Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Pathologic yawning can be a manifestation of stroke, seizures, hysteria, and disorders involving muscles responsible for the act of yawning. Several neurotransmitters and neurohormones are involved in the regulation of yawning. Several areas in the brain are implicated in yawning, but no definite yawning center has been identified. Propranolol can reduce the severity of yawning.
|
• Pathological spontaneous yawning has been reported with migraine, cerebral infarction, brain tumors, epilepsy, demyelinating disorders, and psychogenic disorders. | |
|
• Susceptibility to contagious yawning is reduced in patients with disorders that affect the ability for social interaction, such as autism spectrum disorders, psychopathy, and schizophrenia. | |
|
• Painful yawning disorders include primary yawning headache, primary stabbing headache with buccal triggers, secondary yawning pain resulting from cranial neuralgia (particularly with trigeminal neuralgia and glossopharyngeal neuralgia), and Eagle syndrome. | |
|
• Painful yawning may also occur with disorders of the musculoskeletal structures involved in yawning, as with temporomandibular joint pain, head and neck cancers, and postsurgical pain. | |
|
• Several drugs have been reported to induce repeated or forceful yawning, including antidepressants (particularly serotonin reuptake inhibitors), opioids, dopaminergic agents (especially the D2 dopamine agonist apomorphine), benzodiazepines, and some induction agents for intubation. | |
|
• Yawning involves a distributed neural network of the cerebrum, basal ganglia, cerebellum, brainstem, and upper cervical spinal cord. | |
|
• Yawning likely has a multifactorial purpose that includes increased vigilance, arousal when drowsiness occurs, social communication, and possibly facilitation of respiration and thermoregulatory modulation. | |
|
• The neuropharmacology of yawning is complex and involves several neurotransmitters, hormones, and modulators. |
Hippocrates listed yawning as one of the useful “natures,” and several others in the 16th and 17th centuries advanced theories from the release of tainted humor to the awakening of animal spirits. The metaphors that developed from these theories endured until the 19th century, when Charcot used it as a patient diagnosis during his lectures, and Darwin mentioned yawning in connection with emotional behavior (140).
French neurologist Henri Meige (1866-1940) noted yawning-like movements in a form of focal dystonia, characterized by involuntary oromandibular dystonia and blepharospasm (Meige syndrome, or blepharospasm-oromandibular dystonia syndrome) (109). British neurologist C David Marsden (1938-1998), on the suggestion of British neurologist Reginald Edward Kelley (1917-1990), suggested the name "Bruegel syndrome," believing that Flemish painter Pieter Brueghel the Elder (c1525-1530/1569) had "clearly recognised the syndrome" in the small oval painting "Yawning Man" (103; 49).
However, more recent scholarship suggests that the painting was by his eldest son, Pieter Brueghel the Younger (1564-1638) and that it depicts a rural man yawning with an uncovered mouth, something then considered rude (155). Other versions have also appeared.
|
• Pathological spontaneous yawning has been reported with migraine, cerebral infarction, brain tumors, epilepsy, demyelinating disorders, and psychogenic disorders (ie, "hysteria," conversion disorder). | |
|
• Susceptibility to contagious yawning is reduced in patients with disorders that affect the ability for social interaction, such as autism spectrum disorders, psychopathy (antisocial personality disorders and traits), and schizophrenia. | |
|
• The term "parakinesia brachialis oscitans" refers to the unusual phenomenon of involuntary antigravity movement of an otherwise plegic arm during yawning. | |
|
• Painful yawning disorders include primary yawning headache, primary stabbing headache with buccal triggers, secondary yawning pain resulting from cranial neuralgia (particularly with trigeminal neuralgia and glossopharyngeal neuralgia) or Eagle syndrome. | |
|
• Painful yawning may also occur with disorders of the musculoskeletal structures involved in yawning, as with temporomandibular joint pain, head and neck cancers, and postsurgical pain. | |
|
• Several drugs have been reported to induce repeated or forceful yawning, including antidepressants (particularly serotonin reuptake inhibitors), opioids, dopaminergic agents (especially the D2 dopamine agonist apomorphine), benzodiazepines, and some induction agents for intubation. |
Sleep deprivation, disrupted sleep, and sedating medications. Yawning is an expected phenomenon in association with sleep deprivation, disrupted sleep (eg, sleep apnea), and sedating medications. The most common causes of excessive daytime sleepiness are sleep deprivation, obstructive sleep apnea, and sedating medications. Other potential causes of excessive daytime sleepiness include: (1) obesity-hypoventilation syndrome (Pickwickian syndrome), which consists of the triad of obesity, sleep disordered breathing, and chronic hypercapnia during wakefulness in the absence of other known causes of hypercapnia; (2) other sleep disorders (eg, periodic limb movement disorder, narcolepsy, idiopathic hypersomnia, circadian rhythm disorders); (3) psychiatric conditions (eg, depression, anxiety, schizophrenia); (4) chronic pain (which may disrupt sleep, involve use of sedating analgesic medications, or be associated with anxiety and depression); (5) cancer (due in part to metabolic effects of rapidly growing tumors, depression and anxiety, and medications used for pain); (6) hypothyroidism; (7) catabolic states (eg, HIV infection and HIV-associated wasting, sympathetic overstimulation); (8) conditions in which extra effort is constantly required to perform "normal" activities because of mechanical limitations, weakness, or rigidity (eg, hemiparesis, paraparesis, motor neuron disease, and Parkinsonism); and (9) extreme aging.
Disorders associated with abnormal spontaneous yawning. Repetitive yawning may be pathological, and the number of yawns per day can exceed 100 (157; 158). The occurrence of three or more yawns in 15 minutes without an obvious cause is often used as a threshold for abnormal yawning frequency. However, even yawn frequencies below this may be pathological if they are closely temporally linked with some abnormal episodic behavior (eg, migraine, seizures).
