


































































Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Galen (129-201 CE) correctly described the different functions of the three principal nerves supplying the tongue (lingual, glossopharyngeal, and hypoglossal nerves) and demonstrated their origin at the base of the brain (219).
Printed medical illustrations began in 1490 and, by the beginning of the 16th century, included representations of afferent connections from the special sensory organs to the brain (118). These were typically part of highly schematic diagrams of brain function representing the medieval cell doctrine, in which usually three “cells” or ventricles were assigned functions of sensory integration and imagination, cognition, and memory (119). Indeed, many early-16th-century woodcuts of the medieval cell doctrine show presumptive connections between the organs subserving the special senses, either with the most anterior cell or ventricle of the brain or with a specific portion of it--the sensus communis (ie, sensory commune, or common sense, a structure Aristotle had postulated is responsible for monitoring and integrating the panoply of sensations from which unified conscious experience arises) (118; 119; 120). A representation of the tongue and presumptive pathways to the brain are incorporated into many of these woodcuts (120; 120). These stereotyped 16th-century schematic images typically linked the tongue to an anterior cell or a portion of it. Such images linked the gustation via the tongue to "cells" of "ventricles" before the advent of more realistic images and schematics began to show the neural gustatory pathways beginning in the mid-sixteenth century.
Observational anatomy was largely lost from the time of Galen in the second century, and it became regimented and dogmatized with the scholasticism of the Middle Ages until a few anatomists began to seriously challenge Galen beginning in the 16th century. Most notably, Flemish anatomist Andreas Vesalius (1514-1564) provided much greater realism with the publication of his de Humani corporis fabrica (1543).
Vesalius depicted dissection of the face, isolating the tongue, as part of one of his elaborate depictions of the famous “musclemen.”
The mandible has been split in the midline and separated. (Source: Vesalius' de Humani corporis fabrica [1543]. Courtesy of the U.S. National Library of Medicine, Bethesda, Maryland. Woodcut print edited by Dr. Douglas...
Vesalius also separately made a schematic of the cranial nerves, including innervation of the tongue, but the pathway for taste sensation had not been determined by this point.
Even after Vesalius championed a return to observational anatomy, the medieval cell doctrine and its associated representation of the olfactory pathways persisted well into the 19th century, even if it was gradually moved to the fringes of medical thought (120).
By the 18th century, anatomists were working to realistically represent anatomical structures, as epitomized by the copperplate engravings of Dutch Golden Age physician, anatomist, poet, and playwright Govert Bidloo or Govard Bidloo (1649-1713).
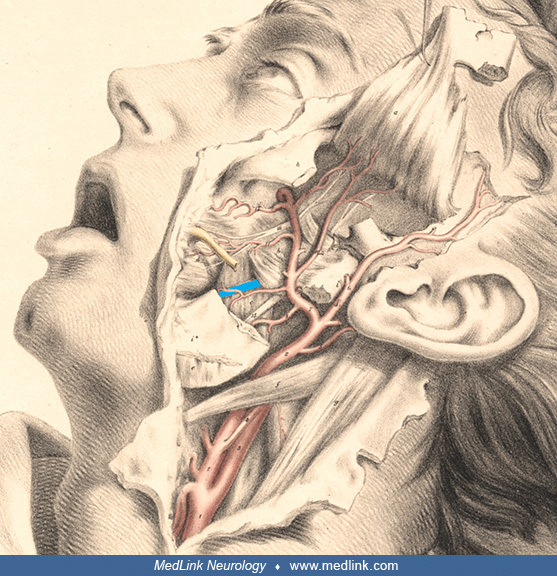
This continued into the 19th century, with amazingly realistic and detailed colored lithographs, including the outstanding examples of Irish-born English anatomist Richard Quain (1800-1887) and German anatomist Christian Wilhelm Braune (1831-1892) in his topographical anatomy atlas (1867-1872).
The lingual nerve passes through the cheek and underneath the anterior border of the mandible. The lingual nerve has been colored blue here for ease of visualization. (Source: Quain R. The anatomy of the arteries of the human b...
The structure of the tongue surface was first described in 1609 by Italian anatomist Giulio Cesare Casseri (1552-1616), and then in 1665 by Italian physician-anatomist Lorenzo Bellini (1643-1704), who published the observations made by Italian biologist, physician, and pioneering microscopist Marcello Malpighi (1628-1694) the previous year (101; 219). After the discovery of taste buds in fish by German zoologist and comparative anatomist Franz von Leydig (1821-1908) in 1851, German anatomist and zoologist Franz Eilhard Schulze (1840-1921) suggested in 1863 that they were chemosensory structures. Nineteenth-century studies focused on cytologic features and nerve supply. By the late 19th century, physicians were readily examining tongues for clinical clues to their patients' illnesses, and this became the subject of numerous caricatures.
"Le docteur. _ Ah! ... si vous avez mangé du raisin tout s'explique: vous avez alors la maladie des pommes de terre dont le remède est encore inconnu ... tranquillisez-vous!" [“The doctor. _ Ah! ... if you have eaten grapes, ev...
The patient holds green spectacles in his left hand. The woman holds a cup with a spoon. Lettering: Der patient (Das Vertrauen). A patient (Confidence). (Source: F. Silber, Berlin, Germany. Courtesy of the Wellcome Library, Lon...
|
• Patients with gustatory symptoms generally report diminution or absence of gustatory sensation (hypogeusia or ageusia, respectively) and forms of distorted gustation (parageusia). | |
|
• Except in unusual circumstances, hypergeusia is a subjective sensation of hyperacuteness of gustation. | |
|
• There is no evidence that pregnant women or migraineurs experience an objective increase in gustatory sensitivity. | |
|
• When patients report alterations in the quality of gustation in response to a tastant (ie, parageusias), the perceptions are almost universally unpleasant, a condition referred to as aliageusia (the perception of unpleasant taste from something that usually tastes pleasant). | |
|
• Aliageusias may involve the perception of fecal or rotten tastes (cacogeusia) or chemical or burned tastes (torqugeusia). | |
|
• Complaints of impaired “taste” are often symptoms of olfactory dysfunction because much of the flavor of a meal derives from olfactory stimulation. Indeed, the complex sensory experience of “flavor” during the consumption of foods and drinks cannot be constructed simply from combinations of the basic taste qualities (sweet, salty, sour, bitter, and umami or savory). | |
|
• Chemosensory deficit may be the first symptom, a "sentinel symptom," in patients with COVID-19, but there is wide variation in the proportion of cases in which this is reported to occur. | |
|
• Presbygeusia (literally “elderly gustation” or “old-age gustation”) is the gradual loss of gustatory abilities that occurs in most people as they grow older. | |
|
• Clinically significant gustatory loss is common in the elderly but frequently unrecognized, partly because deficits typically accumulate gradually over decades--indeed, self-reported gustatory impairment significantly underestimates prevalence rates obtained by gustatory testing. |
Patients use various expressions to describe disorders of taste or gustation (Table 1) (117).
|
Category |
Term | ||
|
Disturbance of perception (any) |
Dysgeusia | ||
|
Alteration of quantity |
Absent |
Ageusia | |
|
Decreased |
Hypogeusia | ||
|
Normal |
Normogeusia | ||
|
Increased |
Hypergeusia | ||
|
Alteration of quality |
Distorted (any) [general term] |
Parageusia | |
|
Specific distortions | |||
|
1 |
Any unpleasant distortion of taste |
Aliageusia | |
|
2 |
"Abhorrent, obnoxious," typically fecal or putrid |
Cacogeusia | |
|
3 |
"Twisted": chemical, metallic, bitter, salty, or burned |
Torqugeusia | |
|
4 |
Inappropriate chemosensory quality of consistent nature1 |
Heterogeusia | |
|
Hallucination2 |
Phantageusia | ||
|
| |||
Patients with gustatory symptoms generally report diminution or absence of gustatory sensation (hypogeusia or ageusia, respectively) and forms of distorted olfaction (parageusia). Except in unusual circumstances, hypergeusia is a subjective sensation of hyperacuteness of gustation. There is, for example, no evidence that pregnant women or migraineurs experience an objective increase in gustatory sensitivity.
When patients report alterations in the quality of gustation in response to a tastant (ie, parageusias), the perceptions are almost universally unpleasant, a condition referred to as aliageusia (the perception of unpleasant taste from something that usually tastes pleasant). Aliageusias, for example, may involve the perception of fecal or rotten tastes (cacogeusia) or of chemical or burned tastes (torqugeusia).
The terminology for alterations in the quality of a gustatory perception (eg, cacogeusia, torqugeusia) can also be employed with hallucinated odors (phantageusias); thus, one can speak of a "cacogeusic phantageusia" for the hallucination of a fecal taste or a "torqugeusic phantageusia" for the hallucination of a burned taste (82).
In addition, complaints of impaired “taste” are often symptoms of olfactory dysfunction because much of the flavor of a meal derives from olfactory stimulation. Indeed, the complex sensory experience of “flavor” during the consumption of foods and drinks cannot be constructed simply from combinations of the basic taste qualities (sweet, salty, sour, bitter, and umami or savory).
Dysgeusia in COVID-19. Disorders of smell and taste are more common among individuals with COVID-19 than those with influenza (28). Chemosensory clinical symptoms are present in at least half of patients with COVID-19 (05; 20; 146; 147; 169; 59; 85). In one study of 922 participants, 20% reported ageusia, 5% reported hypogeusia, and 32% reported hypogeusia and dysgeusia (05).
The risk of COVID-19-associated smell or taste disturbance has progressively fallen with successive waves of infection with the Alpha, Delta, Omicron K, Omicron L, Omicron C, and Omicron B variants, based on their peak intervals (170); consequently, since the Omicron waves, smell and taste disturbances have been of less predictive value in the diagnosis of COVID-19 infection (170).
A chemosensory deficit may be the first symptom--a "sentinel symptom"--in patients with COVID-19, but there is wide variation in the proportion of cases in which this is reported to occur (39; 40; 41; 66; 100; 102; 161; 178; 38; 164). A meta-analysis of eight studies involving 11,054 patients with COVID-19 reported that olfactory and gustatory symptoms appear before general COVID-19 symptoms in 65% and 54% of the patients, respectively, based on European, United States, and Iranian data (181). However, a systematic review of 17 studies found the onset of dysosmia and dysgeusia occurred 4 to 5 days after other symptoms of the infection and that these chemosensory symptoms typically improved after 1 week, with more significant improvements in the first 2 weeks (183).
