








Behavioral & Cognitive Disorders
Academic underachievement
Apr. 18, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Korsakoff syndrome is marked by remote memory impairment and characteristic profound anterograde memory deficits, out of proportion to dysfunction in other cognitive domains, in a fully alert and responsive person. Korsakoff syndrome typically results from a deficiency of thiamine and has a characteristic pathology, making it a specific disease condition, Korsakoff disease. Korsakoff disease is most commonly associated with chronic alcohol abuse, but it can also result from nonalcohol-related malnutrition or malabsorption. An inherited insensitivity to thiamine has been proposed as a risk factor for alcoholism and Wernicke-Korsakoff syndrome. Successful treatment of established Korsakoff disease is infrequent, and memory impairment may be profound and chronic. Clinically, similar disorders of memory can occur with other etiologies and pathologies (eg, head trauma, anterior communicating aneurysm rupture, herpes encephalitis), and these have been referred to with various terms (eg, Korsakowian syndrome, mental syndrome of Korsakoff, amnestic syndrome, etc.), but they could reasonably be included under the umbrella of Korsakoff syndrome (ie, as distinct from the specific disease entity, Korsakoff disease).
• The main clinical characteristic of Korsakoff syndrome is a disproportionate impairment in memory compared to other cognitive functions. | |
• Korsakoff syndrome typically results from a deficiency of thiamine and has a characteristic pathology, making it a specific disease condition, Korsakoff disease. | |
• Korsakoff disease is frequently associated with chronic alcohol abuse, but it has also been observed in the context of several other conditions that cause malnutrition or malabsorption. | |
• Treatment with thiamine may partially improve memory impairment in some patients with Korsakoff disease. |
Russian neuropsychiatrist Sergei Sergeievich Korsakoff (sometimes spelled Korsakov; 1853/1854-1900) described a persistent amnestic confabulatory state that became known as Korsakoff psychosis, or Korsakoff syndrome, the chronic state of the spectrum of the Wernicke-Korsakoff syndrome or Wernicke-Korsakoff encephalopathy (85; 86; 87; 181; 179; 176; 91; 92; 93). In a series of three articles from 1887 to 1889, Korsakoff gave a comprehensive description of a cognitive disorder now known as Korsakoff psychosis, occurring in conjunction with peripheral polyneuropathy, a combination he initially labeled either as “psychosis associated with polyneuritis” or “polyneuritic psychosis” (85; 86; 87; 181; 179; 91; 92; 93). In 1887, Korsakoff initially felt that the cognitive disorder and the polyneuropathy represented “two facets of the same disease…The pathologic cause provoking multiple neuritis may affect several parts of the nervous system, central as well as peripheral, and according to where this cause is localized there will be symptoms either of neuritis or of the brain” (92; 93). By 1889, Korsakoff recognized that the peripheral neuropathic symptoms “may be so slight that the whole disease manifests itself exclusively by psychic symptoms.” Therefore, he concluded that “one might also call it psychosis polyneurotica, but using this designation one must remember that an identical psychic disturbance may occur also in cases in which the symptoms of multiple degenerative neuritis may be very slight or even entirely wanting” (92; 93). The associated polyneuropathy would now be recognized as beriberi, a nutritional neuropathy caused by thiamine deficiency.
Korsakoff noted the characteristic problems in new learning (anterograde amnesia) as well as the deficits in remembering past events (retrograde amnesia), and he emphasized that these occurred in the context of clear attention and consciousness. Although the eponym of Korsakoff psychosis is now often used to indicate the combination of anterograde amnesia and confabulation (with or without neuropathy), Korsakoff originally described a much wider range of mental states in affected patients that often occurred sequentially and included an agitated delirium and an apathetic acute confusional state (92; 93). However, Korsakoff was particularly intrigued by the confabulatory amnestic state, which typically followed an agitated delirium (92; 93). Patients tended to confabulate, sometimes making up stories or events entirely, but more frequently confusing the temporal context of actually experienced events.
Korsakoff based his conclusions on at least 46 patients, about two thirds of whom were alcoholics, and the remainder suffered from a diverse group of disorders associated with protracted vomiting, including postpartum infections, intestinal obstruction, abdominal tumor, typhoid fever, and jaundice. Korsakoff believed the diverse underlying medical conditions that were associated with the disorder could all be “reduced to an incorrect constitution of the blood, developing under their influence and leading to an accumulation in the blood of toxic substances,” which could poison the nervous system; hence, his other appellation: “toxemic cerebropathy (cerebropathia psychica toxemica)” (92; 93). Despite his extensive clinical experience with this disorder, Korsakoff’s writings do not include a pathologic description of the disease because the patients he studied were, in fact, the chronic cases that had been selected for survival, whereas Wernicke encephalopathy was often fulminant, and, therefore, Wernicke was able to describe the associated pathology.
Korsakoff was apparently unaware of the syndrome incorporating a confusional state, ophthalmoparesis and other oculomotor findings, ataxia, and neuropathic features, which had been described by German neuropsychiatrist Carl Wernicke (1848-1905) in 1881 and labeled as “Die acute, hämorrhagische Poliencephalitis superior” (acute hemorrhagic superior poliencephalitis) and is now generally called Wernicke encephalopathy (183; 79; 80). This syndrome, as described by Wernicke, had an acute onset and a fulminant course, leading to death within 10 to 14 days. Korsakoff did mention that “sometimes there are ophthalmoplegia externa, nystagmus, and like manifestations,” but he did not attach any particular significance to these manifestations. Wernicke similarly did not appreciate the close relationship between the disorders that he and Korsakoff had described. In 1896, German neuropsychiatrist Hans Gudden (1866-1940) described atrophy of the mammillary bodies and other pathological changes in the brains of alcoholics with Korsakoff syndrome (56), but it was not until the early years of the 20th century that German neuropsychiatrist Karl Bonhöffer (1868-1948) recognized the close relationship between Korsakoff psychosis, delirium tremens, and Wernicke encephalopathy (14; 15). By 1904, Bonhöffer concluded that neuritis (ie, neuropathy) and a memory disorder were present in all patients with Wernicke encephalopathy (15).
The clinico-pathologic overlap between Wernicke encephalopathy and Korsakoff psychosis was ultimately recognized in the late 1920s and early 1930s (51; 75; 25). Some authors noted an amnestic disorder in all patients presenting with Wernicke encephalopathy and also found the characteristic brain stem pathology of Wernicke encephalopathy in all fatal cases of Korsakoff psychosis. In this same time period, careful pathological studies noted the selective distribution of symmetric lesions, including small dot-like hemorrhages, affecting the mamillary bodies, the grey matter immediately surrounding the third ventricle and involving the hypothalamus and the medial portion of the thalamus, the periaqueductal grey matter (including the oculomotor nuclei), the posterior colliculi, and less frequently the floor of the fourth ventricle. Specific histological changes in affected areas included hyperemia and small hemorrhages, proliferation of small blood vessels, relatively slight evidence of damage to nerve cells, and the absence of inflammatory infiltration.
