Neuromuscular Disorders
Drug-induced myasthenic syndromes
May. 21, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
This article reviews the physiological basis of acupuncture and evaluates its applications in various neurologic disorders. Acupuncture is most frequently used for the relief of pain. Claims in some other conditions, such as stroke, cannot be confirmed by controlled clinical trials. Although used in practice, acupuncture still needs to be further evaluated by well-controlled clinical trials.
|
• Of the alternative methods, acupuncture is the one most integrated into conventional medical practice. | |
|
• Acupuncture is widely used for the treatment of neurologic disorders, particularly for the management of painful conditions. | |
|
• The action of acupuncture in modulating pain pathways has been demonstrated by brain imaging studies. | |
|
• Neurologic complications have been reported from the improper insertion of acupuncture needles. | |
|
• Further controlled and well-designed studies are needed to evaluate the efficacy of acupuncture for neurologic disorders. |
Acupuncture, as the derivation of the word implies (acus meaning needle; puncta meaning puncture), is the insertion of a needle into the skin of the human body. Acupuncture has been practiced in China for several thousand years. The earliest available written record is from 1800 BCE in the Yellow Emperor's Classic of Medicine (51). The ancient Chinese attributed disease to an imbalance between Yin (negative) and Yang (positive) forces. This belief exists for some even today. Acupuncture was supposed to restore the balance between these two forces. The procedure spread to Southeast Asia and Japan and then to Europe in the 1800s. Acupuncture was used for the relief of pain and muscular disability in England more than 125 years ago (46). Osler was familiar with the procedure and considered it to be the most efficient treatment in acute cases of lumbago (36). Osler had occasional failures, as indicated by the following episode:
|
One of these consultations, however, was such an important one that preparations had to be made for it and Ogden (a student of Osler) was requisitioned as an assistant, for the patient was none other than old Peter Redpath, the wealthy Montreal sugar refiner who, being on Montreal General Hospital Board had hopes that the newly appointed physician might be able to cure him of an intractable lumbago. He arrived exhausted after mounting the stairs, in due course they proceeded to treat him by acupuncture. At each jab of a needle, the old gentleman is said to have ripped out a string of oaths, and in the end got up and hobbled out no better off in his pain, to Osler's great distress, for he had expected to give him immediate relief which, as he said, meant millions for McGill University (05). |
Wilder Penfield, a pioneer Canadian neurosurgeon, visited China in 1962 and was invited by Chinese physicians to try acupuncture on a patient. He gave no definite opinions on this procedure (40). Ten years later, acupuncture as practiced in China was evaluated again, particularly for neurologic applications, and the findings were recorded in a book (16). Acupuncture was effectively used for the relief of pain and even as a substitute for anesthesia during neurosurgical procedures. Penfield agreed with the observations and opinions expressed in the book (Penfield W 1974, personal communication). Although Chinese medicine is now more advanced, with new techniques such cell and gene therapies, acupuncture remains part of the healthcare system and is being further investigated.
During the past few decades, acupuncture has become popular in North America, and practitioners of this art, which include some physicians, are numerous. An estimated 10 million consumers use acupuncture each year in the United States.
A lack of scientific studies to prove or disprove acupuncture's claimed effects led to the initial rejection by many practitioners of Western scientific medicine. Now that the mechanisms can be partly explained in terms of neurophysiology, the integration of acupuncture with conventional medicine is possible. Approximately 30% of acupuncture in the United States is done in a multidisciplinary setting, and 70% by solo practitioners of acupuncture. Clinical acupuncturists are credentialed through the American Board of Medical Acupuncture and the National Certification Commission for Acupuncture and Oriental Medicine.
The relevance of acupuncture to the neurologist is as follows:
|
• Several patients referred to neurologists may have undergone acupuncture treatments. Some of these patients may be reluctant to disclose folk medical treatments to Western physicians; therefore, such information may have to be elicited by questioning. | |
|
• Some patients may request to be referred to an acupuncturist. The neurologist may have to decide if acupuncture could be useful for the patient in a situation where no relief has been obtained by conventional treatments. | |
|
• Neurologists should be familiar with rare neurologic complications of acupuncture. | |
|
• The mechanism of effect of acupuncture is a subject of neurophysiological research. |
|
• Acupuncture is performed by the insertion of fine needles at selected acupuncture points on the skin. | |
|
• Innovations include the use of computers to locate acupuncture points and electroacupuncture. | |
|
• The most common indication for acupuncture is pain, although it is used for other neurologic disorders and for neurorehabilitation, eg, hemiplegia. | |
|
• Acupuncture is generally safe, although there are some contraindications and complications. |
Acupuncture is performed at certain specified points (acupuncture points) varying in size from a few millimeters to, less frequently, a few centimeters. These points are located on the 12 major meridians of the body, each corresponding to a major organ system of the body. More than 1000 such points exist; they have been determined by trial and error, and about 350 of these are used in clinical practice. Auricular acupuncture refers to the use of various acupuncture points on the external ear: master points, musculoskeletal points, internal organ points, and neuroendocrine points. Some auricular points are used for the treatment of neurologic disorders.
