






Sleep Disorders
Sleep-related urologic dysfunction
Jul. 06, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Spinal meningioma is a rare tumor usually presenting with chronic progressive radicular or myelopathic symptoms and back pain. The authors discuss the clinical manifestations, diagnosis, and management of this tumor. Surgical resection is the treatment of choice for patients with neurologic deficits. Some patients may benefit from the radiosurgery for recurrent or partially resected spine tumors.
|
• Spinal meningiomas are most frequently found in the thoracic area and are histologically grade 1 tumors over 90% of the time. | |
|
• Surgical intervention should be considered in most cases, particularly when patients present with neurologic deficits. | |
|
• The rates of overall complication, tumor recurrence, and poor functional outcome were 9.2%, 7.6%, and 5%, respectively, in one large case series. Age, revision surgery, tumor recurrence, and intervention greater than 12 months after symptom onset were identified as independent predictors of poor functional outcome. | |
|
• Radiotherapy should be considered after subtotal resection or meningioma recurrence. Systemic therapies have yet to show consistent benefit in intracranial meningiomas and have not been studied in the spinal meningioma population. |
In 1887 Horsley performed the first reported successful removal of an intradural, extramedullary tumor (38). With the support of Sir William Gowers, Horsley removed a "fibromyxoma" overlying the spinal cord at the T4 level. Postoperatively, the patient developed a debilitating pain syndrome but later experienced a full neurologic recovery. In the following 50 years, pioneering neurosurgeons such as Elsberg, Frazier, and Cushing took particular interest in extramedullary tumors, recognizing their frequently benign nature and often dramatic recovery from profound neurologic deficit (35; 31; 23). The term "meningioma" was introduced by Cushing in his 1922 Cavendish lecture as a simple designation and is now universally employed. With the development of modern imaging, neuroanesthesia, and microsurgical techniques, Cushing's description of "one of the most gratifying of all operative procedures" is now the expected in most patients with intradural, extramedullary spinal tumors such as meningiomas (68; 59; 11; 60; 17; 91).
|
• Spinal meningiomas are slow-growing tumors that progress over months to years. | |
|
• Time from symptom onset to intervention for spinal meningioma will hopefully shorten as MRI has become more readily available. |
Intradural, extramedullary tumors generally cause a chronic compression syndrome. Symptomatology is due to displacement of the spinal cord and adjacent nerve roots and associated venous engorgement. Slow growth, over months or years, allows the cord to be gradually displaced and deformed. This produces an atrophic-appearing cord with remarkable preserved neurologic function relative to the degree of cord compression.
Initial presenting symptoms vary depending on tumor location. However, the most common presenting symptoms are weakness, gait changes, and back or radicular pain. Bowel or bladder dysfunction has also been frequently reported at presentation (70; 97).
Meningiomas at a high cervical level or the foramen magnum may produce quadriparesis, lower cranial nerve involvement, dysphagia, and respiratory disturbances. Horner syndrome, due to interference with the cervical sympathetic chain, may occur. Interestingly, disturbances in facial sensation may be present due to compression of the descending sensory root of the trigeminal nerve.
The duration of clinical symptomatology is usually of medium range. Of 174 spinal meningiomas reported by Solerno, 117 patients had a clinical history ranging from 6 months to 3 years (91). In the modern MRI era, this prodrome should be shortened if a high index of suspicion is practiced by community physicians and neurologists. In a single-center retrospective chart review of patients with spinal meningioma seen over a 30-year period, mean time from symptom onset to surgery was 8.8 months in the first 17 years of the study period compared to 6.1 months in the latter 12 years (40). This suggests a trend towards more rapid intervention.
Additionally, scans obtained for other complaints or in the trauma setting may reveal spinal meningiomas incidentally.
As spinal meningiomas are generally slow-growing tumors, long-term outcomes have been limited in studies. Management options include observation, surgical resection, and radiotherapy. Maximal safe resection is the preferred treatment strategy for symptomatic spinal meningiomas.
