Peripheral Neuropathies
Clinical evaluation of peripheral neuropathies
Jul. 16, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Small fiber neuropathy is a polyneuropathy affecting the small unmyelinated and thinly myelinated sensory and autonomic nerve fibers. Symptoms typically include numbness, paresthesias, and neuropathic pain and can sometimes include symptoms of autonomic dysfunction. Physical examination may demonstrate loss of small fiber modalities on sensory testing but may be normal, often leading physicians to presume a psychiatric source to patient symptoms. First-line diagnostic tests for sensory symptoms, including EMG/NCS testing and MRI, are normal. Skin biopsy for epidermal nerve fiber density is currently considered the best test for confirming a small fiber neuropathy diagnosis. Laboratory testing is recommended to evaluate for underlying causes for small fiber neuropathy, although in many cases no cause is identified, and the neuropathy is deemed idiopathic. Medications and nonpharmacologic therapies can be used to treat neuropathic pain and autonomic symptoms.
• Small fiber sensory neuropathy often presents with numbness, paresthesias, or pain due to abnormal somatic unmyelinated or small myelinated nerve function. | |
• Autonomic symptoms and subclinical autonomic dysfunction are common with small fiber neuropathy. | |
• Although there is no gold standard diagnostic test, skin biopsy demonstrating reduced epidermal nerve fiber density, in the appropriate clinical setting, is most often used to confirm small fiber neuropathy diagnosis. | |
• Laboratory testing to evaluate for conditions causative of small fiber neuropathy should include those assessing for diabetes, Sjogren syndrome, celiac disease, vitamin deficiencies and toxicities, amyloidosis, and in some cases, genetic disorders. | |
• Frequently, no cause for small fiber neuropathy is identified, and it is idiopathic. | |
• Symptomatic management of small fiber neuropathy includes medications and nonpharmacologic treatments for pain and autonomic symptoms. |
|
• Small fiber neuropathy often presents with numbness, paresthesias, and pain. | |
|
• Presentation is usually length-dependent and slowly progressive but there can be non-length-dependent and acute or subacute presentations. | |
|
• Autonomic symptoms may accompany the sensory manifestations of small fiber neuropathy. |
Patients with small fiber neuropathy typically present with symptoms of numbness, paresthesias, and neuropathic pain. Pain is often described as burning, stabbing, or electrical in quality. Although symptoms most often begin insidiously and worsen slowly, variants occur with an acute or subacute onset. Typically, symptoms begin in a length-dependent fashion, first affecting the toes and feet, then progressing to affect the lower legs and hands, but non-length dependent, asymmetric, and patchy presentations often occur (34; 75). Other symptoms can include itching (06), muscle twitching or fasciculations (70), and muscle cramping (48). Although weakness should not occur with pure small fiber sensory loss, patients often will describe easy fatigability in their muscles or a change in endurance compared to their previous function (54).
The triad of depressed mood, abnormal sleep, and pain in small fiber sensory neuropathy may create a vicious cycle, augmenting neuropathic pain perception, which can further worsen mood and sleep. Symptoms of depression and anxiety are common among patients with small fiber neuropathy and correlate with pain severity (11).
Physical exam findings in small fiber neuropathy are restricted to the sensory component of the neurologic examination, although physical exam may be normal on direct testing. Common sensory findings include decreased sensation to light touch, pinprick, and temperature, most often in a length-dependent pattern; non-length-dependent, focal, or patchy patterns may occur (13). Hyperesthesia or allodynia, rather than sensory loss, may occur in affected areas. Muscle strength should be normal, although some patients may elaborate weakness or have pain-limited strength testing complicating the neurologic exam. Vibratory sensation and deep tendon reflexes are typically normal, although in some cases there may be mild loss of vibration at the toe and ankle jerk reflexes may be depressed or absent.
Vasomotor dysregulation in small fiber sensory neuropathy can cause transient changes in distal extremity skin color and temperature, which may be associated with worsening of neuropathic pain, sometimes referred to as “erythromelalgia.” Raynaud phenomenon may be present. Abnormally increased, decreased, or absent sweating are features of sudomotor dysfunction. Proximal excessive sweating in the setting of impaired distal sweating is a common pattern. Length-dependent hair loss and trophic skin and nail changes may also occur.
