



Epilepsy & Seizures
Febrile seizures
Jun. 02, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Brain stimulation for epilepsy provides an alternative to pharmacotherapy and resective, ablative, or disconnection surgery for patients with medication-resistant epilepsy. Although relatively rarely achieving seizure freedom, these therapies can provide substantial benefits to quality of life, reducing the risk of sudden unexpected death in epilepsy, reducing the burden of common comorbidities, and occasionally reducing antiseizure medications with their associated adverse effects. They can also provide unique insights into epilepsy through ultra-long-term monitoring. Stimulation routes include vagus nerve stimulation, deep brain stimulation, responsive neurostimulation system, and other novel targets. Based on FDA approval in the United States, this article focuses on vagus nerve stimulation, deep brain stimulation, and responsive neurostimulation system.
|
• Responsive neurostimulation system provides targeted stimulation to up to two locations in the brain. | |
|
• Responsive neurostimulation system can augment typical inpatient intracranial EEG monitoring before subsequent neurosurgery. | |
|
• Deep brain stimulation requires less precise localization while also substantially improving seizure frequency and perhaps neurocognitive outcomes. | |
|
• Vagus nerve stimulation provides an alternative to intracranial surgery while also providing both seizure frequency improvement and reducing rates of sudden unexpected death in epilepsy. |
The first neurostimulation therapy was vagus nerve stimulation, which began in 1988 and was licensed in 1997. Subsequently, responsive neurostimulation and deep brain stimulation were shown to be alternatives. Although numerous other targets have been explored, these three have earned U.S. Food and Drug Administration approval. More recently, other techniques and targets are being explored as adjunctive therapies for epilepsy, including focused ultrasound, trigeminal nerve stimulation, transcranial focal cortex stimulation, transcranial magnetic stimulation, transcranial direct current stimulation, and chronic subthreshold cortical stimulation.
These technologies share common goals to modify the abnormal network associated with epileptic seizures. By stimulating these networks, modulation of the network activity is achieved, and ideally, acute stimulation can stop, shorten, or reduce the spread of epileptic seizures. Chronic stimulation may cause network modification to reduce the propensity for epileptic seizures. In this way, the onset of action can be delayed, and the maximum efficacy of neurostimulation or neuromodulation technologies can be years after initiation of treatment. The term neuromodulation reflects how the stimulation from these technologies can modify the epileptic network. The unique perspective of each technology can also provide supplemental information about the pathophysiology of epilepsy both on an individual and population level.
Many patients do not achieve seizure control without adverse effects using antiseizure medication (50). Some of these patients whose seizures are medication-resistant are candidates for curative surgery that could result in long-term seizure freedom without disabling deficits (20; 38; 77). However, many patients have medication-resistant epilepsy and are not candidates for epilepsy surgery. Based on the fundamental principle that epilepsy is a disorder of abnormal electrical activity, neurostimulation aims to directly modify the abnormal electrical activity associated with epilepsy (28).
Neurostimulation can take two, not-mutually-exclusive approaches: continuous stimulation or responsive stimulation. In continuous stimulation, there is a baseline cycle of stimulation to reduce the long-term likelihood of seizure. Similar to selecting doses of an antiseizure medication, the clinician can modify various settings of the stimulation technology to maximize seizure frequency and reduce and minimize unintended adverse effects. In responsive stimulation, the stimulator monitors for quantitative criteria to be met before providing stimulation. By only stimulating when those criteria are met, the number of stimulations per day may be reduced. Therefore, battery life may be longer while also reducing adverse effects incurred by stimulations that have a low likelihood of improving seizure control.
Each neurostimulation device has titratable parameters of stimulation that can be personalized based on seizure response and adverse effects. The initial seizure response to neurostimulation can be low, with 40% of patients experiencing at least 50% reduction (14). Prolonged neurostimulation is thought to modify the underlying network, resulting in as high as 80% of patients with at least a 50% reduction in seizure frequency in prolonged follow-up; however, these results do not include a control group, so the effect of natural history is unknown. Patients may pursue interventions for their epilepsy when their seizures worsen, and, irrespective of the intervention, long-term seizure frequency may naturally be reduced over the course of years (27).
Improved reduction in seizure frequency with neurostimulation over time. Abbreviations: vagus nerve stimulation, anterior nucleus of the thalamus deep brain stimulation, responsive neurostimulation system. (Figure from: Dibue-A...
This article provides a clinical description of the use of neurostimulation for medication-resistant epilepsy. Due to this clinical focus, this article discusses the FDA-approved technologies of vagus nerve stimulation, deep brain stimulation, and responsive neurostimulation system. Although other technologies are emerging, they are not widely clinically available and, therefore, are outside this article’s scope.