The neurologic morbidity of the surgical removal of tumor is directly related to the preoperative neurologic status. Patients with little or no disability preoperatively are at little risk to sustain an injury, whereas patients with more advanced neurologic dysfunction have a greater chance of remaining impaired following surgery. Long-term neurologic recovery is usually excellent (59; 60). Additionally, patients who have a shorter symptomatic interval prior to surgery had faster postoperative neurologic recovery (40).
Other complications are generally related to wound healing and perioperative fistulas. A joint neurologic and plastic surgery approach was developed to reduce the morbidity of wound closure following extensive and complicated laminectomy (102; 101).
Spinal meningiomas are almost always amenable to surgical resection and usually do not recur following radical resection. Long-term follow-ups following operations found a very low recurrence rate ranging from 1.3% to 8% (91; 40; 87).
A 60-year-old Caucasian woman presented with several months of back pain, progressive numbness, and weakness in the lower extremities. She also reported urinary urgency but denied bladder or bowel incontinence. Neurologic examination demonstrated mild spastic paraparesis with a sensory level at T10. An MRI scan with and without contrast of her thoracolumbar spine showed an extramedullary, intradural lesion at T7-8 level with diffuse contrast enhancement and moderate effacement of spinal cord. She underwent urgent decompressive surgery with laminectomy and resection of the lesion. Histopathology was consistent with a meningoepithelial meningioma. Postoperatively, she made good recovery with no residual neurologic deficits. She continued to do well several years after her surgery with no evidence of recurrence.
|
• Traumatic brain injury and radiation exposure have not been reported to be associated with spinal meningioma. | |
|
• There is some, albeit limited, evidence suggesting that spinal meningiomas are associated with breast cancer and are hormonally reactive. |
Prior radiation therapy has a well-established role in promoting growth of cranial meningiomas. This phenomenon falls into two categories: (1) those cases in which radiation was administered in high doses for the treatment of an intracranial growth, and (2) those in which low doses of scalp radiation were given (05; 90; 76). Because radiation therapy was primarily aimed to the scalp, these reported cases were primarily cranial and not spinal meningiomas. One case of cervical meningioma that developed 9 years after the radiation therapy for Hodgkin lymphoma was reported (64). Chemotherapy has also been implicated in the pathogenesis of meningioma, although a true causal relationship has not been established. One case of spinal meningioma was reported that occurred in a patient with essential thrombocythemia who had been on hydroxyurea therapy for 10 years. Paradoxically, hydroxyurea is often employed for the treatment of unresectable meningiomas (37). Traumatic brain injury has been suggested as playing at least a statistically significant role in the development of cranial meningioma in some studies; however, meta-analysis has not identified a consistent relationship between the two (103; 88). Studies have not evaluated a potential relationship between trauma and spinal meningioma.
Meningiomas arise from the endothelium, which lines the leptomeningeal spaces. Meningiomas are firmly attached to the dura and appear to be arising from it. Those tumors are probably derived from sequestered clumps of arachnoid cells that occur within normal dura. In the spinal canal, there are nests of arachnoid cells at the junction of the arachnoid and the dura where they encase the nerve roots on their passage towards the intervertebral foramina (44).
Genetics. The sporadic loss of genetic material from the long arm of chromosome 22 is thought to be critical for the initial development of meningioma in older adults (100). The locus is separate from the neurofibromatosis type 2 gene on chromosome 22 and is between the myoglobin and the c-sis proto-oncogene locus. It is likely to be a tumor suppressor gene. Progression of a meningioma to a higher grade probably requires other chromosomal changes. Similar findings were seen in whole-genome analysis of spinal meningiomas seen at a single institution over a 20-year period, where 77% of spinal meningioma DNA profiling revealed broad or complete loss of chromosome 22q (30).
The growth rate of meningiomas can be measured using a bromodeoxyuridine labeling index that will measure S phase fraction of cells. In intracranial meningiomas, a labeling index of 5% was associated with increased incidence of recurrence and an index of greater than 1% with a faster growth rate (45).
