


Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Although usually benign, headache can herald serious intracranial disease. Neuroimaging must be considered whenever secondary causes of headache are suspected. This review focuses on indications for neuroimaging in clinical practice and the contribution that neuroimaging has made to our understanding of headache pathophysiology. Advances in imaging, such as functional MRI to study migraine pathophysiology, now demonstrate the role of the hypothalamus, brainstem structure, and network abnormalities. This review also highlights serious secondary causes of headache such as vascular disorders and tumors as a trigger for headache and, occasionally, cluster headache as well as neuroimaging findings in patients headache related to COVID-19.
• Most patients with headache do not need neuroimaging. | |
• Use “red flags” based on history and exam findings to determine the necessity of neuroimaging.” | |
• Although neuroimaging is usually normal in patients with migraine, unusual primary headaches such as trigeminal autonomic cephalalgias or cough headache may be an exception. |
Headache diagnosis is clinical, based on a careful history and physical exam (51). The International Headache Society Classification defines headaches as primary, based on their clinical features or genetic markers, or secondary due to another proven cause (43). For primary headache disorders such as migraine, diagnosis does not rely on neuroimaging.
Neuroimaging and headache etiology. Standard neuroimaging such as CT or MRI aid in the diagnosis of secondary headache disorders. CT scanning is important in the emergency setting and can often be used as a screening tool for serious conditions such subdural or intracranial hemorrhage. MRI shows greater anatomical detail looks at areas that CT scanning does not cover well, such as the sella and posterior fossa. In the research setting, newer neuroimaging techniques, such as functional MRI, PET scanning, diffusion tensor MRI, SPECT, and blood oxygen level dependent (BOLD) fMRI, have improved our understanding of headache physiology and pathogenesis.
Clinical vignette. A 38-year-old, right-handed woman was admitted to the hospital for control of an intractable, throbbing headache. She described her headache as bilateral, with both frontal and occipital components. It was associated with phonophobia and nausea. She said that her head at times felt stuffy, and she described a subjective hearing loss. In addition, she noted an occasional rumbling sound, which she compared to the sound of a helicopter. She was unable to sit or stand because she experienced severe worsening of her pain on changing position. Her pain improved dramatically when she was supine.
Her prior history was remarkable for an upper respiratory tract infection in the week leading up to the onset of this headache and for insulin-dependent diabetes. She was a nonsmoker. Her only medication was insulin.
After 3 weeks of conservative therapy with a variety of nonsteroidal and opioid medications, she was referred to a neurology clinic. At that time, CT scan and lumbar puncture were performed. The CT scan was unremarkable. Her cerebrospinal fluid was remarkable only for evidence of a traumatic tap and a mild elevation in protein (0.65 g/L). There were no organisms, no pleocytosis, and no xanthochromia. Unfortunately, her CSF pressure was not measured.
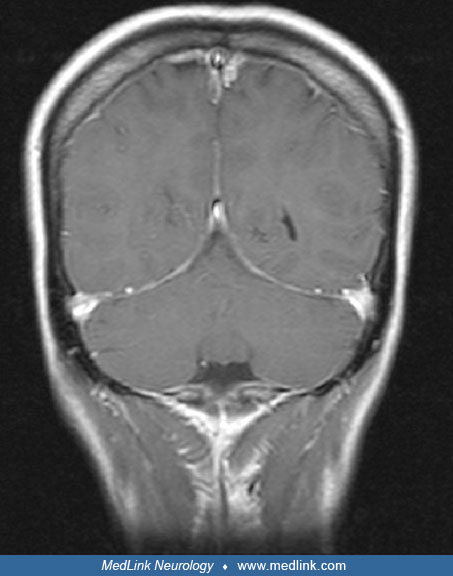
Gadolinium enhanced MRI demonstrated diffuse enhancement and dural thickening consistent with intracranial hypotension.
Treatment with dexamethasone and bedrest was initiated, and the patient's symptoms resolved within 4 days. However, within the month, her symptoms recurred, and she returned to the hospital. At this time, radionuclide cisternography was carried out to search for a cerebrospinal fluid leak.
This showed evidence of multiple ectatic nerve root sleeves, lateral tracking of CSF at the right T9 nerve root sheath, and early renal uptake at 3 hours consistent with a CSF leak.
A thoracic epidural blood patch and a subsequent lumbar epidural blood patch failed to resolve her symptoms, and she was referred for neurosurgical consultation. After 2 more weeks of bedrest and high fluid intake, the patient had no relief of symptoms. She underwent a right T9 laminectomy with intraspinal, extradural rhizotomy, and application of fibrin glue. Following the surgery, she experienced complete resolution of her symptoms.
