


Sleep Disorders
Sleep-related urologic dysfunction
Jul. 06, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The article offers an overview of the sleep disorders along with brief descriptions of the most recent developments advancing the field. This area of medicine has experienced a quasi-explosive expansion since the early development of clinical sleep laboratories in the 1970s. Sleep medicine oversees conditions as common as insomnia, restless legs syndrome, and sleep apnea, which have emerged as important risk factors for vascular disease and other ailments, such as diabetes. New information points to moderate to severe sleep apnea as a factor in cognitive decline. Sleep neurology also covers less common but equally socially destructive disorders, such as narcolepsy and the circadian dysrhythmias. Many neurologic disorders have associated sleep dysfunctions. The study of sleep physiology and pathophysiology is a window to the function of the brain. Overall successful clinical management of sleep disorders, whether breathing disorders, insomnias, hypersomnias, or parasomnias, improves the quality of life. This article discusses the most salient innovations and discoveries in sleep medicine that have occurred during the preceding year. Recent imaging of the brain has added valuable information on brain function during sleep, in sleep apnea, and in narcolepsy. The discovery of the glymphatic system has changed our understanding of the biology of sleep.
|
• Sleep medicine oversees conditions as common as insomnia, restless legs syndrome, and sleep apnea that reduce the quality of life and diminish the health of the individual. | |
|
• Some of these conditions have emerged as important risk factors for vascular disease, diabetes, and cognitive decline. | |
|
• It also covers less common but equally socially destructive disorders such as narcolepsy and the circadian dysrhythmias. | |
|
• Many neurologic disorders have associated sleep dysfunctions. | |
|
• The study of sleep physiology and pathophysiology is a window to the function of the brain. | |
|
• Successful clinical management of sleep disorders, whether insomnias, hypersomnias, parasomnias, or breathing disorders, improves the quality of life and ameliorates the health of the individual. | |
|
• Sleep dysfunctions may underlie modifiable cognitive degradation. | |
|
• Insomnia may have deleterious consequence if persistent and pervasive. | |
|
• The current COVID-19 pandemic has decompensated various sleep disorders. |
Although sleep is a universal experience, it was not studied systematically by scientists and physicians until the 20th century. Prior to the discovery of brain electrical activity, sleep was often assumed to be a passive response intended to rest during reduced cerebral stimulation associated with mental and cerebral inactivity. Aristotle believed that the condition of sleep was initiated by warm vapors from the stomach (54). Others attributed sleep to the effects of vascular congestion or anemia or to the buildup of "hypnotoxins." Sleepiness, dreaming, and cataplexy are eloquently displayed in Dante Alighieri’s (1265-1321), Divine Comedy, a journey into the afterlife (98). Franz Kafka was obsessed and plagued with insomnia, delayed sleep phase disorder, inadequate sleep hygiene, and chronic sleep deprivation (64).
Berger's demonstration of changes in the electroencephalogram (EEG) during sleep followed by the sleep-EEG studies of Loomis and colleagues provided the first definite evidence that the brain is not passive during sleep (17; 77). Studies of encephalitis lethargica by von Economo, of hypothalamic and thalamic stimulation by Hess, and of the reticular activating system by Moruzzi and Magoun provided major advances in the understanding of the neuroanatomical substrate of sleep and wakefulness (128; 53; 88). The discoveries of rapid eye movement (REM) sleep (09) and repetitive cycles of REM and NREM sleep throughout the night (37) led to a new view of sleep as an active process with distinctive neurophysiological substrates underlying the two major sleep states.
Physicians have known for centuries that sleep disturbance is often a sign of disease, but the recognition that primary sleep disorders are common, serious, and often treatable has occurred mainly in the second half of the 20th century. Narcolepsy, recognized in the 19th century, was often considered a form of epilepsy or a psychiatric disturbance until the discovery of its association with abnormal REM sleep (104; 121). This discovery made narcolepsy the first identified primary sleep disorder; that is, a disorder associated with abnormalities of the sleep process related to brain dysfunction. The discovery of the hypocretin-1 deficiency syndrome responsible for narcolepsy certified this concept.
In the mid-1960s, two other discoveries led to the recognition that sleep could facilitate the appearance of specific disorders. The first was the identification of abnormal breathing patterns during sleep in association with obesity (Pickwickian syndrome) (43; 69); the second was the discovery of regular recurring patterns of leg movements during sleep (78), now called periodic limb movements of sleep. Further study of breathing during sleep led to the recognition of the importance of upper airway occlusion as a primary cause of sleep-related breathing disturbance (107).
Sleep disturbances have taken central stage in cognitive degradation. A variety of disorders such as REM sleep behavior disorder (RBD), excessive daytime sleepiness, and sleep apnea are emerging as strong vascular risk factors affecting the brain.
In the 1970s, the first sleep clinics devoted specifically to diagnosis and treatment of a broad range of sleep disorders were created. The Association of Sleep Disorders Centers, organized in 1975, provided a focus for development of the field of sleep disorders medicine. Subsequent major events included the publication of Sleep, the first journal devoted specifically to sleep disorders medicine. As the breadth of the field emerged, it became apparent that a nosology devoted to sleep disorders was required. The Association of Sleep Disorders Centers published the first classification of sleep disorders in 1979 (10). A more comprehensive classification was published by the American Sleep Disorders Association in 1990 as the International Classification of Sleep Disorders and revised in 2000 (05). It was updated in 2005 by the American Academy of Sleep Medicine and again in 2014 and 2023 (03; 04) (Table 1). The American Board of Sleep Medicine (ABSM) was established in 1979 with the objective to promote excellence in medical care for patients with sleep disorders. ABSM certification is a lifetime credential that was intended to provide a standard of excellence by which “the public and members of government and regulatory bodies could identify skill, experience and competence”. Starting in 2007, authorized member boards of the American Board of Medical Specialties (American Board of Psychiatry and Neurology, American Board of Family Medicine, American Board of Internal Medicine, American Board of Otolaryngology and American Board of Pediatrics) began offering certification exams in sleep medicine every two years. Waivers of formal fellowship training to apply for the new exam expired in 2011. Diplomates are required to recertify their title every 10 years by complying with Maintenance of Certification normatives, some of which have been contested by specialty associations (122).
|
1. Insomnia | |
|
Appendix A: Sleep related medical and neurologic disorders | |
Sleep complaints generally fall into six major categories: (1) insomnia, (2) excessive somnolence, (3) snoring and sleep breathing difficulties, (4) sleep-wake disruption (circadian dysrhythmia), (5) bizarre sleep-related behaviors (parasomnias), and (6) sleep-related movement disorders. Insomnia includes complaints of difficulty falling asleep, staying asleep, awakening too early, and a feeling that sleep has not provided the usual sense of restoration with related daytime manifestations despite opportunity to rest adequately. Excessive daytime sleepiness refers to uncontrollable drowsiness and unwanted sleep episodes during waking hours. The term hypersomnia should be restricted to conditions of excessive sleep duration whereas hypersomnolence means excessive daytime sleepiness. Circadian dysrhythmias refer to disorders of timing of the sleep-wake pattern with the night-day cycle. Parasomnias are defined as undesirable physical phenomena that occur primarily during sleep. A particular sleep disorder may be associated with one or more of these major categories of symptoms. For example, obstructive sleep apnea may be associated with restless sleep and frequent awakenings (insomnia); choking, gasping, and mumbling during sleep (parasomnia); and irresistible drowsiness (hypersomnia).