In younger patients, germline mutations in the NF2 gene are frequently seen in patients with multiple meningiomas (71). Furthermore, germline mutations in SMARCE1 predispose to the clear cell variant of intracranial meningioma in young patients, though data for whether this applies to spinal meningioma is lacking. Amongst intracranial meningiomas, some of those without NF2 mutation exhibit mutations of either AKT or SMO. SMO mutations most frequently occur in the olfactory groove and AKT at the skull base (12). In one study of WHO grade 1 spinal meningiomas in patients with no clinical suspicion or family history of neurofibromatosis type 2, AKT mutations were detected in 30% of samples and were significantly more likely to be associated with meningothelial histology, and were found in the cervical spine rather than thoracic, as is most commonly seen (46). Additionally, AKT mutations in spinal meningiomas were not shown to have evidence of calcification on imaging, which is important as some studies suggest that tumor calcification may increase risk of challenging tumor resection and decreased neurologic recovery (83).
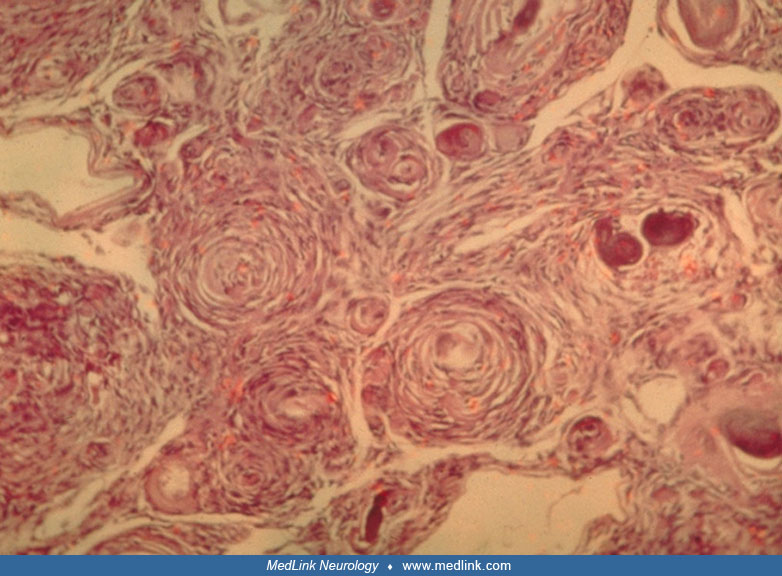
Pathology. In its simplest forms, the tumor is seen as a pinkish round or oval mass with a smooth, granular, or lobulated surface. The texture is usually firm but sometimes may be sufficiently friable to be removed with suction. Calcium deposits (psammoma bodies) are common, and cystic degeneration, hemorrhage, and lipid changes may occur.
The microscopic appearance of meningiomas was classified into three basic types: (1) syncytial, (2) transitional, and (3) fibroblastic (78).
Meningiomas are rarely anaplastic or malignant with mitotic figures and necrosis. Spinal meningiomas and midline skull base meningiomas are predominantly meningothelial meningiomas. Analysis of the increasingly available data on genetic and topographic characteristics of meningothelial meningiomas suggests that they may represent a unique entity, contrary to the prevailing belief that all benign meningiomas are identical tumors (58).
The 2021 WHO classification system for meningiomas incorporates both histological and molecular markers for grading. Grade 1 and grade 2 classifications have remained unchanged. The majority of meningioma variants are WHO grade 1 (“benign”), with the choroid and clear cell variants being classified as grade 2 (“atypical”). When compared to the 2016 classification system, grade 3 meningiomas are no longer based on histopathologic variants but rather the presence of telomerase reverse transcriptase (TERT) promoter mutation and homozygous deletion of cyclin-dependent kinase inhibitor 2A/B (CDKN2A/B), with at least 20 mitoses per 10 high-power fields or malignant cytology (61; 92).
In a series of nearly 200 patients, 91.5% of spinal meningiomas were grade 1, with 8.5% of patients having higher grade lesions (57). Similar results were seen in another single-center study, with 91.9% of the 74-patient cohort with grade 1 and 8.1% with grade 2 spinal meningiomas (70). Recent work evaluating the epigenetic landscape of meningiomas has also provided valuable prognostic information. It is uncertain if this holds true for spinal meningiomas.
Pathophysiology. The meningeal attachment may be broad, rendering the tumor sessile, or narrower than the tumor's maximal diameter. Vascular supply usually comes from this attachment; thus, the dura is often thickened and vascular.
