Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Pathologic laughter and crying occur in several neurologic disorders. This article describes the anatomical location of various brain centers for laughter and crying as well as the pathophysiology. Differential diagnosis, diagnostic workup, and management are described. In patients with cerebrovascular disease, pathologic laughter and crying may be warning signals that require prompt investigation and treatment of the underlying pathology. Antidepressants have been found to be useful in the management of these disorders.
|
• Pathologic laughter and crying are manifestations of neurologic disorders. | |
|
• Disturbances at various levels of the central nervous system are involved, although lesions of the brainstem are associated with pathologic laughter and crying. | |
|
• Neurologic investigations for these symptoms are aimed at detection of treatable lesions, eg, benign intracranial neoplasms. | |
|
• Antidepressants, particularly serotonin reuptake inhibitors, are usually effective for the symptomatic management of pathologic crying and laughter. | |
|
• Pathological laughter and crying are common and impair the quality of life, but treatment is available to manage these problems. |
Laughter has occupied philosophers from antiquity to modern times. It is generally associated with joy and humor. Laughter is elicited by a variety of stimuli and may be a reflex or a voluntary reaction to a certain situation or an expression of psychopathology. Pathologic laughter is defined as laughter that is inappropriate, uncontrolled, or dissociated from any stimulus. Pathologic laughter, often associated with crying, is also referred to as pseudobulbar affect and can occur as a part of emotional incontinence in neuropsychiatric disorders. Inappropriate laughter can occur in Witzelsucht and manifest as a tendency to tell inappropriate jokes or euphoric behavior due to focal right-orbitofrontal parenchymal lesions (83).
Less severe forms of the disorder following brain injury are often referred to as "emotionalism"; they are further specified as emotionalism-laughter or emotionalism-crying. Pathologic laughter or crying are included in the category of “involuntary emotional expression disorders” because they are disorders of emotional expression rather than affective mood disorders in which laughter and crying are associated with feelings of happiness or sadness. Episodes have been reported of spontaneous, uncontrollable laughter erupting from the congregations, even during times of solemn ceremony or messages from the pulpit. These episodes of "holy laughter" in charismatic Christian sects are not pathologic.
One of the oldest documented cases of pathologic laughter and crying is that by Ambroise Pare, the 16th-century French surgeon. He described women who wept and laughed without reason and did not respond to any treatment (33). A French physician, Trousseau, described pathologic laughter accompanying epileptic seizures (79). In 1886, cases of exaggerated emotional behavior, laughter as well as crying, were described in patients with lesions along the descending pathways to the brainstem termed “Zwangslachen und Zwangsweinen” in German (57).
Several isolated case reports in the literature over the past 20 years have described the association of pathologic laughter with a wide variety of neurologic disorders. The French refer to pathologic laughter preceding cerebrovascular ischemia as fou rire prodromique, which is translated as "prodrome of crazy laughter," and was first described by Charles Fere in 1903 (23). Although laughing and crying are lumped together, either of these may be the only manifestation. Fere reported pathologic laughter heralding an apoplectic event and was also among the first to describe gelastic epilepsy (30). Seizures accompanied by crying are referred to the rare condition “dacrystic seizures” first described by Zilgien in 1904 (87).
There has been considerable speculation in the past about the neural mechanisms of laughter. Wilson considered the mechanism to be in the region of the mesial thalamus, hypothalamus, and subthalamus (02). Papez hypothesized that supranuclear pathways, including those from the limbic system, mediate emotional expressions such as laughter and synapse in the reticular core of the brainstem (81). This fits in with a later postulate that the tegmentum near the periaqueductal gray matter contains the integrative mechanism for emotional expression (38). Pseudobulbar affect may be related to white matter degeneration, particularly in corticobulbar tracts (73).
|
• Pathologic laughter and crying may have an acute or gradual onset in chronic neurologic disorders. | |
|
• Episodes of laughter may alternate with crying spells and may rarely be the first or the sole manifestation. | |
|
• The prognosis depends on the primary pathology. |
Pathologic laughter or crying occurs out of context to the social setting, is usually unprovoked, and is not necessarily associated with the patient's underlying emotion. Pathologic laughter episodes resemble severe, spontaneous, nonpathologic laughter. Darwin's classical description of laughter is as follows:
|
During excessive laughter, the whole body is often thrown backwards and shaken, or almost as often, convulsed; respiration is much disturbed, the head and the face become engorged with blood, with the veins distended; the orbicularis muscles are spasmodically contracted...to protect the eyes. Tears are freely shed (18). |
Pathologic laughter may have an acute or gradual onset in chronic neurologic disorders. It is usually a part of a set of neurologic and neurobehavioral manifestations but may rarely be the first or sometimes the sole manifestation. The episodes of laughter may alternate with crying spells. Usually there are no triggering factors, but occasionally, smiling at a patient with this disorder might precipitate a fit of laughter.
