





Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author explains the clinical presentation and pathophysiology of Foix-Chavany-Marie syndrome (bilateral anterior opercular syndrome). Manifestations include volitional paralysis of masticatory, facial, pharyngeal, and lingual muscles innervated by cranial nerves V, VII, IX, X, and XII, with preserved autonomic and emotional innervation of these muscles. Thus, although volitional movements are absent, emotional smiling, laughter, crying, and automatic yawning are preserved. Pseudobulbar paralysis in Foix-Chavany-Marie syndrome must be distinguished from bulbar paralysis and from disorders of the cranial nerves and neuromuscular junction, such as botulism and myasthenia gravis.
|
• Foix-Chavany-Marie syndrome is a rare cortical form of supranuclear (pseudobulbar) palsy caused by bilateral anterior opercular lesions; in this syndrome, there is an “automatic-voluntary dissociation” of motor function of lower cranial nerves. | |
|
• Manifestations include volitional paralysis of masticatory, facial, pharyngeal, and lingual muscles innervated by cranial nerves V, VII, IX, X, and XII, with preserved autonomic and emotional innervation of these muscles (eg, emotional smiling, laughter, and crying as well as automatic yawning). | |
|
• Pseudobulbar paralysis in Foix-Chavany-Marie syndrome is clinically distinguished from bulbar paralysis and from disorders of the cranial nerves and neuromuscular junction (eg, botulism and myasthenia gravis) by normal eye movements, preserved or hyperactive brainstem reflexes (eg, jaw jerk), the dissociation of automatic and volitional movements of the bulbar muscles with preservation of automatic movements, and the absence of atrophy and fasciculations of the lower motor neuron-innervated muscles. | |
|
• The cortical form of pseudobulbar palsy is clinically distinguished from the noncortical type of pseudobulbar palsy by its acute onset, prominent voluntary-automatic dissociation of the bulbar muscles, absence of emotional lability, and absence of bowel and bladder incontinence. | |
|
• There are five predominant clinical groups of Foix-Chavany-Marie syndrome (87): (1) an acute form, typically with bilateral infarction of the anterior opercula; (2) a subacute form, typically caused by central nervous system infections; (3) a developmental form, attributed to neuronal migration disorders; (4) a reversible form in children with epilepsy; and (5) a rare chronic progressive form associated with neurodegenerative disorders. |
The bilateral anterior opercular syndrome was first described by Magnus in 1837 and later more extensively investigated by French neurologists Charles Foix (1882-1927) and Jean Alfred Émile Chavany (1892-1959) with French pediatrician Julien Marie (1899-1987) in 1926 (36; 35; 52; 16). These reports are the basis for the eponym Foix-Chavany-Marie syndrome to describe the clinical manifestations of bilateral anterior opercular dysfunction. Although also used, the terms opercular syndrome and anterior opercular syndrome are not sufficiently specific to distinguish Foix-Chavany-Marie syndrome from the very different manifestations of unilateral or posterior opercular lesions.
In the 1950s, a developmental form of the bilateral anterior opercular syndrome was described by Worster-Drought, a consultant neurologist at an institution for children with communication disorders, and this congenital form is sometimes now referred to as the Worster-Drought syndrome (88; 89; 90; 20), although some use this eponym more loosely to refer to bulbar cerebral palsy (21). Kuzniecky and colleagues termed the congenital form “congenital bilateral perisylvian syndrome” (49). Others have suggested the term “congenital suprabulbar palsy,” but this again is insufficiently specific to distinguish this from subcortical causes of pseudobulbar palsy.
