
Sleep Disorders
Sudden infant death syndrome
Jul. 05, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Irregular sleep-wake rhythm disorder (ISWRD) is characterized by the absence of circadian synchronization with an individual’s sleep-wake cycle, which results in at least three major and several minor periods of sleep spread across the 24-hour period. Irregular sleep-wake rhythm disorder is typically seen in children with neurodevelopmental disorders and adults with neurodegenerative disorders, such as Alzheimer dementia, or institutionalized elderly patients, and has also been observed in patients with traumatic brain injury. Increased exposure to circadian zeitgebers, such as bright light and structured activities, may minimize the disturbance, but evidence is limited. Pharmacologic therapy with melatonin was generally ineffective in randomized control trials despite encouraging results in small open-label studies. This article enables a basic understanding of the circadian clock biology and its interactions with the sleep-wake cycle.
|
• Individuals with irregular sleep-wake rhythm disorder present as fragmented sleep at night and multiple naps during the day. | |
|
• Patients lack a clearly defined single major sleep period but demonstrate multiple irregular sleep bouts (at least three). | |
|
• Irregular sleep-wake rhythm disorder is commonly seen in elderly institutionalized patients, adults with neurodegenerative disorders, or children or adults with neurodevelopmental disorders. | |
|
• The irregular sleep wake rhythm may contribute to further decline in cognition and mood. | |
|
• Loss of neurons in the suprachiasmatic nuclei (SCN), age-related changes in melatonin/pineal secretions, and decreased exposure to zeitgebers may contribute to the presence of irregular sleep-wake rhythm disorder. | |
|
• Other medical, neurologic, or psychiatric disorders and medication side-effects may contribute to the sleep-wake cycle disruption. | |
|
• Multimodal therapy that includes a combination of timed light and melatonin treatment and nonpharmacological interventions like scheduled contacts, physical activity, and enriched environment may improve the sleep-wake pattern. |
The basis of biological rhythms and cycles in humans has long been a point of interest. Kleitman described a variety of changes across these approximately 24-hour cycles (19). The term “circadian” was introduced by Halberg in 1959 to account for both the day and nighttime phenomena of the rhythm (13; 25). Descriptions of aberrant rhythms followed, postulating that they may be an indication of health issues or have a direct impact on health (25). The current formal name established in the third edition text revision of the International Classification of Sleep Disorders is irregular sleep-wake rhythm disorder (02). However, irregular sleep-wake disorder was recognized as an issue involving the circadian pattern for decades prior to the classification (17).
|
• Irregular sleep-wake rhythm disorder presents with an erratic schedule of sleep and wake interspersed across the 24-hour time frame, typically with no clear major repeating period of sleep. | |
|
• Patients and their caretakers may complain of the patients having excessive daytime sleepiness, insomnia, or both. | |
|
• Although these types of schedules are sometimes brought on voluntarily, they can also indicate underlying neurodevelopmental, neurodegenerative, or other neurologic maladies. |
Irregular sleep-wake rhythm disorder presents when a patient or caregiver reports chronic or recurrent patterns of sleep or irregular sleep-wake episodes throughout a 24-hour period. The chief complaint may be a various combination of sleep-onset insomnia, poor sleep maintenance at night, or excessive daytime sleepiness with frequent napping. These patients or caregivers note symptoms of insomnia at night or excessive daytime sleepiness that result in no clear pattern of sleep-wake cycle (02). Symptoms must be present for at least 3 months; sleep logs should be kept, and, if possible, actigraphy should be performed for at least 7 days (preferably 14 days), documenting no major sleep period and three or more irregular sleep bouts during a 24-hour period. For many, the longest sleep period is typically between 2:00 AM and 6:00 AM, although this is commonly not seen. The unpredictability of the timing of sleep or wake is a key feature.
