











Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
For patients who survive lightning strikes, neurologic complications can be devastating. The great majority of prolonged or permanent complications involve the central nervous system. These lesions include posthypoxic encephalopathy, intracranial hemorrhage, cerebral infarction, and myelopathy. Many lightning survivors are plagued with persistent neuropsychological and behavioral problems that interfere with employment and family life. These neurologic complications are especially tragic because they often involve young, healthy people who had been engaged in sports or recreation. For these reasons, individuals should be familiar with lightning safety recommendations and take prudent precautions to prevent a lightning injury. Ball lightning encephalopathy resembles the clinical condition seen in patients with lightning strikes.
Early deities and mythological gods used thunderbolts to punish their enemies and wayward humans. These early deities included Thor, the Scandinavian god; Zeus, the Greek king of gods; and Jupiter, the Roman god. The splendor and horror of lightning have been captured in the poetry and writings of many great writers, including English playwright and poet William Shakespeare (1564-1616) and English dramatist and poet Sir William Schwenck Gilbert (1836-1911).
In 1752, American scientist and diplomat Benjamin Franklin (1705-1790) made a major breakthrough in the scientific understanding of lightning when he deduced that lightning was a form of electricity.
Nearly two centuries after Franklin’s kite experiment, researchers established that cloud-to-ground lightning is a transient, high-current electric discharge. The subsequent lightning return strokes have peak currents on the order of 20 to 40 kA (52).
Although many authors cite French neurologist Jean-Martin Charcot (1825-1893) as the first to describe lightning-induced paralysis (keraunoparalysis), transient lightning-induced limb weakness was described earlier by English physician James Parkinson (1755-1824) in 1789 (69; 64; 17; 19; 72). Parkinson reported that two men were struck by the same lightning strike during a violent storm on July 17, 1787.
One of the men was described by James Parkinson:
|
[He] had been taken up to all appearance dead, and by the accounts of the neighbours, had remained in that state upwards of a quarter of an hour; but, when I saw him, the vital organs had resumed their functions, although so very imperfectly as to render the circumstance of their having been suspended, highly credible: respiration was performed with much difficulty and irregularity; and the circulation of the blood still carried on so partially as not to be discoverable at all by the pulse in the lower extremities; nor, without extreme attention, in the arteries at the wrist, although the pulsation of the carotids, at the same time, was not perceptibly different from that with might be supposed to be natural. His head was bent considerably backwards, in which state it remained immoveable, notwithstanding his endeavors, and those of his attendants, to bring it forward. His countenance was flushed; and his eyes, which he had almost lost the power of moving, were red, and, in consequence of their not being both directed to the same object, appeared wild and staring, which appearance was farther increased by the eyelids being widely opened and the pupils considerably dilated. His hands and legs resembled those of a corpse, being excessively cold, and of a dark livid colour, nearly approaching to black. A large red streak appeared on his right side, and several lesser ones on his legs, the skin in all those places being evidently scorched. He complained of a total loss of sense and motion in the lower extremities, and of much pain in the head and chest; which last was aggravated by a frequent cough, by which a considerable quantity of blood was thrown up…He was then put to bed…an universal sweat soon broke out, which was followed by an easy sleep, from which he awoke so much relieved, that, when I saw him, two hours after, his head and chest being free from pain, the spitting of blood stopped, the muscles at the back of the neck relaxed, and the use of the limbs restored (69). |
Parkinson also described a peculiar erythematous, painless, branching skin pattern, which is now called “Lichtenberg figures.” Lichtenberg figures (German: Lichtenberg-Figuren), or "Lichtenberg dust figures," are branching electric discharges that sometimes appear on the surface or in the interior of insulating materials, including the skin. Lichtenberg figures are now known to occur on or within solids, liquids, and gases during electrical breakdown. Lightning itself is a naturally occurring 3-dimensional Lichtenberg figure. Lichtenberg figures are named after the German physicist Georg Christoph Lichtenberg (1742-1799), who originally discovered and studied them in 1777.