The bilateral anterior opercular syndrome has been more frequently recognized and reported in the international literature since the advent of CT and MRI imaging.
|
• Foix-Chavany-Marie syndrome is a rare cortical form of supranuclear (pseudobulbar) palsy, resulting from bilateral anterior opercular lesions that produce an “automatic-voluntary dissociation” of motor function of lower cranial nerves. | |
|
• Manifestations include volitional paralysis of masticatory, facial, pharyngeal, and lingual muscles innervated by cranial nerves V, VII, IX, X, and XII, with preserved autonomic and emotional innervation of these muscles (eg, emotional smiling, laughter, and crying as well as automatic yawning). | |
|
• There is a pseudo-peripheral bilateral facial paresis, with involvement of both the lower and upper face such that the face appears totally expressionless and immobile with volitional efforts, yet such patients furrow their brows with upgaze, blink, close their eyes completely while sleeping, and move the jaw and facial muscles with spontaneous emotional responses (eg, laughing or crying). | |
|
• The palate, pharynx, and tongue are paralyzed, typically with severe dysphagia necessitating tube feeding. | |
|
• Although the tongue is immobile or nearly so, atrophy and fasciculations are absent. | |
|
• Although some patients can make inarticulate sounds when they attempt to speak, most are anarthric or mute but can communicate by writing or with gestures. |
Foix-Chavany-Marie syndrome is a rare cerebral form of supranuclear (pseudobulbar) palsy caused by bilateral anterior opercular lesions; there is an “automatic-voluntary dissociation” of motor function of lower cranial nerves.
Manifestations include volitional paralysis of masticatory, facial, pharyngeal, and lingual muscles innervated by cranial nerves V, VII, IX, X, and XII, with preserved autonomic and emotional innervation of these muscles (eg, emotional smiling, laughter, and crying as well as automatic yawning) (56; 87). The mouth hangs slackly open, and patients are generally unable to volitionally close it or open it further. There is a pseudo-peripheral bilateral facial paresis, with involvement of both the lower and upper face such that the face appears totally expressionless and immobile with volitional efforts, yet such patients furrow their brows with upgaze, blink, close their eyes completely while sleeping, and move the jaw and facial muscles with spontaneous emotional responses (eg, laughing or crying) (12; 56; 87; 76). The palate, pharynx, and tongue are similarly paralyzed, typically with severe dysphagia necessitating tube feeding. Although the tongue is immobile or nearly so, atrophy and fasciculations are absent. Although some patients can make inarticulate sounds when they attempt to speak, most are anarthric or mute; they are not aphasic and can communicate by writing or gestures. Other manifestations include sialorrhea, preserved corneal reflexes, a hyperactive jaw jerk, and a depressed or absent gag reflex.
Bilateral opercular infarcts with extension of ischemia into the subcortical tracts can produce a variant of the anterior opercular syndrome with supranuclear gaze palsy (43).
Although some authors have used the term apraxia (as in lingual-buccal-facial apraxia or buccofacial apraxia) concerning the restriction of voluntary movements with preserved automatic movements in this syndrome (34; 11), this is actually a paralytic disorder rather than an apraxia, ie, loss or impairment of the ability to execute complex coordinated movements without muscular or sensory impairment.
Similarly, some authors have referred to the anarthria or mutism as "aphemia," an apraxia of speech characterized by complete articulatory failure in the presence of preserved writing, comprehension, and oropharyngeal function (27). However, oropharyngeal function is not preserved in Foix-Chavany-Marie syndrome.
Although language dysfunction and limb sensorimotor manifestations are typically absent in cases of Foix-Chavany-Marie syndrome, they may be variably present in occasional cases due to concomitant pathology extending beyond the anterior operculum on one side or the other.
Clinical findings in the congenital form vary in severity and associated features. The congenital form may be associated with persistent mutism with normal language comprehension, mental retardation, epilepsy, and orofacial diparesis or pseudobulbar palsy of variable severity (40; 67; 77; 49; 50; 87; 48; 39; 63; 85; 22; 21). Other associated findings can include variable developmental delay, learning disability, behavioral difficulties, epileptic drop attacks, dysarthria, limitation of tongue movements, drooling, motor manifestations from mild limb pyramidal signs to spastic quadriparesis, ataxia, ventriculomegaly, poor palatal function, hypotonia, arthrogryposis, micrognathia, pectus excavatum, and hearing loss (40; 86; 39; 47; 21). Epilepsy is common, though not a constant feature, and when present it varies in type and severity (39). Many patients have intractable seizures (47). Seizure types reported include atypical absence, atonic or clonic, generalized tonic-clonic, and less commonly infantile spasms, and complex febrile, partial, and complex partial seizures (49; 50; 55; 58). Seizures are poorly controlled or intractable in half to two thirds of affected patients (49; 50).