The duration of episodes of laughter is usually short (ie, less than a minute) but may last up to an hour or until the patient is exhausted. Accompaniments may include spasmodic skeletal muscle contractions or seizures. Following the cessation of laughing, there is a variable period during which the muscles remain flaccid. Occasionally, paralysis in stroke patients may be observed after the fit of laughing is over.
The prognosis of pseudobulbar affect depends principally on its etiological substrate. When precipitated by acute cerebral insults, such as stroke or traumatic brain injury, gradual neurologic restitution may yield partial amelioration of affective lability, whereas pseudobulbar affect associated with chronic, progressive neurodegenerative disorders—including multiple sclerosis, Parkinson disease, amyotrophic lateral sclerosis, and primary lateral sclerosis—tends to persist or worsen alongside the underlying disease (25). Although pseudobulbar affect is not inherently life-limiting, it imposes considerable morbidity (02). Socially incongruent, uncontrollable paroxysms of laughter or crying foster embarrassment, stigmatization, social withdrawal, and heightened anxiety or depressive symptomatology. Concomitant bulbar dysfunction may provoke dysphagia, predisposing individuals to aspiration pneumonia, impairing speech, and necessitating enteral nutrition in severe cases to avert choking and malnutrition. Moreover, frequent misdiagnosis as a primary mood disorder delays appropriate intervention, thereby exacerbating psychological distress and obstructing timely symptom management.
The following is an instructive case report. A 59-year-old right-handed man with a history of episodes of ischemic stroke in the territory of the left middle cerebral artery, which resulted in right hemiparesis and aphasia, presented with pathological laughter and crying (20). A differential diagnosis between gelastic seizures and episodes of pathological laughter as a manifestation of repeated ischemic attacks was made. MRI showed lacunar infarcts in the left lenticular-capsular-thalamic area. There was some atherosclerosis in the carotid arteries and mitral stenosis, but no cardiac source of thromboembolism was identified. Transient ischemic attacks continued despite anticoagulation. Eventually, the mitral valve was replaced resulting in cessation of ischemic attacks and relief from pathological laughter and crying.
|
• Control of laughter may occur at the cortical or bulbar level with integration at the subthalamic level. | |
|
• Expression of laughter depends on an involuntary system involving the amygdala and the brainstem, as well as a voluntary system originating in the frontal areas and leading through the motor cortex and pyramidal tract to the ventral brainstem. |
The neuroanatomical localization of laughter is poorly defined. Control of laughter may occur at one or more of the following three levels: (1) a cortical level, probably the cingulate gyrus; (2) a bulbar or effector level; and (3) an integrative level, probably in the subthalamic. Lesions at any of these levels may produce pathologic laughter.
The medulla is the putative center for laughter and crying in the brainstem. Lesions in many areas of the brainstem cause abnormal emotional activity. The serotonergic raphe nuclei in the brainstem, which plays a role in the mechanism of pathologic crying, give rise to long projections to the limbic forebrain structures. The major ascending pathway from the rostral raphe nuclei joins the medial forebrain bundle in the lateral hypothalamus. Fibers leaving this main ascending bundle enter the substantia nigra, the intrathalamic nuclei, the stria terminalis, the septum, and the internal capsule.
Studies on volunteers during laughter show fMRI activity in the anterior supplemental motor area. Although the ventromedial frontal lobe is likely the center for perceiving what is funny, the accompanying laughter and feeling of mirth may be triggered by connections to other areas of the brain that are involved in control of movements of the mouth as well as positive emotions. Brain imaging with MRI shows pathological changes in the cerebellum, pons, pontocerebellar tracts, inferior olivary nuclei, and olivocerebellar tracts, but no degenerative changes are found in the corticobulbar or corticospinal tracts or in the serotoninergic raphe nuclei (84). A study revealed an augmented functional connectivity between the middle cerebellar peduncles and the posterior cingulate cortex, as well as a reduced functional connectivity between the middle cerebellar peduncles and the left middle frontal gyrus in patients with relative to patients without pseudobulbar affect. These findings suggest that certain distortions of the fronto-tempo-parietal-cerebellar circuits could be associated with the occurrence of pseudobulbar affect in amyotrophic lateral sclerosis. Notably, the anomalous functional connectivity between the cerebellum and the posterior cingulate cortex and the left middle frontal gyrus in pseudobulbar affect patients compared to those without pseudobulbar affect emphasizes the role of the cerebellum in regulating the expression of emotions in patients with amyotrophic lateral sclerosis (78).