Irregular sleep-wake rhythm disorder is commonly seen in patients with neurodevelopmental or neurodegenerative disorders. The most common neurodegenerative disorder associated with this sleep-wake pattern is Alzheimer disease, although it can be seen in other disorders such as dementia with Lewy bodies, vascular dementia, Parkinson disease, multisystem atrophy, and Huntington disease (40). Irregular sleep-wake disorder may also be seen in children with neurodevelopmental disorders such as Angelman syndrome, Smith-Magenis syndrome, autism, Asperger syndrome, or pervasive developmental disorder. In patients with particularly severe cognitive impairment, a rudimentary circadian sleep-wake pattern may be present, comprised of short (2- to 3-hour) periods of interrupted sleep alternating with quiet wakefulness but punctuated once a day by a period of agitated wakefulness occurring at nearly the same time every day. Families may also complain that patients are seldom awake during daytime visits. Patients with bipolar disorder may also have irregular sleep-wake schedules that appear associated with more frequent depressive episodes (29).
Irregular sleep wake rhythm may also start in part related to poor sleep hygiene (36). This irregular pattern of sleep may also predispose adolescents to further mood and impair attention (29; 07; 21). Similarly, the pattern is associated with decrease in cognitive function in older adults (30). Although the presence of the pattern may be an early indicator of underlying neurologic issues, improvement in the sleep pattern shows improvement in the symptoms (07).
In general, prognosis and course of these disorders are largely unstudied but most likely follow the course of the underlying process. Clinical experience suggests the prognosis is dependent on the chronicity, severity, and underlying cause of the disorder. Some individuals may have opted for the irregular schedule due to poor sleep hygiene and may improve in mood and function with a regular schedule (07; 36). Individuals who are early in the course with mild disease tend to do better for the short term than individuals with severe chronic debilitating disease. Some individuals, especially those with certain developmental disorders, chromosomal syndromes, or severe dementia, will have minimal response to conservative therapies (36). Others, such as those with post-concussive issues, have a better chance of responding to a combination of light, daily activity, and melatonin. Pharmacologic therapy in the form of hypnotics and neuroleptics are often initiated due to complaints of insomnia from either patients or caregivers and may exacerbate symptoms. Hypnotic dependence may occur in the cognitively intact, whereas significant drug toxicity can occur in patients with neurodegenerative disorders, particularly in the elderly. Disturbance of the caregiver's sleep by nocturnal agitation or wandering in the home setting leads to caregiver fatigue and is a frequent cause of institutionalization.
Additional evidence raises the possibility that an irregular sleep schedule may increase the likelihood of atherosclerotic disease and mortality. Dong and colleagues found that railway workers who had irregular sleep wake schedules had higher risk of dyslipidemia (09). Similarly, in a United Kingdom Biobank prospective analysis of nearly 89,000 participants, Cribb and colleagues found that those with irregular sleep had a higher mortality of cardiovascular disease and cancer (06). Irregular sleep patterns appear to have an impact on not only cardiometabolic disease but also mortality. Regular sleepers with optimal sleep duration had 39% lower mortality than subjects with irregular and insufficient sleep (16). These studies suggest the irregular sleep wake timing may play a role in the higher disease risk, but it is unclear if this is related to volitional changes in the sleep wake timing or related to an underlying circadian rhythm disorder.
An 82-year-old male presented to the sleep clinic with his family with complaints of sleep onset, maintenance insomnia, and excessive sleepiness during the day. The patient was residing in a nursing home due to Alzheimer disease. The family reported the patient to “always be sleeping” when they came to visit him during the day, and the lights were often off and the window shades were closed. He frequently became agitated during early evening hours. At night, he slept 1 to 2 hours, usually in the beginning of the night, and then he remained awake for the remainder of the night, but would intermittently doze. Multiple pharmacologic agents had been tried without success to help the patient sleep at night, including zolpidem, trazodone, quetiapine, and lorazepam. Some of these medications increased his confusion. Due to his nocturnal vigilance and confusion, the nursing staff noted difficulties in keeping up with his schedule. The nursing staff also reported difficulty in having the patient participate in daily activities due to his excessive daytime sleepiness from not getting restful sleep at night. The nursing staff was instructed to turn the lights on in his room at 6:00 AM and to open his window shades at that time to expose the patient to natural bright light. Structured activities were added during the day to diminish the opportunity to sleep. This schedule of full daylight exposure and structured events improved his sleep-wake schedule and his participation in daytime activities. A relatively consolidated period of night sleep between 10:00 PM and 4:00 AM appeared, with a daytime 1- to 2-hour nap in the late morning.