Prognosis for recovery of functional speech and volitional swallowing with vascular Foix-Chavany-Marie syndrome is generally poor, although some childhood cases associated with epilepsy (eg, benign epilepsy of childhood with centrotemporal spikes, also known as benign Rolandic epilepsy) are reversible, and the extremely rare unilateral cases may do somewhat better (42). Occasional patients with Foix-Chavany-Marie syndrome due to bilateral traumatic opercular injury may experience a remarkable recovery over a period of months (29; 03). Most patients require alternative communication strategies (eg, writing) and feeding tubes. Aspiration pneumonia is a frequent complication.
Case 1. Foix-Chavany-Marie syndrome with acute left anterior opercular stroke and prior asymptomatic right opercular infarct (65). A 52-year-old right-handed woman presented to the emergency department acutely unable to open her jaw on wakening. She also reported dyspnea, dysphagia, tongue numbness, and anarthria for several hours. Her past medical history was significant for hypertension, hyperlipidemia, a prior stroke 5 years ago without any residual deficits, aortic stenosis with atrial fibrillation, congestive heart failure (ejection fraction 20% to 25%), type 2 diabetes mellitus, chronic obstructive pulmonary disease, gastroesophageal reflux disease, and hypothyroidism. She reported compliance with her medications, which included apixaban, carvedilol, lisinopril, furosemide, atorvastatin, insulin, glipizide, and levothyroxine.
On admission, she was afebrile, normotensive, tachycardic, and tachypneic on her home oxygen therapy requirement of 2 liters of oxygen via nasal cannula. She was aphonic, but there was no receptive aphasia: she communicated by writing on a notepad and answered all questions appropriately. She had a marked reduction in volitional movement of her jaw and marked flaccid bifacial and tongue weakness. She was unable to smile, puff out her cheeks, protrude her tongue, or move her tongue from side to side. Muscle power was normal in her limbs, and she had normal stretch reflexes. Abnormal lab findings were notable for blood glucose 226 mg/dL (reference range 74-106 mg/dl), troponin level of 426 ng/L (reference range < 53.7 ng/L), and B-type natriuretic peptide level of 4522 pg/L (reference range 5-125 pg/L).
An electrocardiogram showed sinus tachycardia with first-degree atrioventricular block and right axis deviation but no acute ischemic changes. Carotid ultrasound showed no significant stenosis of the common and internal carotid arteries. Chest x-ray showed pulmonary edema with widespread interstitial infiltrates and cardiomegaly. Computed tomography of the chest showed interstitial edema, mild bibasilar atelectasis, and cardiomegaly. Echocardiography showed left ventricle dilation with severe diffuse hypokinesis, reduced systolic function, and ejection fraction of 15% to 20%. There was also moderate-to-severe aortic stenosis and moderate pulmonary hypertension, with an estimated pulmonary artery systolic pressure of 55 mmHg. A modified barium swallow study showed silent aspiration of thin liquids.
MRI of the brain showed an acute left opercular infarct and a chronic right opercular infarct on diffusion-weighted imaging, which was confirmed with apparent diffusion coefficient imaging. Chronic bilateral cerebellar infarcts, chronic small vessel ischemic disease, and mild cerebral atrophy were also present.
She presented to the emergency department beyond the time window for intravenous thrombolytic therapy. Her antihypertensive medications were also held to optimize cerebral blood flow. Her home medication regimen was modified to adequately treat her decompensated heart failure, with concurrent, type-2, non-ST-elevation myocardial infarction and acute hypoxic respiratory failure. Over the ensuing 5 days, she had significant improvement in speech, swallowing, and movement of her tongue. She was discharged to rehabilitation.