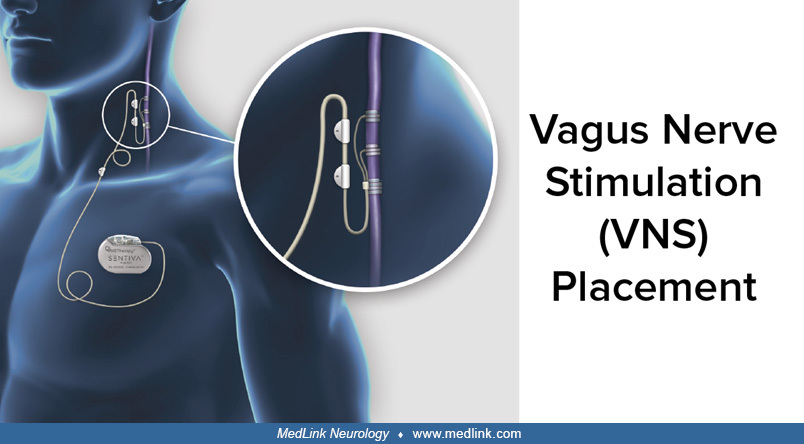
Vagus nerve stimulation. The vagus nerve stimulator is a coiled electrode placed on the vagus nerve in the neck. Placement of the vagus nerve stimulator is a relatively low-risk procedure. However, once placed, scar tissue can form around the stimulation coil. This significantly complicates removal; therefore, if the vagus nerve stimulator is ineffective and the patient desires to remove the device, this coil can be left in place while the remainder of the hardware is removed. However, long-term studies have demonstrated a low incidence of adverse effects when the hardware remains in place; therefore, the risk of a surgical procedure with anesthesia may outweigh the low risk of complications from leaving the hardware in place lifelong (95; 54). Thus, patients should be advised that the hardware might not be removed once placed.
The placement of conductive material in the neck can complicate the acquisition of MRI due to the potential for local heating and unintended ablation of the vagus nerve or injury to the carotid artery (86). Comprehensive epilepsy centers often have specific MRI parameters to ensure safety and image quality, so brain MRIs can be obtained at 1.5T and 3T (22).
The MRI risk is reduced if removed according to the standard of leaving less than 2 cm of the lead. These safety protocols frequently focus on MRIs of the brain, but there is a region directly over the stimulator battery and hardware where MRI is contraindicated, even when the device is off or the battery is dead (eg, direct chest imaging or magnetic resonance cholangiopancreatographic [MRCP]). Therefore, patients with epilepsy and comorbid diseases that may warrant MRI in these regions should be counseled about this contraindication.
The stimulation provided by the vagus nerve has a typical duty cycle of 30 Hz stimulation with a current of 1.5 to 2.25 mA for 30 seconds, then 5 minutes of no stimulation (96). A higher amplitude of stimulation is associated with more activation and potentially more antiseizure activity up to currents of about 2.0 to 2.5 mA. However, a higher amplitude of stimulation is associated with more side effects of hoarseness and cough due to stimulation of the recurrent laryngeal nerve. Similar to a medication, some patients acclimate to this effect over time. Starting at a low level of stimulation and slowly titrating up may allow patients to achieve a higher amplitude of stimulation without this adverse effect. In addition to titration of the amplitude, the on- and off-times also can be titrated. An increase in the total duration of stimulation leads to shorter battery life. Rapid cycling also shortens battery life; therefore, it should be minimized unless clinical benefit is evident (62). At typical settings, the battery needs to be replaced every 3 to 8 years (10).
In addition to this chronic stimulation, there are two types of responsive stimulation. When a patient feels an aura or pre-seizure warning, the patient can place a magnet over the device. This provides stimulation with the goal of aborting or shortening that individual seizure (96). Additionally, more recent versions of the vagus nerve stimulator include an autostimulation function that provides automated monitoring of the patient’s heart rate. Based on reports that 82% of epileptic seizures may be preceded by an abrupt increase in heart rate (17), the vagus nerve stimulator monitors a titratable, abrupt increase in heart rate, and additional stimulation is provided when the threshold is surpassed with the goal of either aborting or shortening the seizure. To avoid false-positive stimulation, there are safeguards against prolonged stimulation (and stimulation for normal heart rate patterns, eg, exercise) (58). The autostimulation parameters also can be modified if the patient or provider notes excessive false-positive stimulation.