Traditional acupuncture uses fine stainless-steel needles that are sterilized, and some are disposable. The needle is inserted at the identified acupuncture point and held for 10 to 20 minutes. Patients usually feel a slight numbness or tingling radiating from the insertion point, which is a sign of effect. If it is absent, the needle may be manipulated gently to elicit it. Modern technical innovations have been applied to acupuncture. Electroacupuncture involves stimulation of acupuncture points by electric current, rather than manipulation. Electroacupuncture, compared to other methods of acupuncture, seems to better deliver stimuli that activate powerful opioid and nonopioid analgesic mechanisms. Low-level laser stimulation has been used in place of acupuncture needles. In Japan, electronic gadgets are used to locate acupuncture points by measuring the alteration of skin resistance to electric current. Computers are used in acupuncture, and computerized manikins are available as a guide for the location of acupuncture points corresponding to certain symptoms.
Acupuncture is aimed at restoring the balance in the body and promoting natural healing. In symptomatic terms, it is most often intended for pain relief.
Acupuncture is mostly used and recognized for the management of pain due to a variety of causes, both neurologic and non-neurologic. It is part of the treatment protocol in several pain clinics. One important indication is the management of pain associated with cancer. In some cases, the cause of pain is not known. Neurologic disorders that have been treated with acupuncture are listed in Table 1. Because of the poor quality of primary studies, available evidence on the use of acupuncture for neurologic disorders does not allow any firm conclusions to be drawn on the use of acupuncture for epilepsy, Alzheimer disease, Parkinson disease, ataxic disorders, multiple sclerosis, amyotrophic lateral sclerosis, and spinal cord injury.
|
• Pain relief | |
|
- backache | |
|
• Sequelae of traumatic brain injury | |
|
- hearing loss | |
|
• Spinal cord lesions: paraplegia and spasticity | |
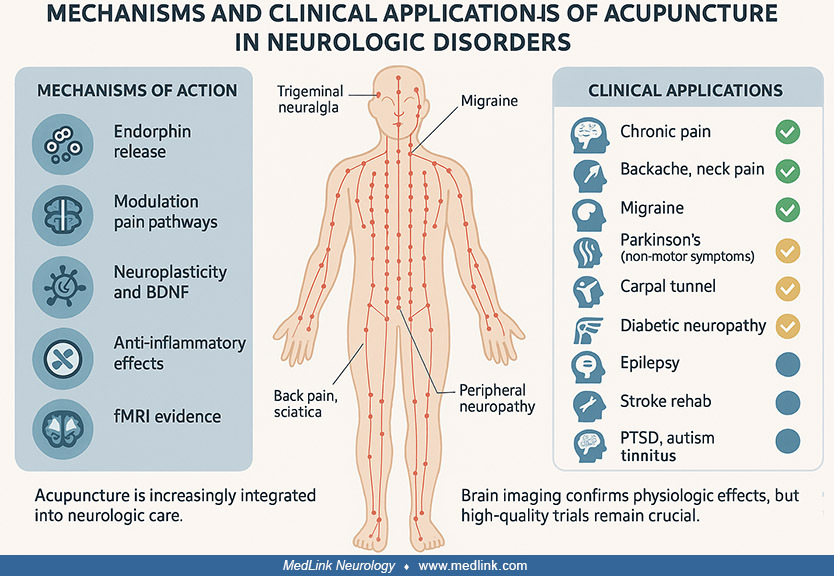
Illustration of acupuncture’s mechanisms and clinical applications in neurologic disorders, highlighting pain modulation pathways, neuroplasticity, and evidence-based uses such as chronic pain, migraine, and stroke rehabilitati...
Some obvious contraindications to acupuncture are known such as infections of the skin and soft tissues. Electroacupuncture should not be used in patients with implanted pacemakers. The insertion of needles should be avoided in the head region of patients with bony defects associated with trauma, surgery, or congenital malformations. Acupuncture should be avoided in infants.