In cases of alcoholic origin, the Diagnostic and Statistical Manual of Mental Disorder (DSM-IV) designation for Korsakoff syndrome is alcohol-induced persisting amnestic disorder (05), and the new DSM-V designation is “alcohol-induced major neurocognitive disorder, amnestic confabulatory type” (06). Clinically, among alcoholics, the term Korsakoff syndrome is limited to patients with a disproportionate disorder of memory, whereas the term alcoholic dementia is used for patients with a more global cognitive impairment (143). However, the nosological distinction between Korsakoff syndrome and alcoholic dementia is somewhat controversial because the clinical differentiation is imprecise and no distinct neuropathological basis has been established for alcoholic dementia (178). Indeed, some have concluded that alcohol-related cognitive disorders can more appropriately be seen as varying along a continuum of severity (18).
Korsakoff syndrome is marked by remote memory impairment and characteristic profound anterograde memory deficits, out of proportion to dysfunction in other cognitive domains, in a fully alert and responsive person. Korsakoff syndrome typically results from a deficiency of thiamine (ie, a recognized etiologic agent), and then has a characteristic pathology, making this constellation a specific disease condition, Korsakoff disease. Clinically, similar disorders of memory can occur with other etiologies and pathologies (eg, head trauma, anterior communicating aneurysm rupture, herpes encephalitis); these have been referred to with various terms (eg, Korsakowian syndrome, mental syndrome of Korsakoff, amnestic syndrome, etc.), but they could reasonably be included under the umbrella of Korsakoff syndrome (ie, as distinct from the specific disease entity, Korsakoff disease). However, a somewhat idiosyncratic use of the term “syndrome” has traditionally been applied with “Korsakoff syndrome,” and many authors continue to use this terminology for the specific disease condition in which the memory disorder results from thiamine deficiency with its consistent pathological alterations. The present chapter tries to maintain the distinction between a syndrome and a disease, where a syndrome is an aggregate of signs and symptoms associated with any morbid process, and a disease is a specific morbid process with an identifiable group of signs and symptoms, resulting from a recognizable etiologic agent, which produces consistent pathological alterations in tissues or organs.
• The cognitive and behavioral symptoms of Korsakoff syndrome include anterograde and retrograde amnesia, confabulation, executive dysfunction, apathy, and affective and social-cognitive impairments. | |
• The principal manifestation of Korsakoff syndrome is anterograde amnesia for both verbal and nonverbal information, but retrograde amnesia is also typical. | |
• Declarative memory (factual knowledge) is significantly impaired in Korsakoff syndrome, whereas procedural memory (motor learning) is relatively preserved. | |
• Confabulation may also occur, although primarily in the disorder’s acute (Wernicke) stage. | |
• The cognitive deficits outside of the memory domain that are most commonly noted in Korsakoff patients are deficits in planning, decision-making, and problem-solving and deficits linked to impaired frontal-executive control. | |
• The initial clinical presentation of Korsakoff syndrome is variable. Although often marked by the acute signs of Wernicke encephalopathy, the disorder can also have an insidious onset without clinical evidence of antecedent Wernicke encephalopathy. |
Korsakoff syndrome, the chronic state following inadequate or delayed treatment of Wernicke encephalopathy, is characterized by confabulation, memory loss, and gait abnormalities that are often irreversible (91; 92; 93; 79; 80; 134; 33). A diagnosis of Korsakoff syndrome should be reserved for those with cognitive impairments that are restricted to isolated or disproportionate memory impairment, whereas those with widespread cognitive impairment are best encompassed within the diagnostic categories of "alcohol-related brain damage" or "alcoholic cognitive impairment" (83).
The cognitive and behavioral symptoms of Korsakoff syndrome include anterograde and retrograde amnesia, confabulation, executive dysfunction, apathy, and affective and social-cognitive impairments (07).
The principal manifestation of Korsakoff syndrome is anterograde amnesia for both verbal and nonverbal information (45). Even in the face of multiple repetitions, patients cannot learn new names, faces, or facts and forget events that happened shortly before. These deficits are not due to an inability to attend to incoming information, as patients can repeat information without any delay. However, as soon as any distracting activity is interposed, the information is forgotten. This sensitivity to interference is the principal characteristic of the memory impairment and is thought to be due to a combination of two factors: (1) a failure to fully encode all the aspects of incoming information, and (2) a failure of retrieval, stemming from an inability to inhibit competition from irrelevant information (177). In addition, in Korsakoff syndrome, a disproportionately large encoding deficit is observed (130; 129).
Retrograde amnesia is also a typical feature of the disorder, commonly extending back 25 years or more. Memory for autobiographical information, as well as knowledge of public events and facts, is affected. A significant memory defect for contextual (spatial and temporal) information is also observed (77). Regardless of the nature of the information, memories from childhood and early adulthood are remembered better than memories from the recent past (136). This temporal gradient is markedly steeper than that seen in dementing disorders such as Alzheimer disease (81; 43). Retrograde and anterograde amnesia co-occur in Korsakoff syndrome, but the severity of these impairments is poorly correlated, suggesting that they reflect distinct underlying deficits.
Declarative memory (factual knowledge) is significantly impaired in Korsakoff syndrome, whereas procedural memory (motor learning) is relatively preserved (180). Korsakoff patients have compromised declarative memory functioning with the lowest performance with encoding compared to working memory and delayed recall (122). With respect to the content, visuospatial memory is relatively better preserved than verbal memory (122). Korsakoff patients also exhibit defects in involuntary conscious (or explicit) memory but less clearly in involuntary unconscious (or implicit) memory (40). However, when compared with alcoholic patients and control subjects, patients with Korsakoff syndrome do have lower cognitive procedural learning abilities (10) can learn a motor task only when directive feedback is provided (160). Regardless of the significant declarative (explicit) memory defect, patients with Korsakoff syndrome present a normal memory for implicit contextual information (ie, the ability to acquire contextual information from one’s surroundings without conscious awareness) (124). Visuoperceptual learning (eg, recognition of incomplete pictures) may be preserved (44). Some improvement in memory test performance is observed in Korsakoff syndrome patients when explanations and encouragement are provided and when additional processing and responding time are allowed (173).
Despite earlier beliefs that confabulation mainly occurs in the post-acute phase, confabulations may be present throughout the course of Korsakoff syndrome (123). Two types of confabulation can be distinguished: provoked or spontaneous (98). The former is more frequently observed in Korsakoff syndrome. Spontaneous confabulation involves an unprovoked outpouring of unrealistic episodic autobiographical claims (17; 55). These may represent patients’ tendency to fill in gaps in memory when faced with questions they cannot answer. Less commonly, patients will spontaneously tell bizarre, unrealistic stories. But in general, patients confabulate in response to questions about experiential (episodic) memory and questions to which the answer is unknown (174). The presence and persistence of confabulation do not depend on the severity of the memory disorder, suggesting again that different mechanisms are involved. Furthermore, confabulation is not specific to Korsakoff syndrome but is seen in various patients with lesions in the frontal lobes, basal forebrain, or both. Confabulation is caused by disrupted cognitive processes needed for effective reality monitoring, such as temporal discrimination, source monitoring, and self-initiated memory retrieval (72). Impaired performance in temporal order memory (39), source memory (78), and working memory tasks (172) is also observed. When comparing cued recall (ie, retrieval of information from memory is facilitated by the provision of cues) and recognition memory (ie, ability to recognize previously presented items) in Korsakoff patients, unilateral medial-temporal lobectomy patients, and normal controls, Korsakoff patients present a general memory deficit in both the cued recall and the recognition condition, and the degree of memory impairment is greater in Korsakoff syndrome than in the patients following medial-temporal lobectomy (167).