Although large pathological studies are lacking, we believe the irregular sleep-wake pattern in developmental and degenerative disorders of the brain may result from lesions in or degeneration of the endogenous circadian timing system in the hypothalamus, or its connections, or of systems mediating sleep and arousal. Reduced melatonin secretion by the pineal gland and decreased exposure to zeitgebers also play a role in the development of irregular sleep-wake rhythm disorder. Some of the developmental disorders, such as Smith-Magenis syndrome, are found to have profoundly disturbed melatonin secretion profiles. For those with advancing medical issues, inhibition of other circadian clues, such as alterations in the ability of the eyes to transmit and receive light as seen in age-related cataracts and macular disorders, can contribute to irregular sleep-wake rhythm disorder. Lack of structured physical and social activities can contribute to the loss of circadian cueing. Medications, such as beta-adrenergic blockers, may block the release of melatonin, and other medical, neurologic, or psychiatric disorders may contribute to the sleep-wake cycle disruption. In some cases, multiple factors may also play a role. Kokash and Vendrame report on two individuals who developed irregular sleep wake rhythm disorder after gender reassignment and hormone replacement therapy (20). Each of these cases indicates the importance of identifying possible modifiable factors contributing to the circadian disruption.
Review of circadian mechanisms. All living organisms possess an inherent circadian rhythm. This near 24-hour cycle modulates a variety of physiologic and behavioral processes, such as sleep-wake cycle, body temperature, mood, hormone secretion, and many others. The paired suprachiasmatic nuclei of the hypothalamus have been established as the “master clock” that sets the timing of the mammalian circadian system. The suprachiasmatic nuclei are composed of 10,000 anterior ventromedial hypothalamic neurons that maintain a self-sustaining daily rhythm. This cycle is achieved through a complex system of timed gene expression that creates an autoregulatory feedback loop. A variety of genes are involved in this cycle, including Clock, Per, Bmal1, and Cry. Changes in these genes or those related to proteins that regulate the core genetic clock can result in circadian rhythm disruption (22).
The biological clocks of normal humans of all ages have a natural endogenous circadian cycle of slightly more than 24 hours, generally about 24.2 hours. Therefore, the internal body clock must be adjusted on a daily basis to align with the 24-hour day, a process called entrainment. Entrainment involves using zeitgebers (German for “time givers”) to reset the internal clock slightly each day. Common zeitgebers include light, melatonin, food intake, social interaction, and exercise. Each of these factors can independently change the timing of the circadian pacemaker, thereby altering the time of all physiologic processes that are regulated on a circadian basis.