Case 2. Foix-Chavany-Marie syndrome with infarcts of the left anterior periventricular white matter and the right anterior operculum as well as subjacent white matter (54). A 58-year-old right-handed man was mute on awakening. His history included a stroke 2 years previously with right hemiparesis and transient dysarthria (without aphasia) from which he had almost completely recovered. On examination, he was anarthric except that with great effort he could elicit a harsh grunt. He was unable to volitionally open his mouth, smile, or frown. He could minimally move the tongue to the edge of the lips, and his tongue deviated leftward with attempted protrusion. Despite his volitional paresis/plegia of various bulbar muscles, he blinked spontaneously and to threat, closed his eyes fully while sleeping, opened his mouth, and retracted his tongue with yawning. Vision, eye movements, trapezius and sternomastoid strength, confrontational strength of his extremities, and sensation were normal. His jaw jerk was increased, but his gag reflex was absent. He was mildly clumsy with his right hand and had a right pronator drift. Although he was (mis)diagnosed with a brainstem stroke clinically, a noncontrast CT showed hypodense areas in the left anterior paraventricular white matter and the right anterior operculum and subjacent white matter. Carotid ultrasound and carotid angiogram showed bilateral carotid artery occlusion.
Case 3. Foix-Chavany-Marie syndrome with bilateral opercular infarcts (54). A 42-year-old man with a 180-pack-per-year smoking history developed an acute left-sided weakness involving the face and arm. The initial noncontrast CT was normal, but carotid angiograms showed bilateral internal carotid artery occlusions. Four days after admission he developed seizures. An emergent carotid endarterectomy was done (despite the carotid occlusion), and postoperatively he became mute and dysphagic. A noncontrast CT a day after his endarterectomy (5 days after admission) showed hypodense areas in the opercular bilaterally. Examination 3 days after endarterectomy showed an alert but mute man who was unable to move his facial muscles voluntarily, although reflex movements were present. He used writing as his major mode of communication and had intact grammar and syntax. He had mild weakness of his left-hand grip and circumducted his left leg when he walked. Muscle stretch reflexes were symmetrically hyperactive with bilateral Babinski signs. Three weeks later, a contrast CT showed enhancing lesions in the bilateral opercular areas, caudate heads, and the right basal ganglia. Seven years later he continued to have severe dysarthria and hypophonia, used writing as his means of communication, and ate a mechanical soft diet.
|
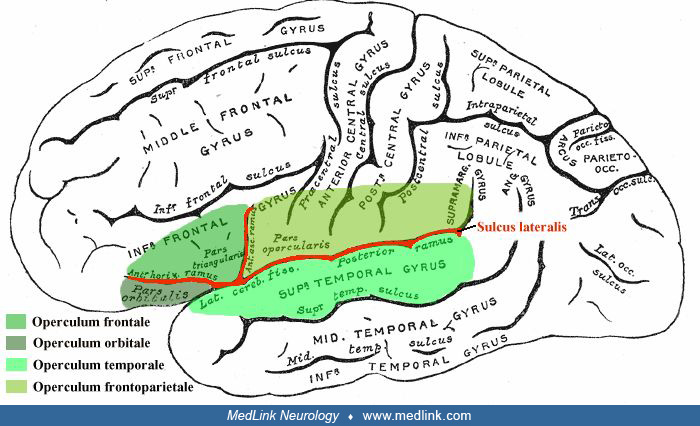
• The "operculum of the insula of Reil" or operculum (meaning “little lid”) is formed by cortical convolutions of the frontal, parietal, and temporal lobes bordering the lateral sulcus (Sylvian fissure). | |
|
• The anterior frontal operculum is involved bilaterally in Foix-Chavany-Marie syndrome. | |
|
• In adults, this is most often due to sequential infarctions, although rarely it can be caused by acute, simultaneous, isolated bilateral infarcts, demyelinating disease, trauma, or other causes. | |
|
• In the congenital form, Foix-Chavany-Marie syndrome is typically due to neuronal migration disorders with presylvian dysgenesis (polymicrogyria). |
The "operculum of the insula of Reil," or operculum (meaning “little lid”) is formed by cortical convolutions of the frontal, parietal, and temporal lobes bordering the lateral sulcus (Sylvian fissure).