The cognitive deficits outside of the memory domain that are most noted in Korsakoff patients are deficits in planning, decision-making, and problem-solving and deficits linked to impaired frontal-executive control (19). Patients perform poorly on clinical tests of frontal function such as the Wisconsin Card Sorting test, verbal fluency, and Trails B (155; 68). Because the frontal lobes play an important role in the planning and initiation of systematic memory search, frontal deficits may contribute to the inability to retrieve premorbidly acquired information. Korsakoff patients are impaired on tests of memory, fluency, cognitive flexibility, and perseveration, and although non-Korsakoff alcoholics may also show some frontal-executive system deficits, these are generally milder (20; 121; 101). Brokate and colleagues investigated a sample of 17 patients with Korsakoff syndrome, 23 alcoholics without Korsakoff syndrome, and 21 controls with peripheral nerve diseases, all matched for intelligence and education (20); Korsakoff syndrome patients, but not the non-Korsakoff alcoholics, showed marked memory impairment and scored lower in each of the executive tasks. In a study of 16 chronic alcoholics without Korsakoff syndrome and 15 patients with Korsakoff syndrome, the Korsakoff subjects were significantly more impaired than the chronic alcoholics without Korsakoff syndrome in the Behavioural Assessment of the Dysexecutive Syndrome test (101). Korsakoff patients manifest marked impairments across all forms of past and future thinking as well as the generation of episodic details on an implausible event simulation task (69). Visuospatial and visual-perceptual deficits are observed in patients with Korsakoff syndrome on various concept formation tests that require discrimination and classification of complex visual stimuli (82). Personality changes are typical of Korsakoff syndrome. Korsakoff patients typically lack insight, are apathetic about ongoing events, and are unconcerned about personal appearance, but some reportedly have relatively preserved awareness of functional deficits (54). A lack of interest in alcohol is also striking.
The initial clinical presentation of Korsakoff syndrome is variable, although often marked by the acute signs of Wernicke encephalopathy; the disorder can also have an insidious onset without clinical evidence of antecedent Wernicke encephalopathy. Furthermore, a minority of patients who present with Wernicke encephalopathy do not develop Korsakoff syndrome and are left with only minimal cognitive deficits following recovery (180). Jauhar and Montaldi studied eight patients with Korsakoff syndrome; only four had a documented Wernicke episode (70). All subjects showed amnesia without a general intellectual deterioration. MRI abnormalities were similar in both groups (with atrophy of mammillary bodies and, to a lesser extent, the thalamus and cerebral cortex), and no MRI measure differentiated the groups. Cerebral blood flow was also similarly reduced in both groups, particularly to the anterior temporal regions bilaterally extending to the parietal lobes. Thus, patients with an insidious onset of Korsakoff syndrome have the same general pathological substrate as those with classical Wernicke-Korsakoff disease.
Although the acute neurologic signs associated with Wernicke encephalopathy usually recover, up to 60% of Korsakoff patients continue to show ocular and cerebellar signs. A slow, cautious/unsteady, wide-based gait and inability to walk tandem are typical.
Anaphylactic reactions thiamine formulations are quite rare (164).
The prognosis of Korsakoff syndrome (and more specifically of Korsakoff disease) is generally bleak, and most patients are left with a permanent and devastating memory disorder, even if other neurologic features (eg, nystagmus, ataxia, and neuropathy) may improve markedly or even recover completely (46; 163; 102). Some limited recovery of the amnestic disorder may occur within 1 to 3 months and may continue for up to 1 year or more (163). Only about 20% of patients make a substantial recovery (180). Patients' lack of insight further complicates their behavioral management. Patients may survive for many years, and their death is typically unrelated to the original neurologic disease. Cognitive test performance of detoxified alcoholic Korsakoff patients remains stable over at least 2 years; neither accelerated cognitive decline nor onset of dementia-like symptoms is observed (49).
In a cross-sectional study of 281 nursing home residents with Korsakoff syndrome from nine specialized nursing homes in the Netherlands, cognitive impairment, female gender, staying in a nursing home for at least 5 years, and impaired awareness were significantly associated with higher dependence in activities of daily living, whereas (oddly) chronic obstructive pulmonary disease was significantly associated with lower activities of daily living dependence (13).
Fluorodeoxyglucose positron emission tomography shows bilateral thalamic and severe bilateral temporal-parietal hypometabolism (46). Longitudinal assessment may reveal modest improvements in clinical state and neuropsychological performance that parallel improvements in cerebral glucose metabolism. In an anecdotal case, metabolic rates increased from 7% to 24% in cortical areas during a 9-month remission period, but thalamic glucose metabolism remained severely disturbed over time (46).
Alcohol-induced damage to the liver is a common comorbidity in patients with Korsakoff disease. Chronic liver dysfunction contributes to impaired cognitive performance in alcoholics (23), but to what extent it further exacerbates the deficits seen in Korsakoff disease is unclear. In approximately 15% of patients, decompensated liver disease is the primary cause of death. Other complicating factors derive from the alcoholic's hazardous lifestyle, including trauma, anoxia, and the effects of polydrug abuse or drug overdose. An increased frequency of diabetes mellitus in patients with Wernicke-Korsakoff syndrome has also been reported (186).
A right-handed white man with a 25-year history of alcohol abuse was hospitalized in April 1986 at 62 years of age with dehydration and malnutrition. He had been fired from his job earlier that month, which prompted increased alcohol consumption and exacerbated his poor diet. At the end of May, his son noted that he was more forgetful and that he was hallucinating and delusional. During the hospitalization, the patient was confused and agitated. He was diagnosed with acute Wernicke encephalopathy and treated with folic acid and thiamine. He was transferred to another hospital in November. During this time, he was severely disoriented and was unable to remember the location of his room or the reason for his hospitalization. He misestimated his age to be 35 years. He often confabulated, stating, for instance, that he was in the hospital for an appendectomy. He was then given a diagnosis of alcoholic Korsakoff disease.
Neurologic exam in November 1986 was significant, particularly for an abnormal mental status. He was alert but was only oriented to person. He did not know the date or the name of the hospital. His immediate span of attention was intact. He recalled three of three words without distraction after 30 seconds,but zero of three words after 5 minutes of intervening activity. He was unable to recall personal information that occurred in the recent past. He was unable to state the current president’s name, but he correctly stated that Franklin Delano Roosevelt had been president during World War II. Serial neuropsychological evaluations revealed a consistent pattern of deficits, particularly affecting aspects of memory. His anterograde amnesia was extremely dense and disproportionate to his other cognitive deficits. Performance on all measures of new learning was severely impaired. He also demonstrated extensive retrograde amnesia; he had difficulty recalling autobiographical events in response to verbal cues. His recall of famous individuals conformed to the classic Korsakoff pattern, with better recall of remote versus recent individuals. In addition, he demonstrated low-average performance on tests of intelligence. He performed normally on tests of simple attention, but on more complex attentional tasks, his performance was slow and characterized by frequent perseverations. Basic language skills were relatively preserved, although he had some problems with confrontation naming. Basic perceptual abilities were intact, but he performed tasks requiring visuospatial integration poorly. Other neurologic examination findings included bilateral end-point nystagmus, mild dysmetria on finger-to-nose testing, dysdiadochokinesis, mild ataxia with tandem gait, absent ankle jerks, and decreased pinprick sensation in his feet.