In cases where autonomic function is more severely affected, patients may demonstrate resting tachycardia or orthostatic hypotension on orthostatic vital sign testing. Other autonomic symptoms can include constipation, postprandial nausea and bloating, urinary retention, sexual dysfunction, and dry eyes or mouth.
The prognosis and disease course for small fiber neuropathy depends on the underlying cause. In cases where a treatable source for the neuropathy is identified and addressed, symptoms and epidermal nerve fiber density can improve. Most patients with small fiber neuropathy from diabetes or impaired glucose tolerance have stable or slowly worsening symptoms over time, although one study reported improvement in impaired glucose tolerance neuropathy with an aggressive regimen of diet and exercise (64). Patients with idiopathic small fiber neuropathy have variable disease course. A subset of patients appear to have a monophasic illness that improves over months to years. Many have stable or slowly worsening symptoms over time. In most cases, the pathology remains restricted to small fiber nerve involvement, but in some cases, large fiber neuropathy may occur over time. In cohort studies of patients with small fiber neuropathy, 25% to 30% of patients progress to large fiber involvement of neuropathy over time (23; 43).
• There are many possible etiologies underlying small fiber neuropathy, including metabolic, inflammatory, toxic, and genetic causes. | |
• Diabetes and impaired glucose tolerance is the most common cause of small fiber neuropathy. | |
• Toxic small fiber neuropathy can occur with chemotherapy, some antibiotics, and excessive alcohol use. | |
• A number of inflammatory or autoimmune conditions are associated with small fiber neuropathy, including Sjogren syndrome, lupus, inflammatory bowel disease, and celiac disease. | |
• Increasingly, genetic causes of small fiber neuropathy are being identified. | |
• Despite extensive testing, often no cause for small fiber neuropathy is identified and is, thus, deemed idiopathic. |
There are several possible conditions associated with small fiber sensory neuropathy, and mechanisms of disease are often incompletely understood. A suggested list of laboratory testing in the evaluation of small fiber neuropathy is shown in Table 1.
Metabolic | |
• Hemoglobin A1c | |
• Vitamin B12 and methylmalonic acid (MMA) | |
• Copper (if signs of myeloneuropathy or risk factors for malabsorption) | |
Inflammatory/Autoimmune | |
• Sjogren and lupus testing - antinuclear antibody (ANA), extractable nuclear antigen (ENA), anti-RO (SSA), and anti-La (SSB) | |
• Celiac antibodies - gliadin, tissue transglutaminase, and/or endomysial antibodies | |
• Sedimentation rate (ESR), C-reactive protein (CRP), antineutrophil cytoplasmic antibody (ANCA) if clinical features are suggestive of vasculitis | |
Infectious | |
• HIV | |
• Hepatitis B | |
• Hepatitis C | |
Paraneoplastic | |
• Serum protein electrophoresis with immunofixation, quantitative immunoglobulins, and free light chains | |
• Antibody testing - ANNA-1, CRMP-5, P/Q VGCC, PCA-2, LGI1, CASPR2 | |
Toxic | |
• Vitamin B6 (if taking vitamin supplementation) | |
• Heavy metals screen (in appropriate clinical context) | |
Genetic – consider for younger patients, those with family history of neuropathy | |
• TTR gene | |
• SCN9A, SCN10A, SCN11A | |
• Hereditary sensory and autonomic neuropathies (HSAN) | |
• GLA if other clinical features of Fabry disease | |
The disorder is localized to the somatic small nerve fibers (Aδ and C fibers), with or without clinical autonomic involvement. The mechanism of small fiber dysfunction probably varies depending on etiology. Vasomotor and sudomotor signs and symptoms can be attributed to neurogenic dysregulation of small blood vessel caliber and sweat gland function mediated by the autonomic system.
In diabetic neuropathy, the most common cause of small fiber sensory neuropathy, the main hypotheses for neuropathic dysfunction are the polyol pathway, glycation, reactive oxygen species, and altered protein kinase C activity. Causes for diabetic small fiber sensory neuropathy pain are incompletely understood (39). The relationship between impaired glucose tolerance/prediabetes and small fiber sensory neuropathy is less firmly defined and remains somewhat controversial, although the association is established in a number of studies (65; 17). Obesity and hypertriglyceridemia (metabolic syndrome) are more common in patients with small fiber neuropathy (68; 43).
