





























































Peripheral Neuropathies
Clinical evaluation of peripheral neuropathies
Jul. 16, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
This article discusses intramedullary cranial polyneuropathies that are supranuclear, internuclear, nuclear, fascicular, or some combination. Supranuclear cranial polyneuropathies result from bilateral disease, usually of the hemispheres, and include pseudobulbar palsy and Foix-Chavany-Marie syndrome. Cranial polyneuropathies with an internuclear component typically result from pontine lesions and include one-and-a-half syndrome and associated paralytic pontine exotropia, as well as more extensive forms with intramedullary involvement of other cranial nerves--the one-and-a-half syndrome spectrum disorders. Cranial polyneuropathies with nuclear or fascicular involvement include a variety of brainstem syndromes, such as facial colliculus syndrome, Millard-Gubler syndrome, Foville syndrome, superior cerebellar artery syndrome, anterior inferior cerebellar artery syndrome, lateral medullary syndrome, medial medullary syndrome, Avellis syndrome, and Garcin syndrome (spanning the cranial nerves on one side).
|
• Supranuclear cranial polyneuropathies result from bilateral disease of the rostral neuraxis, usually of the cerebral hemispheres, and include pseudobulbar palsy and Foix-Chavany-Marie syndrome. | |
|
• Cranial polyneuropathies with an internuclear component typically result from pontine lesions and include one-and-a-half syndrome and associated paralytic pontine exotropia, as well as more extensive forms with intramedullary involvement of other cranial nerves—the one-and-a-half syndrome spectrum disorders. | |
|
• Cranial polyneuropathies with nuclear or fascicular involvement include a variety of brainstem syndromes, such as facial colliculus syndrome, Millard-Gubler syndrome, superior cerebellar artery syndrome, anterior inferior cerebellar artery syndrome, lateral medullary syndrome, medial medullary syndrome, Avellis syndrome, and Garcin syndrome (spanning the cranial nerves on one side). |
Supranuclear cranial polyneuropathies. Supranuclear cranial polyneuropathies result from bilateral disease of the rostral neuraxis, usually of the cerebral hemispheres, and include pseudobulbar palsy and Foix-Chavany-Marie syndrome.
Pseudobulbar palsy. Berlin physician A Magnus reported the first case of pseudobulbar palsy in 1837 in a patient with multiple infarcts (76). In 1877, French physician and physiologist Jacques Raphaël Lépine (1840-1919) introduced the term pseudobulbar palsy (72).
Bilateral anterior opercular syndrome (Foix-Chavany-Marie syndrome). Bilateral anterior opercular syndrome (Foix-Chavany-Marie syndrome) was more extensively investigated by French neurologists Charles Foix (1882-1927) and Jean Alfred Émile Chavany (1892-1959) with French pediatrician Julien Marie (1899-1987) in 1926 (39).
Cranial polyneuropathies with an internuclear component. Cranial polyneuropathies with an internuclear component typically result from pontine lesions and include one-and-a-half syndrome and associated paralytic pontine exotropia, as well as more extensive forms with intramedullary involvement of other cranial nerves—the one-and-a-half syndrome spectrum disorders.
One-and-a-half syndrome. Canadian neurologist C Miller Fisher (1913-2012) provided a masterful description of one-and-a-half syndrome in 1967 (38):
In lesions of the brainstem, vascular particularly, demyelinative or neoplastic more rarely, there occasionally occurs a paralysis of eye movements in which one eye lies centrally and fails completely to move horizontally while the other eye lies in an abducted position and cannot be adducted past the midline. ... We have attributed the syndrome to a lesion in or near the pontine conjugate lateral gaze centre on one side (causing the conjugate gaze palsy) plus an internuclear ophthalmoplegia due to the interruption of the ipsilateral medial longitudinal fasciculus after it has crossed the midline from its site of origin in the contralateral vestibular nucleus (causing failure of adduction of the ipsilateral eye). ... This syndrome which we have colloquially termed the 'one and a half syndrome' because it consists of a conjugate lateral gaze palsy in one direction, plus one half of a gaze palsy in the other, provides evidence that the medial longitudinal fasciculus fibres running to the opposite ocular adductors cross to the other side caudally in the pons near their origin in the vestibular nucleus rather than running cephalad for some distance before crossing (38; page 386). |
Paralytic pontine exotropia. In 1974, paralytic pontine exotropia as a sign of acute unilateral pontine gaze palsy and internuclear ophthalmoplegia was described by James A Sharpe and colleagues Michael A Rosenberg, William F Hoyt, and Robert B Daroff (118).
Cranial polyneuropathies with nuclear or fascicular involvement. Cranial polyneuropathies with nuclear or fascicular involvement include a variety of brainstem syndromes, such as facial colliculus syndrome, Millard-Gubler syndrome, superior cerebellar artery syndrome, anterior inferior cerebellar artery syndrome, lateral medullary syndrome, medial medullary syndrome, Avellis syndrome, and Garcin syndrome (spanning the cranial nerves on one side).
Midbrain syndromes.
Weber syndrome. Weber syndrome, or superior alternating hemiplegia, involves the cerebral peduncle and the fascicles of the oculomotor nerve on one side, causing ipsilesional oculomotor nerve palsy and contralesional hemiparesis; occasionally, the substantia nigra can also be involved. The syndrome was described in 1863 by Sir Hermann David Weber (1823-1918), a German-born physician working in London (139; 147).
Benedikt syndrome. Benedikt syndrome, a paramedian midbrain stroke syndrome that involves the fascicles of the oculomotor nerve and the red nucleus, was first described by Hungarian-Austrian neurologist Moritz Benedikt (1835-1920) in 1889 (16; 146). French neurologist Jean-Martin Charcot (1825-1893) named the syndrome with the eponym Benedikt syndrome in 1893 (23).
Claude syndrome. Claude syndrome, ipsilesional oculomotor nerve palsy and contralesional limb ataxia, was first described by French neurologist Henri Claude (1869-1945) in 1912 (25; 25).
Nothnagel syndrome. In 1879, German internist Carl Wilhelm Hermann Nothnagel (1841-1905) described a rare syndrome of the midbrain tectum that involves the oculomotor nerve fascicles and superior cerebellar peduncle, causing bilateral oculomotor nerve palsy and limb ataxia, respectively (96; 97; 74).
Pontine syndromes.
Raymond syndrome. In 1896, French neurologist Fulgence Raymond (1844-1910) described a ventral medial mid-pontine syndrome with ipsilesional abducens palsy and contralesional central facial paresis and hemiparesis (107; 145).