Foix-Chavany-Marie syndrome almost always results from bilateral lesions of the anterior opercular cortex and subjacent white matter but rarely has been attributed to unilateral anterior opercular lesions in the dominant hemisphere or to unilateral lesions with associated seizures spreading to the homologous contralateral region (54; 87; 42; 44). In adults, Foix-Chavany-Marie syndrome is most often due to sequential (or "asynchronous") infarctions involving the anterior operculum (60; 73; 65), although rarely it can be caused by acute, simultaneous, isolated bilateral infarcts (13; 19), small vessel disease (possibly superimposed on prior large-vessel disease) (53; 74; 05), demyelinating disease, trauma, or other causes (15; 14; 83; 57; 80; 46; 94).
An 81-year-old right-handed man presented with acute sound volume loss, inability to swallow and speak, inability to move his tongue, and difficulty chewing food. His past medical history was remarkable for a prior stroke, diab...
A 66-year-old man with diabetes, hypertension, and tobacco use had right-sided hemiplegia 1 year before he developed Foix-Chavany-Marie syndrome acutely 2 days before admission. CT of the brain showed an acute left perisylvian ...
A 48-year-old man with diabetes and hypertension had right-sided hemiplegia 1 year before he developed Foix-Chavany-Marie syndrome acutely 2 days before admission. CT of the brain showed bilateral infarcts in the posterior limb...
Foix-Chavany-Marie syndrome has been reported following acute unilateral anterior opercular infarction with preexisting extensive bilateral leukoaraiosis (70; 84). In the congenital form, Foix-Chavany-Marie syndrome is typically due to neuronal migration disorders with presylvian dysgenesis (polymicrogyria). Such cases may result from in utero infection or ischemia (06; 25). Depending on the extent of the lesions, bordering areas may be affected with associated distal weakness of the arms (precentral gyri), paresthesias of the hand and mouth (cheiro-oral distribution, postcentral gyri), and Broca aphasia (12; 54).
Martino and colleagues reported a case of Foix-Chavany-Marie syndrome that developed intraoperatively in a 25-year-old man during surgery to resect the patient's right fronto-temporo-insular tumor (57). While resecting the anterior part of the pars opercularis via a transopercular approach, the patient suddenly developed anarthria and bilateral facial weakness that persisted for 8 days. Postoperative diffusion tensor imaging tractography demonstrated damage to the connections of the pars opercularis of the right inferior frontal gyrus with the frontal aslant tract (FAT) and arcuate fasciculus. The frontal aslant tract is a bilateral intralobar tract that connects the superior and inferior frontal gyri through an oblique course from the medial-superior to the inferior-lateral region (17). The frontal aslant tract may mediate supplementary motor area control of orofacial movements (57).
Anecdotal cases have presented some unique circumstances for presentation with Foix-Chavany-Marie syndrome (10; 64; 72; 71). Bradley and colleagues reported a 77-year-old man who developed Foix-Chavany-Marie syndrome after sequential bilateral corona radiata infarcts, first on the left and later on the right (10). Ohtomo and colleagues reported a 76-year-old man with an acute unilateral left opercular infarction who presented with Foix-Chavany-Marie syndrome (64); the authors attributed the presentation to the combination of the new lesion in the left operculum superimposed on an old infarct in the contralateral pons. Sá and colleagues reported a patient with a unilateral left opercular lesion associated with a chronic asymptomatic contralateral cerebellar lesion (72). Rózsa and colleagues reported a 70-year-old woman with an acute unilateral right anterior opercular infarction who presented with a transient pseudobulbar syndrome with difficulty swallowing and speaking (71). Yoshii and colleagues reported a right-handed 53-year-old woman who presented with Foix-Chavany-Marie syndrome after a new infarct in the left corona radiata following a prior history of an old cerebral hemorrhage affecting the right anterior opercula (from an arteriovenous malformation) (93). You and colleagues reported a 66-year-old man who presented with Foix-Chavany-Marie syndrome after an acute infarct in the left corona radiata with a preexisting right-sided arachnoid cyst (94).
Bilateral anterior opercular lesions involving the precentral motor cortex produce a diplegia of the masticatory, facial, pharyngeal, and lingual muscles with voluntary-automatic dissociation (15). There are bilateral direct projections from the primary motor cortex in the precentral gyrus to the nuclei of the 5th, 7th, 9th, 10th, and 12th cranial nerves in the pons and medulla; these convey signals for volitional control of the corresponding muscles of the jaw, face, pharynx, and tongue, whereas emotional control of the muscles is thought to use alternate polysynaptic pathways.
