






Epilepsy & Seizures
Driving and epilepsy
Jul. 08, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Patients in the intensive care unit are critically ill and require multimodal continuous physiological monitoring. Like telemetry and pulse oximetry for the cardiorespiratory systems, EEG allows for real-time neurophysiological monitoring. EEG measures electrical activity in the brain and can sensitively detect changes in brain functioning and structure (84). When EEG is set up to run “continuously,” it allows for prolonged simultaneous recording of electrical brain activity and clinical behavior. This is most often used in the ICU setting to identify changes in brain function to correlate with altered mentation or atypical movements, specifically to evaluate for evidence of nonconvulsive seizures or nonconvulsive status epilepticus. These seizures can be difficult to diagnose as they can be brief and without clinical correlation other than coma or confusion and can only be diagnosed using EEG-based diagnostic criteria (44; 109; 42; 115).
The importance of their proper diagnosis is their reported association with significant morbidity and mortality (134; 111) and the fact that delay in the diagnosis and treatment of nonconvulsive seizures and nonconvulsive status epilepticus can lead to worse outcomes (44). Nonconvulsive seizures and nonconvulsive status epilepticus can occur in different settings, including the neurosurgical, neurologic, medical, and general surgical intensive care units (85; 91; 67; 68; 26; 48), and in pediatric and adult cases in which seizure monitoring is the focus (42; 119; 32; 115). This has led to more widespread use of continuous EEG with outcome benefits (05).
Continuous EEG is valuable in detecting seizures to facilitate diagnosis and monitoring a response to treatment. Many have also found utility in using cEEG for prognostication and guiding clinical and sedative management in those with traumatic or hypoxic-ischemic brain injuries and in the detection of ischemia warranting intervention in the setting of subarachnoid hemorrhage (44; 111; 43).
Despite benefits derived from its use, cEEG requires significant resources, and its performance should be triaged appropriately using clinical history and routine or STAT EEG results to determine its indication (108). Given the complex nature of cEEG interpretation, specialized training in cEEG interpretation is required (36).
This article will review EEG monitoring in the intensive care unit setting, highlight clinical indications and goals of its use, discuss important EEG patterns that may aid in clinical diagnosis and prognosis, consider the duration of EEG monitoring, and present recent information in this evolving field.
|
• Continuous EEG monitoring is defined as EEG monitoring performed for extended periods, ranging from hours to days. | |
|
• cEEG is used for a variety of indications, including the detection of nonconvulsive seizure and nonconvulsive status epilepticus, assessing response to therapy in patients who experience status epilepticus, monitoring level of sedation, ischemia detection, and prognostication. | |
|
• Duration of cEEG monitoring differs depending on the clinical situation and EEG patterns present during the early portion of the recording, but, at minimum, should be 12 to 24 hours if ordered to detect seizures. | |
|
• cEEG is becoming more widespread in its use, but there are significant barriers that need to be removed for better access, given its utility in clinical management. | |
|
• Quantitative and “rapid” EEG techniques are becoming more widely used and available and may provide more capability to provide efficient and timely diagnosis and institution of treatment, regardless of institutional resources and clinician expertise, leading to improved outcomes. | |
|
• Artificial intelligence using deep learning methods has the potential for improving the accuracy and efficiency of evaluating critically ill patients with cEEG monitoring for seizure detection and neuroprognostication. |
Techniques to monitor multiple organ systems for patients in the intensive care unit have been present for some time, but neurologic monitoring was historically performed through “neuro-checks.” This alone is well-known to be a suboptimal way to monitor neurologic changes in comatose or sedated patients that would require urgent interventions (54). In the 1980s, many felt that EEG could be used to monitor neurologic patients in the ICU (08; 25) and for coma prognosis (09; 11). Until digital EEG technology was introduced, compressing this data had been exceedingly difficult and arduous (53). Over the past 20 years, cEEG use has expanded, and quantitative EEG techniques have become available to further aid in the interpretation of EEG data (110). The implementation of artificial intelligence in the ICU and continuous EEG monitoring should enhance our understanding and accuracy in detecting ictal and interictal patterns. Through the use of deep learning paradigms, artificial intelligence can enable more accurate and efficient cEEG interpretation, helping clinicans keep up with the increasing demand (35; 65; 50; 06). Artificial intelligence may also facilitate the understanding of complex neurophysiological signals that can be analyzed in various clinical situations encountered in the ICU, such as in prognostication in brain injury (37).
The COVID-19 pandemic posed unprecedented challenges to the healthcare system, and restricted access to EEG services significantly affected the ability to care for critically ill patients with COVID-19 complications (30). This included reduced inter-hospital transfers for inpatient EEG and cEEG (135). EEG technologist shortages also had an impact, with fewer capabilities to set up conventional routine EEG and cEEG studies in hospitals (66; 77; 135). The importance of providing a pandemic-proof inpatient EEG service line, including cEEG, has been highlighted and should lead to improvements to avoid limited resources in the future should another emergency arise (30).
Performing an EEG entails placing electrodes on the scalp to detect voltage fluctuations that correspond to electrical brain activity. The EEG electrodes are placed on the scalp using an adhesive substance, and the locations where electrodes are placed are determined via an international standardized 10-20 system, including a single channel of electrocardiogram (ECG) (03). A video recording most often accompanies the EEG recording so that any clinical activity can be correlated to the EEG recording. The recorded EEG activity is converted to a digital signal that is then stored in computer memory for subsequent interpretation (104).
cEEG is defined as EEG monitoring for much longer periods of time, which can range from several hours to several days, depending on the monitoring goals (44).