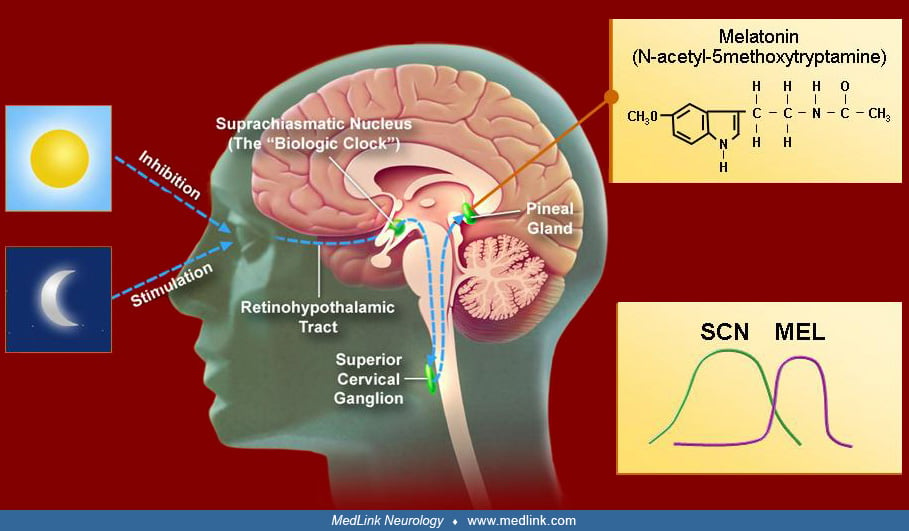
Light is the main zeitgeber for endogenous clocks in humans. The human circadian system is more sensitive to short-wave, blue-green light than to long-wave red-spectrum light. The major afferent input to the SCN consists of a melanopsin-containing subset of photosensitive retinal ganglion cells whose axons synapse on SCN cells.
This retinohypothalamic tract transmits nonvisual, light-dark information to the SCN, which is mediated through glutamate and pituitary cyclase-activating peptide. In addition to a direct pathway, retinal ganglion cells also project to the intergeniculate leaflet of the lateral geniculate body, which, in turn, projects to the SCN. Neuropeptide Y and GABA are the main neurotransmitters. Other time clues appear to influence the SCN through serotonergic input from the brainstem raphe nuclei.
The key to understanding the zeitgebers is that the response of the circadian rhythm depends on when the stimulus is delivered. For example, light delivered prior to the temperature nadir (typically 4:00 AM in normal phase individuals) will cause a delay in the body clock. Light delivered after the body temperature nadir will advance the clock. Thus, for light therapy to be appropriately used, understanding the true timing of the circadian rhythm is essential. The temperature nadir is typically 1.5 to 2 hours before the undisturbed natural wake-up time. Therefore, if a person is naturally waking at 11:00 AM without an alarm, the temperature nadir would most likely be between 9:00 and 9:30 AM.
Similar to light, melatonin also has a time-dependent effect on the phase of the circadian rhythm. Melatonin is produced during darkness periods and is suppressed by light of sufficient duration and intensity, but melatonin has its own endogenous rhythm in which the peak occurs during the evening several hours prior to the nadir of core body temperature. The melatonin circadian rhythm is highly robust, has low intra-individual but high inter-individual variability, and is appreciably masked only by light. Because melatonin is also governed by an endogenous circadian rhythm, individuals will typically have a pulse of melatonin release in the evening when it would be dark. The time of this dim light melatonin onset can be a clue to the circadian rhythm timing and is currently used as a marker of the circadian phase (24). Exogenous melatonin delivered at different times has the opposite effect of light, such that melatonin delivered in the evening causes a phase advance, whereas morning use may cause a mild phase delay. The SCN exhibit dense melatonin receptors, likely establishing a feedback mechanism for the sleep-wake cycle. Melatonin and other potential factors, such as light, help synchronize the multitude of endogenous rhythms in the brain and other organs. Synchronization of these endogenous rhythms is important to optimal body function (34).
Neurodegenerative disorders usually affect older individuals, and these individuals, even when healthy, tend to exhibit an earlier bedtime and morning awakening. Healthy elderly tend to show a circadian phase-advancement and sleep phase-advancement, as well as less consolidated sleep (31; 28). The elderly may exhibit changes in interrelationships (the phase-angle difference) between the master circadian rhythm (manifest as melatonin and core body temperature rhythms) and sleep-wake cycle, particularly the shortening of the time between core body temperature nadir and the habitual waking time. The changes in sleep consolidation and in sleep timing in the healthy elderly may be due to a reduction in the homeostatic drive for sleep and in the circadian drive that promotes sleep in the early morning (18).