Neuroimaging has been pivotal for elucidating the neural circuitry underlying pseudobulbar affect, revealing structural and functional abnormalities across a distributed emotion-regulation network. MRI studies, especially in multiple sclerosis cohorts, show that patients with pseudobulbar affect harbor characteristic lesions in the pons, bilateral inferior parietal cortex, and medial inferior‐ and superior-frontal regions, implicating widespread frontal, parietal, and brainstem pathways (26). Diffusion-based metrics further link pseudobulbar affect severity to microstructural degeneration of the bilateral corticobulbar tracts, mirroring clinical pseudobulbar palsy (25). Resting-state fMRI and DTI highlight reduced integrity and volume within midbrain, pontine, and superior cerebellar peduncular pathways, particularly in amyotrophic lateral sclerosis populations, underscoring brainstem-cerebellar contributions to emotional outbursts (78). Functional connectivity analyses corroborate these findings, demonstrating disrupted communication between cortical and subcortical regions tasked with suppressing inappropriate affect. Quantitative lesion and atrophy measures further distinguish pseudobulbar affect patients from controls and pinpoint how regional damage drives symptomatology (81). Collectively, these imaging insights map lesions and microstructural compromise to corticobulbar tracts, brainstem nuclei, cerebellar connections, and frontal-parietal cortices while revealing aberrant network synchrony, thereby furnishing objective evidence for the distributed circuit dysfunction that produces pseudobulbar affect and offering biomarkers for diagnosis and therapeutic monitoring (39).
Acute stimulation of an electrode located in the subthalamic nucleus during treatment of Parkinson disease induces loud laughter if stimulation parameters are raised higher than therapeutic level. Deep cerebellar electrical stimulation during treatment of patients with cerebral palsy can produce episodes of laughter.
Expression of laughter depends on two partially independent neuronal pathways:
|
(1) An “involuntary” or “emotionally driven” system, involving the amygdala, thalamic/hypo- and subthalamic areas, as well as the dorsal/tegmental brainstem. | |
|
(2) A “voluntary” system, originating in the premotor/frontal opercular areas and leading through the motor cortex and pyramidal tract to the ventral brainstem. |
These systems and the laughter response are coordinated by a center in the dorsal upper pons. Analysis of pontine lesions associated with pathological laughter and crying reported in the literature indicate a regulatory center in the pons with the most consistently involved region in the anterior paramedian pons, which may also be the site of a faciorespiratory center (21).
Pathologic laughter and crying are due to damage of pathways that arise in the motor areas of the cerebral cortex and descend to the brainstem to inhibit the center for laughter and crying. Based on this concept, laughter and crying would be considered "disinhibition" or "release" phenomena. Based on a case study, it has been proposed that the critical lesions in pathologic crying and laughter occur in the cerebro-ponto-cerebellar pathways (63). Therefore, the cerebellar structures that automatically adjust the execution of laughter or crying to the cognitive and situational context of a potential stimulus receive incomplete information. This results in inadequate and even chaotic behavior manifested as pathologic crying and laughter. Occurrence of pathologic laughter in cerebellar types of multiple system atrophy supports the view that cerebellum and its interconnected structures may be involved in the regulation of emotional expression.
Although pathologic laughter is mainly observed in various neurologic diseases in adults, rarely children may be affected. A 6-year-old child with acute cerebellitis after varicella presented with ataxia, dysmetria, mutism, and pathological laughter (15). Clinical-anatomic correlations performed in patients with focal infarcts in the basilar pons reveal that pathologic laughter results from rostral and medial pontine lesions and may result from disruption of the pontine component of associative corticopontocerebellar circuits. Increased pontine activation in pathologic laughter has been demonstrated with functional MRI but disappeared after successful treatment with paroxetine, a selective serotonin reuptake inhibitor (43).
Intraoperative electric cortical and subcortical stimulation mapping in an awake patient with diffuse astrocytoma of the right superior frontal gyrus and stimulation of the cingulum medially and inferiorly to the tumor elicited laughter without mirth (24). These findings support the role of the cingulum in the motor component of the mechanism, which is a useful functional landmark to identify the cingulum during subcortical mapping as a functional limit of the resection of intrinsic tumors.
Emotional incontinence manifested as episodes of crying and laughter are frequent in patients with small lenticulocapsular stroke. The findings appear to be consistent with the role of damage to serotonergic fibers in emotional incontinence, as they are particularly abundant in the internal globus pallidus.
A case of severe pathologic crying has been described after a limited left anterior choroidal artery territory infarction (19). This condition may be attributable to stroke-induced unilateral damage of the left capsular ascending projections of the serotonergic raphe nuclei. A single limited subcortical left-sided lesion with a critical topography regarding serotonergic pathways may cause permanent pathologic crying.
Furthermore, a case pseudobulbar affect was reported in an elderly woman with small vessel ischemic disease and alcohol abuse disorder (66). Thus, it is essential to recognize the possibility that pseudobulbar affect could occur in these disorders.
In cases of unilateral lesions, the left-sided lesions are more often associated with crying and the right-sided lesions with laughter. The cause of this dichotomy is not clear, but one explanation is that the left hemisphere's frontal lobes mediate emotions with a positive valence, and the right hemisphere mediates emotions with a negative valence.
In the circuitry involved in pathologic laughter and crying, ventral pons appears to be a crucial location, but further investigations are needed to determine how lesions in the basis pontis affect the activity of the cerebellum and the brainstem (62).