Migraine. Yawning is a feature of both the prodrome and the postdrome of migraine (13; 65; 53; 76; 73; 74; 61; 43; 60; 63; 75; 160; 83). Yawning is a common self-reported symptom preceding or accompanying migraine attacks and is associated with aura, nausea, vomiting, osmophobia, and cutaneous allodynia in patients with migraine (55). Yawning is among the premonitory symptoms most predictive of a migraine (others include photophobia, drowsiness, increased thirst, and blurred vision) (43).
Between one fifth and one third of migraineurs report "dopaminergic" premonitory symptoms (25; 09); the most frequent dopaminergic symptom is yawning, followed by somnolence, nausea, vomiting, fatigue, mood changes, and diuresis (09). Migraine patients with dopaminergic symptoms had significantly longer attack duration, more frequent osmophobia, allodynia, and unilateral cranial autonomic symptoms than patients without dopaminergic symptoms (09).
Migraine patients usually exhibit hypersensitivity to dopaminergic agonists; in particular, migraineurs exhibit enhanced responsiveness to apomorphine challenge, with a significantly higher incidence of dopaminergic symptoms (eg, yawning, drowsiness, nausea, vomiting, dizziness, sweating) than controls, supporting a central dopaminergic hypersensitivity (14; 32; 20; 41).
Cerebrovascular disease. Abnormal yawning may occur in association with cerebrovascular disease, involving both infratentorial and supratentorial vascular distributions (84; 19; 141; 21; 86; 150).
Krasnianski and colleagues reported a 62-year-old woman with locked-in syndrome due to a vascular malformation of the basilar artery (megadolichobasilar artery) who could still yawn despite bilateral masticatory spasms and persistent trismus (84).
Cattaneo and colleagues reported two patients with brainstem stroke involving the upper pons and the pontomesencephalic junction who presented with transient excessive pathologic yawning (19).
Singer and colleagues reported seven cases of pathologic yawning (more than three yawns per 15 minutes) caused by acute middle cerebral artery strokes (141). Associated findings included gaze palsy (n=7), aphasia (n=5), and unimodal or multimodal neglect (n=3). Because of the large lesions, topographic lesion analysis was not attempted.
Krestel and colleagues studied 10 patients with acute anterior circulation stroke and pathologic yawning (ie, three or more yawns per 15 minutes without an obvious cause). Areas in which the ischemic brain lesions overlapped (in nine patients) involved the insula or the caudate nucleus (86).
In a series of 161 patients with acute middle cerebral artery stroke, Aksoy Gündoğdu and colleagues found that 43% had pathologic yawning, which was associated with stroke severity, presence of cortical involvement (70%), and insular (40%) as well as opercular infarcts (34%) (02). Clinical outcomes and mortality rates were not significantly associated with the occurrence of pathologic yawning.
Parakinesia brachialis oscitans. An unusual phenomenon of involuntary antigravity movement of an otherwise plegic arm during yawning was labeled "la parakinesie brachiale oscitante" [parakinesia brachialis oscitans] by Olivier Walusinski and colleagues (159; 157; 150), where the Latin oscitans (for oscitation) means to open the mouth wide and take in air deeply, often as an involuntary reaction to tiredness, sleepiness, or boredom.
(Source: Teive HA, Munhoz RP, Camargo CHF, Walusinski O. Yawning in neurology: a review. Arq Neuropsiquiatr 2018;76(7):473-80. Creative Commons Attribution [CC BY] License. A color version of the image is available in: Zorzetto...
Axial T1-weighted magnetic resonance image showing irregular signal characteristics in the left lateral frontal cortex and white matter extending to operculum, precentral gyrus, sylvian cortex (blue arrow), as well as gliosis i...
Axial gradient echo image showing hypointense foci with blooming effect, suggesting hemorrhage (red arrows). (Source: Chowdhury A, Datta AK, Biswas S, Biswas A. Parakinesia brachialis oscitans: a rare post-stroke phenomenon. Tr...
The magnetic resonance angiogram shows loss of flow signal in the intracranial portion of the left internal carotid artery (blue arrow), the left middle cerebral artery (green arrow), and the A1 segment of the left anterior cer...
(Source: Chowdhury A, Datta AK, Biswas S, Biswas A. Parakinesia brachialis oscitans--a rare post-stroke phenomenon. Tremor Other Hyperkinet Mov (N Y) 2022;12:6. Creative Commons Attribution 4.0 International License [CC-BY 4.0]...