Both mobile machines and “hard-wired” rooms can be used for cEEG monitoring. Hard-wired rooms typically may have one or more cameras and computers to enable repeat patient monitoring. Mobile EEG machines have a camera affixed to a mobile platform. These can be rapidly moved to other areas in the hospital, such as the emergency department or to the ICU, where the electrodes can be secured for cEEG monitoring. Hybrid systems allow for rooms to be fitted with cameras, but the EEG machine is brought into the room when needed. Internet connectivity can transfer EEG data to a workstation where they can be interpreted remotely. Data transfer occurs continuously, allowing for live streaming of EEG, or are transferred intermittently, where EEG is uploaded online every several hours for review. Bluetooth-enabled systems are available to allow live streaming or storing data on the Cloud using wireless technology (14).
EEGs that are obtained to address the presence of nonconvulsive seizures and nonconvulsive status epilepticus are often urgent or emergent. However, the need for technologists to intermittently set up the standard EEG can delay diagnosis and treatment. This has led to the development of rapid EEG systems that can be used as a screening tool and performed like cEEG for longer monitoring (75). There are a few of them, including those with full (75) and reduced (12; 23; 125) montages. They allow for quicker EEG setup without the need for technicians to be called in from out of the hospital, which can often delay diagnosis and treatment, particularly in facilities without frequent after-hour or overnight availability of a technologist (75; 131). Rapid reduced montage EEG demonstrates decent sensitivity when specifically ordered to evaluate for nonconvulsive status epilepticus and provides the ability for quick diagnosis and initiation of treatment when compared to standard technologist-guided EEG (125). Rapid reduced montage EEG has also demonstrated earlier detection of seizures, leading to reduced ICU stays (21). As a result, these rapid EEG systems have become more utilized in ICU settings when EEG technologists are unavailable. The feasibility and sensitivity of the full montage system rapid EEG has received more limited attention, though presumably offers similar benefits in performance time and treatment initiation (75).
When studying reduced EEG montage in adults and pediatric patients, some have found a sensitivity for detecting seizures of 54% to 72% depending on the population (61; 82; 96; 114; 106), though others have found higher sensitivity or specificity (118; 57; 71; 89; 124; 40; 74) for identifying seizures and status epilepticus. There is demonstrated accuracy for reduced montage in prognostic capability following cardiac arrest (73). As of 2015, the American Clinical Neurophysiology Society recommends using montages with fewer than 16 electrodes only in emergencies (42).
EEG monitoring, particularly processed EEG (pEEG) with a reduced montage system, is becoming more widely used in the ICU setting to monitor sedation in critically ill patients (93). pEEG involves the compression and simplification of EEG signals and creates indices that can be easily interpreted (bispectral index, patient state index, etc.). This is crucial given the need for monitoring sedated patients to ensure the comfort of the patient while avoiding excessive sedation, which can lead to morbidity and mortality (87; 86). It is recommended that all patients receiving sedation in the ICU who cannot be clinically monitored for depth of sedation should be assessed using pEEG (93).
Continuous EEG can be analyzed and efficiently reviewed using quantitative EEG, which is based on time frequency analyses to detect seizures; more recent standardization of quantitative EEG nomenclature allows for higher inter-rater agreement amongst experts regarding ICU EEG patterns (136). Further, quantitative EEG has shown high rates of sensitivity in diagnosing seizures in patients with high seizure burden (04) and can be used by novices and experts alike (04; 56). Though not yet commercially available, automated monitoring systems using artificial intelligence and machine learning models hold promise in providing more accurate and timely interpretation of cEEG in critically ill patients (35).
The American Clinical Neurophysiology Society published guidelines for the clinical use of cEEG (42) and since that time, only two other governing neurologic societies have made formal recommendations on the indications for cEEG (80; 117). See Table 1 for indications used from both guidelines.
|
• Diagnosis of nonconvulsive seizures, nonconvulsive status epilepticus, or other paroxysmal events | |
|
• Assessment of efficacy of therapy for nonconvulsive seizures or nonconvulsive status epilepticus | |
|
• Identification of cerebral ischemia | |
|
• Monitoring the level of therapeutic sedation or burst suppression | |
|
• Assessment of severity of encephalopathy and prognostication | |
|
| |
Diagnosis of nonconvulsive seizures and nonconvulsive status epilepticus. Convulsive status epilepticus is defined based on the duration of convulsive seizures using two different time points. The most recent consensus statement from the International League Against Epilepsy (ILAE) denotes the first time point (t1, 5 minutes) as the period at which convulsions are unlikely to cease without medical intervention and the second time point (t2, 30 minutes) at which neuronal injury has been shown to occur in animal and clinical studies (122).
Convulsive status epilepticus may subsequently evolve to nonconvulsive seizures, and up to 15% develop nonconvulsive status epilepticus (19; 99). Though nonconvulsive status epilepticus may occur without preceding clinical seizures, roughly one half of patients who develop nonconvulsive seizures/nonconvulsive status epilepticus have a preceding clinical seizure (16; 01; 68). Nonconvulsive status epilepticus is defined as a subtype of status epilepticus without prominent motor activity, with or without coma (122). Those without coma can demonstrate subtle ictal activity, and others have electrographic seizures with coma as the only clinical manifestation (46).