Deep brain stimulation. Deep brain stimulation also provides chronic stimulation but has an intracranial target. The only FDA-approved target in the United States is the anterior nucleus of the thalamus due to projections to the temporal lobes, but other targets have been explored, including the centromedian nucleus of the thalamus (thought to be effective in generalized-onset multifocal seizures and Lennox-Gastaut syndrome) (11; 75), and pulvinar targets (projects to the temporal-occipital region) (01; 89; 92), as well as other targets, including the subthalamic nucleus (used in Parkinson disease), hippocampus, inferior caudate, cerebellum, parafascicular nucleus of the thalamus, or the patient’s specific seizure-onset zone (98).
(Reproduced from NINDS and modified from: Edwards CA, Kouzani A, Lee KH, et al. Neurostimulation devices for the treatment of neurologic disorders. Mayo Clin Proc 2017;92(9):1427-44. Other helpful information for patients and p...
Placement of the device has similar a surgical technique and procedure compared to depth electrodes for surgical evaluation of epilepsy or responsive neurostimulation. Surgical targeted techniques can be used to create a small hole in the cranium that allows the stimulation electrode to pass with minimal trauma to surrounding structures. One of the main concerns about placement is avoidance of cerebral arterial and venous vasculature, as well as other eloquent structures. Asymptomatic clinically insignificant hemorrhages occurred in 4.5% of participants in the pivotal trial, SANTE (23). With the development of robotic guidance of electrode placement, this complication rate has been substantially lowered (07; 55). These complications can occur in patients with unrecognized coagulation disorders (eg, von Willebrand disease) and supplements with anticoagulant effect, including, but not limited to, ginkgo biolab, chondroitin-glucosamine, melatonin, turmeric, and chamomile (30). Once placed, the electrodes are fixed and stabilized using the skull, and stimulation wires are tracked down to the stimulation device, which is placed on the chest. Tracking the wires down to the stimulation device is similar to the techniques used for ventricular-peritoneal drains. The stimulation device and battery are placed similar to a cardiac pacemaker.
After placement and time for healing, stimulation begins (23). The standard stimulation settings in the pivotal trial were 5 V amplitude at 145 Hz with a cycle of 1 minute on and 5 minutes off. Alternate stimulation parameters include increasing voltage to 7.5 V and increasing frequency to 185 Hz, but these were not studied rigorously in trials. Typical settings range from 1 to 10 V and frequencies from 100 to 250 Hz, with different targets of deep brain stimulation having different canonical settings. Based on experiences with hoarseness from vagus nerve stimulation, one would presume that the adverse effect of paresthesias reported in 18.2% of patients may be related to direct stimulation of the thalamus; therefore, changing the amplitude or frequency of the signal may reduce this adverse effect, but this is not well studied. Rarely, patients have transient acute stimulation-associated seizures when the deep brain stimulation is turned on. In this case, the deep brain stimulation should be turned off and restarted at a lower voltage. Acute stimulation-associated seizures have not been associated with poor treatment response or prognosis (67).
Responsive neurostimulation system. Compared to vagus nerve stimulation and deep brain stimulation that have a standard approach for most patients, with some personalization, the stimulation target of each patient with a responsive neurostimulation system is personalized to the exact localization of the patient’s seizure onset zone (83). This localization is determined based on an epilepsy surgical evaluation for medication-resistant epilepsy that may include intracranial monitoring with depth or strip electrodes. Some patients may have a responsive neurostimulation system placed without depth or strip electrode monitoring. Despite completion of a surgical evaluation, the responsive neurostimulation system is FDA-approved as an adjunctive therapy for patients who are not candidates for resective or ablative epilepsy surgery. There are multiple reasons why a patient is not a candidate for resective or ablative epilepsy surgery.
The patient may not have been a candidate because resection of the target area would result in intolerable neurologic deficits (eg, aphasia or paresis). Although continuous stimulation or ablation of the area may result in these intolerable neurologic deficits, the responsive neurostimulation system only stimulates when a preictal or early ictal EEG signature is detected.
Alternatively, the patient may have multifocal epilepsy including but not limited to bilateral anterior temporal lobes. In this case, resection or ablation of both anterior temporal lobes would cause loss of declarative memory similar to patient HM (71). However, the patient may benefit from two responsive neurostimulation system electrodes placed with one in each seizure-onset zone to reduce seizure frequency and severity – (the current generation responsive neurostimulation system is limited to two strip or depth electrodes and each has four contacts.) In addition to these direct effects on seizures both acutely and through neuromodulation, the responsive neurostimulation system records snippets of the electrocorticography based on features concerning for seizures. These electrocorticography data can be uploaded via the internet for review by the treating epileptologist.