New-onset chemosensory dysfunction is also common in patients with symptomatic COVID-19 after complete vaccination. In one study of 153 such patients, approximately half reported associated rhinorrhea, which is a much higher proportion than in unvaccinated cases (211).
Available reports present conflicting data on whether COVID-19 severity is associated with either the degree of gustatory dysfunction or the prognosis for recovery of gustation, but multiple reports suggested that chemosensory symptoms were most common among those with milder presentations of COVID-19 (25; 43; 168; 186; 85). Few studies used validated psychophysical tests to specifically address gustation, and subjective reporting does not correlate well with more objective psychophysical findings, often leading to overestimation of subjectively impaired taste (85).
Psychophysical testing showed significantly reduced intensity perception and identification ability for both taste and smell functions in patients with COVID-19 (31), although some studies using quantitative testing found olfactory disturbances in nearly all subjects during the acute infection phase, whereas taste or chemesthetic deficits were low (65; 147). Curiously, psychophysical data produced substantially lower estimates of dysgeusia after COVID-19, perhaps because of misinterpretation of impaired retronasal olfaction as gustatory dysfunction (86). Smell and taste loss in COVID-19 are closely associated, although a minority of individuals can experience one or the other (32; 59). Most patients with taste dysfunction after COVID-19 did not have true taste dysfunction, but rather perceived altered flavor sensations associated with olfactory dysfunction (147). The taste of salt may be less severely affected than other taste qualities (32), whereas complete loss of bitter taste was the most prevalent specific ageusia (174).
Chemosensory impairment may be persistent (17; 20; 146; 147; 169), even 1, 2, or 3 years after mild COVID-19 (17; 20; 147; 193), although chemosensory recovery from the Omicron BA.1 subvariant was more favorable than that after the first wave of the pandemic (19). In a prospective observational study, measuring the prevalence of altered sense of smell or taste at follow-up and their variation from baseline, on 403 consecutively assessed adult patients who tested positive for SARS-CoV-2 RNA by polymerase chain reaction during March 2020, 66% reported an altered sense of smell or taste at baseline, whereas 14%, 7%, and 5% reported such alterations at 6 to 24 months, 2 years, and 3 years, respectively (20). Late improvement was possible: of the patients who still experienced smell or taste dysfunction 2 years after COVID-19, 28% and 38% recovered completely and partially, respectively, at the 3-year follow-up (21). Olfactory dysfunction is most likely to persist after 1 year, whereas objectively measured taste dysfunction has typically recovered by that time (193).
Gustatory hallucinations (phantageusias) can occur through irritative (eg, epilepsy, migraine) or "release" (eg, ageusia or hypogeusia) mechanisms (42).
Phantageusia and phantosmia are associated with decreased brain GABA levels (127). In a study of olfactory and gustatory hallucinations in 28 normal volunteers and 19 patients with persistent phantageusia or phantosmia, GABA levels in several CNS regions (ie, the cingulate, right and left insula, and left amygdala) were lower in patients before treatment than in normal volunteers and were the only biochemical changes found (127). After treatment that inhibited sensory distortions, CNS GABA levels increased to levels at or near normal, consistent with functional remission of these symptoms.
Epileptic olfactory and gustatory hallucinations. Olfactory hallucinations often occur with a lesion in the inferior and medial parts of the temporal lobe, whereas gustatory hallucinations can occur in temporal lobe disease with lesions in the insula and parietal operculum (110). Of course, epileptic discharges can also spread to these areas from areas that are proximate or intimately connected with the temporal lobe, operculum, and insula (97). For example, a 4-year-old boy had ictal fear as his primary epileptic manifestation, associated with complex visual and gustatory hallucinations, oral automatisms, and pain in the left leg; investigation showed that his seizures resulted from the rapid spread of epileptic discharges from his frontal lobes to the right anterior temporal region (97).
Of 718 patients investigated for intractable epilepsy with stereo-electroencephalography (SEEG), 30 (4%) manifested gustatory hallucinations as part of their seizures (77). Gustatory hallucinations, which occurred as one manifestation of parietal, temporal, or temporoparietal seizures, resulted from disorganization of the parietal or Rolandic operculum. Electrically induced seizures, which included a gustatory hallucination as an ictal event, occurred mainly with stimulation of the hippocampus and amygdala.
Selected cases with gustatory hallucinations indicate the range of lesions responsible:
|
Temporal lobe epilepsy following seronegative limbic encephalitis. A 25-year-old man with drug-resistant temporal lobe epilepsy following seronegative limbic encephalitis related to non-Hodgkin lymphoma experienced musicogenic right temporal seizures triggered by listening to rock music; the seizures were characterized by déjà vu, piloerection, and gustatory hallucinations (150). | |
|
Third-ventricular colloid cyst. A 46-year-old man experienced prolonged episodes of olfactory and gustatory hallucinations that abruptly resolved with stereotaxic aspiration of a third-ventricular colloid cyst (58). | |
|
Partial status epilepticus, resulting from glioblastoma multiforme involving the hippocampus and amygdala. In one patient, new-onset olfactory and gustatory hallucinations were a presenting feature of partial status epilepticus resulting from a previously unrecognized glioblastoma multiforme involving the hippocampus and amygdala (29). | |
|
Schizencephaly. A patient with schizencephaly and normal intelligence had frequent simple partial epileptic seizures with visual, auditory, and gustatory hallucinations (15). |
In contrast to individuals with "purely temporal" epilepsies, those with "temporal plus" epilepsies--characterized by seizures involving a complex epileptogenic network including the temporal lobe and neighboring structures (eg, orbito-frontal cortex, insula, frontal and parietal opercula, and temporo-parieto-occipital junction)--more frequently have gustatory hallucinations, rotatory vertigo, and auditory illusions at seizure onset (12). Indeed, the most frequently reported auras among individuals with "purely temporal" epilepsies are gustatory hallucinations, vestibular illusions, laryngeal and throat constriction, and atypical somatosensory symptoms (perioral and bilateral acral paresthesias, etc.) (08).
Although déjà vu is common and qualitatively similar whether it occurs as an epileptic aura or as a normal phenomenon, patients with epilepsy are more likely to report olfactory and gustatory hallucinations, prior fatigue and concentrated activity, associated derealisation, fear, and physical symptoms such as headaches or abdominal sensations (215).
Although epileptic presentations of phantageusia are typically "irritative" hallucinations in Cogan's dichotomy of hallucinations, some cases of postictal phantageusia may instead represent "release" hallucinations akin to a Todd paralysis (42). For example, a 32-year-old man with epileptic seizures due to a grade 1 astrocytoma of the right sylvian region experienced gustatory hallucinations as a postictal symptom (07).
Olfactory and gustatory hallucinations in Parkinson disease. Bannier and colleagues reported that olfactory hallucinations occurred in 10% of the 87 patients with Parkinson disease in their series (11). Olfactory hallucinations were rare, short-duration, unpleasant odors that were not frightening and were recognized by the patients as hallucinations (like their visual hallucinations typically are recognized as unreal). Compared with controls, patients with Parkinson disease and olfactory hallucinations had olfactory impairment of both detection and identification, but there was no difference in their olfactory abilities compared with patients with Parkinson disease but no olfactory hallucinations.
Solla and colleagues similarly reported that olfactory hallucinations occur frequently in patients with Parkinson disease, particularly in women, and are often concomitant with visual and auditory hallucinations without any association with olfactory impairment (200). In a sample of 273 patients, 141 with Parkinson disease and 132 healthy controls of similar age, olfactory hallucinations were found in 11% of those with Parkinson disease and none of the controls (200). Among patients with Parkinson disease and olfactory hallucinations, 3% also had gustatory hallucinations (200). Visual or auditory hallucinations and female gender were independent predictors of olfactory hallucinations (200).
Other studies have reported lower frequencies of olfactory and gustatory hallucinations in patients with Parkinson disease (225). Holroyd and colleagues studied 98 patients with Parkinson disease, among which there were 26 with visual hallucinations, only one of whom (1% of the total) was reported to have concomitant gustatory hallucinations, whereas none apparently had auditory, tactile, or olfactory hallucinations (90). None of the patients, therefore, had any unimodal hallucinations other than visual.
Olfactory and gustatory hallucinations in migraine. Olfactory and gustatory hallucinations occur occasionally in migraineurs (09; 151). Among 46 new female referrals for migraine headache, 15% reported olfactory or gustatory hallucinations and distortions of body image as part of most migraine attacks (151).
Olfactory and gustatory hallucinations in psychotic disorders. Among patients with schizophrenic or schizoaffective disorder, auditory hallucinations are by far the most common, followed by visual hallucinations and then by tactile and olfactory or gustatory hallucinations (153).
There are subgroups with psychosis that experience a higher frequency of olfactory and gustatory hallucinations. A subgroup of schizophrenia, characterized by premorbid eating disorders (ie, eating disorders preceding fulfillment of diagnostic criteria for schizophrenia), is more common in women and is associated with a higher frequency of gustatory hallucinations (136). In a sample of 36 patients with first-episode psychosis reporting nonauditory hallucinations and 31 controls from the same clinical population without nonauditory hallucinations, dissociation remained significantly associated with nonauditory hallucinations after adjusting for childhood sexual abuse, other types of childhood adversity, and emotional distress (132).
Tactile, olfactory, and gustatory hallucinations are often thought to be rare in primary psychotic illness. In a descriptive study of a large cohort of psychotic patients with schizophrenia, schizoaffective disorder, or bipolar I disorder, olfactory and gustatory hallucinations were present in 15% and 4% of the total sample, respectively (Table 2) (128). Hallucinations in the various sensory modalities occurred in patients across these diagnoses, and no modality-specific pattern is characteristic of a particular type of psychotic disorder. Tactile, olfactory, and gustatory hallucinations were associated with somatic delusions, delusions of control, thought broadcasting, earlier age at onset, and a lifetime history of depressive episodes (128).
|
Schizophrenia (n=133) |
Schizoaffective (n=101) |
Bipolar disorder (n=186) |
Total Sample (n=420) | |
|
Auditory |
76% |
68% |
27% |
52% |
|
Visual |
24% |
29% |
16% |
22% |
|
Tactile |
20% |
21% |
8% |
15% |
|
Olfactory |
17% |
23% |
8% |
15% |
|
Gustatory |
7% |
2% |
2% |
4% |
|
Total |
79% |
73% |
41% |
61% |
|
| ||||
In another cross-sectional study of 766 patients with adult psychotic disorders across the diagnostic categories of schizophrenia (n = 227), schizoaffective disorder (n = 210), and bipolar I disorder (n = 329), 26% had visual hallucinations (36). Visual hallucinations were independently associated with hallucinations in other modalities, history of a suicide attempt, catatonic behavior, and specific types of delusions (ie, delusions of control and religious, erotomanic, and jealousy delusions) (36).