(1) Motor cortex; (2) interhemispheric fissure; (3) anterior surface of the spinal cord; (4) corticobulbar fibers; (4') decussation of the corticobulbar fibers in the caudal pons (although Raymond localizes the decussation too ...
Defoville (Foville) syndrome. Defoville syndrome (sometimes called Foville syndrome) is a rare inferior medial pontine syndrome first characterized in 1858 by French psychiatrist and neurologist Achille Louis François Foville (1831/1832-1887) (40; 143; 19). On the title page of his doctoral thesis in 1837, Foville spelled his name "Defoville" to distinguish himself from his father, Achille Louis Foville (1799-1878), who was an anatomist, psychiatrist, and neurologist. The syndrome consists of ipsilesional horizontal gaze palsy, peripheral facial palsy, and contralesional hemiparesis resulting from a lesion in the lower pons.
The responsible lesions for various brainstem syndromes are shown with colored ovals. The crossed neurologic symptoms observed in the Defoville (Foville) syndrome are shown in the lower pons. The diagram was drawn by Dr. Nathan...
The diagram was drawn by Dr. Nathan Beucler. (Source: Beucler N, Boissonneau S, Ruf A, Fuentes S, Carron R, Dufour H. Crossed brainstem syndrome revealing bleeding brainstem cavernous malformation: an illustrative case. BMC Neu...
Superior cerebellar artery syndrome. In 1908, and in more detail in 1912 with the results of autopsy, Philadelphia neurologist Charles Karsner Mills (1845-1931) described the superior cerebellar artery syndrome in a 34-year-old man with a history of syphilis who presented initially with vertigo, nausea and vomiting, left arm clumsiness, right emotional facial palsy, and right-sided sensory impairment that involved the face, limbs, and trunk (84; 85; 126). At autopsy, Mills and neurologist and pathologist William Gibson Spiller (1863-1940) found a lesion involving the cerebellum and dentate nucleus, the superior cerebellar peduncle, and the red nucleus on the opposite side, with the main symptoms being ataxia of the extremities ipsilateral to the main lesion (intention tremor, dysmetria, and asynergia) and contralateral "deafness, paralysis of emotional expression in the face, and loss of the senses of pain, heat and cold over the entire half of the body" (85; 126; 29).
Anterior inferior cerebellar artery syndrome. In 1943, American neurologist and neuropathologist Raymond Delacy Adams (1911-2008) first described the clinical and pathologic features of occlusion of the anterior inferior cerebellar artery (02).
The so-called Millard-Gubler syndrome. According to recent formulations, the so-called Millard-Gubler syndrome, caused by a unilateral lesion in the ventral pons, manifests as an ipsilateral palsy of cranial nerves VI and VII with contralateral hemiplegia (60). In fact, the original descriptions of Millard and Gubler did not include cranial nerve VI paresis, nor did they include gaze paresis, facial sensory loss (cranial nerve V), vertigo, or deafness (cranial nerve VIII).
The Millard-Gubler syndrome, as described in 1856 by the two eponymous French physicians Auguste Louis Jules Millard (1830-1915) and Adolphe-Marie Gubler (1821-1879), was simply a crossed paresis of the peripheral facial nerve on one side and a contralateral hemiparesis (47; 83; 142). Millard and Gubler separately described patients with this combination of signs due to a lesion of the pons--a classic crossed brainstem syndrome. However, modern references to this syndrome are almost all in error in defining the syndrome as involvement of both the sixth and seventh cranial nerves on one side, typically with a contralateral hemiparesis; this combination would indicate involvement of the caudal pontine tegmentum, sparing the abducens nucleus (which would produce a gaze palsy) and medial structures (paramedian pontine reticular formation and medial longitudinal fasciculus, which together would produce a one-and-a-half syndrome). Gubler’s cases included three with a tumor, one with a stroke, and one with a brownish softening, whereas Millard reported one case due to pontine hemorrhage. Millard's case was described in a letter to the editor in the journal where Gubler reported his cases. None of these cases had a reported ocular motility disturbance or vertigo. The lesions must have all involved the basis pontis as well as the CN VII fascicle (and possibly the facial nerve nucleus) but could not have extended more medially or dorsally to involve the CN VI nucleus or fascicle or the paramedian pontine reticular formation, nor could they have extended further laterally and dorsally to involve CN VIII or the cochlear and vestibular nuclei. The eponym is erroneously applied to a combined CN VI and CN VII lesion. The original reports were translated by Wolf, who correctly emphasized that neither Millard nor Gubler reported a CN VI paresis, but who then suggested that the syndrome was due to involvement of the facial nerve nucleus, when it is also possible for it to involve the facial nerve fascicle (47; 83; 142).
Medullary syndromes.
Lateral medullary syndrome (Wallenberg syndrome). Prussian internist, neurologist, and neuroanatomist Adolf Wallenberg (1862-1949) is most remembered for his eponymous clinical and pathological descriptions of the lateral medullary syndrome (Wallenberg syndrome) (136; 137; 140; 144; 15; 69; 70; 123). Wallenberg’s detailed clinical (but not pathological) description in 1895 (136) preceded American neurologist Henry Hun’s (1854-1924) clinicopathological description in 1897 (52; 69), but both reports were partially anticipated by others.
Sensation of pain or differentiation between the tip and head of a pin. The double-hatched areas indicate those regions where deeper pinpricks can still be felt as the head, and temperature differences of 30° to 40° C cannot be...
The double-hatched areas in the diagram indicate those regions where deeper pinpricks can still be felt as the head, and temperature differences of 30° to 40° C cannot be recognized. In the single but closely hatched areas, the...
Based on his knowledge of neuroanatomy, Wallenberg had correctly localized his patient’s lesion to the lateral medulla and attributed it to occlusion of the posterior inferior cerebellar artery. Still, it was not until 1901, 4 years after Hun’s clinicopathological report, that Wallenberg reported the pathological findings on his patient, who died in 1899 (136; 137). Wallenberg thought the syndrome in his case was due to embolization of the posterior inferior cerebellar artery (136; 137); however, the most common cause is thrombosis of the vertebral artery.
This drawing illustrated extensive atherosclerotic disease. (Source: Wallenberg A. Anatomischer Befund in einem als “acute Bulbär-aVection [Embolie der Art. cerebellar. post. inf. sinistr?]” bescreidenen Falle. Archiv für Psy...
Areas of atherosclerotic plaque shown from the 1901 autopsy of Adolf Wallenberg's 1895 case of lateral medullary syndrome. (Source: Wallenberg A. Anatomischer Befund in einem als “acute Bulbär-aVection [Embolie der Art. cerebe...
