Sleep Disorders
Sudden infant death syndrome
Jul. 05, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author discusses the pathophysiology and treatment of this circadian rhythm sleep disorder. Hallmarks of this disorder include an advance in the habitual bedtime and wake time by several hours. The early morning awakening seen in this disorder may be mistaken for insomnia or depression. This is the first circadian rhythm sleep disorder for which a genetic cause was demonstrated. Current treatment primarily depends on the use of evening light therapy. Timed melatonin may theoretically be efficacious, but further trials are needed.
|
• Advanced sleep-wake phase disorder consists of stable, advanced habitual sleep and waking times, which can be seen more frequently in elderly individuals. | |
|
• Several large kindreds with autosomal dominant familial advanced sleep-wake phase disorder have been described. | |
|
• In some families, various missense mutations in clock genes were found. | |
|
• This is the first hereditary circadian rhythm variant described in humans. | |
|
• Treatment is largely empirical; timed light and melatonin may be tried. |
This disorder was initially referred to as advanced sleep phase syndrome, then was later classified as circadian rhythm sleep disorder, an advanced sleep phase type. Throughout this article the formal name advanced sleep-wake phase disorder, established in the third edition of the International Classification of Sleep Disorders, will be used (01). The preferred common name is advanced sleep phase disorder.
|
• Advanced sleep-wake phase disorder is characterized by habitual sleep-wake times advanced in relation to conventional or socially acceptable time and is present for at least 3 months. | |
|
• Symptoms of advanced sleep-wake phase disorder include evening sleepiness, early sleep onset, and early morning awakenings. | |
|
• The prognosis of advanced sleep phase syndrome is uncertain. | |
|
• The main complications of advanced sleep-wake disorder include restriction of social activities and evening driving. |
Patients with advanced sleep-wake phase disorder have their habitual sleep-wake times advanced in relation to the conventional or socially acceptable time; this results in symptoms of evening sleepiness, early sleep onset, and early-morning awakening (01). The symptoms must be present for at least 3 months. Despite efforts to delay sleep to later hours, sleep onset routinely occurs between 6:00 PM and 9:00 PM. During this time window, the patient may fall asleep at social gatherings or while driving. Patients routinely curtail or avoid evening activities due to the need to go to bed earlier than the social norm. Final awakening is much earlier in the morning than is desired or necessary to meet social or occupational obligations, typically well before dawn between 2:00 AM and 5:00 AM. Delaying evening sleep onset and extending sleep later into the morning are intractably difficult for these patients; however, if patients are able to sleep during their biologically preferred time window, sleep duration and quality are normal. Unlike other disorders with prominent early morning awakening, eg, depression, the early morning awakening in advanced sleep phase syndrome occurs after a normal amount of relatively consolidated sleep, and there is no major mood disturbance during waking hours.
The prognosis of advanced sleep phase syndrome is uncertain. Restriction of normal social activities due to the need to retire early is the main complication of advanced sleep phase syndrome. Evening driving may be dangerous due to sleepiness.
A 69-year-old woman slept well and led an active social life until 3 years before she came into the clinic. Being an avid concert fan, she found it progressively difficult to stay awake during the evening performances and had to give up her season tickets. She thought something was the matter with her sleep at night because she would arise early (about 5:00 AM) although she would feel alert at that time. Her past medical history included coronary artery disease; she had undergone coronary artery bypass graft 6 years previously; arterial hypertension was treated with beta-blockers and diuretics. Polysomnography revealed a mild sleep-related breathing disorder that was judged to be not clinically significant. Actigraphy showed a relatively consolidated nocturnal sleep episode with average bedtime and waking time at 9:00 PM and 4:30 AM hours, respectively. The patient was treated with bright light exposure at 7:30 PM. The treatment delayed the habitual bedtime and waking time to about 10:30 PM and 6:00 AM, respectively. The patient was able to stay awake later and resumed her favorite evening activities.