Chronic pain. Among the various indications, acupuncture is mostly used for the relief of chronic pain. A systematic review of randomized controlled trials of acupuncture for chronic pain has shown its effectiveness, even though it is modest (52). A systematic review of randomized controlled trials using double-blind designs found that traditional acupuncture produces significant pain improvement (mean difference approximately 0.97 on the visual analog scale [VAS]; 95% CI 0.66-1.27) compared with controls, with no serious adverse events reported (42). Significant differences between true and sham acupuncture indicate that acupuncture is more than a placebo. A randomized controlled trial in older adults with chronic low back pain (“BackInAction” trial, N≈800) demonstrated that acupuncture plus usual care leads to greater pain reduction and functional improvement than usual care alone, with effects sustained at 12 months (07). A meta-analysis of patient data from high-quality randomized trials of acupuncture for chronic pain shows that approximately 50% of pain relief persists at 12 months following a course of acupuncture (31). A randomized trial found that 20 sessions of acupuncture over 8 weeks resulted in greater improvement in symptoms of moderate to severe chronic prostatitis or chronic pelvic pain syndrome compared with sham therapy, with durable effects 24 weeks after treatment (43).
Backache. Several studies have shown the value of acupuncture in the management of chronic backache. Acute lumbar sprain has been managed successfully with acupuncture. According to the guidelines of the American College of Physicians, there is low-quality evidence for the efficacy of acupuncture as a noninvasive initial treatment for acute, subacute, and chronic low back pain (41). The National Health Service of the United Kingdom authorizes up to 10 sessions of acupuncture over a period of 12 weeks for persons with low back pain that has persisted for more than 6 weeks.
Most of the studies of acupuncture on low back pain are not designed adequately to assess its efficacy, and further basic studies on the mechanism of pain relief and controlled clinical studies are needed (22). A review of randomized trials of acupuncture for backache reveals that there is a need for improvement of instruments and scales for Comparative Effectiveness Research (CER) to evaluate available clinical data (56). More recent meta-analytic evidence also shows that acupuncture combined with exercise (eg, core muscle training) yields greater improvements in pain and function in chronic nonspecific low back pain than either intervention alone (26).
Chronic neck pain. A review of randomized clinical trials suggests that acupuncture relieves chronic neck pain better than sham acupuncture, as measured at the completion of treatment and at short-term follow-up (48). For chronic neck pain, a systematic review up to March 2024 demonstrates durable effects on pain severity, functional disability, and quality of life at least 3 months post-treatment (10).
Cancer pain. The National Comprehensive Cancer Network guidelines for adult cancer pain recommend acupuncture, as one of several integrative interventions, in conjunction with pharmacologic intervention as needed (29). However, a systematic review of randomized clinical trials concluded that there is insufficient evidence for evaluating the efficacy of acupuncture for treating cancer pain in adults (39). Also, a systematic review demonstrated that acupuncture may be an effective and safe treatment associated with pain reduction in the palliative care of patients with cancer (62).
Endometriosis-associated pain. A multicenter randomized single-blind placebo-controlled trial introduced acupuncture as an effective and safe intervention for alleviating dysmenorrhea, reducing the duration of pain, and enhancing overall well-being and quality of life in women experiencing endometriosis-related pain. However, the therapeutic benefits tend to diminish following the cessation of treatment (24).
Epilepsy. In China, acupuncture is often used as a supplement to antiseizure medications in the treatment of epilepsy to improve seizure control, reduce drug-related side effects, and ameliorate cognitive impairment. Several experimental studies have been done to demonstrate a rational basis for this treatment. Systematic reviews and meta-analyses of randomized controlled trials show that acupuncture plus Western medicine significantly reduces seizure frequency (standardized mean difference [SMD] approximately −3.29; 95% CI −3.51 to −3.07) and EEG discharge frequency, compared with antiseizure medications alone. Acupuncture also improves quality of life and decreases adverse events (60).
Acupuncture might exert its antiepileptic effect through GABA because the inhibiting effect of acupuncture is abolished by the injection of 3-mercaptopropionic acid, which blocks the action of GABA. Mechanistic animal-model studies now indicate that acupuncture modulates multiple pathophysiological pathways in epilepsy, including anti-inflammatory effects (eg, reduced COX-2), activation of antioxidant pathways such as Nrf2-ARE, regulation of voltage-gated ion channels, modulation of oxidative stress, inhibition of apoptosis, and even effects on gut microbiota (61).
Seizures induced by penicillin injection into the hippocampus of animal models can be inhibited by electroacupuncture, probably by decreasing enkephalin content in the hippocampus. Electroacupuncture may regulate the biosynthesis of preproenkephalin in the hippocampus during seizures by altering gene transcription. Although older studies emphasized GABAergic and enkephalin pathways, more recent data suggest that the main benefits of acupuncture in clinical contexts may come from modulating neuroinflammation, oxidative stress, and neural excitability (ion channels, synaptic transmission) rather than solely via enkephalins. Additionally, a randomized controlled trial using thread-embedding acupuncture in drug-resistant epilepsy showed improvement in seizure control and changes in autonomic indices (heart rate variability), though larger trials are needed (35).