Potential etiopathogenic factors in congenital cases include genetic factors, perinatal hypoxic-ischemic injury, and mid-gestation ischemia associated with death of a co-twin in the context of monozygotic twinning (86; 85; 92; 82; 25). Congenital bilateral perisylvian syndrome is a neuronal migration disorder characterized by pseudobulbar palsy and bilateral perisylvian dysplasia and often associated with mental retardation and epilepsy (48; 07; 21). The most common basis is congenital bilateral perisylvian polymicrogyria, which is frequently evident on MRI (37; 21; 28). Congenital bilateral perisylvian polymicrogyria is the most frequent type of polymicrogyria in children (28). Genetic factors are likely, and developmental Foix-Chavany-Marie syndrome with polymicrogyria and incomplete opercular formation has been reported in identical twins (37). Pathological examination may show bilateral failure of opercular closure, opercular polymicrogyria, periventricular gray-matter heterotopias, and absence of the septum pellucidum (08; 77). Some other cases show bilateral perisylvian ulegyria, which can be considered a form of cerebral palsy (47). Ulegyria is a static injury of the cerebral cortex sustained in the perinatal period; the gyri are pathologically distorted with gliosis involving the gyral bases and subjacent white matter, sparing the crown. Ulegyria is often seen in term neonates who have other evidence of hypoxia. Intrauterine infection may also produce polymicrogyria (06).
Cases of Foix-Chavany-Marie syndrome have been misdiagnosed as neuromuscular junction disorders (myasthenia gravis, botulism), Guillain-Barré syndrome, brainstem stroke, and psychogenic disorders (54; 26). Corticobasal syndrome may present with clinical features mimicking Foix-Chavany-Marie syndrome (62).
Pseudobulbar paralysis in Foix-Chavany-Marie syndrome is clinically distinguished from bulbar paralysis and from disorders of the cranial nerves and neuromuscular junction (eg, botulism and myasthenia gravis) by normal eye movements, preserved or hyperactive brainstem reflexes (eg, jaw jerk), the dissociation of automatic and volitional movements of the bulbar muscles with preservation of automatic movements, and the absence of atrophy and fasciculations of the lower motor neuron-innervated muscles (54; 87). The gag reflex is variably absent in Foix-Chavany-Marie syndrome and is not by itself a clear discriminator.
The cortical form of pseudobulbar palsy is clinically distinguished from the noncortical type of pseudobulbar palsy by its acute onset, prominent voluntary-automatic dissociation of the bulbar muscles, the absence of emotional lability, and the absence of bowel and bladder incontinence (54). The absence of a gag reflex and absence of emotional lability (so-called pseudobulbar affect) with Foix-Chavany-Marie syndrome are not by themselves clear discriminators because the gag reflex is variably absent in Foix-Chavany-Marie syndrome and emotional lability is variably absent in some cases of noncortical pseudobulbar mutism (41).
There are five predominant clinical groups of Foix-Chavany-Marie syndrome (87): (1) an acute form, typically with bilateral infarction of the anterior opercula; (2) a subacute form, typically caused by central nervous system infections; (3) a developmental form, attributed to neuronal migration disorders; (4) a reversible form in children with epilepsy; and (5) a rare chronic, progressive form associated with neurodegenerative disorders. The acute form is the most common and is usually seen with sequential atherothrombotic or embolic infarctions of the anterior opercula (ie, presenting acutely with the second opercular infarction, contralateral to the first). Other reported causes of acute presentations of acquired Foix-Chavany-Marie syndrome include acute disseminated encephalomyelitis, multiple sclerosis, progressive multifocal leukoencephalopathy, cardiogenic emboli from atrial myxomas, thromboangiitis obliterans, moyamoya disease, vasculitis, and head injury (09; 51; 79; 29; 30; 33). The subacute form due to infections has been reported most commonly with herpes simplex encephalitis, but other infectious causes reported include other causes of meningoencephalitis, a Nocardia brain abscess superimposed on cortical hypoplasia, toxoplasmosis, HIV infection, Epstein-Barr virus encephalitis, and tuberculous meningitis (61; 67; 87; 38; 04; 75; 68; 01; 59; 45). The developmental form due to neuronal migration disorders may result from underlying intrauterine infection or ischemia. Polymicrogyria can be caused by infection in the third trimester of gestation, and cerebral microgyria can be caused by fetal ischemia (06; 25). The reversible epileptic form is usually seen in children with benign rolandic epilepsy or hemispheric malformations who develop a reversible Foix-Chavany-Marie syndrome in status-epilepticus, but adult cases have also been reported (23; 87; 81). A slowly progressive form of Foix-Chavany-Marie syndrome has been reported as a rare precursor of a primary progressive aphasia (83).