He was admitted to long-term care in 1989, where he remained until his death in 1992. During this period, he remained abstinent from alcohol. He led a rather isolated existence, was apathetic with regard to daily activities, and demonstrated limited insight into his medical condition.
|
• Korsakoff syndrome usually results from a deficiency of thiamine (vitamin B1) and leads to consistent pathological changes in the brain, making this constellation of clinical findings, etiologic agent, and pathology a specific disease condition, Korsakoff disease. | |
|
• Korsakoff disease has also been described in the context of several other disorders that can cause malnutrition or malabsorption, or in some cases, a potential increase in metabolic requirement for thiamine. | |
|
• In alcoholic Korsakoff disease, direct neurotoxic effects of alcohol on cortical association areas may be responsible for the visuoperceptual and problem-solving deficits seen in Korsakoff patients as well as in nonamnesic chronic alcoholics. | |
|
• Bilateral, symmetrically placed, punctate lesions in the area of the third ventricle, fourth ventricle, and aqueduct are the hallmarks of Korsakoff disease. |
Korsakoff syndrome usually results from a deficiency of thiamine (vitamin B1) and leads to consistent pathological changes in the brain, making this constellation of clinical findings, etiologic agent, and pathology a specific disease condition, Korsakoff disease. Korsakoff disease is mostly associated with chronic alcohol abuse, in which case low dietary intake of thiamine is compounded by alcohol-induced impairments in thiamine absorption and metabolism (156; 148; 192). There may also be a contribution from an age-related vulnerability to diencephalic amnesia produced by thiamine deficiency (133).
Korsakoff disease has also been described in the context of several other disorders that can cause malnutrition or malabsorption or, in some cases, a potential increase in metabolic requirement for thiamine (Table 1). Compared to alcohol-related Korsakoff disease, nonalcoholic Korsakoff disease is associated with female gender, younger age, shorter duration of precipitating illness, and better survival rates (145).
|
• Alcoholism (85; 86; 87; 181; 179) | ||
|
- Hyperemesis gravidarum (01; 191; 117; 111) | ||
|
• Gastrointestinal obstruction (eg, pyloric stenosis) (85; 86; 87; 181; 179; 35; 38) | ||
|
- Small bowel obstruction and paralytic ileus (35) | ||
|
• Starvation (142; 58) | ||
|
- Hunger strike (142) | ||
|
• Psychiatric disorders | ||
|
- Psychotic disorder (58; 04) | ||
|
- Depression (36) | ||
|
- Social withdrawal syndrome (hikikomori syndrome) (162) | ||
|
• Psychiatric disorders | ||
|
• Dialysis (113) | ||
|
- Gastrointestinal tract malignancies (85; 86; 87; 181; 179; 118; 66; 38) | ||
|
• Infections | ||
|
- Typhoid fever (Korsakoff, 1887, 1889a; Korsakoff, 1887, 1889b; 181; 179) | ||
|
• Chronic subdural hematoma (64) | ||
Caine and colleagues performed a systematic literature review of reports of Wernicke encephalopathy reported in nonalcoholic subjects (24) (Table 2). More than half of the 625 cases identified were associated with cancer (18%), gastrointestinal surgery (17%), hyperemesis gravidarum (12%), or starvation/fasting (10%) (24).
|
Clinical condition |
Percent of reported cases |
|
Cancer |
18 |
|
Gastrointestinal surgery |
17 |
|
Hyperemesis gravidarum |
12 |
|
Starvation/fasting |
10 |
|
Gastrointestinal tract disease |
8 |
|
AIDS |
5 |
|
Malnutrition |
4 |
|
Dialysis and renal diseases |
4 |
|
Parenteral nutrition |
4 |
|
Protracted vomiting |
2 |
|
Psychiatric diseases |
2 |
|
Stem cell or bone marrow transplantation |
2 |
|
Other |
8 |
|
Unknown |
3 |
|
| |
In alcoholic Korsakoff disease, direct neurotoxic effects of alcohol on cortical association areas may be responsible for the visuoperceptual and problem-solving deficits seen in Korsakoff patients as well as in nonamnesic chronic alcoholics (22). However, the relationship between frontal dysfunction and alcohol abuse per se is unclear because frontal deficits have also been observed in nonalcoholic Korsakoff disease. This suggests that diencephalic lesions may also cause or contribute to cortical dysfunction. Others have suggested that Korsakoff disease might produce cognitive dysfunction by disconnecting cerebello-cerebral pathways in brain areas known to be affected in Wernicke encephalopathy (184).
When comparing brain structure volumes on MRI in patients with Korsakoff disease, patients with chronic alcoholism without Korsakoff syndrome, and healthy control subjects, the patients with alcoholism without Korsakoff syndrome had normal cognitive performance and normal brain structure volumes, whereas the patients with Korsakoff disease had performance deficits on tests of memory, visuoperception, and executive functions as well as reduced brain structure volumes (88); these results suggest that the cognitive deficits cannot be ascribed solely to chronic consumption of alcohol.
Vulnerability to Korsakoff disease is highly variable. Among alcoholics with extensive drinking histories and malnutrition, only a minority develop the disease. A genetic predisposition to impaired thiamine metabolism has been postulated in individuals with Korsakoff disease (57), particularly to the possibility of abnormalities in the metabolism of transketolase, an enzyme that requires the active form of thiamine, thiamine pyrophosphate, as a cofactor (107). A subgroup of patients may be predisposed to more severe brain damage due to abnormalities in the transketolase enzyme (61). Manzardo and Penick proposed that an inherited insensitivity to thiamine can precipitate brain abnormalities early in life that will increase the risk of developing alcoholism and Wernicke-Korsakoff syndrome in adulthood (104).
Bilateral, symmetrically placed punctate lesions around the third ventricle, fourth ventricle, and aqueduct are the hallmarks of Korsakoff disease. Lesions in the midbrain and cerebellum are responsible for the neurologic symptoms of the Wernicke stage, whereas lesions in the diencephalon (including the mammillothalamic tract) are critical for the amnesia that characterizes Korsakoff disease (189; 188). The characteristic neuropathology of Korsakoff disease includes neuronal loss, microhemorrhages, and gliosis in the paraventricular and peri-aqueductal grey matter. Interactions involving the thalamus, mammillary bodies, hippocampus, frontal lobes, and cerebellum are important for new memory formation and executive function; the impairment of these circuits significantly contribute to the cognitive defects found in Korsakoff disease (74; 132). However, the minimal lesion(s) necessary for severe amnesia has not been resolved. Victor and colleagues suggested that damage to the dorsomedial nucleus of the thalamus is essential in the causation of memory deficits of Korsakoff disease (180), whereas others have implicated both the mammillary bodies and other thalamic nuclei in the anterior and midline areas, including the preretinal nucleus (103; 22; 84; 89).