About 7% to 10% of meningiomas are intradural with extradural extension, and 3.5% are entirely extradural (41; 65). More recently, exclusively extradural meningioma has been limited to case reports (08; 97). As it is rare for spinal meningiomas to be exclusively extradural and arachnoid cells that comprise meningiomas to be located intradurally, the pathophysiology of development is thought to have unique causes from those involving the intradural space. Some postulate they arise from ectopic arachnoid cells or that clusters of arachnoid cells migrate into the extradural space (08).
Spinal meningiomas have not been shown to involve bone. This may be due to an enlarged spinal epidural space filled with fat, venous plexuses, and nerve roots.
Spinal meningiomas are most frequently found in the thoracic area (68; 77; 53).
In a meta-analysis of 705 spinal meningiomas, 80.9% were found in the thoracic spine, 16.8% in the cervical area, and 2.3% near the conus and the lumbar spine (68). More recent studies, albeit with smaller samples sizes of 68 to 116 patients, have also shown a thoracic spine predominance, with thoracic spine meningiomas reported in 67% to 79% of patients: 19% to 28% in the cervical spine and 1% to 4% in the lumbar spine (54; 70; 30; 96). The lumbosacral canal may allow a slow-growing tumor to reach large size (34). There is no clear explanation for the predilection of meningiomas for the thoracic canal. However, the predilection for the thoracic spine may only be applicable to female gender, suggesting a hormonal component in the development of thoracic spinal meningiomas (59).
Meningiomas have been associated with pregnancy and menstruation (10), obesity (06), and breast cancer (85; 97), further raising the suspicion that these tumors are hormonally reactive and, therefore, may respond to hormonal manipulation. This was primarily suspected in the intracranial meningioma population but had not specifically been reported in the spinal meningioma population until recently. In a UK cohort of 258 patients with spinal intradural tumors, 68 of whom were found to have meningiomas, nine had a history of breast cancer, which was significantly higher than expected when compared to the expected UK prevalence and to the other intradural tumors in the study cohort. Eight of the nine spinal meningioma patients with breast cancer histories had estrogen receptor–positive breast cancer; all eight underwent surgical resection and hormonal therapy, and seven received radiotherapy (97). Several studies have shown that progesterone receptors are present in a high percentage of cranial meningiomas and are more common than estrogen receptors. In one study comparing progesterone and estrogen receptor intracranial meningioma status, progesterone-positive tumors exhibited significantly increased gene expression variability in genes on chromosome 22q, suggesting a link between progesterone receptors and genes near the NF2 gene (20). Several laboratory studies have shown that meningiomas in tissue culture had their growth suppressed by either progesterone (39) or progesterone antagonists such as RU486 (69). Other researchers suggested that progesterone receptors may play a role in the production of edema around cranial meningiomas (07). These drugs have not demonstrated any meaningful benefit when evaluated in clinical trials of intracranial meningiomas.
Simultaneous occurrence of multiple meningiomas in different neuraxial compartments is uncommon but rarely reported, even without underlying neurofibromatosis. Bhatoe reported a young patient with multiple meningiomas, two intraspinal and several intracranial, which were histologically different (09).
|
• The overwhelming majority of CNS meningiomas are found intracranially; however, spinal meningiomas are the most common intradural tumor. | |
|
• Spinal meningiomas have a strong and consistently reported preponderance for female gender in the sixth decade of life. |
Spinal meningiomas account for only 1.2% to 12% of all CNS meningiomas (98) but up to 45% of primary intradural spine tumors (84). A large series of 1322 primary intraspinal tumors, reported from the Mayo Clinic, recorded an incidence of 29% schwannomas, 25.5% meningiomas, 22% gliomas, and almost 12% sarcomas (89). Meningiomas in the spinal canal are far less frequent than those within the cranial cavity (31; 89; 78).