These clinical groups of Foix-Chavany-Marie syndrome are not always mutually exclusive. In some cases, patients may sustain damage to the anterior operculum on one side from one cause and then later suffer damage on the opposite side from another cause (24; 87; 66; 78). Cases have been reported with a brain abscess or stroke superimposed on contralateral congenital or perinatal lesions (24; 87), with a brain abscess superimposed on a contralateral old stroke (78), or with a hemispheric stroke on one side and a tumor on the other (66). Rarely a unilateral opercular infarction is thought to cause Foix-Chavany-Marie syndrome (91), but the pathophysiology of these cases is controversial (64).
|
• The diagnosis is established clinically with confirmation by CT or MRI. |
The diagnosis is established clinically with confirmation by CT or MRI. In most patients with the congenital form, MRI shows evidence of bilateral perisylvian cortical malformation consistent with polymicrogyria (49; 50; 18; 39; 63; 85; 55). SPECT and PET show decreased cerebral blood flow and metabolism in the anterior opercular and insular areas bilaterally (11; 02).
EEG typically shows abnormalities in the background rhythms over the centro-parietal regions, often with generalized spike-wave abnormalities and less frequently with multifocal discharges (50; 55).
Fiberoptic endoscopic evaluation of swallowing (FEES) or videofluoroscopy is required before initiation of swallowing techniques.
When resection of a benign mass lesion of the insula or operculum (eg, a low-grade glioma) is contemplated, preoperative metabolic imaging and electrophysiological investigations combined with intraoperative functional mapping should be used to identify and preserve the corticosubcortical facial motor structures even when contralateral damage is not evident on structural brain imaging (31; 32).
|
• Management depends on the etiology and clinical type, with primary therapeutic efforts focused on treatment and prevention of further progression of the underlying etiology. | |
|
• Because rapid return to oral feeding is unlikely, early gastric tube placement can prevent adverse effects of nasogastric tube feeding. |
Management depends on the etiology and clinical type, with primary therapeutic efforts focused on treatment and prevention of further progression of the underlying etiology (eg, cerebrovascular disease, central nervous system infection, epilepsy). In addition, speech therapy (emphasizing alternative communication strategies), facilitation of adequate nutrition and hydration (eg, feeding tube), and prevention of aspiration pneumonia (eg, feeding tube) are key aspects of symptomatic management.
Because rapid return to oral feeding is unlikely, early gastric tube placement can prevent adverse effects of nasogastric tube feeding. In some cases (depending on results of fiberoptic endoscopic evaluation of swallowing or videofluoroscopy), nutrition and hydration can be augmented with liquid injection techniques and postural changes to allow liquids to be propelled further into the pharynx, avoiding the deficient musculature.
In some children with polymicrogyria and intractable seizures, anterior callosotomy, temporal lobectomy, or other resective surgery can be helpful (40; 49; 50; 48; 47).
A case has been reported in which the preserved involuntary pharyngeal and esophageal swallowing phases were adequate once initiated or triggered, thus, avoiding a percutaneous endoscopic gastrostomy, but this is unlikely to be workable in most cases (69).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neurobehavioral & Cognitive Disorders
May. 20, 2026
Infectious Disorders
May. 01, 2026
Neurogenetic Disorders
Apr. 30, 2026
General Child Neurology
Apr. 29, 2026
Neuroimmunology
Apr. 26, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Movement Disorders
Apr. 12, 2026