A comparison of MRI data from Korsakoff disease patients, alcoholic patients without Korsakoff syndrome, and healthy control subjects revealed considerable similarities in the pattern of gray and white matter damage in the first and second groups, although some cerebral regions, including the medial thalami, mammillary bodies, and corpus callosum, were more severely damaged in patients with Korsakoff disease than in alcoholic patients without Korsakoff syndrome (131). Volumetric MRI analyses revealed thalamic, mammillary body, and variable frontoparietal atrophy in Wernicke-Korsakoff patients, with relative sparing of medial temporal lobe structures (138; 151; 71). However, shrinkage of the mammillary bodies and frontal lobes is visible on MRI for both patients with Korsakoff disease and nonKorsakoff alcoholics (68; 41), even if it tends to be more severe in those with Korsakoff disease. However, volumetric decreases in the anterior diencephalon appear selectively among Korsakoff patients (71; 149). Further evidence for cortical dysfunction in Korsakoff disease comes from functional imaging studies, which have demonstrated widespread depression of metabolism in major portions of the frontal and parietal lobes as well as in the cingulate gyrus (73; 126). Periaqueductal and periventricular gray matter and collicular bodies are also affected in Korsakoff disease (159). Using structural MRI volumetric analysis in patients with organic amnesia (ie, Korsakoff syndrome, herpes encephalitis, and focal frontal lesions), patients with Korsakoff disease show decreased thalamic measurements but no significant changes in the medial temporal lobes, whereas patients with herpes encephalitis show severe medial temporal but not thalamic atrophy, and patients with frontal lobe lesions show reduced frontal lobe volume but no significant temporal lobe or thalamic atrophy (31).
Among patients with permanent amnesia (ie, Wernicke-Korsakoff encephalopathy or postanoxia syndrome) studied with positron emission tomography, permanent amnesia, regardless of the cause of amnesia, was associated with hypometabolism in the thalamus, posterior cingulate cortex, and mesial prefrontal cortex (near the anterior cingulate gyrus) bilaterally, as well as in the left supramarginal and middle temporal gyri (09).
Anterograde amnesia in Korsakoff syndrome may be the expression of damage to an extended hippocampal system. In a Wernicke-Korsakoff patient, no hippocampal activation was observed during either encoding or recognition on tests of episodic memory for faces using functional MRI, whereas in controls, both the encoding and recognition tasks activated anterior and posterior hippocampal regions (28). Although the damage in Wernicke-Korsakoff syndrome did not involve the medial temporal lobe, the hippocampal memory encoding was absent.
Anterograde amnesia in Wernicke-Korsakoff encephalopathy is associated with a disconnection between diencephalic and hippocampal structures (114). Korsakoff disease patients, but not alcoholic patients without Korsakoff syndrome, showed (1) absence of early, left medial temporal lobe-dependent positive evoked potentials following immediate picture repetitions (during a continuous picture recognition task) and (2) disruption of the fornix, which connects diencephalic and hippocampal structures (as assessed using diffusion tensor imaging) (114).
Ataxia and cerebellar signs may be also observed in alcoholics with or without Korsakoff syndrome, and these clinical manifestations are associated with changes in the volume of tissue in the cerebellar hemispheres and also with gray and white matter volume deficits in anterior superior but not posterior inferior vermis (158; 95). The regional distribution of cerebellar volume deficits is similar in alcoholic individuals whether or not they are complicated by Korsakoff syndrome (158). By MRI, alcoholics without Korsakoff syndrome may have gray but not white matter cerebellar hemisphere volume deficits, whereas alcoholic patients with Korsakoff syndrome have deficits in both tissue types. Ataxia in Korsakoff disease has also been associated with elevated cerebellar glucose metabolism (47).
The pathogenic mechanism determining the formation and distribution of brain lesions in Korsakoff disease is not fully understood. Thiamine is intimately involved in several enzymatic reactions essential for glucose metabolism and neurotransmitter reactions. Animal studies of thiamine deprivation suggest that reductions in thiamine-dependent enzymes trigger a series of metabolic events, including decreased intracellular energy levels, increased histamine release, glutamate accumulation, and, ultimately, cell death. Diencephalic areas may be especially vulnerable because of their high energy demand (90). Alternatively, glutamate may accumulate in peripheral tissues and reach a concentration in the blood at which it passes into cerebral ventricles and contiguous brain areas, thus, preferentially affecting periventricular brain tissues (108).
Although several neurotransmitter systems are affected by thiamine deprivation, it is unclear which neurotransmitters are implicated in Korsakoff amnesia. Significant reductions in 3-methoxy-4-hydroxyphenylglycol, the primary metabolite of norepinephrine, have been demonstrated in the CSF of Korsakoff disease patients, and the magnitude of this reduction is correlated with the severity of memory impairment (110; 109). Administration of the norepinephrine agonist clonidine had a beneficial effect on performance on a small number of anterograde memory tests, but these findings have been difficult to replicate (120). Serotonin has also been implicated, and modest improvements in memory were reported with the administration of the serotonin uptake inhibitor fluvoxamine (106). Finally, because of its known role in memory, the possible contribution of acetylcholine depletion in Korsakoff amnesia has been addressed. Thiamine deprivation does affect acetylcholine synthesis, and a reduction in neurons in the cholinergic basal forebrain has been described in at least some Korsakoff patients. However, cholinergic dysfunction does not account for the memory disorder, and the degree of damage to the cholinergic system is insufficient to cause the persisting amnesia in Wernicke-Korsakoff syndrome (115).
Conditions that impact the same brain structures as those affected in the Korsakoff disease can produce a similar disorder clinically, even if the pathogenesis is different and does not specifically involve a disturbance of thiamine metabolism. For example, head trauma with bilateral lesions of the limbic circuit may result in a memory disorder resembling Korsakoff psychosis, which is frequently referred to as a traumatic "Korsakowian syndrome" (or “Korsakovian syndrome”) or the "mental syndrome of Korsakoff" (21), but which may also be simply subsumed under the term Korsokoff syndrome (193). Acute Korsakoff-like syndromes have been reported, for example, from the combination of a left anteromedian thalamic infarct and a right hippocampal hemorrhage (137), from bilateral infarction of intralaminar and dorsomedial thalamic nuclei due to occlusion of the artery of Percheron (193), from infarction of the right thalamus involving the right mamillothalamic tract (188), and from ischemic stroke of the fornix and genu of the corpus callosum (12).
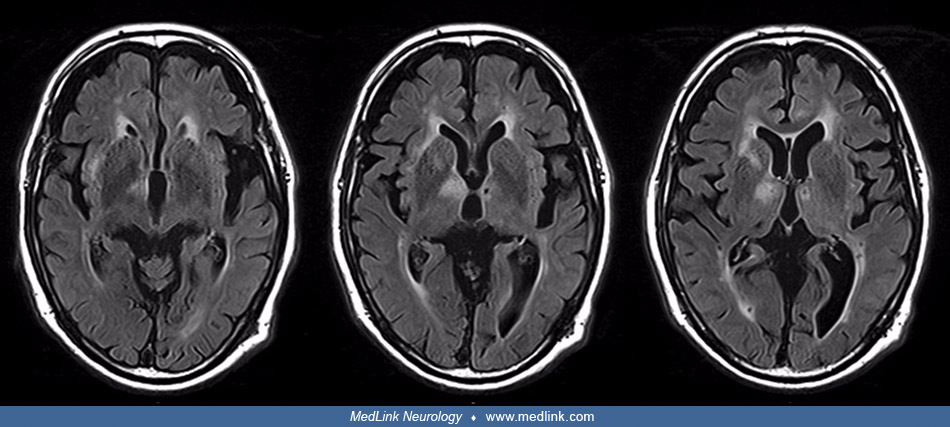
A 97-year-old man presenting with acute-onset “vascular” Korsakoff syndrome with bilaterally damaged mammillothalamic tracts. Diffusion-weighted images on admission showed fresh cerebral infarction in the right thalamus involvi...
