












Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Central auditory disorder is a continuum of dysfunction involving the processing and interpretation of sounds, ranging from detecting the presence of simple sounds to comprehending complex auditory stimuli such as environmental sounds and music. This article reviews the range of clinical syndromes occurring in both acquired and developmental cases and their associated pathophysiology.
|
• Central auditory disorders are rare disorders that affect specific forms of auditory processing. | |
|
• Various distinct subtypes affect the processing of different auditory stimuli, including words (word deafness), environmental sounds (nonverbal auditory agnosia), and music (amusia). | |
|
• These subtypes usually co-occur but can occasionally be affected in isolation. | |
|
• Central auditory disorders usually result from damage in the temporal regions near the auditory and auditory association cortex. | |
|
• Diagnosis must be comprehensive due to the co-occurrence of other deficits and should include audiological as well as neuropsychological tests. |
Central auditory disorder refers to a dysfunction in the ability to recognize sounds, despite adequate hearing. There are several types of central auditory disorders, including the inability to recognize environmental sounds (nonverbal auditory agnosia), understand spoken language (word deafness, also called verbal auditory agnosia), process certain aspects of music (amusia), and recognize the identity of a speaker from the sound of their voice (phonagnosia). Whereas “pure” cases of these subtypes have been reported, patients usually exhibit mixed forms of two central auditory disorders. Central auditory disorders usually occur following temporal lobe lesions to the left or right hemisphere or both. Although central auditory disorders usually occur in conjunction with aphasias, they can occur in the absence of any deficits in language processing.
Central auditory disorders were first described in the 19th century, including reports by German physician Ludwig Lichtheim (1845-1923), French psychiatrist (1864-1947), and French neurologist Jules Dejerine (1849-1917), and German neurologist and psychiatrist Hugo Liepmann (1863-1925) (57; 87; 16; 17).
In 1898, German neurologist and psychiatrist Hugo Liepmann published a case study that provided early anatomical evidence for the "disconnection" theory of pure word deafness (54). Liepmann published the postmortem findings of a patient who had experienced symptoms of pure word deafness, including severe difficulty comprehending and repeating spoken language, despite having normal hearing and intact abilities to speak, read, and write. The autopsy revealed a hemorrhage in the patient's left temporal lobe. Crucially, this lesion was found to have interrupted two key neural pathways: (1) the left acoustic radiation, the pathway carrying auditory signals to the left hemisphere, and (2) transcallosal fibers connecting the auditory cortex in the right hemisphere to the language processing centers in the left hemisphere. The result was that neither the left nor the right hemisphere's auditory input could reach the brain's language areas for processing. Liepmann's findings supported the idea that word deafness was not a simple deficit in a single brain region but rather a "disconnection" between the language areas and the primary auditory cortex. This insight was most notably expanded by American behavioral neurologist Norman Geschwind (1926-1984) in 1965 (32), who proposed that lesions in strategic locations could prevent the language area (Wernicke's area) from receiving auditory stimulation from both sides of the brain.
Auditory agnosia can be divided into perceptual-discriminative and associative-semantic subtypes. Early research by Finkelnburg (1870) and Hughlings Jackson (1878) found a high instance of nonverbal auditory agnosia in patients with aphasia, suggesting an intimate relationship between processing verbal and nonverbal stimuli. Word deafness can also be divided into two subtypes: a temporal processing disorder and a phonemic processing disorder (04).
Historically, there has been considerable debate about the existence of truly “pure” cases of word deafness, with many studies failing to adequately assess processing in other domains (10). For instance, Yaqub and colleagues reported that their patient could “recognize and appreciate music,” but did not carry out formal testing (109). In that vein, using more controlled laboratory tests, Pinard and colleagues found that a patient who was previously classified as a “pure” case of word deafness (66) also had nonverbal auditory agnosia and amusia (72). However, as several cases that can be classified as “pure” do exist in the literature (67; 92; 35; 89), pure word deafness may be a real, but very rare, disorder.
