


Sleep Disorders
Sudden infant death syndrome
Jul. 05, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Autism spectrum disorder is a neurodevelopmental condition characterized by persistent impairments in social communication and interaction, restricted and repetitive behaviors or interests, and atypical sensory processing. Presentation and severity vary widely, reflecting autism spectrum disorder’s heterogeneity. This review summarizes the clinical features, historical context, epidemiology, biological basis, diagnosis, associated conditions, and up-to-date evidence-based management strategies, and discusses emerging and alternative therapies.
|
• The incidence of autism spectrum disorder has increased dramatically over the last 20 years, with an estimate of 1 in 30 8-year-olds in the United States (04). This increase is thought to be in response to a broader case definition and increased identification, but a true increase cannot be entirely ruled out. | |
|
• Autism spectrum disorder is about four times as common in males as in females. | |
|
• No single or precise etiology has been identified. | |
|
• Early identification is critical for better outcomes. | |
|
• To date, no evidence-based medical treatment has been shown to improve the core symptoms of autism spectrum disorder; pharmacotherapy is used primarily to address associated behavioral difficulties. | |
|
• Interdisciplinary intervention (ie, pharmacological when indicated, behavioral therapy, community-based support) is crucial for short- and long-term treatment and for improved outcomes of an ever-growing population of adults diagnosed with autism spectrum disorder. |
The word “autism” is derived from the Greek word “autos,” meaning “self.” Over 100 years after Swiss Psychiatrist Eugine Bleuler coined the term “autism,” autism spectrum disorder has shifted from being conceptually framed as a behavioral disorder influenced by parenting style to a neurodevelopmental condition with distinct clinical features. Pioneering work by Dr. Grunya Sukhareva in the 1920s, followed by Dr. Leo Kanner and Dr. Hans Asperger in the 1940s, led to the autism spectrum disorder case definition, which has been recognized in the Diagnostic and Statistical Manual of Mental Disorders since 1980.
|
DSM-I (1952) |
No term for autism or pervasive developmental disorder |
|
DSM-II (1968) |
No term for autism or pervasive developmental disorder |
|
DSM-III (1980) |
Pervasive developmental disorders: infantile autism, childhood-onset pervasive developmental disorder, atypical autism |
|
DSM-III-R (1987) |
Pervasive developmental disorders: autistic disorder, pervasive developmental disorder not otherwise specified |
|
DSM-IV (1994) |
Pervasive developmental disorders: autistic disorder, Asperger disorder, pervasive developmental disorder not otherwise specified, childhood disintegrative disorder, Rett syndrome |
|
DSM-IV-TR (2000) |
Pervasive developmental disorders: autistic disorder, Asperger disorder, pervasive developmental disorder not otherwise specified, childhood disintegrative disorder, Rett syndrome |
|
DSM-5 (2013) |
Autism spectrum disorder (pervasive developmental disorder not otherwise specified, childhood disintegrative disorder, Rett syndrome no longer recognized as disorders) |
|
DSM-5 TR (2022) |
Autism spectrum disorder |
The average age of diagnosis internationally remains approximately 43 months, yet parents often report concerns regarding development by 12 to 18 months of age.
Early signs typically include:
|
• Reduced eye contact, gestures, and facial expression or gestures (eg, not pointing, not waving bye-bye, no gaze monitoring to another person) |
Language delay is the most common presenting symptom, especially in young children. Over time, children exhibit variable language profiles, from nonverbal to delayed onset of words and phrases to fluently verbal. Persons with autism spectrum disorder may not engage in meaningful pragmatic communication and may lack reciprocity, resulting in an impaired ability to sustain conversation. Spoken language may be stereotyped in form and marked by immediate and delayed echolalia, prenominal reversal, and idiosyncratic word usage. The rate of language regression has been reported to be 41%, and there is some evidence that regression, defined as language loss, is specific to autism spectrum disorder.