A 97-year-old man presenting with acute-onset “vascular” Korsakoff syndrome with bilaterally damaged mammillothalamic tracts. T2-weighted images revealed a microbleed scar over the left mammillothalamic tract. (Source: Yoneoka ...
A 97-year-old man presenting with acute-onset “vascular” Korsakoff syndrome with bilaterally damaged mammillothalamic tracts. Fluid attenuation inversion recovery (FLAIR) images confirmed bilateral lesions of both mammillothala...
A 97-year-old man presenting with acute-onset “vascular” Korsakoff syndrome with bilaterally damaged mammillothalamic tracts. In the enlarged images, (A) infarction is shown over the right mammillothalamic tract; (B) a microble...
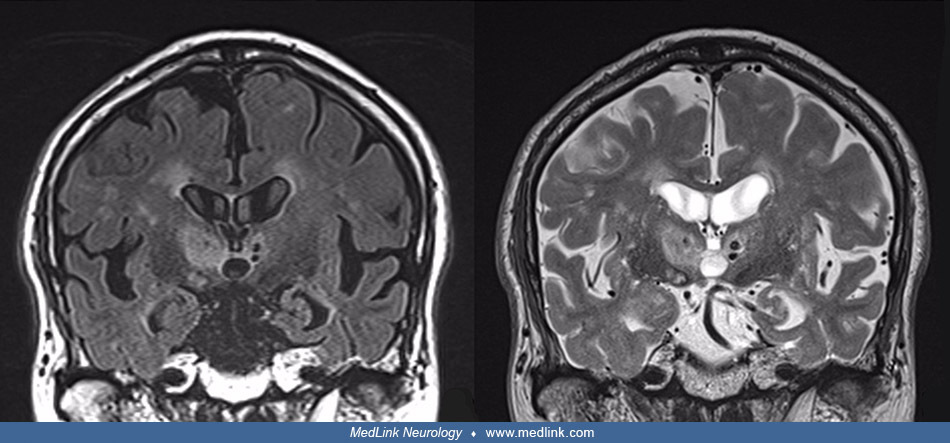
Coronal images confirm bilateral symmetrical locations of the mammillothalamic tract lesions. The right mammillothalamic tract infarction in this 97-year-old man is located between the right mammillary body and the right anteri...
Four patients have been reported with reversible Korsakoff syndromes caused by suprasellar retrochiasmatic lesions compressing the mammillary bodies and adjacent caudal hypothalamic structures (144); three of the patients had pituitary macroadenomas, whereas the fourth had a large cystic craniopharyngioma filling the third ventricle and compressing the midline diencephalic structures. Herpes encephalitis and cytomegalovirus may cause a similar clinical picture (168; 169; 26).
|
• The incidence of Korsakoff disease has been estimated at approximately 10 per million first psychiatric admissions. | |
|
• Several large autopsy studies have found neuropathological changes consistent with Wernicke-Korsakoff syndrome in 2% to 3% of postmortem examinations, suggesting a much higher prevalence of this syndrome. | |
|
• A majority of cases found to have neuropathological changes consistent with Wernicke-Korsakoff syndrome on postmortem examination were never clinically diagnosed with Wernicke-Korsakoff syndrome during life. | |
|
• The low concordance between clinical and pathological diagnosis of Wernicke-Korsakoff syndrome may result from a combination of factors: (1) underrecognition of the disorder by clinicians; (2) pathological changes occurring with subclinical disease; and (3) Wernicke-Korsakoff encephalopathy superimposed on a more general dementia picture. |
The incidence of Korsakoff disease has been estimated at approximately 10 per million first psychiatric admissions (29). However, several large autopsy studies have found neuropathological changes consistent with Wernicke-Korsakoff syndrome in 1% to 3% of postmortem examinations, suggesting a much higher prevalence of this syndrome (170; 60; 50). Most of these cases were never clinically diagnosed with Wernicke-Korsakoff syndrome during life (170; 50). A systematic review of autopsy series found a wide range for the proportion of cases of Wernicke encephalopathy who were diagnosed antemortem: overall 32% of alcoholics with Wernicke encephalopathy on postmortem examination had this diagnosed antemortem (87 of 273 autopsy-confirmed cases), and only 6% of nonalcoholics with Wernicke encephalopathy on postmortem examination had this diagnosed antemortem (2 of 35 cases) (50). A retrospective review of medical records of autopsy-confirmed Wernicke-Korsakoff syndrome cases found that less than 16% exhibit all three symptoms of the classical clinical triad (ie, encephalopathy, ataxia, and ophthalmoplegia) during the acute phase immediately before death (60). The low concordance between clinical and pathological diagnosis of Wernicke-Korsakoff syndrome may result from a combination of factors: (1) underrecognition of the disorder by clinicians; (2) pathological changes occurring with subclinical disease (175); and (3) Wernicke-Korsakoff encephalopathy superimposed on a more general dementia picture.
|
• Thiamine supplementation of some staple food products (eg, flour) is an easy and safe measure that can potentially improve the thiamine reserve of different human groups and function as a means of primary prevention of thiamine-deficiency disorders. | |
|
• Because alcohol abuse is the primary cause of Korsakoff disease, moderation of or abstinence from alcohol is an important preventative measure; however, because alcoholics often have multiple presentations with thiamine-deficient states and because they often present after significant neurologic damage has occurred, prevention opportunities are constrained even with optimal recognition and medical management. | |
|
• The possibility of thiamine deficiency should be considered carefully in all patients with a history of alcoholism, malnutrition (eg, anorexia nervosa), or protracted vomiting (eg, hyperemesis gravidarum), with an emphasis on low-threshold diagnosis and prompt treatment. | |
|
• In patients with Wernicke encephalopathy, rapid and aggressive treatment with parenteral thiamine is critical to prevent progression to Korsakoff disease and also to prevent fatal outcomes. This should be done before administration of glucose-enriched fluids. |
Thiamine supplementation of some staple food products (eg, flour) is an easy and safe measure that can potentially improve the thiamine reserve of different human groups and function as a means of primary prevention of thiamine-deficiency disorders (59).
Because alcohol abuse is the primary cause of Korsakoff disease, moderation of or abstinence from alcohol is an important preventative measure. However, because alcoholics often have multiple presentations with thiamine-deficient states and often present after significant neurologic damage has occurred, prevention opportunities are constrained even with optimal recognition and medical management. The possibility of thiamine deficiency should be considered carefully in all patients with a history of alcoholism, malnutrition, or protracted vomiting, with an emphasis on low-threshold diagnosis and prompt treatment (190). Recognition and treatment of maternal Wernicke-Korsakoff syndrome (eg, with hyperemesis gravidarum) can decrease the frequency of chronic neurologic sequelae and also the number of maternal deaths (182). Similarly, earlier recognition and treatment of Wernicke-Korsakoff syndrome in patients with anorexia nervosa can decrease the frequency of chronic neurologic sequelae in such patients (125).