The second man reported by Parkinson had Lichtenberg figures:
|
A red streak, about two inches wide, passed down his right side, from which, on each side, several ramifications branched out, exactly representing, in figure, those vivid corrusgations, which are so frequently seen to fly off, from any little pointed elevation on the surface of an electrified insulated conductor. A similar, but lesser streak, with similar branches, appeared on his right arm, and on the fore part of each leg and thigh; from all these he felt considerable burning pain…By the next day he was entirely free from all his complaints, except the burning pain which he still felt where the lightning had so beautifully marked him; this, however, was soon lessened by the use of a saturnine [lead] lotion; the streaks becoming, in two days time, of a brownish colour, and, in a few days more, no other vestige remained than the roughness of the cuticle, which was then peeling off (69). |
|
• Among survivors of lightning strikes, neurologic complications are the most devastating. | |
|
• Neurologic complications of lightning strikes, varying from transient benign symptoms to permanent disability, have been categorized into four distinct groups: (1) immediate and transient; (2) immediate and prolonged or permanent; (3) delayed and progressive; and (4) lightning-linked secondary trauma from falls or blast. |
About 10% to 30% of lightning strike cases are fatal, usually due to cardiac arrest (04; 62). Rain on the scalp improves the chances of surviving a lightning strike due to: (1) lower current amplitude in the brain before a fully formed flashover, and (2) reduced mechanical and thermal damage (62). Among survivors, neurologic complications are the most devastating.
Neurologic complications of lightning strikes, varying from transient benign symptoms to permanent disability, have been categorized into four distinct groups (16; 75):
(1) Immediate and transient. These symptoms are often dramatic but are the most benign because they are fleeting. The symptoms include brief loss of consciousness, amnesia, confusion, headache, weakness, and paresthesias (87). Nearly 75% of patients have a brief loss of consciousness, and 80% have brief limb weakness and paresthesias, which usually normalize within a few hours (87). A seizure may also result from a lightning strike (31).
Many patients experience a temporary lightning-induced paralysis called “keraunoparalysis” (88; 50; 54; 37; 75). The transient paralysis is accompanied by sensory loss, pallor, coolness of the limb, and extreme vasoconstriction (even to obliteration of the pulse in the limb) (88; 50). It affects the lower limbs more than the upper limbs and is specific to lightning victims.
Cerebellar dysfunction is an uncommon but established complication of lightning strikes (28; 07). Fortunately, the symptoms are usually temporary.
(2) Immediate and prolonged or permanent. The great majority of these complications involve the central nervous system. Often seen on imaging studies, these lesions can be devastating (79). Posthypoxic encephalopathy often ends tragically with death or serious cognitive deficits. As in other cases of out-of-hospital cardiac arrests, the prognosis for many of these lightning-strike patients is poor. Initial MRI and CT scan images often show evidence of cerebral edema. The relative contributions of lightning injury and secondary hypoxic-ischemic injury related to cardiac arrest are often unclear, but in some cases, a well-executed Advanced Cardiac Life Support and Basic Life Support chain can result in return of spontaneous circulation and intact neurologic survival (01; 80).
Patients who have been struck by lightning can also present with an abrupt cerebral salt-wasting syndrome (41). Unless this problem is detected and treated, it can worsen cerebral edema.
Lightning-induced intracranial hemorrhages include subarachnoid and intracerebral hemorrhages (16; 13). The most susceptible locations in patients struck by lightning are the basal ganglia and the brainstem because electric current entering via cranial orifices (ie, eyes, ears, and nose) travels caudally toward the basal ganglia and brainstem (05). In contrast, cerebral infarction is an uncommon sequel of lightning injury, which is surprising because blood vessels and nervous tissues are selectively damaged with lightning (34). There is only one reported case of lightning-induced cerebral infarction evident on MRI (29).
Myelopathy and cauda equina syndrome are uncommon but devastating complications of lightning strikes (86). Affected patients usually have permanent disability. However, occasional patients with spinal cord injuries do recover (55). The degree of functional independence through rehabilitation depends on a combination of factors, including injury severity, level, age, and motivation (56).
Other uncommon neurologic complications of lightning strikes include chronic epilepsy, locked-in syndrome, radiculopathy, and optic neuropathy (18; 01; 87; 65).
(3) Delayed and progressive complications. Delayed sequelae are reported to follow lightning injuries by days to weeks and years, but whether the lightning was, in fact, the cause of the subsequent neurologic conditions is questionable in some cases. Delayed-onset cognitive deficits following lightning injuries have been attributed to posttraumatic stress disorder (76). Other delayed neurologic syndromes after lightning injury include motor neuron disease and movement disorders. Progressive cataract in conjunction with optic neuropathy has also been reported following a lightning injury (92).
With delayed neurologic damage of vascular origin, free radicals resulting from oxidative stress may gradually damage vascular endothelial cells, cutting off blood supply or inducing late thrombosis and ending in neuronal death (77). With delayed demyelination without vascular damage, free radicals from oxidative stress may form directly from the abundant lipids in myelin cells (77). The “electroporation hypothesis,” the formation of additional pores in neurons, has been proposed to explain immediate or progressive changes in structure and function after lightning or electrical injury (77).