Joint attention, defined as the coordination or sharing of attention between two people and an object or event, is often delayed or impaired in young children with autism spectrum disorder. Individuals with autism spectrum disorder may be affectionate and desire social attention but may lack the skills needed to interact with others effectively.
Features associated with autism spectrum disorder are as follows.
Intellectual disability. Surveillance data published in 2025 by the Autism and Developmental Disabilities Monitoring Network reported that 39.6% of children with autism spectrum disorder were classified in the range of intellectual disability (05). Cognitive skills in individuals with autism spectrum disorder may also show uneven development.
Attention, mood, and behavioral disorders. Attention deficit hyperactivity disorder commonly co-occurs with autism spectrum disorder and is now recognized as a separate diagnosis. Conditions such as anxiety, obsessive-compulsive disorder, and conduct disorders are identified in 70% to 90% of children and youth with autism spectrum disorder.
Feeding and gastrointestinal disorders. Atypical eating behaviors have been found significantly more frequently in children with autism spectrum disorder than in children with other disorders or in typically developing children. Additionally, research has shown a significant relationship between avoidant restrictive food intake disorder and autism spectrum disorder. Also, children with autism spectrum disorder have a higher incidence of gastrointestinal issues in comparison to control and developmentally disabled subjects.
Sleep problems. Sleep disorders are common. Up to 86% of individuals with autism spectrum disorder experience at least one sleep problem daily (29). Anxiety has been identified as the strongest cross-sectional predictor of sleep disturbance, along with elevated IQ, greater autism spectrum disorder severity, sensory sensitivities, and gastrointestinal issues.
Seizures. The prevalence of epilepsy is higher in children with autism spectrum disorder than in the general population. Research has revealed that children diagnosed with autism spectrum disorder tend to have subclinical electroencephalographic abnormalities in the right temporal lobe (21.5%), followed by central and bilateral temporal regions (20.2%) (15). An EEG is not recommended for all individuals with autism spectrum disorder but should be considered if there is a history of atypical regression, suspected seizures, or other neurologic symptoms.
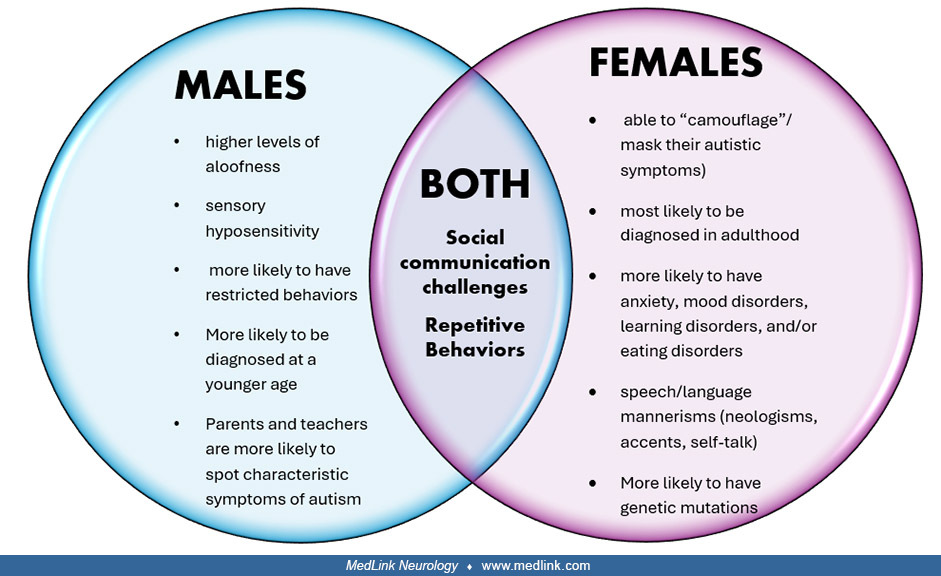
Gender differences. Initially noted by Dr. Sukhareva in the 1920s but more recently gaining added attention is the recognition of differences between the male and female presentation of autistic symptoms. Females often present with subtler social communication deficits, also known as social camouflaging. In what is known as the Female Protective Theory, females diagnosed with autism are likely to show more genetic or environmental hits than males (14).