Nonconvulsive seizures and nonconvulsive status epilepticus can be difficult to diagnose, often because the diagnosis relies solely on the EEG. Periodic epileptiform discharges are a common feature on EEG in patients who are critically ill, though the precise pathology associated with periodic epileptiform discharges is often uncertain (98). Lateralized periodic discharges usually reflect an acute or subacute injury of the cortex, though infrequently they may reflect a postictal feature in patients with epilepsy or have an underlying chronic structural basis. Stroke is perhaps the most common structural etiology generating lateralized periodic discharges, but it probably reflects the prevalence rather than the specificity of stroke. Periodic epileptiform discharges may also involve a spectrum of EEG findings. Lateralized periodic discharges associated with fast activity have a strong association with status epilepticus, and their finding on standard EEG should prompt further investigation with cEEG. Other periodic epileptiform discharges include bilateral independent periodic epileptiform discharges, generalized periodic epileptiform discharges, and stimulus-induced rhythmic, periodic, or ictal discharges. Electrographic patterns that appear to be potentially ictal lie on the “ictal-interictal continuum” (46). These include the following: any periodic discharge or slow wave pattern that averages 1 to 2.5 Hz over 10 seconds; any periodic discharge or slow wave pattern averaging 0.5 to 1 Hz over 10 seconds but has a plus modifier or fluctuation; any lateralized rhythmic delta activity averaging more than 1 Hz for at least 10 seconds with a plus modifier or fluctuation (46). Rhythmic patterns may also be difficult to interpret regarding their ictogenic potential and may relate to the clinical situation. For example, some have suggested that generalized rhythmic delta activity, even with plus modifiers that signify a higher ictal potential, may not be related to a high enough risk of seizures on cEEG to warrant long-term monitoring (108), but this may not generalize to all patients, such as those with NMDA-associated autoimmune encephalitis who are critically ill (51). In general, if there is clinical concern for nonconvulsive status epilepticus and EEG patterns on the continuum are encountered, one should consider antiseizure treatment and cEEG monitoring for seizure detection and treatment response assessment.
The Salzburg criteria can be used to more formally define and diagnose nonconvulsive seizures with EEG and clinical features in patients without known epileptic encephalopathy: the presence of epileptiform discharges greater than 2.5 Hz or epileptiform discharges less than or equal to 2.5 Hz or rhythmic delta/theta activity on EEG and at least one of the following; both EEG and clinical improvement with antiseizure medication, the presence of subtle clinical ictal manifestations associated with these EEG findings, or spatiotemporal evolution of these EEG features. In those with epileptic encephalopathies, the diagnosis is made when there are more prominent or frequent EEG features as noted above, with observable clinical change and improvement with antiseizure medications (07). The Salzburg criteria is accurate and reliable (70) with the use of cEEG (52; 46). It is hypothesized that both t1 and t2 in nonconvulsive status epilepticus is likely longer than that seen in convulsive status epilepticus, and it is unclear if irreversible brain injury occurs in these cases, though this depends on the clinical context (52).
The frequency of nonconvulsive seizures and nonconvulsive status epilepticus in ICU patients varies depending on the population studied as well as the underlying comorbidities.
One study demonstrated nonconvulsive seizures in 21% of ICU patients being monitored with cEEG (112). In the neurologic ICU, 15% of those monitored are found to have nonconvulsive seizures (20). Those with aneurysmal subarachnoid hemorrhage show nonconvulsive status epilepticus in 3% to 13% and nonconvulsive seizures in 7% to 18% of cases (62).
In the acute postneurosurgical period, roughly 19% of adults referred for cEEG demonstrate nonconvulsive seizures, with a higher incidence seen in those with lobar tumor, subarachnoid hemorrhage, or who underwent evacuation of a subdural hematoma (29). In pediatric intensive care units, up to 71% of patients may show nonconvulsive seizures if cEEG is indicated for possible seizure or altered mentation/coma (90).
Up to 48% of adults and 33% of children who present with convulsive status epilepticus may go on to develop nonconvulsive seizures after the clinical seizures cease, whereas about 15% of adults will develop nonconvulsive status epilepticus (19; 99). The Neurocritical Care Society and American Epilepsy Society recommend cEEG monitoring for those who do not return to their functional baseline 60 minutes after convulsions resolve, given the high risk of nonconvulsive seizures/nonconvulsive status epilepticus after convulsive seizures when patients remain poorly responsive or comatose (10; 38).
The importance of diagnosis and treatment of nonconvulsive seizures and nonconvulsive status epilepticus is related to their association with morbidity and mortality.
The presence of nonconvulsive seizures on EEG is associated with higher rates of disability, whereas a higher nonconvulsive seizure burden is also associated with worse short-term outcomes (90; 129). Conversely, when treated, seizures and status epilepticus may not be associated with worse prognosis or outcome (102). Therefore, diagnosis and intervention may improve outcomes in nonconvulsive seizures and nonconvulsive status epilepticus.
Given that treatment of nonconvulsive seizures and nonconvulsive status epilepticus could lower morbidity and mortality, one must consider the clinical scenarios in which there is a higher likelihood of detecting nonconvulsive seizures using cEEG. The clinical situations that warrant cEEG to detect nonconvulsive seizures and nonconvulsive status epilepticus (42) are listed in Table 2. The European Society of Intensive Care Medicine and the Neurocritical Care Committee of the Chinese Society of Neurology recommend cEEG monitoring for the detection of nonconvulsive status epilepticus and nonconvulsive status epilepticus in patients presenting with convulsive status epilepticus and those with a primary brain injury, such as trauma or ischemia, as well as in comatose patients in the intensive care unit who do not have a primary brain injury but whose mental status is altered for unclear reasons (17; 80).