General approach to neuroimaging in patients with headache. The primary headache disorders (migraine without aura, migraine with aura, cluster headache, tension-type headache, etc.) are diagnosed on the basis of clinical criteria detailed in the International Headache Society Classification and do not dictate the use of neuroimaging under normal circumstances (43). Finding underlying pathology in the context of migraine and a normal neurologic examination is rare (0.18%), and it is for this reason that neuroimaging should not be employed as a screening tool in patients presenting with migraine (71). In fact, the prevalence of meaningful neuroimaging abnormalities in patients with migraine is similar to the general population (36; 113).
The US Headache Consortium developed evidence-based practice guidelines for when to image non-acute headaches (which were defined as headaches present for greater than 4 weeks during a patient’s lifetime) (71). On the basis of an extensive literature review and meta-analysis, the recommendations of this group were incorporated into an AAN Practice Guideline as follows:
Consider neuroimaging in the following: | |
1. Patients with non-acute headache and an unexplained abnormal finding on neurologic examination (grade B evidence). | |
2. Patients with atypical headache features or headaches that do not fulfill the strict definition of migraine or other primary headache disorder (or have some additional risk factor, such as immune deficiency), when a lower threshold for neuroimaging may be applied (grade C). | |
Neuroimaging is not usually warranted in the following: | |
1. Patients with migraine and a normal neurologic examination (grade B). | |
No evidence-based recommendations are established for the following: | |
1. Presence or absence of neurologic symptoms (grade C). | |
2. Tension-type headache (grade C). | |
3. Relative sensitivity of MRI as compared with CT in the evaluation of migraine or other non-acute headache (grade C) (103). | |
Exceptions should be considered in the following cases: | |
1. When patients are disabled by their fear of serious pathology. | |
2. When the care provider is suspicious of underlying pathology, even in the absence of known predictors of neuroimaging abnormalities (71). | |
Clinical judgment should be used when considering whether neuroimaging is indicated for an individual patient. For example, many patients with migraine have some headaches that awaken them from sleep, and if the patients’ clinical features are typical for migraine, neuroimaging is probably not necessary. Studies show that clinicians consistently order neuroimaging examinations when they are not indicated (08). However, progressive or new onset headache can still signify secondary headache, even with a normal neurologic examination. About 12% of patients with brain tumor present with headache as their only symptom (42). Patients with any “red flags,” such as unexplained abnormal neurologic findings on examination, rapidly progressive headache syndromes, and the sudden onset of a new headache suggestive of subarachnoid hemorrhage, should be imaged.
The “SNOOP-4” mnemonic provides a list of red flags that would suggest secondary headache and indicate a need for further evaluation, usually with neuroimaging (119).
• Systemic symptoms (fever, weight loss) or Systemic disease (cancer, immunodeficiency) |
A review update suggested adding other red flags, including pregnancy or puerperium, overuse of medications, and a painful eye with autonomic features due to high prevalence of secondary headache disorders in patients with these presentations (15).
When considering the evaluation of nontraumatic, nonacute headache, MRI is usually preferred to CT due to the lack of radiation exposure and its ability to identify abnormalities in the pituitary or posterior fossa, venous sinuses, and optic nerve (91; 58). However, CT is usually fairly good at identifying abnormalities in the acute setting and may be preferred in those with sinusitis (102). Given the potential for toxicity, the routine use of gadolinium should be avoided unless there is a high index of suspicion for secondary headache disorders such as intracranial hypotension or venous sinus thrombosis (80).
Neuroimaging may also be indicated for new onset or suddenly worsening headache in pregnancy and the immediate postpartum period. Although migraine is still the most common diagnosis, in one study about one third of patients had a secondary disorder, such as preeclampsia or eclampsia, posterior reversible encephalopathy syndrome (RCVS), or pituitary disease. Hypertension, abnormal neurologic findings, and fever increase the odds of abnormal neuroimaging findings (84).
In cases of secondary headache, the location of the lesion can impact the clinical presentation. Occipital lobe arteriovenous malformations (AVM) are much more likely to produce migraine symptoms than arteriovenous malformations in other areas (32). Headache characteristics and location unfortunately are not reliable predictors of secondary headache, as confirmed by a study of headache associated with acute ischemic stroke (101). In the study, lesions of the posterior insula, the operculum, and the cerebellum were especially likely to trigger headache, phonophobia was most common in those with cerebellar lesions, nausea was linked to posterior fossa stroke, and lesions of the parietal lobe, the somatosensory cortex (SI), and the middle temporal cortex increased the risk of cranial-autonomic symptoms.