Autism spectrum disorder is lifelong, though symptom expression evolves. Approximately 9% of individuals diagnosed in early childhood may no longer meet full diagnostic criteria in adulthood. Early language and cognitive abilities predict functional outcomes. Adults with autism spectrum disorder face increased risk of health disparities, particularly during transitions from pediatric to adult care. Quality of life is strongly associated with access to family, educational, vocational, and community support.
|
• Autism spectrum disorder is a complex neurodevelopmental disorder with no single etiology. | |
|
• There is a high concordance in monozygotic twins and a higher percentage of recurrence in the siblings of an affected individual. | |
|
• There are hundreds of susceptibility genes and possibly environmental and epigenetic factors. | |
|
• Advanced paternal age, prematurity, and other pre- or perinatal complications have also been reported as risk factors for the development of autism spectrum disorder. | |
|
• Researchers have proposed a neuroanatomic or neurophysiological basis for autism spectrum disorder. | |
|
• Vaccinations have not been associated with autism spectrum disorder. Hundreds of studies have shown that the components of vaccines (thimerosal or mercury) or combined vaccines (eg, MMR) are not associated with the development of autism spectrum disorder. |
Genetics. Autism spectrum disorder has strong genetic underpinnings, with monozygotic twin concordance rates of 50% to 60% and sibling recurrence risk of 10% to 20%. Genes implicated in autism spectrum disorder span synaptic function, neurotransmission, chromatin remodeling, and immune regulation. The five major databases of genetic variations associated with autism spectrum disorder are listed in Table 2.
|
Database |
Year first presented |
Website |
Strength of database |
Weakness of database |
|
VariCarta |
2019 |
Focuses on the genetic variance and the associated evidence. |
No standardized gene-scoring system | |
|
Autism Speaks MSSNG database |
2014 |
Provides raw, extensive WGS data for all genetic variation. |
No curation of the data accumulated. | |
|
ClinVar |
2013 |
Consolidating conflict interpretations and enabling automated workflows. Helpful for clinical decision-making. |
Conflicting interpretations; allows for the inclusion of data based on anecdotal bias. | |
|
SFARIgene |
2007 |
Uses a standardized gene-scoring system to assess evidence strength. Focuses on the genes themselves and the associated evidence. |
Does not consider genetic variants. | |
|
AutDB |
2007 |
Has the highest percentage of autism spectrum disorder candidate genes database. |
Provides detailed information (eg, variant type, inheritance, parental transmission) only for rare variants and not for common ones. | |
|
Autism Genetic Resource Exchange (AGRE) |
1997 |
Houses data from thousands of families (multiplex families with multiple affected members and simplex families) |
Only has data from families with multiple children diagnosed with autism. Genetic heterogeneity is not recognized in the database; can’t recognize common variation. |
ASD is associated with several genetic syndromes, including fragile X syndrome, tuberous sclerosis, Prader-Willi syndrome, and trisomy 21. Other genes of interest for their correlation with autism spectrum disorder are SOX genes 5, 7, and 11 and chromosome 15 q13.2-13.3. The latter has been associated with autism spectrum disorder, although not strongly, and is also associated with attention deficit hyperactivity disorder, mood disorder, schizophrenia, and aggressive or self-injurious behavior.
Neuroanatomy. Studies have found increased gray matter in subjects with autism spectrum disorder, including the anterior temporal, dorsolateral prefrontal, and frontal lobe regions. Autopsied brain samples from patients with autism spectrum disorder have revealed a loss of Purkinje cells in the hippocampus, amygdala, and cerebellum. A study evaluating infants using brain MRIs found that those who later developed autism spectrum disorder had significantly greater extra-axial fluid at 6 to 9 months, which remained elevated at 18 to 24 months (27). However, there is a lower prevalence of definite pathology on brain MRI in children with autism spectrum disorder without an abnormal neurologic examination, headaches, or seizures.