Though newer paradigms for risk stratification of seizures in critically ill patients are helpful when triaging patients and considering the need cEEG monitoring (107), broader clinical information should still be considered. The following risk factors have been associated with a higher risk for developing nonconvulsive seizures and nonconvulsive status epilepticus in patients with altered mental status: clinical seizures and in particular convulsive status epilepticus before altered mentation, a history of epilepsy, coma, younger age, remote history of encephalitis or meningitis, presence of a brain tumor, having an active CNS infection, presence of an intracerebral hemorrhage, MRI evidence of encephalomalacia, or having recently undergone a neurosurgical procedure, in particular those undergoing neurosurgery for subarachnoid hemorrhage or with subarachnoid hemorrhage perioperatively, or those undergoing craniotomy for subdural hematoma evacuation (19; 128; 16; 13; 01; 67; 99; 68; 29). One must also consider sepsis and the newer broad-spectrum medications used to treat infection in critically ill patients, particularly cefepime, which may confer a higher risk of seizures (72; 27). Continuous EEG monitoring should be considered in these patients even if there are no ongoing clinical signs of seizure activity. In those without a primarily neurologic injury or clinical seizure history, with the indication for EEG being to diagnose the cause of altered mentation in a critically ill patient, the utility of cEEG is unclear. One study showed that performing cEEG did not demonstrate improved outcomes as opposed to repeated routine EEG, although it did show increased detection of ictal activity (94).
|
• Following generalized convulsive status epilepticus if the patient is not regaining consciousness | |
|
• Acute supratentorial brain injury with concurrently altered mental status | |
|
• Fluctuating mental status without a clear explanation for it in those without known brain injury | |
|
• Epileptiform abnormalities on routine (30-minute) EEG | |
|
• Pharmacological paralysis in patients with recurrent seizures or those at risk for seizures | |
|
• Paroxysmal neurologic events of unclear etiology that may reflect seizures |
Assessment of efficacy of therapy. Once nonconvulsive seizures or nonconvulsive status epilepticus are detected, EEG is used to monitor therapy response. Continuous EEG has been shown to significantly impact the use of sedatives and antiseizure drugs (45). Overuse of sedatives could lead to worsened outcomes, so accurate titration of antiseizure medications with cEEG is vital to avoid greater risk than benefit (43). Given the lack of consistent clinical correlation, EEG may be the only physiologic marker to assess the effectiveness of sedation or antiseizure medications.
EEG monitoring for cerebral ischemia. Cerebral ischemia may occur for various reasons, including hypoxia, encephalopathy, ischemic stroke, and following subarachnoid hemorrhage, to name a few. However, the most frequent reason to use cEEG is to detect ischemia associated with vasospasm is in the setting of subarachnoid hemorrhage. EEG can detect ischemia when it occurs and is still reversible, in contrast to other forms of ischemic injury (47). Continuous EEG provides real-time data, so rapid treatment can be initiated before irreversible ischemia leads to infarction (43). Ischemia may be delayed following subarachnoid hemorrhage, and prolonged cEEG is a noninvasive means necessary for early detection (33; 62). MRI is impractical for ischemia screening as it is difficult to perform acutely, and CT will only detect ischemia hours after neuronal injury has occurred. Transcranial Doppler ultrasonography is commonly used in place of angiography to screen for cerebral vasospasm after subarachnoid hemorrhage (78). However, transcranial Doppler ultrasonography can only be performed intermittently, in contrast to cEEG. When using EEG for ischemia detection, there are specific electrographic patterns using raw EEG data, including regional or hemispheric loss of high-frequency fast activity and relative increase in background slowing that can be early indicators of developing cerebral ischemia (47). Quantitative EEG techniques may identify trends signifying a change in the power spectra that incorporates changes in the alpha/delta ratio to provide added sensitivity to ischemia detection compared to conventional EEG monitoring. This may identify ischemia hours before it would be demonstrated with transcranial doppler ultrasonography (16; 33). Early detection of ischemia may facilitate timely confirmation with cerebral angiography and earlier initiation of therapeutic interventions with intra-arterial vasodilators to potentially improve neurologic outcomes. This is necessary to provide an ongoing, real-time basis to allow timely diagnosis and treatment that is made feasible with cEEG monitoring.
Monitoring during iatrogenic burst suppression and sedation. The goals of therapy for ongoing nonconvulsive seizures and nonconvulsive status epilepticus aim at achieving seizure suppression that, in some cases, reduces cerebral metabolic rates by achieving a suppression-burst pattern on the cEEG (64; 55; 10).
Pharmacologically induced suppression-burst (or burst-suppression) with sedating anesthetic drugs, such as midazolam, propofol, and pentobarbital, are used in cases of refractory status epilepticus and in some cases to control intracranial hypertension secondary to traumatic brain injury in addition to other acute brain injury (92; 10).