The chief complaint provides a focus for assessing the patient's concerns and for eliciting the history. Information from the bed partner or other observers must often be obtained, as most patients are unaware of the frequency and severity of snoring and cannot describe leg jerks, twitches, sleepwalking, or violent behavior during sleep. The duration of the complaint and the circumstances at the onset of sleep difficulties are important pieces of information. Chronic insomnia is a most prevalent disorder that includes persistent sleep difficulty, adequate sleep opportunity and associated daytime dysfunction (03; 04).
The daily schedule, including time of awakening and going to bed; time of naps; time of meals and social activities; and time and use of caffeine, alcohol, tobacco, and prescription and over-the-counter medications may point to particular sleep disorders. The bedtime routine and the method of awakening (ie, spontaneous, with an alarm, or by a family member) should be determined, and the sleep schedule during weekdays, weekends, or days off from work or school should be compared. The sleeping environment may play a role in sleep disruption; excessive noise, extreme temperatures, or an uncomfortable bed may be significant factors. The relationship between sleep disturbance and medical illness should be assessed as such disorders as chronic pain, arthritis, asthma, heart disease, gastroesophageal reflux, and psychiatric disorders are commonly associated with disturbed sleep.
Patients with excessive daytime sleepiness may describe drowsiness, increased need for sleep, or irresistible daytime sleep episodes. Others have little awareness of their daytime sleep episodes or believe that they represent normal states of being. For some patients, falling asleep while driving or in other dangerous situations is the impetus that leads to evaluation. Mild sleepiness is most often apparent during the afternoon in quiet, boring situations; with more severe sleepiness, the patient may report falling asleep while eating, in conversation, or while standing. Symptoms associated with sleepiness provide important clues to diagnosis. Loud snoring and witnessed apneas during sleep strongly suggest obstructive sleep apnea syndrome. Bilateral muscle weakness in conjunction with laughter or other emotions is characteristic of cataplexy, which in combination with excessive sleepiness, is diagnostic of narcolepsy type 1.
Patients who complain of nocturnal insomnia and daytime sleepiness may have circadian rhythm sleep disorders. For example, difficulty falling asleep at night followed by normal sleep and difficulty waking up in the morning may be due to delayed sleep phase syndrome.
Patients with parasomnias may complain of a variety of nocturnal sensations or exhibit bizarre movements, behaviors, or bodily events. Some patients are entirely unaware of the nighttime activity, and a history from the bed partner or other observers is necessary. Some of the more distressing symptoms include nocturnal urinary incontinence (enuresis), shouting or screaming, and violent behavior. Patients may be particularly concerned about the possibility that serious medical illnesses are responsible for nighttime episodes of chest pain, gasping or choking, and palpitations. Furthermore, other patients are rightly distressed about possible nocturnal accidents or injuries to the bedmate. Adults falling out of bed while asleep should always consult a sleep specialist.
Sleep and sleep disturbances have taken a prominent stage in explaining the development of cognitive changes in progressive chronic neurologic diseases and in old age. The importance of such descriptions lies in the fact that many of the offending sleep problems are modifiable, thus opening a window of opportunity for the prevention and amelioration of cognitive disturbances in association with progressive neurologic diseases and in old age.
The prognosis depends on the particular sleep disorder. Therapeutic CPAP administration reduced mean arterial blood pressure by 3.3 mm Hg in a controlled study of hypertensive patients with moderate or severe obstructive sleep disordered breathing (96). The drop was observed after 3 to 4 weeks of continuous treatment, affecting systolic and diastolic pressures and during periods of being both asleep and awake. Patients with most severe sleep apnea disorder benefited the most, particularly if they were taking drug treatment for hypertension. The extrapolation of these results suggests that a fall of 3.3 mm Hg in blood pressure would be expected to be associated with a stroke risk reduction of 20% and a coronary heart disease event risk reduction of 15%. The estimated combined stroke and coronary event risk for moderate and severe sleep disordered breathing is 3% per year (71). Up to 1.5% of adult men have sleep-disordered breathing of this severity (116). Therefore, effective treatment of sleep disordered breathing could prevent 12,600 vascular events in men per year in the United States. Such reduction is comparable to that seen in the pharmacological treatment for control of hypertension.
There is a strong association between sleep apnea, as measured by the sleep apnea-hypopnea index, and traffic accidents (123). In patients with an apnea-hypopnea index of 10/hr or higher, the odds ratio for having a traffic accident is 6.3 (2.4 to 16.2 confidence interval). Consumption of alcohol increases the odds even further. Patients with narcolepsy and other forms of excessive daytime sleepiness also have a higher chance of being involved in automobile accidents.
In untreated men with severe obstructive sleep apnea-hypopnea (AHI > 30) the risk of fatal and nonfatal cardiovascular (MI, acute coronary insufficiency, and stroke) events is increased as compared to healthy subjects (fatal risk, OR 2.87, 95%CI 1.17-7.51; nonfatal risk, OR 3.17, 95%CI 1.12-7.51) (81). Patients with obstructive sleep apnea have a peak in sudden death from cardiac causes during the sleeping hours (midnight to 6 AM). People without obstructive sleep apnea have a nadir in sudden death from cardiac causes during the same period of time (41). Evidence is mounting that acute stroke patients have a high prevalence of sleep apnea (31), and when severe, it modifies cerebral blood flow and may facilitate neurologic deterioration. This has been termed “reversed Robin Hood syndrome” (02). Prompt application of noninvasive ventilation may reduce the risk of neurologic deterioration in patients with acute stroke and sleep apnea, but further clinical research is required. The ICSD-3 (03) incorporates respiratory effort related arousals as recognizable obstructive events in the PSG that should be counted towards the obstructive sleep apnea diagnostic criteria in association with obstructive apneas, mixed apneas, and hypopneas to conform the respiratory disturbance index.
Abnormal sleep patterns have a distinct impact on endocrine function in general and glucose metabolism in particular. Experimentally induced sleep deprivation in young men is associated with glucose intolerance as well as with other alterations of endocrine function and metabolic regulation (114). Hypercortisolism has been observed in idiopathic hypersomnia, and hypothalamic-pituitary axis relative activation has been linked with chronic insomnia (127). Provocative research associates sleep alterations and diabetes type II in men and in women but surprisingly finds evidence of a link only in women (126). In the China Kadoorie Biobank prospective cohort study, data were recorded from 487,200 adults 30 to 79 years of age who were free of stroke, coronary heart disease, and cancer at baseline (137). Three insomnia symptoms were assessed: self-reported difficulties initiating or maintaining sleep, early morning awakening, and daytime dysfunction for at least three days per week. The authors also assessed cerebrovascular incidents. They found that during a median of 9.6 years of follow-up cerebrovascular incidents occurred in 130,032 cases. The analysis showed that insomnia symptoms were associated with increased risk of cerebrovascular incidents with adjusted hazard ratios (HR) as follows: initiating and maintaining sleep HR 1.09 (95% CI 1.07–1.11); early morning awakening HR 1.07 (95% CI 1.07–1.11); and daytime dysfunction HR 1.13 (95% CI 1.09–1.18). Participants had higher risk of ischemic stroke but not hemorrhagic stroke. The authors concluded that individual and coexisting insomnia symptoms are independent risk factors for cerebrovascular incidence, especially among young adults.