Neurotransmitters. Serotonin and dopamine appear to play a role in the pathophysiology of autism spectrum disorder. Oxytocin and vasopressin are pituitary neuropeptides that have been shown to play a role in social behavior. Single-nucleotide polymorphisms in oxytocin and vasopressin receptors have been associated with autism spectrum disorder. GABA modulators (eg, arbaclofen) have been studied in open-label trials, but additional studies are needed before they can be considered in the treatment of core symptoms of autism spectrum disorder. Glutamate is an excitatory neurotransmitter, and two of its receptors have been implicated in autism spectrum disorder.
Hormonal and immunologic mediators. Research examining biological mechanisms in autism spectrum disorder has highlighted abnormalities across both hormonal and immune systems. Elevated fetal testosterone levels have been linked to increased autism-related traits, and dysregulation of the hypothalamic-pituitary-adrenal axis has been observed through altered cortisol, adrenocorticotropic hormone, and dehydroepiandrosterone profiles, with higher cortisol levels in individuals with more severe presentations suggesting a potential neurotoxic influence. Parallel immunologic findings demonstrate significant elevations in pro-inflammatory cytokines (including IL-1β, IL-6, IL-8, and IL-12p40), particularly among children with regressive autism, in whom heightened cytokine activity correlates with greater communication impairments and behavioral challenges. Additional studies have identified altered T cell function, further supporting the role of immune dysregulation in the pathophysiology of autism spectrum disorder.
Prenatal and perinatal factors. Prenatal exposure to ethanol, thalidomide, misoprostol, and antidepressants is associated with an increased incidence of autism spectrum disorder. A 2024 New England Journal of Medicine article confirmed valproic acid’s association with an increased incidence of autism while excluding topiramate and lamotrigine (Hernandez-Diaz et al 2024). There is no established causal link between prenatal acetaminophen (paracetamol) exposure and autism, although some studies report small associations that may be confounded by other factors (19).
Prenatal cytomegalovirus infection and pre-eclampsia have also been considered risk factors for autism spectrum disorder. In a meta-analysis of prematurity and autism spectrum disorder, the prevalence estimate was 20% when using screening tools and 6% when using diagnostic assessments. The odds of an autism spectrum disorder diagnosis were 3.3 times higher in individuals born prematurely than in the general population (18). Advanced paternal age is also an established risk factor.
Vaccines. Hundreds of studies have shown that the components of vaccines or combined vaccines are not associated with the development of autism spectrum disorder. A study conducted in Denmark recruiting more than 1 million children found no association between childhood vaccines and autism (01).
Autism spectrum disorder has been found to have an inheritance rate of 30%. Table 3 summarizes heritability studies in first- and second-degree relatives.
|
Family relations |
ASD in relation to ASD without intellectual disability (per 1,000) |
ASD in relation to ASD with intellectual disability (per 1,000) |
|
First-degree relatives | ||
|
Father |
10.9 |
2.7 |
|
Mother |
22.5 |
15.2 |
|
Brother |
129.7 |
135.5 |
|
Sister |
71.2 |
61.6 |
|
Second-degree relatives | ||
|
Uncle |
8.5 |
7.1 |
|
Aunt |
4.4 |
3.1 |
|
Half brother |
59.1 |
62.6 |
|
Half-sister |
28.5 |
25.1 |
|
• Autism spectrum disorder is one of the most common neurodevelopmental disorders in children. | |
|
• Data from the Global Disease Study 2021 puts global incidence at an estimated 61.8 million people, or one in 127 (10) | |
|
• The prevalence of autism spectrum disorder has increased 300% over the last 20 years. |
Autism spectrum disorder is reported to occur in all racial, ethnic, and socioeconomic groups. Surveillance data from the Autism and Developmental Disabilities Monitoring Network (ADDM) indicate an increase in autism spectrum disorder prevalence among African American (1 in 27), Hispanic (1 in 30), and Asian-Pacific Islander children (1 in 26) in comparison to white children (1 in 36) (26).