Practical considerations include patients who expect neuroimaging as part of the evaluation of headache and those who have significant anxiety about their disease. Patients who request neuroimaging are no more likely to have significant abnormalities than the general population (75). Although neuroimaging does initially alleviate anxiety of patients with migraine in other studies, this benefit was lost after 1 year of follow-up (46).
Migraine without aura. Novel imaging studies have uncovered evidence that specific brain regions play a role in migraine generation. Using PET imaging, Weiller and colleagues demonstrated an area of the dorsal rostral midbrain that appeared to act as a "migraine generator" in patients with migraine without aura (115). The area became active at the onset of migraine symptoms and remained active after headache resolution following treatment. A PET study also revealed activation in the dorsal rostral pons in a series of chronic migraine patients with suboccipital stimulators, both when the stimulators were on and when they were off. The authors suggest that the changes in this area may reflect a "constant dysfunctional activation of this structure, as might be predicted in chronic migraine" (64). Goadsby reported a patient who developed chronic migraine with episodic exacerbations following a hemorrhage in a brainstem cavernoma located in the dorsal rostral midbrain (35). Although brainstem structures are active in migraine, studies implicate the hypothalamus as the primary site of migraine initiation. Using high-resolution functional MRI, Schulte and colleagues found the posterior hypothalamus becomes activated in the acute pain phase, whereas the anterior hypothalamus appears to be more involved with attack generation and migraine chronification (96). Studies suggest hypothalamic and dopaminergic activation are important in the premonitory phase of migraine in the 24 hours before an attack. The authors suggest the concept of a single migraine “generator” is too simplistic, and altered connections between brain networks are more important in migraine pathogenesis (97).
Welch and colleagues have demonstrated alterations in nonheme iron homeostasis in the periaqueductal gray of patients with episodic and chronic migraine. They proposed that migraine-associated hyperoxia in combination with abnormally high iron concentrations in the periaqueductal gray make the neurons in this region vulnerable to free-radical damage. This may result in progressive neuronal dysfunction and impairment of the antinociceptive mechanisms of the periaqueductal gray (116).
Functional neuroimaging suggests abnormalities in patients with migraine in response to stimuli, even between acute attacks. Using fMRI scanning, Moulton and colleagues demonstrated that in response to a heat stimulus, migraine subjects have hypofunctioning of the nucleus cuneiformis (a component of pain modulation) compared with controls (73). Interictal abnormalities of basal ganglia are greater in patients with frequent attacks, and the volume of the caudate is less in these subjects. Differences in response to pain also differ in the 2 groups (60). One interictal fMRI study found patients with allodynia during migraine attacks to have lower pain-induced activation in the dorsolateral pons. This area contains the nucleus cuneiformis, an inhibitor of pain responses. In a similar manner, intranasal ammonia stimulation in patients with migraine demonstrates abnormal pain processing with increased activation in areas such as the insula, cingulate cortex, amygdala, cerebellum, caudate, anterior cingulate cortex, and pons (109).
Osmophobia is a common symptom during migraine. In one fMRI-controlled study, a rose odor produced activation in areas implicated in migraine, such as the amygdala, insula, rostral pons, and cerebellum (108).
An elegant study examined the findings of H2O PET in the premonitory phase of nitroglycerine-induced migraine in a group of patients with episodic migraine (61). The findings of this study revealed an increase in the neuronal activation in the posterior hypothalamus, ventral tegmental area, and periaqueductal grey. These changes were ipsilateral to the side of headache.
Several reports of vascular abnormalities on angiography and MR angiography of patients with migraine have been published. These have included segmental narrowing or stenosis and segmental narrowing and dilation. These abnormalities have been attributed to vasospasm and inflammation respectively. However, the relationship between vascular abnormalities and migraine remains unclear (106; 98). In retrospect, some of these previously described abnormalities could have been due to cases of unrecognized reversible cerebral vasoconstriction syndrome.
A published study managed to examine subjects during a spontaneous migraine attack using high-resolution MR angiogram. The authors examined the diameter of intracranial and extracranial arteries on the ipsilateral side of pain and compared it to the contralateral side and to another scan done during a headache-free period. Both the ipsilateral intracranial (middle cerebral) and extracranial (middle meningeal) arteries were dilated during the migraine attack on the side of migraine (01). After taking sumatriptan, the middle meningeal dilation resolved, but the middle cerebral dilation persisted (02). This suggests that sumatriptan does not act on intracerebral vessels but instead acts peripherally.
Interestingly, in cases of secondary headache the location of the lesion can impact the clinical presentation. For example, occipital lobe arteriovenous malformations (AVM) are much more likely to produce migraine symptoms than AVM in other areas (32).