Toxic small fiber sensory neuropathy is a group of disorders including neuropathies caused by exposure to environmental agents or prescribed medications that are toxic to the small fiber nerves. Alcohol may cause small fiber sensory neuropathy, although in many cases, it has large fiber involvement (51). Comorbid vitamin deficiencies often complicate alcoholic neuropathy. Certain chemotherapeutic agents are prone to causing sensory neuropathy with prominent small fiber sensory involvement, including vinca alkaloids (vincristine), paclitaxel and docetaxel, cisplatin, carboplatin, oxaliplatin, and bortezomib. Immune checkpoint inhibitor chemotherapy has been reported to cause a range of inflammatory neurologic disorders, including small fiber neuropathy (15). Please see the dedicated MedLink chapter reviewing toxic peripheral neuropathies.
Amyloidosis also can cause a small fiber polyneuropathy, particularly in the early stages. Amyloid related to light chain deposition (AL amyloidosis) or amyloid in transthyretin (TTR) amyloidosis (hereditary or wild type) both may present with small fiber sensory neuropathy with autonomic involvement. There are approved small interfering RNA (siRNA) and antisense oligonucleotide (ASO) therapies for hereditary TTR amyloid polyneuropathy (01; 02; 04; 10); therefore, screening for TTR gene mutations should be considered in any patient with small fiber neuropathy with carpal tunnel, cardiomyopathy, or a family history of similar disorder.
Small fiber neuropathy can occur in a number of autoimmune or inflammatory disorders. Isolated small fiber sensory neuropathy without large fiber peripheral neuropathy is common in Sjogren syndrome (60). Patients with dryness of the mouth or eyes for greater than 3 months (sicca symptoms) should be evaluated for this syndrome with Sjogren serologies, and in some cases, lip biopsy (35). Small fiber neuropathy can also be seen in systemic lupus erythematosus (25) and less often, sarcoidosis (26; 67). Described in some patients with idiopathic small fiber neuropathy are antibodies to trisulfated heparan disaccharide (TS-HDS), fibroblast growth factor receptor-3, and Plexin-D1, suggesting a possible autoimmune etiology in these cases (47), although the specificity and management of neuropathies with these antibodies are yet to be clarified, as a high percentage of patients with idiopathic small fiber neuropathy are reported to be positive, the false-positive rate in disease controls is not small, and there is not a clear correlation with abnormal epidermal nerve fiber density (69; 53). A double blind, placebo-controlled trial of intravenous immunoglobulin in patients with TS-HDS and FGFR3- antibodies showed no benefit (31).
Small fiber sensory neuropathy can be associated with ulcerative colitis and Crohn disease. A retrospective analysis showed a frequency of small fiber sensory neuropathy in 18% of patients with inflammatory bowel disease (32). Another series reported 38.7% of patients with inflammatory bowel disease meeting criteria for peripheral neuropathy (61).
Uncommonly small fiber or autonomic neuropathy presents as a paraneoplastic phenomenon, most often in association with breast, ovarian, and lung cancer. Paraneoplastic antibodies may be present, including anti-Hu or ganglionic acetylcholine receptor antibodies.
Celiac disease may cause small fiber sensory neuropathy or sensory ganglionopathy, as evidenced by reduced intraepidermal nerve fiber density with frequent facial involvement and, at times, non-length-dependent patterns (05). One series reported 38.9% of celiac disease patients meeting peripheral neuropathy criteria (61).
HIV infection can cause peripheral neuropathy, and in some cases, small fiber only neuropathy with prominent pain. The risk for neuropathy in HIV is greater in advanced disease with greater viremia and immunosuppression and, thus, it has become less common with widespread use of antiretroviral therapy. Some antiretroviral agents including stavudine, didanosine, and nevirapine are associated with peripheral neuropathy, although most of the newer agents much less likely to have the same neurotoxicity.
Peripheral neuropathy, including small fiber neuropathy, is also seen in association with synucleinopathies, including Parkinson disease, multiple system atrophy (MSA) and Lewy body dementia (73). Skin biopsy can demonstrate phosphorylated α-synuclein deposits in epidermal nerve fibers in patients with synucleinopathies (30).