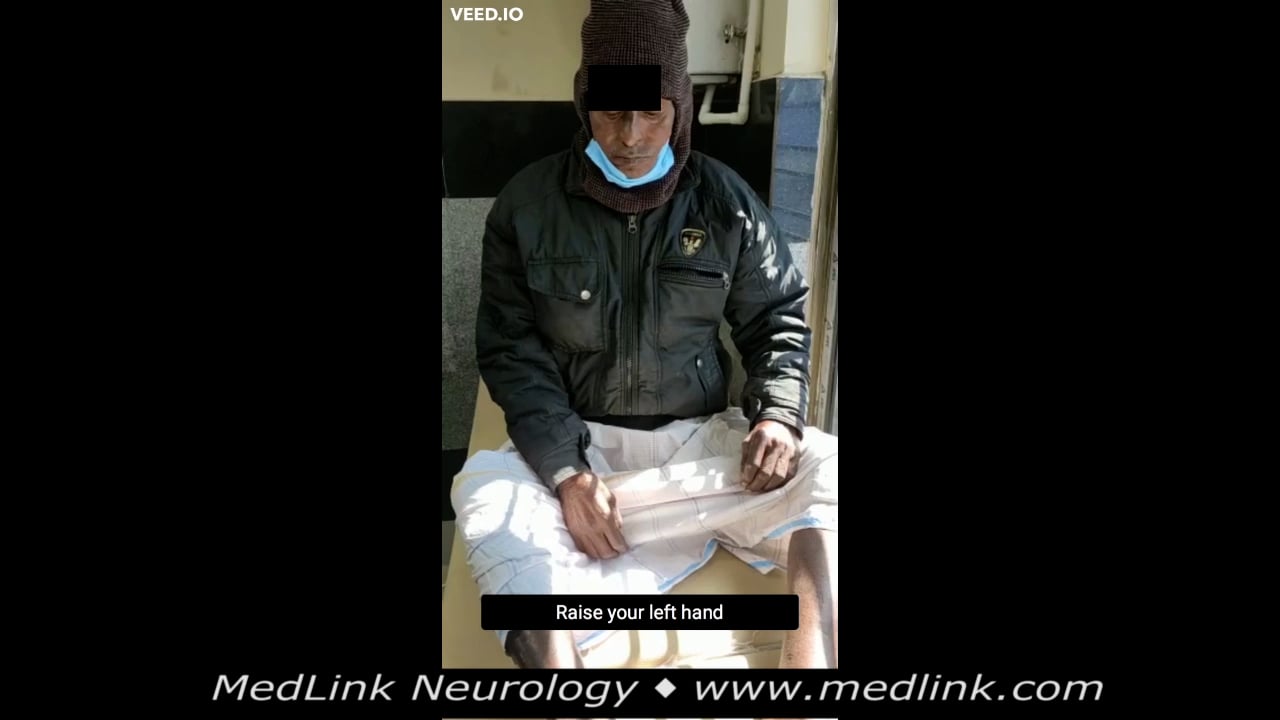
The video shows involuntary movement of the right arm during yawning, both while supine and apparently drowsy, and while seated. Source: Chowdhury A, Datta AK, Biswas S, Biswas A. Parakinesia brachialis oscitans--a rare post-st...
The reports of Walusinski and colleagues, along with prior and subsequent reports, have clarified some of the features of parakinesia brachialis oscitans (12; 117; 153; 159; 157; 19; 108; 33; 70; 170; 42; 72; 86; 150; 22; 95). Parakinesia brachialis oscitans has been reported much more frequently in men than women (sex ratio greater than 6:1) (94; 22). Loci of the cerebrovascular lesions in affected individuals have spanned much of the brain, including the cerebral cortex and subcortex (frontal, temporal, and occipital hemispheres), centrum semiovale, internal capsule, thalamus, basal ganglia (lenticular nucleus or just putamen), cerebellum, pons, and medulla oblongata (94; 22). Almost all of these areas have a role in motor control or are proximate to such areas. Ischemic strokes are strongly predominant among reported cases, with only occasional cases having reported hemorrhagic strokes or CADASIL (94; 22). Onset is typically delayed for 2 to 4 days from stroke onset but may range from stroke onset to as long as 4 months from stroke onset (22). The duration of parakinesia brachialis oscitans has been reported as ranging from 12 hours to more than 3 years (22).
Brain tumors. Intractable yawning as a predominant symptom of supratentorial tumor is rare (139; 11; 89). Cases have been reported with a teratoma in the supramedial cerebellum that compressed the dorsal side of the midbrain and upper pons (139), a meningioma of the foramen magnum extending down to the C1 level in a woman with neurofibromatosis type 2 (11), and a ganglioglioma in the posterior part of the inferior temporal gyrus (89).
Infratentorial causes for pathologic yawning include dorsal compression at the junction between the midbrain and pons. Saura and colleagues reported a 19-year-old woman with intractable yawning, whose MRI showed a tumor in the supramedial cerebellum that compressed the dorsal side of the midbrain and upper pons; the yawning completely disappeared after subtotal resection of the tumor, which was demonstrated on surgical pathology to be a mature teratoma (139).
Bayri and colleagues reported a 17-year-old woman with NF2 who underwent ventriculoperitoneal shunting and radiosurgery for a right vestibular schwannoma and a falcine meningioma (11). Fourteen months later, she was evaluated for an involuntary tilt of her head to the right side. Attempts to correct her head position precipitated intractable yawning. Cranial MRI revealed a 10 × 12 × 15 mm meningioma toward the right side of the foramen magnum extending down to the C1 level. The tumor was totally resected by a posterior approach using a dorsal midline skin incision between the external occipital protuberance and the spinous process of C2. Surgical pathology showed a psammomatous grade 1 meningioma. Following surgery, she could hold her head in the normal anatomical position and had complete resolution of the prior head-position-induced yawning.
Kutty and colleagues reported an 18-year-old woman with a ganglioglioma in the posterior part of the inferior temporal gyrus who presented with a 2-year history of bouts of abnormal yawning (89). Yawning bouts followed an initial period of absence of awareness lasting for 1 to 2 minutes. During these bouts, she yawned at least 20 to 30 times in succession, after which she experienced a mild headache and drowsiness. Bouts occurred at least 10 to 12 times at irregular intervals during a day. Pharmacologic therapy with carbamazepine was not effective. After clonazepam was added as a second drug, her episodic loss of awareness subsided, and she was left with bouts of intractable yawning. Cranial MRI showed no significant compression of brainstem structures. She underwent a craniotomy with total excision of the lesion. Surgical pathology revealed a temporal lobe ganglioglioma. Postoperatively, her yawning bouts improved and ultimately ceased, even after her medications were gradually withdrawn.
Epilepsy. Excessive yawning has been reported as part of the peri-ictal or ictal manifestations of epilepsy, most commonly in temporal lobe epilepsy (128; 52; 115; 116; 107; 165; 87; 146), although also rarely reported with other forms of epilepsy, including frontal lobe epilepsy, absence epilepsy, and infantile spasms (52; 35; 163). In one study of 97 patients with temporal lobe epilepsy, peri-ictal yawning was observed in 4.1% of patients and 1.8% of seizures, in the postictal period in all cases (87); peri-ictal yawning occurred only in patients with right-sided, nondominant temporal lobe epilepsy.