With the advent of MRI technology, nonspecific white matter hyperintensities have become an emerging issue in headache imaging. These abnormalities are common in patients with migraine headache but are not specific for migraine. They are also seen to various degrees in patients with hypertension and genetic diseases such as cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL), cerebrovascular disease, tension-type headache, and normal aging (13; 62). However, it is clear from controlled trials that the incidence of these abnormalities is higher in migraine than in controls (78; 13). One meta-analysis found that patients with migraine are at increased risk for white matter abnormalities as compared to controls, with an odds ratio of 3.9 (95% CI 2.26-6.72) (110). White matter hyperintensities are seen as focal abnormalities on T2-weighted, fluid attenuation inversion recovery, and proton density MRI sequences (24). These abnormalities tend to be located preferentially in the deep subcortical white matter of the frontoparietal regions (49; 24; 13). It has been suggested that these lesions are present in up to 46% of migraineurs; however, some studies suggest that the frequency of these abnormalities is as low as 6% to 12%, particularly when taking into account other medical conditions, such as hypertension and diabetes (24; 10; 87). The issue of white matter hyperintensities is also somewhat controversial with respect to the importance of migraine subtype. Although Fazekas and colleagues suggest that the incidence of white matter hyperintensities is greater in patients with aura, De Benedittis and colleagues and Cooney and colleagues found no difference in white matter hyperintensity frequency between migraine with and without aura subgroups and no difference in frequency of white matter hyperintensities with duration of migraine history. In addition, De Benedittis and colleagues found the same incidence of white matter hyperintensities in patients with chronic tension-type headache (13; 10). Interestingly, patients with new daily persistent headache typically do not have these white matter hyperintensities or infarct-like lesions (89).
On follow-up, these white matter hyperintensities persist, and migraine, as well as length of the disease, correlates with infarct number, especially in the posterior circulation. There is also increased brain iron accumulation in the putamen, globus pallidus, and red nucleus, a marker for increased metabolic activity (52). Headache and these brain lesions do not appear to affect cognition, so they remain of unclear clinical significance (54). Follow-up studies suggest white matter abnormalities are more common in all persons with significant migraine or tension-type headache (45) but that enlargement of perivascular spaces does not differ between persons with and without headache (47).
The pathologic significance of white matter hyperintensities also remains uncertain. There are few pathologic data on patients with migraine; however, studies using diffusion tensor MRI suggest that the areas of parenchymal abnormality in migraine patients with white matter hyperintensities actually extend outside of the white matter hyperintensities themselves into normal-appearing white matter as seen on T2-weighted images. Rocca and colleagues showed that there were differences in the diffusion properties in the normal-appearing white matter of migraineurs; however, these abnormalities were mild compared with other conditions, such as CADASIL and cerebrovascular disease (85). CADASIL should be considered in patients with migraine with aura whose MRIs show the distinctive distribution of white matter hyperintensities in frontal and anterior temporal lobes; they usually have a suggestive family history of stroke, dementia, and migraine with aura (34).
In addition, preliminary evidence suggests functional changes in the cortices of patients with migraine, which may arise secondary to subcortical changes. Functional MRI of patients with white matter hyperintensities demonstrated alterations in the activation of the contralateral somatosensory cortex and the supplementary motor cortex during simple motor tasks when compared with matched controls. In particular, it was shown that activation of the contralateral somatosensory cortex was greater in patients with migraine and that the supplementary motor area was rostrally displaced compared with controls. The extent of these changes correlated with the extent of subcortical white matter change (86). MR spectroscopy studies suggest an abnormal energy metabolism in migraine as compared to control subjects. This abnormality has been noted in all types of migraine and seems to be proportional to the severity of the disease (59).
Multiple fMRI studies have confirmed that migraine subjects have generally stronger functional connectivity in areas involved with pain, sensory, memory, and affective-emotional processing, such as the periaqueductal gray, hippocampus, amygdala, thalamus, and anterior cingulate cortex (38; 48; 99). It is unclear if these functional connections are the cause or result of repeated migraine attacks. It is also possible that functional connectivity changes may predict clinical features such as attack frequency (74). Patients with chronic migraine based on attack frequency appear to have significantly greater functional connectivity than those with episodic migraine in both the periaqueductal gray and areas involved in affective processing (100). In spite of this research, the field has been limited by the lack of confirmatory studies and poor reproducibility, meaning no specific fMRI finding is a biomarker for migraine or a useful tool to guide treatment decisions at this time (105).