|
• Nearly every cell in an organism has molecular oscillators that regulate circadian gene expression in response to various time cues. | |
|
• The paired suprachiasmatic nuclei of the hypothalamus is the central mammalian circadian oscillator and is the “master clock” that regulates peripheral molecular oscillators by transmission of circadian timing signals. | |
|
• The biological clocks of normal humans have a natural endogenous cycle of about 24.2 hours. | |
|
• The 24-hour cycle is maintained by daily synchronization of internal clocks with the shorter environmental cycle through a phase advancement of a fixed time period daily. | |
|
• Light is the main zeitgeber of endogenous clocks in humans. | |
|
• The circadian neuronal system is activated by darkness and suppressed by light. | |
|
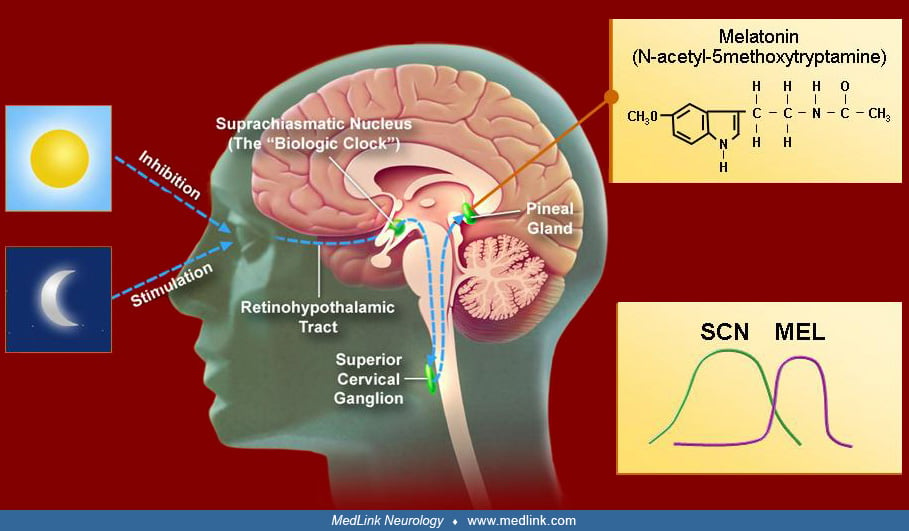
• The daily rhythm of melatonin secretion is controlled by the endogenous master pacemaker. Timing in the suprachiasmatic nucleus is regulated by melatonin. Light for entrainment is only effective a few hours before or after the core body temperature nadir. Light exposure before the core body temperature minimum delays the phase. Light exposure after the core body temperature minimum advances it. The amount of maximal daily resetting by light is limited to 1 to 3 hours. | |
|
• Dim light melatonin onset is currently the most commonly utilized marker of the circadian phase. | |
|
• Melatonin plays a modulatory role in the human circadian system. | |
|
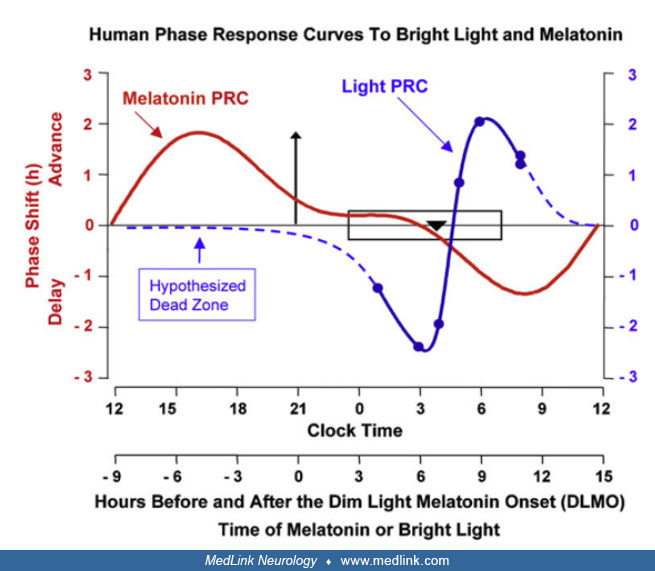
• Exogenous melatonin can shift circadian phase, exhibiting a phase-response curve that roughly mirrors the phase-response curve of light. Peak phase advance occurs prior to the time of dim-light melatonin secretion onset, whereas peak phase delay occurs about 12 hours later. | |
|
• Sleep propensity is governed by the interaction of an oscillating circadian process that promotes sleepiness at night and a steadily increasing homeostatic process that reflects prior sleep deprivation. | |
|
• The etiology of advanced sleep-wake phase disorder is unknown in the majority of cases. | |
|
• Advanced sleep-wake phase disorder increases in prevalence with age. | |
|
• Several mutations in CLOCK, BMAL1, PER, CRY, CKI-delta, and TIMELESS genes have been identified in familial cases of advanced sleep-wake phase disorder. |
Normal circadian physiology in humans. Almost every cell in the organism has active molecular oscillators that regulate circadian gene expression in response to various time cues, including light and chemical changes induced by feeding and temperature changes. In the absence of a central master clock, the myriad peripheral pacemakers would produce a cacophony of rhythms that would make a coordinated circadian behavior impossible.