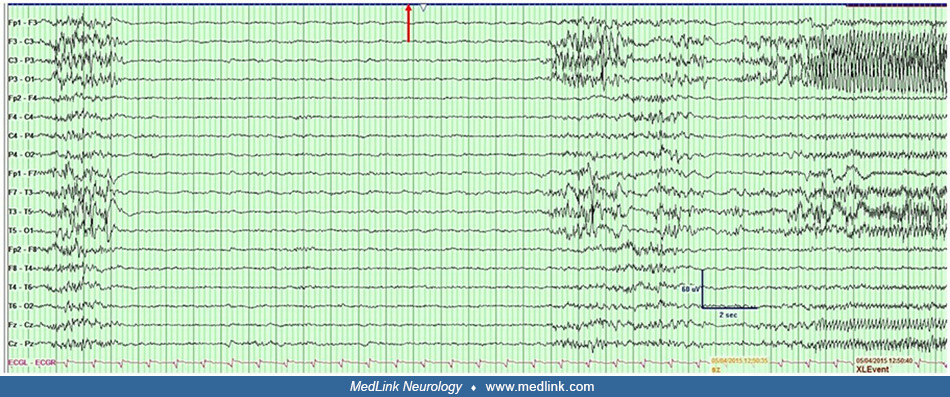
Suppression-burst during cEEG after levetiracetam, valproate, phenytoin, and propofol in a 78-year-old man with acute left parietal intraparenchymal hemorrhage. Note the left electrographic focal seizure at the end of the epoch...
In those who require neuromuscular blockade (eg, cisatracurium) for respiratory control and intravenous infusion of anesthetic drugs for treatment, cEEG monitoring is recommended for neurologic monitoring. By monitoring sedation status via cEEG, continuous infusions of sedating agents can be titrated more accurately to an endpoint and oversedation, along with its associated adverse effects, can be avoided (42).
Monitoring depth of sedation in critically ill patients is vital, and it has been recommended for those who cannot be clinically assessed for depth of sedation (93). This is important given that oversedation can lead to worse outcomes, including delirium and mortality (136). Reduced montage EEG with pEEG can enable more efficient and widespread use of neurophysiological monitoring in ICU patients to assess depth of sedation (22; 93). pEEG provides a simplified analysis of raw EEG data with spectral analysis, which allows non-neurophysiologist physicians and nurses to perform bedside analyses of depth of sedation for real-time decision-making (121; 93). pEEG can augment, but is not expected to replace, clinically validated sedation scales in the ICU (93). Further study is underway to improve current pEEG technology, particularly in relation to significant environmental artifacts that can degrade the neurophysiological recording (41).
Prognostication after cerebral injury. EEG has been shown to aid in predicting an ultimate prognosis in cases following severe cerebral insults, including hypoxic ischemic injury (particularly after cardiac arrest), traumatic brain injury, and subarachnoid hemorrhage (127; 15; 24).
In cases of hypoxic ischemic brain injury following cardiac arrest, EEG is vital in the prognosis, as well as the diagnosis and treatment, of nonconvulsive seizures (24) and can be used in those with post-hypoxic myoclonus to differentiate benign and malignant patterns (28; 31). Electrographic status epilepticus may cause secondary brain injury (73) and as such, urgent diagnosis and treatment is recommended (83). The presence of EEG continuity and reactivity, normal voltage background, and low suppression ratio on quantitative EEG suggest a good outcome in patients after cardiac arrest (95; 31), whereas a lack of reactivity, generalized periodic discharges, burst-suppression pattern, or early epileptiform activity and status epilepticus may indicate a poor prognosis (95; 31). It is unclear if there are differences regarding EEG features and prognostication with or without post-hypoxic myoclonus (31). The demonstration of EEG features on the ictal-interictal continuum is important both as a possible marker of poor outcome or a predictor of high risk for subsequent seizures that require treatment (18; 120; 47; 95; 105). Continuous EEG is more sensitive than intermittent EEG monitoring and could therefore be of more utility in the evaluation of comatose patients following cardiac arrest, though it may be more valuable in detecting nonconvulsive seizures/nonconvulsive status epilepticus than in actual prognostication itself, depending on the timing of monitoring (120; 24).
In those with moderate to severe traumatic brain injury, lack of posterior dominant rhythm, or N2 sleep transients, predominant delta background activity, or discontinuous background have all independently been associated with poor outcome (69).
Other features predicting poor prognosis are isoelectric or burst-suppression pattern, periodic discharges, and seizures; on the other hand, the presence of normal background and sleep activity has been shown to suggest a favorable prognosis (113; 42). Given that cEEG increases the yield for detecting seizures and other possible prognostic EEG features, it may be beneficial to perform cEEG in patients with traumatic brain injury as opposed to intermittent routine EEG (69).
Similar to those with traumatic brain injury, lack of normal sleep architecture and the presence of periodic discharges have been shown to be associated with poor outcomes in those with subarachnoid hemorrhage who are monitored with cEEG. Nonconvulsive status epilepticus and lack of reactivity are also predictive of poor prognosis (15).
The use of cEEG monitoring is a safe and noninvasive technique. As such, there are no real contraindications in patients with an intact scalp and skull. However, caution is required when securing electrodes to the head when open scalp wounds are present, following craniotomy, and when the integrity of skin on the scalp is otherwise compromised. In some situations where the scalp wound is particularly large, it may be impossible to place electrodes in some areas, limiting standardized application. However, a modified montage to accommodate patients following neurosurgery, particularly craniotomy or craniectomy, can be used with high specificity, though there is variable sensitivity depending on the array used (74). Needle electrodes are not recommended for routine use, even in nonsurgical patients undergoing EEG (104).