The pathogenesis of irregular sleep-wake rhythm disorder is thought to be due to a reduction of exposure to zeitgebers in the face of changes of SCN functioning, whether through normal aging, developmental issues, or neurodegeneration of the circadian system (04; 40).
The observed output of the suprachiasmatic nucleus may become affected by degenerative changes in its input sources or outflow target systems. This may cause disorganized circadian rhythms reflected in part by a disorganized sleep-wake schedule. Alzheimer dementia can cause neuropathologic changes to the circadian pacemaker in the SCN with the presence of tangles and amyloid plaques (04; 40). Patients with Alzheimer disease may have decreased activity of the SCN through decreased vasopressin and neurotensin neurons and increased glial fibrillary acidic protein astrocytes (39). In addition, animal studies have shown age-related reduced gene expression of light stimulation–induced per1 and per2. Decreased secretion of melatonin by the pineal gland has been observed in patients with Alzheimer dementia. Similar changes have been seen in models of Huntington disease (27). Thus, the destruction of neurons of the SCN can result in alterations in circadian regulation and presence of irregular sleep-wake rhythm disorder.
At the cellular level, expression of melatonin receptors in the SCN is reduced, thus, causing a disruption of the feedback loops serving normal circadian function and circadian influence on sleep.
Decreased exposure to zeitgebers plays a pivotal role in the development of irregular sleep-wake rhythm disorder. Light is important for circadian entrainment. Light is transmitted through the lens synapsing on retinal ganglionic cells containing melanopsin, which are sensitive to blue wavelength light. The retino-hypothalamic neurons utilize glutamate and pituitary adenylate cyclase-activating peptide in transmitting light information to the SCN. Loss of these retino-hypothalamic hair-like axons may contribute to the circadian disruption in traumatic brain injury. Patients with dementia, and especially those that are institutionalized, have reduced environmental clues such as light exposure due to being inside and daytime napping. These individuals may benefit from daily light therapy to accentuate sleep-wake rhythms, which appears to reduce agitation (11). Daytime napping also limits participation in important social and physical activities that are critical inputs to the maintenance of the circadian rhythm. In addition, patients with primary eye disorders, such as cataracts and macular disorders (influencing the retinal ganglion cell layer), have decreased light input to the SCN, which can potentially result in dysfunction of the internal clock.
No exact information is available. However, the pattern of irregular sleep is common in institutionalized patients with neurodegenerative disorders, yet the true frequency of the disorder is unknown (40).
Some animal models of degenerative disorders suggest that enhancing the circadian environmental clues may delay the symptoms of the degenerative process. In both sheep and mice, Morton showed that maintaining circadian clues delayed the symptoms of Huntington disease (27).
The clinician should be alert to first differentiate poor sleep hygiene and voluntary maintenance of an irregular schedule from the involuntary irregular sleep-wake pattern. Some patients with very poor sleep hygiene may demonstrate an irregular sleep wake pattern that quickly reverts with an imposed schedule. Similarly, fragmented sleep-wake cycles may be a result of comorbid psychiatric and medical disorders. Older individuals with current or remitted depression may report more irregular schedules and poor sleep quality reminiscent of irregular sleep-wake pattern (32; 16). Other circadian rhythm sleep disorders, such as delayed sleep-phase syndrome, advanced sleep-phase syndrome, and non-24-hour sleep-wake disorder, should be ruled out, and medication side effects need to be considered. This is especially true in visually impaired individuals who are more likely to subjectively endorse an irregular sleep-wake pattern (37). For these individuals, further investigation using actigraphy or sleep log to differentiate the non-24-hour sleep-wake disorder from true irregular sleep-wake disorder is important (02).