The paired suprachiasmatic nuclei of the hypothalamus have been established as the site of the central mammalian circadian oscillator. This grouping of about 10,000 anterior ventromedial hypothalamic neurons manifests a high-amplitude circadian pattern of firing both in intact, freely behaving animals and in vitro. This suprachiasmatic nuclei “master clock” is composed of multiple single-cell circadian oscillators that, when synchronized, generate a coordinated circadian output that regulates peripheral “clocks” by transmission of circadian timing signals. This regulation is achieved by means of direct and indirect projections to other regulatory brain areas, primarily in the hypothalamus, modulating in turn their circadian outputs and coordinating other overt rhythms (eg, arousal, hormonal secretion, temperature, feeding, etc.). Daily behavioral, vegetative, and circadian firing rhythms of other brain regions desynchronize if the suprachiasmatic nuclei are lesioned.
The biological clocks of normal humans of all ages have a natural endogenous circadian cycle of slightly more than 24 hours, generally about 24.2 hours. If all temporal cues (zeitgeber, German for “time givers”) are removed, the internal rhythms are progressively phase delayed relative to the external clock time. Keeping the basic 24-hour cycle involves daily synchronizing of the internal clocks with the shorter environmental cycle following external zeitgebers (a process known as entraining, a control of one oscillating process by another). This circadian correction is achieved by advancing the internal clocks by a fixed time period (about 0.2 hours) every day. The ability to phase-advance is normally limited.
Light is the main zeitgeber of endogenous clocks in humans, as it is in other animals and plants. The human circadian system is more sensitive to short-wave blue-green light than to the long-wave red-spectrum light. The major afferent input to the suprachiasmatic nucleus consists of a melanopsin-containing subset of photosensitive retinal ganglion cells whose axons depart the optic chiasm to synapse on SCN cells.
There are three fundamental characteristics of the resetting capacity of the human circadian clock by light. First, the maximal response to a specific stimulus only occurs at a specific circadian time, which is stimulus dependent. As an example, light is generally only effective a few hours before or after the core body temperature nadir (between 3:00 AM to 5:00 AM in normally entrained humans). Stimuli applied during most of the daylight period have less effect on circadian phase timing, although there is some evidence that the human circadian pacemaker may be sensitive to bright light throughout the day. Second, the direction of resetting (advance or delay) is dependent on the circadian time at which the exposure occurs; light exposure before the core body temperature minimum delays the phase, whereas exposure after the core body temperature minimum advances it. Third, the amount of maximal daily resetting is limited to 1 to 3 hours. Plots of the magnitude and the direction of response (phase change) against the circadian time of light stimulus application (phase-response curve) reveal increasing amounts of delay from dusk to about halfway through the dark period, which roughly coincides with the nadir in core body temperature.
The direction of phase change then rapidly switches to maximal phase advances when the stimulus is applied near the beginning of the second half of the dark period, after which the advance response declines as the light stimulus moves closer to subjective dawn (34). The daily phase-advance in humans that keeps pace with the 24-hour day is a process that occurs immediately following arising in the morning and exposing the eyes to sufficient light.
