Epilepsy & Seizures
Epilepsy: treatment in low and middle income countries
Apr. 08, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
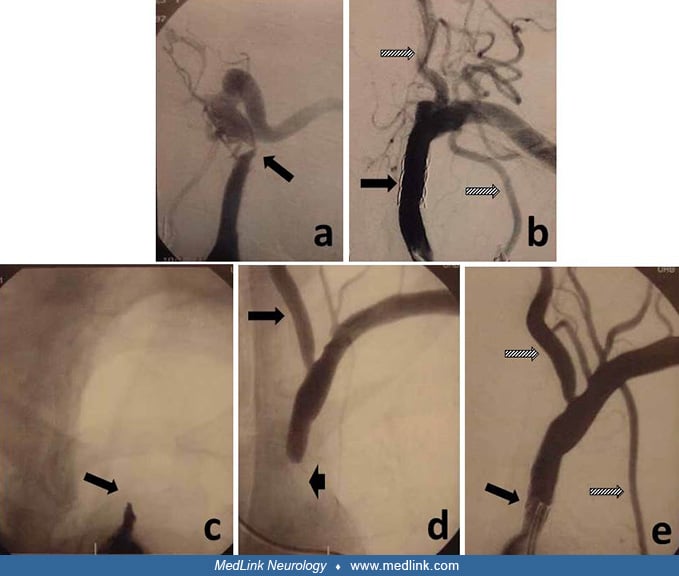
(A) Severe stenosis (arrow) of the proximal left subclavian artery. Note the lack of visualization of either the vertebral artery or the internal mammary artery. (B) Control 6-month angiogram following stenting of the lesion in (A). The stent can be easily seen (black arrow) but, more importantly, both the vertebral artery and internal mammary artery are now visualized (stripped arrows). (C) Occlusion (arrow) of the left subclavian artery causing steal physiology. (D) Injection of the right vertebral artery of the same patient in (C), demonstrating retrograde left vertebral artery flow (long arrow) and the distal end of the occluded segment (short arrow). (E) Post-procedural angiogram of the lesion in (C) and (D), demonstrating correction of the occlusion by the stent (black arrow), with antegrade flow and optimal visualization of the vertebral artery and the internal mammary artery (stripped arrows). (Contributed by Dr. Camilo Gomez.)