From the 1901 autopsy of Adolf Wallenberg's 1895 case of lateral medullary syndrome. The left posterior inferior cerebellar artery (on the left side of the figure) is nearly occluded with a thrombus. (Source: Wallenberg A. Anat...
An area of infarction is evident in the left lateral medulla. The area of infarction extends from the lateral surface inwards as far as the lateral internal arcuate fibers (fibrae arcuatae internae). In the dorsoventral directi...
An area of infarction is evident in the left lateral medulla. The area of infarction extends further medially. Destroyed here are, in addition to the long (spinotectal and spinothalamic) tracts of the lateral medulla, the most ...
An area of infarction is evident in the left lateral medulla. This section contains the largest transverse diameter of the lateral medullary infarction. The softening focus has the shape of an irregular ellipse with the largest...
An area of infarction is evident in the left lateral medulla. After the infarcted area has reached its greatest extent, it rapidly approaches its frontal pole, so that this section only shows the last remnants of the cerebral t...
Wallenberg’s patient, a 38-year-old man, presented with an attack of vertigo associated with pain and hyperesthesia on the left side of the face and body, hypoesthesia of the right half of the face, and loss of pain and temperature sensitivity in the right extremities and the right half of the torso, with retention of the sense of touch (136). He also had dysphagia; impaired sensation on the mucosa of the mouth, throat, and palate; disturbed motility of the soft palate (on the first day bilateral, later left-sided); hoarseness with paralysis of the left vocal cord, and paresis of the left hypoglossal muscle, with no disturbance in the innervation of the facial muscles. He had ataxia of the left extremities without impairment of gross strength and a marked tendency to fall to the left side. At autopsy, the most extensive atherosclerotic changes were in the left vertebral artery and its branches, including a near-occlusive thrombus in the left posterior inferior cerebellar artery.
Hun’s 53-year-old patient had acutely developed ipsilesional ptosis and anhidrosis (but reportedly not miosis), diplopia, ipsilesional analgesia and thermanesthesia of the face, dysphagia, dysphonia, dysarthria, ipsilateral appendicular ataxia, postural instability with a tendency to fall toward the side of the lesion, gait ataxia, contralesional analgesia and thermanesthesia of the body, and vomiting (52; 69). Pathological findings included extensive posterior circulation atherosclerosis, affecting especially the basilar artery, and infarction of the rostral lateral medulla, encompassing the descending trigeminal nucleus and tract, the nucleus ambiguous, the lateral spinothalamic tract, the ventral spinocerebellar tract, fasciculi of the glossopharyngeal and vagal nerves, and the inferior cerebellar peduncle (52; 69). Hun concluded that the manifestations resulted from left posterior inferior cerebellar artery occlusion.
Opalski syndrome. Shortly after World War II, Polish neurologist Adam Opalski (1897-1963) described a rare variant of Wallenberg syndrome with ipsilateral hemiparesis (101; 111).
Medial medullary syndrome. Medial medullary infarction was initially described by William Gibson Spiller (1863-1940) in 1908 (125). In 1914, French neurologist Joseph Jules Dejerine (1849-1917) proposed a diagnostic triad of symptoms: (1) contralateral hemiplegia sparing the face, (2) contralateral loss of deep sensation, and (3) ipsilateral hypoglossal paralysis (31).
Babinski-Nageotte and Cestan-Chenais syndromes. French-Polish neurologist Joseph Babinski (1857-1932) and French neuroanatomist Jean Nageotte (1866-1948) described an intermediolateral medullary syndrome in 1902 (10; 11). Babinski-Nageotte syndrome essentially incorporates lateral medullary syndrome with contralateral hemiparesis or hemiplegia because of extension of the “Wallenbergian” lateral lesion to the corticospinal tract.
Joseph Babinski (1857-1932) is supporting the patient with hysteria, Marie "Blanche" Wittman, while Jean-Martin Charcot (1825-1893) lectures. (Source: Musée d'histoire de la médecine, Paris. Public domain.)
Cestan-Chenais syndrome was described by French neurologist Étienne Jacques Marie Raymond Céstan (1872-1934) and French physician Louis Jean Chenais (1872-1950) in 1903 (21). Cestan-Chenais syndrome includes all symptoms of Babinski-Nageotte syndrome except the ipsilateral hemiataxia because of sparing of the posterior spinocerebellar tract (21; 66).
Reinhold hemimedullary syndrome. German physician Heinrich Reinhold (1862-1927) described the hemimedullary syndrome in 1894 (108; 59). The hemimedullary syndrome is essentially a combination of the lateral and medial medullary syndromes.
Hemimedullary syndrome results from occlusion of a vertebral artery proximal to the posterior inferior cerebellar artery and its anterior spinal artery branches (66).
Avellis syndrome. Avellis syndrome was described by German otolaryngologist Georg Avellis (1864-1916) in 1891 (09). Avellis described 10 cases in which there was unilateral paralysis of the larynx associated with paralysis of the soft palate on the same side. None of the 10 cases came to autopsy. The term "Avellis syndrome" was coined by French otolaryngologist Marcel Lermoyez (1858-1929). Because the Milanese otologist Giovanni Longhi (1843-1893) reportedly described patients with similar symptoms, the syndrome is sometimes referred to as Avellis-Longhi syndrome or Longhi-Avellis syndrome.
Numerous closely related syndromes involving the vagus nerve have been described (55). In 1918, Vernet reviewed the various syndromes associated with laryngeal paralysis and presented a classification of them (134). Since then, others have been added, and further classifications have been presented, only some of which involve the brainstem (53; 56; 138; 128; 58; 63; 64; 106; 51; 67; 50; 153). Many involve the jugular foramen or the extramedullary cranial nerves within the subarachnoid space or extracranially (71; 41).
|
Cranial Nerves |
IX |
X |
XI |
XII | |
|
Vocal Cord |
Palate | ||||
|
Collet and Sicard |
* |
* |
* |
* |
* |
|
Jackson |
* |
* |
* |
* | |
|
Vernet |
* |
* |
* |
* | |
|
Schmidt |
* |
* |
* | ||
|
Avellis |
* |
* | |||
|
Tapia |
* |
* | |||
|
Villaret |
* |
* |
* |
* | |
Lederer proposed a simplified system that avoided eponyms (71), an approach that was supported by subsequent authors (41; 28).
|
Syndrome |
Cranial Nerves Involved |
|
Bulbar |
X and variable combinations of IX, XI, XII (and possibly V, VI, VII, VIII) |
|
Jugular foramen |
X and IX, XI, XII, and sympathetic |
|
Parapharyngeal space |
X and IX, XII (possibly VII), and sympathetic |
|
Arch of aorta |
X and phrenic, sympathetic |
|
• Clinical features depend on the cranial nerves involved and the cause. | |
|
• Prognosis depends on the pathology of the primary lesions. | |
|
• Supranuclear palsies result from lesions above (rostral to) the cranial nerve nuclei. | |
|
• Crossed brainstem syndromes typically combine ipsilesional cranial nerve deficits with contralesional long tract signs (eg, hemiparesis or hemianesthesia)--the crossed pattern immediately suggesting localization to the brainstem. | |
|
• Although acute brainstem infarction is the predominant cause of various brainstem syndromes, some cases result from hemorrhage, neoplasm, abscess, demyelination, syringobulbia, brainstem encephalitis, etc. |
Supranuclear palsies result from lesions above (rostral to) the cranial nerve nuclei.