The circadian clock phase (location of a certain event in the near 24-hour cycle), amplitude, and period cannot be measured directly by noninvasive means. Core body temperature varies predictably under circadian influence, even without the masking effect of sleep (which lowers the body temperature regardless of the circadian phase); it may, thus, serve as a circadian marker, but necessitates cumbersome rectal probes and constant routines regarding food intake, activity, and sleep. The rhythm of the pineal hormone melatonin is an easier measure marker of the endogenous circadian rhythm. Melatonin levels in fractional saliva specimens correlate well with plasma melatonin and are less markedly influenced by sleep and posture, although they can be affected by light exposure. This technique has been validated in the home environment (05).
The melatonin circadian rhythm is highly robust, has low intra-individual but high inter-individual variability, and is appreciably masked by light. The dynamics of the daily duration of melatonin secretion is significant in seasonal and reproductive physiology in animals; longer nights characteristic of the winter photoperiod are signaled by longer melatonin secretion duration. Dim light melatonin onset (DLMO) is currently the most commonly utilized marker of the circadian phase (26).
The role of melatonin in the human circadian cycle is modulatory. The suprachiasmatic nucleus exhibits a dense population of melatonin receptors, presumably establishing a feedback mechanism. Exogenous melatonin can shift circadian phase, exhibiting a phase-response curve that is roughly a mirror image of the phase-response curve of light. The direction and the magnitude of the shift depend on the circadian time at which the light or melatonin are applied. Bright light in the evening delays the phase of the circadian clock, whereas bright light in the morning advances the clock; exogenous melatonin does the opposite. With exogenous melatonin, peak phase advance occurs prior to the time of dim-light melatonin secretion onset (about 8:00 PM) and peak phase delay about 12 hours later.
Melatonin also affects other endogenous rhythms, including temperature, cortisol secretion, and the sleep-wake cycle. Appropriately timed light exposure and melatonin may reinforce a desired effect (09); indeed, it is possible that the physiological role of the nocturnal melatonin secretion is to reinforce the daily resetting of the endogenous clock by the morning light and to provide additional fine-tuning (32). Mutually reinforcing timed application of light and exogenous melatonin may be used in treating circadian rhythm sleep disorders (28).
The sleep-wake cycle is a major overt manifestation of the circadian rhythm, possibly through the SCN’s direct and indirect projections to wake- and sleep-promoting brain regions. However, compared to other endogenous rhythms like core body temperature or melatonin, it is more loosely associated with the circadian pacemaker and is also influenced by noncircadian homeostatic factors (eg, prior sleep deprivation). Sleep propensity is governed at any time by the interaction of two processes: (1) an oscillating circadian process coupled to other circadian rhythms (eg, melatonin secretion and core body temperature rhythms) that promote sleepiness at night and contribute to the afternoon napping “siesta” period; and (2) a steadily increasing homeostatic process reflecting prior sleep deprivation that discharges during sleep. The detailed description of the interaction of these processes is beyond the scope of this review; the classic two-process interaction model is an abstraction, and the net result of sleep-alertness is much more than the algebraic sum of the two processes. A significant, partially genetically determined, inter-individual variability exists, which determines, among other factors, the degree to which a person is an evening or morning type (14).
Pathophysiology of advanced sleep-wake phase disorder. Although in some cases genetic mutations have been identified, the etiology is unknown in the majority of cases.
