














Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Myofascial syndrome is defined as a pain disorder involving pain referred from trigger points within myofascial structures, either local or distant to the pain. This article discusses the clinical features, pathogenesis, differential diagnosis, and management of myofascial pain disorder. Starting with the classical work of Travell in the 1980s, this article goes on to describe some of the more recent efforts to manage this syndrome.
|
• Active trigger points are characterized by specific patterns of pain radiation during palpation that depend on the location of the trigger point. | |
|
• Patients who respond to treatment in the acute phase usually have a good prognosis, but chronic nonresponsive patients are a problem in management. | |
|
• Myofascial pain syndrome should be differentiated from other painful conditions involving muscles, such as fibrositis. | |
|
• Noninvasive techniques of management include counterpoint stimulation, spray and stretch, massage, Kinesio taping, and topical medication patches. | |
|
• Various modalities of electrical stimulation include transcutaneous electrical stimulation, pulsed electric neuromuscular stimulation, and pulsed radiofrequency. | |
|
• Injections into myofascial trigger points are usually local anesthetics, but botulinum toxin has also been used. |
Sir William Gowers introduced the term fibrositis for a common, but idiopathic, localized form of muscular rheumatism that is now recognized as myofascial pain syndrome (21).
According to Gowers in 1904, the term “fibrositis” referred to the local tenderness and regions of palpable hardness in the muscle, which he attributed to inflammation of fibrous tissue. Though initially embraced in the literature, the concept of fibrositis as inflamed connective tissue fell into disfavor as subsequent biopsy data failed to substantiate inflammatory pathology. It was not until the late 1930s that Kellgren provided evidence for the pathomechanism and nature of pain originating from deep connective tissue structures (28). Using hypertonic saline injections to irritate different anatomical areas, including fascia, tendon, and muscle, he demonstrated that pain was produced that differed not only in quality but also in its specific referral pattern. Although the term "myofasciitis" was first introduced in 1927 by Albee, it was not until 1939 that Steindler first used the terms "myofascial pain" and "trigger point" (02; 59). Travell and colleagues used the term trigger point in 1942 to describe the site from which pain was referred, and in 1952, adopted the expression "myofascial pain syndrome" (64; 63). In 1954, Schwartz reported that inactivation of trigger points by procaine injection was often an important part of the management of pain in the temporomandibular joint region (49). According to Travell, it was Good who recognized the pathognomonic trademark of myofascial pain syndrome, now called the “jump sign,” where a patient responded with a cry, grimace, or wince to palpation of the painful muscle focus (65).
Travell first published a paper describing the diagnostic criteria and treatment protocols for myofascial pain syndrome in 1942, which laid the foundation for the modern approach to this syndrome. In 1953, Bonica published a text separating myofascial pain syndrome from fibrositis (08). The subsequent work of Travell and Simons elucidated trigger points and zones of radiating pain, as well as the taut bands of myofascial pain syndrome, codifying their locations in virtually every muscle of the body (65; 66). Using the classification of the International Association for the Study of Pain, such localized disease was termed "specific myofascial pain syndrome" (40). Specific terms are being used to describe involvement of certain anatomical regions, eg, myofascial pain dysfunction syndrome in the case of the temporomandibular joint.
Controversies in nomenclature. A source of controversy relative to the acceptance of the concepts of myofascial pain and dysfunction has been the varied terminology used throughout the literature. The term “fibrositis” has been used erroneously to include both myofascial pain syndrome and fibromyalgia, as well as almost any unexplained musculoskeletal pain problem. Other terms used in the past include “myogelosis,” “muscle hardening,” and “muscular rheumatism.” The confusion in nomenclature has been compounded by the widespread belief that these musculoskeletal pain syndromes are psychogenic in nature. As late as the 1970s, most major textbooks considered fibrositis to be a disease with strong psychogenic overtones (48). The terms nonarticular and psychogenic rheumatism, soft tissue disability, tension myalgia, and muscle contraction states also have remained in use, suggesting psychologic dysfunction as their primary cause as opposed to physical factors. Similarly, terms, including overuse syndromes, repetitive trauma syndromes, and repetitive injury or strain syndromes, fail to address the more critical issues regarding pathogenesis, with many of these overlapping disorders representing local forms of myofascial pain, which apparently have not been appreciated as such. No universally accepted terminology enables clinicians to more accurately codify the dysfunction seen in patients who present with musculoskeletal pain and dysfunction.
|
• Myofascial pain syndrome manifests as pain and tenderness localized to a trigger point in a single muscle or region with a unique pattern of radiating pain. | |
|
• Myofascial pain syndrome can involve muscles in various parts of the body. | |
|
• Usually there are no neurologic deficits in myofascial pain syndrome but there can be some autonomic phenomena and local peripheral nerve compression at the site of muscle involvement. |
Myofascial pain is the most common form of musculoskeletal pain and refers to a spectrum of clinical presentations distinct from other musculoskeletal conditions, such as fibromyalgia, strains, and sprains. Myofascial syndrome is defined as a pain disorder involving pain referred from trigger points within myofascial structures, either local or distant from the pain. A trigger point is defined as a localized tender area within a taut band of skeletal muscle or its associated fascia. These points occur most frequently in the head, neck, shoulders, and lower back. Active trigger points are also characterized by specific patterns of pain radiation during palpation that depend on the location of the trigger point. The patterns of referral for each trigger point are consistent among different persons. Myofascial pain due to active trigger points can present as an acute, recurrent, or chronic pain syndrome. The patient with acute-onset myofascial pain usually associates the onset of pain with a specific overload of the muscles and, therefore, expects it to be self-limited like post-exercise soreness. The mechanisms that produce the symptoms of myofascial pain are also largely speculative. Travell and Simon have proposed that the initial changes may be precipitated by such factors as local trauma, fatigue of the muscles from repeated overuse, chronic postural imbalance, and psychological distress (66). The characteristics of myofascial pain syndrome may long outlast the initiating events, setting up a self-generating pain cycle that is perpetuated through lack of proper treatment, sustained muscle tension, distorted muscle posture, pain-reinforcing behavior, and the failure to reduce other contributing factors, such as sleep disturbances. Generally, no neurologic deficits are associated with this syndrome, unless neurovascular compression with weakness and diminished sensation coincide with the muscle trigger points.
Signs and symptoms. The principal clinical features of myofascial pain syndrome include pain and tenderness localized to a single muscle or region, associated with a unique and stereotypic pattern of radiating pain. Palpation of the affected muscles reveals a hyperirritable focus of localized pain, which is discrete and lies within a structure known as the "taut band." A taut band is defined as an area within skeletal muscle of increased consistency or hardness that extends along the length of the muscle and runs parallel to the direction of the muscle fibers at that point in the muscle. The localized pain within the taut band is known as a "trigger point."
Trigger points are classified as either active or latent and range from 2 to 5 mm in diameter. Active trigger points are hypersensitive and can be associated with two types of pain that may occur spontaneously with muscle use or with palpation on examination. Most commonly, a sharp localized pain that is well demarcated can be elicited, as can a radiating or referred pain, described as deep (subcutaneous and muscular) and aching in character, with slightly blurred edges that project well beyond the originating trigger point. The region of referred pain within the myotome specific for each individual muscle-derived trigger point displays continuous pain in a "zone of reference." These pain reference zones, which remain stereotypic between individuals, may or may not mimic more traditionally recognized dermatomal, myotomal, or sclerotomal referred pain patterns. The associated symptoms observed with active trigger points include muscle stiffness, tenderness, and pain that radiates (41). Without perpetuating factors, referred pain may spontaneously subside within a few days or weeks, and an active trigger point tends to revert to and persist as a latent trigger point. When latent, the trigger points are quiescent and result primarily in muscle tightness and dysfunction without the presence of persistent or spontaneous pain except when palpated. In the presence of one or more perpetuating factors, trigger points usually persist and become chronic. They may then propagate to other muscles as secondary and satellite trigger points.
|
Local pain and tenderness |
Usually limited to one or a few discrete muscles within a specific region or miotic unit. |
|
Taut band |
A discrete area of increased consistency or hardness within a muscle and associated with a trigger point. |
|
Active trigger point |
A hyperirritable focus within a taut band that is tender on palpation and refers pain in a characteristic pattern unique to the muscle. |
|
Latent trigger point |
A subclinical trigger point that does not spontaneously cause pain but elicits a zone of muscle-specific referred pain on palpation. |
|
Satellite trigger point |
A trigger point that becomes active because it falls within the zone of reference of another trigger point. |
|
Zone of reference |
A unique region within the myotome specific to each muscle-derived trigger point and to which pain, paresthesias, and tenderness may refer. |
|
Trigger point inactivation |
The immediate alleviation of pain and weakness by elongation of the muscle or trigger point injection. |
|
Epiphenomena |
Neurovascular entrapment, referred to as autonomic phenomena, psychosocial dysfunction, and deconditioning. |
|
Myotatic unit |
A group of agonist and antagonist muscles, which function together as a unit because they share common spinal reflex responses. |
Referred pain. Patients' patterns of referred pain elicited from trigger points in a muscle are reproducible, predictable, and are often the key to the diagnosis of a myofascial pain syndrome. Though pain referred from visceral internal organs to somatic body structures is well recognized by physicians (ie, myocardial ischemia, peptic ulcer disease, and pancreatitis), the irritable areas such as myofascial trigger points in skeletal muscle may cause pain to be perceived in distant locations. The seminal work by Louis and Kellgren documented and mapped the stereotypical referred pain patterns of many major muscles by injecting hypertonic saline into the muscles of numerous volunteers and themselves (28). Less appreciated is an associated phenomenon, referred tenderness, which can often be elicited at the site of pain referral.