In patients with Wernicke encephalopathy, rapid and aggressive treatment with parenteral thiamine is critical to prevent progression to the Korsakoff disease and also to prevent fatal outcomes. This should be done before administration of glucose-enriched fluids. Given proper vitamin supplementation, the confusional state seen in Wernicke encephalopathy typically clears, with marked improvement or resolution of the oculomotor manifestations, ataxia, and peripheral neuropathy (beriberi) (150). Effective treatment and prophylaxis may only be achieved using parenteral vitamin supplements because oral supplements may not be adequately absorbed (32). Unfortunately, evidence is still insufficient to decide the exact dose, frequency, or duration of thiamine treatment to prevent or treat Wernicke-Korsakoff syndrome associated with alcohol abuse (34; 65). Thiamine repletion with at least 100 to 200 mg/day intravenously or intramuscularly is recommended (62), and some advocate for much more aggressive initial treatment regimens of 1000 mg or more daily, particularly for the first 3 to 5 days and as long as 2 months (11; 65). Paparrigopoulos and colleagues reported a case of complete recovery from undertreated Wernicke-Korsakoff syndrome following aggressive thiamine treatment (600 mg/day orally and 300 mg/day intramuscularly) in a 52-year-old man with a 10-year history of heavy alcohol abuse (127). Bilici and colleagues reported significant improvement with intensive thiamine treatment (1000 mg daily intravenously) in a 40-year-old man with Wernicke-Korsakoff encephalopathy presenting 1 year after onset of symptoms; he was able to return to his normal life and regained most of his motor and cognitive abilities (11). Infante and colleagues similarly report gradual cognitive and behavioral improvement and brain MRI normalization in two patients using large doses of parenteral thiamine (900 to 1200 mg/d for 1 to 2 months, gradually reducing dosage after clinical and radiological improvement, and maintaining 200 mg/d intramuscularly for at least 1 year) (65).
In a North American teaching hospital inpatient psychiatry unit, the prevalence of Caine-positive Wernicke-Korsakoff syndrome among 262 consecutive admissions was 12%; only about half (53%) of these were using alcohol at the time of admission (96). Patients with Caine-positive Wernicke-Korsakoff syndrome who completed a high-dose intravenous thiamine regimen demonstrated clinically significant neurocognitive improvement; the thiamine regimen employed was based on guidance from the Royal College of Physicians (London) Report (165; 166) and consisted of 400 mg three times on day 1, and 200 mg once daily on days 2 to 4 (96).
Ishibashi and colleagues reported that the acute axonal polyneuropathy (ie, beriberi) associated with Wernicke-Korsakoff encephalopathy can improve within 2 weeks after intravenous thiamine infusion (67). More typically, the peripheral neuropathic manifestations improve slowly over a period of months so that many are walking fairly normally within 6 months (150).
Few studies have compared neuropathology in different periods at the same institution to assess whether there have been changes in the recognition and management of Wernicke encephalopathy. In an autopsy study from Norway, the authors compared two time periods (1975–1979 and 1983–1987) and found a considerable, albeit not statistically significant, reduction of the frequency of active and inactive Wernicke encephalopathy in alcoholics, suggesting that diagnostic and therapeutic procedures had improved over this time interval (97).
Persistent global amnesia can occur as a consequence of a number of neurologic disorders, including cerebrovascular accidents, rupture, and surgical repair of anterior communicating artery aneurysms, encephalitis, and anoxia. The presentation of the amnesic syndrome may be strikingly similar regardless of etiology; therefore, these neurologic conditions should all be considered in the differential diagnosis. Traumatic brain injury may occasionally result in a selective memory disorder as well. Because patients under the influence of alcohol are prone to head injury from falls and other accidents, it is important to rule out a traumatic etiology.
A careful history of alcohol consumption and nutritional status is of primary importance in the differential diagnosis. A history of Wernicke encephalopathy allows a confident diagnosis of Korsakoff disease as a chronic sequela, but Korsakoff disease can occasionally occur without signs of a preceding Wernicke encephalopathy. Attention to the course of illness is critical because the memory disorder seen in Alzheimer disease is progressive, whereas it is stable in established Korsakoff disease.
Severe memory disorders can also be seen in the context of more global intellectual deterioration. A diagnosis of alcoholic dementia is warranted if patients demonstrate, in addition to amnesia, severe deficits in conceptual and problem-solving abilities as well as marked impairments on visuospatial and visuo-constructive tasks (143; 139). In contrast to the acute onset of Korsakoff disease, the global cognitive deficits seen in alcoholic dementia usually develop more gradually.
|
• Korsakoff disease is a clinical diagnosis based on the identification of the characteristic amnesic syndrome, usually following an episode or episodes of Wernicke encephalopathy and occurring in the context of a history of alcohol abuse, malnutrition, or protracted vomiting. | |
|
• A diagnosis of Korsakoff disease can be made only when the confusional state associated with Wernicke encephalopathy has sufficiently cleared. | |
|
• A diagnosis of Korsakoff syndrome (or, more specifically, of Korsakoff disease) is warranted only when memory deficits are much more prominent than other cognitive disorders in language, visuoperceptual functioning, problem-solving, and judgment. | |
|
• Repeated episodes of subclinical Wernicke encephalopathy, or episodes of frank but unrecognized Wernicke encephalopathy, may cause Korsakoff syndrome, leaving patients with debilitating permanent memory impairments. | |
|
• Laboratory testing is routinely performed with special attention to folate and thiamine levels, tests of electrolytes (including magnesium), and liver function studies. | |
|
• Magnesium is a cofactor for some thiamine-dependent enzymes, and magnesium deficiency (common in alcoholics) can exacerbate manifestations of thiamine deficiency, impair treatment with thiamine, and negatively impact clinical outcomes. | |
|
• Computed tomography or MRI is useful in ruling out other causes of amnesia, such as stroke, tumor, or contusion. The presence of hemorrhagic lesions surrounding the third and fourth ventricle, however, does not in itself allow differentiation between Korsakoff disease and alcoholic dementia. |
The Caine criteria for Wernicke-Korsakoff syndrome include two or more of the following conditions: (1) dietary deficiency, (2) delirium or memory impairment, (3) cerebellar dysfunction/ataxia, and (4) oculomotor abnormalities (24; 50). These criteria are broader and more sensitive than applying the classic triad for diagnosis of Wernicke encephalopathy but really focus on Wernicke encephalopathy. Their utility is in recognizing Wernicke encephalopathy when it might not otherwise be considered or recognized, thereby allowing time for aggressive treatment to prevent Korsakoff disease.
Korsakoff disease is a clinical diagnosis based on the identification of the characteristic amnesic syndrome, usually following an episode or episodes of Wernicke encephalopathy and occurring in the context of a history of alcohol abuse, malnutrition, or protracted vomiting. A diagnosis of Korsakoff disease can be made only when the confusional state associated with Wernicke encephalopathy has sufficiently cleared. All cognitive functions should be thoroughly evaluated to characterize the pattern and severity of the memory disorder and to screen for the possibility of a general intellectual decline. A diagnosis of Korsakoff syndrome (or, more specifically, of Korsakoff disease) is warranted only when the memory deficits are much more prominent than other cognitive disorders in language, visuoperceptual functioning, problem-solving, and judgment.