In addition to guiding the selection of responsive neurostimulation system parameters, the relative burden of seizures associated with each responsive neurostimulation system could guide future curative epilepsy surgery. Data from these ultra-long-term recordings have demonstrated that although inpatient intracranial monitoring for a week or two may observe a small and different number of seizures, this short-term seizure count may not reflect the patient’s chronic burden (43). Consider a hypothetical patient who experienced one left temporal-onset and six right temporal-onset seizures during inpatient intracranial monitoring, and bilateral temporal responsive neurostimulation system was placed. After 12 months of follow-up, if all seizures were observed by the right temporal responsive neurostimulation system, it could be reasonable to propose a potentially curative right temporal lobe resection (33). In a series of 24 patients with bilateral temporal epilepsy treated with a responsive neurostimulation system and a subsequent mesial temporal lobe resection, nine patients had unilateral electrographic seizures, and all were seizure-free, whereas 15 patients had resection of the more active side, and 53% (8 of 15) were seizure-free (33).
In addition to these FDA-approved targets, there is increasing interest in responsive neurostimulation targeted to the thalamus, similar to deep brain stimulation. The FDA has approved any intracranial placement of the responsive neurostimulation system without excluding thalamic or other subcortical targets, but no randomized trials of thalamic targets have yet been published. A hypothesis is that dual cortico-thalamic stimulation of both the seizure onset zone (eg, temporal) and the associated thalamic nucleus (eg, anterior nucleus) could further modulate the network involved in the epilepsy and produce improved seizure control. In addition, there is an ongoing trial evaluating the use of responsive neurostimulation targeted to the thalamus for generalized-onset epilepsy (NAUTILUS, NCT05147571). For these thalamic targets, the neurophysiologic signal differs from that of the cortex. Additionally, the responsive nature of the responsive neurostimulation system means that it cannot be programmed to exactly match the stimulation parameters of a deep brain stimulator, but it can be programmed to have a high false-positive rate that may mimic deep brain stimulation. The impact of these pseudo-closed-loop parameters on battery life is not completely known.
Compared to vagus nerve stimulation and deep brain stimulation that are continuously stimulating with chosen parameters, the responsive nature of the responsive neurostimulation system allows for more flexibility. If all seizures could be detected and aborted early without changing the underlying normal neural activity, patients would theoretically achieve seizure freedom without side effects. In this way, the responsive neurostimulation system is a closed-loop system that uses electrocorticography to detect preictal or early ictal features and provide stimulation to halt the seizure or stop propagation. When the device is placed, the provider selects the electrocorticographic features that will trigger data to be saved, with three default triggers: magnet swipe by the patient, high amplitude saturation of the electrocorticography data, or sustained changes in the electrocorticography, called long episodes. Each of these events could indicate a seizure. The latter two triggers also can be modified by the provider after placement to, for example, change the bandpass filter or reduce the line length detector to detect smaller changes in the electrocorticogram.
There are five stimulation settings, three of which are personalized. Stimulation frequency typically is set at 200 Hz, and burst duration is set at 100 ms (values based on recommendations of NeuroPace physician manual).
|
(1) Current: initial setting 1.0 mA and adjusted in steps of 0.5 mA with a median setting 6 mA with a 90% range from 6 to 12 mA. | |
|
(2) Frequency: median setting of 160 microseconds, with a 90% range from 160 to 200 microseconds. | |
|
(3) Bursts per day: median setting 570, with a 90% range from 100 to 1330. |
In addition to these stimulation parameters, the provider can select which electrodes provide the stimulation. As the strip and depth electrodes include both stimulation and recording electrodes, this can be changed after implantation. In patients who had an incomplete response to these stimulation settings, alternative stimulation strategies have been pursued (eg, low-frequency stimulation) (03).
When changing parameters and stimulation locations, providers should evaluate for evidence of clinical symptoms or after-discharges from stimulation both in the clinic and through the patient data management system. After-discharges are associated with stimulation-induced seizures as compared to the desired effect of stimulation-aborted seizures.
There is a significant variation in estimated battery life based on stimulation parameters. NeuroPace estimates that 5% of batteries last less than 5.1 years and 5% last more than 9.4 years, with the median battery lasting 8.4 years. Increased current, frequency, and bursts per day can reduce battery life, as can prolonged interrogation of the device for more than 10 minutes per day.