In individuals with schizophrenia, referential or control delusions promote the generation or maintenance of olfactory hallucinations, which are associated with and frequently co-occur with hallucinations in other modalities, particularly somatic, tactile, and gustatory hallucinations (116). Olfactory hallucinations are also associated with social anxiety and depression in schizophrenics, with self-smells being particularly associated with self-deprecation (116).
Among 86 outpatients with DSM-IV delusional disorder, those with comorbid Axis I disorders (47%) had a fairly specific collection of additional features, which included more common olfactory and gustatory hallucinations, personality psychopathology, somatic delusions, and suicide risk (46); they also had more severe psychopathology, particularly in terms of emotional dysregulation. In contrast, those with delusional disorder without psychiatric comorbidity (ie, "pure" delusional disorder; 53%) had worse overall neurocognitive performance, mainly affecting working memory (46).
Among 43,339 patients with schizophreniform or affective disorder diagnoses, 0.54% had tactile hallucinations, 0.24% had olfactory hallucinations, and 0.06% had gustatory hallucinations (13). Tactile, olfactory, and gustatory hallucinations were associated with schizophreniform diagnosis, worse disorder severity, male gender, and black ethnicity (13). In fully adjusted multivariate statistical models, tactile and olfactory hallucinations were independently associated with prior mention of use of non-benzodiazepine hypnotics (“Z drugs,” such as zolpidem or zaleplon) (13).
Patients have been reported who were mistakenly thought to suffer from depression but actually had unnoticed drug-induced dysosmia and dysgeusia (126). Among individuals that superficially appear depressed, it is essential to distinguish (1) those with dysosmia or dysgeusia with reactive depressive manifestations and (2) those with primary neuropsychiatric illness with olfactory or gustatory hallucinations (126).
Disorders of the chemosensory senses, smell and taste, are usually less disabling than disorders of the other special senses (vision and hearing). Nevertheless, chemosensory impairment adversely affects quality of life, and self-reported changes in flavor perception is a predictive factor for involuntary weight loss (159; 44). Taste and smell alterations are common in pediatric cancer patients due to chemotherapy (71; 212) and are associated with impaired nutritional status 6 months after chemotherapy (71).
Chemosensory dysfunction in COVID-19. COVID-19-associated chemosensory loss has a substantial negative impact on health-related quality of life beyond mere inconvenience (40; 55). Indeed, altered taste and smell with COVID-19 may cause severe disruption of daily living and quality of life that impacts psychological well-being, physical health, and interpersonal relationships (26; 40; 55). Affected individuals variously reported reduced desire and ability to eat and prepare food; weight gain, weight loss, and nutritional insufficiency; reduced emotional well-being; and impaired intimacy and social bonding (26; 68). "Reduced enjoyment of food" was the most common complaint (87%) in one study (40).
Among healthcare workers who contract COVID-19, olfactory and gustatory loss was associated with emotional distress, anxiety, and depression (52). Moreover, the psychological impact tends to persist even after recovery from the disease, adding to the risk of work-related distress (52).
The loss of smell and taste improves at a high rate after disease onset in most series (16; 66; 95; 138; 171; 25; 155; 179; 202; 207; 32; 38). However, a substantial proportion (approximately 4% to 5%) of patients with COVID-19 might develop long-lasting changes in their sense of smell or taste (206). Rapid recovery of olfaction is observed in two thirds of COVID-19-infected people, but the remainder experience a slower pattern of recovery (109). By 1 month, almost all patients have a significant improvement in olfactory threshold and odor discrimination but not odor identification (95; 155). The recovery of gustation typically occurs before the recovery of olfaction (74). The mean duration of anosmia is 7 days (104), but many of these cases progress from anosmia to hyposmia and parosmia.
Nevertheless, some series report that between one third and one half of patients have persistent qualitative changes in olfaction (parosmia or phantosmia), typically accompanied by qualitative disorders of gustation (parageusia and phantageusia) (149; 57; 67; 91; 192; 135). Some experience long-term deficits with no self-reported improvement at 6 months (57; 67; 91). Persistent parosmia is common even in those who report at least some recovery of olfactory function (91).
Persistent loss of smell or taste was not associated with persistent SARS-CoV-2 infection (16).
Age younger than 40 years and presence of nasal congestion at the time of COVID-19 infection were associated with improved rates of smell recovery, whereas difficulty breathing at the time of COVID-19 infection and prior head trauma were associated with worsened rates of recovery (41).
Presbygeusia. Presbygeusia (literally “elderly taste” or “old-age taste”) is the gradual loss of taste that occurs in most people as they grow older. The elderly have higher detection and recognition thresholds for taste than younger individuals, and taste sensitivity is further compromised by medications and comorbid medical problems (187; 204). Healthy elderly people have higher thresholds for each taste category (sweet, sour, salty, bitter, and umami or savory), particularly for bitter substances, with the average threshold for taste rising fourfold in the elderly (62; 187; 204). The changes in taste sensitivity make food seem relatively tasteless and contribute to difficulties in complying with dietary regimens (such as a low-salt diet for the management of hypertension) (187).
Chemosensory deficits reduce the pleasure of eating and represent risk factors for nutritional deficiencies and nonadherence to dietary regimens (53; 187). Lower olfactory perception in elderly women is associated with lower interest in food-related activities (such as cooking and eating a varied diet), a lower preference for foods with either a predominantly sour or bitter taste (such as citrus fruits) or pungency (such as horseradish), a higher intake of sweets, and a lower intake of low-fat milk products (53). Nutritional adequacy should be assessed in elderly women with a self-reported or measured difficulty perceiving odors or flavor (53). Flavor-enhanced food positively affects food intake and can increase the enjoyment of food and improve the quality of life for elderly patients with chemosensory deficits (187). Flavor enhancements with simulated flavors can amplify odor intensity, improve the enjoyment of eating, and facilitate adequate nutrition in the elderly with hyposmia (but not anosmia) (187). Simulated flavors are mixtures of odoriferous substances that are either extracted from natural substances (as with concentrated orange juice or vanilla) or synthesized de novo (as with vanillin in artificial vanilla).
Burning mouth syndrome. Burning mouth syndrome is an uncommon painful intraoral disorder affecting mostly postmenopausal women (204). The pain is described as an uncomfortable, constant burning sensation in the mouth, affecting particularly the anterior tongue, palate, and lips. This may be associated with paresthesias or a numb sensation in the mouth or on the tip of the tongue, as well as a sensation of dry mouth and increased thirst without associated mucosal lesions. Approximately two thirds of affected individuals report dysgeusia or persistent abnormal taste sensations (which might be termed “palingeusia”) (204). Most have alterations in sensations of saltiness, and some have alterations in sweet, sour, and bitter tastes (204). The persistent taste sensations are most often described as bitter or metallic (torqugeusia) (204). Risk factors include older age, female gender, menopausal status, status as a “supertaster” (with a high density of lingual papillae), upper respiratory infection, previous dental procedures, medications, traumatic life events, and stress (23). The etiology of burning mouth syndrome appears to be multifactorial; various conditions have been associated with it, including menopause, endocrine disorders (such as diabetes and hypothyroidism), nutritional disorders (such as deficiencies of iron, zinc, thiamine, riboflavin, pyridoxine, folate, and cobalamin), xerostomia (such as from Sjögren syndrome or other causes), medications (especially anticonvulsants and angiotensin-converting enzyme inhibitors), gastroesophageal reflux, postnasal drip, oral candidiasis, tongue plaque, removable dentures, halitosis, and mouth irritation (such as from overbrushing of the tongue, mouthwash, or acidic drinks) (204; 180). Many cases, however, are idiopathic. Burning mouth syndrome can be disabling and may cause various complications, including anorexia, weight loss, insomnia, irritability, depression, anxiety, and impaired socialization. The treatment depends on the etiology (if it can be identified). For primary (idiopathic) burning mouth syndrome, saliva-replacement products, oral rinses, clonazepam (applied topically or taken orally), gabapentin, selective serotonin reuptake inhibitor antidepressants, alpha-lipoic acid, B vitamins, and capsaicin have all been employed, with variable but limited success (although high-quality trials are lacking) (145; 224).
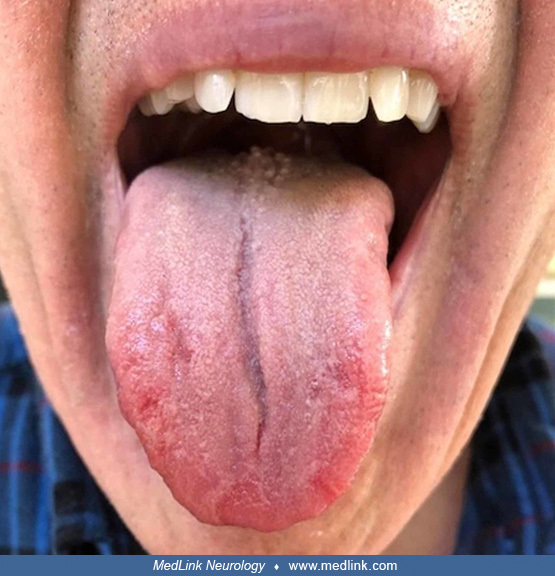
Psoriatic dysgeusia and burning mouth syndrome. Oral psoriasis is an overlooked cause of dysgeusia. Manifestations can include patches of red skin with yellow or white edges, sores, peeling skin on the gums, pustules, pain or burning (especially when eating spicy foods), fissured tongue, geographic tongue (red patches on the tongue resembling islands on a map), and swollen or infected gums.
A geographic tongue is often asymptomatic but may be associated with a burning sensation, especially with eating hot, acidic, and spicy foods. Photograph by Dimitrios Malamos on November 23, 2015. (Creative Commons Attribution ...
Clinical vignette. A 66-year-old patient presented to an oral medicine clinician with a 10-week history of “burning tongue, red at the tip, white bumps in the rear,” dysgeusia, and difficulty speaking (60). His physician had previously placed him on a nystatin topical rinse for 1 week without resolution. He had replaced his usual toothpaste with one that was supposedly free of the surfactant sodium lauryl sulfate. Eating spicy foods was not problematic. Pain was negligible on waking up but increased as the day progressed, although it did not interfere with his sleep. The patient was taking apixaban for atrial fibrillation, atorvastatin for cholesterol, lansoprazole for gastric reflux, fexofenadine and azelastine for seasonal allergies, and a vitamin D supplement. He had no known drug allergies. On examination, the anterior dorsal tongue was erythematous, but there was no lymphadenopathy or other abnormalities. He was referred to an allergist for food hypersensitivity, and the evaluation studies were negative. His symptoms seemed to improve after he eliminated paprika from his diet but then recurred.