REM sleep behavior disorder may herald the onset of alpha-synucleinopathies (Parkinson disease, multiple system atrophy, and dementia with Lewy bodies) by as many as 50 years (23; 63).
Parasomnia overlap disorder is emerging as an important neurologic condition (55). Parasomnia overlap disorder occurs when patients demonstrate features of both NREM parasomnias and REM sleep behavior disorder (111). In ICSD-3 parasomnia overlap disorder is considered a subtype of REM sleep behavior disorder where REM sleep behavior disorder is combined with a disorder of arousal (sleepwalking, confusional arousal, or sleep terror, sleep-related eating disorder), sexsomnia, or rhythmic movement disorder. Other authors have argued that parasomnia overlap disorder is a distinct pathophysiologic parasomnia and not a subtype of REM sleep behavior disorder (38). Polysomnography in parasomnia overlap disorder typically demonstrates NREM sleep instability in combination with REM sleep without atonia, at times with dream enactment behaviors. One third of patients with parasomnia overlap disorder have brainstem lesions and, therefore, formal neurologic evaluation is necessary, particularly if the results of the neurologic exam are abnormal. Treatment of REM sleep-related parasomnia disorders should be focused initially on creating a safe sleep environment while resolving comorbid conditions that fragment sleep, such as sleep-disordered breathing, and elimination of suspected precipitating pharmacology. Clonazepam is often effective, particularly for patients with violent dream enactment behavior.
Cognitive decline in patients with vascular dementia and neurodegenerative disease may be accelerated by uncontrolled moderate to severe sleep apnea (91; 103). There is preliminary evidence that treatment with CPAP may delay progression of cognitive impairment (103). Frequent snoring (β = -29; p = 0.0007), severe daytime sleepiness (β = -29; p = 0.05), and long sleep duration (β = -29; p = 0.04) predicted decline in executive function, adjusting for demographic characteristics, in the Northern Manhattan Study (102).
Pediatric sleep disorders may have a profound effect on cognitive development and behaviors. Specifically, uncontrolled sleep apnea has been associated with cognitive deficits in growing children. Manifestations of a sleep disorder in children may be different than those prevailing in adults. Sleepiness may not occur in sleep apnea, but the child may display disturbing behavioral and learning problems. Tonsillectomy rather than CPAP may likely be the treatment of choice in children with obstructive sleep apnea.
A 26-year-old man fell asleep in the dentist’s chair. He had a history of excessive sleepiness during daytime hours that he attributed to his poor nocturnal sleep. His work productivity had declined, and he had been cited to appear in court because of several unexplained car accidents. His family physician had requested an EEG as part of the evaluation of a sudden fall at a party where people were cracking jokes. The patient’s father had been killed in an automobile accident and the presumption was that he had fallen asleep at the wheel.
The physical and neurologic exams were normal, but the EEG showed abundant sleep with possible REM activity and the interpreter suggested performing nocturnal polysomnography. The overnight study showed short onset REM sleep latency of 20 minutes and 30% REM sleep. Nocturnal sleep was fragmented because of arousals and awakenings. The multiple sleep latency test showed a short sleep latency of three minutes, short onset REM sleep latency of one minute, and REM sleep in four of four naps. A diagnosis of narcolepsy with possible cataplexy was made.
The patient was counseled by the treating sleep physician who recommended two daytime naps of 15 minutes duration each, at 13:00 after lunch and at 17:00 when the patient arrived home from work. He also recommended a regimented sleep hygiene and extended a prescription for modafinil to take 200 mg in the morning. He advised the patient to call his office if modafinil showed only partial efficacy and to report more episodes of falling asleep were these to occur. Three months later the patient reported improved daytime alertness and increased work productivity. There had been no more car accidents or near-misses. The treating physician kept open the possibility of cataplexy and advised the patient to report any incidents of muscle weakness precipitated by emotions. The physician discussed the administration of sodium oxybate with the patient, for future reference.
|
• Functional and structural imaging of the brain has brought forth new pathogenetic information in several sleep disorders. | |
|
• The newly discovered glymphatic system is a metabolic waste removal brain system that is most active in slow wave sleep. | |
|
• Increasing evidence associates sleep fragmentation and short sleep duration with gut dysbiosis, leading to inflammation and fatigue. |
A variety of functional brain alterations have been identified in patients with insomnia. Generally, these point to hyperactivation in response to sleep-related and negative emotional stimuli or hypoactivation in response to tasks involving executive control. Functional MRI (fMRI) studies have found greater activation in response to emotional stimuli in the amygdala in individuals with insomnia when trying to re-interpret the meaning of negative pictures (39). In the limbic network, functional connectivity has been noted to be decreased between the thalamus and left amygdala, parahippocampal gyrus, putamen, pallidum, and hippocampus (138). In contrast, structural brain alterations are inconsistent.
In narcolepsy with cataplexy, structural alterations encompass the hypothalamus and its projections, in line with the loss of hypocretin neurons in the hypothalamus. Investigation of resting wakefulness in narcolepsy suggests decreased activity in regions that are targets of hypocretinergic projections (27). Functional alterations are observed in the hypothalamus during both resting wakefulness and while performing cognitive tasks or during positive emotions or cataplexy attacks. Alterations in white matter integrity have been found in the hypothalamus-thalamus-orbitofrontal pathway and in the brainstem, as well as in the inferior fronto-occipital fasciculus (46).
Imaging studies in patients with REM sleep behavior disorder reveal smaller gray matter volume in the thalamus, ponto-mesencephalic tegmentum, and temporal, frontal, and parietal cortices (42).
A meta-analysis of studies involving sleep apnea patients showed lower activation during various cognitive tasks, specifically in the dorsolateral prefrontal and orbitofrontal cortices, although higher activation was found in the insula, anterior cingulate cortex, amygdala, and hippocampus (58).
Glymphatic system. The glymphatic system is based on lymphatics, astrocytes, and glial cells, thereby its name (61). Surrounding the arteries and veins is the perivascular space. During the day norepinephrine levels are high, shrinking arteries and veins; during sleep, norepinephrine is low, opening up the vessels.
Spinal fluid goes into the perivascular space. From there it is transferred into astrocytes through a channel system called aquaporin-4. Fluid is transferred via the aquaporin channels into the astrocytes and then diffuses into the interstitial space.
Waste metabolic products abundantly produced by neuronal activity (ie, amyloid) are washed out from the interstitial space into the perivascular space around the veins (83). Fluid containing waste products enters the veins and is washed out via the kidneys into the urine. In summary, the glymphatic system is a drainage system for the brain.
The passage of fluid through the glymphatic system is dependent on the stage of sleep and is most active during slow-wave sleep (131). Insufficient slow-wave sleep reduces the activity of the glymphatic system allowing toxic products like amyloid to accumulate in the brain. Laboratory studies corroborate the functions of the glymphatic system (50).
Gut microbiota. Gut microbiota (microbial communities inhabiting the gastrointestinal tract) and its metabolites have been shown to exhibit diurnal rhythmicity that responds to the feeding and fasting cycle. Increasing evidence associates sleep fragmentation and short sleep duration with gut dysbiosis, leading to inflammation and fatigue (82). This is a new area of research that may influence the management of disorders affecting sleep, the immune system, and the metabolic system (120).