Hereditary small fiber sensory neuropathy was traditionally considered a rare cause of the disease, but with increased accessibility to genetic testing, it is being diagnosed in more patients. A number of studies have reported variants in SCN9A, SCN10A, and SCN11A genes in 10% or more of patients in cohorts with idiopathic small fiber neuropathy (22; 42; 38; 16). Recently identified variants in the TRPA1 gene have also been associated with small fiber neuropathy and pain syndromes (50). Genes associated with hereditary sensory and autonomic neuropathy (HSAN) can also cause small fiber predominant sensory loss, including SPTLC2 (HSAN type I), IKBKAP (HSAN type III), and NGF (HSAN type V) (09). RFC1 repeat expansions are a common cause of idiopathic sensory neuropathy; a small percentage of patients with pure small fiber neuropathy are described to also have biallelic RFC1 gene expansions (66). Fabry disease, an X-linked lysosomal storage disease with frequent kidney, cardiac, and dermatological involvement due to the accumulation of glycolipids, also can cause small fiber neuropathy in affected patients as well as some female carriers. However, screening for Fabry disease in patients with an isolated small fiber sensory neuropathy without the expected systemic dysfunction is of low diagnostic yield (19). Patients with mitochondrial DNA mutations may also present with small fiber neuropathy. Other genetically inherited systemic diseases that can include small fiber neuropathy include porphyria, hereditary transthyretin amyloidosis, Fragile X syndrome, and Ehlers-Danlos syndrome (09). Genetic testing in the evaluation of small fiber neuropathy should be strongly considered, particularly in early-onset cases (52).
Other conditions that have been described in association with small fiber neuropathy include morbid obesity (41), monoclonal gammopathy of uncertain significance (MGUS), hypothyroidism, and other nutritional deficiencies.
Although there are many potential causes for small fiber neuropathy, in many cases the cause is idiopathic. In one study of 921 patients with confirmed small fiber neuropathy, a cause for the neuropathy was identified in only 47% of patients. The most common causes included autoimmune disorders, sodium channel gene mutations, diabetes and impaired glucose tolerance, and vitamin B12 deficiency (18). Notably, despite extensive testing, approximately half of patients with small fiber neuropathy remain idiopathic (43).
Large fiber polyneuropathy may have similar symptoms to small fiber neuropathy and often coexists. Large fiber polyneuropathy will typically demonstrate greater loss of strength and vibratory sensation on physical exam, show depressed deep tendon reflexes, and show abnormalities on electrodiagnostic testing.
Fibromyalgia may cause similar symptoms to small fiber neuropathy, with myalgias, easy fatigability, and paresthesias. Many series have demonstrated a prevalence of small fiber neuropathy close to 50% in patients previously diagnosed with fibromyalgia (28; 36).
Erythromelalgia is a disorder that can also cause skin color changes and neuropathic quality pain in the legs and feet. The clinical entity of erythromelalgia likely encompasses a few pathologically different disease states. There is an association with polycythemia vera; therefore, if this diagnosis is suspected, a blood count is indicated. Some cases of erythromelalgia associate with sodium channel mutations (SCN9A and others), and in these cases, the clinical phenotype can overlap significantly with small fiber neuropathy. One study demonstrated abnormal small fiber nerve function in many patients diagnosed with erythromelalgia (49).
Complex regional pain syndrome (CRPS), previously named reflex sympathetic dystrophy, is another condition that can cause sensory symptoms, vasomotor changes, and pain. Although the condition of CPRS is physiologically separate from small fiber neuropathy, they can be clinically difficult to distinguish. Some series have described skin biopsy abnormalities in these patients (55).
Patients with hypermobility type Ehlers Danlos syndrome also can have prominent pain, paresthesias, and autonomic symptoms. One series described abnormal skin biopsy demonstrating small fiber neuropathy to be common in Ehlers Danlos syndrome (08). Whether small fiber neuropathy is a component of Ehler Danlos or a disease mimic is not clear.
Some patients diagnosed with postural orthostatic tachycardia syndrome (POTS) have low epidermal nerve fiber density (37). Evaluating for underlying small fiber neuropathy in patients with symptoms of postural orthostatic tachycardia syndrome may be considered.
Patients with prominent bladder and pelvic pain, including interstitial cystitis, may also have abnormal nerve fiber density on skin biopsy (72).