To guide modification of these seizure detection and stimulation parameters, patients are trained to interrogate their device daily and sync with the remote patient data management system weekly. Although patients are typically seen every 3 months by their responsive neurostimulation system provider, any responsive neurostimulation system provider can log into this system remotely between visits to review the records.
In selecting the appropriate detection parameters, the provider aims to detect the electrographic signature of a disabling seizure as early as possible while also balancing sensitivity and specificity. If trigger detection has low sensitivity but high specificity, then patients may experience seizures that could be aborted if stimulated (false negatives). In contrast, if the triggers are set with high sensitivity but low specificity, multiple stimulations may reduce battery life and potentially produce stimulation-related adverse effects (false positives). However, due to the observation that chronic neurostimulation may result in neuromodulation and progressive improvements in seizure frequency, the provider may opt to have more false positive stimulations that may result in neuromodulation, compared to favoring a high false negative rate with low stimulation frequency. Each of these choices can be individualized in discussion with the patient and caregivers.
Patients with epilepsy are defined as medication-resistant if two or more appropriately chosen antiseizure medications have failed in adequate trials (50). Approximately 70% of patients with epilepsy will be medication responsive and, unless there are unique situations, these patients should not be considered for neurostimulation because the risks and efficacy of neurostimulation are likely inferior to tolerated pharmacotherapy (83; 16; 14; 82). For patients with medication-resistant epilepsy that are good candidates for resective, ablative, or disconnection surgery, the rates of seizure freedom in these surgical approaches is superior to neurostimulation (21; 38; 15; 06). Therefore, unless there is evidence that surgery would result in an intolerable neurologic deficit in that specific patient, then surgery should not be delayed in favor of neurostimulation. This is because epilepsy surgery is potentially curative and the success of epilepsy surgery is associated with reduced time from seizure onset to curative surgery (57; 52; 56; 94; 19). Some clinicians refer to any epilepsy surgery in which the goal of surgery is not seizure freedom, including neurostimulation, as “palliative.” Due to the association with palliative care at the end of life, this phrasing may have unintended emotional content and also may not adequately communicate that the majority of patients who underwent those surgeries had more than 50% seizure reduction and improved quality of life after surgery (36).
Although vagus nerve stimulation does not require localization of the seizure-onset zone, a responsive neurostimulation system requires precise localization, and deep brain stimulation covers a broad area that should contain the seizure-onset zone. Deep brain stimulation of the anterior nucleus of the thalamus allows for effects that project onto larger areas of cortex that likely will contain the epileptogenic zone and thereby reduce the propensity for epileptic seizures. A responsive neurostimulation system requires the identification of no more than two lead placements that are similar in specificity to the field of view of recording electrodes. More recently, clinicians have utilized the two lead placements for a cortical (eg, temporal) target and a thalamic (eg, anterior nucleus) target. Investigations of responsive neurostimulation systems with purely thalamic targets mimic deep brain stimulation. Specifically, there is an ongoing trial evaluating the use of responsive neurostimulation targeted to the thalamus for generalized-onset epilepsy (NAUTILUS, NCT05147571).
As with many subspecialized treatments for epilepsy, there are racial and socioeconomic disparities in the usage of neuromodulation devices. Specifically, neuromodulation was underutilized in patients who were Black or African American or had insurance through Medicare or Medicaid (02; 91). This disparity should not be due to the cost of the technology. Although the cost-effectiveness of epilepsy surgery has been well-established, there is evidence that neuromodulation also may be cost-effective for medication-resistant epilepsy (65).
Each neurostimulation technology addresses a unique population of patients with epilepsy and has unique cautions.
Vagus nerve stimulation has the fewest contraindications. However, a vagus nerve stimulation is a coil around the vagus nerve that is intended to conduct electricity. Consequently, vagus nerve stimulation can cause complications with the acquisition of magnetic resonance images of the neck, chest, and upper abdomen. The MRI restrictions for vagus nerve stimulation depend on the generator model. The artifact from vagus nerve stimulation also can influence magnetoencephalography but not electroencephalography or electrocardiogram (ECG or EKG) (47). Vagus nerve stimulation has been associated with the development of central and obstructive sleep apnea; therefore, patients and providers may avoid vagus nerve stimulation placement in patients with preexisting, untreated sleep apnea (99; 25).
As discussed in the Indications section of this article, a responsive neurostimulation system requires precise localization of the seizure onset zone. If the hypothesis for this zone is too broad to be captured by one or two responsive neurostimulation system electrodes, then a responsive neurostimulation system may be ineffective.