The etiology of sleep disorders is a function of the individual disorder. Narcolepsy research suggests an important role for the hypothalamic peptide neurotransmitter hypocretin 1 (35) also called orexin A and B. Experimental studies have shown that narcolepsy is caused in dogs by a deletion in the hypocretin receptor-2 gene (hypocretin-2) (75). Another group of investigators showed that hypocretin knockout mutant mice developed REM sleep or cataplexy while awake (21). These discoveries led to the hypothesis that reduced production of hypocretin in cells of the perifornical area in the lateral and posterior hypothalamus could underlie most cases of human narcolepsy. Further observations in humans support the notion that narcolepsy is an acquired disorder in the context of a predisposing genetic background and caused by destruction of cells in the hypothalamus (112). One hundred percent of patients with low CSF hypocretin-1 levels are positive for HLA DQB1*0602 but approximately 25% of normal individuals are also HLA positive, so this genetic variation is not sufficient to precipitate narcolepsy. In a study to evaluate the possible association between Pandemrix® vaccination and narcolepsy in Norway, 58 vaccinated children and adolescents (35 girls, 23 boys) aged 4 to 19 years (mean age 10.5 years) were diagnosed as new cases of confirmed narcolepsy, most within six months after vaccination (52). Thirty-seven patients who were analyzed had tissue type HLADQB1*0602. The authors concluded that there is a significantly increased risk for narcolepsy with cataplexy (P< .0001) and reduced CSF hypocretin levels in vaccinated children during the first year after Pandemrix® vaccination, particularly in genetically predisposed subjects.
Genetic involvement may also contribute to disorders such as circadian rhythm disorders (genetic polymorphism in gene hPer2 and hPer3), restless legs syndrome, periodic limb movements, and congenital central hypoventilation (PHOX2B gene) (06; 08; 115; 125).
Sleep-related obstruction to the flow of air in obese patients with a small oropharynx remains the most common mechanism for development of sleep apnea. However, other pathogenetic factors, mostly central in origin, are at play potentiating a clinically significant expression and disease. There is an intimate relationship between the autonomic nervous system and sleep. The concept of a state-dependent regulation of the autonomic nervous system has been addressed. Lugaresi and colleagues were the first to describe intense changes in systemic and pulmonary blood pressure associated with apneas and the renewal of breathing in patients with sleep apnea (79). This discovery opened a line of investigation that promises to uncover major pathophysiologic interactions between the sleep circuits and the autonomic nervous system involving thermoregulation, respiratory functions, cardiovascular regulation, and hormonal secretions (26).
Chemoreflex-mediated sleep apnea and hypoventilation are other areas of inquiry (124). Central sleep apnea may occasionally occur in patients with obstructive sleep apnea during titration with a continuous positive airway pressure (CPAP) device. In a large retrospective study of 1286 patients with a diagnosis of obstructive sleep apnea, 6.5% had CPAP-related central sleep apnea now called treatment-emergent sleep apnea (03). CPAP-emergent central sleep apnea is generally transitory and is eliminated within eight weeks after CPAP therapy. The prevalence of CPAP-persistent central sleep apnea has been about 1.5%. Severity of obstructive sleep apnea, a central apnea index of 5 or greater per hour of sleep, and use of opioids are potential risk factors (65).
Chronic intermittent hypoxia may damage the endothelium and trigger the release of proinflammatory factors, plasma cytokines, tumor necrosis factor-alpha, and interleukin-6. Furthermore, chronic intermittent hypoxia as observed in untreated sleep breathing disorders may lead to vascular dysfunction by increasing endothelin, increasing neurovascular oxidative stress, decreasing vascular neuromuscular reserve, decreasing vascular reactivity, and increasing susceptibility to injury (59).
In pregnant women with sleep apnea, placental hypoxia may precipitate a cascade of active factors from the placenta that generate profound effects on the maternal cardiovascular system causing hypertension, endothelial dysfunction, and preeclampsia.
Central dopamine metabolism and reduced iron stores, in a pattern that suggests that the homeostatic control of iron is altered, have been associated with restless legs syndrome and periodic limb movements (109). Alterations of the dopaminergic system also underlie REM sleep behavior disorder (RSBD). RSBD may herald the onset of a synucleinopathy more than 10 years before its clinical expression. Patients with the idiopathic form of RSBD with decreased striatal dopamine transporters imaging, substantia nigra hyperechogenicity, and hyposmia have an increased short-term risk for developing the classical motor, dysautonomic, and cognitive symptoms of a synucleinopathy (62).
Sleep disturbances after traumatic brain injury occur in 30% to 70% of individuals suffering from brain trauma (92). Insomnia, fatigue, and sleepiness are the most frequent complaints after head injury. The two main types of traumatic brain injury leading to altered sleep involve contact and acceleration/deceleration injuries. Diagnosis of a sleep disorder after traumatic brain injury may include polysomnography, multiple sleep latency test, and actigraphy. Treatment is disorder specific and includes the use of medications, continuous positive airway pressure (or similar device), and behavioral modifications.
Psychiatric and behavioral disorders are frequently encountered in the differential diagnosis of primary sleep disorders. These include anxiety disorders, mood disorders, schizophrenia, and somatoform disorders.
Hypoxia, autonomic dysfunction with loss of autoregulation, blood pressure instability, and inflammation may decrease cerebral blood flow in the territory of medullary penetrating arteries that irrigate the periventricular white matter. Small vessel disease of the brain generally affecting the subcortical and periventricular white matter is common in patients with advanced sleep apnea, old age, comorbidities (ie, diabetes), COPD, and smoking (22; 72). The subcortical white matter irrigated by long, small-caliber, medullary, terminal arteries is functionally a border zone area highly vulnerable to changes in blood pressure, altered vascular autoregulation, and hypoxia. Advanced small vessel disease increasingly disconnects the thalamic core of the brain from the frontal cortex, provoking a clinical picture where cognitive decline is dominant (105). Individuals with moderate-to-severe obstructive sleep apnea are almost four times more likely to have moderate-to-severe diffuse white matter hyperintensities than those with none-to-mild sleep apnea, independent of demographics and cardiovascular risk factors (36). The end of the spectrum is characterized by subcortical dementia, gait disturbance, and urinary incontinence, a condition that neuropathologists call Binswanger disease (33).
The inflow and outflow parameters of the glymphatic drainage system in patients with sleep apnea are changed, indicating impairment or deficient drainage (129). Parameters of the outflow are associated with the degree of cognitive impairment, as well as the hypoxia level. Importantly, continuous positive airway pressure applications enhance performance of the glymphatic drainage system after one month of treatment in sleep apnea patients. The authors propose that ventilation improvement in patients with sleep apnea might be a new strategy to ameliorate the impaired drainage of the glymphatic drainage system due to intermittent hypoxia, likely improving the cognitive decline.
Sleep disorders are common. About one third of adults report insomnia occurring at least occasionally over the course of a year, and one half of them describe it as a serious problem. About 10% of the population suffers the full clinical syndrome of chronic insomnia disorder (difficulty initiating or maintaining sleep, with excessive nocturnal awakenings; daytimes symptoms of fatigue, sleepiness, and related complaints; adequate opportunity to sleep and rest; and the sleep disturbance occurs at least three times per week and has been present for 3 months) (03). Twenty percent of adults in the United States use medication for insomnia in a given month (18). Up to one fourth of young to middle-aged adults use alcohol or medications to help with sleep problems (67). Insomnia is rapidly emerging as a disorder with ample medical ramifications (130). Clinical research suggests that adolescents with low sleep efficiency had a 4.0+/-1.2 mm Hg higher systolic blood pressure than other children (P< 0.01), and the authors concluded that poor sleep quality is associated with prehypertension in healthy adolescents (66). Insomnia, sleep fragmentation, and any kind of sleep deprivation in general may be associated with diabetes type 2 (14; 47; 126).