Causes of pathological laughing and crying can be classified in two groups (07):
|
(1) Altered behavior with unmotivated happiness: Angelman syndrome, schizophrenia, manias, dementia, etc. | |
|
(2) Interference with the inhibitory and excitatory mechanisms: gelastic epilepsy, fou rire prodromique in strokes, multiple sclerosis, amyotrophic lateral sclerosis, Parkinson disease, traumatic brain injury, brain tumors, etc. |
Another concept is that lesions of the corticopontine projections can produce pathological laughing and crying whereas direct activation of the emotional pathway can result in emotional lability and the laughing or crying of gelastic epilepsy (45). A 2-hit model of pathological laughter and crying has been proposed, which is based on the analysis of lesion network-symptom-mapping: a combination of direct lesion and indirect diaschisis effects cause pathological laughter and crying through the loss of inhibitory cortical control of a dysfunctional emotional system (41).
A novel classification is based on pathogenesis as well as clinical and imaging findings of patients with disorders of laughter and crying. Patients are divided, according to intensity and frequency of laughter and crying, into hypoactive or hyperactive disorders of laughter and crying and subdivided into five subtypes: sensory (positive and negative), motor (positive and negative), and mixed (29). “Positive" and "negative" describe causation by irritative versus destructive lesions, respectively.
Pathophysiologically, pathological laughing and crying involves white matter degeneration, which can impair voluntary control over emotional expressions (73). Additionally, damage to the cortico-subcortical-thalamo-cerebellar circuitry and dysregulation of neurotransmitters like serotonin and norepinephrine further contribute to emotional dysregulation. This complex interplay of neural and chemical disruptions underscores the multifaceted nature of pathological laughing and crying and the need for targeted therapeutic approaches.
Beyond structural lesions, alterations in neurotransmitter systems play a pivotal role in the pathophysiology of pseudobulbar affect. Dysregulation of serotonergic, glutamatergic, and noradrenergic pathways within the cortico-ponto-cerebellar and cortico-limbic circuits contributes to the loss of inhibitory control over emotional expression. For instance, reduced serotonin availability in key brainstem and subcortical regions correlates with increased emotional lability, supporting the clinical efficacy of selective serotonin reuptake inhibitors (SSRIs), such as paroxetine, in mitigating symptoms. Similarly, modulation of glutamate neurotransmission by agents like dextromethorphan/quinidine has shown benefit, highlighting the importance of excitatory-inhibitory balance in emotional regulation (02). These neurochemical insights not only clarify the multifaceted nature of pseudobulbar affect but also guide the development of targeted pharmacological therapies aimed at restoring network stability and improving patient quality of life.
Pathological crying. This is devoid of any emotional counterpart, and crying spells known to occur due to various brainstem, cortical hemispheric, or cerebellar lesions or, quite rarely in "dacrystic" epilepsy. Following a mild left thalamic stroke, a patient presented with crying spells triggered by thumb-index rubbing of his right hand with no emotional counterpart (11). In this patient, loss of sensation seemed to generate crying spells rather than the more common allodynia. The authors speculate that the pathway providing inhibition from the lateral to the medial segment of the ventral postero-lateral thalamus, which is linked to the anterior cingulate (limbic) cortex engaged in emotional behavior, might have been selectively affected. Pathologic tearfulness is reported in 50% of cases of autoimmune limbic encephalitis with no neuropsychiatric manifestations and indicates abnormalities in networks of emotion regulation beyond the acute hippocampal focus (06).
Disorders that are known to be associated with pathologic laughter and crying are shown in Table 1.
|
• Angelman syndrome |
Angelman syndrome. This is a genetic disorder that is associated with a deletion on chromosome 15 and is characterized by abnormalities or impairments in neurologic, motor, and intellectual functioning. Inappropriate and excessive laughter may occur in this syndrome.
Brain tumors. Tumors, mostly benign and occurring in a wide variety of locations, can manifest as pathologic laughter. Among the hemisphere tumors, those involving the frontal and temporal lobes are more likely to be associated with episodes of laughter.
Several case reports indicate that intrinsic as well as extrinsic tumors in the region of the brainstem are associated with pathologic laughter. Involuntary and inappropriate laughter may be an early sign of a meningiomas compressing ventrolateral brainstem and is relieved after resection of the tumors. Pathological laughter was one of the presenting symptoms of a giant clivus chordoma compression in the brainstem and was relieved following resection of the tumor by a transsphenoidal approach (32). Two cases of acoustic schwannoma presented with pathologic laughter that was resolved in each case by complete resection of the tumor (49). Cranial nerve tumors, arising in the cerebellopontine angle and compressing the brainstem, may produce similar effects. In several patients with trigeminal schwannoma who displayed symptoms of pathologic laughter and crying, there was no recurrence of laughter and crying attacks after total removal of the tumors. A patient who presented with pathologic crying caused by a trigeminal schwannoma was shown to have a tumor-associated cyst indenting the pons (13). Similarly, a patient with trochlear nerve neurinoma presented with pathologic laughter as the principal symptom, which was cured by tumor resection (50). Another case of trochlear nerve neurinoma presenting with pathological laughter and diplopia was reported, which resolved after excision of the tumor (67).
