Stroke & Vascular Disorders
Medical complications of stroke
May. 03, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Acute ischemic stroke accounts for more than half of the hospitalizations for neurologic disease. Reperfusion therapies, such as intravenous thrombolysis and mechanical thrombectomy, are the gold standard for treatment of acute ischemic stroke; however, only a small percentage of patients are eligible to receive these treatments due to numerous exclusionary criteria and limited resources in certain communities. Therefore, meticulous, aggressive supportive care for the acute stroke patient is imperative to achieve the best possible outcome and to avoid the many medical complications that frequently follow stroke. The author provides an overview of the current literature, including the most recent guidelines from the American Stroke Association.
|
• At acute ischemic stroke onset, permissive hypertension up to blood pressure 220/120 is recommended in accordance with general guidelines. Reducing blood pressure to lower values should be avoided. When thrombolytic therapy is intended, lowering pressures acutely to just below 185/110 is recommended. | |
|
• Volume repletion and circulatory volume maintenance are crucial; hypotonic saline and intravenous dextrose should be avoided. | |
|
• The head of the bed should be lowered if perfusion limitation during acute ischemic stroke is suspected but raised when mounting cerebral edema or elevated intracranial pressures are suspected. | |
|
• Meticulous medical care, including good glycemic control, prompt treatment of fever and infection, early and effective measures to prevent deep vein thrombosis, and the continuation or early addition of statin therapy improves outcome. | |
|
• Early mobilization reduces the frequency of medical complications and improves outcomes. |
Supportive care for patients with acute ischemic stroke has two main objectives: (1) to minimize injury to potentially ischemic brain tissue and (2) to prevent and treat the many neurologic and medical complications that may occur in the immediate period following stroke. As far as advancing therapeutics in ischemic and hemorrhagic stroke is concerned, it continues to have a more broad potential of including those candidates who, at some point, were thought to have no interventions (60). Duncan and colleagues described the importance of post-acute care and outcome follow-up (24). They indicated the need for a paradigm shift regarding rehabilitation readiness of comprehensive stroke care centers where most stroke needs are met.
As cerebral blood flow drops below approximately 25 ml/100 gm tissue/min, neurons begin to malfunction, and neurologic symptoms become manifest, but normal function may be restored with reperfusion. As blood flow is reduced further, neurons begin to suffer irreversible damage. The extent of irreversible neuronal injury (ie, infarction) varies based on the degree and the duration of hypoperfusion (39). The region of cerebral tissue that is hypoperfused yet not irreversibly injured is referred to as the “ischemic penumbra.” Measures to increase cerebral perfusion may prevent permanent damage to this penumbral tissue. Furthermore, additional factors, such as hyperglycemia, hyperthermia, and endothelial dysfunction, may negatively impact salvage of the penumbra by accelerating neuronal damage. Many of the medical and neurologic complications to which stroke patients are susceptible may contribute to neuronal injury in an obvious manner, as in the case of cerebral edema or hypoxemia, or more subtly, as in the case of infection causing fever or the release of inflammatory cytokines (62). There is, therefore, considerable overlap between the goals of protecting neuronal tissue and preventing medical and neurologic complications. Saini and colleagues stated that out of approximately 14 million strokes in 2016, 10% to 20% had large vessel occlusion, less than 5% of patients received thrombolytics, and less than 1% received mechanical thrombectomy (85).
All ischemic stroke patients should receive supportive care. Although there may be a natural inclination to be less aggressive in patients with major stroke, particularly in older patients, it should be noted that even in these populations, the most patients will survive their stroke. The degree of functional recovery, however, may be dramatically impacted by the intensity and appropriateness of supportive care.
Blood pressure management. Extremes of both high and low blood pressure in acute stroke are detrimental to clinical outcomes and should be avoided. Observational studies correlating initial blood pressure values and ischemic stroke outcome suggest a U-shaped curve, with the nadir (ie, best clinical prognosis) observed around systolic blood pressure 150 mmHg (57). This U-shaped relationship is observed in patients with previous hypertension as well as patients without previous hypertension, with a shift toward a relatively higher pressure by about 20 mmHg in the group with previous hypertension (69). Pathophysiologically, poor outcomes due to hypotension are thought to be related to decreased cerebral and coronary perfusion, whereas poor outcomes due to hypertension are thought to be related to the progression of brain edema, elevated intracranial pressure, or elevated risk of stroke recurrence (54; 57).
Decisions regarding blood pressure management in acute ischemic stroke require knowledge of the pathophysiology and natural behaviors of blood pressure after cerebral ischemia. Over 60% of patients presenting to the emergency room with acute stroke are found to be hypertensive (77). The elevation of initial blood pressure in acute stroke is of multifactorial etiology; although it is most frequently a reflection of chronic hypertension, there may be contributions from an acute hypertensive response to brain injury, Cushing reflex from increased intracranial pressure, direct damage to the brain regions involved in autonomic regulation, and stress response to the hospitalization (16). Elevated blood pressure after stroke is not static, however. An older observational study examined the blood pressure trend in 334 consecutive admissions for acute stroke and found that blood pressure was elevated in 84% of patients on the day of admission; there was a spontaneous reduction of blood pressure by an average of 20 mmHg systolic and 10 mmHg diastolic within 10 days following the acute event without any specific antihypertensive therapy (103). Interestingly, only one third of the cases remained hypertensive on the tenth day of hospitalization.