Among the elderly, sleep disturbances are even more common and are often associated with poor physical health, heart disease, or depression. All neurodegenerative disorders are associated with some form of sleep dysfunction. Particular mention should be made of Parkinson disease, a condition that provokes many manifestations of sleep dysfunction, whether insomnia, excessive daytime sleepiness, circadian dysrhythmia, or parasomnias.
Symptoms of sleep apnea occur in 2% to 4% of the working adult population in the United States (135). In selected subpopulations, the prevalence of sleep disordered breathing is even higher. For example, in a population of Canadian male grain workers, many of whom were overweight, the prevalence of sleep disordered breathing was estimated to be 25% (70). Sleep apnea syndrome of moderate to severe intensity affects 17% of 50 to 70-year-old men and 9% of 50 to 70-year-old women (93). Sleep disordered breathing is a risk factor for the development of systemic hypertension (90; 94), myocardial infarction, stroke (81; 133; 32), atrial fibrillation (40), and other ailments such as diabetes (60). The condition is common in patients recovering from stroke and may affect the functional outcome of the rehabilitation process. Sleep disordered breathing may be a life-threatening disorder in patients with neuromuscular disorders (29).
Cognitive impairment may be yet another long-term effect of uncontrolled sleep apnea. Among older women, those with sleep-disordered breathing compared with those without had an increased risk of developing cognitive impairment, according to a prospective sleep and cognition study of 298 women without dementia (mean age 82.3 years) who had overnight polysomnography performed (132). Compared with the 193 women without sleep-disordered breathing, the 105 women (35.2%) with sleep-disordered breathing were more likely to develop mild cognitive impairment or dementia (31.1% [n = 60] vs. 44.8% [n = 47]; adjusted odds ratio [AOR] 1.85; 95% [CI] 1.11-3.08). Elevated oxygen desaturation index (≥15 events/hour) and high percentage of sleep time (> 7%) in apnea or hypopnea (both measures of disordered breathing) were associated with risk of developing mild cognitive impairment or dementia (AOR 1.71 [95% CI 1.04-2.83] and AOR 2.04 [95% CI 1.10-3.78], respectively). The arousal index and wake after sleep onset that measure sleep fragmentation were not associated with risk of cognitive impairment.
Partial sleep deprivation and disturbed sleep patterns are common in shift workers in most industrialized societies. Twenty percent of the work force in industrialized countries engages in shift work activities (03). Emerging evidence suggests that breast and endometrial cancer may be linked to shift work. The International Agency for Research on Cancer (IARC) has listed shift work as a probable human carcinogen (117). Many studies have shown that telomeres are the caps at the end of each strand of DNA protecting chromosomes; short telomere length is associated with premature cellular aging and generally associated with increased cancer risk. Studies have demonstrated telomere shortening in nurses with intensive night work schedules for a period of more than five years (108). Although the association of short telomere length with breast cancer risk is inconclusive, a short telomere length might be a contributing factor for breast cancer risk among female shift workers. Interestingly, individuals with obstructive sleep apnea also have shorter telomere lengths, suggesting that sleep apnea is another factor causing premature cell aging (57). Sleep disorders are also common problems in children, and most adolescents probably do not get enough sleep to maintain optimal daytime alertness. The estimation has been made that 1500 fatal motor vehicle accidents per year in the United States are the consequence of falling asleep at the wheel (89).
During the third trimester of pregnancy, 10% of women may develop clinically significant sleep apnea, particularly if obese (99).
Education pertaining to sleep, sleep hygiene, and awareness of sleep disorders is probably the most important means of prevention. The 10 Commandments of Sleep Hygiene are posted on the World Sleep Day® website. High school and college students learn little about sleep and the effects of sleep deprivation. Although physicians are well positioned to educate patients about sleep and sleep disturbance, they also receive little education on this topic.
Obesity and the metabolic syndrome may underlie the epidemic progression of sleep disordered breathing (95). Bariatric surgery has become a popular form of treatment for morbidly obese patients.
Sudden death in sleep may be preventable. The quasi-epidemic of nocturnal sudden death affecting young men of Southeast Asian extraction may be due in part to the Brugada syndrome, a channelopathy that may lead to cardiac arrest. In patients suspected of harboring the Brugada syndrome, implantation of an automatic cardioverter-defibrillator could be lifesaving (19).
CPAP use delayed the age of onset of mild cognitive impairment (72.11 years vs. 82.10; p < 0.01) (91).
The differential diagnosis for patients with sleep disorders depends on the signs and symptoms. The International Classification of Sleep Disorders, 3rd Edition, provides a comprehensive nosology of sleep disorders (03).
Sleep disorders caused by medical, neurologic, and psychiatric disorders are not primary sleep disorders; they tend to vary in severity with the underlying disorder. For example, disturbed sleep is a prominent symptom in many patients with major depression and is common in a variety of medical diseases, including chronic obstructive pulmonary disease, end-stage renal disease, and congestive heart failure. Sleep disorders are prominent in various neurologic disorders (30). Patients with Parkinson disease complain frequently about their sleep problems (110) and may exhibit REM sleep behavior disorder several decades before the onset of classic motor signs of extrapyramidal motor disorder. Patients with headache disorders commonly have sleep disruption, or the occurrence of their headache is modulated by the sleep pattern. Patients with multiple sclerosis may have an intrinsic form of hypersomnia in addition to other causes of sleep-wake disorder and patients with myotonic dystrophy and other more rare neuromuscular conditions are also afflicted with sleep-wake problems. Epilepsy and sleep are intimately linked, and some seizure variants appear exclusively during nocturnal sleep. Parasomnias need to be differentiated from other ictal events occurring at night including seizures. In many instances testing in the sleep laboratory is necessary.
The possibility that complaints of disturbed sleep or daytime sleepiness are not due to a primary disorder of sleep must also be considered. Patients with complaints of fatigue or tiredness may believe that their symptoms are due to abnormal sleep when in fact they are more often related to medical or psychiatric illness. A loss of a sense of well-being, difficulty with attention and concentration, and an inability to function at an expected level may be attributed erroneously to disturbed sleep. With each of these symptoms, a sleep disturbance may be the cause, but other diagnoses are more likely.
For some patients, diagnosis can be established based on the history and the physical examination with no need for laboratory testing or additional evaluation. In other patients, the diagnosis may be strongly suspected, but laboratory tests are needed to determine the severity of the disorder and thereby direct treatment (28; 74). For example, obstructive sleep apnea may be strongly suspected based on the history and physical examination, but treatment recommendations may depend on the frequency of apneas, the severity of associated hypoxemia and sleepiness, and the occurrence of cardiac arrhythmias. Sleep logs, in which the patient records the times and amounts of sleep obtained over one or more weeks, are helpful, particularly in patients with suspected circadian rhythm sleep disorders and in those with insomnia. Actigraphy for 7, or even better, 14 days may be sufficient to diagnose a circadian sleep-wake disorder (87).