Pathologic laughter reported in children with pontine glioma is due to disruption of a network of cerebro-ponto-cerebellar pathways (34). Pathologic laughter and gelastic syncope have been reported as the sole presenting features of cerebellar ependyma (22). Hypothalamic hamartomas are frequently associated with gelastic and dacrystic seizures. A patient with a poorly differentiated metastatic pulmonary carcinoma in the pons presented with involuntary, persistent, and unmotivated laughter that preceded other clinical manifestations (65). A patient with glioblastoma multiforme in the right prefrontal area presented with pathologic laughter, which resolved after resection of the tumor (80). Well before other neurologic signs/symptoms, pathologic laughter may be the only symptom of a focal mass lesion causing ventrolateral upper brainstem compression such as petroclival meningioma (31).
Disseminated encephalomyelitis. Pseudobulbar affect due to acute disseminated encephalomyelitis is rare. According to a case report, a young Chinese woman manifested pseudobulbar affect due to disseminated encephalomyelitis for seven years (46). The patient's principal symptoms were extreme emotions or tears on hearing about sad news and uncontrollable laughter.
Drugs and toxins. Pathologic laughter can be a side effect of therapeutic drugs, drugs of abuse, or a manifestation of exposure to toxins. Inappropriate, uncontrollable laughter has been reported following intravenous sodium valproate for treatment of epilepsy. Pathologic laughter has been reported to be induced by sumatriptan (10). Uncontrollable laughter has been observed in healthy adults after marijuana intoxication in the absence of any pathologic changes in the brain. Inhalation of an insecticide was reported to induce pathologic laughing lasting 40 minutes, which was controlled by intravenous diazepam (86). Pathologic laughter has been reported in a patient with pontine hemorrhage following administration of atomoxetine as a cognitive enhancer (61). This resolved after discontinuation of atomoxetine. Atomoxetine is a CNS stimulant that increases norepinephrine and dopamine levels in the prefrontal cortex, which might play a role in the development of pathologic laughing.
Dacrystic epilepsy. This rare disorder is also referred to as "crying seizures" or “ictal weeping.” When dacrystic seizures are accompanied by gelastic seizures, the underlying lesion is a hypothalamic hamartoma, but when gelastic seizures are absent, the underlying etiology is of cortical (especially temporal) origin. Patients with dacrystic seizures generally have an underlying brain structural lesion, are frequently refractory to antiepileptic drugs, and often have a poor prognosis for seizure control (14).
Gelastic epilepsy. Laughter seizures are more likely to occur in epilepsies of frontal or temporal lobe origin. These may be associated with brain tumors or cerebral atrophy in these locations. Clinical features include absence of history of other conditions associated with pathologic laughter and presence of other manifestations generally accepted as epileptic. In an infant with intractable gelastic seizures, ictal positron emission tomography demonstrated epileptiform activity within a hypothalamic hamartoma (68). A teenager whose gelastic epilepsy due to an underlying hypothalamic hamartoma was found refractory to various antiepileptic drugs was treated successfully by stereotactic radiosurgery, resulting in total cessation of seizures (72).
Movement disorders. In a pilot study on patients admitted to a movement disorder clinic, 75.7% had pathologic crying, 13.5% had pathologic laughter, and 10.8% had both (70). The prevalence of both crying and laughter in individual diagnostic categories was 4.7% in idiopathic Parkinson disease, 2.7% in primary dystonia, and 3.1% in essential tremor.
Multiple sclerosis. Pathologic laughing and crying, which are distinct from emotional lability, occur in 10% of patients with multiple sclerosis. Severely disabled patients, generally with longstanding disease and cognitive deficits, are more likely to develop it. Pathologic laughing and crying in multiple sclerosis are likely due to involvement of the prefrontal cortex. There is no definite correlation with the location of cerebral lesions in demyelinating disorders. In a young woman presenting with acute pathologic laughter as a manifestation of demyelinating disease, MRI demonstrated lesions in the cerebral peduncles (54). A case has been reported of a patient who presented with paroxysmal hemidystonia along with bursts of pathologic laughter as the first manifestation of multiple sclerosis (01). There is a case report of pathologic laughter as the presenting symptom of clinically isolated brainstem syndrome due to a demyelinating process demonstrated by MRI and magnetic resonance spectroscopy (42).
Neurodegenerative disorders. Several neurodegenerative disorders are associated with pathologic crying and laughter. In one study of Alzheimer disease patients, 25% showed crying and 14% showed laughing or mixed (laughing and crying) episodes (71). Patients with mixed pathologic affect showed significantly more subcortical atrophy on CT than patients with pathologic affect crying. Pathologic laughing and crying seem to be more common in patients with amyotrophic lateral sclerosis than in patients with other neurodegenerative diseases (51). The findings of a study of behavioral physiology in these patients support the idea that pathological laughing and crying represents activation of all channels of emotional response, including behavioral, physiological, and subjective responses (56). Pathologic laughter occurs in 36% of patients with a cerebellar type of multiple system atrophy (63).