Additionally, blood pressure after acute stroke is influenced by impaired cerebral autoregulation. In healthy individuals, intact cerebral autoregulation enables cerebral blood flow to remain constant across a wide range of systemic blood pressures. In contrast, the cerebral vasculature in patients with acute stroke is unable to adjust to variations in systemic blood pressure, and the relationship between cerebral blood flow and blood pressure becomes linear (68). Therefore, sudden lowering of blood pressure may abruptly decrease cerebral perfusion and increase ischemic brain injury. The sensitive and dynamic nature of post-stroke blood pressure necessitates careful consideration of the necessity and urgency of blood pressure correction in acute stroke.
Evidence from randomized controlled trials provides support against the regular practice of acute lowering of blood pressure in acute ischemic stroke. In a small randomized trial of nimodipine as a neuroprotective agent, a correlation was observed between medication-induced blood pressure reduction and worse clinical outcomes (02). A small randomized controlled trial of candesartan, an angiotensin receptor blocker, in acute stroke did report decreased mortality at 12 months; however, no significant differences in blood pressure were reported (88). In a large trial of over 4000 patients with acute ischemic stroke, no advantage to blood pressure lowering could be demonstrated, even in a population where subjects with known large vessel stenosis were excluded (36).
As a general rule, therefore, blood pressure should not be actively lowered in patients with acute cerebrovascular ischemia. Exceptions include patients who are candidates for or have already received thrombolytic therapy because the risk of intracranial hemorrhage is increased in patients with severe hypertension (99), patients with evidence of active hypertensive injury to other organs (eg, myocardial ischemia), and patients with extremely severe hypertension (greater than 220/120). It is generally believed that decisions regarding blood pressure management should also consider the patient's baseline blood pressure status.
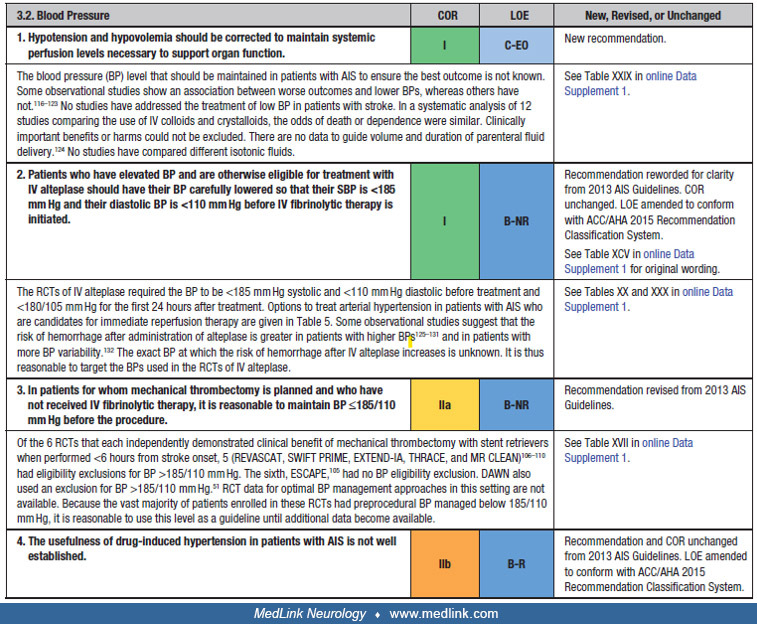
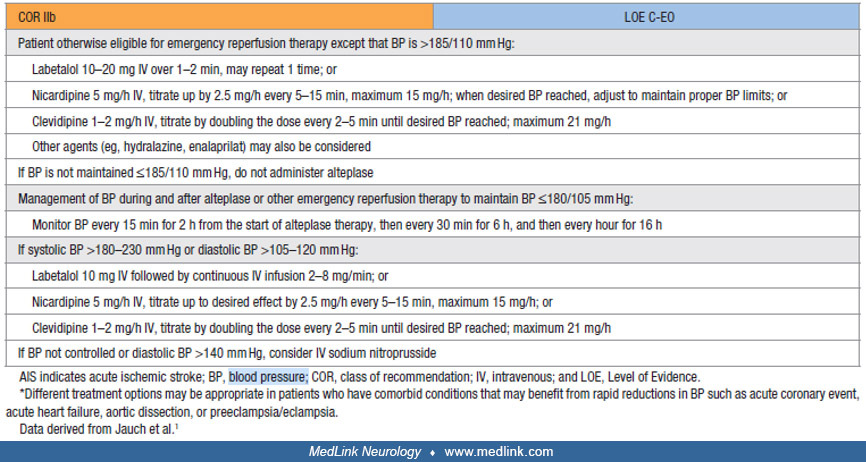
The following tables summarize the current guidelines from the American Heart Association/American Stroke Association for the treatment of elevated blood pressure, including recommendations for patients eligible for thrombolytic therapy (75). In this latter group, the standard protocol for blood pressure management is based on the National Institute of Neurological Disorders and Stroke trial of tPA for acute stroke and should generally be rigidly adhered to.