Autonomic phenomena. Focal or regional autonomic dysfunction, including localized vasoconstriction, persistent hyperemia after palpation, diaphoresis, lacrimation, coryza, salivation, and pilomotor activity, is often associated with trigger point presentation. Because of these associated findings, myofascial pain syndrome may represent one of the milder variants of the autonomically mediated reflex neurovascular syndromes. Disturbance of vestibular function and space perception may originate in trigger points in the clavicular division of the sternocleidomastoid muscle. They can cause imbalance and disorientation of the body in space and postural dizziness. Visual disturbances are also reported with sternocleidomastoid trigger points and include blurring of vision and intermittent double vision without pupillary changes. Tinnitus has been reported to be associated with trigger point palpation in the masseter muscle as well.
Neurovascular entrapment. When a nerve passes through a muscle between taut bands, or when a nerve lies between taut trigger point bands and bone, the pressure exerted on the nerve can produce neurapraxia--the loss of nerve conduction--but only in the region of compression. Occasionally, EMG evidence shows a minor degree of neurotmesis (axonal loss) in addition to neurapraxia. The patient with one of these entrapments is likely to have two kinds of symptoms: (1) aching pain referred from trigger points in the involved muscle, and (2) nerve compression effects of numbness and tingling, hypesthesia, and sometimes hyperesthesia. The signs and symptoms of partial neurapraxia may sometimes be relieved within minutes after inactivation of the responsible myofascial trigger point, which immediately relaxes the taut bands. Effects of severe compression may require days or weeks for full recovery. Several common neurovascular entrapment syndromes are now associated with specific, single-muscle myofascial syndromes.
|
Nerve or vessel |
Muscle |
Clinical syndrome |
|
Greater occipital nerve |
Semispinalis capitis |
Occipital neuralgia |
|
Brachial plexus (lower trunk) subclavian vessels |
Scalenes |
Thoracic outlet syndrome |
|
Sciatic and pudendal nerve, gluteal vessels |
Piriformis |
Piriformis syndrome or "pseudosciatica" |
|
Ulnar nerve |
Flexor carpi ulnaris |
Ulnar nerve palsy |
|
Buccinator nerve |
Lateral pterygoid |
Focal facial numbness |
|
Posterior primary rami |
Paraspinal musculature |
Paraspinal dysesthesias |
|
Brachial plexus and axillary artery |
Pectoralis minor |
Costoclavicular syndrome |
|
Pterygoid venous plexus |
Masseter |
Hemifacial edema |
|
Deep radial nerve |
Supinator |
Extensor weakness of the hand, wrist dysesthesias |
Psychosocial dysfunction. As with many chronic pain conditions, concomitant social, behavioral, and psychological disturbances may precede or follow the development of pain. Patients may report psychological symptoms, such as frustration, anxiety, depression, and anger if acute cases become chronic through inadequate treatment. There is no evidence that behavioral symptoms are more common in patients with myofascial pain than in those with other chronic pain disorders.
Myotatic dysfunction. The myotatic unit is emphasized because the presence of an active trigger point in one muscle of the myotoxic unit is often accompanied by dysfunction in other muscles of the unit, which may develop trigger points as well (65). The propensity for myofascial foci to spread and to develop secondary and satellite trigger points in adjacent muscles of the myotoxic unit provides a mechanism by which myofascial pain from single muscle syndromes can become regional. Though the myotoxic unit is defined as including the synergists, which help the prime mover (agonist), and the antagonists that oppose the agonist, the definition is sometimes extended to include the proximal stabilizer muscles of the shoulder or hip.
Common myofascial syndromes. Myofascial pain syndrome was traditionally viewed as a single-muscle syndrome that may combine to form complex patterns involving many muscles in several regions of the body. Particularly with the patient who has regional pain, it is important to break the problem into its component parts. The most frequently encountered muscles developing myofascial trigger points, categorized by anatomical region, include:
|
(1) head: masseter, temporalis, lateral pterygoid, and medial pterygoid | |
|
(2) head and neck: trapezius and sternocleidomastoid | |
|
(3) neck: levator scapulae and scalenes | |
|
(4) shoulder and arm: infraspinatus and supinator | |
|
(5) back and hip: quadratus lumborum and piriformis. |
Following is a description of the component parts of these frequently encountered single muscle syndromes, categorized by anatomical region in the body. The individual descriptions of each single muscle syndrome are uniformly arranged relative to symptoms, typical referred pain patterns, common activating and perpetuating mechanisms, and associated entrapments. Several of the more common myofascial syndromes reviewed will be immediately recognized as a cause of pain and dysfunction that confronts the clinician daily.
Head
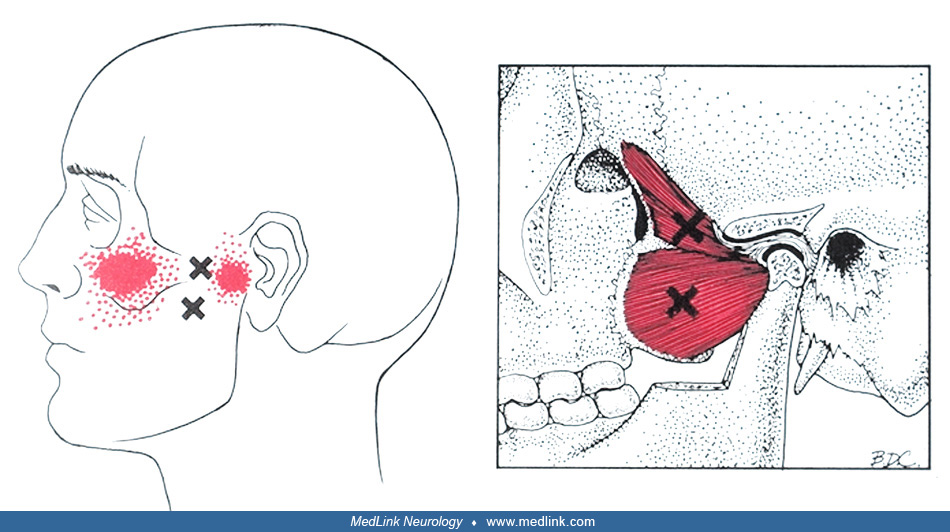
Trigger point: masseter (both superficial and deep points)
|
• Signs and symptoms: TMJ pain and trismus, “sinusitis-like" pain, upper or lower molar pain, and hypersensitivity of teeth, ipsilateral tinnitus. | |
|
• Referred pain patterns: Jaw, adjacent teeth and gums; (A) Maxilla, upper teeth and gums; (B) Eyebrow, temple to jaw; (C) Lower molars and jaw; (D) Pain deep in ear and TMJ. | |
|
• Activation and perpetuation: Bruxism and occlusional disorders, as in dental procedures; gross trauma; normal chewing tolerated. | |
|
• Entrapment syndromes: Compression of the pterygoid venous plexus results in engorgement, producing infraorbital puffiness and hemifacial edema. |
Trigger point: temporalis
|
• Signs and symptoms: Temporal headache, pain above and behind the eye, and maxillary toothache. | |
|
• Referred pain patterns: Temporoparietal and supraorbital pain, downward to upper incisor, maxillary teeth, and TMJ. | |
|
• Activation and perpetuation: Same as masseter. | |
|
• Entrapment syndromes: None. |
Trigger point: lateral pterygoid
|
• Signs and symptoms: A frequent cause of TMJ dysfunction and misalignment. Autonomic symptoms of excess sinus secretions mimic sinusitis. | |
|
• Referred pain patterns: Primary source of referred pain to TMJ and maxilla. | |
|
• Activation and perpetuation: Malocclusion and bruxism. Pain with chewing is proportional to the vigor of the movement. | |
|
• Entrapment syndromes: Entrapment of the buccal nerve causes paresthesias of the cheek and gum and weakness of the buccinator muscle. |
Trigger point: medial pterygoid
|
• Signs and symptoms: Sore throat, difficult and painful swallowing. Ear stuffiness. Restricted jaw opening. | |
|
• Referred pain patterns: Vague pain referred to the back of the mouth, pharynx, and tongue but not the teeth. Below and behind the TMJ, and deep into the ear. | |
|
• Activation and perpetuation: Usually activated secondary to lateral pterygoid involvement, as it is rarely involved alone. Occlusional imbalance. | |
|
• Entrapment syndromes: Ear stuffiness (barohypoacusis) due to medial pterygoid trigger points, which restrict the tensor veli palatini from opening the eustachian tube. |
Head and neck
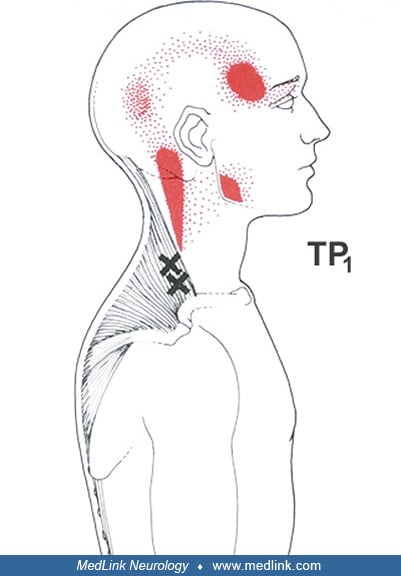
Trigger point: trapezius
|
• Signs and symptoms: Tension head and neck ache; deep suprascapular ache; interscapular burning pain; aching on top of the shoulder; dizziness, most likely due to coactivation of sternocleidomastoid muscle trigger points. | |