|
• Irregular sleep-wake rhythm disorder requires a minimum of 14-day actigraphy or a sleep diary. | |
|
• Actigraphy should demonstrate that there is no major sleep period; however, sleep occurs multiple (at least three) periods in the 24-hour day. |
Evaluation of irregular sleep-wake rhythm requires an understanding of the rest activity pattern over several days. Although patients may report a random occurrence of sleep and wake, tracking the rest and activity episodes will provide a better ability to visualize the exact pattern. Actigraphy and sleep-wake logs can be used to diagnose irregular sleep-wake rhythm disorder (03). Sleep logs or diaries tend to be less reliable than actigraphy as reports are highly subjective based on caregiver observations, and patients are cognitively impaired. Actigraphy involves wearing a wrist sensor on the nondominant hand to record body movements. Actigraphs in patients with irregular sleep-wake rhythm disorder reveal little temporal consistency of sleep onsets or wake times. Sleep occurs in three short (less than 4 hours) interrupted "naps" during each 24-hour period. Marked and unpredictable day-to-day variability in the timing of sleep and wakefulness is present for at least a 3-month time period. Both actigraphy and sleep logs need to be performed for at least 7 days and preferably for 14 days to adequately diagnose irregular sleep-wake rhythm disorder.
|
• Treatment strategies are targeted at entrainment and accentuation of the intrinsic circadian pacemaker. | |
|
• Treatment for irregular sleep-wake rhythm disorder should focus on daytime and nighttime clues. |
Management should focus on two roles: accentuating the clues of the environment and providing for the safety of the patient. Time clues and zeitgebers (ie, light, activity, meals, and social interaction) should be delivered during time periods that would best approximate the desired schedule of being awake during the day and being asleep at night.
Light is the most important zeitgeber to the circadian oscillator. Bright light exposure was found to have phase-shifting effects with phase delay or advance following early morning or late evening exposure, respectively. Thus, bright light given in increments during the day may help set the body clock to accentuate wakefulness. Bright light therapy may also help consolidate the sleep-wake cycle and improve the behavioral disturbances in patients with dementia (03; 36). Both morning and daytime bright light given at ranges of 6000 to 8000 lux have been shown to consolidate sleep at night and minimize napping and sundowning-like behavior during the day. Another study showed that light delivered in the 2500 lux range for 1 hour per day approximately 2 hours before bedtime, as well as daily walking, improved sleep measures (23). Longer periods of moderate-intensity light may be more effective than a shorter exposure period of high-intensity light (08). Limitation of light may also help. Although this has not been studied in irregular sleep-wake disorder, blue light-blocking glasses worn in the evening have shown benefit for individuals with delayed sleep phase, insomnia, and mania (14; 10).
Melatonin is often used to accentuate the signal of darkness (36). The efficacy of utilizing melatonin alone in the treatment of irregular sleep-wake rhythm disorder remains to be determined. In placebo-controlled studies, the data in adults and children are conflicting, probably owing to reduced responsiveness of the SCN to exogenous melatonin due to loss of expression of melatonin receptors (42). Sleep measures may not improve with melatonin treatment at doses of 2.5, 6, and 10 mg in patients with dementia having irregular sleep-wake rhythm disorder (31). Melatonin also did not improve sleep or agitation in institutionalized patients with Alzheimer disease at 8 mg immediate-release and 1.5 mg sustained-release preparations (12). The therapy may be more effective in early stages of neurodegenerative disorders, for example, in mild cognitive impairment preceding overt Alzheimer disease. The clinical practice guidelines of the American Academy of Sleep Medicine suggest that, given the evidence, strategically timed melatonin may be helpful in children with irregular sleep-wake disorder, but that use of melatonin for adults with irregular sleep-wake disorder is discouraged due to lack of effect (03). Additionally, the 2015 clinical guidelines strongly advise against the use of hypnotics in older adults with dementia who have irregular sleep-wake disorder on the basis of the risk of nocturnal falls.