The basic pattern of advanced sleep-wake phase disorder is presumably a phase-advance of the circadian pacemaker coupled with a similar phase-advance of the sleep-wake cycle (27). Advanced sleep-wake phase disorder increases in prevalence with age. Age-related changes in the circadian sleep-wake pattern are frequently observed. There seems to be a consensus about the tendency for circadian phase-advancement, sleep phase-advancement, and less consolidated sleep in healthy elderly. However, opinions vary as to whether this is due to a reduction in the output of the circadian pacemaker (eg, the amplitude of core body temperature changes or melatonin secretion) with increasing age, which may be responsible for decreased sleep consolidation in the elderly. Some studies showed such reduction, whereas others showed none. The elderly may also exhibit changes in the interrelationships between measured circadian outputs (primarily melatonin and core body temperature rhythms) and the sleep-wake cycle, particularly shortening of the time between core body temperature nadir and the habitual waking time, but this is not a universal finding. The changes in sleep consolidation and in sleep timing in the healthy elderly may also be due to reduction in the homeostatic drive for sleep and in the circadian drive that promotes sleep in the early morning. Psychosocial factors (isolation, reduced exposure to light, changes in scheduled activities) may also play a role in the elderly, emphasizing loose coupling between the sleep-wake and the circadian cycles.
At a molecular level, the rhythms of expression of circadian genes Per1, Per2, and Per3 in peripheral blood monocytes in the elderly were as robust as in young subjects, although they were phase advanced. The phase angle between the Per3 (but not Per1 or Per2) expression and the habitual sleep timing was altered in the elderly, suggesting decreased homeostatic sleep drive in the elderly (15). A brief review summarizes the findings and the controversies on the subject of the changes in the circadian system with aging (21).
Interestingly, patients with early-morning insomnia and normal bedtime also exhibited significant advancement of their circadian rhythm; it is possible that, although suffering from a mild advanced sleep phase syndrome, social considerations prevented them from adopting an earlier bedtime. It is difficult to draw clear lines between the normal sleep-wake cycle changes in healthy elderly, early-morning insomnia, and advanced sleep phase syndrome. They may all represent different angles of the same spectrum of age-related changes influenced by psychosocial factors.
The circadian clock consists of a transcription-translation negative feedback loop regulated by activators (CLOCK and BMAL1) and inhibitors (PER and CRY). Several mutations in these genes have been identified in familial cases of advanced sleep-wake phase disorder. In 1999, three large, Caucasian kindreds with familial advanced sleep phase syndrome (FASP) were described. Overall, there were 37 affected individuals (29 affected in one kindred in five generations); the youngest affected patient was 8 years old. The disorder segregated as autosomal dominant with high penetrance. They had phase advance of about 4 hours in the sleep-wake cycle, melatonin, and temperature circadian rhythms. One of the subjects was studied in a time-isolation facility; her circadian period (both sleep-wake and temperature) was 23.3 hours. A missense mutation in one of the circadian genes crucial for resetting the circadian clock in response to light (Per2) in these kindreds was subsequently described. This was the first hereditary circadian rhythm variant described in humans. An additional kindred of eight affected members was described at that time. The disorder also segregated as autosomal dominant. A subsequent study in a Slovenian cohort identified two heterozygous missense variants in the PER3 gene that were highly associated with advanced sleep-wake phase disorder (25). Another missense mutation in CRY2 (Ala to Thr) is reported to result in familial advanced sleep phase (16). Additionally, a missense mutation was described in the CKI-delta circadian gene, which was responsible for familial advanced sleep phase syndrome in another Japanese family. This CKI-delta mutation has also been associated with familial migraine (06). Targeted sequencing of 76 genes in 15 individuals from two Japanese families with FASP found variants in PERIOD1 (PER1), CRYPTOCHROME2 (CRY2), and TIMELESS (TIM) that have not been identified in other families with FASP. The variants known to cause FASP in Caucasian kindreds were not found in these Japanese families (31). Polymorphisms at another circadian gene (Per1) may be associated with extreme morning preference bordering on advanced sleep phase syndrome. A de novo variant in CSNK1 was identified in a 4 year old with advanced sleep wake phase disorder since infancy (Pisan? et al 2025). Finally, mutations in the human TIMELESS gene have been shown to impact negative regulators of the circadian clock leading to familial advanced sleep phase (19). Each of these mutations show that the result can have a similar phenotype of advancement in the circadian phase.