Penfield and Jasper described two adult patients with "autonomic seizures" and yawning but without reported EEGs. One patient with a tumor infiltrating the left temporal lobe and ipsilateral basal ganglia had seizures beginning with a headache associated with yawning, hiccup, urge to void, and focal sensory phenomena. The other had attacks characterized by sweating of her hands and scalp, a prickling sensation in her scalp and back, repetitive yawning, palpitations, visual distortions, and weakness (128).
Muchnik and colleagues described two patients with temporal lobe epilepsy and yawning. In one patient, yawning preceded focal seizures, and interictal EEG showed independent, bilateral, temporal epileptiform discharges, but imaging was not reported (115; 116). Their second patient, a 17-year-old woman with insulin-dependent diabetes and a normal cranial MRI, had complex partial seizures with secondary generalization and yawning during the postictal period; interictal EEG showed bilateral temporal spikes.
Yankovsky and colleagues reported a 48-year-old woman with a long history of seizures and irresistible, forceful, and often repetitive postictal yawning during which she was described as "alert" (165). Brain CT and MR imaging were normal. At age 30 years, she had invasive EEG studies, which disclosed epileptiform abnormalities over the right parietal operculum. Because her seizures did not improve following a right inferior parietal and posterior temporal resection, at age 31, she had further resection at the temporal edge of the previous operation, again with no improvement. Subsequent surface EEGs showed interictal epileptic activity over the right centro-parieto-temporal regions. Subsequent serial high-quality cranial MRI studies failed to show a structural lesion, except for postsurgical changes.
Casciato and colleagues reported a 19-year-old woman with Hashimoto encephalopathy (steroid-responsive encephalopathy associated with autoimmune thyroiditis) who had been referred to a psychiatric unit because of "delirium with sexual content" (18). She developed recurrent focal seizures characterized by repetitive forceful yawning, with EEG demonstrating seizures arising from the left temporal region. Antithyroperoxidase antibodies in her CSF and a good response to steroids confirmed the diagnosis of Hashimoto encephalopathy.
Nicotra and colleagues reported an 86-year-old man who had a prolonged seizure with impairment of consciousness and paroxysmal yawning recorded during a routine EEG (121). Clusters of yawns were the most striking manifestation. Ten yawns were observed, all of them occurring during the 14 minutes of unresponsiveness. During this period, the EEG showed diffuse electro-decremental activity while the patient's heart rate declined from 93 bpm to 73 bpm. There was no clinical or EEG response to external stimulation (visual, auditory, tactile, and painful stimulation). The patient became alert and responsive when the event ended, and the EEG returned to its original resting state. This was considered an autonomic complex partial seizure arising from diencephalic or brainstem structures with paroxysmal yawning.
Yawning as a peri-ictal or ictal manifestation of epilepsy may rarely occur with frontal lobe seizures. A 20-year-old man with yawning as a primary seizure semiology had dominant frontal lobe involvement (163). Video electroencephalography recorded eight yawning episodes accompanied by right arm movements that occurred during periods of rhythmic diffuse theta-range activity with left hemispheric predominance; magnetoencephalography coherence source imaging showed areas of high coherence reliably present over the left lateral orbitofrontal region.
Golgie and Green reported an adolescent with “petit mal” seizures in whom there was an association between yawning and 3-per-second spike-and-wave discharges (52).
Yawning may also occur as an unusual variant of infantile spasms. While evaluating video-EEGs, Donat and Wright found background EEGs showing true or modified hypsarrhythmia and yawning events that coincided with generalized attenuation, slow-wave transients, or other EEG ictal changes characteristic of infantile spasms (35).
Demyelinating disorders. Pathologic yawning may be a feature of demyelinating disorders (131; 48; 91; 40; 145).
Yawning during polysomnography is significantly increased in patients with multiple sclerosis compared to normal controls. However, no direct relationship was demonstrated between brainstem lesion on MRI and the presence of excess yawning (40). Curiously, in a study of 60 patients with multiple sclerosis, over one third reported that their multiple sclerosis symptoms improved following a yawn, and of those experiencing relief, nearly half reported that it lasted for several minutes or longer (48).
Excessive yawning spells were the presenting symptom of AQP4-IgG seropositive neuromyelitis optica spectrum disorder in five of nine women (91); yawning spells lasted from 2 to 16 weeks and usually occurred in association with nausea, vomiting, and hiccups.
Excessive yawning spells were also a prominent symptom in the initial presentation of AQP4-IgG seropositive neuromyelitis optica spectrum disorder in a 67-year-old woman (145). The patient was admitted with a 7-day history of progressive left-sided limb ataxia and hypesthesia. She yawned with a high frequency (more than three per minute) and often in bouts of more than eight yawns. MRI of the neck showed findings consistent with cervical myelitis extending over more than three vertebral segments to the lower medulla.
Excessive yawning spells were a significant symptom of AQP4-IgG seropositive neuromyelitis optica spectrum disorder in this 67-year-old woman. (Source: Spahlinger V, Niessen A, Rauer S, Krämer S, Reinhard M. The big yawning: pa...
Excessive yawning spells were a significant symptom of AQP4-IgG seropositive neuromyelitis optica spectrum disorder in this 67-year-old woman. (Source: Spahlinger V, Niessen A, Rauer S, Krämer S, Reinhard M. The big yawning: pa...
Excessive yawning spells were a significant symptom of AQP4-IgG seropositive neuromyelitis optica spectrum disorder in this 67-year-old woman. After treatment with methylprednisolone, plasmapheresis, and immunoadsorption, clini...
Excessive yawning spells were a significant symptom of AQP4-IgG seropositive neuromyelitis optica spectrum disorder in this 67-year-old woman. After treatment with methylprednisolone, plasmapheresis, and immunoadsorption, clini...
Aquaporin-4 antibodies were positive. She met diagnostic criteria for a neuromyelitis optica spectrum disorder (164). After treatment with methylprednisolone, plasmapheresis, and immunoadsorption, clinical symptoms resolved, and the frequency of yawning normalized.