(4) Lightning-linked secondary trauma from falls or blast. Patients may sustain serious head or neck damage when they fall after a lightning strike or are propelled or thrown down by the lightning. Patients have developed subdural hematomas as secondary lesions. Many patients experience blast effects such as ruptured tympanic membranes.
By comparison with neurologic lesions seen after generated electrical trauma, peripheral nervous system lesions are uncommon following lightning. Autonomic nervous system disorders following lightning have rarely been reported (93; 32; 50). Cold temperature insensitivity is a symptom reported by some lightning survivors.
Many lightning survivors are beset with enduring neuropsychological and behavioral problems (98). Their symptoms can begin immediately or a few days or weeks after the lightning strike. These neuropsychological and cognitive deficits resemble those of traumatic brain injury, depression, and posttraumatic stress disorder (98). Similar neurobehavioral patterns are often seen in patients with electric injuries (48). Their symptoms often interfere with employment and family life. A questionnaire study of 100 lightning survivors revealed memory deficit, sleep disturbances, attention deficit, dizziness, chronic fatigue, irritability, depression, and fatigue (74). Other common aftereffects include pain syndromes (eg, backache, arthritis, and headaches). If these patients have not recovered by 3 months, they are at risk for long-term sequelae. The management plan for these troubling symptoms includes a team of empathetic physicians and reassuring counselors, as well as access to understanding support groups.
There have been reports of patients developing encephalopathy after contact with ball lightning and corona discharges (38; 30; 16).
Ball lightning encephalopathy resembles the clinical condition seen in lightning strike patients. Ball lightning is an incompletely understood meteorologic phenomenon associated with lightning storms. Several centers have proposed models to explain the physics of ball lightning (02; 84). Ball lightning is mobile, luminous, vanishing, or exploding. These glowing spheres have been seen floating in the air, following telephone power lines, and traveling down the aisles of airplanes. Corona discharge, another induced electrical event associated with lightning storms, is a process by which a current flows from an electrode with a high potential into a neutral fluid, usually air, by ionizing that fluid to create a region of plasma around the electrode. Corona discharge remains near a conductor and does not move like ball lightning.
Very strong electromagnetic fields can be generated by lightning that can, in turn, generate induction currents in implanted electrodes and potentially even damage the brain (73). One reported case in which lightning affected implanted electrodes occurred in a 66-year-old woman who was being treated with a rechargeable deep-brain stimulation system for neck dystonia; her implantable pulse generator switched off but remained undamaged when her apartment was struck by lightning (73). She suffered no neurologic consequences.
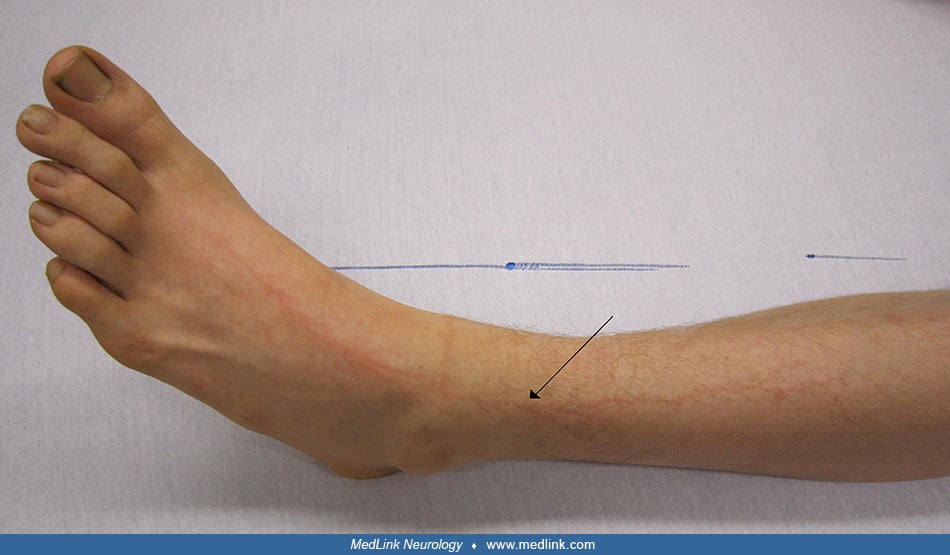
Cutaneous manifestations: Lichtenberg figures, burns, and singed body hair. Cutaneous lightning-induced Lichtenberg figures have been described as “branching” (78), “ferning” (78; 23), “fern-like” (63; 95), “fern leaf” (39; 83), or “dendriform” (49). Like keraunoparalysis, Lichtenberg figures are a transient lightning-induced finding (49; 78; 39; 47; 16; 23; 63; 83; 66; 95; 97; 12; 81; 11). Lichtenberg figures are not a burn, and skin biopsies have not demonstrated major pathologic changes (23; 12). Lichtenberg figures were reported in 9.3% of 270 lightning fatalities (11).