(From: Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline f...
(From: Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline f...
Beyond avoiding therapies that lower blood pressure, induced hypertension using vasopressive agents has been suggested as a possible therapy for acute stroke. Induced hypertension aims to enhance cerebral blood flow and support or salvage ischemic penumbra. In a cohort of patients with acute hemispheric stroke, vasopressor-induced increases in mean arterial pressure were associated with increases in cerebral perfusion pressure (rising from 72.2+/-2 to 97+/-1 mm Hg, P< 0.0001) (92). Of note, there was also a significant, though modest, increase in intracranial pressure (rising from 11.6+/-0.9 to 11.8+/-0.9 mm Hg, P< 0.05). Data for the efficacy of induced hypertension in the acute stroke setting are limited to small randomized controlled trials and retrospective studies yielding mixed and inconclusive results; therefore, its usefulness is not well established. Nonetheless, it is suggested that induced hypertension may have a role in select populations, such as those with severe ipsilateral extracranial or intracranial large vessel occlusion or stenosis, unstable collateral circulation manifesting as fluctuant or progressive neurologic symptoms, those with expected delay to endovascular thrombectomy, or those with persistent large vessel occlusion following endovascular thrombectomy (78). One contemporary trial showed that in patients with acute lacunar infarcts ineligible for reperfusion therapy or with progressive stroke, phenylephrine-induced hypertension of systolic blood pressure up to 200 mmHg was significantly associated with early neurologic improvement (increase in NIHSS ≥ 2 during the first 7 days) and long-term functional independence (mRS 0-2 at 90 days), though there were significantly more patients in the treated group with hemorrhagic conversion on MRI but not symptomatic intracrnial hemorrhage (05).
Volume status. Stroke patients are at a high risk of volume depletion due to decreased oral intake and increased insensible losses. Hypovolemia (based on serum osmolality) has been associated with worse outcomes and increased mortality in acute ischemic stroke (11). Volume depletion undoubtedly has many deleterious effects. One study of 104 patients suggests that dehydration may be progressive post-stroke, and increased osmolality (greater than 297 mOsm/kg) confers a nearly fivefold increased risk of venous thromboembolism in multivariate analysis (48).
In general, isotonic solutions should be used for volume repletion in acute stroke. Hypotonic solutions should be avoided as they may exacerbate cerebral edema in the acute period. In addition, dextrose-containing fluids should also be avoided as hyperglycemia has been associated with worse outcomes following stroke.
Among the commonly available isotonic solutions, “normal” or 0.9% saline is the generally preferred solution in acute stroke. A retrospective study comparing the use of normal saline versus balanced crystalloid solutions (eg, lactated ringers) in 302 patients with acute ischemic stroke treated with intravenous thrombolysis showed that exposure to any balanced solution at any time was associated with an increased risk of disability at 90 days and possibly hemorrhagic transformation in those treated with intravenous thrombolysis (21). The choice of solution should ultimately be individualized per circumstance, including the presence of concurrent electrolyte abnormalities.
Positioning in bed. In acute stroke, head positioning of the patient should be a decision based on the balance of multiple factors, including optimization of cerebral blood flow, reduction of intracranial pressure, and risk of aspiration and other cardiopulmonary complications.
The head-down position during the acute phase of stroke has been consistently shown to improve cerebral blood flow through gravitational effects, though the long-term clinical benefit of this is less clear. In patients with middle cerebral artery occlusion, an upright posture has been shown to decrease cerebral blood flow and increase oxygen extraction in the affected hemisphere (71). Also, small studies have demonstrated that positioning patients flat in bed can improve cerebral blood flow (91). In patients with acute middle cerebral artery stroke, lowering the head of the bed from 30 degrees to 15 degrees increased middle cerebral artery mean flow velocity measured by transcranial Doppler by 12% (p=0.001) and by an additional 8% when lowered from 15 degrees to 0 degrees (p=0.016) (107). Importantly, there was no change in blood pressure or heart rate with these changes in head position.
Few randomized clinical trials have investigated the clinical benefits of head-down positioning during acute ischemic stroke. The largest trial of over 11,000 patients found that disability outcomes at 90 days after acute stroke did not differ significantly between patients assigned to a lying-flat position and patients assigned to a sitting-up position with the head elevated to at least 30 degrees for 24 hours (04). It is speculated that one reason for this is the broad inclusion of stroke patients whose ischemic process may be relatively less perfusion-dependent, including those with milder deficits (median NIHSS score 4) and mechanisms other than large artery occlusions. More recently, a pilot clinical trial of 96 patients with moderate anterior circulation strokes due to suspected large artery atherosclerosis showed that Trendelenburg positioning (-20 degrees) initiated within 24 hours of stroke onset and maintained for 2 weeks resulted in more favorable functional outcomes than guideline-recommended treatment (19).