Chiari malformation type I. Zebian and colleagues reported excessive yawning as a presenting symptom of Chiari malformation type I in two adolescent girls, and in both cases, it resolved following foramen magnum decompression (169).
Foix-Chavany-Marie syndrome. Foix-Chavany-Marie syndrome (bilateral anterior opercular syndrome) is a form of pseudobulbar paralysis. Manifestations include volitional paralysis of masticatory, facial, pharyngeal, and lingual muscles innervated by cranial nerves V, VII, IX, X, and XII, with preserved autonomic and emotional innervation of these muscles. Thus, although volitional movements are absent, including an inability to volitionally perform the motor program of yawning, automatic yawning as well as emotional smiling, laughter, and crying are preserved (112; 99; 142; 166; 134).
Motion sickness. The most characteristic symptoms of motion sickness are pallor, nausea, and vomiting. Motion sickness is generally associated with prominent vegetative disturbances, particularly involving the gastrointestinal and cardiovascular systems. Yawning is commonly associated with motion sickness and has been suggested as a behavioral marker of the onset of soporific effects associated with motion sickness (106).
Psychogenic disorders. Pathological spontaneous yawning has been reported with psychogenic disorders (ie, "hysteria," conversion disorder) (50).
Disorders of contagious yawning. Contagious yawning in response to someone else's yawn is a common and quite normal phenomenon, albeit one that is not well understood. Variation in contagious yawning may be driven by biased attentional processes and yawn detection rather than emotional sharing (44). A study to verify an attentional bias hypothesis of yawning showed that the social bond significantly predicted auditory yawn contagiousness, which was highest between friends and family members (122). However, other studies found no such effects and suggested that the phenomenon remains unexplained (10).
Although controversial, several studies have suggested that contagious yawning involves the mirror neuron system. An fMRI study to assess brain activity during contagious yawning found that visually perceived yawning activates Brodmann area 9 in the right inferior frontal gyrus, a region involved in the human mirror neuron system (58). Similarly, a study of sensorimotor mu oscillations on EEG found greater mu suppression in response to videos of yawning than to videos of control stimuli (26). A study using transcranial magnetic stimulation found that approximately 50% of the variability in the tendency for contagious yawning is determined by cortical excitability and physiological inhibition in the primary motor cortex (16).
Susceptibility to contagious yawning is reduced in patients with disorders that affect the ability for social interaction, such as autism spectrum disorders, psychopathy (antisocial personality disorders and traits), and schizophrenia (57; 56; 39).
Normal children do not exhibit contagious yawning until around 4 years of age (39). Contagious yawning was assessed in a sample of 30 children with autism spectrum disorder aged 6 to 15 years (ie, well beyond the point when normal children exhibit robust contagious yawning) who were compared with chronological-age-matched (n = 28) or mental-age-matched (n = 28) normally developing children: none of the children with autism yawned contagiously, and only three of 10 children with pervasive developmental disorder-not otherwise specified (PDD-NOS) yawned contagiously (PDD-NOS was a previously separate subtype of autism that was folded into "autism spectrum disorder" with the publication of DSM-5 in 2013), compared to 43% of the age-matched normal-development group.
Only some autistic children have an impaired contagious yawn response, which can be predicted by their lower blood oxytocin levels compared to either autistic children not affected by impaired yawning or normal children (101). In a double-blind placebo-controlled study on healthy volunteers, intranasal oxytocin, a hormone involved in social behavior and empathy, did not increase contagious yawning as expected but rather appeared to modulate its expression in ways indicative of an enhanced awareness of the social stigma associated with this behavior (45).
Painful yawning disorders.
Primary yawning headache. Primary yawning headache has been characterized as a recurrent severe paroxysmal headache precipitated by yawning (64). Although pain was induced by yawning, facial gestures, and forceful mouth opening did not reproduce the pain. Cranial nerve testing and MRI of the brain were unrevealing. It is considered a chronic, benign condition that requires no specific treatment but needs to be distinguished from secondary yawning headache, which is of greater clinical relevance.
Primary stabbing headache with buccal triggers. Primary stabbing headache is a primary benign headache syndrome that was first reported by Lansche in 1964, although he did not refer to yawning or other triggers (92). In a later case reported by Marcos and colleagues, yawning was identified as a specific trigger (100). A 75-year-old woman presented with a 2-week history of moderately severe, daily, episodic headaches that were "ultra-brief, lasting 1 second or less" and described by the patient as "stabs." They often occurred up to 50 times a day, significantly limiting her activities. They were right-sided and periorbital without associated autonomic signs, photophobia, phonophobia, or nausea. In addition to spontaneous attacks, she reported various triggers, including yawning, speaking, chewing, and swallowing. Examination disclosed no neurologic abnormalities, and in particular, the following signs were absent: conjunctival injection, lacrimation, eyelid edema, and nasal rhinorrhea or congestion. MRI of the brain and MR angiography of the supra-aortic vessels were normal, and there was no vessel in contiguity with the trigeminal nerve root. She tried paracetamol, ibuprofen, and carbamazepine without effect, but her headaches resolved 2 days following initiation of therapy with indomethacin 25 mg three times a day in conjunction with the proton-pump inhibitor pantoprazole (20 mg a day). Indomethacin was tapered and discontinued without recurrence after 18 months of follow-up.
Secondary yawning pain. Secondary yawning pain may occur in patients with cranial neuralgia, particularly with trigeminal neuralgia and glossopharyngeal neuralgia (29), and in Eagle syndrome.
Yawning is a recognized trigger for attacks of trigeminal neuralgia in susceptible people, occurring in 6% of 120 patients with classic trigeminal neuralgia seen at the Center for Neuropathic Pain at Sapienza University in Rome from 2015 through 2019 (27).