Headache. The most common type of headache treated with acupuncture is migraine. Several studies have shown the beneficial effect of acupuncture in the prophylaxis of migraine. Acupuncture therapy makes sense if it reduces the patient's discomfort and drug intake. A randomized trial has shown that among patients with migraine without aura, true acupuncture may be associated with a long-term reduction in migraine recurrence compared with sham acupuncture (69). An overview of systematic reviews and meta-analyses for randomized controlled trials of acupuncture for migraine suggested that acupuncture has a significant advantage in relief of pain and safety relative to sham acupuncture, or drug treatment, but the quality of the evidence was low (68). Although the primary treatment for migraine is drug therapy, acupuncture is gaining increasing attention as a viable addition to the management of migraine patients due to its effects on both the duration and frequency of migraine attacks (49). However, long-term follow-up of patients who have been treated with acupuncture for migraine is needed to confirm its usefulness.
Peripheral neuropathies. Acupuncture has been used for pain relief in various types of peripheral neuropathies. In drug-induced peripheral neuropathy, pain may not respond to pharmacotherapy, or patients and physicians may be reluctant to add further analgesic drugs, leading to the consideration of acupuncture. Treatment options for chemotherapy-induced peripheral neuropathy are limited. Acupuncture has been reported to relieve pain in these cases, but larger, placebo-controlled trials are needed to confirm or refute the effectiveness (38). A preliminary observational study has shown the relief of pain in a few patients with diabetic peripheral neuropathy, and a larger controlled study is planned (17). A systematic review and meta-analysis revealed that acupuncture therapy significantly improved the clinical efficacy of pain intensity, pain changes, and clinical neuropathy in patients with diabetic neuropathic pain (25).
A pilot randomized clinical trial that compared the effect of real acupuncture versus sham acupuncture or usual care to treat chemotherapy-induced peripheral neuropathy demonstrated the benefit of real acupuncture (02). This trial demonstrated the feasibility of a sham-controlled trial of acupuncture and justification for conducting a large, controlled trial.
Sciatica. Although acupuncture is used frequently for the treatment of sciatica, it is difficult to evaluate the results. The results would depend on the cause of sciatica. Obviously, if the cause is a disc extrusion with neurologic deficit, surgery may be required. Relief of the pain may be the main therapeutic goal in cases where no correctable pathology exists or the cause of sciatica cannot be defined.
Carpal tunnel syndrome. Acupuncture is a minimally invasive therapeutic option for patients who do not respond to conventional medical and surgical treatment. A randomized trial of electroacupuncture at local as well as distal acupuncture points for 16 weeks (eight sessions) showed reduced symptom severity, and improvement was sustained at a 3-month follow-up (33). Verum (local and distal) acupuncture was superior to sham in producing improvements in neurophysiological outcomes, ie, median sensory nerve conduction latency at wrist and digit 2/3 cortical separation distance in the brain. Neurophysiological studies combined with diffusion tensor imaging of the white matter in these cases showed that improvement in median nerve function at the wrist was accompanied by somatotopically distinct neuroplasticity in the primary somatosensory cortex following therapy, which can predict long-term clinical outcomes for carpal tunnel syndrome.
Spinal cord lesions. Electroacupuncture has been used in China in the rehabilitation of paraplegia. Claims have been made that recovery of motor function occurs. A review of various reports and personal observations of this author revealed no evidence to support these claims.
Electroacupuncture has been used for treating spasticity associated with spinal cord lesions. Maintenance of this antispastic effect requires the continuous use of high-frequency electroacupuncture. The subsequent release of dynorphin from the spinal cord into the cerebrospinal fluid is presumed to decrease the excitability of the motor neurons in the anterior horns through the kappa opiate receptors and, thus, ameliorates the muscle spasticity of spinal origin.
Traumatic brain injury. A randomized, blinded, controlled study in China is evaluating the efficacy and safety of electro-acupuncture for the recovery of consciousness in comatose patients with traumatic brain injury (28). A protocol for the systematic review of randomized controlled trials of acupuncture for hearing loss after traumatic brain injury has been published (54).
Stroke. Acupuncture is commonly used in China in the management of stroke patients, both in the acute stage and during rehabilitation. Electroacupuncture has been reported to be beneficial for improving neurologic deficits in stroke, but the short-term effect of a single treatment differs from the cumulative effects of multiple treatments. An explanation of this has been offered by a study of electroacupuncture in rat models of ischemic injury and the finding of differential modulation of expression of neurotrophic signaling molecules (53).