|
Continent |
Prevalence |
Source |
|
North America | ||
|
• Canada |
• 2.0% in 2019 |
Autism spectrum disorder: Highlights from the 2019 Canadian Health Survey on Children and Youth |
|
• Mexico |
• 0.87% in 2016 |
Early detection and intervention for children with autism in Mexico (MHIN) |
|
South America | ||
|
• Brazil |
• 1.2%, in 2022 | |
|
• Guyana |
• 1.4% in 2016 | |
|
Caribbean Islands | ||
|
• Cuba |
• 0.4%, in 2022 | |
|
• Belize |
• 0.695% in 2021 | |
|
Europe | ||
|
• United Kingdom |
• 1.78% in 2021 | |
|
• Denmark |
• 2.8% in in 2020 | |
|
Middle East/North Africa | ||
|
• Qatar |
• 1.5% in 2021 | |
|
• Egypt |
• 0.78% in 2021 | |
|
Sub-Sahara Africa | ||
|
• Nigeria |
• 1.2% in 2025 | |
|
• South Africa |
• 0.08% in 2024 | |
|
Asia | ||
|
• China |
• 1.05% in 2024 | |
|
• India |
• 1.12% in 2024 |
Unraveling the Spectrum: A Comprehensive Review of Autism Spectrum Disorder in India |
|
Australia |
• 1.1% in 2022 |
Intellectual disability and autism prevalence in Western Australia: impact of the NDIS |
|
• The diagnosis cannot be prevented in most cases. | |
|
• Few underlying causes could be controlled, such as ethanol and at-risk drugs or medication consumption. | |
|
• Genetic counseling is recommended for families with an affected child or a high-risk family history. |
The differential diagnosis for autism spectrum disorder includes:
|
• Hearing impairment |
It may be difficult to determine if a diagnosis of autism spectrum disorder is warranted in severe or profound intellectual disability. Qualitative deficits in social and communication skills or the level of cognitive functioning, and the specific behavioral characteristics of autism spectrum disorder may be present.
|
• Trisomy 21 (Down syndrome) |
Multisystem developmental disorder. Before the publication of DSM-5, multisystem developmental disorder was occasionally referenced in relation to autism, largely because earlier diagnostic frameworks required a minimum age of 3 years for an autism spectrum disorder diagnosis. With DSM-5 acknowledging that clinically meaningful signs of autism may emerge before that age (the developmental period that multisystem developmental disorder was originally intended to characterize), the term has been rendered obsolete.
Multiple complex developmental disorder. Multiple complex developmental disorder is not considered part of the autism spectrum and has not been incorporated into DSM-5 nosology. Contemporary literature has suggested that multiple complex developmental disorder may reflect a distinct developmental phenotype rather than an autism-related condition and is positioned more appropriately within the broader domain of developmental delays. It is not recognized as a formal diagnostic entity in contemporary classification systems.
Screening. The American Academy of Pediatrics recommends developmental surveillance with a standardized screening tool at all health care maintenance visits, with an autism-specific standardized screening tool at the 18- and 24-month visits. The Modified Checklist for Autism in Toddlers Revised with Follow-Up (M-CHAT-R/F) is a short parent checklist valid for use between 16 and 30 months of age, with an added algorithm for review of positive responses by the healthcare provider (24). This is intended to reduce the number of false positives. Other screening tools include The Social Communication Questionnaire (07) and the Screening Tool for Autism in Two-Year-Olds (28). Artificial intelligence is being researched as a potentially useful tool for the early identification and diagnosis of autism spectrum disorder.