Painful attacks of glossopharyngeal neuralgia either occur spontaneously or are triggered by yawning, swallowing, talking, laughing, mastication (chewing), coughing, sneezing, or teeth brushing (30; 62; 147; 126; 67; 96; 129; 36; 161). In one series, yawning was a trigger for two of 14 patients (14%) with glossopharyngeal neuralgia (161). The Headache Classification Committee of the International Headache Society (IHS) incorporated yawning as a trigger in The International Classification of Headache Disorders, 3rd edition; a required criterion is "precipitated by swallowing, coughing, talking, or yawning" (60).
The two somatic sensory branches of the vagus nerve, the auricular branch and the superior laryngeal nerve, can also be the site of a pain syndrome resembling tic douloureux (trigeminal neuralgia) (96). The trigger zone of vagal and superior laryngeal neuralgia is usually in the larynx. Like glossopharyngeal neuralgia, attacks are precipitated by yawning, swallowing, talking, or coughing (96).
Eagle syndrome (or stylocarotid artery syndrome), first described by American academic otolaryngologist Watt Weems Eagle (1898-1980) at Duke University in 1937, is caused by elongation or calcification of the stylohyoid ligament and is characterized by neuralgic or steady pharyngeal pain radiating to the ear, which is worsened by swallowing and yawning (37; 38; 114; 168; 28; 71; 93).
A 17-year-old man presented to the emergency department with odynophagia and a foreign body sensation in the throat after choking on a chicken wing. A soft-tissue neck radiograph revealed a 4.6-cm linear object in the vallecula...
(Source: Czako L, Simko K, Thurzo A, Galis B, Varga I. The syndrome of elongated styloid process, the Eagle's syndrome-from anatomical, evolutionary and embryological backgrounds to 3D printing and personalized surgery planning...
(Source: Czako L, Simko K, Thurzo A, Galis B, Varga I. The syndrome of elongated styloid process, the Eagle's syndrome-from anatomical, evolutionary and embryological backgrounds to 3D printing and personalized surgery planning...
A fracture of the right ampullary area is present (arrow) and a gap is seen on the left side of the proximal area (arrowhead). (Source: Lee YW, Chung J. Eagle syndrome after a fracture of complete ossified stylohyoid ligament f...
(Source: Lee YW, Chung J. Eagle syndrome after a fracture of complete ossified stylohyoid ligament from indirect trauma treated using local steroid injection: a case report. Medicine (Baltimore) 2020;99(25):e20818. Creative Com...
The normal styloid process is 2.5 cm (ie, approximately 1 inch) to 3.0 cm in length (38), and any process longer than 3.0 cm is generally considered abnormally elongated (133; 79), although other thresholds from 2.5 to 4.0 cm have been proposed (130; 04). Eagle syndrome can manifest as typical glossopharyngeal neuralgia or carotidynia; it may also produce a foreign body sensation in the throat (globus sensation), dysphagia, and, less commonly, dysphonia and jaw clicking. Complications can include (1) carotid artery compression with cerebral infarction (04); (2) carotid artery dissection with cerebral infarction (03); (3) EXTracranial INternal Carotid arTery pseudoaneurysms ("EXTINCT") (148); and (4) venous nutcracker internal jugular syndrome due to compression of the internal jugular vein between the elongated transverse process of C1 and the styloid process and its ossified ligamentous-tendinous attachments (168; 148), leading to intracranial hypertension and cerebral hemorrhage (148).
A 26-year-old man presented to the emergency department because of a 5-day history of right-hand clumsiness and right arm and hand numbness. His symptoms developed suddenly while he was playing football. He had a prior history ...
Transverse CT image showing prominent styloid processes (arrows) in close proximity to vascular structures. A 26-year-old man presented to the emergency department because of a 5-day history of right-hand clumsiness and right-a...
CT angiography shows elongated styloid processes (arrows) in close proximity to the internal carotid arteries. A 26-year-old man presented to the emergency department because of a 5-day history of right-hand clumsiness and righ...
CT angiography with three-dimensional rendering showing a large left styloid process (black arrow) and a large completely calcified right stylohyoid ligament (blue arrow). A 30-year-old man presented to the emergency department...
A healthy 35-year-old man presented with a short history of left arm weakness and facial droop as well as a right-sided headache and neck stiffness. He later collapsed with left hemiplegia. MRI confirmed multiple embolic infarc...
A healthy 35-year-old man presented with a short history of left arm weakness and facial droop, as well as a right-sided headache and neck stiffness. He later collapsed with left hemiplegia. Magnetic resonance imaging confirmed...
A patient with the "Eagle jugular syndrome" (also known as "internal jugular vein nutcracker syndrome") presented with a 2-year history of pain in the right side of the face, soft tissue swelling (especially in the morning), an...
A patient with the "Eagle jugular syndrome" (also known as "internal jugular vein nutcracker syndrome") presented with a 2-year history of pain in the right side of the face, soft tissue swelling (especially in the morning), an...
The photograph shows the relationship between the elongated styloid process (° in black font) and the internal jugular vein (* in white font). (Source: Zamboni P, Scerrati A, Menegatti E, Galeotti R, et al. The eagle jugular sy...
The photograph shows that the styloid process was approximately 4 cm long, with normal being 3 cm or less. (Source: Zamboni P, Scerrati A, Menegatti E, Galeotti R, et al. The eagle jugular syndrome. BMC Neurol 2019;19(1):333. C...
Eagle syndrome can be diagnosed by digital palpation of the styloid process in the tonsillar fossa and by anteroposterior and lateral skull films (37; 38). Symptoms typically dissipate with surgical resection of the elongated styloid process.
Painful yawning may also occur with disorders of the musculoskeletal structures involved in yawning, as with temporomandibular joint pain (156; 66; 118; 88), head and neck cancers (eg, Hürthle cell carcinoma of the thyroid) (66), and postsurgical pain following a pterional approach for brain tumors (51). Temporomandibular joint dislocation or other injury has been reported during forceful yawning, especially with hyperextension of the mandible (98; 152; 151; 162; 07; 125; 120; 154; 21; 137; 01; 104).