The majority of spinal meningiomas present in the older population, with a peak in the seventh decade in both males and females. Spinal meningiomas have a female preponderance estimated between 3.8:1 to 9:1 (68; 91; 77; 53; 47), although males have a higher rate of tumor recurrence (47) and mortality (98) with these tumors. Malignant spinal meningiomas are also more common in a slightly younger population: 45 to 64 years of age (36). Meningiomas are rare in children and young adults. In this age group there is an increase of malignant variants when compared to adults and a higher association with neurofibromatosis (26; 66). Familial occurrence of meningiomas, usually multiple, is found largely in the context of von Recklinghausen disease (aka, neurofibromatosis I) (28). Spinal meningioma incidence is significantly higher in White populations when compared to Asians and Pacific Islanders, non-White Hispanics, and Black Americans, though these data were not controlled for socioeconomic status (36).
These tumors are most commonly found in the thoracic spine, potentially because this is the largest region of the spinal cord, although site is not associated with mortality.
There are no known preventative measures for spinal meningiomas.
The most common differential diagnosis for an intradural-extramedullary spinal lesion is between a meningioma, schwannoma, or neurofibroma (60). Spinal schwannomas arise indiscriminately from any of the spinal nerves and almost invariably from the sensory roots. Therefore, there is a high incidence of radicular pain as the presenting symptom. When schwannomas are part of von Recklinghausen disease, the affected portion of the nerve is commonly diffusely swollen in spindle fashion with irregular enlargements. Because schwannomas arise from the nerve, they tend to grow laterally and enlarge the intervertebral foramen, occasionally forming a further mass outside the spinal canal (ie, a dumbbell tumor). These hourglass or dumbbell tumors occur most commonly in the cervical or thoracic regions. Dural metastases should also be considered on the differential diagnosis. Breast cancer and prostate cancer have the highest incidence of dural metastases amongst the solid tumors. Sarcoidosis may also rarely present as an intradural extramedullary mass which can easily be confused with meningioma on neuroimaging studies (43).
Meningiomas, including spinal meningiomas, are a major feature of the syndrome formerly termed “neurofibromatosis type 2” but now called neurofibromatosis type 2–related schwannomatosis. When multiple meningiomas are seen on imaging, suspicion for neurofibromatosis type 2–related schwannomatosis and other related syndromes should be raised (02).
|
• MRI with contrast is the imaging of choice for the diagnosis of meningioma. |
Plain films are insensitive in evaluating patients with suspected intradural pathology. Even secondary bony changes such as erosion or foraminal widening are better demonstrated with computed tomography (95). Plain films are better, however, for diagnosis of instability and quantification of scoliosis and kyphosis.
MRI with contrast is the diagnostic procedure of choice for primary spinal tumors (94; 67). More than 95% of meningiomas enhance homogeneously and brightly following gadolinium injection and have sharply defined margins.
In cross-sectional images, one can visualize the dural base of the tumor vis-à-vis the compressed cord. Spinal meningioma may occasionally be associated with diffuse leptomeningeal enhancement (62). "Dural tail sign" is as common in spinal meningiomas as in cranial meningiomas (01), with a specificity of 100% but sensitivity of 75% in spinal meningiomas (93). Occasionally, spinal meningiomas can be calcified and ossified, which is important for surgical planning, as these tumors are generally more difficult to resect, are associated with higher rates of neurologic injury, and can require a wider laminectomy margin (52). Ossified/calcified meningiomas are easily identified on plain x-rays and CT scans, and typically appear as hypointense lesions on both T1- and T2-weighted MRI scans.
MRI features can be helpful in differentiation of spinal meningioma from schwannoma. Diagnosis of schwannoma is more likely when a spinal intradural extramedullary tumor shows hyperintensity on T2W images or intense enhancement without dural tail sign. Otherwise, meningioma is more probable (25). Coexisting spinal meningioma and schwannoma have been reported in neurofibromatosis (18).
If surgical resection is pursued, the tumor should be sent for histopathology and molecular testing.
|
• Surgical intervention should be considered in most cases, particularly when patients present with neurologic deficits. | |
|
• Radiotherapy should be considered after a subtotal resection or in the case of tumor recurrence. | |
|
• Systemic therapies have been explored without benefit in intracranial tumors; their role in spinal meningiomas has yet to be seen. |
Surgery. Spinal meningiomas are typically managed surgically, and despite the challenge presented by lesions ventral to the cord or at the craniovertebral junction, the vast majority of patients have significant postoperative improvement (11; 17; 86; 55; 56; 21; 22). The indications for surgery include axial pain worse with recumbent positioning, radiculopathy, radiographic malignant appearance or tumor growth, or neurologic deficits, such as motor weakness, sensory disturbance, loss of bowel or bladder function, myelopathy, or gait impairment (13).