(Source: Ferris WJ, Mikula S, Brown R, Farquharson A. Oral psoriasis of the tongue: a case report. Cureus 2019;11[12]:e6318. Creative Commons Attribution [CC BY 3.0] License, https://creativecommons.org/licenses/by/3.0.)
On biopsy, periodic acid-Schiff (PAS) staining showed candidiasis, and H&E staining at medium magnification demonstrated elongated rete pegs (ie, the epithelial extensions that project into the underlying connective tissue in both skin and mucous membranes, also known as rete processes or rete ridges).
(H&E, medium magnification) (Source: Ferris WJ, Mikula S, Brown R, Farquharson A. Oral psoriasis of the tongue: a case report. Cureus 2019;11[12]:e6318. Creative Commons Attribution [CC BY 3.0] License, https://creativecomm...
The papillary connective tissue was noted to show lymphocytic inflammation and dilated blood vessels approximating the epithelial margins. Lower magnification showed marked collections of neutrophils seen in the parakeratin, consistent with Munro microabscesses (ie, a cardinal sign of psoriasis where they are seen in the hyperkeratotic and parakeratotic areas of the stratum corneum). He was treated with oral fluconazole 100 mg daily for 2 weeks, but his condition further deteriorated. A fungal DNA identification culture and sensitivity assay was negative for candida, aerobic, anaerobic, and acid-fast bacilli.
(Source: Ferris WJ, Mikula S, Brown R, Farquharson A. Oral psoriasis of the tongue: a case report. Cureus 2019;11[12]:e6318. Creative Commons Attribution [CC BY 3.0] License, https://creativecommons.org/licenses/by/3.0.)
At this point, a consultant determined that the patient had previously been treated for cutaneous psoriasis that had begun in his teens with dry, red, blotchy lesions of the legs, trunk, and face. Calcipotriene ointment (a vitamin D analogue) for the trunk and leg lesions and desonide (a topical steroid) for the facial lesions had been sufficient to control the condition. The patient’s lesions subsequently resolved with a topical dexamethasone elixir rinse, supporting a diagnosis of oral psoriasis. The steroid rinse was discontinued as a challenge, and in 2 weeks, the erythema and sensitivity returned. On resuming the topical steroid regimen, the lesions again resolved. A biological therapeutic was considered but deferred as the more conservative topical was effective.
(Source: Ferris WJ, Mikula S, Brown R, Farquharson A. Oral psoriasis of the tongue: a case report. Cureus 2019;11[12]:e6318. Creative Commons Attribution [CC BY 3.0] License, https://creativecommons.org/licenses/by/3.0.)
(Source: Ferris WJ, Mikula S, Brown R, Farquharson A. Oral psoriasis of the tongue: a case report. Cureus 2019;11[12]:e6318. Creative Commons Attribution [CC BY 3.0] License, https://creativecommons.org/licenses/by/3.0.)
Cerebrovascular disease. Taste disorders are common, although underrecognized, in acute stroke, with hypogeusia occurring in approximately 30% of cases (79). Stroke-related hypogeusia is typically unilateral with brainstem strokes (114) but is strictly unilateral in only a minority of patients with cerebral infarction (79). Risk factors for stroke-associated gustatory loss include male gender, greater stroke-related functional impairment, dysphagia, and anterior circulation location, especially involving the peri-opercular frontal lobe (79). Interruption of the gustatory pathway in the brainstem usually occurs with lateral pontine stroke (114). Thalamic hypogeusia may be associated with a cheiro-oral syndrome (182). Stroke-related damage to the left insula causes an ipsilateral deficit in taste intensity but a bilateral deficit in taste recognition, suggesting that the left insula is dominant for taste recognition (166; 140). Stroke-associated dysgeusia and hypogeusia often persist, whereas other deficits improve and can contribute to unwanted weight loss poststroke (140; 61).
Alpha-synucleinopathies. Although less common than olfactory defects, impaired taste appreciation is also present in about a quarter of patients with clinically defined Parkinson disease, independent of age, disease severity, or olfactory deficits (191). Given the sparing of the first- and second-order taste neurons in Parkinson disease, a disorder of taste may indicate involvement of primary or secondary gustatory cortical areas, although confounding by drug effects (such as anticholinergic drugs) and changes in salivary constitution are possible (191).
Substance abuse. Taste detection and taste recognition thresholds of individuals with substance use disorder are impaired, and the threshold scores for sour, salty, sweet, and umami taste recognition are significantly lower compared with non-users (209).
Myasthenia gravis. Among 1688 patients with myasthenia gravis enrolled in a disease registry, 6% had taste disorders (210). Taste disorders were significantly more common in women, and those with severe symptoms, refractory myasthenia gravis, or thymoma-associated myasthenia gravis, and were less common with ocular myasthenia gravis (210). Taste disorders often occurred after the onset of myasthenia gravis and often responded to myasthenia gravis treatments (210).
Oncology. Taste alterations are common with antineoplastic drugs and in pediatric patients undergoing hematopoietic stem cell transplantation (185).
|
• Gustation, like disorders of the other special senses, can be conveniently divided into conductive, sensorineural, and central disorders, where (1) conductive disorders involve transmission of the sensory stimuli to the sensory receptors (usually but not always by impeding transmission); (2) sensorineural disorders involve dysfunction of the sensory receptors or conduction of signals from the sensory receptors to the brain; and (3) central disorders involve dysfunction of processing sensory information within the CNS, particularly within the brainstem and cerebrum. | |
|
• Age-related gustatory loss (presbygeusia) is common in the elderly and results from normal aging, certain diseases (especially Parkinson disease and dementia with Lewy bodies), medications, surgical interventions, and prior environmental exposures. | |
|
• The elderly have higher gustatory thresholds, perceive suprathreshold tastes less intensely, and are less able to discriminate tastants or recognize and identify common tastants. | |
|
• COVID-19-related chemosensory dysfunction results primarily from a loss of function of olfactory sensory neurons and taste buds, mainly caused by infection, inflammation, and subsequent dysfunction of supporting non-neuronal cells in the mucosa. |
The tongue and taste buds. Modern anatomical illustrations show the details of lingual anatomy clearly with labeling.
The tongue was very well illustrated at the beginning of the 19th century with clear anatomic drawings showing the angle of vallate papillae near the back of the tongue by German physician-anatomist Samuel Thomas von Sömmerring (1755-1830) (201). Still, even though some papillae were noticed and drawn, their function was not understood for about 60 years.
Taste buds in humans were first independently described in 1868 by Swedish physician Otto Christian Lovén (1835-1904) and German anatomist Gustav Schwalbe (1844-1916) (134; 189; 190).
They are bulb-shaped structures composed of about 50 to 120 bipolar cells. The average person has about 10,000 taste buds that are replaced approximately every 2 weeks.
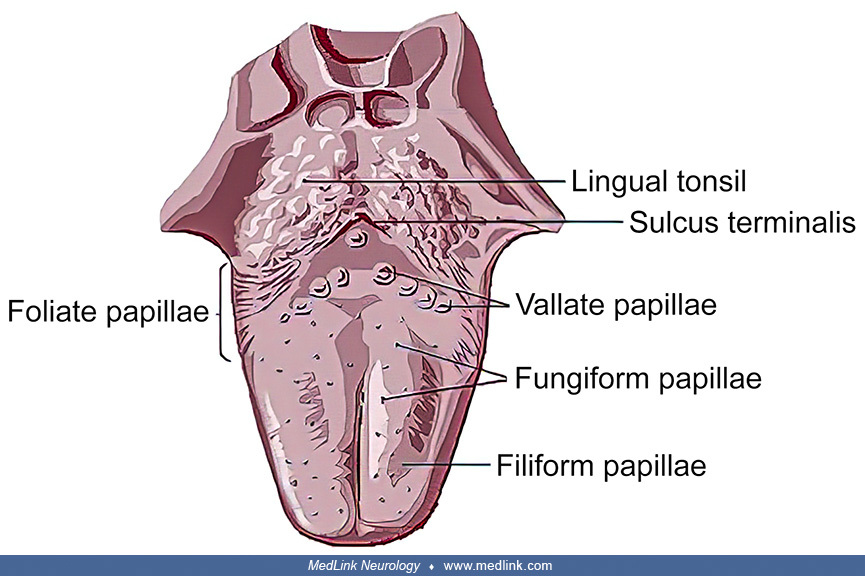
Lingual papillae are small structures on the upper surface of the tongue that give it a rough texture. The four types of papillae on the human tongue have different structures and are accordingly classified as circumvallate (or vallate), fungiform, filiform, and foliate.
The root of the tongue, the "lingual tonsil," is free of papillae and instead has mucous glands and lymphatic tissue. The large vallate papillae are positioned in a V-shaped array at the back of the tongue. The sulcus terminans is located posterior to the vallate papillae and separates the tongue from the lingual root. From the vallate papillae posteriorly to the tip of the tongue, the tongue is covered in filiform and fungiform papillae.
All lingual papillae except the filiform papillae are associated with taste buds.
Foliate papillae (without taste buds) were first reported in humans by German-born Dutch anatomist Bernhard Siegfried Albinus (originally Weiss; 1697-1770) in 1754 (04): they are located bilaterally along the posterolateral margins of the tongue surface and consist of parallel rows of ridges (folia) and valleys, which lie adjacent to the lower molar teeth (88).
Fungiform papillae have taste buds at the apex, whereas vallate and foliate papillae have taste buds arranged in arrays along the epithelial walls of the papillary trenches.
There are also extra-lingual taste buds embedded in the surface mucosa without papillae (eg, on the soft palate, oropharynx, epiglottis, and the upper esophagus).
Legend: (A) isolated taste bud, from whose upper free end project the ends of the taste cells; (B) supporting or protecting cell; (C) taste cell. (Source: Hollis EW. A Text-Book in General Physiology and Anatomy. New York, Cinc...