In population-based studies looking at variants in the genes known to cause familial advanced sleep wake phase disorder, the PER3 P415A/H417R variant was associated with earlier sleep timing, although the effect size was only 7.8 minutes compared to 4 hours in those with familial advanced sleep phase (33). Carriers of pathogenic variants of CRY2 and TIMELESS, however, were not associated with earlier sleep times (33).
Individuals with autism spectrum disorder have been identified as having PER2 variants. Of 5102 individuals with autism spectrum disorder, four were found to have PER2 variants (17). None of them were previously diagnosed with a sleep disorder, but three of them reported sleep difficulties, with one subject having symptoms suggestive of a familial advanced sleep-wake phase disorder. A cross-sectional study of Sudanese children with autism spectrum disorder demonstrated that advanced sleep-wake phase disorder is the second most common sleep disorder reported, suggesting a relationship between circadian dysregulation and autism spectrum disorder; however, this requires further study (22). It has also been demonstrated that individuals born prematurely with very low birth weight were more likely to have an advanced sleep phase as adults, though the underlying mechanism remains unclear at this point (04).
|
• The overall prevalence of advanced sleep-wake disorder is rare and is estimated to be between 0.25% and 7.13%. |
There are few formal prevalence studies, but clinical experience suggests that the disorder is rare. A national survey of New Zealand adults estimated a prevalence of 0.25% to 7.13%, depending on the definition used (23). A study in North America estimates the prevalence of advanced sleep phase to be 0.33%, whereas familial advanced sleep phase is 0.21% and advanced sleep-wake phase disorder is at least 0.04% (10). A cross-sectional study in Cyprus also estimates a similar prevalence of advanced sleep wake phase disorder in the general population at approximately 0.5% (13). A telephone survey was completed in Japan among 157 visually impaired individuals (30). The prevalence of advanced sleep-wake phase disorder in the visually impaired was estimated to be 3.8%. The prevalence may be higher in the elderly population, in visually impaired individuals, and in genetically affected families.
|
• Evening light therapy can potentially prevent advanced sleep-wake phase disorder. |
The clinical phenotype of advanced sleep-wake phase disorder can be prevented in part by evening light therapy as described below in management.
Early morning awakening is one of the hallmarks of major depression. It was shown that women in a current major depressive episode had earlier melatonin onset compared to controls without history of mental illness, and this correlated to poor mood (07). The biological interrelationships between advanced circadian rhythms and major depression have been suggested, but no clear etiological ties have been established. On the other hand, depressive symptoms characterize many patients with delayed, rather than advanced, sleep phase syndrome.
Habitual evening napping (eg, in front of the television) due to chronic sleep deprivation or disrupted nocturnal sleep from a sleep disorder such as obstructive sleep apnea (OSA) should also be excluded by careful history taking.
|
• Sleep logs or actigraphy for 1 to 2 weeks is recommended to confirm the diagnosis of advanced sleep-wake phase disorder. | |
|
• A detailed psychiatry history is needed to rule out mood disorders. | |
|
• Sleep recording at the patient’s usual sleeping hours should show normal sleep-onset latency, staging, and duration for age and should rule out other causes of pathologic sleepiness. |
Sleep logs or wrist-motion monitoring (actigraphy) for 1 to 2 weeks are recommended to confirm the history of chronic daily sleep onsets earlier than 9:00 PM and offsets before 4:00 AM. A careful psychiatric history should be obtained to rule out an affective disorder. Sleep recorded at the patient's usual sleeping hours should show normal sleep onset latency, staging, and duration for age. If the recording is done at conventional (later) hours, initial sleep latency should be short, or the patient may fall asleep while being prepared for recording. A prolonged period of wakefulness is typically present at the end of the night. No other cause of pathologic sleepiness (sleep apnea, severe periodic limb movements in sleep) should be present. Sleep architecture should be normal for age.
