






Neurobehavioral & Cognitive Disorders
Mental status examination
Jun. 17, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author explains the clinical presentation, pathophysiology, diagnostic work-up, and management of swallow syncope. Swallow syncope is most commonly associated with esophageal disorders that affect the afferent limb of a vagovagal reflex, including such disorders as hiatal hernia, gastroesophageal reflux, diffuse esophageal spasm, esophageal carcinoma, esophageal stricture, esophageal stenosis from ascending aortic aneurysm, distal esophageal Schatzki ring, hypertensive peristaltic waves (“nutcracker esophagus”), achalasia, and esophageal diverticula.
|
• Swallow syncope may occur within 3 to 5 seconds of swallowing. Many bouts result only in presyncope, with associated visual greyout, tunnel vision, etc. | |
|
• Swallow syncope is frequently triggered by liquids, particularly cold, carbonated beverages. | |
|
• Swallow syncope is caused by stimulation, irritation, or dysfunction of the afferent origin of a vagovagal reflex (eg, the distal esophagus), the vagus nerve itself, or the efferent target of the vagovagal reflex (ie, the heart). | |
|
• Swallow syncope may be confused with epilepsy, particularly as the syncopal attacks may be associated with secondary arrhythmic convulsive jerks of the extremities (ie, convulsive syncope). |
Swallow syncope is a loss of consciousness during or immediately following a swallow (59). Recognition of the disorder dates from the late 1700s, but most cases have been reported since 1900 (59). Swallow syncope is usually caused by upper gastrointestinal-cardiac vagovagal reflexes initiated by swallowing and rapid gastric distention (76). As such, swallow syncope is often considered one of a number of neurally mediated, "situational" syncopes that include those which occur after micturition, defecation, coughing, or, rarely, laughing (29). Cases have also been reported in animals (79).
|
• Swallow syncope may occur within 3 to 5 seconds of swallowing. | |
|
• Many bouts result only in presyncope, however, with associated visual greyout, tunnel vision, etc. | |
|
• Swallow syncope may occur several times a day and may occur while either upright or supine. | |
|
• Swallow syncope is frequently triggered by liquids, particularly cold, carbonated beverages. |
Swallow syncope may occur within 3 to 5 seconds of swallowing. Many bouts result only in presyncope, however, with associated visual gray out, tunnel vision, etc. Swallow syncope may occur several times a day and may occur while either upright or supine. There may be associated brief jerking or rhythmic movements (ie, convulsive syncope), but there is no associated incontinence, tongue biting, or postictal state (94). Recovery usually occurs within seconds without vasomotor or other sequelae. Patients are amnestic for the period of lost consciousness.
Swallow syncope is frequently triggered by liquids, particularly cold, carbonated beverages (13; 08; 27; 45; 46; 74; 49; 30; 85; 17), but selective precipitation of swallow syncope by solids has also been reported in individual patients (27; 87; 91; 100; 67). In one 76-year-old man, swallow syncope associated with atrioventricular block and sinus arrest was only induced by eating citrus fruits, citrus jelly, and acidic foods but not by other drinks and foods (107).
The long-term prognosis of swallow syncope depends largely on the prognosis of the underlying condition, but syncope itself can result in severe bodily injury (86).
Case 1 (10). A 65-year-old woman noted brief attacks of dizziness while eating for almost two decades, and later experienced occasional syncope while eating. Both eating and esophageal balloon dilation precipitated second-degree atrioventricular block (Mobitz type II) with sinus bradycardia accompanied by dizziness. Radiologic and manometric examinations of the esophagus demonstrated diffuse esophageal spasm associated with increased upper esophageal sphincter pressures, gastroesophageal reflux, and a sliding hiatal hernia. The patient refused pacemaker implantation. She had significant clinical improvement with treatment with atropine sulfate.
Case 2 (65). A 68-year-old woman was brought to the emergency room with complaints of worsening intermittent lightheadedness and dizziness. The day before admission, she lost consciousness after swallowing a pickle, an event witnessed by her family. She remained unconscious for about 20 minutes until paramedics arrived.
She had a history of (1) coronary artery disease with three stents; (2) a transient ischemic attack with left-sided weakness two months before admission; (3) breast cancer with resection 7 months before admission; and (4) a neuroendocrine tumor of the terminal ileum with resection 7 years before admission. Other medical history included obesity, hypertension, diabetes, interstitial lung disease for which she was on oxygen, and a recently discovered thyroid nodule.