|
• Referred pain patterns: Posterolateral neck and temple cervico-occipital and acromion. Medial scapular and paraspinal TP-7 causes a nonpainful "shivery" sensation on lateral arm with pilomotor erection. | |
|
• Activation and perpetuation: Acute trauma as with falls or whiplash. Repetitive stress from prolonged elevation and extension of the arms as when typing, or overloading its key role in neck stabilization with tilt of the shoulder-girdle axis. | |
|
• Entrapment syndromes: The trapezius contributes a shearing stress to the primary entrapment of the greater occipital nerve by the semispinalis capitus as it emerges below the occiput. |
Trigger point: sternocleidomastoid
|
• Signs and symptoms: Atypical facial pain associated with visual blurring, tearing, and ptosis (orbicularis spasm) is seen with sternal sternocleidomastoid muscle trigger points. Clavicular trigger points cause tension headaches, postural dizziness, and disequilibrium with veering. | |
|
• Referred pain patterns: Although the two divisions of the sternocleidomastoid muscle have distinct facial and cranial pain patterns, neither refers pain to the neck. Throat pain and focal swelling have been reported. | |
|
• Activation and perpetuation: Protracted neck rotation (from sleeping on two pillows) or neck extension (working overhead). Postspinal headaches that can activate sternocleidomastoid muscle trigger points have been reported to produce a chronic myofascial headache. | |
|
• Entrapment syndromes: Entrapment of the spinal accessory nerve as it emerges through the sternocleidomastoid muscle may cause paresis of the ipsilateral trapezius muscle. |
Neck
Trigger point: levator scapulae
|
• Signs and symptoms: The most common cause of "stiff neck." Painful limitation of ipsilateral neck rotation. | |
|
• Referred pain patterns: At the angle of the neck, extending to the medial scapular border and posterior shoulder. | |
|
• Activation and perpetuation: Prolonged turning of the head and neck and unilateral shoulder shrugging. | |
|
• Entrapment syndromes: None. |
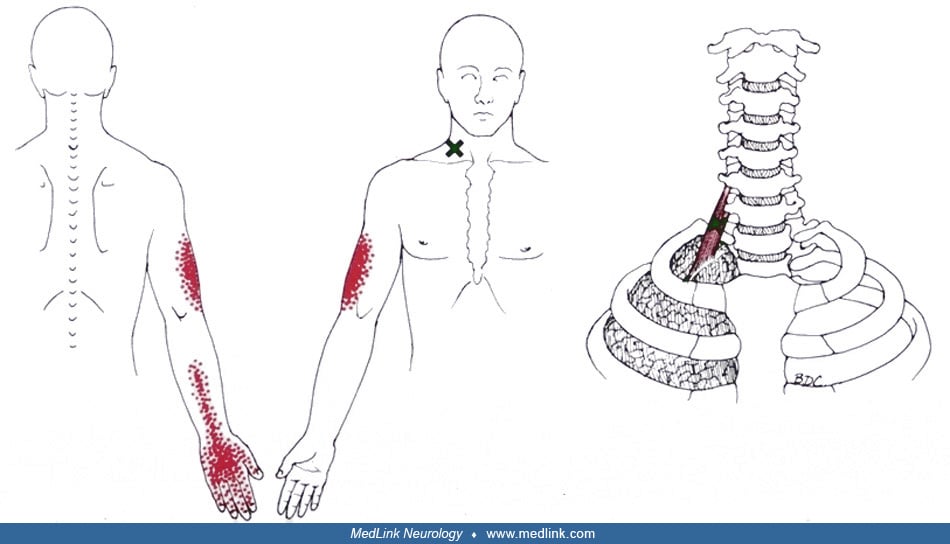
Trigger point: scalenes
|
• Signs and symptoms: Thoracic outlet symptoms of ulnar pain and numbness, hand weakness, and swelling combine with myofascial pain and shoulder and radial aspect of arm and hand. | |
|
• Referred pain patterns: Pectoral and medial scapular pain, extending down the lateral arm and radial aspect of forearm, thumb, and index finger. | |
|
• Activation and perpetuation: Pulling, lifting, or tugging. Referred pain from the cervical spine frequently activates and perpetuates scalene trigger points. | |
|
• Entrapment syndromes: Lower trunk of brachial plexus compression elicits ulnar pain, paresthesias, and the unexpected dropping of objects. Edema of fingers due to the subclavian vein. |
Shoulder and arm
Trigger point: infraspinatus
|
• Signs and symptoms: “Shoulder joint pain” causing difficulty sleeping on either side. Inability to reach behind. | |
|
• Referred pain patterns: Deep anterior deltoid pain, extending to the anterolateral arm. At times, radial aspect of hand. | |
|
• Activation and perpetuation: Usually results from overload reaching backward and up. | |
|
• Entrapment syndromes: None. |
Trigger point: supinator
|
• Signs and symptoms: "Tennis elbow," or lateral epicondyle pain with activity or rest. At times, hand weakness. | |
|
• Referred pain patterns: Lateral epicondyle, and often the dorsal aspect of the web and base of thumb. | |
|
• Activation and perpetuation: Excessively forceful, repetitive, or sustained supination of the hand. | |
|
• Entrapment syndromes: Deep radial nerve may cause weakness with extension of the hand, fingers, and thumb. |
Back and hip
Trigger point: quadratus lumborum
|
• Signs and symptoms: Deep aching "low back pain" at rest and severe aching in unsupported standing or sitting. | |
|
• Referred pain patterns: Deep trigger points refer to sacroiliac joint and lower buttock. Superficial trigger points refer to hip, iliac crest, and groin. | |
|
• Activation and perpetuation: Acute trauma as with awkward lifting or repetitive trauma as when walking with a limp. | |
|
• Entrapment syndromes: None. |
Trigger point: piriformis
|
• Signs and symptoms: "Pseudosciatica." Trigger points entrap the nerve (neurogenic symptoms) and gluteal vessels and contribute to sacroiliac joint dysfunction and referred hip pain. | |
|
• Referred pain patterns: Sacroiliac region, buttock, and posterior thigh. Trigger point pain is increased with walking, sitting, or standing. | |
|
• Activation and perpetuation: Acute overload from forceful rotations on one leg or a fall. Prolonged positioning during obstetric or urologic procedures with knees spread apart. | |
|
• Entrapment syndromes: Trigger points entrap multiple nerves and vessels at the sciatic foramen. Sciatic and gluteal neurovascular compression evoke numbness and pain with the pudendal nerve causing sexual dysfunction. |
Trigger points: puborectalis/pubococcygeus/rectus abdominis. Anderson and colleagues evaluated painful myofascial trigger points and pain sites in men with chronic prostatitis/chronic pelvic pain syndrome (03). The most prevalent pain sites were the penis, in 90.3% of men, the perineum in 77.8%, and the rectum in 70.8%. Puborectalis/pubococcygeus and rectus abdominis trigger points reproduced penile pain more than 75% of the time (p < 0.01). External oblique muscle palpation elicited suprapubic, testicular, and groin pain in at least 80% of the patients at the respective pain sites (p < 0.01) (03).
Although no long-term studies have been done to determine the natural history of this condition, most patients with an acute or subacute onset of symptoms who respond to treatment within a few weeks to a few months have a good prognosis. Chronic pain patients with symptoms persisting after several months usually have limited benefit from treatment, and pain may persist for several years.
|
• Myofascial trigger points are linked to myofascial pain syndrome, but the pathomechanism is not quite clear, and several hypotheses have been proposed. | |
|
• One concept is that myofascial trigger points are initiated by overload injury of the myotendinous unit, muscle spindle discharges, spinal segment sensitization, etc. | |
|
• It is difficult to differentiate between active and latent myofascial trigger points, but biochemical differences have been demonstrated between the two types of points. | |
|
• CNS plays a primary role in patients with chronic myofascial pain in whom nociceptive processes are demonstrated to be qualitatively altered. | |
|
• Sympathetic hyperinnervation in myofascial trigger points can partially explain the symptoms and help in the diagnosis and treatment of myofascial pain syndrome. |
A popular concept of the pathogenesis of myofascial pain syndrome is that an extra leakage of acetylcholine at the neuromuscular junction induces persistent contracture knots with the background of some “integrated hypotheses,” which state that myofascial trigger points are initiated by overload injury of the myotendinous unit, muscle spindle discharges, spinal segment sensitization, etc. (75). Repetitive and prolonged activity without periods of recovery can cause overloading of the muscle fibers, resulting in muscle hypoxia and ischemia. Dysfunction of intracellular calcium pumps due to energy depletion of muscles leads to increase of intracellular calcium, which induces sustained muscle contraction resulting in the development of taut bands (52). Moreover, inflammatory mediators caused by muscle injury contribute to pain and tenderness of the affected muscles.