Based on these data, it seems reasonable to maintain acute stroke patients in the flat or nearly flat position acutely. There are no data to suggest a definitive time period; however, a common practice is to maintain the flat position for the initial 24 hours after presentation. If neurologic status worsens on head elevation, the patient should be returned to the flat position, and measures to improve cerebral perfusion and maintain collateral blood flow should be considered. In patients with increased intracranial pressure due to swelling from large hemispheric stroke, elevating the head of the bed may improve venous drainage and reduce intracranial pressure, but this may come at the cost of reduced cerebral perfusion pressure. There are few data to guide decision-making in this difficult situation. In patients who cannot tolerate lying flat in bed due to orthopnea or other medical conditions, the head of the bed should be kept at the lowest level tolerated by the patient. Finally, frequent changes in body position (regardless of head position) may help awake and alert patients tolerate lying flat and are indicated to minimize the risk of pressure sores. More data on aspiration risk, the risk of decreased venous outflow, and net clinical benefit are needed.
Glycemic control. In the hyperacute setting, it is important to recognize that both hypoglycemia and hyperglycemia may mimic acute stroke presentations. Hence, the measurement of blood glucose must precede the initiation of intravenous thrombolysis and, in fact, is the only serum measurement required before treatment according to current American Heart Association/American Stroke Association (AHA/ASA) guidelines (75).
Considerable evidence supports a link between hyperglycemia and poor outcomes after stroke. Hyperglycemia within the first 24 hours after acute ischemic stroke is associated with worse outcomes, including increased mortality (64). Compared with normoglycemic patients, patients with acute stroke who present with hyperglycemia have larger infarct volume, poorer functional outcomes, and less favorable outcomes after treatment with thrombolysis, including a higher likelihood of hemorrhage (25; 50; 99) as well as lower likelihood of recanalization (81). Hyperglycemic patients also have reduced salvage of penumbral brain tissue (72; 84). One study suggests that capillary glucose levels higher than 155 mg/dL anytime in the first 48 hours after admission for acute stroke is associated with a 2.7-fold risk of poor outcome at 90 after stroke when corrected for stroke severity, infarct volume, known diabetes, or age (30).
Despite extensive literature demonstrating worse stroke outcomes, current literature does not demonstrate a clear benefit of intensive glucose lowering in hyperglycemic patients in the acute phase of stroke. The SHINE (Stroke Hyperglycemia Insulin Network Effort) trial of over 1100 patients demonstrated no significant improvement in 90-day functional outcomes in those treated with intensive glucose lowering using continuous insulin infusion (target blood glucose concentration 80 to 130 mg/dL) compared with those receiving standard treatment with subcutaneous sliding scale insulin (target blood glucose concentration 80 to 170 mg/dL). Severe hypoglycemia (glucose level lower than 40 mg/dL) occurred in 2.6% of the intensive group (43). Another study of intense insulin therapy utilized a unique protocol with the addition of brain MRI analysis for the assessment of infarct growth. Episodes of asymptomatic hypoglycemia (lower than 54 mg/dL) occurred in 5.7% of the intense insulin therapy group and 0% in the control group. The intense insulin therapy group exhibited significantly larger infarct growth as well as greater occurrence of symptomatic extracranial hemorrhagic transformation (52). Current AHA/ASA guidelines recommend treating hyperglycemia with short-acting intravenous insulin to maintain glucose levels between 140 and 180 mg/dL regardless of whether the patient has a known history of diabetes (75).
Temperature control. Fever is a common finding in acute stroke patients, with as many as 25% generating a temperature of 38.0°C or more within the first 48 hours of admission (34). Increased core temperature in the acute stroke patient may result in an increase in neuronal metabolic demands, neurotransmitter release, inflammatory mediator activity, and free radical production within the ischemic penumbra. Body temperature in acute stroke patients has been correlated with initial stroke severity, infarct size, mortality, and functional outcome in survivors (104). For each 1°C increase in body temperature, the risk of death or severe disability more than doubles (79). A large observational study found that 35% of ischemic stroke patients were febrile sometime during acute hospitalization, but, additionally, the study demonstrated a strong correlation between fever burden (peak temperature duration product) and dismal outcome, death, or hospice such that patients with a fever burden of more than four “degree days” had a nearly 7-fold risk of dismal outcome (74). Therapeutic hypothermia has been shown to improve neurologic outcomes in patients with cardiac arrest (09; 100). However, important differences between resuscitated cardiac arrest and stroke (global vs. focal brain insult, complete reperfusion vs. incomplete or no reperfusion) limit extrapolation of these trials. Studies of acute stroke have shown that induced hypothermia is not beneficial and is potentially even harmful, though this is not considered conclusive due to heterogeneous methods and small studies.