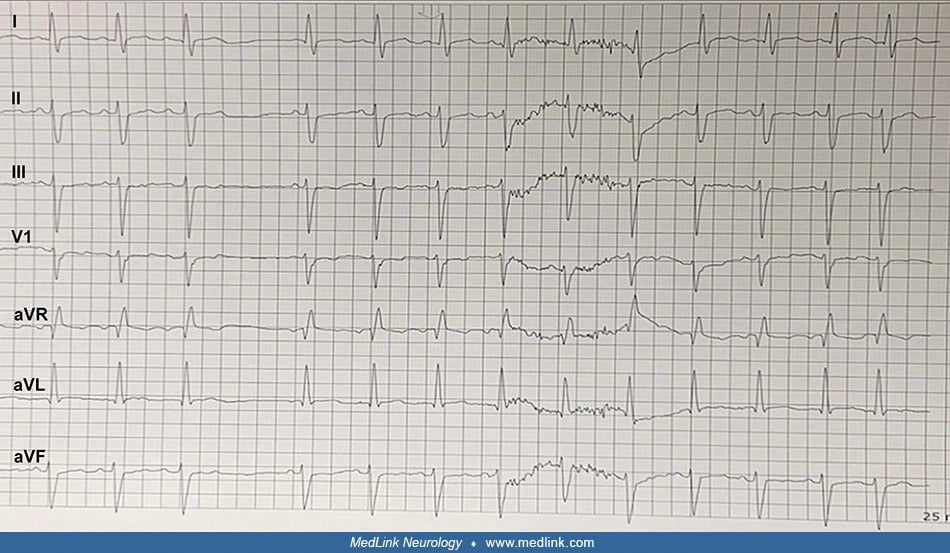
Vital signs included a heart rate of 88 beats per minute, blood pressure of 172/83 mmHg, respiratory rate of 20 breaths per minute, and oxygen saturation of 97% on 2 L of oxygen. Orthostatic blood pressures showed no orthostatic hypotension. She was given an ABCD2 score of 4. ECG showed a bifascicular block, which was new since her prior ECG. Chest x-ray showed no relevant findings. Transthoracic echocardiogram with contrast showed normal left ventricular diastolic function, mild mitral regurgitation, and an estimated ejection fraction of 60% to 65%. An esophagram showed no major deficits.
After the initial ECG, the patient was monitored overnight while on telemetry. Telemetry only alerted for bradycardia. However, when the rhythm strip was personally examined, it showed a high-grade, second-degree AV block with three consecutively blocked P waves. The patient reported that she was eating at the time of the abnormal findings and that she had a brief episode of lightheadedness. A repeat ECG showed no severe abnormalities. Beta-blocker medications were discontinued.
On clarifying her recent medical history, her prior symptoms of lightheadedness and dizziness over “multiple years” were almost always associated with swallowing and usually resolved within an hour after swallowing. She found that cutting her food into tiny pieces helped prevent the presyncopal episodes. When asked to drink cold water while on telemetry as a provocative test of swallow syncope, she reported dizziness and lightheadedness immediately after swallowing. Demonstrating a close temporal relationship between swallowing, symptoms of lightheadedness, and corresponding ECG changes established a diagnosis of swallow (pre)syncope. A permanent, dual-chamber, rate-modulated pacemaker was placed, which immediately terminated these events.
Case 3. A 64-year-old woman presented to an emergency department with complaints of episodic dizziness and lightheadedness while eating over the prior three months (43). She had a past medical history of a non-ST elevation myocardial infarction, prior coronary artery bypass grafting procedure, diabetes mellitus, hypertension, gastroesophageal reflux disease, and status post an uncomplicated total thyroidectomy.
A barium swallow was normal with normal initiation of swallowing, normal esophagus with normal peristalsis, no evidence of strictures, and no hiatal hernia.
Holter monitor revealed frequent sinus pauses during swallowing of both soft and hard foods, establishing a diagnosis of "deglutition syncope" (sic, deglutition presyncope). The patient was given multiple therapeutic options, including placing a pacemaker, undergoing surgery, or being prescribed a selective serotonin reuptake inhibitor. The patient was prescribed a selective serotonin reuptake inhibitor (sertraline). Repeat Holter monitor revealed paroxysmal atrioventricular (AV) block with up to 5.1 seconds of asystole during swallowing; her sinus pauses were associated with transient dizziness (for a few seconds).
On examination, she had a regular heart rate and rhythm, with normal cardiovascular and pulmonological auscultation. An electrocardiogram showed normal sinus rhythm with no ST segment of T wave changes and no AV block. Telemetry showed similar monitoring findings.