(Source: Byard RW. Lichtenberg figures-morphological findings. Forensic Sci Med Pathol 2023;19(2):269-72. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creativecommons.org/licenses/by/4.0.)
Histological examination revealed no interstitial hemorrhage, inflammation or epidermal, dermal or subcutaneous injuries. The only findings were subtle dermal capillary dilatation, contrasting with adjacent normal skin. (Source...
Linear burns, punctate burns, and thermal injuries also commonly occur with lightning injuries, affecting at least half of the cases (12; 71; 81; 11; 65).
Prominent interstitial hemorrhage may be present in sections from areas of punctate burning from arcing (12; 71).
Prominent interstitial hemorrhage was present only in sections from areas of punctate burning from arcing. Superficial skin loss is noted. (Source: Byard RW. Lichtenberg figures-morphological findings. Forensic Sci Med Pathol 2...
Burns may be internal as well, as in the case of a 26-year-old man hiking on an Italian mountain who had extensive burns of his supraglottic structures after being directly hit by a lightning strike (71).
CT scan of the hypopharynx and oropharynx in a 26-year-old man following a direct lightning strike on the head image shows obstruction with a complete narrowing of the supraglottic space: edema of vocal cords (black lines) and ...
Prognosis depends on many variables, including premorbid health and the time interval between the lightning strike and pre-emergency and emergency treatment.
The case fatality of lightning strikes is about 10% to 15% (26; 85). If a patient is conscious immediately or shortly after being struck by lightning, he or she is likely to remain alive.
Lightning current can reach a person via at least three routes: (1) direct strike, (2) side flash from a tall object such as a tree, and (3) ground current. Death and serious neurologic complications can result from all three routes. However, direct strikes to the head carry an especially poor prognosis, with death or serious brain damage more than 50% of the time.
Initial physical symptoms generally resolved over time, with only about 10% to 20% continuing to experience physical symptoms more than a decade after injury (85). Among patients who experience neurologic symptoms, those with immediate and transient findings have the best prognosis. Those with immediate and prolonged or permanent neurologic manifestations have a more guarded prognosis for developing prolonged or permanent disability. Vision problems persist in approximately half of those injured by lightning (85). Some patients with cerebral infarction or cerebellar syndromes can improve and recover. By contrast, patients with posthypoxic encephalopathy often have a poor prognosis. Unfortunately, many die or are left with major cognitive problems. The prognosis is especially poor for those patients with prolonged coma and those whose myoclonic seizures are unresponsive to anticonvulsants. Patients with spinal cord injury often have permanent neurologic abnormalities.
Patients with neuropsychological and behavioral problems may have persistent symptoms; however, they may improve in time, especially with help from concerned physicians and an understanding support group. Psychological symptoms, such as depression or anxiety, often have a later onset and are more likely to be chronic (85).
Case 1 (01). A 29-year-old man was hit by a lightning strike while farming. Cardiopulmonary resuscitation was provided first by coworkers and later continued with success by the medical rescue service. After advanced cardiac life support with therapeutic hypothermia, he was recognized to have quadriplegia with facial diplegia. MRI was consistent with hypoxic-ischemic encephalopathy, and diffusion-weighted MRI showed marked damage along the corticospinal tract. A reactive electroencephalogram pattern and, ultimately, his ability to communicate with eye blinking supported the clinical diagnosis of locked-in syndrome. Two weeks after admission, he was transferred to a neurologic rehabilitation center. In this case, direct lightning-induced damage, secondary hypoxia from his cardiac arrest, or both may have contributed to his neurologic impairment.
Case 2 (65). A 29-year-old man working as a gardener took shelter under a tree during a thunderstorm and was struck by lightning. He was wearing hearing protection, which shattered on impact. He suffered a cardiac arrest, but a man working nearby promptly contacted emergency services and initiated cardiopulmonary resuscitation. When emergency services arrived, he was found in asystole with a Glasgow Coma Scale score of 3/15. He returned to sinus rhythm after three cycles of CPR and was then sedated and intubated. The no-flow duration was less than 2 minutes, and the low-flow duration was approximately 15 minutes.
