Steroids should generally be avoided if the antibiotic regimen includes vancomycin because CSF vancomycin levels may be decreased by corticosteroids (65).
Although survival was not different in adults with anthrax meningitis who received steroids (two of six) compared with those who did not, patients who received mannitol had higher odds of survival than those who did not (OR = 24; 95% CI = 1.7–347.9) (168). Two of the rare survivors of anthrax meningitis received mannitol or mannitol with hyperosmolar therapy (19; 137).
Based on bacterial meningitis studies in animal models, 3% hypertonic saline might be beneficial for treating symptomatic cerebral edema (135; 27).
Other management. In addition to antibiotic and antitoxin management, patients with anthrax meningoencephalitis may require aggressive intensive care unit care, including respiratory support and dialysis. Seizures, increased intracranial pressure, subarachnoid and intracerebral hemorrhage, electrolyte disturbances, hypotension, shock, disseminated intravascular coagulation, and other complications may all require targeted management.
Precautions. Because respiratory secretions do not spread the disease, standard precautions are adequate.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Infectious Disorders
May. 15, 2026
General Neurology
May. 13, 2026
Infectious Disorders
May. 12, 2026
Infectious Disorders
May. 12, 2026
Infectious Disorders
May. 05, 2026
Infectious Disorders
May. 01, 2026
Infectious Disorders
Apr. 30, 2026
Headache & Pain
Apr. 10, 2026