Other causes of neuropathic pain, numbness, and paresthesias can include lumbar or cervical spinal stenosis or radiculopathy, cervical or thoracic myelopathy, or CNS demyelinating disease, such as multiple sclerosis. Patient history, physical exam, and testing results should guide the clinician on when it is appropriate to pursue imaging of the spine and brain when a workup for small fiber neuropathy fails to yield a diagnosis.
The various underlying causes of small fiber neuropathy are discussed in the Biological basis section above.
|
• Small fiber neuropathy is diagnosed using a combination of history, physical exam, and diagnostic testing modalities. | |
|
• Electrodiagnostic testing (EMG/NCS) is normal in pure small fiber sensory neuropathy. | |
|
• Small fiber neuropathy diagnosis can be confirmed using skin biopsy to evaluate epidermal nerve fiber density or with the quantitative sudomotor axon reflex test (QSART) testing. | |
|
• Many patients with typical neuropathy symptoms and known risk factors (eg, diabetes) may not need confirmatory testing to establish a clinical diagnosis of small fiber neuropathy. |
Although there is no gold standard test to diagnose small fiber sensory neuropathy, the diagnosis can usually be established using a combination of patient history, physical exam, electrodiagnostic testing, and skin biopsy for epidermal nerve fiber density testing. Published criteria for small fiber neuropathy emphasize the importance of combining both clinical signs and symptoms with confirmatory diagnostic testing (14; 40).
When there is reasonable suspicion for peripheral sensory dysfunction, nerve conduction studies and electromyography (NCS/EMG) are the first step in evaluating for peripheral neuropathy. Patients with small fiber neuropathy will typically have normal NCS/EMG testing. For many patients who have classic symptoms of small fiber sensory neuropathy, particularly those with a history of diabetes or chemotherapy exposure, and normal NCS/EMG testing, the findings on history and exam are sufficient for diagnosis without further diagnostic testing.
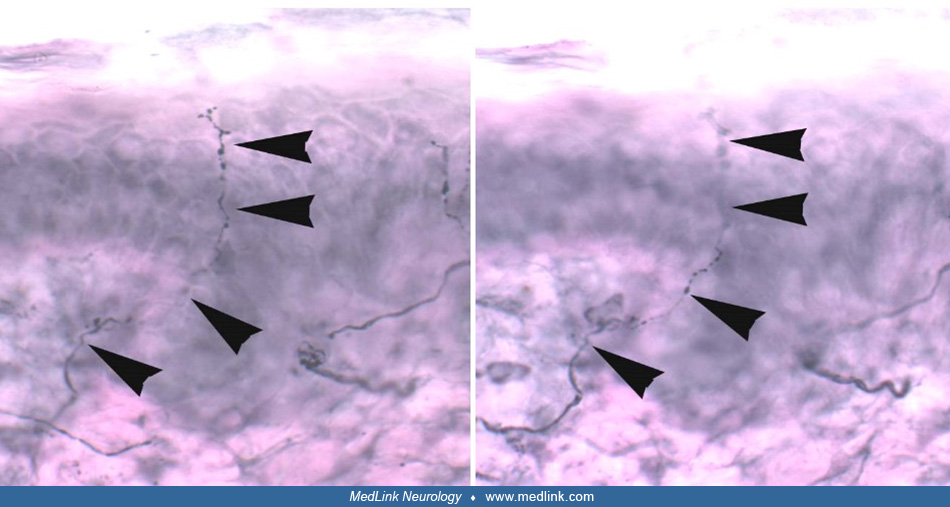
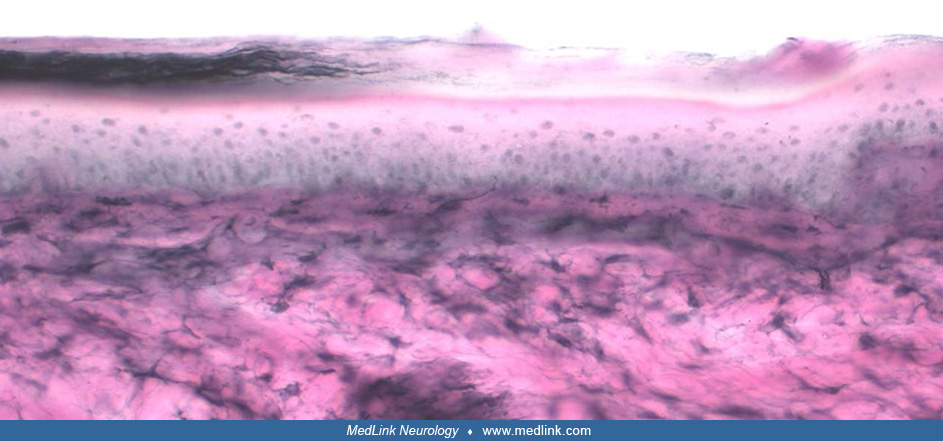
Further confirmation of small fiber neuropathy is possible using skin biopsy for intraepidermal nerve fiber density evaluation. The procedure for skin biopsy involves a 3 mm punch biopsy taken from a number of possible sites, but most often from the foot, distal leg, or thigh sites to establish length dependent pathology. The tissue is placed in either periodate-lysine-paraformaldehyde (PLP) or Zamboni fixative. Staining with antiprotein gene product 9.5 antibody (PGP 9.5) allows quantification of the density of small nerve fibers in the skin layer and assessment of morphological changes in the small fiber nerves (71; 45; 44). Normative reference values are available stratified by decade of life (46). Skin biopsy for intraepidermal nerve fiber density is included in a 2009 practice parameter on the evaluation of peripheral neuropathy (21).