For both deep brain stimulation and a responsive neurostimulation system, if a patient’s skull does not have the structural integrity for the electrodes to be mounted and affixed, they are not a candidate for these therapies. This includes but is not limited to patients who are too young for their skull to be ossified, patients with prior neurotrauma, or patients with destructive skull lesions (eg, Paget disease).
These neurostimulation technologies are not identical; therefore, they can be used in conjunction. An increasing body of literature demonstrates the clinical scenarios when the placement of multiple neurostimulation systems may be warranted (42; 84).
In addition to these listed contraindications, one must consider the risks of the specific procedure to implant the devices, including but not limited to perioperative cardiovascular risk, local infection, and the prognosis of other comorbidities.
A primary goal of neuromodulation is to reduce seizure frequency. Just as some antiseizure medications have fortuitous side effects that benefit common comorbidities of epilepsy, there is some evidence that neuromodulation can address these comorbidities. As compared to resective or ablative surgery for epilepsy, the goal is not seizure freedom, although seizure freedom does rarely occur (5% to 16% of patients) (13; 51; 05; 61). For vagus nerve stimulation and deep brain stimulation, the mechanism of action is not to directly abort a detected seizure, although there is some evidence that vagus nerve stimulation can, and the use of auto-stimulation based on heart rate changes is intended to, abort seizures. Instead, the stimulation changes the underlying network to transition toward a state that is less likely to generate epileptic seizures.
This perspective is based on the finding that the initial reduction in seizure frequency is moderate and improves over time within individual patients and across patients. The initial reduction in seizure frequency is likely due to the stimulation itself, and the delayed response over years is thought to be from neuromodulation (14).
Improved reduction in seizure frequency with neurostimulation over time. Abbreviations: vagus nerve stimulation, anterior nucleus of the thalamus deep brain stimulation, responsive neurostimulation system. (Figure from: Dibue-A...
The caveat to this interpretation is that the duration of the randomized trials of each technology is short. After the blinded phase, providers can personalize the stimulation parameters based on the individual patient’s response and adverse effects. Similar to titration of an antiseizure medication, this personalization can balance reductions in seizure frequency with adverse effects or practical considerations like battery life. This personalization may be another cause for improved outcomes over time. Once placed, however, the surgical risk of removing neurostimulation devices frequently outweighs the benefit of removal. Therefore, if the device is ineffective, the device is typically turned off but not removed.
In addition, the indication for placement of vagus nerve stimulation, deep brain stimulation, and responsive neurostimulation system differ; therefore, the seizure reduction rates may not be comparable directly across technologies.
Vagus nerve stimulation. In the pivotal trials of vagus nerve stimulation (04; 63), the mean seizure reduction in the high-stimulation arm over the 12-week trial was moderate (25%), but mean seizure reduction improved to 56% after 5 years. Reported a different way, 44% and 65% of patients had at least a 50% reduction in seizure frequency after 1 and 5 years, respectively (29). In a meta-analysis including 3321 patients, seizures were reduced by at least 50% in about 50% of patients at last follow-up (21). This has been shown to be a cost-effective treatment for medication-resistant epilepsy (73).
Of note, vagus nerve stimulation may be used for both focal and generalized epilepsies, including Lennox-Gastaut syndrome (34). The response to vagus nerve stimulation may vary based on indication.
Deep brain stimulation. SANTE, the pivotal trail of anterior nucleus of the thalamus for epilepsy, demonstrated a 40% reduction in seizure frequency in the active stimulation arm and a 15% reduction in the off group. The median seizure reduction improved to 69% after implantation. This corresponded to 43% and 68% of patients experiencing at least a 50% reduction in seizure frequency after 1 and 5 years, respectively.
Responsive neurostimulation system. The seizure frequency improvement expected from a responsive neurostimulation system is similar to vagus nerve stimulation and deep brain stimulation. The pivotal trial showed a mean seizure reduction of 38% in the treatment and 17% in the sham (60). When all patients had stimulation, seizure frequencies were reduced by 50% and 66% at 1 and 6 years, respectively. This corresponded to 44% and 55% of patients having at least a 50% reduction in seizure frequency after 1 and 6 years, respectively (05; 61).
Although some patients note mood and cognition improvement associated with improved seizure control, there is not thought to be an independent effect of responsive neurostimulation system on comorbidities of epilepsy or other nonseizure aspects of quality of life.