In the hospital, physical examination revealed burns on both feet, ankles, pubic area, torso, back, and left ear as well as a tympanic membrane perforation.
Creatine kinase level was elevated at 3700 UI/L (range 100 to 200 UI/L). Cerebral and cervical CT scans showed no evident bleeding or structural injuries. He remained intubated and sedated for 3 days.
When he awoke on day 3, paraparesis became evident. The American Spinal Injury Association Impairment Scale (AIS) grade was C, with a motor level L2 and a sensory level T11, resulting in a neurologic level of injury of T11. He reported bilateral lower limb dysesthesia, hypoesthesia, and hypopallesthesia. Persistent T11 to T12 neuropathic pain required pregabalin initiation and subsequent dose escalation. Muscle stretch reflexes were absent in the legs, and Babinski sign was absent.
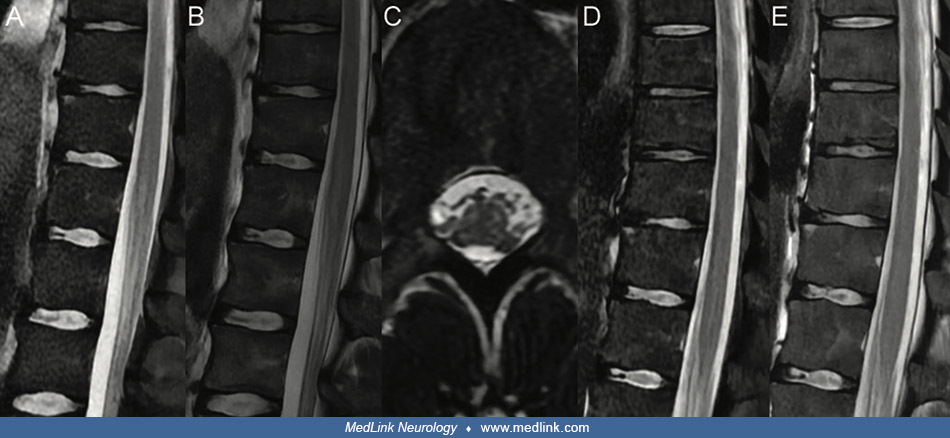
Spinal cord MRI 4 days after the strike revealed a linear hyperintensity on sagittal T2-weighted and short tau inversion recovery (STIR) sequences in the conus medullaris, extending approximately 5 cm from T11/T12 to L2.
Axial T2-weighted images showed focal hyperintensities in a quadrifocal topography of the peripheric white matter in the conus medullaris. Follow-up spinal cord MRI 15 days after the strike demonstrated complete resolution of previously observed signal abnormalities on both sagittal T2-weighted and STIR images, with no further anomalies identified.
A cerebral MRI 14 days after the strike showed no abnormality. One month post-injury, a total body muscle MRI identified no muscular necrosis and no signs of fatty infiltration.
Despite initial bladder retention necessitating catheterization, he subsequently regained normal voluntary bladder voiding. However, persistent urinary symptoms, including false urinary urgency and abdominal discomfort, prompted urodynamic evaluation, which revealed detrusor hypocontractility, with no evidence of bladder instability and preserved bladder capacity.
Five months post-injury, the neurologic level of injury was determined to be T11 with partial recovery of sensation noted on the right, with sensitivity level improving to L3, while the left remained at T11. The AIS classification remained C, but a slight motor recovery was also observed. The subject regained the ability to walk within his room and during physiotherapy sessions using a walking aid, while continuing to rely on a manual wheelchair for longer distances.
|
• Lightning damages tissues and organs through mechanisms that include thermal effects, electrical current effects, induced electrical currents, blast effects, injuries related to falls, and electroporation. | |
|
• Electroporation refers to nerve cell membrane defects produced by electric currents too weak to cause heat injury but yet strong enough to damage the lipid layer membranes. |
Lightning damages tissues and organs through mechanisms that include thermal effects, electrical current effects, induced electrical currents, blast effects, injuries related to falls, and electroporation. Fatal cases may show fresh bleeding in the subarachnoid and subpleural spaces and interlobular rupture in the lungs (67).
The electrical current involved in lightning strikes is a unidirectional, massive (direct) current impulse, in contrast to the alternating current that typically causes household and industrial electric injuries (59). The direct current delivered by a lightning strike ranges from approximately 30,000 to 50,000 amps, which exceeds that of alternating current injuries (59). However, the exposure duration from lightning is brief, lasting only about 10 to 100 milliseconds, which may be insufficient to cause Joule heating (ie, the process in which electrical energy is converted into heat as an electric current passes through a material with resistance) (59).