Migraine with aura. Neuroimaging has been used to advantage in the investigation of migraine with aura. In addition to the identification of white matter hyperintensities common to many migraineurs (with and without aura), functional neuroimaging has led to a better understanding of the aura itself.
Migraine aura has been attributed to the phenomenon of cortical spreading depression (57). Functional MRI technology has allowed a clear demonstration of the predicted changes in cortex to support the theory of cortical spreading depression as the mechanism for migraine aura. A blood oxygen level-dependent fMRI study of 3 patients with migraine aura demonstrated alterations in blood oxygenation levels in the contralateral visual cortices. These alterations spread over the corresponding retinotopically organized region and corresponded with the onset and cessation of the visual auras. These changes were associated with subsequent decreases in regional blood flow in the occipital cortex (37). A mechanism similar to spreading depression, but one that does not result in aura symptoms, may initiate the headache attacks in migraine without aura, but this remains to be proven.
As case reports of abnormal imaging during attacks have emerged, hemiplegic migraine has been touted as a means to better understand prolonged migraine aura. Using SPECT technology, Crawford and colleagues demonstrated contralateral cerebral hemispheric and ipsilateral cerebellar hemispheric hypoperfusion in a child with hemiplegic migraine (11). In clinical practice, CT perfusion may demonstrate hypoperfusion of the contralateral cortex in patients with hemiplegic migraine during evaluation for possible stroke (40). In contrast, in a case report of a pregnant woman with a history of hemiplegic migraine, Barbour and colleagues reported MRI and SPECT findings consistent with prolonged hyperperfusion and edema of the affected hemisphere. Interestingly, both cases reported meningeal enhancement over the affected cerebral hemisphere. Barbour and colleagues suggest that this finding, along with hemispheric hyperperfusion, lends support to the theory of trigeminovascular activation resulting in vasogenic edema and alterations in cerebrovascular autoregulation (05). The crossed cerebellar diaschisis reported by Crawford and colleagues may underlie the cerebellar symptomatology frequently associated with the aura (and interictal periods) of hemiplegic migraine (11).
Vestibular migraine is another area of special interest. One study using BOLD fMRI demonstrated increased thalamic activation in patients with vestibular migraine after ear irrigation (90). MRI with voxel-based morphometry shows reduced gray matter volume in superior, inferior, and middle temporal gyrus and occipital cortex, in addition to those areas typically involved in migraine (77).
Recommendations. As the overall yield of neuroimaging in migraine patients with a normal neurologic examination and with typical migraine features is low (0.18%), Frishberg and colleagues made the following recommendation based on literature review and expert opinion (30):
In adult patients with recurrent headaches defined as migraine, including those with visual auras with no recent change in headache pattern, no history of seizures, and no other focal neurologic signs or symptoms, the routine use of neuroimaging is not warranted. In patients with atypical headache patterns, a history of seizures, or focal neurologic signs or symptoms, CT or MRI may be indicated (29). |
Another study provides data that reinforce some of the above recommendations. Of 920 migraine patients with a normal clinical examination who were referred to a neurologist, the rate of significant intracranial abnormalities on neuroimaging was 0.4% (95% CI 0.1, 1.4) (102). The abnormalities found were pituitary adenoma, hydrocephalus, arteriovenous malformation, and colloid cyst. In contrast, of 188 patients where the headache diagnosis was considered “indeterminate,” 3.7% showed significant intracranial abnormalities (95% CI 1.5, 7.5). Routine neuroimaging in pediatric patients with headache is also fairly low yield. Although 9.3% of patients had some neuroimaging abnormalities, less than 1% of patients (11 of 1204) required surgical intervention as a result. Abnormal neurologic examination was the only reliable predictor of abnormal neuroimaging findings (83).
A large systematic review and guideline from the American Headache Society stated there is no need for neuroimaging in patients with migraine and a normal neurologic examination without atypical features or red flags (21). Neuroimaging may be considered for patients with migraine and atypical features, changes in clinical features, or after recent head trauma.
As for the type of imaging to pursue when neuroimaging is warranted, local medical resources and the time-course of the headache must be taken into consideration. CT scanning is more sensitive for acute hemorrhage, bony abnormalities, and calcified lesions. Its sensitivity for intraparenchymal masses is increased with contrast media, which shows areas of blood-brain barrier breakdown (33).
For patients who need neuroimaging, MRI has several advantages over CT scanning. MRI is more accurate in identifying small masses, nonacute hemorrhages, dural sinus thromboses, small arteriovenous malformations, venous anomalies, and abnormalities in the posterior fossa, in the region of the internal auditory canals, and in the area of the temporal bones (33). The planar imaging made available by MRI is also useful in the diagnosis of Chiari malformations, which are most easily seen on sagittal images.