Pseudobulbar palsy. Pseudobulbar palsy is a supranuclear palsy caused by bilateral disturbance of the corticobulbar tracts, which carry upper motor neuron input to motor nuclei of the trigeminal, facial, glossopharyngeal, vagus, accessory, and hypoglossal nerves in the pons and medulla. Thus, the corticobulbar tracts exert supranuclear control over mastication, facial expression, deglutition, and speech. Pseudobulbar palsy is characterized particularly by facial and tongue weakness, dysarthria, dysphagia, and emotional lability. In addition to various acquired forms, pseudobulbar palsy can be seen in a congenital bilateral perisylvian syndrome (95).
Foix-Chavany-Marie syndrome. Foix-Chavany-Marie syndrome is a specific cortical form of supranuclear (pseudobulbar) palsy resulting from bilateral anterior opercular lesions that produce an “automatic-voluntary dissociation” of motor function of lower cranial nerves. Manifestations include volitional paralysis of masticatory, facial, pharyngeal, and lingual muscles innervated by cranial nerves V, VII, IX, X, and XII, with preserved autonomic and emotional innervation of these muscles (eg, emotional smiling, laughter, and crying as well as automatic yawning). There is a pseudo-peripheral bilateral facial paresis, with involvement of both the lower and upper face such that the face appears totally expressionless and immobile with volitional efforts, yet such patients furrow their brows with upgaze, blink, close their eyes completely while sleeping, and move the jaw and facial muscles with spontaneous emotional responses (eg, laughing or crying). The palate, pharynx, and tongue are paralyzed, typically with severe dysphagia necessitating tube feeding. Although the tongue is immobile or nearly so, atrophy and fasciculations are absent. Although some patients can make inarticulate sounds when they attempt to speak, most are anarthric or mute but can communicate by writing or with gestures.
One-and-a-half syndrome spectrum (including paralytic pontine exotropia). In one-and-a-half syndrome, there is horizontal immobilization of one eye combined with an adduction deficit of the opposite eye: a horizontal gaze palsy (ie, one gaze palsy) combined with an internuclear ophthalmoparesis (half of a gaze palsy).
In paralytic pontine exotropia, the acute presentation of a one-and-a-half syndrome, paralytic external deviation of one eye is associated with horizontal immobility of the opposite eye resulting from a lesion involving the paramedian pontine reticular formation and the medial longitudinal fasciculus on the side opposite the deviated eye (118). The exotropic eye manifests abduction nystagmus with attempted gaze to that side and with marked slowness of adduction saccades. Midbrain ocular motor functions are normal, including vertical gaze, convergence, and pupillary constrictor reflex activity (118).
There has been a rather absurd escalation of named "syndromes" that are all variants or formes frustes of the one-and-a-half syndrome originally described by Fisher (38). Most of these subsequent elaborations are one-off case reports and can hardly be considered "syndromes," despite some rather grandiose paper titles. These also all suffer from conceptual problems with their fanciful names (eg, "half-and-half," "1 plus 1," "7 and a half," "8," "8 and a half," "9," "13 and a half," "15 and a half," "16," "16 and a half," "20," "20 and a half," and "24 and a half" syndromes). For example, an "8 and a half" syndrome is a 1-and-a-half plus ipsilateral peripheral CN VII paresis (34; 05).
Rightward gaze test in a 77-year-old man with so-called eight-and-a-half syndrome due to a pontine ischemic stroke. Limited adduction of the left eye on rightward gaze is noted. (From: Almeida PL, Félix T, Evangelista R, Gomes ...
Leftward gaze test in a 77-year-old man with so-called eight-and-a-half syndrome due to a pontine ischemic stroke. Limited adduction of the left eye and impaired abduction of the left eye were noted, which did not reach the mid...
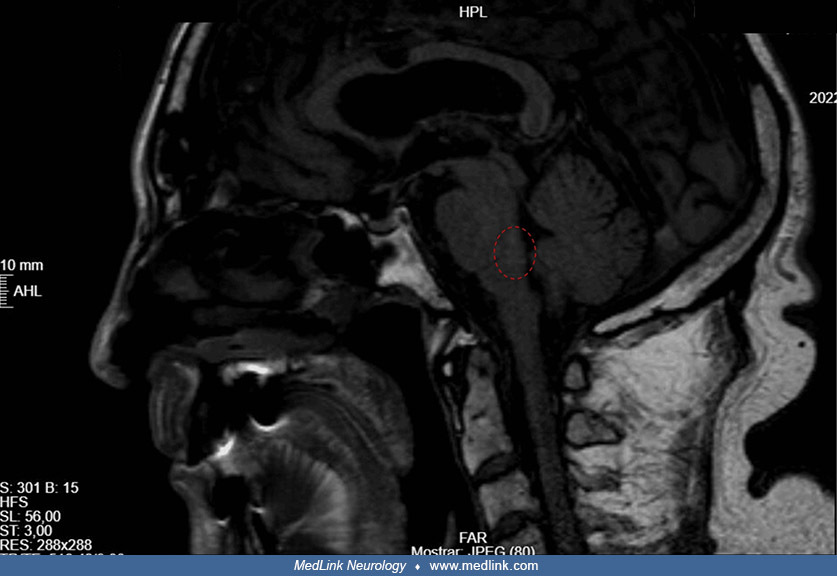
MRI confirming acute ischemic lesion in the dorsal pontine tegmentum (red circle) in a 77-year-old man with so-called eight-and-a-half syndrome due to a pontine ischemic stroke. (From: Almeida PL, Félix T, Evangelista R, Gomes ...