Muscle and nerve damage in lightning injuries often occurs through electroporation, a process in which an imposed transmembrane potential reorganizes lipids in the cell membrane, forming pores that increase membrane permeability. Electroporation-induced nerve cell membrane defects are produced by electric currents too weak to cause heat injury yet strong enough to damage the lipid layer membranes (57).
When cellular metabolic energy stores cannot maintain transmembrane concentration gradients, cell death occurs. Skeletal muscle and nerve cells are particularly vulnerable to electroporation because their length is directly proportional to the transmembrane potential. The delayed onset of neurologic sequelae following a lightning strike may be due to the cumulative effects of electroporation.
Lightning generates a large magnetic field. An individual in the vicinity of a lightning strike can experience enough magnetically induced current to produce destructive effects (10). When current enters the body, it flows through (and can damage) tissues with the least resistance (58). Tissues with high fluid and electrolyte content are blood vessels and nerves. In addition to the damaging effects of direct lightning current, magnetic field changes associated with lightning may induce a loop current with the body (25). These induced currents may be responsible for asystole or ventricular fibrillation. Low-intensity lightning can cause ventricular fibrillation without leaving skin marks (91).
|
• There is a 10-to-1 ratio of casualties to fatalities following lightning strikes. | |
|
• In the earlier part of the 20th century, lightning victims were more likely to be working (farming and ranching), whereas in the latter part of the 20th century and the early 21st century, lightning victims are more likely to be engaged in outdoor recreation and sports. | |
|
• The typical lightning strike victim is a healthy male in his mid-30s. | |
|
• Male lightning-strike victims outnumber females by about 4.5:1. |
In the United States, most lightning casualties occur in the Southeastern and Rocky Mountain states (60). Florida’s central Gulf Coast has more lightning strikes and thunderstorms than any other place in North America (36). From a global analysis, the highest number of lightning storms occurs in the mountains of Rwanda.
Many available data on lightning casualties and fatalities are found in “Storm Data,” a monthly National Oceanic and Atmospheric Administration (NOAA) publication. Because the source of the data was compiled primarily from newspaper clippings, those numbers were underreported (61). From 1959 to 1994, Storm Data reported 9818 injuries and 3239 deaths, or a ratio of approximately three to one (35). However, these Storm Data results underreported the number of lightning injuries by at least 50% and fatalities by 10%, a bias in favor of fatal outcomes, likely because fatal strikes are more likely to receive media attention (06). The National Center for Health Statistics reported 1906 lightning fatalities in the United States between the years of 1979 and 2004 (89), with the largest number of lightning deaths in Florida and Texas (03). A Colorado study, based in part on hospital information using codes of lightning injury in both inpatients and outpatients, reported a 10-to-1 ratio of casualties to fatalities (26).
In the earlier part of the 20th century, lightning victims were more likely to be men working in farming and ranching, as continues to be the case in less developed countries (67). In the United States and other highly developed countries, lightning victims are more likely to be engaged in outdoor recreation and sports in the latter part of the 20th and early 21st century (60). These activities include golf, mountain biking, hiking, camping, swimming, boating, fishing, horseback riding, and ball-field sports (15). The risks are much higher during summer months, but even winter sports, such as skiing, pose some risk (20).
The typical lightning strike victim is a healthy male in his mid-30s. Males outnumber females by about 4.5:1. This ratio is consistent with data from Colorado and Sweden (42; 15).
Lightning strikes during pregnancy are rarely reported in the medical literature or the news media, but when it occurs, it may be associated with fetal ischemic brain injury (44).
|
• It is imperative that adults in charge of children, such as teachers, coaches, counselors, and lifeguards, know and implement lightning safety guidelines. | |
|
• Individuals should have a lightning safety action plan before initiating an outdoor sports or recreation activity, which should include knowledge about the weather patterns of the location where they are located. | |
|
• If an individual can see lightning or hear thunder, he or she is already at risk. | |
|
• To reduce the risk of being struck by lightning, one should seek shelter in a large structure (eg, school, office building, house) that has plumbing and electrical wiring or, as a next resort, a fully enclosed metal vehicle. | |
|
• Situations of high risk include: (1) standing or leaning on the outside of a car or bus; (2) standing by isolated trees or flag poles; (3) being in open fields (including ball fields and golf courses); (4) swimming in pools (both indoor and outdoor pools) or open water (rivers, lakes, ocean); (5) standing on beaches; and (6) standing by or touching metal fences. | |
|
• Golf carts, bicycles, and motorcycles are unsafe during lightning storms. |
Lightning injuries are especially tragic because the victims are often healthy, young people engaged in sports or recreation when suddenly and seriously injured. Individuals at risk should understand what measures must be taken to reduce the risks of being struck by lightning. It is imperative that adults in charge of children, such as teachers, coaches, counselors, and lifeguards, know and implement lightning safety guidelines (82).