Drug-induced yawning. Several drugs have been reported to induce repeated or forceful yawning (144; 127; 113), including antidepressants (particularly serotonin reuptake inhibitors, eg, fluoxetine, escitalopram) (125; 136; 80; 113), opioids (yawning may remain a residual symptom during the management of opioid withdrawal with buprenorphine), dopaminergic agents (eg, levodopa, apomorphine) (90; 14; 110; 111), benzodiazepines, induction agents for intubation (eg, propofol, thiopental) (81; 82; 07; 77; 123; 124), methylphenidate (two anecdotal reports) (119; 47), and valproate sodium (single case report, successfully treated with pimozide, a diphenylbutylpiperidine antipsychotic drug) (135).
A review of drug-induced yawning reported as an adverse drug reaction in the French pharmacovigilance database from 1985 through 2004 found that 28 adverse drug reactions were recorded involving 38 drugs, mainly serotoninergic agents (serotonin reuptake inhibitors [n=12]), dopaminergic agents (levodopa [n=3], dopamine agonists [n=3], monoamine oxidase B inhibitor [n=1]), opioids (n=4: morphine [n=1], methadone [n=1], buprenorphine [n=1], dextromethorphan [n=1]), benzodiazepines (n=4), and sodium channel inhibitors (lidocaine [2], flecainide [1]). Four adverse drug reactions were rated "serious," leading to hospitalization. Patient outcomes were usually favorable after drug withdrawal.
Apomorphine, a morphine derivative and D2 dopamine agonist used to treat "off" episodes in advanced Parkinson disease, has a very high frequency of drug-induced yawning (90; 149; 14). Apomorphine-induced yawning in nine healthy volunteers (14). This may be mediated by intracellular nitric oxide in the paraventricular nucleus of the hypothalamus (110; 111); morphine can block the yawning effect of apomorphine by preventing the increase in the paraventricular nitric oxide production induced by apomorphine (111).
Intractable "yawning" has also been reported during a course of electroconvulsive therapy with concurrent neuroleptic withdrawal (34). However, the patient was reported to have "begun to yawn incessantly. [H]er mouth remained open for hours at a time. As opposed to common yawning, the patient's yawning was not accompanied by pandiculation (stretching of the arms); instead, she appeared like a person who had lockjaw. The patient was unable to give a cogent explanation for this behavior. She denied feeling tired or bored but simply stated that she 'felt like yawning.'" Although the authors accepted this as "yawning," this adult-onset stereotypical motor behavior is more consistent with a motor stereotypy, functional movement disorder, or oromandibular dystonia. A motor stereotypy is an abnormal, involuntary, stereotyped, non-goal-directed movement pattern or vocalization that repeats continuously for a period and is typically distractable (78; 143): "fragments of normal actions that are continually repeated without purpose ... without conscious control, although consciousness remains intact" (97). Oromandibular dystonia affects the lower half of the face and mandible with sustained or intermittent, involuntary muscle contractions, which can cause sustained abnormal postures in the lower face (08; 68).
Yawning-associated tinnitus. In a report of the first case of a solitary cavernous hemangioma in the mastoid antrum, a 68-year-old woman presented with tinnitus of the right ear, especially when she yawned or swallowed (59). Both tympanic membranes appeared normal on otoscopic examination. Minimal hearing loss (up to 25 dB) was detected in the right ear on pure-tone audiometry. Temporal bone computed tomography revealed a 7.0 mm × 4.5 mm × 5 mm, solitary soft tissue mass in the aditus ad antrum (ie, the short passageway that connects the middle ear to the mastoid antrum). An excisional biopsy, which completely removed the mass without ossicular chain damage, established that the mass was a cavernous hemangioma. During follow-up, the patient's tinnitus and right low-frequency hearing loss was improved.
Yawning-induced alternobaric facial palsy. Alternobaric facial paresis is a temporary peripheral facial nerve weakness caused by sudden pressure changes in the middle ear, compressing the facial nerve. This is typically associated with diving or flying, but it has been reported after a prolonged yawn in an otherwise normal 27-year-old man (17).
The prognosis of pathologic yawning depends on that of the associated disorder.
|
• Yawning involves a distributed neural network involving the cerebrum, basal ganglia, cerebellum, brainstem, and upper cervical spinal cord. | |
|
• Yawning likely has a multifactorial purpose that includes increased vigilance, arousal when drowsiness occurs, social communication, and possibly facilitation of respiration and thermoregulatory modulation. | |
|
• The neuropharmacology of yawning is complex and involves several neurotransmitters, hormones, and modulators. |
Yawning is a fairly stereotyped motor program that is under only partial voluntary control. Yawning lasts 5 to 10 seconds and is accompanied by generalized stretching of body musculature, particularly the arms. Like swallowing, yawning is a reflexive phenomenon that is often repetitive and is difficult to modify by voluntary action. Yawning can be divided into three distinct phases: a long inspiratory phase, a brief pause, and a rapid expiration (31). Spontaneous yawning follows a circadian pattern, typically occurring just before going to sleep and on waking. Yawning is also associated with boredom.
Yawning results from the activity of an interconnected network of various supra- and infra-tentorial brain regions (24; 85). Both clinical and pharmacological studies indicate that yawning involves the paraventricular nucleus (PVN) of the hypothalamus, the brainstem (V, VII, IX, X, XI, and XII cranial nerve nuclei and fascicles; brainstem reticular formation; and the locus coeruleus), the spinal cord (innervating the phrenic nerve C1-4 and intercostal muscles), and probably the insula and limbic structures. Although the neuroanatomical localization of the brainstem motor pattern that orchestrates yawning is still disputed (06), multiple distinct neural pathways participate in the control of yawning: (1) oxytocinergic neurons in the paraventricular nucleus that either project to the hippocampus or to the brainstem; (2) neurons in the paraventricular nucleus that are activated by adrenocorticotropic hormone (ACTH) and alpha-melanocyte-stimulating hormone (alpha-MSH), and that project to the medial septum where they activate cholinergic septohippocampal neurons; (3) direct activation of septohippocampal or hippocampal neurons; and (4) a serotonergic-cholinergic pathway involving the insula and the hippocampus (05; 138; 24; 86).