Arts and colleagues proposed a definition of Korsakoff syndrome (07):
|
[Korsakoff syndrome] is a largely irreversible residual syndrome, caused by severe thiamine deficiency and occurring after incomplete recovery from a Wernicke encephalopathy, predominantly in the context of alcohol abuse and malnutrition, characterized by an abnormal mental state in which episodic memory is affected out of all proportion to other cognitive functions in an otherwise alert and responsive patient, whose psycho-logical make-up may be further distinguished by executive dysfunction, fattened affect, apathy, lack of illness insight, and possibly by fantastic confabulations in the early stage. |
Repeated episodes of subclinical Wernicke encephalopathy, or episodes of frank but unrecognized Wernicke encephalopathy, may cause Korsakoff syndrome, leaving patients with debilitating permanent memory impairments (117). When the episodes are seen later at the time of a Korsakovian state, patients may not show an obvious confabulatory tendency as this often subsides over time. Therefore, the absence of prior diagnoses of Wernicke encephalopathy certainly does not exclude the diagnosis of Korsakoff disease. Korsakoff syndrome should be considered in patients with long-term memory impairment who are seen in a psychiatric context, and such patients should be evaluated for previously unrecognized Wernicke encephalopathy.
A complete history should be taken with particular emphasis on alcohol use and nutritional status, protracted vomiting or diarrhea, evidence of an acute episode of Wernicke encephalopathy, and any associated features. Information should also be obtained regarding other medical conditions that may be part of the differential diagnosis (eg, encephalitis, anterior communicating artery aneurysm, head injury, tumor) or that may be precipitating conditions (ie, contributing to the development of thiamine deficiency). A complete physical and neurologic examination is necessary.
A diagnosis of nonalcoholic Korsakoff syndrome is not often considered in patients with memory impairments, and, in particular, for patients seen in a psychiatric context, there is a tendency to attribute evident memory abnormalities to a cognitive manifestation of a suspected underlying psychiatric disorder or the effects of psychotropic medications (117).
Laboratory testing is routinely performed with special attention to folate and thiamine levels, tests of electrolytes (including magnesium), and liver function studies. Magnesium is a cofactor for some thiamine-dependent enzymes, and magnesium deficiency (common in alcoholics) can exacerbate manifestations of thiamine deficiency, impair treatment with thiamine, and negatively impact clinical outcomes.
Computed tomography or MRI is useful in ruling out other causes of amnesia, such as stroke, tumor, or contusion. The presence of hemorrhagic lesions surrounding the third and fourth ventricle, however, does not in itself allow differentiation between Korsakoff disease and alcoholic dementia. Lough reviewed 53 case reports of Wernicke encephalopathy published from 2001 to 2011 and found that 81% were nonalcohol-related (99). Korsakoff disease or long-term cognitive neurologic changes were reported in 28% of patients. In some cases (13%) MRIs were normal, and normal or high thiamine blood levels were found in 8% of patients. The author concluded that neither diagnostic tool can be relied on exclusively to confirm a diagnosis of Wernicke encephalopathy.
Electroencephalography is normal in approximately half the cases and is not typically useful for diagnosis.
|
• Based on anecdotal evidence, aggressive treatment with high-dose thiamine for a prolonged period is increasingly being employed, even in patients in the Korsakoff phase of Wernicke-Korsakoff encephalopathy. | |
|
• After maximum treatment benefits of thiamine repletion have been achieved, pharmacological approaches remain unable to overcome the severe memory deficits seen in these patients (although various anecdotal reports suggest some benefit of a wide range of pharmaceuticals, none have been confirmed). | |
|
• Some memory rehabilitation strategies may be helpful in Korsakoff syndrome patients, though results even in anecdotal reports are modest at best, and there are few controlled trials. |
The various somatic and psychiatric comorbid conditions of patients with Korsakoff syndrome and their behavioral and functional problems are compounded by poor self-awareness regarding health status and functioning. Patients with Korsakoff syndrome have limited ability to perform daily activities and limited social functioning. This makes management quite challenging, even with integrated case management.
Aggressive treatment with high-dose thiamine for a prolonged period is increasingly being employed, even in patients in the Korsakoff phase of Wernicke-Korsakoff encephalopathy (see Prevention). The evidence for this approach is anecdotal.
A double-blind, randomized controlled trial of 127 symptomatic subjects found no significant differences in outcomes for any dosage condition: 100 mg thrice daily, 300 mg thrice daily, or 500 mg thrice daily for 5 days (37). This study found no clear short-term benefit of high-dose thiamine over intermediate or lower doses of thiamine for treating cognitive and neurologic abnormalities related to Wernicke-Korsakoff syndrome. The authors concluded that "the absence of conclusive evidence for the superiority of high-dose thiamine supports a recommendation for patient-specific treatment, while ensuring that the potential impact[s] of other biochemical factors (eg, magnesium and other B vitamin deficiencies) are considered and corrected if necessary" (37).
After maximum treatment benefits of thiamine repletion have been achieved, pharmacological approaches remain unable to overcome the severe memory deficits seen in these patients. Although anecdotal reports of improvement have appeared following treatment with cholinesterase inhibitors (63; 27; 30), small controlled studies failed with donepezil (142) and rivastigmine (100). The serotonin-uptake inhibitor fluvoxamine maleate (100 to 200 mg/d) produced a small but significant improvement in episodic memory performance in some small double-blind crossover studies (157; 105; 106) but not in others (119). In the studies in which fluvoxamine was found to be helpful, improvements in episodic memory were significantly correlated with reductions in levels of cerebrospinal fluid 5-hydroxyindoleacetic acid, the main metabolite of serotonin, suggesting that facilitation of serotonergic neurotransmission may ameliorate the episodic memory failure in patients with Korsakoff syndrome (157; 105; 106). Some modest success was suggested with memantine in an anecdotal report (16) and in a small pilot trial (140), but this trial was methodologically limited and has not been replicated.
Some memory rehabilitation strategies may be helpful in Korsakoff syndrome patients, though results even in anecdotal reports are modest at best, and there are few controlled trials (173; 161; 02; 53; 146). For example, providing support for executive difficulties in Korsakoff syndrome patients, by allowing extra processing and retrieval time, additional explanation, and explicit encouragement, may improve the ability of such patients to encode and make use of semantic, contextual, and sequential information (173; 161; 02).
In a study that highlights the potential of using smartwatches as external memory aids for Korsakoff patients in everyday life, smartwatch reminders proved as effective as verbal reminders in patients with Korsakoff syndrome (153).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD FAAN MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Behavioral & Cognitive Disorders
Apr. 18, 2024
Behavioral & Cognitive Disorders
Apr. 17, 2024
Behavioral & Cognitive Disorders
Mar. 29, 2024
Neuroimmunology
Mar. 24, 2024
Infectious Disorders
Mar. 24, 2024
Stroke & Vascular Disorders
Mar. 21, 2024
Behavioral & Cognitive Disorders
Mar. 07, 2024
Behavioral & Cognitive Disorders
Mar. 07, 2024