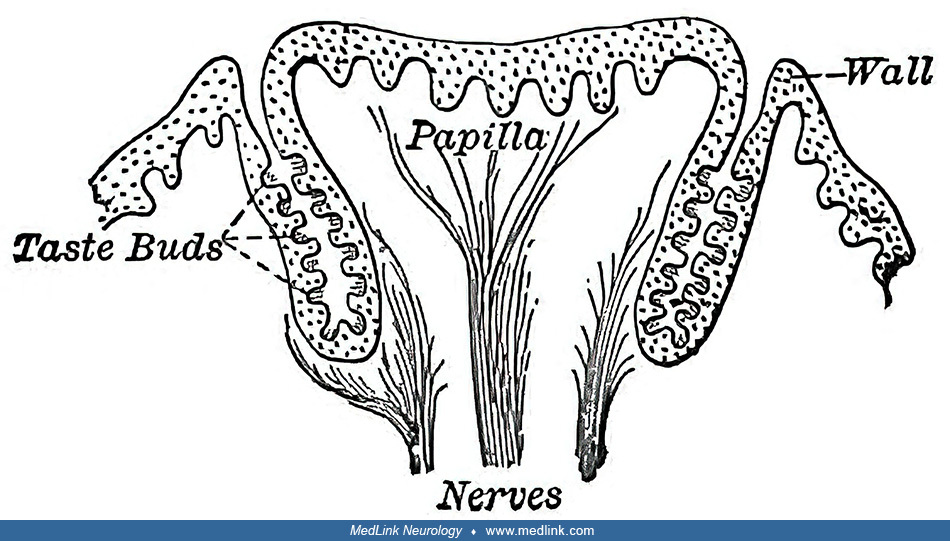
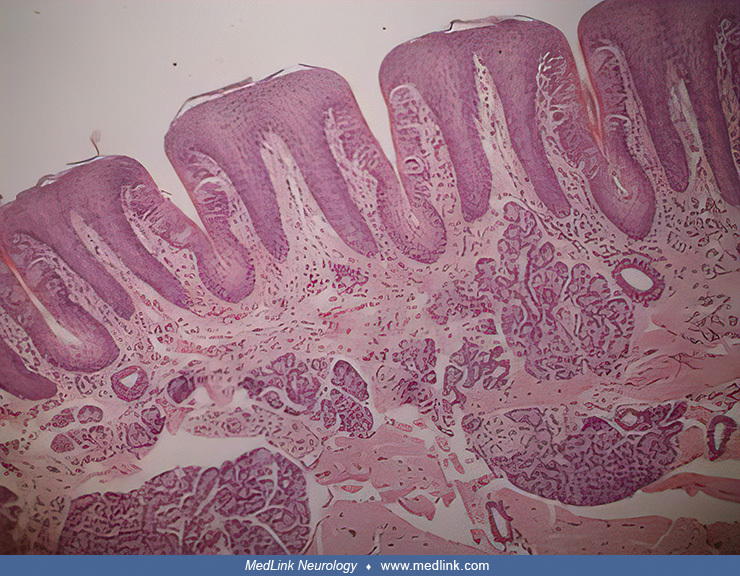
The foliate papillae (papillae foliata) encompass numerous projections arranged in several transverse folds on the lateral lingual margins just anterior to the palatoglossal fold. (Source: Plate 1021 in: Gray H. Anatomy of the ...
(x18) "The papillae foliatae, or gustatory lamellae of Turner, of the human tongue, offer an excellent area in which to study the taste-bulbs. They consist of five to eight irregular folds or ridges, with rounded or flattened c...
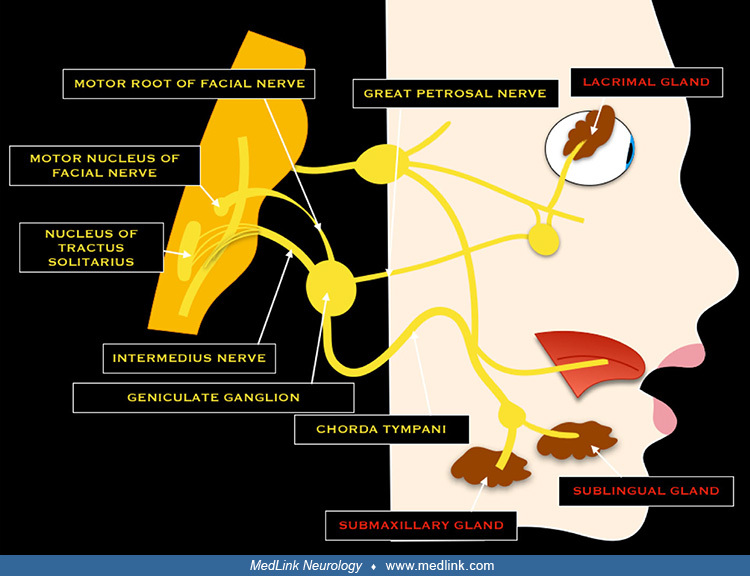
Sensorineural pathways. Three cranial nerves carry taste signals to the brainstem: the facial nerve (via the chorda tympani from the anterior two thirds of the tongue and via the greater petrosal nerve from the soft palate), the glossopharyngeal nerve (from the posterior one third of the tongue), and the vagus nerve (from a small area of the epiglottis).
The glossopharyngeal nerve mediates taste in the back third of the tongue. (Source: Gray H, Spitzka EA. Anatomy: Descriptive and Applied. Philadelphia and New York: Lea & Febiger, 1913. The original figure has been...
The chorda tympani nerve arises from the mastoid segment of the facial nerve, carrying afferent special sensation from the anterior two thirds of the tongue via the lingual nerve (a sensory nerve that arises from the mandibular division of the trigeminal nerve) as well as efferent parasympathetic secretomotor innervation to the submandibular and sublingual glands.
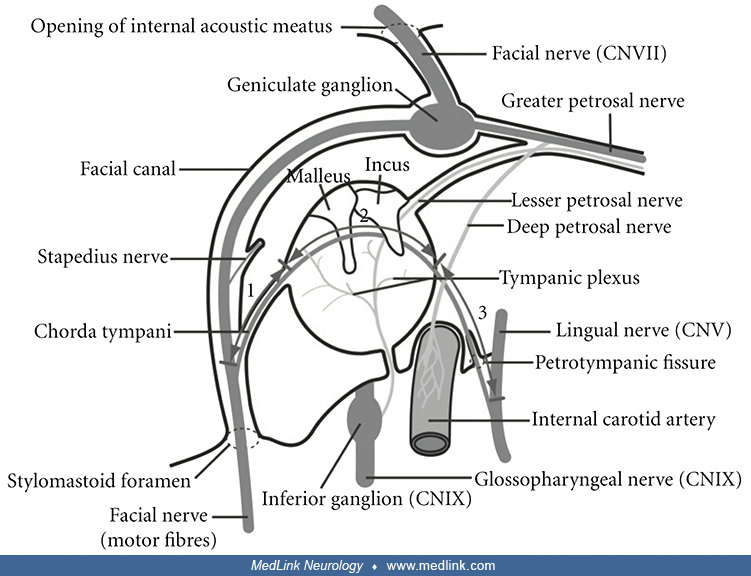
The chorda tympani nerve exits the cranial cavity through the internal acoustic meatus along with the facial nerve.
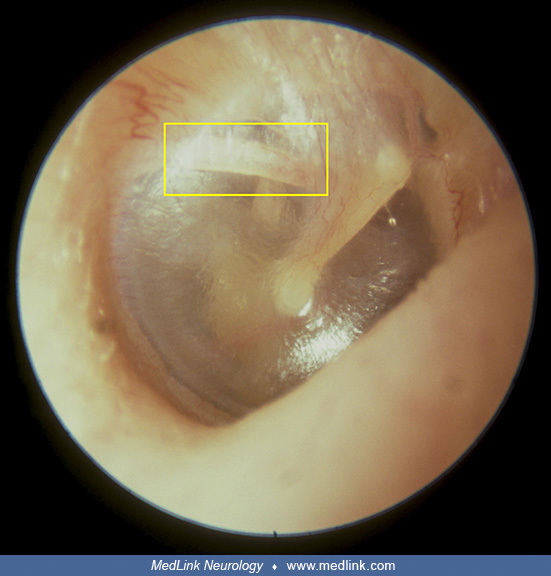
The chorda tympani nerve then accompanies the facial nerve inside the facial canal but separates before the stylomastoid foramen and travels through the middle ear, crossing behind the upper portion of the tympanic membrane on the medial surface of the neck of the malleus between the malleus and the incus.
Legend: (a) short process of the incus; (pl) fold of the posterior pouch of the tympanic membrane; (ct) chorda tympani nerve; (h) head of the malleus; (n) niche in the outer wall of the tympanic cavity, in the squama. The fold ...
The chorda tympani nerve exits through the petrotympanic fissure and descends in the infratemporal fossa, where it joins the larger lingual nerve (a branch of the mandibular nerve) (130).
Each ganglion has three roots: the motor root is indicated by broken lines, the sensory root by dotted lines, and the sympathetic root solid lines. Mesial view, left side.
Legend: (c.a.) carotid artery; (c.g.) cil...
Section 1: mastoid process. Section 2: tympanic cavity. Section 3: submandibular fossa. (Source: Liu L, Arnold R, Robinson M. Dissection and exposure of the whole course of deep nerves in human head specimens after decalcificat...
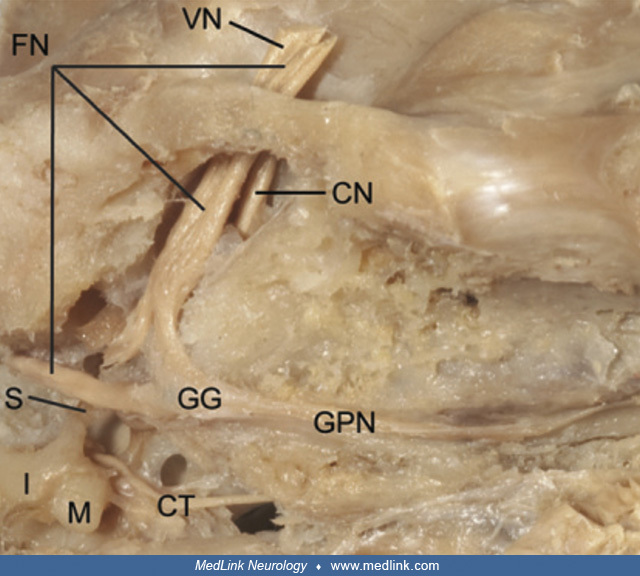
Legend: (VN) vestibular nerve, (FN) facial nerve, (S) stapes, (I) incus, (M) malleus, (CT) chorda tympani nerve, (GG) geniculate ganglion, (GPN) greater petrosal nerve, (CN) cochlear nerve, (PTF) petrotympanic fissure. (Source:...