Joshi and colleagues reported a 46-year-old woman with intractable epilepsy in whom electrical stimulation of the putamen consistently elicited yawning (69). She had invasive depth electrode monitoring and cortical stimulation mapping as part of her presurgical epilepsy evaluation. The first two contacts of a depth electrode that was intended to sample the left insula were in contact with the putamen. Stimulation of these contacts consistently elicited yawning on two separate days, but yawning did not occur during stimulation if she was simultaneously engaged in arithmetic and motor tasks. These findings suggest that the putamen may play an important role in the execution of motor movements of yawning and that activation of the anterior insult during attention and focused tasks could inhibit the putaminal processing necessary for yawning.
Yawning likely has a multifactorial purpose that includes increased vigilance, arousal when drowsiness occurs, social communication, and possibly facilitation of respiration and thermoregulatory modulation (31; 54; 85).
Neuropharmacologic regulation of yawning. Most of the evidence for the pharmacology of yawning was obtained in animals, particularly rats. The neuropharmacology of yawning is complex and involves several neurotransmitters, hormones, and modulators, including dopamine, serotonin, acetylcholine, glutamate, gamma-aminobutyric acid, nitric oxide, oxytocin, adrenaline, adrenocorticotropic hormone (ACTH), alpha-melanocyte-stimulating hormone, sexual hormones, and opiate peptides.
Important neural pathways involved in the regulation of yawning include: (1) two groups of oxytocinergic neurons projecting from the paraventricular nucleus of the hypothalamus (PVN) to the CA1 region of the hippocampus, or the...
Yawning is particularly influenced by the dopaminergic and serotonergic systems, which activate the cholinergic system. Dopamine may secondarily activate oxytocin production in the paraventricular nucleus of the hypothalamus, which in turn may then activate cholinergic transmission in the hippocampus (31). A surge in plasma ACTH levels at night and just prior to awakening from sleep is also associated with yawning in humans.
|
Neurotransmitter |
Effect on yawning |
Receptor(s) |
Brain region |
|
Acetylcholine |
stimulatory |
M1 |
hippocampus |
|
ACTH/MSH |
stimulatory |
MC4 |
hypothalamus |
|
Adrenergic |
enhancing |
α2-adrenergic |
? |
|
inhibitory |
β-adrenergic |
? | |
|
Dopamine |
stimulatory |
D3 |
PVN |
|
inhibitory |
D2 |
PVN | |
|
Excitatory amino acids |
stimulatory |
NMDA |
PVN |
|
GABA |
inhibitory |
GABAA/GABAB |
PVN, hippocampus |
|
Opioid peptides |
inhibitory |
μ-opioid |
PVN, other |
|
Oxytocin |
stimulatory |
OTXR |
PVN, hippocampus |
|
Nitric oxide |
stimulatory |
not applicable |
PVN, other |
|
Serotonin |
stimulatory |
5-HT2C |
? |
|
inhibitory |
5-HT2/5-HT1A |
? | |
|
| |||
Yawning and thermoregulation. Brain centers that control yawning are also involved in thermoregulation. According to the thermoregulatory theory of yawning, its function is to cool the brain in part by countercurrent heat exchange with the deep inhalation of ambient air (46; 105). The expression of contagious yawning in humans is altered by seasonal climate variation. Atypical yawning may function in part as a reactive mechanism in thermoregulatory disorders.
Yawning has been proposed to serve both physiological and social functions, the latter were likely to have developed later in its evolution. A central hypothesis is that yawning cools the brain, but whether yawning is a thermoregulatory mechanism that is activated during hyperthermia (ie, thermoregulatory failure) or is activated in any instance of brain temperature increase (eg, also during fever) is unclear, and experimental assessments of yawning during fever are lacking.
To assess the effect of experimentally induced fever on yawning frequency, 22 healthy human subjects participated in a randomized, placebo-controlled, cross-over study, where the subjects received an injection of bacterial endotoxin lipopolysaccharide in one condition and placebo in the other (102). Yawning frequency, scored from video recordings from 30 minutes before to 4 hours after the injection, significantly increased over time during experimentally induced sickness, and particularly during the rising phase of body temperature, but not in the placebo condition, although no significant correlation was found between body temperature increase and yawning frequency.
There are no epidemiologic studies of pathologic yawning. Most available studies are case reports and small hospital-based case series.
Yawning is a common phenomenon that is not often confused with other symptoms. Occasional reports have incorrectly labeled psychogenic disorders or oromandibular dystonia as pathologic yawning (34), but awareness of both functional (psychogenic) movement disorders in the stomatognathic system (167) and Meige syndrome (08; 68) should help avoid such clinical errors.
|
• Diagnostic procedures depend on the suspected cause or associated disease. |
Diagnostic procedures for pathologic yawning depend on the suspected cause or associated disease based on the other presenting manifestations. Excessive daytime somnolence may require investigations for sleep disorders, eg, detection of sleep apnea.
|
• Treatment for pathologic yawning is seldom necessary apart from the treatment of the underlying condition. | |
|
• Most cases of pathologic yawning resolve with appropriate treatment of the underlying condition. | |
|
• Drug-induced yawning usually responds promptly if the responsible drug is withdrawn. | |
|
• There is no approved drug for excessive or pathologic yawning. |
Treatment for pathologic yawning is seldom necessary apart from the treatment of the underlying condition. Fortunately, most cases of pathologic yawning resolve with appropriate treatment of the underlying condition. Drug-induced yawning usually responds promptly if the responsible drug is withdrawn. There is no evidence-based pharmacologic treatment for excessive or pathologic yawning.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neuro-Ophthalmology & Neuro-Otology
Apr. 07, 2026
General Neurology
Apr. 06, 2026