Complete blood count, serum chemistries, and thyroid function tests are indicated in selected patients. Pulmonary function tests, including arterial blood gases, are helpful if a hypoventilation syndrome due to obesity or neuromuscular disease is a consideration. Human leukocyte antigen testing may be useful in some cases of suspected narcolepsy and should be done if CSF analysis is contemplated because a negative HLA test will exclude a hypocretin insufficient syndrome and avoid the need for lumbar puncture. Urine toxicology screen may uncover evidence of drug abuse that is contributing to or causing sleep disturbance.
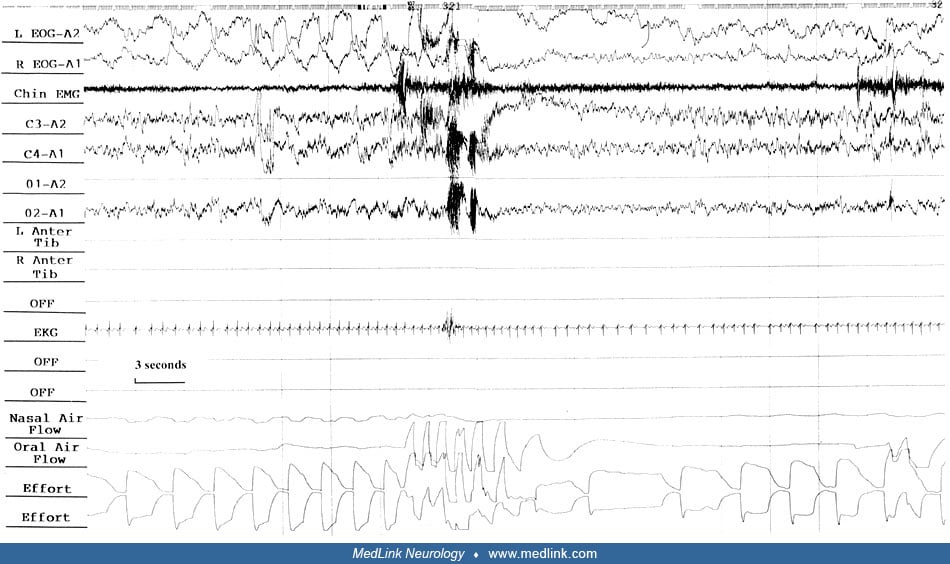
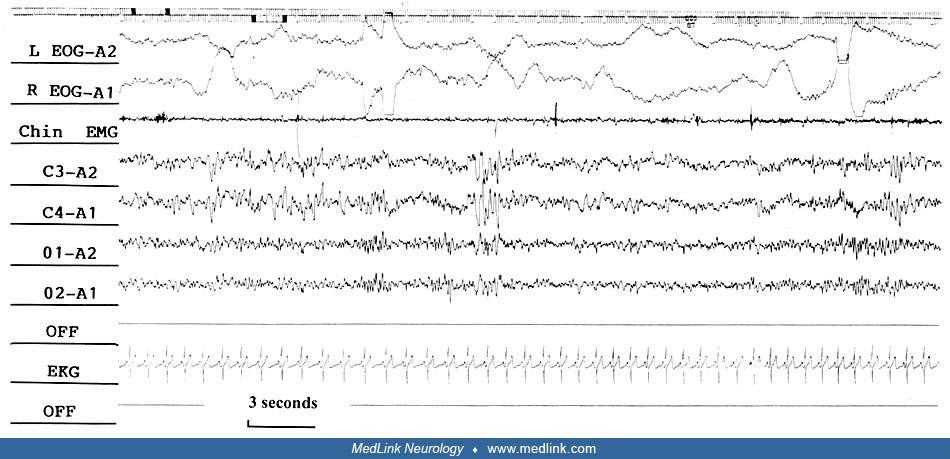
Polysomnography, with simultaneous monitoring of EEG, eye movements, heart rate, respiratory effort and airflow, oxygenation, and muscle tone, is used to confirm the diagnosis of sleep apnea and to assess the severity of associated sleep disruption and hypoxemia.
Polysomnography is also useful in the diagnosis of narcolepsy and in some cases of suspected periodic limb movements, nocturnal epilepsy, REM sleep behavior disorder, and other parasomnias. Although polysomnography is not required for diagnosis in many patients with complaints of insomnia, it may be helpful in some patients with refractory insomnia or in whom sleep state misperception is suspected and to exclude other primary sleep disorders.
The multiple sleep latency test provides diagnostically useful information in the hypersomnolence disorders and is performed the day after nocturnal polysomnography (11). With this test, patients are asked to nap for up to 20 minutes at 2-hour intervals; the time to the onset of sleep (sleep latency) and from sleep onset to the onset REM sleep (REM-sleep latency) are calculated for each nap. The mean sleep latency provides a measure of the severity of sleepiness, and the occurrence of REM sleep in two or more naps supports a diagnosis of narcolepsy.
The Maintenance of Wakefulness Test (MWT) is designed to test the capacity of the individual to remain awake over 40 minutes of testing time in the sleep laboratory (76) and is useful to assess the ability to drive and be awake performing duties.
Although laboratory polysomnography is the preferred diagnostic modality, portable monitoring has been developed as an alternative diagnostic approach for sleep apnea evaluation. A portable monitor records fewer physiologic variables but is typically unattended and can be performed in the home. In March 2008, the U.S. Centers for Medicare and Medicaid Services released a statement allowing the use of portable monitoring to diagnose sleep apnea and to prescribe continuous positive airway pressure. This action has opened the door for more widespread use of unattended portable home monitoring devices (24).
Cerebral function can be studied with neuroimaging techniques in sleep in human subjects in the course of clinical research. Work has provided provocative images of the dormant brain (34). Human brain activity during sleep alternates within specific areas in relation to the sleep stage and previous waking activity. The work on neuroimaging has provided new data that describe some aspects of the pathophysiology of disorders such as insomnia, sleep apnea, and restless legs syndrome. Future studies, conducted with state-of-the-art techniques on large numbers of patients, will be able to address important issues related to sleep and contribute significantly to the understanding of the neural basis of sleep pathophysiology. This will offer the opportunity to use neuroimaging in correlation with clinical and electrophysiological evaluations as a helpful tool in the diagnosis, classification, treatment, and monitoring of sleep disorders in humans.
Measurement of hypocretin-1 in CSF may play a role in the diagnosis of narcolepsy. The test results should be interpreted within the clinical context. Mignot has determined that 110 pg/ml of hypocretin-1 in CSF is the cut-off value to diagnose narcolepsy (86). Patients with idiopathic hypersomnia, sleep apnea, restless legs syndrome, or insomnia have normal hypocretin-1 levels. Patients with narcolepsy-cataplexy have predicted values of less than 110 pg/ml with a specificity of 99% and a sensitivity of 87%, which is higher than for the multiple sleep latency test. When cataplexy is absent or atypical, the predictive power is limited with high specificity (99%) but low sensitivity (16%). Most of these patients will have normal hypocretin-1 values, creating a dilemma for the clinician because this is precisely the group of patients in need of accurate diagnostic studies. The measurement of hypocretin-1 in CSF may be most useful in cases of narcolepsy without cataplexy, in children with excessive somnolence who have not, as yet, developed cataplexy, when the multiple sleep latency test is difficult to interpret because of medication effect, or in psychiatric conditions (86; 84). A negative HLA test will exclude a hypocretin insufficient syndrome and avoid the need for lumbar puncture.