Oxygenation. One of the more intuitive priorities in caring for the acute stroke patient is maintaining adequate tissue oxygenation. However, given that many stroke patients do not have significant lung disease or respiratory compromise, it is not clear that all patients require supplemental oxygen. A quasi-randomized study found no benefit of supplemental oxygen given to stroke patients (82). A randomized trial of high-flow oxygen via face mask in patients with ischemic penumbra present on MRI diffusion and perfusion imaging reported reduced diffusion volume at 4 hours and improved National Institutes of Stroke Scales at 1 week, but there were no significant differences at 3 months (95). These investigators also showed a strong correlation between favorable apparent diffusion coefficient changes and MR spectroscopy measurements of brain lactate and n-acetyl-aspartate (96); however, clinical utility remains to be demonstrated. American Stroke Association recommends administering supplemental oxygen as needed to maintain an oxygen saturation of more than 94%. There is no convincing evidence to suggest the benefit of hyperbaric oxygen in stroke, with the exception of stroke due to arterial air embolism. Hyperbaric oxygen therapy is also associated with claustrophobia and middle ear barotrauma, as well as an increased risk of seizures (08; 37; 75).
Statin therapy. In addition to having lipid-lowering actions, statins (3-hydroxy-3-methyl-glutaryl-CoA reductase inhibitors) may have a neuroprotective effect during the acute phase of ischemic stroke due to their pleitropic actions. A large observational study of over 12,500 patients found that statin use before and during stroke hospitalization is strongly associated with improved post-stroke survival and that statin withdrawal in the hospital, even for a brief period, is associated with worsened survival (27). These findings confirmed those of prior smaller studies (12; 29; 66). Furthermore, the Flint and colleagues study found that the highest survival rates were associated with earlier statin treatment and higher doses. Additionally, initiating statins during hospitalization may be advantageous in terms of post-stroke compliance and meeting national cholesterol guidelines (87). Data from randomized controlled trials, however, are limited; one small study failed to show a difference in long-term outcomes at 90 days when statins were initiated within 24 hours versus on the seventh day (108). Current AHA/ASA guidelines state a moderate recommendation for initiating or continuing a statin in those previously taking one (Class IIa recommendation).
Prevention and management of neurologic complications. Neurologic complications following acute stroke include cerebral edema, recurrent stroke, intracranial hemorrhage, and seizures. Frequent neurologic examinations, followed by repeat neuroimaging if a significant change is noted, may allow rapid identification and treatment of these complications.
Cerebral edema. Patients with large hemispheric or cerebellar infarction are at highest risk of developing clinically significant cerebral edema. Edema typically peaks between 3 and 5 days after stroke onset. Malignant edema resulting from a large territory infarct may be symptomatic, with global symptoms of elevated intracranial pressure such as headache, depressed mental status, nausea or vomiting, or Cushing’s triad (hypertension, bradycardia, respiratory depression). Focal neurologic symptoms may also be specific to the infarction location. These include decreased level of consciousness from compression of thalamic and midbrain reticular activating system, enlargement of the ipsilateral pupil from oculomotor nerve compression, ipsilateral lower extremity weakness or hyperreflexia from subfalcine herniation with compression of the previously unaffected anterior cerebral artery, and ipsilateral upper and lower extremity weakness or hyperreflexia due to Kernohan notch phenomenon (83). Large cerebellar infarctions may cause acute hydrocephalus due to occlusion of the fourth ventricle, resulting in the blockage of cerebrospinal fluid drainage pathways, which manifests as poor mental status and brainstem dysfunction.
Medical management of patients with cerebral edema and increased intracranial pressure from ischemic stroke is empiric, with limited data to support any particular strategy (01). In general, invasive intracranial pressure monitoring does not appear to be of great utility (89). Raising the head position to 30 degrees or greater may increase venous drainage and decrease intracranial pressure but may decrease cerebral perfusion. Hyperventilation can rapidly reduce intracranial pressure, but the effect is short-lived (on the order of hours) and, therefore, of limited utility in the absence of definitive therapy to lower intracranial pressure. Osmotic agents, such as mannitol, glycerol, and hypertonic saline, which have a longer duration of effect than hyperventilation, may be used to “buy time” until edema begins to subside spontaneously. A common strategy is to give a bolus of mannitol 1.0 g/kg, followed by 0.25 to 0.5 g/kg every 4 to 6 hours for several days or until clinical or radiographic evidence of decreased edema is present. There are no convincing data that these agents improve outcomes. Steroids have been shown to be ineffective in ischemic stroke and may increase the rate of infectious complications (67).