Individuals should have a lightning safety action plan before initiating an outdoor sports or recreation activity. That plan should include knowledge about the weather patterns of the location where he or she is located. For example, Rocky Mountain climbers should know that the high-density lightning-flash hours increase after late morning and continue during the afternoon and evening. Therefore, mountain climbers should plan the climb so that they begin early in the morning and are off the mountain by 11:00 AM (15).
Unfortunately, lightning tragedies occur even when the skies are clear. Patients have been struck by “bolts from the blue” (21; 51).
Lightning safety recommendations were drafted in 1998 by the Lightning Safety Group and should be understood by all those at risk of lightning strike (99). If an individual can see lightning or hear thunder, he or she is already at risk. Outdated "flash-to-bang" thresholds to seek shelter should not be used (82). Although no place is absolutely safe, there are places of low risk. To reduce the risk of being struck by lightning, one should seek shelter in a large structure (eg, school, office building, house) that has plumbing and electrical wiring. A fully enclosed metal vehicle is a relatively safe place. By contrast, standing or leaning on the outside of a car or bus is a dangerous situation. Other places of high risk to avoid include isolated trees, flag poles, open fields (including ball fields and golf courses), swimming pools (indoor and outdoor pools), beaches, rivers, and metal fences. Golf carts, bicycles, and motorcycles are unsafe during lightning storms (See Table 1).
|
• Open spaces |
Golfers should avoid standing under an isolated tree. Too often, golfers make the mistake of seeking shelter from the rain under a single tree and place themselves at risk. Golf carts are not safe. The golfer should stay inside the clubhouse.
Bicyclists are vulnerable to lightning strikes in the open. Rubber tires do not protect from lightning. The bicyclist should find a safe building or enclosed motor vehicle.
Lightning danger may persist for up to 30 minutes after the last evidence of thunder or lightning. Therefore, remaining in a safe shelter for 30 minutes before returning to the outdoor activity is prudent.
Much of the sound advice on lightning safety known in the 21st century was available over 60 years ago:
|
The moment a thunderstorm threatens, get into the house, preferably into a large house…Stay away from windows, open doors, stoves, pipes, chimney, and fireplace…Keep away from tall, isolated trees, wire fences, poles, tractors, and other metal objects. Get away from beaches, swimming pools, and fishing ponds. Make for depressions, valleys, or dense woods. If you are in your car it is the safest place…Steel topped busses and trains are equally safe. (09). |
Because most lightning strike cases are witnessed by the victim or others nearby, there is usually little or no question about the cause of the patient’s neurologic complications. However, when lightning is the cause of death, and there are no witnesses, the cause of death may not be obvious. When investigating the sudden, unexpected death of individuals discovered outdoors, the common differential diagnoses include cardiac arrhythmia, cerebral hemorrhage, seizures, pulmonary embolism, trauma (falls, suicide, homicide, animal attacks, etc.), and lightning (15).
Forensic clues suggesting a lightning strike include ruptured tympanic membranes, skin lesions of burns and ferning patterns (Lichtenberg figures), and burned clothing and shoes (45; 08; 90). Lichtenberg figures are pathognomonic of lightning injury (23; 45; 08; 90).
Other tools now available to the investigator are satellite and meteorologic data from the National Lightning Data Network. Such data can prove that lightning did occur where the victim was found and can identify the time of the lightning.
|
• Most permanent neurologic complications of lightning injury involve the central nervous system (brain and spinal cord) rather than the peripheral nervous system. | |
|
• Imaging studies are important in determining the site and nature of the lesion in the brain and spinal cord. |
Most permanent neurologic complications of lightning injury involve the central nervous system (brain and spinal cord) rather than the peripheral nervous system.
Imaging studies are important in determining the site and nature of the lesion in the brain and spinal cord. For example, a CT scan of the head helps identify intracranial hemorrhages (68) and may show massive loss of grey-white matter differentiation, especially involving the fronto-temporal lobes bilaterally (79). Cranial MRI helps evaluate neurologic complications, such as posthypoxic encephalopathy, cerebral infarction, and cerebellar atrophy (28). Unilateral hemispheric leukoencephalopathy on MRI has been reported as an incidental finding in an individual who sustained a lightning strike during infancy (53).