In addition to staining and quantification of the intraepidermal nerve fiber density, skin biopsy can be assessed for the nerve fiber density of sweat glands. Sweat glands, which are found in the deep dermal and subcutaneous layers of skin, are innervated by unmyelinated autonomic nerve fibers. Assessing for the sweat gland nerve fiber density can increase the sensitivity of skin biopsy for small fiber neuropathy and assess for autonomic neuropathy (29).
Although skin biopsy is primarily performed to establish a diagnosis of small fiber neuropathy rather than to find the cause of the neuropathy, in occasional cases, the cause of the neuropathy can be identified on biopsy. Skin biopsy may detect amyloid deposits establishing amyloidosis (light chain or transthyretin) as the cause of the neuropathy. Occasionally, evidence of vasculitis or sarcoidosis may also be detected by skin biopsy, although the yield is considered low when evaluating for these specific disorders. In cases in which an underlying neurodegenerative disorder in suspected, staining for phosphorylated alpha synuclein can accompany epidermal nerve fiber density testing (30).
Corneal confocal microscopy is another method for measuring nerve fiber density in the cornea. It has been demonstrated to be a sensitive marker for detecting diabetic peripheral neuropathy (03; 74). A comparison of corneal confocal microscopy to intraepidermal nerve fiber density suggested that skin biopsy was a more accurate test and preferred by patients (59).
Thermal and vibratory thresholds obtained with quantitative sensory testing (QST) can be used for diagnosis of small fiber neuropathy but cannot distinguish sensory dysfunction of central origin from peripheral nervous system localization and may be abnormal in patients with psychogenic disorders. Quantitative sensory testing is still used at times for research purposes (24).
Autonomic testing may be abnormal in small fiber sensory neuropathy patients, even in the absence of overt autonomic dysfunction. A battery of autonomic tests may be considered in patients with small fiber sensory neuropathy (21). The most sensitive tests are the thermoregulatory sweat test and the quantitative sudomotor axon reflex test (QSART). QSART correlates moderately well with skin biopsy measures. Sympathetic skin response and heart rate variability with deep breathing are simple tests that can be performed using routine electrodiagnostic testing equipment, but both have lower sensitivity and are more commonly abnormal in later stages of autonomic dysfunction. The thermoregulatory sweat test is only available in a few specialized centers.
A simple bedside test for small fiber neuropathy can also include assessment for wrinkling of the fingers with water immersion. In normal skin of the distal fingers, water triggers increased sympathetic firing and vasoconstriction of glomus bodies, creating wrinkling. In small fiber neuropathy and sympathetic fiber loss, wrinkling will not occur (57).