Clinical evaluation. A detailed developmental and behavioral history should be taken. Information should also be obtained regarding any history of maternal infections during pregnancy, perinatal or postnatal insult to the patient's brain, meningitis, encephalitis, or seizures. An inquiry should be made into any family history of autism and other genetic disorders, related developmental disorders, or psychiatric disorders.
Physical examination should include assessment of any dysmorphic features or neurologic deficits.
Mental status examination should attempt to assess:
|
(1) The child's relatedness to and interest in the professionals, caregivers, siblings, peers, and other people in the child's environment. | |
|
(2) The quality of reciprocal social exchange in verbal and nonverbal communication (eye contact, gestures, facial expression, stereotyped speech, echolalia, pronominal reversal). | |
|
(3) The child's ability to engage in reciprocal imaginative play with representational toys | |
|
(4) The presence of perseverative, stereotypic, and ritualistic behavior. | |
|
(5) The presence of problematic behaviors, such as attentional difficulties, high activity level, aggression, and self-injurious behavior. |
Medical investigation. Hearing should be assessed, especially if there is a speech delay. If the child is unable or unwilling to cooperate with audiometry, or the initial test is suboptimal or equivocal, hearing should be tested with brainstem auditory evoked response.
Genetic testing is recommended for children diagnosed with autism spectrum disorder, including microarray analysis and testing for fragile X syndrome. Whole-exome sequencing is being performed in some children whose microarray and fragile X testing did not reveal an etiology.
An EEG is not recommended for all individuals with autism spectrum disorder but should be considered if there is atypical regression, seizures, or other neurologic symptoms.
Metabolic screening, amino acid chromatography, serological tests for evidence of intrauterine infections, and tests for phenylketonuria, serum copper, and ceruloplasmin are indicated if symptoms of autism appear after 3 years of age or are progressive.
Additional assessments. Assessment of the child's level of cognitive functioning, adaptive behavior, and language skills is a key component in elaborating a comprehensive treatment plan. A child assessment team evaluation should be obtained for school-aged children. This assessment will help develop an individualized educational plan for the child and provide specific guidelines for intervention by classroom teachers. A functional behavioral assessment completed by a behavioral specialist may be needed to develop a behavioral intervention plan if the child exhibits disruptive or potentially dangerous behavioral problems.
|
• Early identification is critical. Any child with autism spectrum disorder (or suspected) should be referred to early intervention programs as soon as possible. | |
|
• Applied behavioral analysis is the therapy method with the strongest research support. | |
|
• Children with autism spectrum disorder also benefit from social skills training. | |
|
• For teenagers and young adults, it is important to provide vocational counseling and training when applicable. | |
|
• Physical and occupational therapy are helpful for motor, self-help, and sensory processing impairments. Feeding therapy may be useful for the feeding disorders associated with autism spectrum disorder. | |
|
• Parent involvement has been consistently documented as key to therapy effectiveness. | |
|
• Healthcare professionals must be familiarized with the variety of treatment methods (effective, more research is needed, not tested, or ineffective) so parents can make the most informed decisions and avoid potentially costly and unproven treatment. |
Applied behavioral analysis. Applied behavior analysis uses principles of operant conditioning to help a child reduce the frequency of negative interfering behavior associated with autism spectrum disorder by teaching the child skills broken down into small steps. Several reviews have concluded that a considerable body of evidence exists to support the use of applied behavioral analysis in children with autism spectrum disorder. Applied behavioral analysis is the only evidence-based treatment for autism spectrum disorder; it is endorsed by Autism Speaks, the NIH, the American Psychological Association, and the American Academy of Pediatrics. The number of hours of applied behavioral analysis-based intervention at an early age correlates positively with improvement on a wide variety of measures, with a gold standard of 40 hours per week according to research evidence.