Several studies have been carried out in other countries to evaluate the effect of acupuncture in stroke patients. Although the safety was demonstrated, there was no evidence of efficacy.
Spasticity is a common symptom in stroke patients, and its management constitutes a major problem in their rehabilitation. Acupuncture has been applied with moderate effect. Meta-analyses of data from rigorous randomized sham-controlled trials did not show a positive effect of acupuncture as a treatment for functional recovery after stroke (19).
Controlled clinical trials and a systematic review of the literature show that acupuncture has therapeutic effects on aphasia after stroke, and it could be useful for the rehabilitation of these patients (43). A meta-analysis of published randomized clinical trials of acupuncture for aphasia in various databases concluded that the clinical efficacy of acupuncture combined with speech rehabilitation training and medication treatment for aphasia is superior to that of speech rehabilitation training and medication treatment alone (44).
An overview of evidence from systematic reviews of clinical trials and meta-analyses of publications has shown that acupuncture is relatively safe, but its effectiveness for stroke is inconclusive, mainly due to poor methodology and an inadequate number of subjects in clinical trials. Randomized controlled trials with long-term follow-up are needed.
A meta-analysis of randomized trials shows that acupuncture is an effective and safe treatment for poststroke depression, and outcomes were better than drug therapy (67). Further high-quality randomized controlled clinical trials are needed to develop standardized acupuncture protocols for this indication.
Tinnitus. Acupuncture is used frequently for treating tinnitus. In a randomized study, acupuncture was found to be more effective for tinnitus than Chinese herbs and Western medicine (45).
Trigeminal neuralgia. The effects of electroacupuncture have been investigated in patients with idiopathic or secondary trigeminal neuralgia. It was found to be an effective treatment for all kinds of secondary trigeminal neuralgia. Results in the idiopathic form vary according to preceding medical treatments and the duration of the disease.
Bell palsy. Acupuncture is used in China for the treatment of Bell palsy, and several publications in the Chinese literature report encouraging results. Cochrane Database of Systematic Reviews has reported that the quality of the included trials was inadequate to allow any conclusion about the efficacy of acupuncture (12). Further high-quality trials are needed to settle this issue. Secondary analysis of a prospective multicenter randomized controlled trial of acupuncture for Bell palsy has shown that personality traits might influence the results, and the needle sensation of fullness could predict better outcomes of facial function as a result of acupuncture treatment (65). These factors should be considered in acupuncture treatment and research.
Cerebral palsy. Acupuncture is used in China for the treatment of cerebral palsy. A randomized study showed that laser acupuncture has a beneficial effect on reducing spasticity in cerebral palsy (06).
Parkinson disease. A systematic review of clinical trials indicates the potential effectiveness of acupuncture for treating Parkinson disease, but the results are limited by methodological flaws, and well-designed, placebo-controlled trials are needed (20). Other randomized controlled trials and meta-analyses also suggest that acupuncture may reduce anxiety, improve quality of life, and ameliorate nonmotor symptoms in Parkinson disease (57).
A review of experimental studies indicates that acupuncture has a neuroprotective effect in Parkinson disease by enhancing the production of brain-derived neurotrophic factor and glial cell line-derived neurotrophic factor, as well as by attenuation of apoptosis and oxidative stress to substantia nigra dopaminergic neurons (18). Mechanistic research in animal models and in vitro has expanded these findings, showing that acupuncture modulates alpha-synuclein aggregation, regulates oxidative stress and mitochondrial dysfunction, enhances autophagy, suppresses neuroinflammation, and influences gene expression (eg, Sgk1) associated with neuronal survival (63). Some studies also point to modulation of GABAergic signaling and neurotransmitter balance in basal ganglia circuits as possible mechanisms (30). However, well-powered placebo-controlled randomized controlled trials with longer follow-ups are still needed, especially to delineate which symptoms (motor vs. nonmotor) respond best and which acupuncture protocols are optimal (points, duration, frequency) and to assess enduring neuroprotective effects in humans (61).
Posttraumatic stress disorder. There is only one published clinical trial of the efficacy of acupuncture in posttraumatic stress disorder, and no scientific basis has been established. However, acupuncture has some effects that are relevant to posttraumatic stress disorder pathology. Clinical and biological data support the possible efficacy of acupuncture for posttraumatic stress disorder, and further definitive research is required to support the use of acupuncture for posttraumatic stress disorder (13).
Autism spectrum disorders. A systematic review of randomized clinical trials combining acupuncture and speech therapy provides mixed evidence of acupuncture's effectiveness, whereas some trials in which acupuncture and speech therapy are combined show some beneficial effects (21).