Many patients undergoing cEEG will need an MRI for further evaluation of the cause of the patient’s neurologic condition. Typically, EEG electrodes are not MRI compatible, so the patient would need to be removed and unhooked from the EEG machine in order to obtain MRI studies unless MRI-compatible electrodes are used (79).
Additionally, for some younger children and other patients who are combative or unable to cooperate with the test, sedation may be required for EEG lead placement. In this case, the risks of using sedation must be contrasted with the benefits of continuous EEG monitoring and are assessed on a case-by-case basis.
As it is a noninvasive procedure, continuous EEG has limited adverse effects. EEG electrodes may cause pressure on the skin sites when used for long-term applications over several days. The electrodes are regularly examined to prevent skin breakdown. At times, it may be necessary to remove and stagger the electrodes to alternate adjacent sites or temporarily suspend monitoring to promote skin healing (58). Additionally, infection is a potential adverse effect that can be minimized by regular daily care by the technologist. Electrodes should be regularly disinfected to avoid skin or wound infections, and special care should be used in patients with active transmissible diseases. Disposable electrodes can be considered to avoid this risk (104).
Duration. If seizures are detected and treatment begun, continuous EEG monitoring should be continued for at least 24 hours after cessation of seizures (42). In situations where a continuous infusion of antiseizure or sedative drug is necessary for seizure control, most clinicians continue EEG monitoring for at least 24 hours following discontinuation of the continuous infusion, sometimes longer depending on the half-life of the drug (02).
There is considerable debate regarding the optimal duration of EEG monitoring to adequately screen for nonconvulsive seizures or nonconvulsive status epilepticus. A routine (30-minute) EEG is likely inadequate as only about 50% of nonconvulsive seizures will be detected in this time period (16; 112; 39). Monitoring should be performed for no fewer than 12 hours in patients with a clinical indication for cEEG monitoring (108), but most clinicians will use continuous EEG monitoring for at least 24 to 48 hours (02; 34; 108). Some have shown that 80% to 88% of nonconvulsive seizures or nonconvulsive status epilepticus will be detected in the first 24 hours and 87% to 93% in the first 48 hours whereas the remaining patients require more than 48 hours of cEEG monitoring during the course of treatment (16; 49). However, this may depend on the EEG pattern when first being monitored and the clinical indication for EEG and clinical circumstances.
Specific EEG patterns, such as diffuse slowing without other abnormalities, are associated with a low risk of nonconvulsive seizures developing later during cEEG monitoring, and a shorter duration of EEG monitoring can be considered in those patients (112) or may even be deferred in specific clinical situations if there are no epileptiform discharges (108). However, decreased background reactivity (49), epileptiform discharges (103; 132; 100; 107), periodic discharges (16; 49; 112; 107), lateralized rhythmic delta activity (107), and burst suppression (16) are correlated with a higher risk of seizures and longer monitoring is warranted in these situations.
Specific risk factors can also be considered with EEG patterns to stratify which patients may require a longer duration of cEEG monitoring. One study recommended the following durations of monitoring: (1) noncomatose patients with no history of seizures and no EEG abnormalities should receive a standard EEG; (2) patients who are either comatose, have EEG abnormalities, or have a history of seizure should get at least 24 hours of cEEG monitoring; and (3) patients with a history of seizures, are comatose, and have epileptiform abnormalities on EEG require at least 48 hours of cEEG monitoring (107). Once nonconvulsive seizures or nonconvulsive status epilepticus are detected, cEEG monitoring is continued for at least 24 hours following seizure cessation or 24 hours after discontinuation of a continuous antiseizure drug infusion, if one is being used (02; 42).
When considering the duration of cEEG monitoring after cardiac arrest, whether for prognostication or clinical management, there is no clear consensus. One study showed no benefit in cEEG monitoring as opposed to briefer intermittent studies, specifically in adding more data for prognosis, but was more sensitive in detecting ictal activity (24). The sensitivity to detect seizure activity was also observed with longer cEEG monitoring in another study, but was attributed to weaning of sedation later in the course of treatment, and the detection of ictal activity did not appear to add to prognostication in all cases (76). The early EEG pattern may also be important in determining the length of cEEG, given that a “benign” EEG in the first 12 hours after arrest is a good indicator of a positive prognosis and longer cEEG monitoring would not be needed (120). Further, a study suggested that aggressive treatment of rhythmic or periodic EEG patterns in comatose survivors of cardiac arrest did not have any effect on outcomes (97). Therefore, the use of cEEG to monitor and treat may not be beneficial if these patterns are encountered. See Table 3 for recommendations on the duration of EEG monitoring based on the clinical situation.
|
Goal of Monitoring |
Recommended Duration of cEEG Monitoring |
|
Seizure urgencies and emergencies |
24 to 48 hours, shorter or longer depending on risk factors |
|
Assessment of efficacy of therapy for nonconvulsive seizures or nonconvulsive status epilepticus |
24 hours of seizure freedom or for 24 hours after discontinuation of continuous infusion |
|
Identification of cerebral ischemia |
For subarachnoid hemorrhage: within 3 days of hemorrhage onset until 14 days post-hemorrhage or when risk for vasospasm is felt to diminish |
|
Monitoring the level of therapeutic sedation or burst suppression |
Individualize to clinical situation |
|
Assessment of severity of encephalopathy and prognostication in brain injury |
No consensus on longer-term monitoring versus 30 minutes of EEG |
|
| |
When cEEG is used to detect ischemia, the duration of cEEG monitoring depends on the underlying risk factors and the time when the patient is most susceptible to developing ischemia. Monitoring for ischemia in non-subarachnoid hemorrhage patient groups (where 3-14 days is high risk) is often limited to 24 to 48 hours (42). Limited information exists to define the optimal duration for cEEG monitoring during iatrogenic sedation and for prognostication, and, therefore, the decision of how long to continue cEEG monitoring in these situations must be individualized.