Legend: (FN) facial nerve, (I) incus, (M) malleus, (CT) chorda tympani nerve, (GG) geniculate ganglion, (GPN) greater petrosal nerve, (PTF) petrotympanic fissure, (LN) lingual nerve, (TM) tympanic membrane, (SF) stylomastoid fo...
Special sensory (taste) fibers extend from the chorda tympani to the anterior two thirds of the tongue via the lingual nerve. Fibers of the chorda tympani also travel with the lingual nerve to the submandibular ganglion, where preganglionic fibers of the chorda tympani synapse with postganglionic fibers that innervate the submandibular and sublingual salivary glands.
The cell bodies of the facial nerve associated with taste are located within the geniculate ganglion; the axons of these taste neurons enter the brainstem at the pontomedullary junction and travel caudally to the medulla oblongata, where they synapse at the nucleus solitarius.
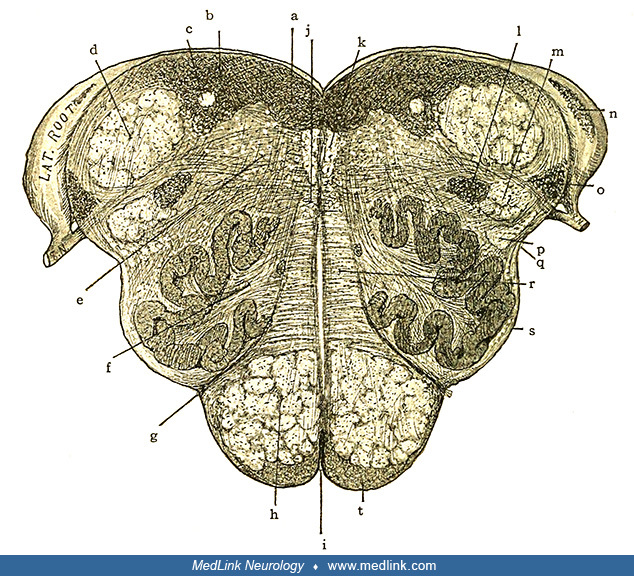
Motor nuclei in red; primary terminal nuclei of afferent nerves in blue. Optic and olfactory centers are omitted. (Source: Gray H, Spitzka EA. Anatomy: Descriptive and Applied. Philadelphia and New York: Lea & Febi...
The nucleus solitarius is in the area marked "IX and X" on the figure. Optic and olfactory centers are omitted. (Source: Gray H, Spitzka EA. Anatomy: Descriptive and Applied. Philadelphia and New York: Lea & Febige...
Despite anatomical evidence for the bilateral symmetry of the nerves innervating the tongue and the oral cavity (195), and despite focused studies of this issue beginning in the latter part of the 19th century and continuing to the present, the neural pathways to the gustatory cortices continue to be contested and remain unclear (70; 98; 194; 63; 64; 108; 01; 184; 197; 76; 160; 94). There is no consensus on whether the afferent taste information projects to the ipsilateral or contralateral gustatory cortex, or both, and at what level of the nervous system any crossing occurs (94).
One proposed framework for the taste pathways is as follows (195). Information derived from taste-responsive cranial nerves converges on the rostral division of the nucleus tractus solitarius (rNTS) in the medulla, the principal visceral-sensory nucleus of the brainstem. Fibers projecting from the rNTS join the central tegmental tract and synapse directly in the parvicellular part of the ventroposterior medial nucleus of the thalamus (VPMpc). Efferent fibers from VPMpc project to the primary gustatory cortex, the region of cerebral cortex responsible for the perception of taste and flavor; it is comprised of the anterior insula (of the insular lobe) and the frontal operculum (of the frontal lobe). The primary gustatory cortex sends projections to the central nucleus of the amygdala, and from there, gustatory information reaches the lateral hypothalamus and midbrain dopaminergic regions. The primary taste and olfactory cortices both project to a secondary gustatory cortex in the caudolateral orbitofrontal region. The lateral hypothalamus also projects to the orbitofrontal cortex, so taste responses can be modulated by satiety states. Finally, cortical taste areas send afferents to the rNTS and the gustatory parabrachial nuclei (PBN) of the pons, providing a means for top-down modulation of gustatory processing at the brainstem.
Available evidence indicates that (1) there is a relationship between handedness and gustatory processing; (2) the results of various studies are not consistent for different tastants; (3) asymmetries are evident in the CNS processing of gustatory information; (4) for right-handed individuals, there is a predominantly ipsilateral flow of taste information in the left-side pathway, especially for saltiness; (5) for right-handed individuals, taste information from the right oral cavity projects to the insula bilaterally; and (6) there is a direct input from the primary gustatory cortex in the left insula to the secondary gustatory cortex (94).
The left insula is predominantly activated by gustatory imagery tasks (106). In addition, the middle and superior frontal gyri participate in the generation of gustatory hallucinations but are not activated by gustatory perception; these regions of the frontal cortex may participate in "top-down" control of retrieving gustatory information from long-term memory (106).
Types of dysgeusia. Gustation, like disorders of hearing and the other special senses, can be conveniently divided into conductive, sensorineural, and central disorders, where (1) conductive disorders involve transmission of the sensory stimuli to the sensory receptors (usually but not always by impeding transmission); (2) sensorineural disorders involve dysfunction of the sensory receptors or conduction of signals from the sensory receptors to the brain; and (3) central disorders involve dysfunction of processing sensory information within the central nervous system, particularly within the brainstem and cerebrum.
Conductive gustatory disturbances. Conditions that impede or alter the contact of tastants with the taste receptors produce conductive (or “transport”) hypogeusia or dysgeusia. Such conditions can include poor oral hygiene, dental caries, periodontal disease, denture use, gastroesophageal reflux, upper respiratory infections, oral candidiasis (thrush), and oral cancer. With oral candidiasis, for example, the growth of yeast produces a barrier that precludes contact of the tastants with the gustatory receptors. Similarly, elderly patients frequently develop a thick, whitish mucoid coating on the tongue (“tongue plaque”), which is evident on arising and can interfere with taste acuity.
Conditions that interfere with chewing or salivation are also likely to produce conductive hypogeusia. During mastication, food is crushed and ground by the teeth (chewed), warmed, and mixed with liquid saliva. These actions release tastants from the food and facilitate the conveyance of tastants in a liquid or semiliquid state to the gustatory receptors (among other actions, such as facilitating enzymatic breakdown of food components). Therefore, conditions that interfere with chewing or movement of the food bolus (such as lack of teeth, poorly fitting dentures, temporomandibular joint dysfunction, jaw claudication, and dysphagia) can lessen the experience of taste.
Because saliva is necessary to help soften the masticated food and to convey tastants in a liquid state to the gustatory receptors, disorders that interfere with saliva production result in hypogeusia or dysgeusia. In addition, saliva helps to prevent pathologic growth of bacteria and fungi and to maintain oral pH and ionic composition at proper levels; disruption of any of these can alter taste sensation (204).
Saliva also modulates some long-lasting flavors by trapping free thiols produced by oral anaerobic bacteria (205). Bacteria convert odorless sulfur compounds in some fruits and vegetables (grapes, onions, and bell peppers) into odoriferous thiols after the foods have been swallowed (the so-called “retro-aromatic effect”). The odoriferous thiols can be perceived after 20 to 30 seconds and persist for several minutes.
Xerostomia (dry mouth due to a lack of saliva, sometimes colloquially called “cotton mouth” or “dough mouth”) is a common cause of conductive hypogeusia in the elderly. Xerostomia can occur with the use of various medications (such as anticholinergic medications and diuretics) and with tobacco smoking, diabetes mellitus, radiation therapy for head and neck cancers, and Sjögren syndrome (204).
Sensorineural and central gustatory disturbances. Taste sensations are mediated by polarized neuroepithelial cells that are clustered into taste buds scattered across the dorsal surface of the tongue and are present to a lesser degree on the soft palate, pharynx, epiglottis, larynx, and the first third of the esophagus. The facial (via the chorda tympani), glossopharyngeal, and vagus nerves transmit taste signals from the taste receptor cells to the rostral portion of the nucleus of the solitary tract in the dorsal medulla. Chemesthetic (pungent) sensations in the oral cavity are mediated separately via the trigeminal nerve and via free nerve endings in the chorda tympani, glossopharyngeal, and vagus nerves. Such sensations are a form of nociception distinct from taste (187).
From the nucleus of the solitary tract, taste-responsive axons project through the ipsilateral central tegmental tract in the pons, decussate at a higher level (probably in the midbrain), and project to the ventro-postero-medial nucleus of the thalamus and to other sites, including the lateral hypothalamus and the amygdala (123; 182). In the elderly, interruption of the central gustatory pathway in the brainstem most commonly results from lateral pontine strokes (182; 114). Gustatory neurons in the thalamus project to the primary gustatory cortex, which in humans has been tentatively localized to the transition area between the posterior insula and parietal operculum and the central sulcus (107). Cortical areas involved in processing gustatory stimuli are in the insula, the frontal and parietal opercula, and the orbitofrontal cortex (196). In right-handed individuals, the left cerebral hemisphere contains a gustatory representation of both sides of the tongue (hemi-tongues), whereas only the right hemi-tongue is represented in the right hemisphere (182; 140).
Severe symptomatic neural or central hypogeusia rarely occurs as a clinical entity, particularly in isolation. Nevertheless, sensorineural or central gustatory disorders can potentially result from damage to any part of the gustatory neural pathway from the taste buds via the cranial nerves conveying gustatory sensation (the facial, glossopharyngeal, and vagal nerves) through the brainstem and thalamus to the cerebral cortex (78). Sensorineural and central gustatory disorders in the elderly may be caused by drugs, toxins, and physical agents; damage to the cranial nerves conveying gustatory sensation (for example, isolated cranial mononeuropathy as with Bell palsy, or cranial polyneuropathy); space-occupying processes (particularly with tumors involving the cerebellopontine angle or the jugular foramen); degenerative disorders (such as Parkinson disease or Alzheimer disease); seizures; and depression.