Evaluation of the effectiveness of acupuncture. Meta-analyses of the controlled clinical trials of acupuncture deal with a wide variety of diseases and symptoms, with no major focus apart from the symptom of pain. A substantial number of different techniques and even philosophies are involved. Inadequacies in study design and methods are frequent. These findings may explain why the effectiveness of acupuncture has still not been definitively demonstrated. Cochrane systematic review of randomized clinical trials found a small analgesic effect of acupuncture, which seems to lack clinical relevance and cannot be clearly distinguished from bias (32). In a systematic review of clinical trials published in the English language and retrieved through PubMed, most studies found no statistically significant difference in outcomes, and most of these reported that sham acupuncture may be as effective as true acupuncture (34). The scientific basis of acupuncture needs further evaluation.
Acupuncture is used for a wide range of manifestations of neurologic disorders, and several claims have been made. Some of these are credible and require further investigation. Other claims are difficult to evaluate because of the poor documentation and lack of accurate diagnosis in cases where the treatment is carried out on a symptomatic basis by nonphysician practitioners. Acupuncture is widely accepted to be useful for the management of pain. It may be effective in migraine and backache, but its role in stroke rehabilitation remains uncertain. Findings of some acupuncture studies are encouraging, but others suggest that its clinical effects mainly depend on a placebo response. Evidence from reviews suggests that acupuncture is more than a placebo for commonly occurring chronic pain conditions (14).
Integration of acupuncture into modern medical practice. Acupuncture is the most commonly integrated of the alternative methods into conventional medical practice. It does not conflict with modern neuromuscular anatomy and pain physiology, even though it is based on the classical Chinese concept of a subtle circulation network of a vivifying force called Qi. This hybrid acupuncture approach expresses the best of both worlds by describing a context in which to organize patient symptoms that usually escape attention in the standard medical evaluation. Painful musculoskeletal problems have been shown to be the most frequently and successfully treated disorders. However, medical acupuncture is adaptable to most clinical practices and can be used either as the primary or as a complementary treatment.
Acupuncture is generally safe when performed by qualified practitioners, though adverse events do occur. A 2023 evidence map of 535 systematic reviews documented 33 types of adverse reactions, including syncope, organ or tissue injury, systemic reactions, infection, and more; most adverse events were mild and transient. Serious adverse events are rare, estimated at approximately 0.04 to 0.08 per 10,000 treatments (59).
Common minor adverse events include pain at or after needle insertion, bleeding or bruising (hematoma), dizziness, feeling faint (vasovagal reactions), temporary discomfort, or irritation around needle sites. Infections are much less common but are still reported; they are usually associated with imperfect sterilization, the use of nonsterile needles, or inadequate skin preparation (59).
Severe harms (such as puncture of the lung [pneumothorax], serious organ injury, or major bleeding) remain rare but are documented; risk factors include deep needle penetration, incorrect acupoint selection, inadequate practitioner training, and performing acupuncture in anatomically risky zones.
Reporting of adverse events in clinical trials is often incomplete. A meta-epidemiological study (2014 to 2024) of 476 randomized controlled trials found that 57% reported safety outcomes, and about 27% claimed no adverse events (09). Overall, the reported incidence of adverse events was higher in the acupuncture group than in the control group, but no serious adverse events were noted in the acupuncture group. Most adverse events are preventable by using sterile, single-use needles; performing proper disinfection; selecting acupoint sites with awareness of underlying anatomy; controlling needle depth; adequately training and certifying practitioners; avoiding high-risk points; and monitoring patient status.
Pregnancy is not listed as a contraindication for acupuncture, but the application of needles over the abdomen should be avoided. Moreover, during pregnancy, acupuncture would be safer than drugs for controlling nausea and vomiting. Acupuncture is also used to facilitate the induction of labor at term.
Physiological basis of acupuncture. In traditional Chinese medicine, the effect of acupuncture treatment is explained by the regulation of Qi (vital energy); this energy is thought to circulate in meridians that are accessible at acupuncture points. In this author’s opinion, this concept is poorly defined and is not compatible with modern anatomical and physiological knowledge. Therefore, there has been ongoing research for the past two decades, both in China and in other countries, to establish the neurophysiological basis of acupuncture. Mechanisms underlying the effect of acupuncture are still not clear. According to one hypothesis, the efficacy of acupuncture in neurologic disorders such as Alzheimer disease is associated with its antiapoptotic effect beause apoptosis plays a role in the pathogenesis of these diseases, and mechanisms of beneficial effect include upregulation of neurotrophic factors (04). This hypothesis remains to be proven. Animal experimental evidence indicates that acupuncture can induce neural plasticity, and this has been suggested as an explanation of its beneficial effects in Alzheimer disease and stroke (58). The exact mechanisms underlying acupuncture's effects on neural plasticity remain to be elucidated, but it is likely associated with modulation of neurotrophic factors and neurotransmitters by acupuncture.