|
• “Word deafness,” an auditory agnosia that affects only verbal material, presents as a profound deficit in the comprehension and repetition of spoken language but with preservation of language-processing abilities such as reading, writing, and speaking. | |
|
• Patients with word deafness often exhibit impaired processing of consonants, which are characterized by fast formant frequency transitions between 20 to 50 ms, whereas the processing of vowels, which are characterized by slow formant frequency transitions between 100 and 150 ms, is relatively spared. | |
|
• Nonverbal auditory agnosia refers to the inability to recognize environmental sounds. | |
|
• Generalized auditory agnosia refers to a generalized decrease in the ability to recognize both verbal and nonverbal sounds. |
Word deafness. “Word deafness” or “acquired impairment of acoustic-phonetic perception" is an auditory agnosia that affects only verbal material (ie, verbal auditory agnosia) and presents as a profound deficit in the comprehension and repetition of spoken language. Despite this, affected individuals retain other language-processing abilities, such as reading, writing, and speaking. Several studies have used psycholinguistic measures to characterize a phonemic-processing deficit in word deafness (79; 04; 68; 12; 41; 77). However, the observed deficits may also be due to an inability to process acoustic stimuli with rapid temporal resolution. Patients with word deafness often exhibit impaired processing of consonants, which are characterized by fast formant frequency transitions between 20 to 50 ms, whereas the processing of vowels, which are characterized by slow formant frequency transitions between 100 to 150 ms, is relatively spared (79; 04; 109; 76; 72; 92). The deficits exhibited in word deafness are not specific to speech sounds. For example, although healthy persons require around 1 to 3 ms between two clicks to perceive them as distinct, patients with word deafness require between 15 and 300 ms (01; 04; 97; 11; 35). This suggests a general auditory temporal processing deficit, although the relationship between the verbal and nonverbal temporal processing deficits associated with word deafness remains unclear. Slevc and colleagues found that training on rapid auditory events improved their patients’ ability to perceive rapid temporal differences for non-speech, but not for speech, sounds (89). Furthermore, patients with word deafness may also have difficulty recognizing auditory objects (34). There may be distinct subtypes of word deafness, each resulting from different patterns of lesions (04; 73). Patients with word deafness may have modality-specific dissociations with preservation of number-word processing, despite profound deficits in non-number-word processing (23); this may indicate that the distinction between number word and non-number word processing arises at a sublexical level of representations in speech perception.
Among 73 individuals with chronic residua of left hemisphere stroke, compared to an age- and education-matched control sample, 18% had impaired acoustic-phonetic perception overall, with 44% of these impaired on voicing, 26% on manner, 15% on place, and 14% on vowel discrimination (08). The most critical areas were the transverse temporal gyrus and adjacent medial belt cortex, the acoustic radiation, and the posterior superior temporal sulcus. There were notable differences between lesion correlates for the different types of discrimination, with place discrimination linked to the medial transverse temporal gyrus, vowel discrimination to the lateral transverse temporal gyrus and planum temporale, manner discrimination to the posterior planum temporale, and voicing discrimination to the posterior superior temporal sulcus.
Verbal auditory agnosia may occur as a familial inherited condition (50).
Nonverbal auditory agnosia. Nonverbal auditory agnosia refers to the inability to recognize environmental sounds. Two subtypes of nonverbal auditory agnosia have been proposed: patients with the perceptual-discriminative subtype are unable to analyze the frequency and/or time structure of sounds and so are unable to identify whether two consecutive sounds are identical, whereas patients with the associative-semantic subtype have an abnormal linkage of sound percepts with meaning and are impaired at audio-visual matching or naming. For instance, patients with the associative-semantic subtype are unable to match an environmental sound (eg, “moo”) with an associated visual picture (eg, a cow). Apperceptive forms of auditory agnosia often affect several domains (eg, music and environmental sounds) because of defects in the analysis of acoustic features that are relevant to multiple domains (15; 51).
Amusia and phonagnosia can also be similarly divided into apperceptive and associative subtypes (33). Amusia (often called “tone deafness”) and phonagnosia are disorders affecting a patient’s ability to perceive or understand specific aspects of music and voices, respectively.
Congenital amusia is a neurodevelopmental disorder resulting in impaired pitch perception and memory; however, deficits extend to the time domain, albeit with a smaller effect size, at least when the stimuli have clear pitch content, such as for tone sequences or music (101).
Strokes in the temporal lobe are known to cause acquired amusia (19; 82).
A 39-year-old man was evaluated after a single seizure episode. He was a competent trumpet player and singer, but 2 years before the seizure, he experienced an episode of headache, nausea, and vomiting, after which he developed difficulty appreciating music and carrying a tune (19). An MRI scan obtained after his seizure revealed encephalomalacia and gliosis within the right lateral temporal lobe with areas of hemosiderin deposition, suggesting that the episode 2 years previously was a hemorrhagic stroke. His standard neurologic and cognitive screening examinations were normal. However, on the online version of the Montreal Battery of Evaluation of Amusia, he scored 67% on the off-tune test, 88% on the off-beat test, and 71% on the out-of-key test, consistent with amusia.