Vascular abnormalities. Small arteries (or enlarged arterioles) near active myofascial trigger points showed retrograde flow in diastole, indicating a highly resistive vascular bed. Active myofascial trigger point sites were more likely to have a higher blood flow score compared with latent myofascial trigger points.
Activating mechanisms. Myofascial pain syndromes occur in muscles that have been overused as well as underused. The mechanism underlying their activation in these varied situations is not one of use, but rather one of exceeding a "critical load." Other factors, such as faulty positioning, malalignment of forces, and underlying joint dysfunction, provide important external influences. In these situations, it is presumed that muscle dysfunction occurs in response to an abnormal load imposed on the muscle at any point in time, resulting in premature muscle fatigue and then muscle failure once the critical load has been exceeded. Myofascial trigger points would then develop at a point where the muscle was no longer capable of handling the load, perhaps due to local injury or disruption of the myofibrillar structure.
Perpetuating mechanisms. Several perpetuating factors have been suggested to explain both the chronicity of myofascial pain and the apparent failure of appropriate treatment in many patients. Myofascial perpetuating factors are those mechanical, systemic, and psychological conditions that facilitate either injury of the affected muscle group or provocation of the neuromuscular feedback group theorized to result in chronic myofascial trigger point manifestations.
Of the many mechanical factors that serve to perpetuate myofascial pain, deconditioning caused by lack of exercise, inadequate muscle use, or impaired posture often develops due to an acute myofascial pain condition. Faulty posture is becoming an increasingly common perpetuating mechanical factor with the proliferation of computerized workstations.
Systemic perpetuating factors, including nutritional deficiencies, electrolyte disorders, metabolic or endocrine dysfunction, sleep disturbances, or other concurrent illnesses, have all been intuitively known to cause musculoskeletal stress, although no experimental evidence exists to support their role as a perpetuating factor for myofascial pain (18) (see Table 3).
|
Mechanical |
Systemic |
|
Postural stresses Structural stresses Deconditioning Articular dysfunction Periarticular dysfunction Neurogenic External compression |
Sleep disturbances Nutritional deficiencies Metabolic dysfunction Fatigue Endocrinopathies Temperature Other concurrent disease Medication dependencies Immune-mediated disease Electrolyte disturbances |
Pathogenesis. Although the pathophysiologic mechanisms that produce the symptoms of myofascial pain syndrome remain largely speculative, the complex nociceptive processes and pathways that subserve our perception of myofascial pain do not. In the past, indirect evidence has arisen from the investigation of nociceptive and neuropathic pain mechanisms and has provided indirect evidence, enabling inferences to be made regarding parallel processes that take place in the myofascial model of pain. Human and animal studies suggest that the pathogenesis of the three defining features of the myofascial pain syndrome is related to central nociceptive processing within the spinal cord. These neurophysiologic events, which are elicited by myofascial trigger point stimulation, include referred pain, reflex changes in motor activity (local twitch response), and reflex autonomic phenomena in or around the pain reference zone (53). Further evidence for a primary role of the CNS was confirmed when nociceptive processes were demonstrated to be qualitatively altered in patients with chronic myofascial pain. This study, which compared 40 patients with chronic myofascial pain to 40 normal volunteers, concluded that their nociceptive pain may be mediated by low-threshold mechanosensitive afferents projecting to sensitized dorsal horn neurons (07). The hypothesis that central sensitization plays a role in the pathogenesis of myofascial pain is supported by the finding of delayed and shortened cutaneous silence periods in limbs of volunteers and patients with myofascial pain, which indicates dysfunction in the inhibitory mechanism of the spinal/supraspinal pain pathways (30).
As evidence continues to suggest that the CNS plays a role in these processes, no human biopsy study has ever unambiguously identified the myofascial trigger points that presumably underlie the clinical expression of myofascial pain syndrome. The peripheral mechanism and initiating event of the myofascial trigger point, its associated sensory hyperactivity (variable tenderness), and the taut band are, as well, largely unknown. The concept that the myofascial trigger point represents a transient state of neuromuscular dysfunction is a recent introduction. Support for this evolving concept comes from several clinical observations, including: (1) the restoration of affected muscle tissue to normal with a variety of therapeutic techniques; (2) the identification of latent myofascial trigger points in clinically asymptomatic individuals; and (3) the inconsistent histopathological results obtained in biopsies to date. Simons has expanded on this concept and proposed that any hypothesis that attempts to define these peripheral initiating events and mechanisms of myofascial pain will also need to account for four clinical features: (1) the sustained tension maintained within taut bands, which occurs in the absence of quantifiable EMG motor unit activity; (2) the manner in which multiple and highly variable factors including local muscle overload could precipitate a physiologic event initiating the myofascial trigger point; (3) the presence of substances that sensitize nociceptors in the region of the trigger point and cause their overactivity; and (4) the fact that any technique (ie, TP injections, dry needling, massage) that restores the muscle to its full normal stretch length is therapeutic (54).
Single-voxel proton magnetic resonance spectroscopy ((1)H-MRS) has been used before and after pressure-pain testing to assess glutamate (Glu), glutamine (Gln), N-acetylaspartate (NAA), and choline (Cho) levels in the right and left posterior insulae of individuals with myofascial temporomandibular disorders (20). Glu levels were significantly lower in all individuals after pain testing. Among those with temporomandibular disorders, left-insular Gln levels were related to reported pain, left posterior insular NAA and Cho levels were significantly higher at baseline than in control individuals, and NAA levels were significantly correlated with pain-symptom duration, suggesting adaptive changes. The results suggest that significant central cellular and molecular changes can occur in individuals with temporomandibular disorders.
Progress in nociception research has led to the identification of numerous nociceptive processes that may contribute to the biological basis of myofascial pain. Acute or chronic tissue trauma can result in a cascade of events, including hyperalgesia from nociceptor sensitization and associated somatic (skeletal muscle spasm) and autonomic reflexes (ie, tachycardia, vasoconstriction, pupillary dilation, and sweating). Many nociceptive primary afferent fibers possess dual capabilities, including orthodromic response signaling to the CNS and antidromic release of algogenic substances peripherally (neurogenic inflammation). Prolonged nociceptor activity can be followed by neuronal plasticity at every level of sensorimotor processing and can result in changes that may then become the substrate for chronic pain and autonomic dysfunction. The distribution of nociceptors within skeletal muscle is confined to the fascia between muscle fibers, with the highest concentration of nociceptors near the muscle endplate region, where myofascial trigger points are usually found. It has been proposed that multiple sensitive loci exist in a trigger point region and that each locus contains one or more sensitized nociceptive nerve endings. The colocalization of these sensitive loci to established trigger point regions near the muscle endplate supports the concept that multiple and highly variable causes of local muscle injury are mediated through a common pathogenic pathway, resulting in the development of a predefined trigger point.
Biochemical differences have been described between active and latent myofascial trigger points, as well as in comparison with healthy muscle tissue (51).
Glutamate injection induced higher peak pain intensity than isotonic saline injection into either latent myofascial trigger points or nonmyofascial trigger points. Muscle camps were observed in 92.86% of the subjects following glutamate injection into the latent myofascial trigger points, but not the nonmyofascial trigger points. No muscle cramps were recorded following isotonic saline injection into either the latent myofascial trigger points or the nonmyofascial trigger points. These results suggest that latent myofascial trigger points could be involved in the genesis of muscle cramps. Focal increase in nociceptive sensitivity at myofascial trigger points may constitute one of the mechanisms underlying muscle cramps.
A randomly injected bolus of either hypertonic saline (6%, 0.1 mL each), glutamate (0.1 mL, 0.5 M each), or isotonic saline (0.9%, 0.1 mL each) into a latent myofascial trigger point and a nonmyofascial trigger point located in the right or left gastrocnemius medialis muscles induced a higher visual analog scale (peak) and larger visual analog scale (area under the curve) than nonmyofascial trigger points (35). Moreover, the myofascial trigger points with referred pain after painful injections were found to show higher visual analog scale (peak) and larger visual analog scale (area under the curve) than those without referred pain, confirming the existence of hypersensitivity at latent myofascial trigger points and providing evidence that there is hypersensitivity at latent myofascial trigger points, and the referred muscle pain is associated with higher pain sensitivity at latent myofascial trigger points.
When compared to nonmyofascial trigger points, maximal visual analog scale and the area under the visual analog scale curve are significantly higher and larger during sustained nociceptive mechanical stimulation (SNMS) of latent myofascial trigger points; there is a significant decrease in pedunculopontine tegmental nucleus 10 minutes, 20 minutes, and 30 minutes post-SNMS of latent myofascial trigger points (72). Muscle cramps following SNMS of latent myofascial trigger points are positively associated with the visual analog scale (area under the curve) and the referred pain area. Painful stimulation of latent myofascial trigger points can initiate widespread central sensitization. Muscle cramps contribute to the induction of local and referred pain.