Cluster headache. Our understanding of cluster headache has also been furthered as a result of advances in neuroimaging. Functional MRI, MRS, SPECT, and PET scanning have all been used in the study of cluster headache (68). These studies have been used to demonstrate brain regions activated during cluster headache, including the ipsilateral hypothalamic gray matter (67). Other pain processing regions, such as the anterior cingulate gyrus, insula, and posterior thalamus, have also been shown to be active during cluster headache, but these areas are active during other kinds of pain (68; 67).
Further support for hypothalamic involvement has emerged from structural neuroimaging techniques, such as voxel-based morphometry. This is an automated whole-brain scan that allows comparison of structural images in healthy individuals versus groups of patients. This technique has suggested an increase in the volume of the posterior hypothalamic gray matter in cluster patients, as compared with healthy volunteers. No changes have been noted in the white matter in this region (66). This change in volume seems to be slightly lateralized, ipsilateral to the side of the pain, and similar to the area of activation observed in acute cluster headache attacks through PET scans (66). Further studies have confirmed enlargement of the anterior hypothalamus in both episodic and chronic cluster headache (03). The resting state changes of patients receiving hypothalamic deep brain stimulation confirm these findings, but it is unclear if hypothalamic changes modulate or generate the disorder, or if these changes are the result of cluster attacks (25).
Multiple secondary causes of cluster headache have been reported, including multiple sclerosis, pituitary tumors, carotid dissection, invasive orbital infection, orbital trauma, parainfluenza virus, and tumors in the upper cervical region, posterior fossa, tentorium, and parasellar region (53; 39; 112; 69; 22; 44; 07; 56; 81; 06; 28). A study of 1876 consecutive patients referred to a neurology clinic with non-acute headache included 20 patients with cluster headache (102). All of them were imaged. One abnormality, a pituitary adenoma, was found in 1 of these 20 patients. Neurologic examination had been normal. An example MRI of a growth-hormone secreting adenoma producing cluster-like headache is included.
Favier and colleagues performed a PubMed search for symptomatic cases of cluster headache and found 23 cases (23). These patients had a dramatic improvement or even cessation of headache after treatment was directed at the underlying pathology. Of the 23 patients, 15 fully fit the International Headache Society criteria for cluster headache. The majority of patients had either vascular abnormalities or tumors. Of the tumors, the most common were pituitary tumors. In 2 patients, the lesions were recognized on an MRI scan but not on a CT scan. Sixteen patients demonstrated good response to usual cluster headache treatments. Edvardsson reported on 63 cases of symptomatic cluster headache in the literature (20). In patients with cluster-like headache and prolactin-secreting pituitary adenomas, treatment with dopamine agonists such as cabergoline may resolve the disorder (14).
Cavernous sinus pathology has also been implicated as a cause of cluster headache (41), including overflow into the area due to adjacent pathology such as the superior sagittal sinus invasion from a parasagittal hemangiopericytoma (27). A study found that subjects with cluster headache had wider skulls than controls but no significant differences in the dimensions of the cavernous sinus and surrounding structures (04).
Neuroimaging in this relatively uncommon headache type should be considered in all cases, particularly if the cluster headache has atypical features, there are abnormalities on physical or neurologic examination, or there is a sudden increase or change of symptoms (23). Atypical features may include such things as prolonged duration, progressive worsening, lack of periodicity, persistent pain, onset in an older person, cluster headache in an immunocompromised patient, or resistance to typical cluster headache therapies. Although CT will identify most major intracranial abnormalities, it is less effective in obtaining images of the sella, parasellar region, and posterior fossa; therefore, MRI is the imaging modality of choice for cluster headache. A case report described a new onset of cluster headache in association with a demyelinating lesion in the brachium pontis and new diagnosis of multiple sclerosis (79). If the headache is associated with persistent autonomic symptoms between attacks, vascular imaging may be warranted to rule out dissection (28).
Paroxysmal hemicrania. Paroxysmal hemicrania is a trigeminal autonomic cephalalgia with more frequent but shorter lasting attacks than cluster. Autonomic symptoms are not as severe, and agitation is less common. Importantly, paroxysmal hemicrania is an indomethacin-responsive headache syndrome. Interestingly PET studies showed activation of the posterior hypothalamus as in cluster, but contralateral to the symptomatic side. This activation resolved with successful treatment with indomethacin (63).