Surgical intervention should be considered in most cases, even in older patients with significant neurologic deficits. In a multicenter retrospective study, 102 patients aged 70 years or older with paraplegia or severe paraparesis underwent operation for spinal meningiomas at five French neurosurgical centers between 1990 and 2007. Complete tumor removal was obtained in 93 patients. There was no surgical mortality, and morbidity was 9%. Three months after surgery, seven of the patients were unchanged, 87 patients had improved, and eight were not evaluated. One year after surgery, seven of the 100 surviving patients were clinically unchanged and 93 had improved. Of those who had improved, 49 patients experienced complete recovery. Advanced age is not a contraindication to surgery, even in patients with severe preoperative neurologic deficits; and quality of life can be improved in most cases (79).
Another single institution series of patients treated from 1976 to 2011 found a functional improvement at follow-up in 86.7% of cases, whereas 6.4% of patients remained stable, and 6.9% worsened (73). A low functional grade before surgery was associated with less postoperative improvement. Anterolateral meningiomas were the most represented (42.2%). A gross total resection (ie, Simpson grade I and II) was achieved in nearly 99% of patients, and a macroscopically complete removal without dural resection or coagulation (Simpson grade III) was performed in the remaining 1%. Negative prognostic factors from this study include anterior or anterolateral axial implant, long-lasting symptom duration, WHO grade 2 or 3 tumors, a Simpson grade II or III resection, symptomatology that includes sphincter involvement, and a poor functional grade at onset (74). These authors found surgical complications in seven of 173 cases (4.04%). A total of four patients (two postoperative spinal epidural hematoma, one syringomyelia, and one adverse reaction to dural sealant) required an additional surgery to address the complication. The remaining underwent conservative treatment (three patients with CSF leakage resolved with lumbar drainage).
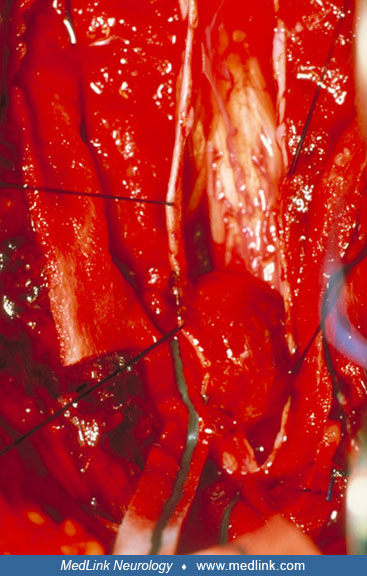
Regarding the operative procedure, usually a subperiosteal dissection of the paraspinal muscles is performed followed by a limited laminectomy over the tumor. If necessary, transdural ultrasonography can be utilized in addition to neuroradiology to further define the location of the tumor vis-à-vis the bone removal (32). The spinal cord is viewed in both sagittal and transverse sections. The rostral and caudal limits of the tumor are immediately obvious. Meningiomas are commonly homogeneously hyperechogenic compared to adjacent tissues, so the tumor mass may be completely visualized.
The dura is then opened in the standard fashion and retracted laterally. Spinal meningiomas have an anterolateral dural attachment and, therefore, the lateral edge will be visualized. Occasionally, the tumor is anteriorly based and not seen initially without lateral retraction of the spinal cord. In such a situation, only minimal and intermittent retraction of the cord is allowed. The bony opening should be generous at the involved side and the microscope positioned in an angle that allows the most lateral view.