Pathological laughter and crying has been reported in three patients with Creutzfeldt-Jakob disease who had a mutation of prion protein gene codon180 (36). Widespread cerebral cortical involvement that is characteristic of this form of Creutzfeldt-Jakob disease was offered as an explanation of these symptoms.
Neurosurgical procedures on basal ganglia. History of neurosurgical procedures helps to identify the cause. Transient episodes of pathologic laughter occasionally follow deep brain stimulation. Emotional incontinence is included in the neurobehavioral complications of pallidotomy. A case has been reported of pathologic laughter after gamma knife thalamotomy, which resolved after treatment with sertraline (55). Pathologic crying has been reported following high-frequency deep brain stimulation in the region of the caudal internal capsule in a patient with Parkinson disease (47). Pathological crying has also been reported after subthalamic nucleus stimulation (60). A patient developed pathologic crying immediately postoperatively following deep brain stimulation of the subthalamic nucleus for Parkinson disease, and spread of the current to adjacent cortico-ponto-cerebellar pathways was considered to be responsible (85).
Pseudobulbar palsy. The term pseudobulbar palsy is used to describe uncontrolled activity of the lower motor neurons of the bulbar region and is a phenomenon that seems to cause laughing and crying not necessarily associated with emotions. The loss of the upper motor neurons also results in loss of control of these physical manifestations of emotion. A patient with pseudobulbar palsy presented with three episodes of spasmodic laughter, which had induced syncope (09).
Psychiatric disorders. Pathologic laughter and crying due to brain lesions are differentiated as emotional incontinence from lability of affect of mood disorders. However, when combined lesion of thalamic or brainstem structures and corticofugal motor projection systems are the pathoanatomic basis of affect incontinence, both affect lability and incontinence may be present. Pathologic laughter and crying may occur as manifestation of posttraumatic stress disorder. Pathologic laughter can present primarily as an obsessive-compulsive phenomenon. Inappropriate laughter has been reported in a patient with mental retardation and personality disorder (12).
Sleep-laughing (hypnogely). In most cases, hypnogely presents as a benign physiological phenomenon related to dreaming and REM sleep (77). Hypnogely is a symptom of neurologic disorders in only a minority of patients. It differs from physiological laughing as the sense of mirth is absent.
Stroke. Approximately one third of stroke patients develop emotional lability. Neuroradiological and neuropathologic studies of patients with pathologic laughter following cerebrovascular events have shown lesions in the internal capsule and thalamus, basal ganglion, hypothalamus, and ventral pons. Pathologic laughter may be the first manifestation of stroke. A transient fit of laughter can be the inaugural symptom of capsular-thalamic infarction. Prodromal pathologic laughter marked the onset of bilateral capsular genu infarction, demonstrated by MRI, in a patient (82). Pathological laughter has been reported as a manifestation of cerebral infarction due to middle cerebral artery occlusion. A patient with subarachnoid hemorrhage whose ruptured aneurysm was successfully obliterated surgically developed vasospasm resulting in cerebral infarction in the territory of middle cerebral artery and impaired consciousness (74). Pathological laughter developed six months after onset of initial ictus and when the patient had recovered consciousness, and it was successfully managed with sertraline. In another patient, sudden onset of left hemiparesis preceded by pathological laughter was overshadowed by severe behavioral changes, so that the diagnosis of stroke was missed until two days later when an MRI showed middle cerebral artery occlusion and the patient had passed the window for thrombolysis (58).
A case that presented with uncontrollable and unemotional laughter lasting an hour was followed by facial-brachial paresis due to pontine ischemia caused by vertebrobasilar stenosis, which progressed to bilateral brainstem infarction and resulted in death (28). A similar case of brainstem ischemia had a more favorable outcome after thrombolysis (17). Basilar artery occlusion is also associated with pathologic crying as a prodromal symptom expressed in French as folles larmes prodromiques (44).
Traumatic brain injury. Patients with traumatic brain injury can develop a pseudobulbar palsy with uncontrollable laughter and crying. The prevalence of pathologic laughter and crying during the first year after traumatic brain injury was 10.9% and usually associated with the presence of anxiety disorder and frontal lobe lesions (75).
Vascular malformations. Large aneurysms of the middle cerebral artery can produce the space-occupying effect of tumors in the temporal lobe region and present with pathologic laughter. A case has been reported of angiographically occult brainstem vascular malformation presenting solely with pathologic laughing and crying, which resolved after occlusion of the malformation by proton beam therapy (08). There was no manifestation of pseudobulbar palsy in this case.