In addition to its influence on seizures, the responsive neurostimulation system is an ultra-long-term intracranial EEG monitoring device. In selected patients, this function can guide future curative treatment of epilepsy. For instance, in patients with bilateral temporal lobe epilepsy or other multifocal epilepsy, bilateral responsive neurostimulation system can monitor seizure counts from each side to identify the lateralization asymmetry (43; 08). Long-term studies of these patients have demonstrated that short-term intracranial monitoring may not reflect the relative burden of seizures association with each temporal lobe. If a large portion of seizures are found with responsive neurostimulation system to come from a single temporal lobe that, if resected or ablated, would not generate disabling deficits in language or memory, these results can motivate unilateral temporal lobe epilepsy surgery (33).
The placement of each neurostimulation device is a surgical procedure with immediate surgical risks of infection and bleeding. Local bleeding is easily controlled when placing a vagus nerve stimulator, but the deep brain stimulation and responsive neurostimulation system devices involve placement of intracranial electrodes. To reduce the risk of intracranial hemorrhage, the surgical approach can be tailored specifically to a patient’s vascular anatomy to avoid this potentially fatal complication. Intracranial hemorrhage occurred in 4.7% of patients with a responsive neurostimulation system, but this has been reduced with robotic techniques (55; 07). Similarly, responsive neurostimulation system and deep brain stimulation were associated with a 5% and 13% risk of intracranial infection (74). In the deep brain stimulation trial, 8.2% of leads were misplaced (23; 74) but subsequent technological advances have improved the accuracy of lead placement. Less severe adverse events associated with placement of deep brain stimulation and responsive neurostimulation system included implant site pain (16%), headache (11%), and abnormal sensations (6%) (31).
After placement, the adverse effects of vagus nerve stimulation pertain to stimulation of other portions of the vagus nerve (12). Stimulation of the recurrent laryngeal nerve from high-intensity stimulation can result in hoarseness or coughing that is phase-locked with the duty cycle of the device. This can be remarkably common (hoarseness in 66% and coughing in 45% of early studies) (48). These adverse effects are direct results of stimulation parameters; therefore, stimulation can be titrated to maximize efficacy while minimizing adverse effects, similar to an antiseizure medication. Consequently, after 2 years of stimulation, hoarseness was reported in only 20% of patients (48). Injury to the recurrent laryngeal nerve rarely can result in vocal cord paralysis in 1% of patients, with its associated sequelae (48). Additionally, vagus nerve stimulation has been associated with central and obstructive sleep apnea; therefore, providers should be cautious when placing vagus nerve stimulation in patients with premorbid sleep apnea and monitor for sleep apnea after placement (99; 25).
Similarly, adverse effects after placement of a deep brain stimulator or responsive neurostimulation to the thalamus pertain to collateral stimulation of the thalamus. Due to the thalamus’ central role in sensation, 23% of patients reported paresthesia associated with stimulation (74). This paresthesia was not disabling. Due to the role of the thalamus and Papez circuit in memory, 13% of patients also reported memory dysfunction. Alteration of limbic activity also can influence mood, as 15% of patients in the active group in SANTE reported depression (2% of inactive group) (81). These neurocognitive and mood effects were not sustained at 5-year follow-up, and patients did not discontinue stimulation due to these adverse effects (87). In fact, the average patient with deep brain stimulation may experience small improvements in memory and cognition (68; 85; 53).
After placement of a responsive neurostimulation system, the targeted and responsive nature of the stimulation limits the adverse effects related to stimulation. Therefore, the long-term risks are similar to patients with other implanted devices like pacemakers.
There is a relative paucity of high-quality evidence for using neurostimulation in pediatric epilepsies. In part, this can be due to practical considerations that children’s brains and skulls continue to develop, potentially resulting in shifting of stimulator locations and other embedded hardware in deep brain stimulation and responsive neurostimulation systems. Although there is increasing clinical comfort in the placement of these devices in children, these technologies have not been FDA-approved in children (46; 78; 97; 41; 40). Of note, many common and widely accepted non-device treatments in pediatric neurology also have not sought formal FDA approval in children.
As a result, vagus nerve stimulation is the most well-studied neurostimulation technique in pediatrics, and it has been approved to age 4 years. Studies comparing efficacy of vagus nerve stimulation in pediatrics have found similar seizure frequency responses to adults (63; 18; 69; 37). Vagus nerve stimulation also has been effective for some medication-resistant pediatric epilepsies with severe effects on development including Lennox-Gastaut syndrome (34; 62).
Although the exact mechanism of action of each neurostimulation technology is not completely understood, some principles guide the understanding of why neurostimulation is effective.