So, although the conceptual framework of Fisher syndrome was consistent in counting the number of gaze palsies (ie, one and a half gaze palsies), none of the other variants or formes frustes of the one-and-a-half syndrome employs any conceptual consistency in the things added together. Many add the ordinal numbers of additional cranial nerves involved: one and a half of one thing (gaze palsy), plus the ordinal number we assign to another thing, such as VII for the facial nerve, rather than another half for a unilateral facial nerve palsy. Examples include "8 and a half," "13-and-a-half", "15-and-a-half," "16-and-a-half," "20-and-a-half," and "24-and-a-half" syndromes. This results in various inconsistencies in addition to the obvious conceptual mess that these schemes adopt for cutesy case-report titles. We don't call bilateral olfactory nerve dysfunction (or, for that matter, a unilateral optic neuropathy) a "2" syndrome, nor a cavernous sinus syndrome a "III + IV + V1 + VI" or "16" syndrome. Some even add "a half" for a hemiparesis or a hemisensory loss, but others do not do this: "9" and "20" syndromes add a "half" for hemiparesis or hemisensory loss, but "24 syndrome" did not do this, even though a hemiparesis was present. In still others, the naming interprets either a gaze palsy or an internuclear ophthalmoparesis as a forme fruste of one-and-a-half syndrome (eg, "half and half syndrome" and "one plus one syndrome", as well as "7 and a half," "8," "16," and "24" syndromes). It is not worth citing the more than 100 such reports, but a rough itemization of some of the proposed "syndromes" is given in Table 3. If some of these reports described interesting anatomical insights brought up by a constellation of abnormalities, that would be fine, but the vast majority do not; simply tallying things in this inconsistent fashion does not make either a worthwhile case report or a new syndrome.
The pontine tegmentum contains portions of the trigeminal nuclei and the vestibular nuclei and, just rostral to the pontomedullary junction, the facial motor nucleus, superior salivatory nucleus, and abducens nucleus.
"Syndrome" | Comments |
Half-and-half (INO and ipsilateral CN VI) | Forme fruste of a one-and-a-half syndrome. |
One-and-a-half (38) | Lesion of the paramedian caudal pontine tegmentum involving PPRF (or CN VI nucleus) and MLF. |
Paralytic pontine exotropia (118) | A useful descriptive phenomenological term for an aspect of acute one-and-a-half syndrome. |
1 plus 1 (bilateral horizontal gaze palsy with preserved convergence) | Forme fruste of a one-and-a-half syndrome. |
7-and-a-half [INO (the half) and ipsilateral peripheral CN VII] | Forme fruste of a one-and-a-half syndrome. |
8 (horizontal gaze palsy plus ipsilateral CN VII) | Forme fruste of a one-and-a-half syndrome. This is facial colliculus syndrome. |
8-and-a-half (1-and-a-half + ipsilateral peripheral CN VII) (34) | |
9 ("8-and-a-half" plus an extra "1/2" for contralateral hemihypesthesia and possibly contralateral hemiparesis) | Lesion of the caudal pons involving the tegmentum and basis pontis. |
13-and-a half (8-and-a-half + CN V) | |
15-and-a-half (1-and-a-half + R/L CN VII) | |
16 (R/L facial colliculus syndrome, R/L horizontal gaze palsy + R/L CN VII) | From the naming conception standpoint, a forme fruste of a one-and-a-half syndrome. |
16-and-a-half (8-and-a-half + CN VIII) | |
20 (15-and-a-half + R/L II + hemiparesis) | |
20-and-a-half (1-and-a-half + R/L CN VII + CN V) | |
24 (R/L horizontal gaze palsy, R/L CN VII, and contralateral CN VIII [1+1+7+7+ 8]) | From the naming conception standpoint, a forme fruste of a one-and-a-half syndrome. Horner syndrome and hemiparesis were also reported but were not counted in the naming scheme. |
24-and-a-half (1-and-a-half + ipsilateral CN VII + R/L CN VIII) | |
| |
Intramedullary nuclear or fascicular cranial polyneuropathies result from lesions in the brainstem. Crossed brainstem syndromes typically combine ipsilateral cranial nerve deficits with contralateral long-tract signs (eg, hemiparesis or hemianesthesia), the crossed pattern immediately suggesting localization to the brainstem. Although acute brainstem infarction is the predominant cause, some cases result from hemorrhage, neoplasm, abscess, demyelination, syringobulbia, brainstem encephalitis, etc.
Midbrain syndromes.
Weber syndrome. The usual cause of Weber syndrome is a midbrain infarction resulting from occlusion of a branch of the posterior cerebral artery or, less commonly, paramedian branches of basilar bifurcation perforating arteries.
A variety of causes have been reported for Weber syndrome (113; 12; 124; 13; 91; 105; 37; 120; 73; 81; 88; 119). These include transient midbrain ischemia (12), Percheron artery infarction (81), anterior choroidal arterial embolism as a complication of mechanical thrombectomy for middle cerebral artery occlusion (73), brainstem tuberculoma (105), neurocysticercosis (124), herpes simplex virus brainstem encephalitis (13), and acute leukemia (91).
Benedikt syndrome. Benedikt syndrome, or paramedian midbrain syndrome, is a midbrain stroke syndrome that involves the fascicles of the oculomotor nerve and the red nucleus. The clinical presentation includes ipsilesional cranial nerve III palsy, contralesional (or crossed) hemiataxia, and choreoathetosis (16; 45; 146; 74; 14; 03; 20).
Claude syndrome. Claude syndrome includes ipsilesional oculomotor nerve palsy and contralesional limb ataxia (25; 25; 74). Claude syndrome is generally caused by occlusion of the small perforating branches of the posterior cerebral artery supplying the dorsomedial aspect of the midbrain. The resulting midbrain infarction involves the oculomotor nucleus, the medial portion of the red nucleus with the rubrodentate fibers, and the superior cerebellar peduncle. Although Claude syndrome is typically unilateral (87; 135; 112; 151; 44; 89; 24; 150; 119), bilateral cases have been reported (141; 48).
Nothnagel syndrome. Nothnagel syndrome is a rare syndrome of the midbrain tectum that involves the oculomotor nerve fascicles and superior cerebellar peduncle, causing bilateral oculomotor nerve palsy and limb ataxia, respectively (96; 97; 74).
The most common cause of Nothnagel syndrome is a neoplasm of the midbrain tectum, but the syndrome can be caused by a tectal hemorrhage (122). Nothnagel syndrome commonly causes bilateral oculomotor nerve dysfunction, but the limb ataxia may be either unilateral or bilateral (96; 97; 32; 122; 18; 74; 04; 115; 132; 119).
Pontine syndromes.
Raymond syndrome. Raymond syndrome is a ventral medial mid-pontine syndrome with ipsilesional abducens palsy, variable contralesional central facial paresis, and contralesional hemiparesis (107; 145).