Pseudobulbar affect is frequently confused with mood disorders, such as major depressive disorder and bipolar disorder, due to the presence of crying or laughing episodes. However, unlike mood disorders, pseudobulbar affect is characterized by sudden, brief, and involuntary emotional outbursts that are typically incongruent or disproportionate to the patient’s actual feelings and the social context. In contrast, mood disorders involve sustained changes in mood lasting weeks to months, with pervasive emotional experience rather than episodic affective expression (05). Other neurologic conditions, such as frontal lobe syndromes, behavioral disturbances in Alzheimer disease, epilepsy (especially gelastic seizures), and traumatic brain injury, may also mimic pseudobulbar affect symptoms. Essential crying, a normal variant seen in some individuals, can be mistaken for pathological crying but lacks the neurologic basis and severity of pseudobulbar affect. Accurate diagnosis relies on careful clinical history, observation of the nature and triggers of emotional episodes, and the use of validated scales like the Center for Neurologic Study–Lability Scale (CNS-LS) or the Pathological Laughter and Crying Scale (PLACS). Recognizing these distinctions is critical because pseudobulbar affect requires different management approaches than mood or psychiatric disorders, and misdiagnosis can lead to inappropriate treatment and prolonged patient distress (02).
|
• Drug screen | |
|
• Brain imaging | |
|
• EEG and EMG | |
|
• Neuropsychological assessment | |
|
• Pathological laughter and crying scale |
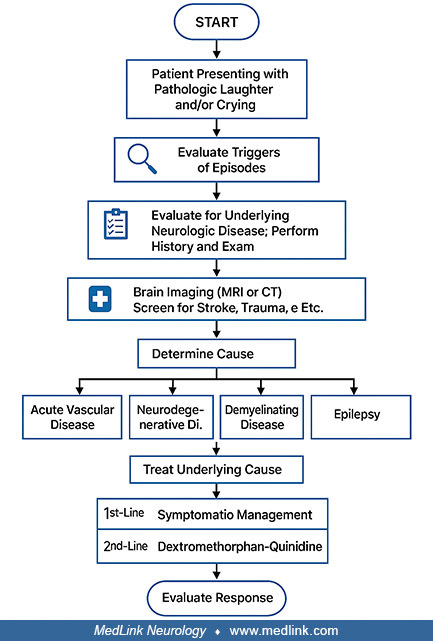
The diagnostic workup of the patient who presents with pathologic laughter and crying depends on the clinical condition suspected from the history. Basic workup should include a drug screen and brain imaging studies, including CT and MRI. Electrophysiological studies such as EEG and EMG are also helpful in the assessment of some of the conditions. Cerebral blood flow studies may be useful in patients with cerebral ischemia. A neuropsychological assessment should be done in these cases.
The Pathological Laughter and Crying Scale is used in the assessment of patients with stroke (02). It has some limitations, including reliance on self-rating and inadequate exploration of "appropriateness of emotion." The Center for Neurologic Study Lability Scale is a short, easily administered, and psychometrically sound measure of affective lability for use with patients with amyotrophic lateral sclerosis (48). It has potential applications as both a clinical screening device and a research tool. A modified Emotional Lability Questionnaire has also been found useful in assessment of patients with amyotrophic lateral sclerosis (52). The use of this scale shows an association of increased emotional lability with pseudobulbar symptoms. The Center for Neurologic Study Lability Scale was used to demonstrate the beneficial effects of dextromethorphan-quinidine for pseudobulbar affect, as manifested by pathologic laughter and crying, in a randomized, controlled trial on patients with multiple sclerosis (59).
In addition to objective assessments, a thorough clinical evaluation is essential for diagnosing pseudobulbar affect. This includes detailed history-taking focused on the nature, frequency, and triggers of emotional episodes, as well as their congruence with the patient’s underlying mood. Differentiating pseudobulbar affect from mood disorders, such as depression or bipolar disorder, is critical as these conditions require different management strategies. Diagnostic criteria, such as those proposed by Poeck and Cummings, emphasize features like sudden, involuntary, and inappropriate emotional outbursts that are disproportionate to or incongruent with the patient’s feelings and that cause distress or functional impairment (27). Caregiver or family reports are often invaluable, especially when patients have cognitive impairments. Combining clinical criteria with validated scales like the Center for Neurologic Study–Lability Scale (CNS-LS) or the Pathological Laughter and Crying Scale (PLACS) improves diagnostic accuracy and helps monitor treatment response (02). Ultimately, diagnosis relies on integrating clinical findings, exclusion of alternative causes, and supportive neuroimaging or electrophysiological studies when indicated.
|
• Removal of the cause by surgery, eg, a brain tumor. | |
|
• Excision of the epileptogenic focus in patients with gelastic epilepsy. | |
|
• Dextromethorphan-quinidine is approved for treatment of emotional lability. | |
|
• Lamotrigine has been used successfully in the treatment of pathologic laughing and crying following traumatic brain injury and stroke. |
The management of benign intracranial tumors associated with pathologic laughter and crying is surgical resection, which usually resolves the symptoms. In a patient who presented with pathologic laughter due to a large suprasellar cyst causing severe compression of the midbrain and pons, spontaneous laughing spells disappeared immediately after surgery (16).