Vagus nerve stimulation. Through the nucleus tractus solitarius and locus coeruleus, the vagus nerve is one of the major drivers of norepinephrine and serotonin within the brain, including to the thalamus and hippocampus (39). Due to the mechanism of vagus nerve stimulation involving the thalamus (32), there may be an overlap in the mechanism of deep brain stimulation and vagus nerve stimulation, but this is poorly understood and only studied in small samples (49). In animal studies, increases in norepinephrine in the hippocampus were associated with suppression of seizures and reduced seizure frequency (72). In humans, the P300 evoked potential is a marker for this increase in norepinephrine (66). It was found that patients whose seizures were reduced with vagus nerve stimulation had more change in P300. There are investigations to see if the change in P300 after noninvasive vagus nerve stimulation could predict future response to permanent vagus nerve stimulation, but these studies are forthcoming. A concern regarding this prediction of future response is that if one of the mechanisms of action of vagus nerve stimulation is long-term neuromodulation, then short-term noninvasive stimulation may not capture patients who would respond in the long term.
Although vagus nerve stimulation has been approved for about 25 years, multiple generations of devices have addressed limitations in prior devices. With the demonstration of the efficacy of closed-loop systems like responsive neurostimulation system, vagus nerve stimulation also has explored modification of stimulation based on patient monitoring. It was reported that 82% of patients with epilepsy have pre-ictal heart rate increases (17); therefore, modern vagus nerve stimulation devices have an option for heart rate monitoring to trigger additional stimulation (58).
Deep brain stimulation. Although there are multiple targets for deep brain stimulation implantation, the only FDA-approved target for epilepsy is the anterior nucleus of the thalamus. The centromedian nucleus of the thalamus may affect generalized-onset epilepsy, frontal lobe epilepsy within the projections of the centromedian nucleus, and Lennox-Gastaut syndrome (24; 90; 88; 51; 76; 44; 97; 75). Other targets include the hippocampus, subthalamic nucleus, inferior caudate nucleus, cerebellum, and parafascicular nucleus of the thalamaus (23; 60; 26; 80). As a reminder of neuroanatomy, the anterior nucleus of the thalamus is a core part of Papez circuit and includes projections to the frontal cortex, cingulate, and hippocampal formation (35). Bilateral high-frequency stimulation or lesions of the anterior nucleus of the thalamus suppressed the spread of seizures in the motor cortex and modified the levels of glutamate and GABA in the hippocampus. This is thought to be similar to the mechanism of action of some antiseizure medications (59). This suggests that although stimulation of the anterior nucleus of the thalamus may not cause seizure cessation, it may inhibit spreading of the seizure to symptomatic areas of the cortex (09).
Due to the broad distribution of the projections of the anterior nucleus of the thalamus, anterior nucleus of the thalamus-deep brain stimulation is effective for a broad range of hypothesized or demonstrated localizations of seizures. However, there are no clear methods to predict response to anterior nucleus of the thalamus-deep brain stimulation. There is emerging literature from essential tremor and Parkinson disease that individualized profiles of functional connectivity may predict response (93), but these have yet to be demonstrated in epilepsy.
Responsive neurostimulation system. Compared to vagus nerve stimulation and deep brain stimulation that influence neural activity throughout large cortex areas, the responsive neurostimulation system is local therapy targeted at each patient’s seizure focus. Direct cortical stimulation has been shown to abort after-discharges, which are a type of epileptiform discharges (70; 64). Based on these observations, the responsive neurostimulator system was designed as a closed-loop system that used limited intracranial EEG to monitor for epileptiform activity or the preictal period. When this abnormal activity is detected, the system automatically stimulates this local area to disrupt the seizure. In addition to this direct effect, longer-term stimulation may alter the neural network of the seizure by suppressing cortical synchronization distal from direct stimulation, resulting in both direct and indirect seizure reduction (79; 45).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Wesley T Kerr MD PhD
Dr. Kerr of University of Pittsburgh School of Medicine received consulting fees from Biohaven Pharmaceuticals and SK Lifesciences.
See Profile
John M Stern MD
Dr. Stern, Director of the Epilepsy Clinical Program at the University of California in Los Angeles, received honorariums from Ceribell, Jazz, LivaNova, Neurelis, SK Life Sciences, and UCB Pharma, and Xenon as advisor and/or lecturer.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jun. 02, 2026
Neuropharmacology & Neurotherapeutics
May. 11, 2026
Epilepsy & Seizures
May. 08, 2026
Epilepsy & Seizures
May. 01, 2026
Epilepsy & Seizures
Apr. 30, 2026
Epilepsy & Seizures
Apr. 20, 2026
Epilepsy & Seizures
Apr. 17, 2026
Epilepsy & Seizures
Apr. 13, 2026