For patients with malignant middle cerebral artery infarction, there is considerable evidence for the effectiveness of early surgical management of edema with decompressive hemicraniectomy. A pooled analysis of three small randomized controlled trials of hemicraniectomy within 48 hours of stroke in patients younger than 60 years old found a higher 1-year survival rate (78% vs. 29%) and a higher percentage of patients with mRS ≤ 3, indicating less disability (43% vs. 21%) (102). This pooled analysis was likely too small to define differences in subgroups; thus, optimal patient selection and timing of this intervention remain uncertain. However, other studies have suggested that younger patients are more likely to achieve favorable outcomes and that earlier interventions may be best (90). For patients older than 60 years of age, there is some evidence that hemicraniectomy reduces mortality by approximately 50%, though there is a tradeoff of an increase in severe disability (46). Therefore, in this older age group, treatment with decompressive hemicraniectomy may be best considered as a life-saving procedure. In patients with large cerebellar infarcts who experience decreasing mental status secondary to brainstem compression and hydrocephalus, there is general agreement that suboccipital craniectomy or ventriculostomy is indicated (61).
Early recurrent stroke. The risk of recurrent stroke after an acute stroke can vary among patients according to the underlying pathology. A higher risk of early recurrent stroke is seen in those with large artery atherosclerosis, particularly of the extracranial carotid artery (58) and vertebrobasilar system (35), on the order of approximately 30% recurrence risk in the first month after the initial event. The specific strategy to mitigate the risk of recurrent stroke immediately after acute ischemic stroke is mechanism-dependent, but in general utilizes a combination of antithrombotic therapy and lipid-lowering therapy. Over the last decade, particular attention has been given to the determination of the optimal antiplatelet regimen to reduce the risk of early recurrent stroke after a minor ischemic stroke or high-risk transient ischemic attack; this risk of recurrence is approximately 5% to 10% within 90 days of the initial event (03). Three trials concluded that a 3-week duration of dual antiplatelet therapy with aspirin and clopidogrel is superior to aspirin alone in reducing the risk of recurrent stroke within 90 days, with minor differences between trials in regards to the criteria of NIHSS and time since stroke onset (105; 45; 31). Further discussion of this is included in the MedLink article titled “Ischemic stroke.”
Intracranial hemorrhage. Patients with acute ischemic stroke are at significant risk of intracranial hemorrhage, especially if treated with anticoagulant or thrombolytic therapy. Small asymptomatic hemorrhages may not require any change in therapy. More significant and symptomatic intracranial hemorrhage mandates cessation of anti-thrombotic therapy and reversal of anticoagulation, if applicable. Patients who have received thrombolytic therapy should be treated with cryoprecipitate; when cryoprecipitate is contraindicated or unavailable, transexamic acid or aminocaproic acid should be administered as per AHA/ASA guidelines. A large randomized trial found that surgical evacuation does not improve outcomes in unselected patients with primary intracerebral hemorrhage (63). Nevertheless, a neurosurgical consultation should be obtained, and it is reasonable to consider emergency surgical evacuation in patients with large (greater than 3 cm) cerebellar hemorrhages or those with large, superficial hemorrhages causing substantial mass effects with a rapidly deteriorating condition.
Seizures. Seizures in the acute ischemic stroke setting have been reported in 1% to 6% of patients (55). Early seizure occurrence has been associated with stroke location (particularly with regard to cortical involvement), size, severity, and hemorrhage (13). Border zone infarction associated with severe carotid artery stenosis has been implicated as a risk factor for early seizure (22). Among 581 young cryptogenic stroke patients, 14 (2.4%) had seizures within 7 days of their event (56). Twenty patients in the overall cohort of 581 patients (3.4%) subsequently developed late seizures (at a mean of 12.9 months), of which only six previously had an early seizure. Four of these six patients had their late seizure while they were already on an anticonvulsant medication. Early seizure was a risk factor for later seizures (hazard ratio=5.1, 95% CI 1.8 to 14.8), a finding that has been reported in another study as well (97). However, the largest collection of ischemic stroke patients published to date, with 1632 patients, did not find early seizure to be a risk factor for recurrent seizures (13). It remains controversial as to whether anticonvulsants should be initiated in all patients with early seizures because the potential for seizure prophylaxis should be weighed against factors such as age, disability, and risk of adverse effects (15). Most neurologists find it difficult not to treat patients with seizures in the setting of acute stroke with anticonvulsants; however, continuing therapy for very long in the absence of recurrent seizures seems not to be justified. There is no evidence to support prophylactic use of anticonvulsants in patients with ischemic stroke who have not had seizures.