A patient who suffered from epigastric psychic auras, complex partial seizures with a gelastic component, and secondarily generalized seizure with ictal involvement of the temporobasal region became seizure-free following right temporal lobe resection (53). Removal of the epileptogenic focus in patients with gelastic epilepsy of frontal lobe origin has been reported to result in good control of gelastic seizures (35).
In patients with cerebrovascular disease, pathologic laughter and crying may be the warning signals, which require prompt investigation and treatment of the underlying pathology. A review of placebo-controlled clinical trials in patients with stroke and emotionalism concluded that antidepressants may reduce the frequency and severity of crying or laughing episodes based on very low-quality evidence, and more reliable data are required before any definite recommendations can be made about the treatment of poststroke emotionalism (03).
In 2010, dextromethorphan-quinidine received approval from the U.S. Food and Drug Administration as first-in-class pharmacotherapy for emotional lability. Selective serotonin reuptake inhibitors (SSRIs) are the drugs of choice for pathologic crying after brain injury and accompanying depression. Potential benefits of SSRIs include treatment without using multiple drugs and the possibility of tailoring treatment to the individual patient (64). Frequently used preparations are fluoxetine, sertraline, citalopram, and paroxetine. Treatment with sertraline has been found to improve patients with pathologic crying and laughter without significant side effects. Citalopram and paroxetine are equally effective in the management of pathologic crying and laughter in patients with traumatic brain injury. The adverse effect after paroxetine is nausea and vomiting, whereas citalopram is usually well tolerated and without adverse effects. In randomized studies, citalopram has been shown to be effective in at least 50% of patients with pathologic crying. Citalopram has been used successfully for the treatment of pseudobulbar affect following progressive multifocal leukoencephalopathy (40). Furthermore, the use of escitalopram for pseudobulbar affect following severe traumatic brain injury was reported (04).
The rationale for the use of SSRIs is based on the evidence that serotonergic neurotransmission may be damaged in emotional incontinence.
If selective serotonin reuptake inhibitors are ineffective or not well-tolerated, second-line treatment options such as tricyclic antidepressants, noradrenergic reuptake inhibitors, dopaminergic agents, and uncompetitive N-methyl-D-aspartate receptor antagonists may be useful.
Significant and rapid recovery in both pathologic laughing and crying following stroke has been reported with lamotrigine treatment. Lamotrigine has been used successfully in the treatment of pathologic laughing and crying following traumatic brain injury. Duloxetine, a serotonin-norepinephrine reuptake inhibitor approved for the treatment of depression and neuropathic pain, is also useful for the treatment of pathologic laughter and crying. A prospective study showed that duloxetine could attenuate pathologic laughing exhibited by stroke patients, but randomized controlled studies are required to validate these findings (69).
A 60-year-old woman with multiple sclerosis presented with unrelenting crying as a manifestation pseudobulbar affect or emotional incontinence and was already unresponsive to SSRIs and dextromethorphan/quinidine but did respond to valproic acid (37).
The outcome of pseudobulbar affect varies widely depending on the underlying neurologic condition and lesion severity. Patients with benign or reversible brain lesions often experience significant relief or resolution of pathological laughter and crying (02). In contrast, those with chronic neurodegenerative diseases, such as amyotrophic lateral sclerosis, multiple sclerosis, Parkinson disease, or stroke tend to have persistent symptoms that may fluctuate but rarely fully remit (25). Importantly, pseudobulbar affect substantially impairs quality of life, social functioning, and emotional well-being, often causing distress disproportionate to the neurologic deficits themselves. Pharmacologic treatments, including selective serotonin reuptake inhibitors (SSRIs) and the FDA-approved combination of dextromethorphan/quinidine, have demonstrated efficacy in reducing the frequency and severity of emotional outbursts across multiple clinical trials. For example, large randomized controlled trials in patients with multiple sclerosis and amyotrophic lateral sclerosis showed that dextromethorphan/quinidine reduced laughing and crying episodes by approximately half compared to placebo (76). Early recognition and treatment of pseudobulbar affect can, therefore, improve symptom control and enhance patient and caregiver quality of life, although the degree of improvement depends on the extent of brain injury and disease progression. Rehabilitation approaches, such as speech therapy, may also support functional communication in affected patients. Overall, the prognosis is favorable in reversible lesions but guarded in progressive neurologic diseases, underscoring the need for individualized management strategies.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Fardin Nabizadeh MD
Mr. Nabizadeh of Iran University of Medical Sciences has no relevant financial relationships to disclose.
See Profile
Victor W Mark MD
Dr. Mark of the University of Alabama at Birmingham has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
General Neurology
May. 13, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neurobehavioral & Cognitive Disorders
Apr. 08, 2026