It is difficult to discern any histological difference between acupuncture points and non-acupuncture points; however, acupuncture points are found in close relation to superficial nerves. Local anesthetic infiltration blocks the effect of acupuncture.
Acupuncture treatment is sometimes accompanied by a feeling like paresthesia spreading along the path of the needle channel. This sensation is accompanied by changes in electromyogram, a decrease in electrical resistance of the skin, and changes in local blood flow. One explanation is that the perivascular autonomic plexus is involved in the propagation of this sensation. Another explanation is that the propagated sensation is the result of a process such as the spread of excitation in the central nervous system.
Mechanism of acupuncture analgesia. This has been studied intensively because of the major application of acupuncture for the relief of pain and acupuncture anesthesia. Some of the hypotheses include the following:
|
• Acupuncture analgesia is mediated by the central nervous system. Acupuncture is known to stimulate A delta fibers entering the dorsal horn of the spinal cord. These fibers mediate segmental inhibition of pain impulses carried in the slower unmyelinated C fibers and, through connections in the midbrain, enhance descending inhibition of C fiber pain impulses at other levels of the spinal cord. | |
|
• Effect via the thalamic gateway. This mathematical model is based on the biomedical experimental data of three kinds of stimulation. First, several experiments show that the model captures the electrophysiological properties of a single thalamic cell, that is, the relay and burst modes of operation. Second, a complete neural network representing the thalamic gateway to the cortex is assembled, and the influences of the cortical projections over the thalamus are analyzed. This shows how the cortex opens and closes the thalamic gate and the relation of this control policy with the phenomenon of attention. Finally, a third set of simulations establishes mechanisms of interaction between neighboring thalamic regions, especially a form of somatosensory competition. This provides a possible theoretical explanation for the mechanism of acupuncture analgesia. | |
|
• Several neurotransmitters appear to be essential elements in the mechanisms underlying acupuncture analgesia. These include serotonin, noradrenaline, and acetylcholine. | |
|
• Some studies have shown that acupuncture or electrical stimulation in specific frequencies applied to certain body sites can facilitate the release of specific neuropeptides in the CNS that elicit profound physiological effects and even activate self-healing mechanisms. Electroacupuncture inhibits inflammatory and neuropathic pain more effectively at 2 Hz to 10 Hz than at 100 Hz (66). | |
|
• Several lines of evidence support the endorphin-mediated mechanism of acupuncture analgesia. High- or low-frequency stimulation induced by electrical acupuncture has been shown to release different types of endorphins. Analgesia produced by auricular acupuncture can be blocked by the opiate antagonist naloxone, indicating the role of endorphinergic systems in understanding the underlying mechanisms of auriculotherapy. | |
|
• The mechanism of the effect of electroacupuncture on peripheral neuropathic pain has been studied in a chronic constriction injury of the sciatic nerve, a model of neuropathic pain in rats. Low-frequency electroacupuncture significantly reduced neuropathic pain in this rat model, and its analgesic effect is likely mediated by the upregulation of miu opioid receptors in the L3-L5 dorsal root ganglion (64). | |
|
• The acupuncture effect has been explained by a reaction to the needle called de qi, which is perceived as a needling sensation by the patient and a pulling sensation by the acupuncturist. Needle manipulation transmits a mechanical signal to connective tissue cells via mechanotransduction, and such a mechanism may explain local and remote, as well as long-term effects of acupuncture. | |
|
• Animal experimental studies indicate that adenosine mediates the effects of acupuncture and that interfering with adenosine metabolism may prolong the clinical benefit of acupuncture (11). | |
|
• Functional imaging studies indicate that the so-called default mode network, which consists of cortical midline structures and lateral parietal regions, plays an important role in the central effects of acupuncture analgesia (37). |
Autonomic responses associated with acupuncture. Acute, transient sympathetic reflexes elicited by needling are generally considered to be pain-related and, thus, are not specific to stimulation of acupuncture points. Research on the autonomic nervous system indicates its connection with acupuncture. The inflammatory reflex via the autonomic nervous system might be a part of analgesia elicited by acupuncture (27).