Autonomic disturbances in myofascial pain. Various perpetuating factors for myofascial pain may generate spontaneous sympathetically maintained intrafusal muscle fiber contraction, causing an involuntary low-grade but symptomatic muscle tension. Sympathetic hyperinnervation in myofascial trigger points can partially explain the symptoms and provide perspective regarding the diagnosis and treatment of myofascial pain syndrome (12). This sympathetic activity would also explain the autonomic symptoms associated with trigger points and provide a mechanism by which local injury and nociception cause local tension and by which emotional factors cause widespread pain and tension. The activity of nociceptive afferent fibers from the trigger point to the spinal cord could then induce a feedback loop that maintains trigger point activity, possibly by nociceptor sensitization or local autonomic dysregulation and vasoconstriction.
Vasovagal responses during dry needling are associated with parasympathetic predominance, reflected by reduced heart rate, increased heart rate variability, pupil dilation, and higher pain threshold (67). These findings indicate significant individual variability in autonomic responses. Monitoring susceptible patients during the procedure is important.
Glutamate injection into myofascial trigger points has been shown to decrease skin temperature and blood flow in the peripheral area; the magnitudes of the reduction are comparable to those induced by the breath-hold maneuver, which has been used to induce sympathetic vasoconstrictor response (32). Kimura and colleagues concluded that the combination of glutamate injection into latent myofascial trigger points, together with the breath-hold maneuver, does not result in further decrease in skin temperature and blood flow, indicating that sympathetic vasoconstrictor activity is fully activated by nociceptive stimulation of myofascial trigger points.
An attenuated skin blood flow response has been demonstrated after painful stimulation of latent myofascial trigger points compared with nonmyofascial trigger points, suggesting increased sympathetic vasoconstriction activity at latent myofascial trigger points (74). Moreover, laser Doppler flowmetry has been shown to be more sensitive than thermography in the detection of changes in skin blood flow after intramuscular nociceptive stimulation.
|
• Myofascial pain syndrome affects 10% of patients in internal medicine practice and 55% to 85% of those attending pain clinics. |
Myofascial pain syndrome is the most common type of pain that brings patients to chronic pain treatment centers. Among 283 consecutive admissions to a comprehensive pain clinic, 85% were assigned a primary organic diagnosis of myofascial syndrome (56). Among 296 patients referred to a dental clinic for chronic head and neck pain of at least 6 months' duration, the primary diagnosis was myofascial pain in 55.4% of cases (19). Acute myofascial pain is also common in general medical practice. Among 61 consecutive consultation or follow-up patients in an internal medicine group practice, 10% of all patients and 31% of those presenting with a pain complaint had myofascial trigger points identified as being primarily responsible for their symptoms (54).
Few controlled studies have been published on the prevalence of this condition. There appears to be a female predominance, with estimates varying between 1.5:1 and 3:1. Numerous anecdotal reports suggest that myofascial pain is commonly a result of musculoskeletal injury, particularly in industry, where it is a frequent cause of disability after trauma, and in motor vehicle accidents, where it is seen as a major component of the whiplash syndrome (15).
Torres and colleagues conducted a 1-year prospective follow-up after breast cancer surgery, which included 116 women. Fifty-two women out of 116 total subjects developed myofascial pain syndrome after breast cancer surgery (44.8%, 95% CI: 35.6 to 54.3) (61).
Insomnia is a risk factor for myofascial pain syndrome. In a population-based longitudinal study with 10-year follow-up, the insomnia patients were 1.93 times more likely to develop myofascial pain syndrome than the control patients after adjusting for age, sex, monthly income, urbanization, and comorbidities (36). Malignant neoplasms and living in urban areas were identified as independent risk factors for myofascial pain syndrome in patients with insomnia.
|
• Postural training is an important initial step in the prevention of myofascial pain. |
Postural training has been advocated as an important initial step in the prevention of myofascial pain, with an emphasis on ideal standing, sitting, and postural alignment. Ergonomic assessment of the workstation and modification of repetitive task-specific movements at the workplace are also recommended. Postural screening of at-risk individuals may identify faulty standing posture, such as seen in the common round-shouldered, head-forward posture, which can activate trigger points in many regions of the body.
Hypothyroidism and vitamin D deficiency are risk factors for myofascial pain and should be corrected.
Muscular pain and dysfunction can arise from several sources and have been categorized into direct (articular, periarticular, and myopathic) and indirect (somatic or visceral referred pain, neuropathic, and psychogenic) causes. Distinguishing myofascial pain from these various conditions, however, has been confusing, in part due to the heterogeneity of the myofascial pain syndromes. Attempts to classify myofascial syndromes based on the number of muscles and joints involved resulted in three distinct categories. These categories range on a continuum from focal (single muscle or two muscles and one joint), to regional (two or more muscles and two or more joints in a single region), to generalized. Diagnostic algorithms pair the focal, regional, or generalized myofascial syndrome with conditions causing direct or indirect muscular pain that resemble their focal or generalized presentation.
Those conditions, which must be differentiated from one or more myofascial syndrome categories, may, as well, coexist with a myofascial disorder and provide an activating or perpetuating function for the secondary development of myofascial symptoms. Several of the more common conditions in the differential diagnosis of myofascial pain have been selected for brief review because of their potential for these additional interrelationships.
Post-exercise delayed soreness. This is also referred to as delayed onset muscle soreness, which occurs 12 to 24 hours after unaccustomed strenuous exercise, lasting several days. Delayed onset muscle soreness manifests as muscle strain or tear, cramps, or chronic leg pain and shares several similarities and differences with myofascial pain syndrome. Vigorous exercise and myofascial trigger points both produce painful, sustained muscle shortening in the absence of quantifiable EMG activity, thus excluding true muscle spasm as a cause in either condition. Additionally, both conditions display a training effect, which protects against post-exercise soreness and trigger point activation. Differences between the two conditions include:
|
• Most individuals with myofascial pain cannot identify a precipitating event, and after its onset, resolution is often protracted, and symptoms may persist for months or years. | |
|
• Although taut bands and discrete tender spots are described in delayed onset muscle soreness, none of these have characteristics that represent the classic myofascial trigger point phenomenon observed in myofascial pain (68). | |
|
• Elevated serum creatine phosphokinase is absent in myofascial pain as compared to delayed onset muscle soreness. Other systemic circulation biomarkers, including inflammatory cytokines and growth factors, are elevated in both conditions, and further studies are required to sort out this overlap. |
Articular and periarticular dysfunction. Articular dysfunction may occur with either joint hypo- or hypermobility. The term "somatic dysfunction" is now commonly used to describe secondary muscular pain precipitated by abnormal joint movement. The secondary muscle dysfunction that may occur can subsequently develop myofascial trigger point phenomena. Alternatively, myofascial dysfunction may create stress on the joints that predispose them to articular dysfunction. Because myofascial trigger points refer pain and tenderness to regions where tendons and bursae are located, tendinitis and bursitis are frequently misdiagnosed.
Referred pain. Regional pain syndromes are frequently based on referred pain. Though visceral sources of referred pain are commonly recognized, somatic sources from deep axial skeletal structures, such as the spine or periosteum, have been described as a cause of regional referred pain, often in an analogous pattern to muscle.
Neuropathic pain. Although neurologic disease can easily be differentiated from myofascial dysfunction, confusion may arise with spasticity that complicates CNS injury. Spasticity may be a primary source of muscular pain or secondarily lead to myofascial dysfunction, as seen in some cases of "frozen shoulder."
Fibromyalgia. Over the last 100 years, the literature has distinguished two primary types of muscular pain: myofascial pain syndrome and fibromyalgia. Unfortunately, however, considerable confusion continues to exist between these two enigmatic conditions, which clinically appear to be on opposite ends of the spectrum. Although myofascial pain is typically a localized disorder without systemic manifestations, in practice, it often has a more complex presentation. When, on occasion, it is reported as generalized, it may appear to be confusing, like fibromyalgia, a chronic systemic condition that affects general pain sensitivity and muscle function. In 1990, the American College of Rheumatology set criteria for the classification of fibromyalgia that include at least 3 months of widespread pain and the presence of at least 11 of 18 specific tender points on examination (71). Diagnostic criteria published in 2010 and modified in 2011 move away from tender points and are more symptom-based, describing fibromyalgia as a widespread pain syndrome that is not dependent on specific trigger points for diagnosis (70). The Analgesic, Anesthetic, and Addiction Clinical Trial Translations Innovations Opportunities and Networks (ACTTION), in partnership with the FDA and the American Pain Society, developed a diagnostic system for fibromyalgia with the following core criteria for usefulness in practice (04):
(1) Multisite pain defined as six or more pain sites from a total of nine possible sites
(2) Moderate to severe sleep problems or fatigue
(3) Multisite pain plus fatigue or sleep problems must have been present for at least 3 months
Myopathic pain. Though myopathies are generally painless, they are a common cause of generalized muscle dysfunction. Infectious myositis can be painful, as can pain from the systemic vasculitides, metabolic dysfunction, or electrolyte disturbance.