Standardized autonomic nervous system testing procedures might corroborate the diagnosis for those few patients with autonomic nervous system involvement symptoms.
Ophthalmology consultation should be considered to evaluate possible eye injury, including delayed cataracts. Otologists may be needed to treat a ruptured tympanic membrane, a common complication of lightning strikes.
For patients with neuropsychological symptoms, neuropsychological assessments and psychometrics may be helpful (40).
|
• Many neurologic complications (such as keraunoparalysis, brief loss of consciousness, confusion, and paresthesias) are immediate and transient and, consequently, require no specific treatment. | |
|
• The prolonged and permanent neurologic complications of lightning strikes involve damage to the central nervous system, including cerebral disorders, spinal cord injury, and neuropsychological symptoms. | |
|
• Early neurorehabilitation is essential for patients with spinal cord injury. | |
|
• Many lightning survivors are plagued with persistent neuropsychological and behavioral problems. |
One should begin emergency evaluation and treatment immediately upon finding the patient or shortly after lightning strikes. If the patient is unconscious, one should begin basic life support, including airway, breathing, and circulation assessment. Cardiorespiratory resuscitation should be instituted immediately if the patient is apneic and has no pulse (33; 99). These patients may have cardiorespiratory arrest with ventricular fibrillation.
The lightning-strike patient does not hold an electrical charge. For that reason, the rescuer need not fear receiving a shock from touching a patient struck by lightning. This is not always the case with patients who are shocked by electrical lines or appliances; in those situations, the rescuers should ensure the electrical current’s source is off or safely removed from the patient. In a lightning situation, rescuers should be careful not to place themselves in danger of being injured by another lightning strike. If rescuers have a mobile phone, they should call 911 for help. The chances of survival are good for the patient struck by lightning who is conscious. However, persistent medical complications are possible.
More neurologic issues are evaluated in an emergency department, outpatient facility, or hospital. Many neurologic complications (such as keraunoparalysis, brief loss of consciousness, confusion, and paresthesias) are immediate and transient; these symptoms should be carefully evaluated but often require no specific treatment. Unfortunately, other patients have permanent or prolonged neurologic sequelae that call for the expertise of many disciplines, including neurologists, cardiologists, neurorehabilitation specialists, intensivists, and others.
The prolonged and permanent neurologic complications of lightning strikes involve damage to the central nervous system, including cerebral disorders, spinal cord injury, and neuropsychological symptoms (96). Patients with catastrophic brain damage will require elaborate measures provided by intensive care units. A comprehensive rehabilitation plan can be instituted in time and with improving mental status (including physical, speech, and occupational therapies). A protracted comatose state and myoclonic seizures unresponsive to anticonvulsants are indicators of poor outcomes.
Early neurorehabilitation is essential for patients with spinal cord injuries (96). Patients with a spinal cord injury may confront many problems, including neurogenic bladder, skin sores, deep vein thrombosis, and severe spasticity. The management plan for lightning-related spinal cord injury is the same as that for other patients with traumatic spinal cord injury.
Neurosurgical consultation should be obtained for patients who suffer intracranial hematomas and spinal cord injuries resulting from falls and blasts associated with lightning. These lightning-linked lesions to the head and spine can be catastrophic. Intracranial hemorrhages (including epidural, subdural, and intracerebral hemorrhages) can be rapidly fatal. CT scan of the head should be obtained on an urgent basis.
Many lightning survivors are plagued with persistent neuropsychological and behavioral problems. Their symptoms (including impaired concentration, sleep disturbances, depression, chronic pain, and easy fatigability) can begin immediately or after a few days and may persist for months or longer. The problems can interfere with employment and family life. Patients may improve with time, especially with assistance from concerned physicians, psychological counseling, and an understanding support group.
A literature review of lightning strikes in pregnancy reveals fewer than 20 reported cases. Although maternal prognosis for survival was good, the literature revealed a dismal outcome for the fetus (14; 46; 70). Fetal or neonatal death was reported in nearly 50% of the cases. Explanations for these catastrophes include (1) severe uterine contractions and uterine rupture, and (2) the uterus and amniotic fluid are good conductors of electricity (94; 43). A fetal autopsy after a lightning-induced miscarriage revealed interstitial hemorrhages of the lungs (14).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neuro-Ophthalmology & Neuro-Otology
Apr. 07, 2026
General Neurology
Apr. 06, 2026