Management depends on the particular sleep disorder. A decision memorandum posted by The Centers for Medicare and Medicaid Services on October 30, 2001, reviews the guidelines for authorized use of CPAP for the treatment of obstructive sleep apnea (51). Under these guidelines, CPAP will be covered under Medicare in adult patients with obstructive sleep apnea if either of the following criteria is met: apnea-hypopnea index greater than 15, or apnea-hypopnea index greater than 5 and less than 14 with documented symptoms of excessive daytime sleepiness, impaired cognition, mood disorders, or insomnia, or documented hypertension, ischemic heart disease, or history of stroke. The American Academy of Sleep Medicine has posted several guidelines for the use of PAP devices.
AutoPAP devices adapt to the required nocturnal airway pressures from breath to breath and record compliance with the machine over many weeks of treatment. Data from the SERVE-HF trial demonstrated an increase in cardiovascular mortality in heart failure patients with a reduced ejection fraction (< 45%) using adaptive servo-ventilation compared to a control group. The manufacturer (ResMed) issued a Field Safety Notice in 2015 stating that adaptive servo-ventilation therapy is contraindicated in this specific patient population (13).
A novel treatment for obstructive sleep apnea consists of adapting an oral interface connected to a pump that creates a negative pressure within the oral cavity while the subject sleeps (25). The objective is to create a pressure gradient that draws the soft palate anteriorly towards the tongue to permit improved oropharyngeal airflow during sleep. In a multicenter study of 63 subjects, the average nightly usage was 6.0±1.4h. There were no severe or serious adverse events, and the authors concluded that clinically significant improvements in sleep quality and continuity were achieved with this device.
The FDA has approved a neurostimulator implant for sleep apnea as a second-line therapy (118; 45). The implant keeps the airway open by stimulating the hypoglossal nerve during inspiration in sleep. Contraction of upper airway muscles causes the base of the tongue to move forward.
Obstructive sleep apnea and hypoxia have been associated with degrading cognitive test results. The polysomnographic study by Zhang and colleagues in 44 patients post-stroke 6 weeks after onset shows that obstructive sleep apnea contributes independently to cognitive dysfunction in stroke patients and strengthens the argument that early treatment of sleep apnea in stroke patients may lead to favorable effects on cognitive functions (68; 136).
Sodium oxybate (gamma hydroxybutyrate, GHB) is the drug of choice for treating patients with narcolepsy who experience episodes of cataplexy (07) not responding to traditional stimulants of wakefulness. Sodium oxybate has also been approved by the FDA for treatment of idiopathic hypersomnia. The low sodium preparation under the brand name of Xywav® is the preferred drug solution for individuals older than 40 years. Because of safety concerns associated with the use of the drug (known popularly as the date-rape drug), the distribution of sodium oxybate is tightly restricted to registered physicians and only dispensed out of one central pharmacy in the entire United States. A one dose per night of extended-release oral suspension of sodium oxybate (ON-SXB, also known as FT218) has been introduced to the market. The once-nightly bedtime dose of ON-SXB removes the need for a middle-of-the-night dose of sodium oxybate (106).
Wake-promoting drugs, some new and some old, are frequently added to the narcoleptic regimen (see chapters on hypersomnia and narcolepsy).
Treatment for chronic insomnia disorder includes cognitive behavioral therapy (CBT) and pharmacologic treatments, both of which are complementary (130). Cognitive behavioral therapy targets dysfunctional behaviors and beliefs that perpetuate insomnia. Cognitive behavioral therapy is conventionally delivered in six to eight settings by therapists with training in sleep disorders. The efficacy of cognitive behavioral therapy depends on adherence to rules that require discipline and regimentation like sleep restriction, stimulus control therapy, reduced arousals in sleep environment, relaxation techniques, and sleep hygiene. Pharmacologic therapy includes administration of benzodiazepine receptor agonists (temazepam, lorazepam, eszopiclone, zolpidem, zaleplon, triazolam), melatonin receptor agonists, antidepressants with sedating effect (doxepin, mirtazapine), and anticonvulsants (gabapentin).
Hypnotic drug development has been focused on the orexin (hypocretin) system that promotes wakefulness. Suvorexant (Merck, MK-4305) is the first compound of the dual orexin receptor antagonist (DORA) class approved by the FDA (119). This agent has a more focal target on a specific receptor than the GABA agonists that target a widespread array of receptors and, therefore, has less potential for adverse effects. Suvorexant does not depress the respiratory function or the central nervous system and may be safe for patients with sleep apnea.
Melatonin administration continues to puzzle clinicians. Melatonin is a hormone secreted by the pineal gland with widespread effects in circadian-related systems. Despite its potent action, melatonin is sold in the United States without prescription and is considered by most to be a hypnotic, which it is not. Melatonin possibly helps organize nocturnal sleep and anchors REM sleep. Clinical observations indicate that melatonin may improve and even affect the natural history of REM sleep behavior disorder, perhaps by changing the behavior of REM sleep in subjects who take it (73). Clinical trials are being considered to test the efficacy and safety of melatonin. A melatonin agonist (ramelteon) has shown small benefits for time to sleep onset.
Light therapy delivered by commercially available light boxes (5000 to 10,000 lux) has emerged as the most effective means of treating intrinsic circadian dysrhythmias (12).
A game changer in the management of sleep apnea has been the approval of weight-loss medications. Clinical guidelines recommend treatment of obesity in patients with obstructive sleep apnea. The Food and Drug Administration (FDA) has approved (fast-track FDA application 2024) the injectable prescription medicine tirzepatide for adults with moderate-to-severe obstructive sleep apnea and obesity (BMI > 30). Tirzepatide is a long-acting glucose-dependent insulinotropic polypeptide receptor and glucagon-like peptide receptor agonist. A two-phase, double-blind, randomized controlled trial involving adults with moderate-to-severe obstructive sleep apnea and obesity (BMI > 30) was conducted with tirzepatide versus placebo (80). Subjects received weekly injections of tirzepatide, 10 to 15 mg or placebo for 52 weeks. The primary end point was the change in the apnea-hypopnea index.
In trial one, subjects did not receive PAP applications, and in trial two, subjects received PAP therapy at baseline. In trial one, results showed that the mean change in apnea-hypopnea index at week 52 was -25.3 events per hour with tirzepatide and -5.3 events per hour with placebo. The estimated treatment difference was -20.0 events per hour (P< 0.001). In trial two, the mean change in apnea-hypopnea index at week 52 was -29.3 events per hour with tirzepatide and -5.5 events per hour with placebo, with an estimated treatment difference of -23.8 events per hour (P< 0.001). There were significant improvements in secondary end points with tirzepatide, including changes in hypoxic burden, patient-reported sleep impairment and disturbance, high-sensitivity C-reactive protein concentration, and systolic blood pressure. Adverse events with tirzepatide included mild to moderate gastrointestinal disturbance.
The authors concluded that up to 50.2% of patients receiving tirzepatide lost sufficient weight to meet the secondary end point criteria of fewer than 15 AHI per hour and ESS score of less than 10 points, making them eligible for PAP discontinuation. Weight loss from tirzepatide must be maintained over time, along with reasonable regular exercise and a balanced diet, to continue experiencing a benefit for sleep apnea.
The long-term health consequences of COVID-19 remain unclear. A study of 1733 of 2469 discharged patients with confirmed COVID-19 in Wuhan, China, between January 7, 2020 and May 29, 2020 showed that patients had a median age of 57.0 (IQR 47.0-65.0) years, and 897 (52%) were men (56). At 6 months after acute infection, COVID-19 survivors mainly complained of fatigue or muscle weakness (63%, 1038 of 1655) and sleep difficulties (26%, 437 of 1655) along with anxiety or depression.
