


Epilepsy & Seizures
Febrile seizures
Jun. 02, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
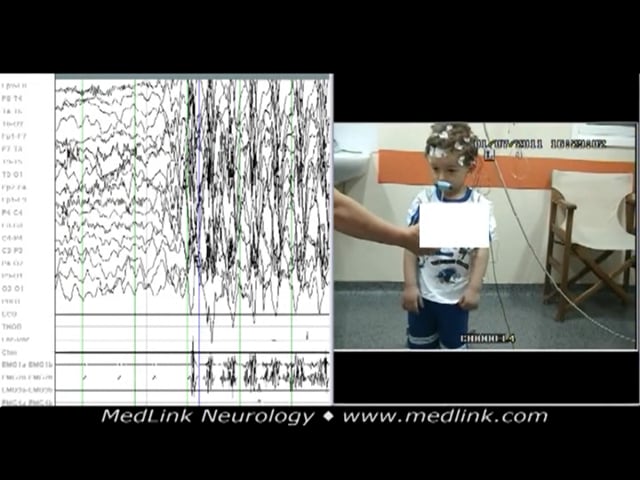
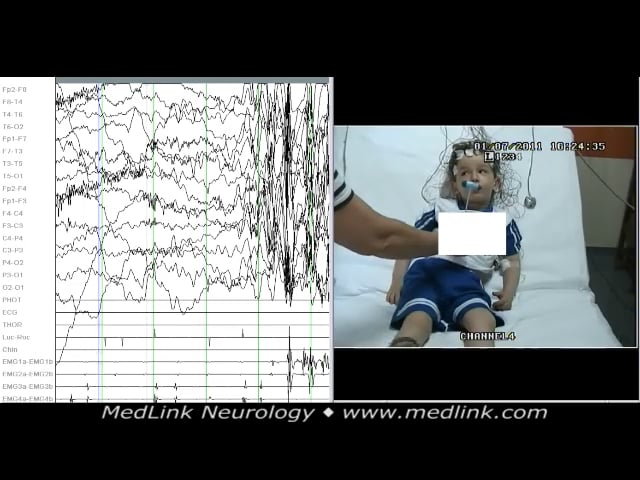
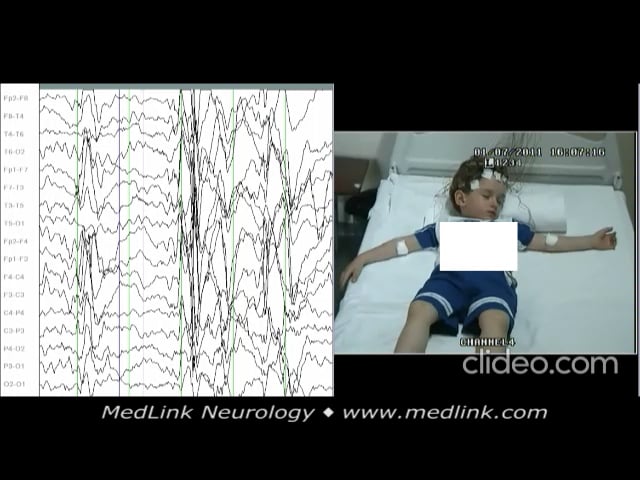
Epilepsy with myoclonic absences is a rare genetic (idiopathic) generalized epilepsy syndrome characterized by frequent (daily) myoclonic absences of abrupt onset and abrupt termination. The age of onset varies from 11 months to 12.6 years (mean 7 years). In contrast to childhood absence epilepsy, where there is a female preponderance (70%), in epilepsy with myoclonic absences, 69% are boys (M: F=2.2:1). Epilepsy with myoclonic absences presents with particular clinical and EEG characteristics. The clinical presentation is characterized by typical absence seizures associated with rhythmic and bilateral severe myoclonic jerks, mainly of the upper body, with a tonic component. The concomitant tonic contraction suddenly raises the arms that start jerking rhythmically. When the patient stands, the upper limbs fling open (tonic phase) and elevate progressively as they jerk; the body may deviate slightly and bend toward the floor with each rhythmic jerk. On EEG, the polygraphic recording shows bilateral rhythmic generalized spike-wave discharge at 3 Hz that is bilateral, synchronous, and symmetric.
At presentation, about 45% to 55% of patients are neurologically and developmentally normal, but nearly 70% eventually develop cognitive dysfunction. In 50% of patients, seizures persist past 20 years of age, particularly in those with generalized tonic-clonic seizures and atonic seizures and those who evolve to Lennox-Gastaut syndrome.
Early control of clinical and EEG characteristic features may prevent subsequent cognitive deterioration and secure better developmental evolution.
|
• Epilepsy with myoclonic absences is a rare generalized epilepsy syndrome of childhood characterized by myoclonic absences. The mean age of onset is 7 years (range 11 months to 12.6 years), and about 69% are boys. | |
|
• Typical absence seizures consist of impairment of consciousness (mild to severe) and bilateral, rhythmic, and severe myoclonic jerks, mainly of the upper body, with a concomitant tonic component. | |
|
• Ictal polygraphic EEG shows rhythmic generalized spike-wave discharge at 3 Hz that is bilateral, synchronous, and symmetric. | |
|
• Correct diagnosis of this specific seizure type rests on direct clinical observation and polygraphic video-EEG recording. | |
|
• The classical treatment is valproic acid monotherapy, usually combined with ethosuximide in appropriate daily doses. |
Myoclonic absences were recognized as a specific type of seizure in 1969 (32). In 1985, it was recognized that myoclonic absences were a different seizure type, and “Tassinari syndrome” was proposed as a specific syndrome wherein myoclonic absences were the only or the predominant seizure type (30). Absence seizures combined with marked clonic or myoclonic components were reported a few years earlier (18). Epilepsy with myoclonic absences was recognized as a syndrome by the International League Against Epilepsy in 1989 (Commission on Classification and Terminology of the ILAE 1989). The commission did not consider the idiopathic type; they classified epilepsy with myoclonic absences among cryptogenic or symptomatic idiopathic generalized epilepsies. Subsequent publications from the same commission classified only the idiopathic form among the idiopathic generalized epilepsies as a syndrome in childhood (14; 15; 03). However, almost two thirds of cases with myoclonic absences belong to the symptomatic or probably symptomatic group.
In the last ILAE classification of epilepsy syndromes with onset in childhood, some syndrome names have been updated using terms directly describing the seizure semiology, such as epilepsy with myoclonic absence (formerly known as Tassinari syndrome) and epilepsy with eyelid myoclonia (formerly known as Jeavons syndrome) (27).
Absence and myoclonic seizures predominate in the phenotypes of epilepsy with myoclonic absences, eyelid myoclonia with and without absences, and facial myoclonia with absences (10).
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125