A systematic review and meta-analysis identified significant risks of gustatory dysfunction with Alzheimer disease, COVID-19, chemotherapy, and rhinosinusitis (133). Another systematic review and meta-analysis found that gustatory dysfunction has been inconsistently associated with Parkinson disease (113). Another systematic review and meta-analysis found that gustatory dysfunction diagnosed by gustatory function testing was closely associated with Alzheimer disease, even though the results of subjective questionnaires were not significantly different between patients with Alzheimer disease and healthy controls (112). Pooled analyses from a systematic review and meta-analysis showed worse global taste threshold and identification (sour in particular) scores in Alzheimer disease subjects than in controls and worse global, sweet, and sour scores in Alzheimer disease subjects compared to subjects with mild cognitive impairment (137). Subjects with Parkinson disease with mild cognitive impairment showed worse global, sweet, salty, and sour scores than controls and cognitively unimpaired subjects with Parkinson disease (137). Taste dysfunction is differentially associated with the severity of cognitive deficits regardless of the specific neurodegenerative disorders, suggesting that gustatory dysfunction may be a cross-disease chemosensory biomarker of neurocognitive disorders (142; 137). Whether gustatory alterations may be a useful preclinical biomarker of neurocognitive disorders requires further study.
Brain olfactory taste receptor (TASR) expression has been documented in neurologic diseases, including Alzheimer disease (06). TAS2R genes are expressed and markedly downregulated in human orbitofrontal cortex at early stages of sporadic Alzheimer disease, preceding the progressive reduction in their protein levels and the appearance of Alzheimer disease-associated neuropathology (06).
Types of phantageusia. In 1973, while trying to characterize the visual hallucinations observed among nonpsychotic patients with visual impairments, Harvard neuro-ophthalmologist David Cogan (1908-1993), then chairman of the Department of Ophthalmology at Harvard Medical School, usefully distinguished what he called “release” hallucinations from other types of hallucinations, particularly those associated with “irritative” processes in patients without psychosis (42). Shortly after this publication, Cogan left Harvard to become Chief of Neuro-ophthalmology at the National Eye Institute of the National Institutes of Health, Bethesda, Maryland.
Release hallucinations are spontaneous sensory phenomena that occur in the setting of sensory loss. Sufficient impairment or removal of normal afferent inputs to the primary visual cortex apparently allows, disinhibits, or “releases” spontaneous activity within the corresponding visual association cortex that is interpreted as a perception, even though there is no corresponding sensory stimulus (a hallucination). A release mechanism for hallucinations is supported by (1) a sensory deficit in the same modality as unimodal hallucinations, with onset of hallucinations in conjunction with or following the sensory deficit; (2) variable content; (3) awareness of the hallucinatory nature of the perception; and (4) no evidence of seizures or other irritative phenomena (including no other positive motor or sensory phenomena, not paroxysmal in character, no epileptiform discharges on electroencephalography, and unresponsive to administration of anticonvulsant medications) (42; 122; 121; 24; 117). Release hallucinations can occur in normal individuals with pansensory deprivation (84; 83). Similarly, modality-specific release hallucinations can occur experimentally (83; 144) or pathologically (80; 122; 121) with unimodal sensory deprivation.
In contrast, an “irritative” mechanism for hallucinations is supported by any of the following: (1) stereotyped content; (2) lack of awareness of the hallucinatory nature of the perception (termed hallucinosis); and (3) evidence of a potentially irritative process (such as migraine, tumor, or seizure) (42; 24). However, the clinical distinction between epileptic and release hallucinations is not always clear, and both types can occur in the same patient (Table 3). Spontaneous neuronal discharges, which can occur with both seizures and deafferentation, may be involved with both mechanisms (125; 54; 35).
|
Characteristic |
Ictal hallucinations |
Release hallucinations |
|
Duration |
Brief (seconds to minutes) |
Often persistent (minutes to hours) |
|
Variability |
Often stereotyped |
Usually variable and change over time; rarely stereotyped |
|
Content |
Simple or complex |
Simple or complex |
|
Sensory deficit in modality of hallucination |
No (except possibly incidental) |
Yes |
|
Environmental triggers |
No |
Common (low light, closing or opening eyes, saccadic eye movements) |
|
Associated ictal behavior, including alterations of consciousness |
Often |
No |
|
Epileptiform discharges or seizures demonstrated on EEG |
Often |
No |
|
|
Cogan's dichotomy can usefully be applied to phantageusia but does not exhaust the possibilities. For example, it was never intended to encompass psychotic or psychogenic hallucinations or factitious disorder with pseudo-hallucinations.
Dysgeusia in COVID-19. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) enters human host cells via mechanisms facilitated by angiotensin-converting enzyme 2 (ACE2) and transmembrane protease serine 2 (TMPRSS2). COVID-19-related chemosensory dysfunction results primarily from a loss of function of olfactory sensory neurons and taste buds, mainly caused by infection, inflammation, and subsequent dysfunction of supporting non-neuronal cells in the mucosa (139). COVID-19 entry receptors are highly expressed in taste buds, thereby intensifying the cytocidal effect.
The COVID-19-induced "cytokine storm" causes secondary damage to taste function, in part because interferon and various proinflammatory cytokines trigger cell apoptosis and disrupt the renewal of taste bud stem cells (213; 214).
Interleukin 6 (IL-6), a pro-inflammatory cytokine that is promptly, but transiently, produced in response to infections and tissue injuries, contributes to host defense through the stimulation of acute-phase responses, hematopoiesis, and immune reactions. The rapid recovery of smell and taste functions in patients with COVID-19 may, in part, be attributable to changes in IL-6 levels rather than to recovery from viral injury to neurons (33; 202).
A high proportion of patients with COVID‐19 describe a loss of taste but standardized functional testing of the gustatory modalities of sweet, sour, salty, and bitter often do not reveal a bona fide hypogeusia (87; 147); therefore, subjectively altered taste is probably caused in part by impaired retronasal olfaction (87; 218; 147). Nevertheless, daily testing demonstrated that orthonasal smell, oral chemesthesis, and taste are each altered by acute SARS-CoV-2 infection; this disruption was dyssynchronous for different modalities, with variable loss and recovery rates across both modalities and individuals (217). Moreover, fungiform papillae biopsies on 16 patients who reported taste disturbance lasting more than 6 weeks after molecularly determined SARS-CoV-2 infection showed evidence of SARS-CoV-2, accompanying immune response, and misshapen or absent taste buds with loss of intergemmal neurite fibers (222).
Paxlovid mouth. The antiviral medication, Paxlovid (nirmatrelvir/ritonavir combination), has shown remarkable efficacy in reducing SARS-CoV-2 viral load and relieving clinical symptoms. However, a persistent bitter/bad taste, referred to as "Paxlovid mouth," is a frequent adverse effect, and this dysgeusia is listed as a main adverse effect of Paxlovid based on clinical trial data (30). Nirmatrelvir is an oral protease inhibitor that inhibits a SARS-CoV-2 protease (MPRO) that plays an essential role in viral replication, whereas ritonavir prolongs the activity of nirmatrelvir by slowing its metabolism; although ritonavir tastes bitter, prior usage of ritonavir in other conditions has not been linked to a persistent bad taste, suggesting that nirmatrelvir is responsible for Paxlovid mouth, possibly by activating one or more of the 25 human TAS2R bitter taste receptors. TAS2R1 is the primary bitter receptor activated by nirmatrelvir, at concentrations as low as 15 μM, which overlaps with plasma concentrations of nirmatrelvir in a subset of patients (30).
|
• There is a high prevalence of olfactory and gustatory dysfunction among patients with COVID-19. | |
|
• Chemosensory disorders are relatively uncommon in pediatric cases of COVID-19 compared with adults. |
Dysgeusia in COVID-19. There is a high prevalence of olfactory and gustatory dysfunction among patients infected with novel coronavirus disease 2019 (COVID-19) (02; 95; 10; 14; 179; 18; 22; 75; 99; 129; 154). Dysgeusia is more common in patients with COVID-19 than in those suffering from other viral infections or controls (165). In a meta-analysis of 24 studies collectively involving 8438 patients with test-confirmed COVID-19 infection from 13 countries, the pooled proportions of patients presenting with olfactory dysfunction and gustatory dysfunction were 41% and 38%, respectively (02). In a separate meta-analysis of eight studies, collectively involving 11,054 patients with COVID-19, dysosmia and dysgeusia symptoms were present in 75% and 81% of COVID-19 cases, respectively (181). The prevalence of olfactory and gustatory dysfunction is negatively correlated with age in adults (02; 74; 124; 93; 158).
Chemosensory disorders are relatively uncommon in pediatric cases of COVID-19 compared with adults (56; 111; 167). In one series, only 6% of 122 pediatric COVID-19 cases had a chemosensory disorder, and all affected children fully recovered by the end of the third week of illness, even though one showed restricted diffusion in the splenium of the corpus callosum (56). In another series, 28% of 141 adolescents had chemosensory dysfunction with a self-reported duration of from 2 to 15 days (mean 5.7 days) (111).
Parageusia and dysfunctions in umami, bitter, and sweet taste perception can be indicators of more severe forms of COVID-19 (34).
The severity of COVID-19-associated chemosensory dysfunction has dropped significantly with the advent of the Omicron variant (18). Some studies also reported that the frequency of chemosensory dysfunction also declined with the advent of the Omicron variant; others found no change in the prevalence of chemosensory dysfunction during the period of Omicron dominance (203; 213; 214). In one study in the Omicron era, individuals with chemosensory dysfunction had significantly higher rates of influenza-like upper respiratory symptoms, xerostomia, and halitosis (213; 214). Moreover, olfactory dysfunction was a risk factor for the prevalence of taste dysfunction in patients with Omicron infection.
Prevention of COVID-19-related chemosensory dysfunction is feasible with vaccination, although vaccinated individuals still carry a risk of developing COVID-19 and related chemosensory dysfunction (211).
When a patient presents with gustatory complaints, the critical considerations are determining whether there is a loss of function (hypogeusia or ageusia), a distortion of function (parageusia), or a perceived taste in the absence of a tastant in the mouth (phantageusia).
Reports of decreased ability to taste, or decreased ability to smell and taste, are often found to represent solely or primarily an impairment of olfaction. A bona fide hypogeusia should be categorized as conductive, sensorineural, or central, as this will greatly focus the evaluation and the differential diagnosis. Acute bilateral impairment of smell and taste is likely related to an adverse drug reaction, an upper respiratory infection, or other viral illness (particularly SARS-CoV-2 during the COVID-19 pandemic). Acute unilateral impairment of taste is most commonly due to a facial nerve disorder (affecting the anterior two thirds of the tongue as in Bell palsy, Ramsay Hunt syndrome, Melkersson-Rosenthal syndrome, etc.) but can be seen also with glossopharyngeal nerve disorders (jugular foramen syndrome with unilateral loss of taste on the posterior third of the tongue), brainstem lesions (eg, cerebrovascular, demyelinating), and opercular lesions.
Distortions of function often accompany a loss of function, and most such distortions are unpleasant--often very unpleasant.