Patient selection. Patients with a variety of clinical conditions with neurologic involvement may benefit from information obtained during cEEG monitoring (42). These conditions are listed in Table 4.
|
Clinical history |
NCS/NCSE detection |
Response to antiseizure medications |
Sedation monitoring |
Prognostication |
Detection of ischemia from vasospasm |
|
Convulsive status epilepticus without return to neurologic baseline; refractory status epilepticus |
X |
X | |||
|
Altered mental status in any clinical context |
X | ||||
|
Subarachnoid hemorrhage |
X |
X |
X |
X | |
|
Intracerebral hemorrhage |
X | ||||
|
Acute ischemic stroke |
X | ||||
|
Coma after TBI |
X |
X |
X | ||
|
Coma after cardiac arrest |
X |
X |
X |
Case 1. A 55-year-old man with a history of right hemispheric ischemic stroke, coronary artery disease, and hypertension became unconscious shortly after calling out to his wife with chest pain. She immediately called 911 and began bystander CPR. Upon EMS arrival, CPR was continued, and the automatic external defibrillator monitor was placed on him. He was found to be in pulseless ventricular tachycardia. He was successfully resuscitated following defibrillation and advanced cardiac life support, with return of spontaneous circulation. He required intubation in the field for airway protection due to persistent alteration in mental status manifest as coma.
On arrival to the emergency room, the ECG ruled out a ST-segment elevation myocardial infarction. He remained unresponsive, with intact pupil and corneal responses, but no gag or cough reflexes and no motor response to pain. He did not require sedation to facilitate ventilation. Emergency consultations with both cardiology and neurology were placed, and temperature control and fluid balance were begun during initial investigation with laboratory, chest x-ray, and cardiac monitoring. Treatment was started with antihypertensives, vasodilators, and targeted hypothermia.
The consulting neurologist ordered a STAT EEG to evaluate the patient for subclinical seizures. During the 30-minute standard EEG, lateralized periodic discharges were noted in the right hemisphere that were maximal in the frontal region, recurring at 1 Hz without evolution but some of the lateralized periodic discharges showed superimposed beta activity.
Given concern for the ictal potential of the lateralized periodic discharges associated with fast activity, the standard EEG was converted to cEEG. Approximately 30 minutes after the cEEG was initiated, recurrent electrographic seizures were captured arising from the right hemisphere. There was no clinical correlate identified (nonconvulsive status epilepticus). As a result, the patient was administered 4 mg of lorazepam intravenously. This was followed by 2 grams of levetiracetam and 1800 mg of valproate, resulting in cessation of the subclinical seizures. He was subsequently begun on a maintenance dose of 1000 mg of levetiracetam twice daily and 500 mg valproate three times daily. The lateralized periodic discharges continued but lessened in their frequency and spatial distribution. No further seizures were detected over the next 24 hours of cEEG monitoring, and the patient ultimately survived and was transferred to a rehabilitation facility.
Case 2. A 72-year-old woman with a history of diffuse large B-cell lymphoma status after chemotherapy with secondary myelodysplastic syndrome was admitted for hematopoietic stem-cell transplantation. The patient developed an altered mental status during her hospital course, complicated by acute kidney injury. On day 11 of her treatment, she developed sepsis and was initiated on broad-spectrum antibiotic treatment with cefepime. Over the next 3 days, she developed waxing and waning mental status, and there was concern for the possibility of nonconvulsive seizures or status epilepticus as a cause. Cefepime was replaced with meropenem, and an EEG was ordered for further evaluation.
In response to the EEG, the patient received empiric treatment with 2 mg intravenous lorazepam, as well as an intravenous load of 3500 mg levetiracetam; there was a reduction in the generalized periodic discharges, but no clinical improvement. The generalized periodic discharges, which reappeared shortly after, waxed and waned, appearing state- and stimulus-dependent. A dose of 200 mg of lacosamide was also loaded intravenously. There was still no clinical response to these treatments, and the EEG results remained unchanged. The patient was monitored for 49 hours, with the generalized periodic discharges waxing and waning with state- and stimulus-dependence and becoming less frequent on the final day of monitoring. No EEG or clinical seizures were recorded. Continuous EEG monitoring was discontinued. A routine EEG was performed 2 days later, with resolution of the previously seen generalized periodic discharges and demonstrated mild diffuse slowing. The patient also demonstrated improved mental status.