Example case of Raymond syndrome (152). A 50-year-old man with hypertension, congestive heart failure, and polysubstance abuse experienced the acute onset of horizontal diplopia, left-sided drooling, and left-sided weakness. On examination, he had right abducens palsy, left central facial paresis, left hemiparesis, and left-side hyperreflexia. The findings were consistent with those of classic Raymond syndrome with facial nerve involvement. Brain MRI 5 days after symptom onset showed a subacute infarct in the right midpons. His symptoms improved significantly in 3 days while on anticoagulation.
Zaorsky and Luo proposed the existence of two types of Raymond syndrome: (1) the "classic type," which may be produced by a lesion in the mid-pons involving the ipsilateral abducens fascicle and the non-decussated corticofacial and corticospinal fibers (68; 121; 152); and (2) the "common type," with a lesion involving the ipsilateral abducens fascicle and non-decussated corticospinal but sparing the corticofacial fibers (116; 99; 98; 82; 152). A lesion in the more dorsal area may produce an isolated abducens nerve palsy (33), whereas a lesion in the ventral caudal pons may produce Millard-Gubler syndrome with ipsilateral abducens and facial paralysis and contralateral hemiplegia (149; 80).
(Source: Zaorsky NG, Luo JJ. A case of classic Raymond syndrome. Case Rep Neurol Med 2012;2012:583123. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creativecommons.org/licenses/by/4.0.)
(Source: Zaorsky NG, Luo JJ. A case of classic Raymond syndrome. Case Rep Neurol Med 2012;2012:583123. Creative Commons Attribution 4.0 International [CC BY 4.0] license, creativecommons.org/licenses/by/4.0.)
Therefore, contralateral central facial paresis may occur due to a unifocal lesion of the basis pontis (68; 121; 152). In at least some people, corticofacial fibers loop down into the ventral part of the upper medulla, cross the midline, and ascend in the dorsolateral medullary region to the facial nucleus (133). The corticofacial projection has also been identified in the medial lemniscus as an aberrant pyramidal tract in the pons through the upper medulla (148).
Superior cerebellar artery syndrome. The features of infarction in the territory of the superior cerebellar artery, involving the posterolateral midbrain and upper lateral pons, potentially include the nucleus and fascicle of CN IV and the nucleus of CN V, as well as the sympathetic tract, spinothalamic tract, medial lemniscus, superior cerebellar peduncle, superior cerebellum (including the superior vermis), and the dentate and fastigial nuclei.
The initially reported cranial polyneuropathy of superior cerebellar artery syndrome was supranuclear involvement of CN V (contralesional), VII (contralesional emotional facial paresis), and VIII (contralesional). Later studies found that this "classic syndrome of the superior cerebellar artery" is uncommon among cases with isolated superior cerebellar artery-territory infarction, with most cases having strictly cerebellar findings (114; 29; 57; 06; 129). Later authors recognized other variable features of superior cerebellar artery infarction, including coma (29; 07), ipsilesional Horner syndrome (42; 75; 36), transient blurred vision (07), diplopia with variable ipsilesional involvement of cranial nerve nuclei or fascicles III, IV, and VI (42; 75; 36), vertigo with nausea and vomiting (36), dysarthria (42; 07; 01), transient ipsilesional chorea or "pseudo-athetotic movements" (29; 57; 36), and ipsilateral hypotonia (110; 29; 42; 07).
Anterior inferior cerebellar artery syndrome. Anterior inferior cerebellar artery syndrome is a syndrome of posterolateral pontine dysfunction potentially involving multiple cranial nerve nuclei (V, VII, vestibular and cochlear nuclei of VIII) and fascicles (VII, VIII), as well as the sympathetic tract, spinothalamic tract, middle cerebellar peduncle, anteroinferior cerebellum (including the flocculus), and the vestibular labyrinth and cochlea (02).
The so-called Millard-Gubler syndrome. Despite numerous erroneous textbook and case report descriptions of Millard-Gubler syndrome as ipsilesional palsy of cranial nerves VI and VII with contralesional hemiplegia, the syndrome as originally described is simply a crossed paresis of the peripheral facial nerve on the lesion side and a contralateral (crossed) hemiparesis (47; 83; 142).
Ipsilesional palsy of cranial nerves VI and VII may occur without a gaze palsy (sparing the sixth nerve nucleus) and with only "slight" transient contralesional hemiplaresis (46).
Note the depressed left corner of the mouth and a flattening of the left nasolabial fold. "Complete paralysis of the left sixth and facial nerves (with inability to move the right eye towards the left) from an acute lesion on t...
Facial colliculus syndrome. Facial colliculus syndrome involves the abducens nerve nucleus, the facial nerve fibers at the genu (and by default, the medial longitudinal fasciculus), resulting in an ipsilateral gaze palsy and a peripheral facial paresis. In younger patients, tumors, demyelination, and viral rhombencephalitis are potential causes, whereas in older patients, the cause is usually an ischemic or hemorrhagic stroke. This is something that occurs frequently and consistently enough to be a "syndrome," and the name is anatomically meaningful (rather than the alternate conceptually problematic terminology of "8-and-a-half" syndrome). Bilateral facial colliculus syndrome has been reported due to a paradoxical embolism and pontine infarction (154).
Defoville (Foville) syndrome. The defining features of Defoville syndrome (sometimes called Foville syndrome) are ipsilateral abducens palsy, gaze palsy, or one-and-a-half syndrome, ipsilateral peripheral facial palsy, and contralateral (crossed) hemiparesis (40; 90; 100; 94; 19; 77; 117; 17). Variable features, depending on the extent of the lesion, can include ipsilateral Horner syndrome, facial hypoesthesia, peripheral deafness, vertigo, dysphagia, and hoarseness, along with contralateral (crossed) hemihypesthesia. These findings typically result from compromised blood flow to the medial caudal pons from obstruction of perforating branches of the basilar artery, although cases have been reported due to pontine vascular (ie, hemorrhage, angioma, or arteriovenous malformation) or malignant lesions (100; 94; 78; 17). This locus includes the sixth nerve nucleus (gaze palsy or one-and-a-half syndrome), the facial nerve fascicle (peripheral facial palsy), the basis pontis (hemiparesis), and the medial lemniscus (crossed hemihypesthesia).
Example case of Defoville (Foville) syndrome (17). A 65-year-old man presented with a 10-day history of sudden-onset binocular diplopia, tinnitus, and gait disturbance. He was taking daily acetylsalicylic acid for the primary prevention of cardiovascular disease. He reported a 50-pack/year history of smoking and chronic alcohol intake (not further specified). His general practitioner introduced an angiotensin II-receptor blocker (candesartan 4 mg daily) on symptom onset. Neurologic examination revealed a left abducens palsy, a left peripheral facial nerve palsy, and a contralateral face-sparing hemiparesis. He reported mild right-sided dysesthesia. MRI of the brain revealed a left-sided brainstem cavernous malformation of the floor of the fourth ventricle with evidence of recent extralesional bleeding and an associated developmental venous anomaly draining both sides of the cerebellum directly into the vein of Galen. The co-existence of an ipsilesional abducens and peripheral facial nerve palsies and a contralesional face-sparing hemiparesis indicated an inferior medial pontine syndrome, specifically the Defoville (Foville) syndrome.