SUNCT. Short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) is classified as one of the trigeminal autonomic cephalalgias. This rare headache syndrome warrants mention in this review because of reports of an association between pituitary pathology and SUNCT. Case reports have appeared in the literature citing cessation of SUNCT after removal of coexistent pituitary adenomas. The incidence of adenomas in SUNCT is not known, because the condition is uncommon; however, based on some reports, it would appear that MRI imaging with dedicated views of the sella is warranted (65; 88).
Similar to cluster headache, the pathophysiology of SUNCT appears to involve the hypothalamus. This has been demonstrated by BOLD-fMRI studies. Significant activation has been noted in the inferior posterior hypothalamic gray during attacks of SUNCT. The side involved seems to be less clearly defined in SUNCT, however. Cohen performed BOLD-fMRI studies in 9 patients and found 5 with bilateral activation, 2 with contralateral activation, and 2 with ipsilateral deactivation of the hypothalamic gray (09; 66).
Trigeminal neuralgia. Trigeminal neuralgia is classified among primary headache disorders, but “classical” trigeminal neuralgia is felt to be related to compression of the trigeminal nerve by blood vessels, such as the superior cerebellar artery. When a secondary neurologic disorder, such as multiple sclerosis, causes trigeminal neuralgia, the disorder is considered secondary (12). MRI features of compression can predict atrophy of the trigeminal nerve and prognosis after surgical decompression (55).
Nummular headache. Nummular headache is characterized by a discrete area of head pain in a focal circumscribed area (as little as 1 cm), which may be constant. Secondary causes of nummular headache, including inflammatory disorders and infections, are not rare, and neuroimaging is generally recommended (118).
Headache secondary to COVID-19. Although the overall incidence of neurologic disease is relatively low in patients with COVID-19, headache is a common compliant. In patients receiving neuroimaging for COVID-19, nonspecific white matter changes and chronic infarcts are more prevalent than acute ischemia or hemorrhage (82). Focal neurologic deficits, but not mental status changes or headache, predicted the incidence of important imaging findings. In rare cases, headache has been reported as the first symptom of COVID-19, including a case report of signal changes in the right lateral ventricle, right mesial temporal lobe, and hippocampus (72).
Thunderclap headache. When discussing neuroimaging of vascular headaches, thunderclap headache should not be overlooked. This severe headache of sudden onset is classically associated with aneurysmal subarachnoid hemorrhage and possibly unruptured saccular aneurysms. However, there are reports of thunderclap headache in association with a variety of other pathologies such as RCVS, dural sinus thrombosis, hypertensive encephalopathy, spontaneous intracranial hypotension, and pituitary apoplexy (19; 18; 111; 16; 117). Given its association with serious secondary headache disorders, thunderclap headache warrants immediate neuroimaging. As thunderclap headache is classically associated with subarachnoid hemorrhage, CT scanning is a first-line investigation, followed, if necessary, by lumbar puncture. This combination of investigations is highly sensitive in identifying subarachnoid blood in the initial 12 hours after headache onset (16). If the CT scan is normal and there is no evidence of xanthochromia, the likelihood of an undiagnosed subarachnoid hemorrhage is low. However, CT is less reliable for the diagnosis of RCVS, dural sinus thrombosis, hypertensive encephalopathy, vasospasm, pituitary apoplexy, and intracranial hypotension. Therefore, in the appropriate clinical setting, an MRI is often necessary. In particular, RCVS may be a relatively common cause of thunderclap headache and is increasingly recognized based on multiple large case series (104). Because RCVS has been associated with thunderclap headache, noninvasive vascular imaging, such as MRA, should also be strongly considered because of the risk of significant neurologic morbidity including stroke (19; 17; 76).
Spontaneous intracranial hypotension. Spontaneous intracranial hypotension refers to a headache due to low CSF pressure. The headache is classically worse when the patient is in the upright position and relieved when he or she is in the supine position. There are 5 characteristic MRI features, which can be remembered with the mnemonic “SEEPS.” S stands for subdural fluid collections, E for enhancement of the pachymeninges, E for engorgement of venous structures, P for pituitary hyperemia, and S for sagging of the brain (92).
Subdural fluid collections are common in this condition, occurring in about half of patients. They usually represent hygromas and are thin, bilateral, and located over the cerebral hemispheres. Enhancement of the pachymeninges is diffuse and does not involve the leptomeninges. The enhancement arises from thin-walled, dilated blood vessels in the subdural area. Sagging of the brain is a very specific sign in spontaneous intracranial hypotension. It can include any of the following: effacement of the perichiasmatic and prepontine cisterns, bowing of the optic chiasm, flattening of the pons, and downward displacement of the cerebellar tonsils (mimicking a Chiari I malformation). Ventricular collapse may also be seen (26; 50; 107; 92).