|
• Continuous EEG is foundational and required for the diagnosis and characterization of nonconvulsive seizures or nonconvulsive status epilepticus. | |
|
• There are diagnostic clinical and EEG features that indicate high-risk patients for nonconvulsive seizures/nonconvulsive status epilepticus to help select patients for cEEG monitoring. | |
|
• There are therapeutic implications for cEEG that include assessing the efficacy of therapy for nonconvulsive seizures or nonconvulsive status epilepticus, identifying cerebral ischemia in subarachnoid hemorrhage, monitoring sedation and suppression-burst activity, and prognosis in brain injury due to trauma, hypoxia, or anoxia, particularly after cardiac arrest. | |
|
• There is significant variability in the incidence of nonconvulsive seizures/nonconvulsive status epilepticus and no uniform use by practitioners despite clinical practice guidelines for cEEG in critically ill patients, and more information and education are needed to better guide clinicians to optimize patient care. | |
|
• In emergent situations, full and reduced montage rapid EEG devices allow for quick assessment of patients to rule out nonconvulsive status epilepticus and are particularly useful in resource-limited situations; however, they are not currently designed to supplant or replace standard EEG recordings. | |
|
• Quantitative EEG techniques are becoming more commonly used and may help overcome the current challenges regarding how often cEEG studies are interpreted. | |
|
• Artificial intelligence using deep learning paradigms can further enhance the sensitivity and specificity of ICU EEG interpretation and holds promise in improving the efficiency of cEEG analyses to accommodate increasing utilization of EEG monitoring. |
In cases of convulsive status epilepticus that have ceased, diagnosing subsequent nonconvulsive seizures and nonconvulsive status epilepticus in patients who remain comatose is difficult because electromechanical dissociation occurs, and clinical manifestations are faintly perceptible if present at all, despite ongoing electrographic seizures (59). As such, EEG is vital in these cases.
The importance of diagnosing and treating nonconvulsive seizures and nonconvulsive status epilepticus lies in the finding that electrographic seizures themselves are associated with metabolic crisis. This has been demonstrated by using microdialysis to measure decreased oxygen and glucose levels in interstitial brain tissue, suggesting an increased regional cerebral metabolic rate, and along with delayed increase in cerebral blood flow, secondary neuronal injury and worsening clinical outcomes can occur (126; 133). The duration of seizures and status epilepticus has a positive correlation with these findings (126). Even EEG features that lie on the ictal-interictal continuum that do not necessarily indicate frank seizures may also cause secondary neuronal injury due to metabolic demand outpacing blood flow and oxygen delivery and may warrant treatment (133).
Further highlighting the need for urgency in treating nonconvulsive status epilepticus is the association between seizure duration and subsequent internalization of GABA receptors and an increase in NMDA excitatory receptor activity (130). Therefore, first-line antiseizure treatments such as benzodiazepines lose their efficacy over time, making treatment more difficult the longer seizures go without complete cessation.
The amount of data being acquired using cEEG also poses challenges, even in larger facilities where resources for performing cEEG require periodic calibration, sophisticated informatics support, software updates, and adequate storage capacity. Neurophysiologists must accurately review a large amount of data within a short time to ensure timely diagnosis and treatment, and some hospitals may not have 24/7 EEG reading available to them. This may require them to rely on non-neurophysiology-trained clinicians to interpret EEGs in real-time and act upon them as quickly as possible (63). Quantitative cEEG and pEEG allow for simplified, compressed displays of EEG data (101; 93). Seizures or activity on the ictal-interictal continuum can then be screened in using quantitative software, improving sensitivity and allowing for quicker diagnosis and treatment. Some quantitative EEG systems have programmable settings, including seizure detection modes (eg, Persyst®, Solana Beach, CA) that can send de-identified .PNG files as emails for both EEG and quantitative EEG panels as images. These can help resource-limited hospitals without access to 24/7 EEG technology coverage to observe continuous EEG for targeted events. These events can then be reviewed by a remote reader, and management changes can be coordinated with the onsite team for any necessary adjustments. An example of an EEG epoch and quantitative EEG is taken from a patient with new-onset refractory status epilepticus who was induced into suppression-burst pattern using pentobarbital.
There is increasing use of cEEG as more evidence demonstrates utility, particularly in diagnosing nonconvulsive seizures/nonconvulsive status epilepticus (81). Despite the concern that nonconvulsive status epilepticus may lead to worsened outcomes with delayed treatment, there is significant variability in the use of cEEG among hospitals in the U.S., Canada, and internationally (88; 60). The reason for this lies in the resources needed to support cEEG, including qualified neurophysiologists, equipment, and trained EEG technologists (60). As noted above, rapid EEG systems may allow many centers and hospitals without these resources to have cEEG capability in their institutions to assist with critically ill patients.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Brin Freund MD
Dr. Freund of Mayo Clinic Florida received research contracts or grants from NeuroOne and UniQure and honorariums from Xenon and UCB as a consultant/advisor.
See ProfileW David Freeman MD
Dr. Freeman of Mayo Clinic Florida has no relevant financial relationships to disclose.
See Profile
William O Tatum IV DO FACNS
Dr. Tatum of Mayo Clinic Florida received consulting stipends from Neurelis and consultant fees from Synergy Medical Solutions.
See Profile
John M Stern MD
Dr. Stern, Director of the Epilepsy Clinical Program at the University of California in Los Angeles, received honorariums from Ceribell, Jazz, LivaNova, Neurelis, SK Life Sciences, and UCB Pharma, and Xenon as advisor and/or lecturer.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jul. 08, 2026
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Epilepsy & Seizures
Jun. 02, 2026
Neuro-Oncology
May. 27, 2026
Movement Disorders
May. 18, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
General Neurology
May. 13, 2026
Neuropharmacology & Neurotherapeutics
May. 11, 2026