Augmentative and alternative communication. Augmentative and alternative communication is an umbrella term that encompasses all communication modalities to augment vocal-verbal communication or as an alternative to vocal speech. There is no evidence that speech production decreases because of augmentative and alternative communication intervention, and some studies have reported increased vocalizations following augmentative and alternative communication use. One popular approach to augmentative communication is the Picture Exchange Communication System program (03). Augmentative and alternative communication programs for smart devices have grown in use over the past decade.
There is a growing availability of electronic devices and online applications and programs that healthcare professionals can recommend to parents for safety monitoring, support of verbal and social skills development, and facilitation of daily task completion.
|
App Name |
Year app was |
Downloadable to |
Downloadable to |
App cost |
|
Communication skills development | ||||
|
Proloquo2 Go |
2009 |
N |
Y |
More than $20/month or $240/year (one-time fee) |
|
Leeloo AAC |
2020 |
N |
Y |
Less than $20/month or $240/year |
|
Avaz AAC |
2010 |
Y |
Y |
Less than $20/month or $240/year |
|
Talk Tales: Simple Sounds |
2023 |
Y |
Y |
Less than $20/month or $240/year |
|
Routine management and planning | ||||
|
AutiPlan |
2011 |
Y |
Y |
Less than $20/month or $240/year |
|
Pictello |
2010 |
Y |
Y |
Less than $20/month or $240/year |
|
Choiceworks |
2012 |
N |
Y |
More than $20/month or $240/year (one-time fee) |
|
Cognitive, fine motor, and social skills development | ||||
|
AutiSpark |
2023 |
Y |
Y |
More than $20/month or $240/year |
|
Social skills modeling | ||||
|
Model Me Going Places |
2010 |
Y |
Y |
Free |
|
Safety or elopement prevention devices | ||||
|
Angel Sense |
2013 |
Y |
Y |
More than $20/month or $240/year |
|
Apple AirTag |
2021 |
N |
Y |
Less than $20/month or $240/year |
|
Jiobit |
2017 |
Y |
Y |
Less than $20/month or $240/year |
Family support. It is important to alleviate family distress by helping the family gain an understanding of their child's behavior. Myths and misplaced guilt regarding the etiology of autism can contribute to marital, individual, and sibling stress. Families need professional and personal support to help them deal with guilt and frustration and with slow or seeming lack of progress. They must advocate for their child's educational needs and for their financial needs for various therapeutic interventions. They need respite care to enable them to attend to other members of the family. There are many self-help and support groups available through the local branches of the Autism Society of America, Autism Speaks, local autism organizations, and social media.
DIR floortime. DIR floortime is a child-directed therapy in which parents set aside regularly scheduled short periods of play with their child, with emphasis on promoting purposeful and positive reciprocal social exchange (11).
TEACCH. TEACCH (Treatment and Education of Autistic and Related Communication Handicapped Children) is based on a structured teaching curriculum with extensive environmental modifications and supports. To date, there are no studies with strong methodological experiment designs evaluating whether TEACCH or DIR is effective. Thus, research findings on these therapies should be interpreted with caution.
Folinic acid supplementation. Interest in folinic acid (leucovorin) as a potential treatment for autism spectrum disorder has increased following the FDA’s announcement of plans to approve it for cerebral folate deficiency, a rare neurologic condition that affects development. Although cerebral folate deficiency and autism spectrum disorder can share overlapping features, cerebral folate deficiency is a distinct diagnosis, and leucovorin is not yet FDA-approved for this indication.
Several small, early studies have examined leucovorin in autism spectrum disorder, with some preliminary evidence suggesting improvements in language and adaptive functioning, particularly among children who test positive for folate receptor alpha autoantibodies (FRAA). Research indicates that up to 38% of autistic individuals may show evidence of cerebral folate deficiency, and approximately 71% may test FRAA-positive (25). In these subgroups, impaired folate transport across the blood-brain barrier may contribute to language delay, irritability, motor differences, and developmental regression. Folinic acid can bypass this impaired transport mechanism, providing a biologically plausible rationale for supplementation.