Patients with cognitive impairment may benefit from creating an “enriched environment” that includes scheduled social contacts, regular daytime physical activity, and increased indirect light exposure (31). Restriction of naps and of time in bed, if the patient’s condition permits, may also be helpful in consolidating the night sleep. Simple measures such as opening window shades and keeping lights on during the day for institutionalized patients can facilitate circadian entrainment. Additionally, maintaining structured routines with carefully timed light exposure and proper sleep environment may help those with underlying neurologic issues, such as dementia (05; 38).
The United States Food and Drug Administration approved ramelteon, a highly selective melatonin agonist with high affinity for melatonin MT1 and MT2 receptors, as a medication for insomnia. In preliminary studies ramelteon was shown to shift circadian phase in both animals and humans (35); it was also found to be effective in alleviating jet lag symptoms in a large field study (43). Another melatonin agonist, tasimelteon, was found to effectively shift a circadian phase and improve sleep in simulated jet lag (33). These may start an era of standardized melatonin agonist preparations with selective activity at various receptors, thus, enabling specific therapeutic effects; however, these agents have not been specifically studied for irregular sleep-wake rhythm disorder and are currently not recommended (03).
Combination therapy using bright light and melatonin does not appear to add benefit over bright light therapy alone. A multimodal strategy, including daytime activity bright light exposure and sleep scheduling, did appear to improve nighttime wakefulness in patients with dementia (23). These measures also increased the daytime wake time and activity levels in institutionalized patients with Alzheimer disease (31). Although the evidence is weak for the mixed modality approaches of combining bright light exposure, exercise, sleep hygiene, structured bedtime routine, and enriched daytime environment, these manipulations have little risk and may benefit some patients.
Many patients may be highly resistant to changing their long-standing poor sleep habits. Gradual institution of a sleep-wake and meal schedule combined with a "prescription" for some kind of daily social interaction may be helpful in such patients if they can be persuaded to be compliant, and it may decrease caretaker fatigue by producing more predictable periods of sleep and wakefulness. One clinical trial evaluates the benefits of timed activity for home-dwelling individuals with dementia, with results expected after 2021 (15). One alternative strategy being examined is the use of hypnotics to improve the sleep-wake schedule. The strategy of sedative medication use does have the potential to exacerbate delirium in patients with dementia, thus, caution should be used. Hypnotics that utilize mechanisms other than GABA may also be a viable alternative. Dual orexin receptor antagonists (DORA) have shown promise in improving sleep characteristics in patients with Alzheimer disease (01). Lemborexant, a dual orexin receptor antagonist, appears to improve sleep in patients with irregular sleep wake rhythm disorder and dementia. In a phase 2 randomized control 4-week trial of lemborexant, an orexin blocking agent in 63 participants, Moline showed improvement in rest wake activity schedules with lemborexant at dosages of 2.5 mg, 5 mg, and 15 mg (26). Other studies, with suvorexant examining insomnia in patients with dementia, suggested a benefit to total sleep time, sleep schedule, and efficiency (01). These works raise that the DORA class of hypnotics may be a reasonable choice for patients with irregular sleep wake rhythm from a neurodegenerative process, if enhancement of other circadian time clues has failed to improve the sleep schedule. Although this is a significant finding, further studies are needed to evaluate whether this strategy is worthwhile for a wider implementation.
Although little is known about irregular sleep wake rhythm disorder and pregnancy, the presence of an irregular schedule may increase risks with the pregnancy. Women who have an irregular sleep wake schedule due to work have higher risk gestational diabetes, and those working nights have higher risk of elevated blood pressure and preeclampsia (41).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Bradley V Vaughn MD
Dr. Vaughn of UNC Hospital Chapel Hill and University of North Carolina School of Medicine has no relevant financial relationships to disclose.
See Profile
Antonio Culebras MD FAAN FAHA FAASM
Dr. Culebras of SUNY Upstate Medical University at Syracuse has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 05, 2026
Sleep Disorders
Jul. 03, 2026
Sleep Disorders
Apr. 10, 2026
Sleep Disorders
Apr. 05, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 04, 2026