A case of acquired amusia resulting from a left-sided focal brain lesion has been reported (82). A 21-year-old semi-professional musician with absolute pitch ("perfect pitch") suffered a left-hemispheric cerebral hemorrhage due to an arteriovenous malformation. One month after the hemorrhage, surgical treatment of the arteriovenous malformation resolved her aphasia and right upper limb clumsiness, but she lost her absolute pitch ability. Before the hemorrhage, she could dictate complex music that she heard, but after her surgery, she could no longer identify even a single tone. Neuropsychological assessments revealed a decreased retention span for auditory information, slight impairment of environmental sound and speech processing, difficulty in understanding the auditory presentation of numbers with more than four digits, and impairments of chord and timbre perception. A brain CT scan 9 months after the hemorrhage revealed low-density areas in the middle longitudinal fascicle, a major fiber connection running principally between the superior temporal gyrus and the parietal lobe, a region associated with language and auditory processing (61), including absolute pitch perception.
Generalized auditory agnosia. Generalized auditory agnosia refers to a generalized decrease in the ability to recognize both verbal and nonverbal sounds. Generalized auditory agnosia may also occur with selected preserved auditory abilities. For example, after a right temporoparietal stroke, a left-handed man lost the ability to understand both speech and environmental sounds, although he could match, describe, and sing melodies (63). He had normal hearing acuity and preserved reading and writing, but poor verbal comprehension (although slower speech, single-syllable words, and minimal written cues facilitated his verbal comprehension). He also had difficulty distinguishing tone sequences and discriminating between two clicks and short-versus-long tones, particularly in the left ear.
Patients with cortical deafness typically deny hearing any sounds, although they still respond to them (64).
Patients with auditory agnosia may have anosognosia for the deficit (51).
Deficits in higher-level segregation processes have been reported following a right hemisphere lesion affecting non-primary auditory cortex (36). A 33-year-old woman developed an unusual pattern of acquired central auditory deficits after an infarct in the right middle cerebral artery territory, causing damage to the part of the auditory cortex including the planum temporale, as well as involving the posterior insula and inferior parietal lobule, but sparing the medial portion of Heschl gyrus. She reported difficulty segregating speech from noise and segregating elements of music. The deficits were most pronounced for sounds presented to the left ear and affected the segregation of words, music, and more basic abstract stimuli. Clinical tests showed no evidence of abnormal cochlear function. Additional testing demonstrated difficulties with auditory segregation in her left ear that spanned multiple domains, including words-in-noise and music streaming. These symptoms were considered analogous to the visual symptom of simultaneous agnosia.
Central auditory dysfunction in Alzheimer disease. Central auditory dysfunction occurs as part of the dementing process in Alzheimer disease; detectable central auditory dysfunction may precede clinical dementia and might possibly be an early marker of incident dementia (31; 29; 28; 27; 81; 14; 99). Indeed, reduced executive functioning is associated with impairments in central auditory processing (30). Slight and moderate peripheral hearing loss markedly increases the risk of environmental sound recognition deficits, suggesting an interaction between peripheral hearing loss and Alzheimer disease pathology (14). Other studies have found an association between hearing loss in Alzheimer disease and loss of brainstem and cerebellar volume (58).
Cortical auditory disorders are generally enduring syndromes, although reversible or partly reversible cases have been reported, for example, in association with seizures, treatment of pineal tumors, and cerebral vasospasm associated with subarachnoid hemorrhage (75; 78; 103; 18; 42).
Therapeutic outcomes have been inconsistent for reasons that are not yet clear. Although some studies find that intensive therapy leads to little or no recovery (108), the outcome may depend on how soon after onset that therapy is initiated, with therapy provided soon after syndrome onset leading to the greatest benefit (37). There do not appear to be any negative consequences of therapy.
Case 1. Pure word deafness and tabes dorsalis (05). A right-handed 45-year-old man with a history of right ear deafness attributed to the explosion of a gun suddenly lost the use of his legs while walking on the street. This persisted "for a period," but he was later able to get about quite well, despite some ataxia. He continued at his lumber business until age 52, when he gave up work. At age 67, he experienced an "attack in which he lost the power of speech. …What he spoke could not be understood; wrong words were used in his sentences, and he could not understand what was said to him." He was admitted to a mental hospital in Michigan, where he was unable to understand anything spoken to him or to repeat words heard, but reacted quickly to sounds. Communication was only possible through gestures and writing. Although he initially had some difficulty reading written questions, with continued efforts, he understood them in about half of the tests. Over about 6 months, his anomia markedly improved so that he spoke with very few paraphasic errors, but his word deafness persisted. He read both printed and written words, with occasional paraphasic errors when reading aloud. Spelling was good except for occasional paraphasic errors. Spontaneous writing and drawing ability were retained, but he could not write from dictation, and he had some ataxia of his writing movements, which seemed characteristic of tabes dorsalis. Objects and colors were correctly recognized and named except for occasional paraphasic responses. He reported considerable pains in his legs and feet, especially at night (which was also attributed to tabes dorsalis).