The syncopal episodes resolved after placement of a dual-chamber pacemaker. Subsequent pacemaker interrogation in the dual chamber pacing (DDD) mode showed normal functioning with no abnormal events.
|
• Swallow syncope is caused by stimulation, irritation, or dysfunction of the afferent origin of a vagovagal reflex (eg, the distal esophagus), the vagus nerve itself, or the efferent target of the vagovagal reflex (ie, the heart). | |
|
• Several pathophysiologic processes that may cause or contribute to swallow syncope include cardiac arrhythmias, a vasodepressor response, and stimulation of hypersensitive carotid sinus. |
Swallow syncope is caused by stimulation, irritation, or dysfunction of the afferent origin of a vagovagal reflex (eg, the distal esophagus), the vagus nerve itself, or the efferent target of the vagovagal reflex (ie, the heart).
Several pathophysiologic processes may cause or contribute to swallow syncope, and sometimes multiple mechanisms can be implicated, even in the same patient (63; 110; 51):
Cardiac arrhythmias. In susceptible patients, swallowing may produce vagally mediated cardioinhibitory responses, with consequent cardiac arrhythmias due to parasympathetic efferent activation and inhibition of the sinoatrial and atrioventricular nodes of the heart (88). Such vagally mediated cardiac bradyarrhythmias include sinus bradycardia (59; 13; 36; 05; 34; 69; 82; 70; 20; 27; 73; 07; 46; 100; 25; 54; 61), sinus arrest (59; 69; 87; 74; 56; 30; 17; 65; 14), and partial or complete atrioventricular conduction block, possibly with junctional or ventricular escape rhythms (59; 60; 22; 05; 53; 26; 106; 68; 41; 48; 24; 52; 84; 93; 04; 27; 45; 91; 101; 09; 54; 01; 44; 102; 107; 43; 66). Vagal stimulation can also induce ventricular asystole in some patients (59; 95; 74; 43), particularly if vagal tone has been accentuated by cholinergic agents (eg, acetylcholinesterase inhibitors), hypoxia, hypercapnia, or tracheal suctioning in the setting of respiratory infection (89; 108; 92; 103; 55). Uncommonly, vagal stimulation may be associated with paroxysmal atrial fibrillation (57) or other arrhythmias (59).
The duration between the onset of swallow and a bradyarrhythmia or asystole is extremely short (2-3 seconds) and is typically elicited by reflex afferent pathways originating in the oropharynx, rather than the esophagus (06).
Swallow-induced paroxysmal atrial tachycardia due to atrioventricular nodal reentry tachycardia has also been reported (40; 21). One woman experienced recurrent presyncope while speaking out loud at her job; Holter electrocardiography revealed atrial tachycardia while swallowing without presyncope (21).
Vasodepressor response. Some patients have a primary or concomitant vasodepressor component with hypotension preceding or in the absence of bradycardia (05; 16; 20; 51). Presumably, vagal afferent stimulation produces sympathetic inhibition with resulting peripheral vascular vasodilation and hypotension. In patients with a significant vasodepressor component, syncope may not resolve with cardiac pacemaker implantation.
Stimulation of hypersensitive carotid sinus. Swallowing may stimulate a hypersensitive carotid sinus and cause reflex hypotension or vagally mediated, high-grade atrioventricular block and syncope. Several possible mechanisms have been proposed, including mechanical pressure effects of accessory neck muscles on the carotid sinus during swallowing.
Glossopharyngeal neuralgia. In patients with Chiari I malformation, compression of the glossopharyngeal and vagus nerves between the herniated tonsil and either the posterior inferior cerebellar artery or the vertebral artery can cause ephaptic transmission (crosstalk) in the nerve fibers and secondary pain and cardiac syncope (02).
In a retrospective study of 3140 patients who underwent head-up tilt testing, 354 (11%) were diagnosed with situational syncope (111). Swallow syncope represented only about 7% of situational syncopes. Swallow syncope was more common in women than in men.
Swallow syncope may be confused with epilepsy, particularly as the syncopal attacks may be associated with secondary arrhythmic convulsive jerks of the extremities (ie, convulsive syncope) (23; 12; 05; 109). However, there is typically no associated aura, postictal confusion, tongue biting, or incontinence with swallow syncope. Rare patients with swallow syncope may have interictal epileptiform activity on electroencephalograms, postictal symptoms, and apparent control of syncope with anticonvulsants, and in such rare cases, swallow-triggered changes in cerebral blood flow or other factors may actually trigger a seizure.