The dural attachment can be vaporized and detached with regular bipolar technique or with the CO2 laser. There should not be an attempt to remove the tumor in one piece. Rather, following coagulation of the dural vascular supply, bits and pieces should be removed using microdissecting scissors, a CO2 laser, and an ultrasonic surgical aspirator (21; 22; 13). The tumor usually has a rich vascular supply and early interruption is necessary for adequate visualization and tumor decompression (13). The surgical specimen should be sent for pathology. The dura should be extensively cauterized with the gap reapproximated with polypropylene sutures. Finally, fibrin and synthetic collagen can be added to seal the primary dural repair and minimize the changes of a CSF leak. If concern for spinal instability is present, a laminoplasty or instrumentation can be added for structural support.
Motor-evoked potentials and somatosensory-evoked potentials are routinely monitored during the surgery (27). Following initial laminectomy, rostral and caudal epidural electrodes are placed. The electrode proximal to the stimulus serves as a control and the distal one is for monitoring the operation. For anesthesia, a combination of propofol and narcotics is usually employed with a standard endotracheal intubation. Some basic principles apply for both somatosensory-evoked potentials and motor-evoked potentials. First, information needs to be immediately available and utilized by the surgeon to modify the operative dissection. Second, data should be continuously updated and communicated to the surgeon. Third, criteria for significant changes should be set and tailored for each patient according to the pathology and the baseline potentials.
For motor-evoked potentials, transcortical electrical stimulation (27) and epidural recordings are a reliable intraoperative technique that monitor the upper motor neuron. It has the disadvantage of not differentiating between left and right. Most surgeons do not push dissection beyond a 50% fall in motor-evoked potential amplitude. If and when such a decline occurred we would stop manipulating the cord in this area and wait for the recovery of potentials.
It has been advocated that an attempt should be made, whenever possible, to excise the dural attachment of spinal meningiomas. Nevertheless, a Simpson grade I resection can be riskier, and one series found that a Simpson grade II removal (coagulation of the dural attachment after gross total resection of the tumor) is an acceptable, safe alternative with very low long-term recurrence rates (51). Accordingly, most surgeons believe that simple coagulation of the dural attachment is sufficient for low recurrence rates (33; 29). Some authors have argued for a dura preservation technique to reduce the risk of CSF leakage, in which the meningioma together with the inner layer of the dura is removed and the outer layer is preserved, and the small case series have reported similar recurrence rates to previously published series (81; 82).
If there is recurrence and it is accessible, repeat surgical excision should be attempted.
Prognostic factors for poor functional recovery following surgery include tumor size occupying greater than 75% of the spinal canal, T2 hyperintense signal change in the spinal cord, and poor preop modified McCormick grade of functional status (63). Additionally, in a single institution retrospective study of surgically managed spinal meningiomas between 1990 and 2020, patients who underwent surgery within 12 months of symptom onset had significantly earlier neurologic recovery than those with preceding symptoms for greater than 12 months (40). Interestingly, there is no evidence that cross-sectional area of remaining cord had a relationship with function before or after surgery, suggesting that persistent cord atrophy after decompression may not indict insufficient cord recovery after decompression (24). Tumor calcification, which can reliably be detected with a CT scan, has been associated with longer operation times, more blood loss, and a significantly lower rate of neurologic improvement after surgery (54).
Operative complications range from 0% to 15% in the literature, with CSF leak, wound infections and dehiscence, and transient deterioration of neurologic status being the most common surgical complication (63). Medical complications include pulmonary embolism and urinary tract infection. Permanent neurologic deficit was seen in about 5% of patients (99).
Radiotherapy. External beam irradiation should be used after subtotal resection or after recurrence of a totally resected meningioma. The Cyberknife® Radiosurgery System for benign spinal tumors may be an acceptable therapeutic option for some patients following subtotal resection or recurrent tumor (80). In one retrospective multicenter study of 52 cases of a third recurrence of grade 1 spinal meningioma, 31 patients underwent a third surgery, 17 underwent radiotherapy, and four received no treatment. More patients in the surgical group had improved motor function at 12 months after intervention compared to the radiotherapy group, but more patients in the radiotherapy group reported improved pain post intervention (42). Of note, patients who underwent surgery had significantly larger tumors, and patients who underwent radiotherapy were thought to be poor surgical candidates due to the risk of complications and risk-versus-benefit multidisciplinary discussions.