|
[H]is usual reply, when one spoke to him, was, "I don't know what you say. I can't tell." He always gave good attention, and his attitude was one of perplexity at his inability to grasp what was said. In the examinations the questions were written or printed and always were read with understanding. His attention could be gained by noises made near him. When blindfolded, he quickly gave attention to the whistling of some one near and spoke of it as a noise. Similar reaction followed the ringing of a bell. The rattling of keys he called "a crackling." The imitation of the cry of a cat he spoke of as " singing. The barking of a dog was called a "noise.” Several tunes were whistled near his left ear; although he gave careful attention, none awakened any certain recognition. As in all attempts to recognize spoken words, his face had a troubled, puzzled look, and often he would shake his head at his inability to grasp the interpretation of sounds he heard. |
About 4 years after the onset of word deafness, he died suddenly of a ruptured aortic aneurysm (possibly also due to syphilis). At autopsy, gross examination of the brain showed severe atheromatous degeneration of the arteries at the base of the brain. Residua of old infarcts in both temporal lobes were evident, involving particularly the superior temporal gyrus and the transverse temporal gyrus (Heschel's gyrus). In the fresh brain, the first temporal convolutions were sunken inward bilaterally. The extent of the infarcted areas was determined more fully from serial sections of the fixed brain.
Coronal section of the brain, passing a little posterior to the beginning of involvement of the left superior temporal gyrus. (Left side) On the left side, the entire lower lip of the superior temporal gyrus is destroyed, inclu...
Coronal section of the brain, passing through about the middle of the transverse convolutions on the dorsal surface of the temporal lobe. (Left side) On the left side, the destruction of the middle temporal gyrus is more extens...
Coronal section of the brain, passing through the extreme posterior end of the transverse convolutions and insula, and through the geniculate bodies. (Left side) On the left side, the cortex of the ventral surface of the superi...
Coronal section of the brain, passing posterior to the insula, and through the extreme posterior end of the superior temporal gyrus. (Left side) On the left side, the lower surface of the superior temporal gyrus shows that the ...
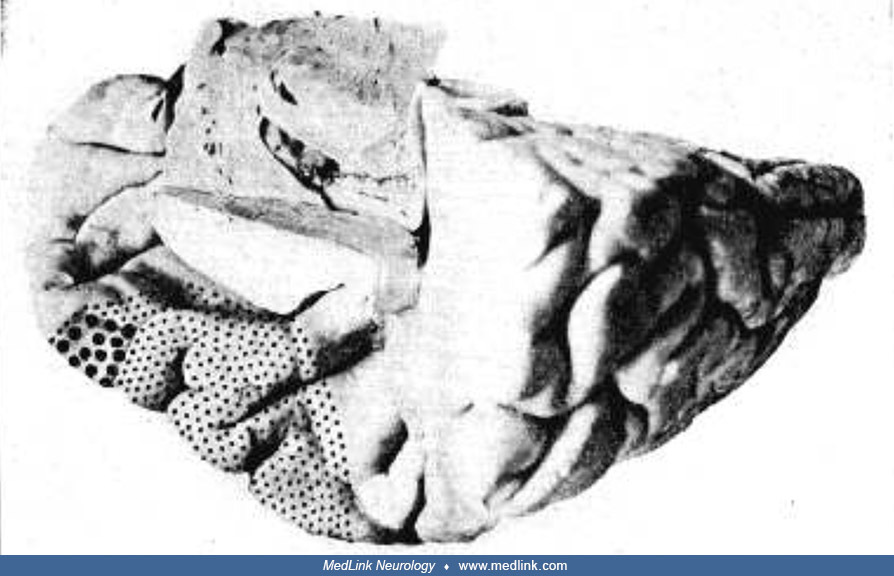
Left temporal lobe, dorsal surface. The large dots cover those areas where the cortex and underlying fibers were destroyed. The smaller dots cover areas of cortex beneath which fibers in the center of the convolution were destr...
Left temporal lobe, outer surface. The large dots cover those areas where the cortex and underlying fibers were destroyed. The smaller dots cover areas of cortex beneath which fibers in the center of the convolution were destro...