Several conditions may cause or contribute to swallow syncope by stimulating the afferent origin of a glossopharyngeal-vagal or vagovagal reflex (eg, the distal esophagus), the vagus nerve itself, or the efferent target of the vagovagal reflex (ie, the heart).
|
Afferent limb of glossopharyngeal-vagal reflex | |
|
• glossopharyngeal neuralgia (82; 70; 02) | |
|
Afferent origin (distal esophagus) of vagovagal reflex | |
|
• hiatal hernia (76; 64; 71; 47; 77; 83) | |
|
• gastroesophageal reflux (35; 28; 30; 32; 17) | |
|
• diffuse esophageal spasm (59; 03; 76; 10; 37; 75; 11; 61) | |
|
• esophageal carcinoma (98; 104; 76; 04) | |
|
• esophageal stricture (97; 99; 76) | |
|
• esophageal stenosis from ascending aortic aneurysm (78) | |
|
• distal esophageal Schatzki ring (31) | |
|
• hypertensive peristaltic waves (“nutcracker esophagus”) (31) | |
|
• achalasia (76; 16; 100; 110) | |
|
• esophageal diverticulum (59; 76) | |
|
• gastric banding (58) | |
|
Vagal nerve disorders | |
|
• carcinomatous meningitis with demyelination of vagus nerve (59) | |
|
• digitalis toxicity (59; 05; 37; 96; 07) | |
|
• whiplash injury (62) | |
|
• exaggerated vagal reflex (81) | |
|
Efferent target (heart) of glossopharyngeal-vagal or vagovagal reflex | |
|
• cardioactive drug therapy (05) | |
|
• myocardial infarction (59; 05; 07) | |
|
• cardiac arrhythmias, including sick sinus syndrome | |
|
• latent cardiac conduction disturbances (05) | |
|
Several factors may increase the likelihood that swallowing-mediated reflex mechanisms will produce syncope | |
|
• orthostatic hypotension | |
|
• hypersensitive carotid sinuses (84; 04; 110) | |
|
• diabetes mellitus (72) | |
|
• Chiari malformation (02) | |
|
• pulmonary arterial hypertension | |
|
• left ventricular outflow obstruction (eg, from idiopathic hypertrophic subaortic stenosis) | |
|
• pericarditis | |
|
• congestive heart failure | |
|
• severe carotid artery or intracranial artery stenosis or occlusion | |
|
• hydrocephalus | |
|
• Pulmonary function studies, a chest x-ray, and an electrocardiogram should be obtained. | |
|
• EKG monitoring can be helpful in identifying associated cardiac arrhythmias, particularly during the swallowing of beverages associated with syncope (eg, cold carbonated beverages), balloon dilation of the distal esophagus, or insufflation of air into the stomach. | |
|
• Barium esophagram, esophagogastroduodenoscopy, 24-hour esophageal manometry, and pH recording, together with Holter monitoring, may be useful in demonstrating esophageal abnormalities (eg, gastroesophageal reflux or esophageal spasm) associated with swallowing and cardiac syncope. |
The diagnostic workup varies depending on the clinical circumstances and the clinically suspected etiologies of swallow syncope. Lung function, cardiac function, blood pressure, and blood volume should be assessed clinically. Pulmonary function studies, a chest x-ray, and an electrocardiogram should be obtained. EKG monitoring can be helpful in identifying associated cardiac arrhythmias, particularly during swallowing of beverages associated with syncope (eg, cold carbonated beverages), balloon dilation of the distal esophagus, or insufflation of air into the stomach (36; 05; 68; 69; 41; 52; 08; 96; 07; 45; 87; 91; 46; 67; 49; 54; 42; 65). Barium esophagram, esophagogastroduodenoscopy, 24-hour esophageal manometry, and pH recording together with Holter monitoring may be useful in demonstrating esophageal abnormalities (eg, gastroesophageal reflux or esophageal spasm) associated with swallowing and cardiac syncope (75; 11; 07; 35; 28; 30; 32). In some patients with suspected vagally mediated arrhythmias, vagal maneuvers can be considered to determine if increased vagal tone can precipitate related clinical outcomes (eg, sinus arrest, atrioventricular block, hypotension, or syncope) (04); such maneuvers can include carotid sinus massage and eyeball compression, but many reported cases of swallow syncope did not have abnormal findings with such maneuvers. More sophisticated cardiac electrophysiologic studies are rarely needed. Echocardiography may be needed in cases of suspected pericarditis or cardiac outflow obstruction. MRI is not routinely indicated. Some cases may require consultation by a gastroenterologist or cardiologist, depending on the clinically suspected underlying etiologies identified. Brain imaging may be helpful in occasional cases (eg, Chiari malformation, glossopharyngeal neuralgia, carcinomatous meningitis, etc.).