Systemic therapy. At this time, there are no established systemic therapies for spinal meningioma. However, work has been ongoing in the evaluation of systemic therapies in intracranial meningiomas. Prior studies have evaluated irinotecan (16), hydroxyurea (15), and temozolamide (04) without evidence of efficacy. Cyclophosphamide, adriamycin, vincristine (CAV) combination therapy was explored and was reported to show partial radiographic response in 3 of 14 patients and stability in the other 11 of 14 patients, though with side effects of myelosuppression and neutropenic fever requiring dose reduction (14). At the time of this writing, these results have not been repeated in publication. Additionally, a phase II trial of trabectedin, an alkaloid FDA approved for the treatment of soft tissue sarcoma and ovarian cancer, was terminated early due to high frequency of adverse events without efficacy in grade 2 and 3 meningiomas (72).
Given the association with breast cancer and changes during pregnancy, hormonal regulation has been explored. In a phase III randomized controlled trial of 164 unresectable meningiomas, mifepristone showed no significant impact on disease progression and overall survival compared to the observation-only arm (48).
Tyrosine kinase inhibitors have also been an area of research in intracranial meningioma. In a phase II trial of 25 recurrent meningiomas who received PTK787, 16 experienced disease progression, and an additional five patients stopped treatment due to toxicities (75). The rest voluntarily withdrew or were no longer eligible for the study, but these patients had radiographically stable disease at that time. Though the trial was not designed to evaluate statistical significance for progression-free survival in the subgroups of grade 2 and grade 3 meningiomas, the data showed a trend towards improved progression-free survival when compared to other trials. Another phase II trial of a small molecule tyrosine kinase inhibitor, sunitinib, in recurrent grade 2 and grade 3 meningiomas showed prolonged progression-free survival in VEGFR2-positive patients compared to VEGFR2-negative patients (6.4 vs. 1.4 months, p= 0.005). However, 8% of the treatment cohort experienced an intracranial hemorrhage, of which one was fatal and three were described as serious (49). At the time of this writing, no randomized controlled trial to follow up appears to be registered.
Systemic therapies for recurrent or refractory spinal meningiomas have yet to be reported in the literature but may be an area of interest moving forward.
Kilinc and colleagues reported functional outcomes after microsurgical resection in a cohort of 119 patients (50). After a mean follow-up of 25.4 ± 37.1 months, the rates of overall complication, tumor recurrence, and poor functional outcome were 9.2%, 7.6%, and 5%, respectively. Age, revision surgery, and tumor recurrence were identified as independent predictors of poor functional outcome. Obesity had an impact on the complication rate, whereas extent of resection and tumor calcification affected the rate of tumor recurrence (50).
For patients with high grade (grade 2 or 3) spinal meningiomas, adjuvant radiotherapy may improve recurrence rates.
Meningioma tends to grow during pregnancy. Few cases of spinal meningioma presenting during second or third trimester pregnancy as new-onset paraplegia have been described in literature (03). Both hormonal and hemodynamic changes during pregnancy play a part (19).
No special precautions are necessary during induction. Neuromonitoring can be performed to help ensure a safe resection is performed and motor responses are not lost during the operation. If there is evidence of cord compressions, some surgeons elect to elevate blood pressure/mean arterial pressure to ensure cord perfusion during the surgery.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Nicholas Butowski MD
Dr. Butowski of the University of California, San Francisco, has no relevant financial relationships to disclose.
See ProfileCorinna Fukushima MD
Dr. Fukushima of Rush University has no relevant financial relationships to disclose.
See Profile
Rimas V Lukas MD
Dr. Lukas of Northwestern University Feinberg School of Medicine received honorariums from Jazz Therapeutics, Novocure, and Servier for speaking engagements, honorariums from Cardinal Health, Catalyx, Merck, and Novocure for advisory board membership, research support from BMS as principal investigator, and an honorarium from GT Medical Technologies for DSMB membership.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 06, 2026
Sleep Disorders
Jul. 05, 2026
General Child Neurology
Jun. 24, 2026
General Child Neurology
Jun. 10, 2026
Epilepsy & Seizures
Jun. 02, 2026
Neuro-Oncology
May. 27, 2026
Neuro-Oncology
May. 27, 2026
Neuro-Oncology
May. 23, 2026