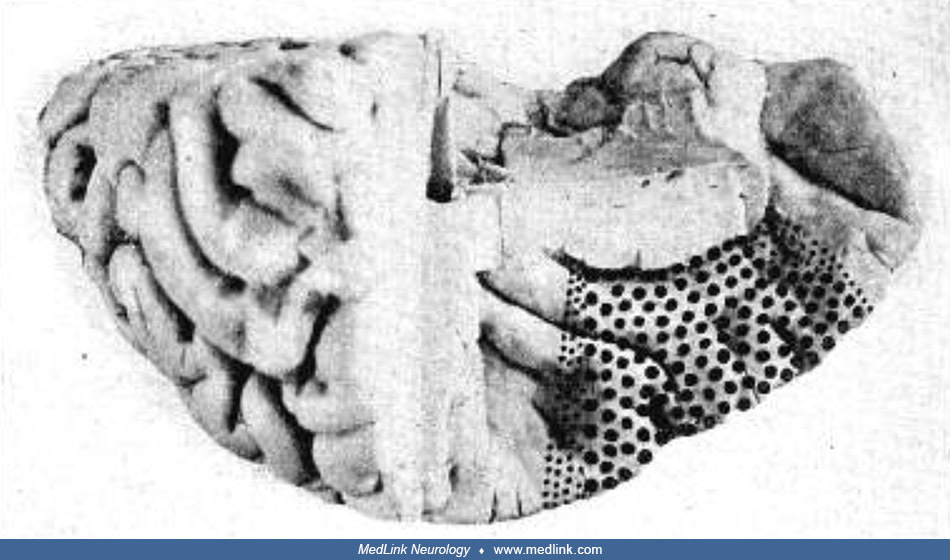
Right temporal lobe, dorsal surface. The large dots cover those areas where the cortex and underlying fibers were destroyed. The smaller dots cover areas of cortex beneath which fibers in the center of the convolution were dest...
Case 2. Nonverbal auditory agnosia (84). A right-handed 62-year-old man (patient “M”) developed the sudden onset of right-sided numbness and difficulty speaking. MRI showed an extensive lesion involving the left temporal and parietal cortex. Language function largely recovered since the infarct, with fluent speech and no measurable speech comprehension impairments, although he did have occasional word-finding difficulties (usually with long or infrequent words). However, even 12 years later, the patient exhibited a severe, persistent impairment in nonverbal auditory comprehension. At age 74, extensive audiological and behavioral testing was conducted to characterize M’s unusual neuropsychological profile. The patient exhibited persistent and severe auditory agnosia for nonverbal sounds in the absence of verbal comprehension deficits or peripheral hearing problems. Acoustical analyses suggested that his residual processing of a minority of environmental sounds might rely on his speech-processing abilities. The patients’ and healthy controls’ neural responses to verbal and nonverbal auditory stimuli were also examined using functional magnetic resonance imaging (fMRI). In the patient’s brain, contralateral (right) temporal cortex, as well as perilesional (left) anterior temporal cortex, were strongly responsive to verbal, but not to nonverbal, sounds, a pattern that stands in marked contrast to the controls’ data. This substantial reorganization of auditory processing likely supported the recovery of M’s speech processing.
Case 3. Apperceptive generalized auditory agnosia (15). A 48-year-old right-handed man became confused after a minor motor vehicle accident. He complained of nausea and a headache. On examination, his blood pressure was 230/120 mm Hg. He had a left central facial paresis with preserved limb power, left-sided visual and sensory neglect, left-sided hyperreflexia, and a left Babinski sign. An unenhanced head CT scan showed an extensive lobar hemorrhage involving the right temporal lobe with extension to the parietal lobe.
Four years later, he awoke with a loud noise (“like a spaceship landing”), vomited, and complained of headache and right arm numbness. On examination, his blood pressure was 156/95 mm Hg. His examination was otherwise significant for disorientation, diplopia on left gaze, and complete deafness. He became progressively more obtunded. An unenhanced head CT scan showed an isolated hemorrhage of the left inferior colliculus with obstruction of the cerebral aqueduct and secondary hydrocephalus.
He improved with the insertion of an intraventricular drain, and by discharge 2 weeks later, he still had no speech comprehension and instead experienced loud and disturbing bilateral subjective tonal tinnitus. His auditory acuity as measured by pure-tone audiometry gradually improved into the normal range over several months. Auditory brainstem-evoked responses, which did not change in the 4 years after the second event, showed a normal response to left-sided clicks, but absent waves IV and V to right-sided clicks, indicating damage to the corresponding generators of these waveforms in the superior olivary complex and inferior colliculus.