Effect of acupuncture on sensory evoked potentials. The sensory-evoked potential methodology has been adopted in the research of acupuncture since the 1970s. In research focusing on the effects of acupuncture on conventional sensory-evoked potentials, variable results have been observed, and two different opinions are available concerning the presence or absence of acupuncture effects on conventional sensory-evoked potentials. The conventional sensory evoked potential is mediated mainly by fast-conducting sensory nerve fibers. As a result, the conventional sensory evoked potential methodology (especially that for recording short-latency sensory evoked potential) may be inadequate for studying acupuncture mechanisms. In the case of the long-latency cortical sensory evoked potential, too few data are available to judge the effects of acupuncture analgesia. Studies on the effects of acupuncture on pain sensory evoked potentials demonstrated that acupuncture has a suppressive effect on the amplitude of the pain sensory evoked potential. It has also been shown to affect latency in experiments with both animals and humans and is accompanied by an increased pain threshold. Thus, acupuncture seems to have analgesic effects that are probably related to the activation of the antinociceptive system, and the application of the pain sensory evoked potential methodology to the study of mechanisms of acupuncture may be promising.
Effect on pain pathways as demonstrated by brain imaging. Studies performed by the Department of Nuclear Medicine at the University of Pennsylvania showed that definite changes occur in PET scans of patients during relief of pain with acupuncture. This key evidence led to the endorsement of acupuncture for pain (01). PET has also demonstrated that minute changes in glucose utilization and in oxygen consumption in different areas of the brain occur after acupuncture stimulation. PET studies in human volunteers have shown that acupuncture activates some of the areas that are also activated in acute and chronic pain states: the left anterior cingulum, the insulae bilaterally, the left superior frontal gyrus, the right medial gyri, and the inferior frontal gyri (03).
Activation of descending antinociceptive pathways and deactivation of multiple limbic areas subserving pain have been demonstrated by fMRI. Monitoring of acupuncture by fMRI has demonstrated that acupuncture mobilizes a limbic-paralimbic-neocortical network (15). An fMRI study has shown that following verum but not sham acupuncture, there is increased sensorimotor network connectivity with pain-related brain regions (08).
Individualization of acupuncture treatment. Acupuncture needs to be tailored to each patient’s symptoms and responsiveness; it is generally recognized that individualization of acupuncture treatment enhances its effectiveness. Studies clarify what “dose” comprises (session frequency, number of treatments, retention time, stimulation strength) and show that these elements influence outcomes. For example, a meta-analysis of 26 randomized controlled trials (1,947 participants) in patients with acute stroke limb dysfunction found that low to moderate frequency (every other day or daily) and short-course treatment (less than 2 weeks) yielded better functional recovery, whereas needle retention time had less consistent effects (55).
A trial in older adults with chronic low back pain (“BackInAction”, N≈800) compared standard acupuncture to standard acupuncture plus maintenance sessions and to usual medical care. It found that standard acupuncture improved disability through 6 to 12 months, but additional maintenance treatments did not provide a statistically significant extra benefit beyond the standard course (07).
Nevertheless, other analyses suggest that individualized protocols (eg, selecting acupoints based on patient-reported symptoms or sensitivity, modulating stimulation strength) may enhance effects in certain conditions. For example, in cancer therapy-induced peripheral neuropathy, meta-analysis indicates that patients receiving about 16 sessions over 8 weeks (twice weekly) tend to reach minimal clinically important differences, pointing toward an individualized time-dose-response relationship (47).
Key gaps remain. Which patients benefit most from individualization versus standardized protocols? How should responsiveness be reliably measured (eg, biomarkers, symptoms, deqi, imaging)? What are the trade-offs of complexity, cost, and training? Clinical guidelines and methodological standards are now calling for better reporting of the “dose” components and detailed descriptions of individualization methods (70).
Limitations of clinical trials in evaluating the effectiveness of acupuncture. Although several clinical trials of acupuncture have been conducted, it is difficult to prove or disprove the efficacy of acupuncture according to Western evidence-based medicine standards for the following reasons (50):
|
• It is difficult to perform control or “sham” acupuncture using nonpenetrating needles or insertion at non-acupuncture points. | |
|
• Acupuncture is more effective as an individualized treatment, and it is difficult to standardize it for a clinical trial. | |
|
• Despite investigations into the scientific basis of acupuncture, the philosophy of action of acupuncture does not fit in with the Western concepts of the pathomechanism of various diseases. |
Cumulative effects of acupuncture. There are cumulative effects of repeated acupuncture stimulation that overlap in pain-related areas and show bimodal characteristics, ie, the response is positive in the beginning and becomes negative at the end (23). The cumulative effect is consistent with habituation effects. There are also cumulative effects of repeated acupuncture in relieving spasticity during stroke rehabilitation.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Fardin Nabizadeh MD
Mr. Nabizadeh of Iran University of Medical Sciences has no relevant financial relationships to disclose.
See Profile
Matthew Lorincz MD PhD
Dr. Lorincz of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuromuscular Disorders
May. 21, 2026
Movement Disorders
May. 18, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuropharmacology & Neurotherapeutics
May. 11, 2026
Neuropharmacology & Neurotherapeutics
May. 11, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026