The MRI abnormalities can improve within hours to weeks after successful treatment of the CSF leak. Generally, clinical improvement occurs first, before MRI changes are seen (92).
Although a CSF leak is not found in all patients, investigations to localize the leak are warranted in some cases. CSF leaks may develop due to cough, minor trauma, or bony protrusions from the spine that disrupt the meninges. CSF leaks may be associated with spinal meningeal diverticula, nerve root sheath tears, ruptured perineural cysts, and direct CSF venous fistulas. With the exception of CSF venous fistulas, most cases are associated with extradural CSF collections (93).
CSF leaks are most common in the thoracic region, but may appear at any level. In a review of 11 patients with spinal CSF leaks, Schievink and colleagues found 2 cervical spine CSF leaks, 3 leaks at the cervicothoracic junction, 5 leaks in the thoracic region, and 1 leak in the lumbar region (95). Localizing the leak is typically accomplished by using radionucleotide cisternography or myelography. Radionucleotide cisternography involves introduction of radioactive tracer into the CSF by lumbar puncture, followed by sequential images of the tracer as it diffuses along the neuroaxis. Leakage along nerve root sheaths and early renal uptake are indicators of a leak. However, the usefulness of radionucleotide cisternography is somewhat limited because of poor resolution, and, therefore, it is less commonly utilized now (92). CT myelography and MRI myelography (where contrast media is injected intrathecally) have greater spatial resolution (50; 31). Although these procedures are somewhat invasive, they are warranted, as their results are used to confirm diagnosis and guide treatment.
If MRI cannot be performed, the work-up of a patient with a postural headache suspicious for spontaneous intracranial hypotension should consist of a routine axial CT and lumbar puncture with opening pressure. If the CT is normal or shows subdural fluid collections and the opening CSF pressure is low (less than 7 cm H2O), further cranial imaging may not be necessary in the context of a typical history for spontaneous intracranial hypotension. The clinical features should be carefully considered, however, as patients with headache and documented CSF leaks have been found to have normal CSF pressures (70; 94).
When MRI is available, a patient with a headache suspicious for intracranial hypotension should first have a brain MRI with gadolinium, as this has the potential to yield so much more information with regard to the diagnosis than CT. Brain MRI is not always abnormal, however, even in patients with proven CSF leaks, and may be normal in as many as 22% of patients (94). If brain MRI is planned, it must be kept in mind that once a lumbar puncture is done, the same MRI abnormalities may occur for a time as a result of CSF leak from the lumbar puncture site.
If the patient’s headache is in keeping with spontaneous intracranial hypotension and MRI findings support the diagnosis, then a lumbar puncture or further investigations may not be necessary. The patient should first receive one or more blood patches (at least 5 days apart) to see if symptoms improve. Sometimes, if patients don’t respond fully to the first blood patch, they may respond to a second, or third, larger volume, blood patch. If little or no improvement occurs, then further tests to localize the CSF leak are warranted.
In order to localize the CSF leak, CT myelography can be used for its greater spatial resolution and sensitivity (50; 31; 94). CT myelography has so far been the imaging modality of choice to define the location and extent of a CSF leak (92), but newer techniques are being increasingly used.
The use of regular spinal MRI as an investigation to determine the existence of CSF leaks (but not necessarily the exact location) has also been promoted for its sensitivity and noninvasiveness (70). Findings on spinal MRI include dilated epidural or intradural veins, dural enhancement, syringomyelia, meningeal diverticula, retrospinal fluid collections (at C1-C2), and extradural CSF collections (92).
One of the newer imaging techniques being utilized to detect CSF leaks in a noninvasive manner is heavily T2-weighted MR myelography. Wang and colleagues compared this technique to invasive CT myelography in a study of 19 patients (6 men and 13 women) with spontaneous intracranial hypotension. MR myelography did not differ from CT myelography in the detection rates of CSF leaks along the nerve roots, high-cervical retrospinal CSF collections, and epidural CSF collections. MR myelography demonstrated more spinal levels of CSF leaks and epidural collections than CT myelography. The authors concluded that heavily T2-weighted MR myelography is accurate in localizing CSF leaks. This noninvasive technique may be an alternative to CT myelography and avoids the large amount of radiation required for CT myelography (114).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Michael J Marmura MD
Dr. Marmura of Thomas Jefferson University received research support from AbbVie, Axome, and Lundbeck and consulting honorariums from Impel and Lumbeck.
See Profile
Stephen D Silberstein MD
Dr. Silberstein, Director of the Jefferson Headache Center at Thomas Jefferson University has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026