By 4 years after the second hemorrhage, he had regained some understanding of speech by reading printed books while listening to the corresponding audiobooks. Although he had excellent performance distinguishing words from nonwords (eg, bus vs. mus), he had a persistent and significantly impaired ability to distinguish minimal pairs of real words (eg, bear vs. pear), and he still could not recognize music and had an impaired ability to recognize environmental sounds. Psychophysical studies demonstrated that his most striking impairment was in the analysis of sounds with a time structure that evolved over time periods of from several to tens of milliseconds.
Central auditory pathways extend from the brainstem to the cerebral cortex.
After sound transduction by the inner hair cells in the cochlea, electrical information is transmitted to the brainstem by the auditory nerve. After initial ipsilateral processing in the dorsal and ventral cochlear nuclei and the nucleus of the trapezoid body, impulses project bilaterally (with a contralateral dominance) to the superior olivary complex and then through the lateral lemniscus to the inferior colliculi in the midbrain. From the inferior colliculi, there is a further partial decussation as the pathway projects to the medial geniculate nucleus before cortical processing in the primary auditory cortex in Heschl gyrus of the medial temporal lobe. Analysis of complex acoustic features progresses over longer time windows at successive stages of the central auditory pathway from brainstem to cortex and involves recruitment of increasingly distributed networks along the way (15). These central auditory pathways with multilevel decussations provide some degree of redundancy for processing speech: indeed, speech can be recognized even when the auditory input is markedly degraded, especially after a period of training, when facilitated by expectations, context, and cross-modal cues (eg, lip-reading) (15).
Central auditory disorders generally result from developmental abnormalities or acquired damage involving the temporoparietal regions, especially the superior temporal and auditory cortices (90; 69) but can result from brainstem and subcortical lesions (52). Bilateral lesions appear to be implicated in severe discrimination deficits (02; 64; 11; 98; 90). Unilateral right hemisphere lesions can lead to deficient discrimination with normal association (104; 22), deficient association with normal discrimination (91), or deficient association and deficient discrimination (25). Unilateral left hemisphere lesions have been implicated in deficient association (83), with normal discrimination (104), although most studies did not test discrimination due to a focus on language deficits.
In children, cortical auditory disorders are primarily developmental but may also be acquired secondary to head injury or tumor (60). Developmental auditory agnosia progressing to cortical deafness over decades has been reported (43). Other causes of central auditory disorders in children, which may persist into adulthood, include Landau-Kleffner syndrome, adrenoleukodystrophy, and mitochondrial disorders (eg, MELAS) (100; 18; 26; 55). Central auditory processing disorder is presumed to result from the dysfunction of processes and neural mechanisms dedicated to audition, although it may stem from a more generalized dysfunction, such as an attention deficit or a neural timing deficit, which affects performance across modalities (03). Because auditory processing disorders are enduring syndromes, such problems are likely to persist into adulthood.
A family has been reported with an autosomal dominant pattern of inheritance of progressive verbal auditory agnosia due to a GGGGCC repeat expansion in C9orf72 (50). The human C9orf72 gene is located on the short (p) arm of chromosome 9, open reading frame 72, hence, the name. The propositus was a 60-year-old right-handed man who presented with poor speech perception, which had been slowly progressive for 8 years. He had difficulty recognizing spoken single-syllable words but had no problem understanding complex written language. He had a heterozygous pathogenic variant carrying 160 hexanucleotide repeats in the C9orf72 gene. His deceased mother had similar symptoms that had progressed over 30 years, and his older brother and youngest sister experienced speech perception difficulty beginning in their early fifties. His symptomatic youngest sister had a heterozygous 159 repeat in the C9orf72 gene, whereas his asymptomatic younger brother had only a heterozygous two repeat. The propositus and his youngest sister had pronounced cortical thinning in the frontotemporoparietal areas.
In adults, central auditory disorders are usually acquired, most often from a unilateral or bilateral stroke involving the auditory cortices of the temporal lobes (95; 09; 70; 07; 96; 34; 44; 59; 90; 36; 51). Bilateral lesions may be staged/sequential or simultaneous. Central auditory disorders may also occur with head trauma, infectious encephalitis (particularly herpes simplex encephalitis), and with neurodegenerative diseases, such as Alzheimer disease (40; 24; 60; 74; 46; 49; 14; 106; 80).
One case of auditory agnosia was reported with sequential bilateral putaminal hemorrhages (94). Other causes of central auditory disorders in adults include paraneoplastic encephalitis, multiple sclerosis, and Moyamoya disease (62; 71). Cases in which adults display symptoms of central auditory disorders in the absence of brain abnormalities are most likely due to developmental causes.