Psychogenic pain. Pain syndromes are rarely the result of hysteria. Although occasional patients present with pain that is primarily psychogenic due to conversion reactions or is largely fabricated for volitional secondary gain, they generally fail to express emotional distress commensurate with their pain and behave as if threatened by increased function. It is not uncommon, however, for diffuse chronic pain syndromes to be labeled as nonorganic pain or psychogenic pain. These designations lack scientific validity, as they are frequently used when a physical cause cannot be identified for a patient's pain.
Chu and Sabourdy reported a case in which severe right upper neck pain, initially diagnosed as myofascial pain syndrome, didn't improve with treatments (14). A thorough chiropractic examination revealed a mass, and further investigation identified a desmoid tumor, emphasizing the need for comprehensive assessment in treatment-resistant cases.
|
• Careful history and identification of pain distribution and areas of referred pain are important for clinical diagnosis of myofascial pain syndrome, as there are few devices for objective diagnosis. | |
|
• A palpable band of muscle fibers is critical for the identification of the trigger point. | |
|
• A “muscle pain detection device” is used to stimulate selected muscles to distinguish between primary and referred muscle pain. | |
|
• Electromyography to detect endplate noise at trigger points. | |
|
• Ultrasound can help to localize myofascial trigger points as hypoechoic regions. | |
|
• A pressure algometer is highly reliable for measuring pressure pain threshold for evaluating the effect of treatment but not as a diagnostic measure. |
Because few objective laboratory studies are available to document the existence of this disorder, the diagnosis mostly relies on the clinical history and the performance of a careful physical examination. A systematic review found nine studies eligible for inclusion in the literature on the reliability of physical examination for the diagnosis of trigger points and concluded that no study to date had reported the reliability of trigger point diagnosis according to the proposed criteria (37). Based on the limited number of studies available and significant problems with their design, reporting, statistical integrity, and clinical applicability, physical examination was not recommended as a reliable test for the diagnosis of trigger points. The reliability of trigger point diagnosis needs to be further investigated with studies of high quality that use current diagnostic criteria in clinically relevant patients (37).
The diagnosis of myofascial pain syndrome, as defined by Simons and Travell, relies on eight clinical characteristics (55). The identification of the pain distribution is one of the most critical elements in identifying and treating myofascial pain. The physician should ask the patient to identify with a single finger the most intense area of pain. Also, an associated, consistent, and characteristic referred pain pattern is experienced on palpation of this trigger point. This referred pain is often not located in the immediate vicinity of the trigger point but is commonly found in predictable patterns, as described by Travell and Simons (Travell and Simons 1983; 54). Pain can be projected in a peripheral referral pattern, a central referral pattern, or a local pain pattern. When a hyperintense area of pain is identified, its area of referred pain should then be identified (58).
The palpable band is critical in the identification of the trigger point. Three methods have been identified for trigger point palpation: flat palpation, pincer palpation, and deep palpation. Flat palpation refers to using a fingertip to slide across the muscle fibers of the affected muscle group. The skin is pushed to one side, and the finger is drawn across the muscle fibers. This process is repeated with the skin pushed to the other side. A taut band may be felt passing under the investigator’s finger. In this method, snapping palpation, like plucking a violin, is employed to identify the specific trigger point. Pincer palpation is a method that employs firmly grasping the belly of the muscle between the thumb and the rest of the fingers. The fibers are pressed between the fingers in a rolling manner to locate a taut band. Deep palpation may be used to locate the trigger point that is obscured by superficial tissue. The fingertip is placed over the muscle attachment of the area suspected of harboring the trigger point. When the patient’s symptoms are reproduced by pressing in one specific direction, it may be presumed that a trigger point has been located.
Muscle pain assessment. To elicit contractions and mimic an active muscle or movement that may lead to pain, a Muscle Pain Detection Device (MPDD) may be utilized. A selected muscle may be stimulated, and painful muscles are precisely detected, allowing distinctions between primary and referred muscle pain as well as distinguishing other functional muscle pain thought to cause myofascial pain syndrome (24).
The MPDD group reported significantly larger improvements in pain, mood, and Oswestry scores compared with the control (P < 0.05). Moreover, the MPDD group reported 82.5% pain relief at 1 month, compared with 53.2% in the control (P < 0.001) (24).
Electromyography (EMG). Needle EMG of trigger points shows high-voltage spike activity and spontaneous, low-voltage endplate noise. Moreover, it rules out neuromuscular disorders.
Localization of myofascial trigger points with ultrasound. Because the palpation technique is not reliable, the use of imaging has been explored as an objective method for the localization of myofascial trigger points. Ultrasound may offer a convenient, accessible, and low-risk approach for identifying myofascial trigger points as hypoechoic spots and for evaluating clinical observations of palpable, painful nodules. Vibration sonoelastography can be useful for differentiating myofascial trigger points from surrounding tissue because it can quantify the relative stiffness of myofascial trigger points. A review of ultrasound imaging techniques that have shown promise in visual localization of myofascial trigger points has identified three approaches: conventional gray-scale imaging, Doppler imaging, and elastographic ultrasound imaging (33).
Pressure algometer. The usefulness of a pressure algometer was shown to be a highly reliable measure of pressure pain threshold for the diagnosis of myofascial pain syndrome in the upper extremity and trunk muscles (43). Pressure pain threshold might be a useful parameter for assessing a treatment’s effect, but it is not useful for diagnosis or even as a screening method.
|
• The use of medications for acute myofascial pain is controversial but nonsteroidal antiinflammatory drugs and muscle relaxants are sometimes useful. Topical anesthesia and diclofenac sodium patch are more effective. | |
|
• Noninvasive techniques include physiotherapy, massage, yoga, counterpoint stimulation, and spray and stretch. | |
|
• Pressure is applied on the trigger point to lengthen the taut muscle. | |
|
• Kinesio taping improves local blood and lymph circulation, reduces edema and pressure pain, and strengthens weakened muscles in myofascial pain syndrome. | |
|
• Manual acupuncture has a favorable effect on pain intensity after stimulation of myofascial trigger points. In a variant of electroacupuncture, special acupuncture needles are used for intramuscular electrical stimulation to relieve chronic pain. | |
|
• Transcutaneous electrical stimulation and pulsed electric neuromuscular stimulus are useful for reducing pain and disability. | |
|
• Ultrasound-guided interfascial pulsed radiofrequency had a better long-term effect on reducing pain than ultrasound-guided interfascial block with lidocaine. | |
|
• Trigger point injections of local anesthetic or botulinum toxin do not have proven benefit, but a combination of the two can be effective. | |
|
• Dry needling or intramuscular stimulation at trigger points provides relief of pain. | |
|
• Miniscalpel-needle release of tense muscle under the trigger point provides some relief of pain. |
Treatment of acute myofascial pain with prompt, efficacious therapy, avoidance of muscle immobilization, and elimination of perpetuating factors is often effective. Although, in theory, myofascial pain is of acute onset, is localized, and is nonchronic, in practice it often has a more complex presentation that, when chronic, appears to respond to multiple therapies with only limited and anecdotal benefit. There appear, however, to be several empiric treatment strategies that could be of potential benefit. A multidisciplinary approach using myofascial trigger point inactivation, active and passive muscle stretching, maintenance exercise, control of predisposing as well as perpetuating factors, and the management of psychological contributing issues is valuable for the treatment of myofascial pain.
Approach to perpetuating factors. Should a patient's myofascial pain prove to be refractory or recurrent following 4 to 8 weeks of appropriate therapy, exploration of possible concomitant or perpetuating conditions is warranted. Management of myofascial pain syndrome then necessarily requires recognition of mechanical (structural or postural), systemic, and psychogenic factors that may have a perpetuating role in the dysfunction seen. Postural contributing factors, whether behavioral or biological, perpetuate trigger points if not corrected (65). Similarly, mechanical abnormalities like spinal scoliosis or leg length discrepancy should be corrected with orthotics and other devices whenever possible. Repetitive task-specific movements in the workplace or at the workstation should be simplified to allow for stretching and the use of alternative muscle groups. Recognition of learned illness behaviors that distract from an adaptive coping style is best remedied with a cognitive behavioral approach.
The results of an assessment of a cohort of myofascial temporomandibular disorder participants using a statistical bootstrapping technique suggest that pain catastrophizing is associated with greater sleep disturbance and that a significant portion of variance in clinical pain severity and pain-related interference attributable to pain catastrophizing is mediated by sleep disturbance (10). Thus, it is conceivable that interventions that reduce pain catastrophizing may concurrently improve sleep and clinical pain.
Medications. The use of medications in the treatment of myofascial pain syndromes remains controversial. The reported benefit of nonsteroidal anti-inflammatory drugs in myofascial pain, though anecdotal, suggests that they may be a valuable adjunct, used not only to treat the underlying dysfunction but also to reduce post-exercise soreness as the patient increases the overall exercise regimen. As restoration of sleep is essential, the use of short-term pharmacotherapy may be appropriate. The empirical use of analgesics for myofascial pain has not been evaluated by controlled studies. Use of muscle relaxants, particularly those that offer dual benefit for both sustained muscle tension and spasticity from CNS disease (baclofen, tizanidine), may be appropriate according to indication.