Delirium. Delirium refers to an acute, transient disturbance in cognition, consciousness, or attention characterized by a fluctuating course. Affecting up to one third of patients in the acute phase of stroke, delirium is a serious neuropsychiatric complication that is associated with poorer outcomes, longer hospital length of stay, greater likelihood of discharge to long-term care facilities, and increased mortality both in-hospital and at 12 months (94). Common precipitating factors include infection, dehydration (causing metabolic derangements), and drug toxicity (most frequently from sedating medications). Risk factors for post-stroke delirium include preexisting cognitive impairment, brain atrophy, anterior circulation large-vessel strokes, and stroke severity (70; 80). Screening for early signs of delirium and prompt intervention on modifiable risk factors such as infection are important. There are limited data on the management of delirium in stroke; hence, the approach is the same as that for delirium in acute medical illness. This involves treating the underlying cause as well as controlling symptoms that can often be disruptive to clinical care, such as agitation, wandering off, or a risk of falling. Non-pharmacologic interventions are the mainstay of treatment, such as environmental manipulations to mitigate disorientation, verbal reorientation, and minimized use of physical restraints. When these measures fail and if the concern is for agitation or harmful behavior, short-term pharmacologic intervention may be carefully considered, such as with low-dose haloperidol. It is important to note that there is a lack of robust evidence suggesting that any pharmacologic agent will resolve delirium more quickly or reduce delirium symptoms other than agitation (23).
Prevention and management of medical complications. Medical complications such as pneumonia, sepsis, pulmonary embolism, and myocardial infarction account for approximately half of the fatalities in the early period following stroke (44). In the United States, hospital discharge data indicate that in-hospital mortality due to stroke has decreased across the decade 1998 to 2007 (odds ratio (OR) 0.75) (101). Among the common medical complications of stroke, the incidence of pneumonia has not changed; however, the incidence of acute myocardial infarction and urinary tract infection has risen modestly (OR 1.39 and 1.18, respectively). The incidences of deep vein thrombosis and pulmonary embolism have risen more (OR 1.69 and 2.39, respectively).
Cardiovascular events. Stroke is frequently complicated by cardiac events such as myocardial infarction and arrhythmia (65). All patients who are admitted with acute stroke should have an ECG to identify active or prior cardiac ischemia and to assess cardiac rhythm. If available, continuous cardiac telemetry is a useful means of identifying intermittent arrhythmias, such as atrial fibrillation, that may have important diagnostic implications in the stroke patient.
It is important to be aware that ECG changes are seen frequently in acute stroke and may occasionally be the result of central nervous system injury and the corresponding hyperadrenergic state (86). More severe strokes are associated with impaired autonomic cardiovascular control (38). Commonly observed electrocardiographic changes include ST segment depression, QT prolongation, inverted T waves, and prominent U waves (73). Cardiac enzymes should be obtained if ischemia is suspected, but again, they must be carefully interpreted. A consecutive series of 160 acute stroke patients (of which 140 were ischemic) found elevated troponin levels in 10 (6%). Troponin levels rapidly normalized, and chest pain, Q-waves, and focal akinesis were rare, implying that modestly elevated troponin levels in stroke patients are primarily neurogenic in origin (17). Minimally elevated troponin T values, at or below 1 ng/ml, are not infrequent in patients with large anterior distribution infarcts (33). In cases of confirmed myocardial infarction following stroke, decisions about double antiplatelet therapy, anticoagulation, glycoprotein IIb and IIIa inhibitors, and invasive procedures must take into account the extent and acuity of the cerebral infarction to estimate the excess risk of intracranial hemorrhage or other complications associated with these therapies.
Chest radiography is useful for assessing heart size and identifying pulmonary edema, which should prompt evaluation and management of congestive heart failure. In patients with significant heart failure, efforts to increase cerebral perfusion with intravenous fluids and cessation of antihypertensive agents may have the opposite effect due to worsening of cardiac output. In these cases, optimization of cardiac output is a reasonable primary goal.
Deep vein thrombosis and pulmonary embolism. Venous thromboembolism is a common and potentially devastating complication of stroke. It has been estimated that pulmonary embolism accounts for up to 25% of fatalities following stroke (49). Risk factors for deep vein thrombosis include advanced age, lower extremity paralysis, and atrial fibrillation. Subcutaneously administered heparin or low-molecular-weight heparin has been shown to reduce the risk of deep vein thrombosis (01). One large randomized trial compared enoxaparin (a low-molecular-weight heparin) subcutaneously once daily to unfractionated heparin 5000 U subcutaneously every 12 h for 10 days and reported that enoxaparin reduced the risk of venous thromboembolism by 43% (p=0.0001) (93). There were no significant differences in the risk of any bleeding or symptomatic intracranial and major extracranial hemorrhage. There is also evidence that elastic compression stockings, aspirin, and sequential compression devices can reduce the risk of deep vein thrombosis, and this effect may be additive with anti-thrombotic medication (47; 49). Stroke patients with diminished mobility should receive some form of prophylaxis against deep vein thrombosis or pulmonary embolism. The benefit of mechanical prophylaxis, which is also generally recommended, is more controversial (76). In patients suspected of harboring deep vein thrombosis, lower extremity ultrasound is indicated. Serum D-dimer is probably a less useful alternative, given the high pre-test probability of deep vein thrombosis or pulmonary embolism in stroke patients. Patients with established deep vein thrombosis or pulmonary embolism should generally be treated with anticoagulant therapy. If anticoagulant therapy is contraindicated, consideration should be given to the placement of an inferior vena cava filter, though the long-term effects of this intervention are controversial (51).