"Organic" phantageusias may occur by either an "irritative" mechanism (eg, epilepsy, migraine) or a "release" mechanism (ie, in the setting of hypogeusia or ageusia or possibly postictally, like a gustatory equivalent of a Todd paralysis). These must be distinguished from gustatory hallucinations that are manifestations of psychosis, psychogenic disorders, and factitious disorders.
|
• Medications that can alter gustatory function are numerous and varied. | |
|
• Sudden onset of dysgeusia during the COVID-19 pandemic generally does not require extensive investigation. |
Complaints of impaired “taste” are often symptoms of olfactory dysfunction because much of the flavor of a meal derives from olfactory stimulation. Indeed, the complex sensory experience of “flavor” during the consumption of foods and drinks cannot be constructed simply from combinations of the basic taste qualities (sweet, salty, sour, bitter, and umami or savory).
Review medications for medication-induced dysgeusia. Carefully review medications, including over-the-counter medications, for possible contributions to either olfactory or gustatory impairment. Medications that can alter taste in elderly patients are numerous and varied and include amitriptyline, baclofen, carbamazepine, phenytoin, levodopa, and propranolol as well as various lipid-lowering drugs, antihistamines, antimicrobials, antineoplastics, nonsteroidal anti-inflammatory drugs, allopurinol, bronchodilators and other asthma medications, antihypertensives and cardiac medications, lithium, antidepressants, and antipsychotics (176; 62; 187; 204; 48; 37). In the FDA Adverse Events Reporting System (FAERS), (1) gustatory adverse effects are more commonly reported than olfactory adverse effects; (2) antineoplastic and immunomodulating medications accounted for 22% and 36% of olfactory and gustatory adverse drug reactions; and (3) the angiogenesis inhibitor lenalidomide (for myelodysplastic syndrome, multiple myeloma, and mantle cell lymphoma) and the tyrosine kinase inhibitor antineoplastic agent sunitinib (for advanced or metastatic renal cancer, gastrointestinal stromal tumors, and pancreatic neuroendocrine tumors) were the drugs most commonly associated with gustatory dysfunction (45).
Dysgeusia in COVID-19. Sudden onset of dysgeusia during the COVID-19 pandemic generally does not require extensive investigation. New loss of taste (ageusia or hypogeusia) is now recognized as a COVID-19-related symptom, often but not always accompanied by dysosmia (eg, anosmia, hyposmia, or parosmia) (103; 138; 148; 173; 175; 156).
Toxin-induced chemosensory dysfunction. The neurologic history should address potential sources of toxin-induced chemosensory dysfunction, although toxin-induced chemosensory dysfunction is commonly associated with loss of smell rather than loss of taste (172; 198). Acute toxin-induced chemosensory loss may be straightforward if associated with a history of immediate-onset hyposmia or hypogeusia and a discrete toxin exposure, although confounding with litigation and financial incentives should be considered. In contrast, chronic exposures are typically more difficult to diagnose (172; 198).
Metabolic causes of taste dysfunction. Diabetes, hypothyroidism, kidney disease, and other metabolic conditions can cause dysgeusia, so screening studies should be done to identify or exclude these common disorders (143; 223).
Physical examination and office testing. Physical examination should include examination of the nose, mouth, and throat as well as neurologic examination.
Office testing of smell can include well-standardized, commercially available tests (such as the University of Pennsylvania Smell Identification Test, or UPSIT) or crude approaches utilizing identification of a few readily available odorants (such as oil of wintergreen or oil of cloves) (50; 51; 47; 48); more complicated odor identification and detection tests are also available but are rarely practical outside specialized diagnostic laboratories (47). The UPSIT is a forced-choice olfactory discrimination test that uses microencapsulated odorants in standardized “scratch ‘n’ sniff” booklets. UPSIT scores are standardized by gender and age and can be used to identify degrees of hyposmia and some malingerers. Irritant substances, such as ammonia, are sometimes employed when psychogenic or malingered anosmia is a consideration because such substances are perceived via trigeminal afferent pathways instead of through the olfactory system.
Office testing of gustatory function remains somewhat crude (188). Testing of taste thresholds is problematic because salivary function and the size of the tongue area stimulated influence threshold assessment, taste intensity may be depressed even with normal recognition thresholds, and changes in threshold detection do not necessarily correlate with suprathreshold taste intensity. Nevertheless, complicated and time-consuming procedures are available for whole-mouth assessment of thresholds for each of the four primary tastes (sweet, sour, salty, and bitter) (220; 221) but are also rarely practical outside specialized diagnostic laboratories. Newer technologies, such as using flavor-impregnated taste strips or tasting tablets, are in development and can potentially include an assessment at multiple thresholds for all of the primary tastes, including umami (savory) gustatory sensation (03; 199; 115).
Special examination methods for assessing gustation. Chemical testing uses chemical tastants (eg, sucrose for sweet, citric acid for sour, sodium chloride for salty, caffeine for bitter, and monosodium glutamate for umami) to assess taste. Unfortunately, routine office testing of taste may not reveal any findings in transient, drug-induced taste disturbances. More complicated methods have been developed that can be used in office environments but that are more typically used in subspecialty clinics or research settings devoted to chemosensory disorders.
The 3-drop method of chemical testing is a subjective, non-localizing ("whole mouth") assessment technique that uses aqueous solutions of the five basic tastes to provide both the detection threshold (ie, the concentration at which the subject correctly identifies the presence of a taste) and the recognition threshold (ie, the concentration at which the subject correctly identifies the particular basic taste) (188; 216; 162). For each forced-choice trial of three separate drops (the two control drops being just water), the subject is asked to select the one that contains the tastant. Larger volumes can be used, in which case the subject must sip, swill, and spit. The tastant must be correctly identified three times, or else the next higher concentration solution is used. One potential confounding factor with this approach is that the aqueous solutions may wash away the saliva, the medium through which tastants are normally conveyed to taste buds, thus altering taste sensitivity (141). The use of tablets or wafers impregnated with the basic tastants eliminates some of the logistical challenges of using aqueous solutions of escalating concentration with controls; these can be easily stored and used for routine clinical practice but suffer the same drawbacks as any whole-mouth testing method (03; 188; 162).
Whole-mouth chemical testing methods are generally sufficient for drug-induced gustatory impairment, but, when necessary, regional chemical testing is possible with commercially available "Taste Strips," paper strips impregnated with one of four tastants (sweet, sour, salty, or bitter) in four different concentrations--16 separate strip types for all tastant-concentration combinations (152; 115; 188; 162). The Taste Strips are placed in a predetermined order on each side of the tongue while it is protruding from the mouth. Lateralizing hypogeusia is identified with side-to-side differences above an established threshold. Regional testing can be used to detect isolated lesions of the chorda tympani (anterior two thirds of the tongue) or glossopharyngeal nerve (posterior tongue).
Electrogustometry is a subjective, localizing assessment technique that uses a small electrical current (1.5 to 400 μA) from a monopolar or bipolar stimulator to assess "taste" detection thresholds in different parts of the tongue. This test can provide localizing information about gustatory deficits (188), but it cannot distinguish between the different qualities of flavor because electrical stimulation invariably elicits a metallic and sour "taste" sensation. Approximately half of the women who receive chemotherapy for gynecological cancer have abnormal electrogustometry test results, with a tendency to develop hypogeusia in the chorda tympani nerve field and hypergeusia in the greater petrosal nerve field (157). Both pathways are extensions of the facial nerve, but the chorda tympani originates from the taste buds in the front of the tongue, whereas the greater petrosal nerve (or greater superficial petrosal nerve) is a branch of the nervus intermedius (nerve of Wrisberg or glossopalatine nerve) that, among other things, carries taste afferents from the soft palate.
Gustatory evoked potentials are a feasible, objective assessment technique that can be used to distinguish ageusia from psychogenic disease or malingering (105; 96; 162). After applying a chemical or electrical taste stimulus, evoked waveforms are recorded from an EEG. Unfortunately, gustatory evoked potentials may be influenced by various confounding factors (eg, thermal, tactile, or olfactory stimulation), are difficult to interpret, and only provide consistent results with sour tastes (162).
Imaging. Cranial imaging (CT and MRI) is most useful for patients with olfactory disorders to detect abnormalities in the nasal cavities (eg, nasal polyposis), nasal sinuses (eg, sinusitis), and anterior cranial fossa (eg, meningioma). They may rarely be useful in gustatory disorders, and there are almost always other neurologic signs that would indicate a central disorder.
Functional MRI and PET are not of clear clinical utility in the clinical evaluation of chemosensory disorders (182; 162).
Management depends heavily on the responsible cause. Management action can improve or resolve dysgeusia with temporal lobe epilepsy and medication-induced dysgeusia.
Underlying olfactory disorders may cause secondary apparent decreased or altered taste sensations.
Burning mouth syndrome. Burning mouth syndrome has been treated with a wide range of drugs belonging to different pharmacological groups (eg, antidepressants, antipsychotics, antiepileptic drugs, analgesics, and mucosal protectors) (145). Although there are anecdotal reports of therapeutic success, an effective treatment modality for most cases of burning mouth syndrome remains to be established (145).
Conductive gustatory disturbances. Patients who have conductive gustatory disturbances due to a thick, whitish mucoid coating on the tongue (“tongue plaque”) should be encouraged to remove this with a soft toothbrush, with a dry gauze pad, or by eating so-called “detergent” foods (hard bread, dry cereal, uncooked vegetables, or fibrous meats). Tongue brushing should also be encouraged twice daily, on rising and before bed, especially in elderly patients with oral prostheses.
Breath mints, sugarless chewing gum or lozenges, artificial saliva products, citric acid mouthwashes, and systemic pilocarpine can each be of modest symptomatic benefit in patients with xerostomia.
Sensorineural and central gustatory disturbances. Sensorineural and central gustatory disturbances are generally much more difficult to manage.
Dysgeusia in COVID-19. A retrospective, hospital-based, observational study of 141 patients in Italy found that administration of steroids during hospitalization was significantly associated with a higher chance of 3‐month recovery from chemosensory dysfunction (131)
Although systemic corticosteroids have been recommended as a therapeutic option in COVID-19-related chemosensory dysfunction, a more cautious approach is recommended until the results of randomized controlled trials are available (92). Reasons for not using systemic corticosteroids for COVID-19-associated chemosensory dysfunction include the following: (1) evidence supporting their usefulness is weak; (2) the rate of spontaneous recovery of COVID-19-related dysosmia is high; and (3) corticosteroids have significant potential adverse effects (92).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
General Neurology
May. 13, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neurobehavioral & Cognitive Disorders
Apr. 08, 2026