Biomarkers such as the salivary dim light melatonin onset are optional. Dim light melatonin onset testing demonstrates an earlier evening (and sometimes afternoon) peak of melatonin consistent with the circadian phase advancement.
|
• Treatments for advanced sleep-wake phase syndrome use chronobiological principles and include evening exposure to bright light and chronotherapy. | |
|
• Early morning low-dose melatonin has not been systematically studied in advanced sleep-wake disorder. | |
|
• Light therapy is considered a safe therapeutic option with limited side effects. |
Treatments for advanced sleep phase syndrome use chronobiological principles to achieve sustained phase shift to the desired sleep-wake schedule. This is performed with intentional changes to amplify environmental time cues using timed light exposure or melatonin. General measures to improve sleep hygiene, exercise, and relaxation may all help to consolidate the new schedule.
Light is the most important zeitgeber to the circadian clock. As described above, bright light exposure has phase-shifting effects with phase advance or delay following early morning or late evening exposure, respectively. Evening exposure to bright light (2500 lux for 2 hours) was found to delay both the sleep-wake and the melatonin rhythm in a patient with advanced sleep phase syndrome, though the AASM Clinical Practice Guidelines published in 2015 do not provide a specific light intensity (03). Various studies have shown varying degrees of efficacy with 2500 lux to 10000 lux. Evening bright light exposure (between 8:00 PM and midnight) delayed circadian phase markers and improved subjective quality of sleep in early-morning insomniacs and in advanced sleep-wake phase disorder. During long-term maintenance treatment, subjective improvement was maintained, but objective changes in sleep parameters were less pronounced. Many commercial light boxes are available, varying in design and light intensity. Longer period of moderate intensity light may be more effective than a shorter exposure period of high intensity light (11), although a more recent paper suggests that 30 minutes of bright light exposure may be sufficient for advancing circadian rhythms (09). It appears that light exposure must be done during the waking hours in order to achieve a phase delay, as a study looking at light delivered through the eyelids of sleeping persons did not show any objective differences between the control and intervention conditions (12).
Melatonin has not been systematically studied in advanced sleep phase syndrome. On theoretical grounds and following its success in other circadian rhythm sleep disorders, early morning low-dose melatonin, either alone or combined with evening bright light exposure, may be beneficial in delaying a patient’s circadian rhythm. Despite the paucity of controlled studies, the original review and practice parameters of the American Academy of Sleep Medicine suggest chronotherapy, timed light exposure, and melatonin administration in the treatment of patients with advanced sleep phase syndrome. However, following criticism about the inclusion of melatonin, the recommendation for use of timed melatonin in this disorder was removed.
Hypnotics to manage early morning insomnia are best avoided.
Light therapy is considered safe if used with recommended intensity and duration (03). Potential side effects include eye irritation, irritability, headache, nausea, sensation of glare, erythema, dryness of eyes and skin, and, rarely, a hypomanic state. This can be managed with adjustment of light intensity, duration of therapy, and humidification. Many patients report initial subjective success; however, relapse is common due to failure to maintain therapy.
Limited data are available on pregnancy and advanced sleep-wake phase disorder. Rodent studies have shown a significant connection between the circadian cycle and the reproductive cycle and have established the role of the suprachiasmatic nucleus in luteinizing hormone surge and ovulation (18). In a study of 68 nurses working shift work, over 50% reported menstrual changes with working shift work, and three of the participants who were attempting to conceive reported infertility attributed to shift work (20). Epidemiological studies have shown associations between shift work and negative pregnancy outcomes, such as low birth weight, preterm birth, and miscarriage, although it is unclear whether this is related to circadian dysregulation or other lifestyle factors related to shift work (08; 02). In particular, phase-advanced mice had a greater negative impact on pregnancy outcomes compared to phase-delayed mice, which suggests significant implications in women with circadian rhythm disorders (29).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Tresa Zacharias MD
Dr. Zacharias of Rush University Medical Center has no relevant financial relationships to disclose.
See Profile
Bradley V Vaughn MD
Dr. Vaughn of UNC Hospital Chapel Hill and University of North Carolina School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jul. 05, 2026
Sleep Disorders
Jul. 03, 2026
Sleep Disorders
Apr. 10, 2026
Sleep Disorders
Apr. 05, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 29, 2026
Sleep Disorders
Mar. 19, 2026