In a study of 1240 adult participants living in a state of COVID-19-induced nationwide lockdown conducted in the Middle East, researchers found that increased levels of anxiety and depressive symptoms negatively influenced sleep health (01). Nearly half reported short sleep duration, and anxiety and depressive symptoms were associated with poor sleep health outcomes.
One of the largest clusters of COVID-19 infections was observed in Italy. The population was forced to home confinement, increasing the risk for insomnia. Through a cross-sectional online survey in an adult population (≥18 yrs), the authors collected information from April 1, 2020 to May 4, 2020 on insomnia severity, depression, anxiety, sleep hygiene behaviors, dysfunctional beliefs about sleep, circadian preference, emotional regulation, cognitive flexibility, perceived stress, health habits, self-report of mental disorders, and variables related to individual differences in life changes due to the pandemic's outbreak (15). They found that out of 1989 persons (38.4 ± 12.8 yrs), the prevalence of clinical insomnia was 18.6%. Insomnia severity was associated with poor sleep hygiene behaviors, dysfunctional beliefs about sleep, self-reported mental disorder, anxiety, and depression.
In another study conducted in France, the prevalence of sleep problems significantly decreased during the last weeks of pandemic-imposed confinement (16). One quarter of the population reported that their sleep was better one month after the end of confinement. Sleep improvement was reported more often by women and people younger than 65 years of age. The study also showed that the possibility of recovering good sleep largely depends on the type of sleep disorder. The decrease in sleep problems occurred mainly among people with mild sleep problems during confinement.
In a study of narcolepsy type 1 patients between April 10, 2020 and May 15, 2020, the authors investigated 50 patients over 18 years of age (40% males) under stable long-term treatment (100). Three groups were studied: unchanged working schedule, forced working or studying at home, and lost occupation. Current sleep-wake habit and symptom severity were compared with pre-lockdown assessments in the three patient groups. The authors found that the lost occupation group exhibited no significant differences compared with pre-pandemic assessments. Patients with unchanged schedules reported more nocturnal awakenings, and narcolepsy type 1 patients working or studying at home showed an extension of nocturnal sleep time, more frequent daytime napping, improvement of daytime sleepiness, and a significant increase in body mass index. Sleep-related paralysis or hallucinations, automatic behaviors, cataplexy, and disturbed nocturnal sleep did not differ. The authors concluded that narcolepsy type 1 patients working or studying at home increased nocturnal sleep time and daytime napping, thus, ameliorating daytime sleepiness despite experiencing an increase in weight.
Some authors have raised the need to conduct more research on narcolepsy as a side effect of COVID-19 vaccines. This concern became more acute with the revelation that the GlaxoSmithKline AS03 adjuvant or other strong adjuvants may be used in the development of COVID-19 vaccines. This adjuvant was used in vaccines associated with narcolepsy in Europe 10 years ago. At the time, wild-type infections were also occurring in Europe, which might have contributed to the development of narcolepsy. The authors concluded that the benefits of the COVID-19 vaccine far outweigh the risks (85).
Some COVID‐19 patients suffer so-called “happy hypoxia” in which complaints of dyspnea and observable signs of respiratory distress are absent despite hypoxemia. COVID‐19 can cause profound hypoxemia with near normal arterial carbon dioxide levels due to ventilation/perfusion ratio maldistribution and shunt. Some individuals with COVID‐19‐induced hypoxemia experience breathing discomfort but others do not; these latter patients have been labeled as having “happy hypoxia,” a term that trivializes the pathology; “silent hypoxemia” would be more appropriate (113). It is not known how silent hypoxemia affects sleep apnea patients, although one can assume that the condition could become decompensated in severe cases of sleep apnea. Monitoring for silent hypoxemia should be recommended for sleep apnea patients contracting the COVID-19 infection, particularly in the absence of symptoms.
In a study of adult participants with positive COVID-19 ribonucleic acid polymerase chain reaction diagnostic results, 443 participants (9.5%) with sleep apnea had an increased all-cause mortality rate (11.7%) compared with sleep apnea controls (6.9%) (P = 0.001; odds ratio = 1.79; 95% confidence interval = 1.31–2.45) (20). Associations were somewhat attenuated after adjusting for body mass index class and diagnoses associated with sleep apnea. The results of this U.S. healthcare system–based analysis identify sleep apnea as a risk factor for COVID-19 mortality, highlighting the need for close monitoring of patients with sleep apnea who become infected. The authors conclude that research is warranted to understand whether sleep apnea–related hypoxemia, endothelial dysfunction, coagulopathy, inflammation, and cardiac dysfunction contribute to the excessive COVID-19 morbidity and mortality observed in obese individuals at risk for sleep apnea.
Pregnancy may be associated with altered breathing during sleep. In the third trimester of pregnancy, reduced functional respiratory residual capacity due to weight gain and changes in the shape of the diaphragm and thorax can alter respiratory function and increase the incidence and severity of sleep-disordered breathing. Up to 10% of pregnant women are at risk for development of sleep apnea (99). The condition may lead to arterial hypertension and endothelial dysfunction.
Preeclamptic toxemia is characterized by hypertension, proteinuria, and edema. Preeclampsia may affect 7% to 10% of all pregnancies in the United States (48) and constitutes a major cause of fetal and maternal morbidity and mortality. The likely triggering event in preeclampsia is placental ischemia (44), which may precipitate the release of a cascade of active factors from the placenta that generate profound effects on the maternal cardiovascular system causing hypertension and endothelial dysfunction.
Sleep apnea in pregnancy may cause placental hypoxia. It has been proposed that at the very least, sleep apnea is a significant contributing factor for the development of preeclampsia, in particular in pregnant women who are vulnerable for the occurrence of sleep apnea (134; 97). Overweight women and women with metabolic syndrome are at particular high risk for development of sleep apnea and in consequence preeclampsia.
Overnight ambulatory unattended polysomnography is a reasonable test to use in the third trimester of pregnancy at home in women who snore, report sleepiness, and show hypertension. The aim would be to objectively demonstrate and measure clinically significant sleep apnea. A sleep apnea-hypopnea index of five per hour of sleep or more might lead to further testing in the sleep laboratory or the indication of continuous positive airway pressure treatment.
In a prospective study of 12 pregnant women, Guilleminault and associates concluded that early application of nasal CPAP in pregnant women alleviated sleep-related breathing disturbances but was not sufficient to prevent negative pregnancy outcomes (49). Obesity and prior preeclampsia appeared to be important risk factors and were associated with the worst complications. In a parallel study, Poyares and colleagues indicated that in pregnant women with hypertension and chronic snoring, nasal CPAP use during the first eight weeks of pregnancy combined with standard prenatal care was associated with better blood pressure control and improved pregnancy outcomes (101).
Sleep apnea should always be reported to the anesthesiologist prior to any intervention requiring central anesthesia. Medical clearance by a sleep specialist may be desirable for patients with moderate to severe sleep apnea.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Antonio Culebras MD FAAN FAHA FAASM
Dr. Culebras of SUNY Upstate Medical University at Syracuse has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 06, 2026
Sleep Disorders
Jul. 05, 2026
Sleep Disorders
Jul. 03, 2026
Sleep Disorders
Apr. 10, 2026
Sleep Disorders
Apr. 05, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 29, 2026