The Cochrane Review identified two studies with a total of 79 participants (34). One study, with 41 participants, compared cyclobenzaprine with clonazepam and with a placebo. Participants taking cyclobenzaprine had some improvement of pain intensity compared to those on clonazepam, mean difference -0.25 (95% CI: -0.41 to -0.09; P-value 0.002), and placebo, mean difference -0.25 (95% CI: 0.41 to -0.09; P-value 0.002). The other study, with 38 participants, compared cyclobenzaprine with lidocaine infiltration. Thirty days after treatment, there were statistically nonsignificant differences between comparison groups, favoring lidocaine infiltration for the mean for global pain, mean difference 0.90 (95% CI: -0.35 to 2.15; P-value 0.16), and for the mean for pain at digital compression, mean difference 0.60 (95% CI: -0.55 to 1.75; P-value 0.30). There were no life-threatening adverse events associated with the medications. The authors concluded that there was insufficient evidence to support the use of cyclobenzaprine in the treatment of myofascial pain.
Noninvasive techniques. Noninvasive techniques have the advantage of decreased relative risk as compared to invasive techniques. Some elements of these conservative therapies involve teaching the patient about posture and exercise, which will prevent further myofascial complications from developing.
Counterpoint stimulation. Once a symptomatic trigger point has been identified, its inactivation is accomplished through a variety of counterstimulation techniques coupled with active and passive stretching, which may include postural rehabilitation (62). The goal is to restore the muscle to its normal length, posture, and full range of motion. Maintenance of an exercise program with concomitant control of activating or perpetuating factors prevents the recurrence of trigger points while restoring optimal function to the injured muscle and minimizing the risk of reinjury.
Spray (freeze) and stretch. Spray and stretch therapy involves the passive stretching of an affected muscle while simultaneously administering a vasocoolant spray to the overlying skin. The spray is directed over the reference zone of pain identified during trigger point palpation. Repeated application of the vasocoolant stream is followed by the progressive-passive stretch of the muscle until pain and point tenderness over the trigger point are eradicated. Travell and Simons advocate passive stretching of the affected muscle after application of sprayed vapocoolant to be the “single most effective treatment” for trigger point pain (65).
The proper technique depends on patient education, cooperation, compliance, and preparation. The patient should be positioned comfortably, ensuring that the trigger point area is well supported and under minimal tension. The position should place one end of the muscle with the trigger point zone securely anchored. The patient should be marked after careful diagnosis of the trigger point region, and the reference zone should be noted. The skin overlying the trigger point should be anesthetized by use of a vapocoolant spray (ethyl chloride or dichlorofluromethane-trichloromonofluromethane [Fluori-Methane]) over the entire length of the muscle (55). This spray should be applied from the trigger point toward the direction of the reference zone until the entire length of the muscle has been covered. The vapocoolant should be directed at a 30-degree angle to the skin.
Immediately after the first vapocoolant spray pass, passive pressure should be applied to the other end of the muscle, resulting in a stretch. Multiple slow passes of spray over the entire width of the muscle should also be performed while maintaining the passive muscle stretch. This procedure is repeated until the full range of motion of the muscle group is attained, totaling a maximum of three repetitions before rewarming the area with moist heat. Care must be taken to avoid prolonged exposure to the vapocoolant spray, assuring that each pass is less than 6 seconds per spray. Patients must be warned not to overstretch muscles after a stretch and spray therapy session.
The mechanism of the stretch and spray technique is proposed to involve the inhibition of the reflex spasm that prevents passive stretching of the muscle. The vapocoolant spray sends a cold perception to the dorsal column of the spinal cord, which inhibits the nociceptor input from the trigger point, causing muscular tension. This spray inhibits muscle spasm and allows for passive stretch of the muscle. Through this mechanism, the spinal cord feedback loop is interrupted, and the trigger point is relieved (55).
Acupuncture. Sun and colleagues compared a group of patients with chronic neck myofascial pain syndrome receiving acupuncture to a group of patients receiving sham acupuncture (60). Acupuncture had greater improvement in physical functioning and emotional role of Short Form-36 quality of life at 12 weeks after treatment than sham acupuncture (60). Results of a meta-analysis of randomized trials using sham treatment as control suggest a favorable effect of manual acupuncture on pain intensity after stimulation of myofascial trigger points in patients with myofascial pain syndrome (69).
Physical therapy. Some of the best measures to quell cyclic myofascial pain are to identify perpetuating factors. Therapists see their patients in multiple sessions and are often able to correct elements of poor posture and body mechanics.
In a randomized study of pelvic floor myofascial physical therapy compared to global therapeutic massage in women with newly symptomatic interstitial cystitis or painful bladder syndrome, the response rate was 26% in the global therapeutic massage group and 59% in the myofascial physical therapy group (17).
A single-blind, randomized, controlled clinical trial was conducted to determine whether lidocaine injections into myofascial trigger points combined with a physical therapy program would be more effective than each separate treatment alone in improving pain, function, and quality of life in a group of patients with myofascial pain syndrome of the shoulder girdle and cervical region (38). There were no differences between the groups except that the physical therapy and physical therapy + lidocaine injection groups had higher right upper limb hand-back maneuver scores compared to the lidocaine injections alone group at both 1 and 3 months.
Rahman and colleagues conducted a study of 60 patients with myofascial pain syndrome causing upper back pain, randomly assigning them to two groups (46). One group received thermotherapy, anti-inflammatory drugs, and activity of daily living instructions, whereas another group had the same plus rehabilitation exercises. Results showed significant improvement in the second group, emphasizing the value of incorporating rehabilitation exercises in treating myofascial pain syndrome.
Transcutaneous electrical stimulation. Transcutaneous electrical stimulation is used as a common adjuvant therapy in chronic and acute pain management. Various studies have reported some beneficial effect of transcutaneous electrical stimulation in myofascial pain syndrome, but the placement of electrodes is arbitrary and may be over the myofascial trigger points or the zone of pain radiation. A randomized controlled trial has shown that the short-term therapeutic effects of transcutaneous electrical stimulation in myofascial pain of temporomandibular disorder are superior to those of placebo, as assessed by reported facial pain, deep pain sensitivity, and improvement of masticatory muscle EMG activity (16).
Intramuscular electrical stimulation. This is a variant of electroacupuncture in which special acupuncture needles are used for intramuscular electrical stimulation to relieve chronic pain. A double-blind, randomized, sham-controlled trial has tested the effect of cervical paraspinal intramuscular electrical stimulation as well as repetitive transcranial magnetic stimulation on pain and disability associated with chronic myofascial pain syndrome in the craniofacial region (ClinicalTrials.gov: NCT02381171). The results suggest a bottom-up effect induced by electrical stimulation by reduction of analgesic use as well as improved pain and disability, which might be mediated by an enhancement of corticospinal inhibition as seen by an increase in intracortical amplitude and a decrease in amplitude of motor evoked potential (09).
Pulsed electric neuromuscular stimulus. Microcurrent electric neuromuscular stimulation has been proposed in pain management for its effects on normalizing the bioelectricity of cells. Modulated low-intensity pulsed electric neuromuscular stimulus is an innovative therapy that acts on the transmission of pain through the stimulation of A-beta fibers and restores tissue homeostasis. Results of a prospective-analytic longitudinal study showed that low-intensity pulsed electric neuromuscular stimulus can be considered as an effective treatment to reduce pain and disability in patients with myofascial pain syndrome (25).
Pulsed radiofrequency. Pulsed radiofrequency works by delivering an electric field and heat bursts to targeted nerves or tissues without damaging these structures, and it has been reported to be safe and effective in alleviating many types of chronic pain. In a randomized study for the management of myofascial pain syndrome of the trapezius muscle, ultrasound-guided interfascial pulsed radiofrequency had a better long-term effect on reducing pain and quality of life compared to ultrasound-guided interfascial block with lidocaine (13).
Ultrasound. Ultrasound may be employed as an adjunctive means of treatment. Ultrasound transmits vibration energy at the molecular level; approximately 50% reaches a depth of 5 mm. The true mechanism of action is not well understood but is thought to be a combination of thermal and chemical means. The local effects may alter the release of acetylcholine or alter the effects of the energy crisis. A randomized study of myofascial pain syndrome involving the trapezius muscle has shown that ultrasound treatment is effective (27).
Extracorporeal shock wave therapy. A prospective randomized single-blinded pilot study of the comparative effect of high- and low-energy extracorporeal shock wave therapy (ESWT) for patients with myofascial pain syndrome of the upper trapezius showed that high-energy ESWT was more effective in improving neck disability index and neck flexion range of motion compared to low-energy ESWT (44). A systematic review of randomized clinical trials shows that ESWT benefits patients with myofascial pain syndrome of the trapezius by alleviating pain. ESWT may not replace conventional therapies but could serve as an adjunct therapeutic method (73).
Massage. Massage is described as a “deep stroking” or “stripping” massage when the patient is positioned comfortably to allow the muscle group being treated to be lengthened and relaxed as much as possible (55).
Yoga and meditation. An open comparative study on a small number of patients with myofascial pain syndrome has shown that yoga and meditation, in combination with conventional, noninvasive methods of treatment, show some beneficial effect in the relief of pain as well as in improvement of function as compared to either modality alone (29). Larger controlled trials are needed to confirm these findings.