Infection. Infection is commonplace in patients with acute stroke. Pneumonia and urinary tract infections occur most frequently, each affecting about 10% of acute stroke patients (44; 06). A systematic review finds that infection complicates care in 30% of acute stroke patients (106). Less frequent infectious processes include cellulitis and sepsis. Acutely ill patients, particularly the elderly, may not immediately generate fever and may instead present with unstable vital signs, decreasing oxygenation, or a change in neurologic exam. A high index of suspicion for infection must be maintained and a rapid evaluation of possible sources initiated when appropriate. Close attention should be paid to urinary catheters and intravenous and central lines. Empiric antibiotics are reasonable for patients in whom infection is strongly suspected pending the results of diagnostic tests. However, a randomized trial of 3 days of levofloxacin in patients with acute stroke as prophylaxis against infection on admission to the hospital found that those who received antibiotics actually did worse than those who did not receive them (18). Aggressive treatment of fever is indicated, as described previously.
Dysphagia and malnutrition. Poor nutritional status at hospital admission is associated with worse outcomes following stroke due to increased risk of infection, gastrointestinal bleeding, and bed sores (28). Further, acquired malnutrition following a stroke is also associated with a worse prognosis (20). Swallowing dysfunction is common in acute stroke patients and is associated with a high risk of inadequate nutritional intake and aspiration (59). A meta-analysis found that the risk of pneumonia and risk of death were both four times higher in patients with acute stroke and post-stroke dysphagia compared to those without post-stroke dysphagia (07). The same study identified risk factors for post-stroke dysphagia that included hemorrhagic stroke, previous stroke, severe stroke (higher NIHSS score), female sex, and comorbid diabetes mellitus. Swallowing evaluation should be performed in all patients with dysarthria, aphasia, or facial, buccal, or lingual weakness. An inability to swallow safely should precipitate early placement of a nasogastric tube in order to ensure gastrointestinal access for nutrition and medications. If swallowing difficulties persist greater than 1 to 2 weeks a percutaneous gastrostomy tube should be considered.
Airway compromise. Patients with brainstem stroke or a decreased level of arousal due to large hemispheric stroke have an increased risk of airway compromise secondary to loss of protective reflexes or oropharyngeal weakness (53). Patients who are unable to protect their airway should undergo endotracheal intubation, with the recognition that those who require intubation have a poor prognosis, with a mortality rate of over 60% (14).
Activity level. Rapid mobilization after the acute period may reduce the risk of pneumonia, deep vein thrombosis, pulmonary embolism, and pressure sores. Shorter time to mobilization and rehabilitation training has been associated with greater odds of discharge to home (as opposed to a nursing home or death) at 6 weeks (41). As soon as a patient has become neurologically stable, physical therapy should be initiated.
Organizational strategies: stroke units and transitional care. Specialized units for caring for stroke patients arose in the late 1970s and early 1980s. Such units typically offer continuous cardiovascular and respiratory monitoring and are staffed by a team of healthcare providers—vascular neurologists, neurologic nurses, rehabilitation experts—who have specialized expertise in stroke care. The organizational breadth of these units varies considerably based on geography; in Europe, such units generally encompass the prolonged rehabilitation care of patients, whereas in the United States, they more typically provide care for a shorter time period, with patients transitioning to separate rehabilitation units. These differences complicate the interpretation of studies that have been performed to evaluate the effectiveness of stroke units. Nevertheless, randomized trials have consistently demonstrated that stroke units decrease mortality, increase the likelihood of being discharged to home, and improve functional status and quality of life (42). These benefits are durable, persisting up to 10 years after discharge (40). A large meta-analysis of 19 trials with 3249 patients comparing stroke units to general medical wards found that stroke units reduced mortality, death or institutionalization, and death or dependency without a significant increase in length of stay (98). Although many trials have not detected a differential benefit based on stroke subtype, there is some evidence that small vessel infarctions may benefit less compared to other stroke subtypes (26). In a study by Bettger and colleagues, transitional care from hospital to home varied widely among hospitals, and no single strategy was applied universally or provided across hospitals (10). Gesell and colleagues demonstrated that comprehensive post-acute stroke services were associated with better functional status (32). However, the implementation appears diverse, with some challenges, particularly in reaching out to the patients and ensuring consistent delivery of follow-up visits.
Conclusion. The period immediately following an acute ischemic stroke is a time of significant risk. Meticulous attention to the care of the stroke patient during this time can prevent further neurologic injury and minimize common complications, optimizing the chance of functional recovery. There exists a large gap among eligible patients and low utilization rates of thrombolysis and mechanical thrombectomy for these patients. Multiple initiatives are underway worldwide to improve systems of care and bridge this gap.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Ainie Soetanto MD
Dr. Soetanto of Maimonides Medical Center in Brooklyn, NY, has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
May. 03, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026
Stroke & Vascular Disorders
Mar. 10, 2026