Associated conditions may be identified in up to 50% of small fiber sensory neuropathy cases, with important treatment implications. A significant number of patients remain idiopathic, but diabetes mellitus is common (20; 43). Aside from diabetes screening, other lab testing to consider in patients presenting with small fiber neuropathy includes evaluation for autoimmune conditions, vitamin deficiencies, monoclonal gammopathies, celiac disease, HIV, and hepatitis C. In patients with young age of onset or a family history of similar symptoms, genetic testing for sodium channel mutations and other hereditary sensory and autonomic neuropathies should be considered. Table 1 lists recommended laboratory testing to consider in evaluating patients with small fiber neuropathy.
|
• Treatment of an underlying cause of small fiber neuropathy can result in improved symptoms. | |
|
• Symptomatic management of pain and autonomic symptoms is a prominent part of treating patients with small fiber neuropathy. |
Supportive measures for management of peripheral neuropathy are separately discussed in Peripheral neuropathies: supportive measures and rehabilitation.
In patients diagnosed with small fiber neuropathy in whom an underlying medical cause can be identified, treatment of the associated condition may result in improvement in severity of neuropathy symptoms and in epidermal nerve fiber density measures.
Patients with impaired glucose tolerance associated with small fiber neuropathy can see improvement in epidermal nerve fiber density with a program of diet and exercise to improve blood glucose (63).
Patients with toxic small fiber neuropathy due to chemotherapy or other exposures typically have stabilization of symptoms after the toxic agent is discontinued and often partial improvement in the months following, although some neuropathy symptoms often persist indefinitely.
Patients with an immune-mediated cause of small fiber neuropathy identified may benefit from immunotherapy treatment, although there is little published research to support this approach. There have been no randomized controlled trials of immunotherapy for small fiber neuropathy associated with Sjogren syndrome but there have been a number of small case series describing improvement in neuropathy symptoms with intravenous immunoglobulin (IVIG) and subcutaneous immunoglobulin therapy (58). Patients with other autoimmune disorders, including lupus and inflammatory bowel disease, may benefit from immunotherapy but there is significant practice variability amongst even neuropathy specialists. A placebo-controlled trial of intravenous immunoglobulin for patients with small fiber neuropathy and TS-HDS or FGFR-3 antibodies showed no benefit (31).
The treatment of idiopathic small fiber neuropathy is focused on symptom management. A randomized controlled trial of intravenous immunoglobulin (IVIG) in idiopathic small fiber neuropathy showed no benefit (27). It is notable that patients with autoimmune diagnoses were excluded from this study.
Symptomatic treatment for neuropathic pain is addressed in other clinical summaries in MedLink Neurology. A panel of experts published guidelines for the treatment of painful diabetic neuropathy (07), and similar treatment strategies can be applied for painful small fiber sensory neuropathy. Medications often used to treat pain in small fiber neuropathy include gabapentin, pregabalin, tricyclic antidepressants, duloxetine, and venlafaxine. Other options include carbamazepine, topiramate, mexiletine, phenytoin, and lacosamide. Lacosamide has been investigated for use in treating pain in patients with sodium channel mutations (12). Topical medications, including lidocaine, capsaicin, and compounded formulations may have some added benefit when pain is localized. Opiates are increasingly avoided with concern for long-term hyperalgesic effects. Other nonmedication treatment options include transcutaneous electrical nerve stimulation (TENS) and spinal cord stimulator in refractory cases. A study showed significant benefit of high frequency spinal cord stimulation in patients with diabetic peripheral neuropathy (56). Some patients find benefit from complementary and alternative medicine approaches to pain, including acupuncture. Ongoing clinical trials are investigating novel therapeutics targeting sodium channels and other targets in the treatment of pain in association with small fiber neuropathy.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Rebecca E Traub MD
Dr. Traub of the University of North Carolina, Chapel Hill received research support from Alnylam Pharmaceuticals, Ionis Pharmaceuticals, Pharnext, Argenx, Immunovant, and Takeda as principal investigator and served on advisory boards for Argenx and Intellia.
See Profile
Louis H Weimer MD
Dr. Weimer of Columbia University received a consultant honorarium from Roche and Ovid Therapeutics.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jul. 16, 2026
Peripheral Neuropathies
Jul. 14, 2026
Peripheral Neuropathies
Jun. 26, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Peripheral Neuropathies
Jun. 11, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
Peripheral Neuropathies
May. 12, 2026