Virtual reality. A retrospective study evaluated the effectiveness of virtual reality therapy in managing pain and anxiety in 91 patients with chronic musculoskeletal pain, predominantly fibromyalgia, during a 2-week interdisciplinary program. Virtual reality use resulted in moderate short-term reductions in pain and anxiety, with greater benefits seen in patients with high baseline anxiety, nociplastic pain, and traits such as alexithymia. At 1-month follow-up, about half of the participants reported sustained relief, indicating that virtual reality therapy may be a promising adjunctive tool in CMP management (45).
Kinesio taping. This technique, developed in Japan, involves the use of Kinesio Tape -- a thin, light, and elastic material that does not restrict joint movement, relieves pain and muscular spasm, and increases the range of motion. Kinesio taping also improves local blood and lymph circulation, reduces edema, and strengthens weakened muscles. Results of a randomized, double-blind, placebo-controlled study show that Kinesio taping in patients with myofascial pain syndrome leads to improvements in pressure pain threshold and cervical range of motion, but not disability in the short term, and it may be used as an alternative method in treatment (06).
A systematic review and meta-analysis of randomized clinical trials of kinesio taping for the management of myofascial pain syndrome has shown it to be superior to other noninvasive techniques in relieving pain intensity and improving range of motion (76).
Ischemic compression therapy. The term ischemic compression therapy refers to the belief that the application of pressure to a trigger point produces ischemia, which will ablate the trigger point. As one of the theoretic etiologies of trigger points is relative ischemia, it seems counterintuitive that further ischemia would improve symptomatology. Simons and colleagues argue that the emphasis should not be on ischemia of the trigger point area but on lengthening the muscle. In their method, pressure is applied to the point of increasing resistance. Pressure is then maintained until the physician feels a relief of tension. The patient may feel mild discomfort but should not experience profound pain. The process is repeated for each band of taught muscle encountered (55).
Topical medications. Local anesthetics have been used for topical application. In a placebo-controlled study, lidocaine patch and infiltration decreased pain significantly; effects at muscle trigger points and target areas were greater with infiltration (01). Discomfort from therapy was greater with infiltration than with the lidocaine patch. No adverse events occurred in any group.
In a double-blind, placebo-controlled, randomized study, the diclofenac sodium patch was superior to the control patch for reducing pain and improving functional outcomes in myofascial pain syndrome of the upper trapezius, and it did not result in significant adverse effects (23).
Trigger point injection. A trigger point injection involves the injection of medication directly into the trigger point, which is identified as a palpable tender area that produces a referred pain pattern. A study has compared the feasibility of ultrasound-guided myofascial trigger point injection with that of a blind injection technique following the use of shear wave elastography for the measurement of stiffness at the trigger point in patients with trapezius myofascial pain syndrome (26). Ultrasound-guided injection was shown to be more useful than a blind injection.
Local anesthetics. Local anesthetics have been most frequently investigated for the treatment of myofascial trigger points. As mentioned previously, pain relief following injection of the trigger point outlasts the duration of action of the local anesthetics. Local anesthetic injections have been shown to improve subjective outcome measures on pain scale, range of motion, and algometry pressure thresholds. Injection of local anesthetic can result in local myotoxicity, and it may be aggravated by the addition of epinephrine, resulting in muscle necrosis. The necrosis usually resolves within a few weeks, but repeated injections may retard muscle regeneration.
In The Trigger Point Manual, Simons and colleagues recommend the use of a 0.5% procaine solution in physiologic saline (55). Higher concentrations have shown no additional anesthetic effect. Procaine is selective for small, unmyelinated fibers that control pain perception and spares motor fibers. Lidocaine is a common substitute for procaine, but no study has compared both. Intramuscular injections of cocaine, bupivacaine, and mepivacaine were all noted to cause muscle necrosis. Their use in treating trigger points is not recommended.
Controlled studies of local trigger point injection therapy using either a local anesthetic or saline demonstrate no significant difference between solutions relative to the substantial benefit observed, suggesting that relief of pain may be due to reflex mechanisms rather than to the pharmacological effects of the injected solution or other direct needle mechanisms. Trigger point injections with local anesthetics are preferred as they are generally more comfortable than dry needling or injecting other solutions and may improve the duration of benefit as well. A systematic review of randomized controlled trials concluded that there is no clear evidence of either benefit or ineffectiveness of myofascial injection (50). The reviewers commented that the only advantage of injecting anesthetic into trigger points may be to reduce the pain of the needling process, which may be an insignificant benefit. In a systematic review of controlled clinical trials of local anesthetic injections for the short-term treatment of head and neck myofascial pain syndrome, a significant improvement in pain was reported as compared to dry needling, but sensitivity analysis of double-blind trials revealed no statistically significant differences in secondary outcomes between local anesthetic injections and all other interventions (42).
Botulinum toxin. Myofascial trigger point injection with botulinum toxin has been reported to be effective in some studies. Low-dose botulinum toxin injection into myofascial trigger points produces muscle relaxation by inhibition of the release of acetylcholine as well as by blockage of the neuromuscular junction in the gamma motor neurons, leading to a reduction in spindle afferent activity, which is disproportionate to the actual weakness that it causes. Botulinum toxin A also inhibits the release of inflammatory mediators from sensory nerves, which are involved in peripheral and central sensitization in chronic myofascial pain.
In a placebo-controlled study of botulinum toxin A as a prophylactic treatment for chronic tension-type headache with myofascial trigger points producing referred head pain on a near-daily basis, patients in the botulinum toxin A group reported greater reductions in headache frequency during the first part of the study compared with placebo, but these effects dissipated by week 12 (22). Reductions in headache intensity over time did not differ significantly between groups, although a larger proportion of botulinum toxin A patients showed evidence of statistically significant improvements in headache intensity in the time series analyses. There were no differences between the groups on any of the secondary outcome measures. Injection of botulinum toxin A directly into the ubiquitous myofascial trigger points in chronic tension-type headache is partially supported in this pilot study. Definitive trials with larger samples are needed to test this hypothesis further. A Cochrane review of controlled trials comparing botulinum toxin A injections with placebo in patients with myofascial pain did not show a statistically significant difference between the two groups in reduction of pain intensity (57). The duration of pain relief following botulinum toxin was usually of short duration. However, patients with myofascial pain syndrome previously treated with a local infiltration of anesthetic and steroids, who then received a single injection of botulinum toxin, experience significantly reduced pain for a relatively long time (11). A pilot study of direct injection of prabotulinumtoxinA, a highly purified preparation of botulinum toxin A, into painful muscle groups in cervical and shoulder girdle myofascial pain showed improvement in pain scores and quality of life lasting at least 12 weeks, with no serious adverse effects (31). Larger randomized and controlled clinical trials are suggested.
Dry needling. Dry needling or intramuscular stimulation involves multiple advances of a needle into the muscle at the region of a trigger point. Much like any injection technique, the physician should aim to elicit a local twitch response, reproduction of the patient’s symptomatology, and relief of muscle tension. Several studies found no long-term difference between local anesthetic injections and dry needling. Local tenderness following dry needling peaks within the first 24 hours after therapy. It can be minimized using heat packs and stretch therapy. A position paper of the Israeli Society of Musculoskeletal Medicine states that intramuscular stimulation is one of the preferred treatments for myofascial pain syndrome as it is evidence-based, effective, safe, and inexpensive (47).
Results of a randomized controlled study suggest that stretching exercises associated with local anesthetic or dry needling injections were effective in the decrease of pain levels in myofascial pain syndrome, as well as the increase in cervical range of motion and decrease in depressive mood levels of individuals (05). No statistically significant differences were seen between local anesthetic injections and dry needling.
Miniscalpel-needle release. Eighty-three trigger points in 43 patients with myofascial pain syndrome were treated and randomly assigned to three groups: group 1 received miniscalpel-needle release in conjunction with self-neck-stretching exercises; group 2 received acupuncture needling treatment and performed self-neck-stretching exercises; and group 3, the control group, was assigned self-neck-stretching exercises only (39). The improvement of pain intensity, pressure pain threshold, and contralateral bending range of motion of the cervical spine was significantly greater in groups 1 and 2 than in the control group at 2-week and 3-month follow-ups. Compared with group 2, patients in group 1 had a statistically significant reduction in pain intensity and an increase in pressure pain threshold and contralateral bending range of motion of the cervical spine at 3-month follow-up.
Concluding remarks on management. Many treatments are available for patients with myofascial pain, but none is definitive or universally applicable. It would be desirable to have the patient evaluated by a multidisciplinary pain clinic to choose the best treatment or combination of treatments for the individual patient.
The only issues unique to pregnancy in myofascial pain syndrome relate to the evolving lumbar lordosis as the patient approaches term. These associated postural changes can become activating or perpetuating factors for myofascial trigger points.
There are no apparent contraindications to local, regional, or general anesthesia for patients with myofascial pain syndrome. Anecdotal concerns related to prolonged, static positioning during procedures requiring anesthesia have been reported as a potential activating mechanism for myofascial trigger points.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Ravi Uniyal MD DM
Dr. Uniyal of King George's Medical University has no relevant financial relationship to disclose.
See Profile
Randolph W Evans MD
Dr. Evans of Baylor College of Medicine received speaker honorariums from Abbvie.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026