|
• Trigger foods, such as cold carbonated beverages, should be avoided. | |
|
• The underlying conditions associated with swallow syncope may require specific targeted management (eg, esophageal disorders, hypoxia, cardiac dysfunction, postural hypotension, hypovolemia, or cerebrovascular stenosis). | |
|
• Patients with swallow syncope associated with cardiac arrhythmias, even if vagally mediated, may benefit from treatments designed to suppress vagal tone or accentuate sympathetic tone. | |
|
• In many patients with swallow syncope, pacemaker implantation is considered the safest and most definitive treatment approach. |
Trigger foods, such as cold carbonated beverages, should be avoided (30). The underlying conditions associated with swallow syncope may require specific management directed at these conditions [eg, esophageal disorders, hypoxia (39), cardiac dysfunction, postural hypotension, hypovolemia, or cerebrovascular stenosis]. In some cases, correction of underlying conditions may cure or prevent the swallow syncope (eg, with digitalis toxicity and some esophageal disorders). Patients with syncope that is not medically controlled should be advised not to drive automobiles or other motorized vehicles (38).
Surgical correction of associated esophageal abnormalities has met with variable success (97; 105; 33; 05; 64). Various surgical treatments have been reported to have abolished swallow syncope in single case reports, for example Nissen fundoplication in a patient with a hiatal hernia (64), esophageal dilation in a patient with an esophageal stricture (97), peroral endoscopic myotomy for esophagogastric junction outflow obstruction that failed medical therapy (50), or achalasia (100).
Patients with swallow syncope associated with cardiac arrhythmias, even if vagally mediated, may benefit from treatments designed to suppress vagal tone or accentuate sympathetic tone. Such treatments include administration of atropine, ephedrine, procaine block of the vagus nerve in the neck, or section of afferent or efferent reflex pathways (59; 36; 41; 07; 55; 25; 30).
However, in many patients with swallow syncope, pacemaker implantation is considered the safest and most definitive treatment approach (80; 05; 106; 69; 41; 24; 52; 96; 04; 72; 27; 07; 46; 31; 100; 74; 101; 09; 56; 67; 54; 30; 01; 44; 17; 06; 62; 102; 107; 19; 94; 65; 14). If a definitive diagnosis of cardiac rhythm disturbance associated with swallowing or balloon-mediated esophageal distention cannot be made, a temporary pacemaker can be employed to establish therapeutic benefit before a permanent pacemaker is implanted (05). Patients with a significant vasodepressor component may not benefit from pacemaker implantation and should generally be managed pharmacologically (05; 90; 16; 20).
Patients with swallow syncope associated with hypersensitive carotid sinus syndrome may benefit from similar treatments to patients with vagally mediated cardiac arrhythmias, including administration of atropine and vasoconstrictors, procaine block of the vagus nerve in the neck, carotid sinus denervation, and, in some cases, pacemaker implantation. Prevention of the heart rate response by pacing or atropine will not prevent the reflex hypotensive response in patients with both cardioinhibitory and vasodepressor components (18). Some patients with mixed carotid sinus hypersensitivity (eg, with both cardioinhibitory and vasodepressor response patterns) may require treatment with anticholinergic and alpha-adrenergic medications in combination with carotid sinus denervation.
Patients with swallow syncope associated with glossopharyngeal neuralgia may benefit from anticonvulsant therapy (eg, with carbamazepine or phenytoin) (15; 82; 70; 94). Surgical treatment of patients with swallow syncope and glossopharyngeal neuralgia may involve microvascular decompression or section of selected rootlets of the glossopharyngeal and vagus nerves (82). Some patients with swallow syncope, glossopharyngeal neuralgia, and Chiari type I malformation may require surgical decompression with suboccipital craniectomy and resection of the posterior arch of C1 (02).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neurobehavioral & Cognitive Disorders
Jun. 17, 2026
Neuro-Oncology
May. 27, 2026
Neuropharmacology & Neurotherapeutics
May. 14, 2026
General Neurology
May. 13, 2026
Neuro-Oncology
Apr. 30, 2026
Neuropharmacology & Neurotherapeutics
Apr. 23, 2026
Neuropharmacology & Neurotherapeutics
Apr. 20, 2026
Neurobehavioral & Cognitive Disorders
Apr. 08, 2026