(Source: Beucler N, Boissonneau S, Ruf A, Fuentes S, Carron R, Dufour H. Crossed brainstem syndrome revealing bleeding brainstem cavernous malformation: an illustrative case. BMC Neurol 2021;21[1]:204. Creative Commons Attribut...
(Source: Beucler N, Boissonneau S, Ruf A, Fuentes S, Carron R, Dufour H. Crossed brainstem syndrome revealing bleeding brainstem cavernous malformation: an illustrative case. BMC Neurol 2021;21[1]:204. Creative Commons Attribut...
Note the black arrow showing the drift of the outstretched right arm. (Source: Beucler N, Boissonneau S, Ruf A, Fuentes S, Carron R, Dufour H. Crossed brainstem syndrome revealing bleeding brainstem cavernous malformation: an i...
Note that he is pulling up on his pants to sustain holding his left leg off of the bed. (Source: Beucler N, Boissonneau S, Ruf A, Fuentes S, Carron R, Dufour H. Crossed brainstem syndrome revealing bleeding brainstem cavernous ...
Acetylsalicylic acid was stopped. Considering this was the first bleeding episode, the non-exophytic character of the pontine hemorrhage, and the mild degree of disability, he was managed conservatively. Five months later, he was admitted for recurrent symptoms with a House-Brackman grade V peripheral facial palsy and complete abducens palsy on the left side, associated with contralateral face-sparing hemiparesis. Brain CT showed rebleeding. After 2 weeks of close monitoring in the intensive care unit, the brainstem cavernous malformation was excised, but the developmental venous anomaly was left intact. The postoperative course was complicated by (1) a surgical-site infection requiring surgical revision, placement of a temporary external ventricular drain, and combined antibiotic therapy; (2) a left-sided House-Brackmann grade VI peripheral facial nerve palsy, which was complicated by a corneal ulcer; and (3) a left-sided glossopharyngeal nerve palsy causing dysphagia and aspiration pneumonia and requiring a temporary gastroplasty. The patient was discharged to neurologic rehabilitation 3 months after the procedure.
Post-contrast T1-weighted sequence. A suboccipital telovelar approach was used to gain access to the rhomboid fossa (D). Then the infrafacial triangle was used as an entry point to the pons (C) to perform microsurgical excision...
Surgical sequences in a 65-year-old man with Defoville (Foville) syndrome caused by a medial pontine hematoma from a brainstem cavernous malformation. (A) Hockey stick fashion opening of the dura mater, discovering the cerebell...
Medullary syndromes.
Lateral medullary syndrome. The features of lateral medullary syndrome from occlusion of the vertebral artery or the posterior inferior cerebellar artery were largely explicated in the late 19th century and potentially include multiple cranial nerve nuclei (V, vestibular nuclei of VIII, IX, X) and fascicles (IX, X), as well as the sympathetic tract, spinothalamic tract, inferior cerebellar peduncle, and the posteroinferior cerebellum (including the uvula and nodulus of the inferior vermis) and the paraflocculus. Wallenberg thought the syndrome was due to embolization of the posterior inferior cerebellar artery (136; 137); however, the most common cause is thrombosis of the vertebral artery.
Opalski syndrome. Opalski syndrome results from the extension of a lateral medullary lesion caudally to the corticospinal tracts after their decussation, resulting in lateral medullary syndrome with ipsilesional hemiparesis or hemiplegia (27; 86; 61; 43; 92; 103; 104; 62; 49; 109). The pattern of weakness in Opalski syndrome differentiates it from that in the Babinski-Nageotte syndrome, in which the corticospinal tract is involved before the decussation, causing the lateral medullary syndrome with contralesional hemiparesis or hemiplegia. Opalski syndrome may be associated with 5th or 7th cranial nerve palsy (109).
Medial medullary syndrome. According to Dejerine's triad, medial medullary infarction consists of (1) contralateral hemiplegia sparing the face, (2) contralateral loss of deep sensation, and (3) ipsilateral hypoglossal paralysis (31). Medial medullary syndrome typically produces dysfunction of a single cranial nerve, a nuclear or fascicular lesion of the hypoglossal nerve; however, bilateral medial medullary infarction is not uncommon, and this often includes bilateral hypoglossal nerve palsy, as well as other cranial nerve involvement, depending on the extent of the responsible lesion (131).
Babinski-Nageotte and Cestan-Chenais syndromes. Unfortunately, in many textbooks, Babinski-Nageotte syndrome is incorrectly used synonymously with the hemimedullary syndrome. Babinski-Nageotte syndrome is an intermediolateral medullary syndrome with extension of the “Wallenbergian” lateral lesion to the corticospinal tract, resulting in the lateral medullary syndrome with contralateral hemiparesis or hemiplegia (93; 30; 54; 127; 102; 22; 79). Symptoms include ipsilesional cerebellar ataxia, facial sensory impairment, and Horner syndrome, along with weakness and loss of sensation on the contralesional side of the body.
Babinski-Nageotte syndrome is intermediate between the Reinhold hemimedullary syndrome and the lateral medullary syndrome (Wallenberg syndrome) but is distinct from Cestan-Chenais syndrome (65; 66).
The rare Cestan-Chenais syndrome includes all symptoms of Babinski-Nageotte syndrome except the ipsilateral hemiataxia caused by sparing of the posterior spinocerebellar tract (21; 66).
Reinhold hemimedullary syndrome. The hemimedullary syndrome is essentially a combination of the lateral and medial medullary syndromes. Hemimedullary syndrome results from occlusion of a vertebral artery proximal to the posterior inferior cerebellar artery and its anterior spinal artery branches (66).
Avellis syndrome. Avellis syndrome is characterized by ipsilesional paralysis of the soft palate and vocal cords and contralesional loss of pain sensation and temperature sense (09). Avellis syndrome usually results from occlusion of the vertebral artery with ischemic damage to the nucleus ambiguous and pyramidal tract. Horner syndrome may be associated. In the original description, the vagus and glossopharyngeal nerves were involved (09); concomitant involvement of the neighboring cranial nerves was observed later (63).