Several studies have found a strong link between deficits in processing verbal and nonverbal stimuli. In a study investigating verbal and nonverbal comprehension deficits in the same aphasic patients, Varney found that impairments in environmental sound recognition were only seen in subjects with impaired verbal comprehension (102). Aphasic patients with intact verbal comprehension also had intact nonverbal comprehension. In an analysis of a large group of patients with unilateral brain damage, Schnider and colleagues found that the semantic deficits exhibited by the patients with left hemisphere damage were highly correlated with their scores on the Western Aphasia Battery (48; 85). Saygin and colleagues performed a large-scale neuropsychological and lesion-mapping study to compare the abilities of aphasic patients to match environmental sounds and complex linguistic phrases to associated pictures (83); they found that the aphasic patients were equally impaired in the verbal and nonverbal domains, showing extremely high correlations between accuracy (r = 0.74) and reaction times (r = 0.95). Using both lesion overlays and a novel lesion-symptom mapping technique called voxel-based lesion-symptom mapping (06), Saygin and colleagues found that damage to the posterior regions in the left middle and superior temporal gyri and to the inferior parietal predicted deficits in both speech and environmental sound processing. In fact, Wernicke area was more strongly associated with performance in the nonverbal than the verbal domain. The large overlap between regions for processing sounds in the verbal and nonverbal domains suggests that their processing shares neural resources. fMRI studies with normal controls have been consistent with this hypothesis (53).
Dissociations between the processing of verbal and nonverbal sounds, although rare, have been reported (84). For example, a right-handed man (patient “M”) suffered a left hemisphere stroke and had persistent difficulty with environmental sound comprehension, despite having largely recovered language function (84). fMRI revealed that the contralateral (right) temporal cortex, as well as the perilesional (left) anterior temporal cortex, were strongly responsive to verbal, but not to environmental, sounds. Thus, reorganization of auditory processing may explain the recovery of M’s language comprehension abilities.
The neuroanatomical locus of lesions causing word deafness is debated. Word deafness has been reported following bilateral lesions to the temporal lobes (68; 97; 109; 11; 76; 107; 78; 34), unilateral left temporal lobe lesions (79; 12; 67; 105; 92; 89), or lesions to subcortical areas (35). Most reported cases of word deafness had lesions to the bilateral superior temporal cortex (71% of 59 reviewed cases) (73). A case study reported the presence of word deafness following lesions to the superior temporal gyrus bilaterally (78); resolution of the lesions following medical treatment also resolved the patient’s word deafness. Cases of unilateral damage to the left temporal cortex (16 out of 59 reviewed cases) tend to extend deep into subcortical transcallosal projections, suggesting that word deafness is a “disconnection syndrome.” However, this claim has been directly tested in a word deafness patient with unilateral left temporal lobe damage (89): diffusion tensor imaging revealed that transcallosal white matter connections from the right auditory cortex to the left temporal lobe remained intact, undermining the claim that word deafness following unilateral left damage is necessarily due to a disconnection between auditory processing in the two hemispheres. In another case associated with a small stroke in the left temporal gyrus, selective impairment in auditory language processing was accompanied by intact processing of nonspeech sounds and normal speech, reading, and writing (59). Behavioral and neuroimaging results in this case could not be easily integrated into either a pure cortical or disconnection framework because damage to the primary auditory cortex in the left superior temporal gyrus was only partial, and the Wernicke area was not completely isolated from left- or right-hemisphere input (59). The discrepancy between speech and nonspeech sounds raised the possibility of selective damage to a language-specific left-lateralized network involved in phoneme processing (59).
Word deafness may occur as a stage in recovery from aphasia (13). A 29-year-old right-handed man presented with severe aphasia and multiple bilateral ischemic lesions in the distribution of the middle cerebral artery, including bilateral lesions to the temporal lobe, consistent with cardioembolic infarcts (13). His language function evolved from severe aphasia to an atypical form of word deafness, where auditory linguistic processing was impaired at the sentence level. Hearing was preserved. Using behavioral testing and multimodal neuroimaging, he was shown to have a predominant auditory linguistic deficit in sentence and narrative comprehension, with markedly reduced behavioral performance and absent brain activation in the language network exclusively in the spoken modality. He had near-unimpaired behavioral performance and robust brain activations in the language network for the linguistic processing of words, irrespective of modality.
Several studies have investigated the neuroanatomical locus of both acquired and developmental amusia. A meta-analysis of case and group studies indicated a network of superior temporal, temporoparietal, insular, and frontal areas as the neural substrate for the deficits associated with amusia (93). Most of these regions were in the right hemisphere. Developmental amusia has been linked with abnormalities in cortical thickness (38) and functional connectivity (39). Developmental amusics exhibited decreased frontotemporal connectivity and increased connectivity between the auditory cortex and the default mode network during the resting state (56).
Examples of generalized auditory agnosia from unilateral lesions are rare, but in one case, a 73-year-old right-handed man developed generalized auditory agnosia following a subcortical ischemic stroke involving the left acoustic radiation (95).
The prevalence of central auditory processing disorders in children is 2% to 3%, with a 2:1 ratio of boys to girls (21). Developmental amusia affects approximately 4% of the general population (45).
Cortical auditory disorders must be differentiated from disorders of hearing acuity, memory, attention, and language. Difficulty arises because these disorders are not mutually exclusive and may coexist to some extent in the same person. In adults, sensory aphasia, other language disorders, and dementia must be ruled out (65). For example, a person with a syntactical language disorder will have a comprehension deficit that is proportional to the complexity of the syntax of the spoken message. Thus, shorter, less complex sentences (eg, “The cat meowed”) will be more easily comprehended than longer, more complex sentences (eg, “The cat with the brown stripes sitting on a fence meowed”). Patients with disease or acquired injury of the frontal lobes from stroke, tumor, infection, hydrocephalus, etc. may also have an intrinsic inability to initiate behavior (ie, abulia). The inability to respond to the environment in any fashion should not be misconstrued either as a sensory aphasia or a form of cortical auditory disorder. One should also consider language barriers for non-native speakers. Because many children with central auditory processing disorder also have attention disorders, it is important to include attentional tests in their evaluation. Children with delayed or disordered overall language skills may present similarly to those with auditory processing disorders, although their comprehension difficulty may not originate from impaired auditory processing. The challenge for the clinician arises from the possible co-occurrence of language disorders and auditory processing disorders in the same patient.
The symptoms of dyslexia and other reading disorders also significantly overlap those of auditory processing disorders. Due to the phonological processing deficits seen across these disorders, differentiating between dyslexia and auditory processing disorders can be difficult (20; 88). Children with dyslexia and reading disorders perform significantly more poorly than controls on tasks of auditory encoding and processing. Both children and adults with these types of developmental learning difficulties can demonstrate auditory processing difficulties (20; 88).
|
• The diagnostic workup for central auditory disorders should include a hearing test and comprehensive language testing as well as assessments of attention, short-term memory for auditory information, and the ability to interpret specific auditory stimuli. |
The diagnostic workup for central auditory disorders should include the following, and may include testing by an audiologist, speech-language pathologist, and neuropsychologist. The spheres of assessment and tests are representative of those that could be used.
|
(1) Hearing test to document hearing loss and hearing acuity disorders | |
|
(2) Auditory processing and integration testing in children | |
|
(a) span of apprehension (test of auditory-perceptual skills) | |
|
(3) Pediatric comprehensive language testing – the Clinical Evaluation of Language Disorders IV (86) | |
|
(4) Adult comprehensive language testing – Boston Diagnostic Aphasia Examination; Western Aphasia Battery | |
|
(a) phonological awareness | |
|
(5) Attention | |
|
(a) selective | |
|
(6) Short-term memory for auditory information | |
|
(7) Interpretation of specific auditory stimuli, comparing input modes with output modalities to ensure that the main deficit is in the incoming auditory realm | |
|
(a) words | |
|
• Following a diagnostic workup, therapy should focus on the specific auditory processing deficit. | |
|
• Management should target compensation and restoration for the disorder. | |
|
• For children with cortical auditory processing disorders, special accommodations within the school environment are frequently suggested and may result in improved academic performance. |
Following a diagnostic workup, therapy should focus on the specific auditory processing deficit. Management should target compensation and restoration for the disorder. Speech-language pathologists most often treat patients with cortical auditory disorders, although audiologists and neuropsychologists may also treat such patients. The optimal length and intensity for therapy vary with syndrome severity and the patient’s response to treatment. Most clinicians will review and revise therapy goals and objectives, as well as session length and frequency, on a continual basis.
For children with cortical auditory processing disorders, special accommodations within the school environment are frequently suggested and may result in improved academic performance.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neurobehavioral & Cognitive Disorders
May. 20, 2026
General Child Neurology
May. 12, 2026
Infectious Disorders
May. 01, 2026
Neurogenetic Disorders
Apr. 30, 2026
General Child Neurology
Apr. 29, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026