Prognosis depends on the underlying pathology of the primary lesions.
|
Pathological conditions that can cause pseudobulbar palsy include the following: | |
|
• traumatic brain injury | |
|
• cerebrovascular diseases (eg, multi-infarct dementia, subcortical arteriosclerotic encephalopathy or Binswanger disease, bilateral thalamic infarction) | |
|
• neurodegenerative disease (eg, progressive supranuclear palsy, amyotrophic lateral sclerosis, progressive subcortical gliosis) | |
|
• limbic encephalitis | |
|
• neoplasms (eg, brainstem glioma, glioblastoma with spread across the midline, multiple cerebral metastases) | |
|
• demyelinating disorders (eg, multiple sclerosis, progressive multifocal leukoencephalopathy, cerebral malaria) | |
|
• metabolic abnormalities (eg, osmotic demyelination, Hashimoto encephalitis) | |
|
• neurotoxicity (eg, toluene, methotrexate) | |
|
• infectious disorders (general paresis or neurosyphilis, neurocysticercosis, subacute bacterial endocarditis) | |
|
• neurodevelopmental disorders of the opercular or insular cortex | |
|
Pathological conditions that can cause cranial neuropathies due to intrinsic pathology of the brainstem include the following: | |
|
• traumatic and penetrating brain injury | |
|
• cerebrovascular diseases (eg, anterior inferior cerebellar artery, posterior inferior cerebellar artery, superior cerebellar artery, top of the basilar) | |
|
• neoplasms (eg, brainstem glioma, cerebral metastases) | |
|
• demyelinating disorders (eg, multiple sclerosis) | |
|
• neurodegenerative disorders (eg, amyotrophic lateral sclerosis, Kennedy disease, syringobulbia) | |
|
• metabolic abnormalities (eg, osmotic demyelination) | |
|
• infectious disorders (general paresis or neurosyphilis, tuberculoma) | |
|
• genetic disorders (eg, Kennedy spinal and bulbar muscular atrophy, Wolfram syndrome, sickle cell disease) | |
|
• inflammatory or infective diseases (eg, bulbar poliomyelitis, West Nile virus encephalitis) | |
|
• Although multiple intracranial nerve palsies are not rare, no figures are available on the incidence or prevalence due in part to the multiplicity of disease processes involved. | |
|
• Crossed brainstem syndromes are rare except for Wallenberg syndrome. |
Although multiple intracranial nerve palsies are not rare, no figures are available on the incidence or prevalence due in part to the multiplicity of disease processes involved.
Crossed brainstem syndromes are rare except for Wallenberg syndrome. In a study of 308 consecutive patients with signs and symptoms indicative of acute brainstem infarction, only about 6% matched clinical criteria for recognized crossed brainstem syndromes, yet more than 20% showed different, so far unnamed, crossed symptom combinations (80). By far, most recognized cases of crossed symptom combinations had Wallenberg syndrome: 14 had Wallenberg syndrome, two had Babinski-Nageotte syndrome, two had Raymond-Cestan syndrome, one had Weber syndrome, and one had Claude syndrome (80).
No information is available on preventing intramedullary cranial nerve palsies per se; however, some of the underlying diseases (eg, stroke, syphilis, and tuberculosis), which may incidentally cause intramedullary cranial nerve palsies, may be partially preventable.
The differential diagnosis of multiple cranial nerve palsies involves several important steps:
|
(1) Localization of nervous system involvement, based on the specific cranial nerves involved, as well as other accompanying neurologic manifestations and CNS imaging studies. | |
|
(2) Exclusion of pseudo-cranial neuropathies (eg, supranuclear and internuclear disorders, Graves' orbitopathy and restrictive myopathy, myasthenia gravis). | |
|
(3) Determination of the pathology of the lesion based on laboratory, radiologic, and pathologic studies. |
Intramedullary cranial polyneuropathies must be distinguished from extramedullary cranial polyneuropathies. Intramedullary cranial polyneuropathies can be supported by clinical signs (eg, crossed brainstem syndromes, long track signs) and neuroimaging.
|
• MRI is more sensitive than CT to early parenchymal changes of brainstem infarction and other brainstem pathology (eg, demyelinating disorders, arteriovenous malformations, mass lesions). | |
|
• Extracranial neurovascular ultrasound and transcranial Doppler provide alternative methods for acquiring real-time information about vertebrobasilar hemodynamics and the vascular wall of the vertebral arteries. | |
|
• CTA or MRA provides an anatomic assessment of the flow in the vertebrobasilar system and its larger branches (posterior inferior cerebellar artery, anterior inferior cerebellar artery, superior cerebellar artery). | |
|
• Extracranial neurovascular ultrasound and transcranial Doppler provide alternative methods for acquiring real-time information about vertebrobasilar hemodynamics and the vascular wall of the vertebral arteries. |
During the hyperacute phase of ischemic stroke management, CT and CTA are practical and informative and are built into many protocols, although CT does not image the brainstem well. CT perfusion is of low utility for brainstem vascular disorders because CT perfusion protocols are centered on the basal ganglia and supra-ganglionic level, which excludes the posterior fossa; in addition, small infarcts are poorly visualized on perfusion maps due to their low resolution.
MRI is more sensitive than CT to early parenchymal changes of brainstem infarction and other brainstem pathology (eg, demyelinating disorders, arteriovenous malformations, mass lesions). Its clinical application during the hyperacute phase of ischemic stroke management is limited by its availability in many institutions. MRI diffusion-weighted imaging sequences and apparent diffusion coefficient maps increase the sensitivity of detecting ischemic brainstem tissue, even in the hyperacute stage. In infratentorial strokes, multiple DWI lesions and a distribution of subsidiary, clinically silent DWI lesions in the anterior circulation suggest a cardioembolic stroke etiology (35). With infratentorial strokes, DWI lesion volume does not correlate with the NIHSS scores and does not predict outcome (35). Gradient refocusing echo sequences can demonstrate small areas of hemorrhagic transformation.
CTA or MRA provides an anatomic assessment of the flow in the vertebrobasilar system and its larger branches (posterior inferior cerebellar artery, anterior inferior cerebellar artery, superior cerebellar artery). Extracranial neurovascular ultrasound and transcranial Doppler provide alternative methods for acquiring real-time information about vertebrobasilar hemodynamics and the vascular wall of the vertebral arteries.
Catheter cerebral angiography is reserved for individuals whose noninvasive testing does not provide sufficient information to make appropriate therapeutic decisions.
Management depends on the underlying etiology.
The outcome of treatment depends on the cause of nerve palsies and the method of treatment.
Problems can arise during anesthesia in children with Moebius syndrome. There is a high incidence of difficult or failed intubation, with the potential for problems with aspiration of oral secretions. Premedication to reduce salivary secretion is recommended. Children with Moebius syndrome have a high incidence of other anomalies, including congenital heart disease.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jul. 16, 2026
Peripheral Neuropathies
Jul. 14, 2026
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026