Despite these promising findings, many critical questions remain unanswered, including which children may benefit, optimal dosing, treatment duration, and appropriate monitoring. Reported side effects include irritability, agitation, activation or hyperactivity, sleep disturbances, gastrointestinal discomfort, headache, and, rarely, increased stereotypy. FRAA testing is expensive, must be ordered through specialized laboratories, and is typically not covered by insurance.
Major professional organizations agree that evidence is insufficient to recommend folinic acid as a treatment for autism spectrum disorder. These groups emphasize that medications target associated behaviors rather than core autism features and that behavioral and developmental interventions should be implemented before considering any pharmacologic approach.
Given the limited evidence and outstanding questions, we do not recommend leucovorin treatment or FRAA testing for autistic patients at this time.
|
Study |
Design |
Sample |
Population characteristics |
Dose and duration |
Primary outcomes |
Key findings |
|
(08) |
Randomized, double-blind, placebo-controlled trial |
Approximately 48 |
Children with ASD; subset FRAA-positive |
Approximately 2 mg/kg/day folinic acid (max 50 mg/day), 12 weeks |
Verbal communication (CELF), adaptive behavior |
Significant improvement in verbal communication vs. placebo, especially in the FRAA-positive subgroup |
|
(08) |
Controlled open-label trial |
Approximately 44 |
ASD + FRAA |
High-dose folinic acid, approximately 2 mg/kg/day |
Language, behavior, adaptive skills |
Improvements in language, attention, and stereotypy; strongest effects in FRAA-positive children |
|
(23) |
Case series |
Approximately 5 to 20 per series |
Children with CFD, many with ASD features |
High-dose folinic acid (up to 1 to 2 mg/kg/day) |
Neurologic function, ASD symptoms, CSF 5-MTHF |
Normalization of CSF folate; improvements in communication, irritability, motor symptoms; uncontrolled data |
|
(21) |
Case series |
7 |
CFD with ASD or autistic features |
Folinic acid 0.5 to 1 mg/kg/day |
Language, social interaction, motor symptoms |
Reported improvements in communication and social engagement; uncontrolled |
|
(Scalais et al 2018) |
Case series |
6 |
CFD with ASD phenotype |
Folinic acid 1 to 2 mg/kg/day |
Global functioning, irritability, motor symptoms |
Clinical improvements noted; no control group |
|
Ongoing RCT (NCT02839915) |
Multicenter randomized controlled trial |
Target 134 |
ASD + moderate language impairment |
Folinic acid versus placebo, 12 weeks |
Language outcomes, biomarkers |
Results not yet published |
|
| ||||||
There is no evidence that art therapy, animal therapy, PROMPT, sensory integration therapy, auditory integration, chelation, or special diets are effective in managing autism spectrum disorder symptoms.
Stem cell therapy. Stem cell therapy has emerged as a proposed intervention for autism, based on the hypothesis that dysregulated immune-related genes in autism might be corrected through the infusion of cord blood cells expressing non-defective neuroimmunology profiles. However, significant concerns have been raised regarding the scientific validity and ethical implications of this approach. To date, there is no evidence supporting stem cell therapy as an effective treatment for autism spectrum disorder.
|
Drug Class |
Example of drugs |
Mechanism of action |
Connection to autism treatment |
Side effects |
Other autism-related information |
|
Atypical antipsychotics |
Risperidone |
Risperidone is a potent dopamine D2 or serotonin (5HT) receptor antagonist. Aripiprazole has a high affinityfordopamineD2 and D3 receptors and serotonin 5-HT1A and 5-HT2A receptors |
A RUPP multi-site randomized control trials study found that the greatest benefits reported by parents were for self-injurious behaviors and aggression (20) |
- Weight gain |
Only FDA-approved medications for treating the core symptoms of autism spectrum disorder |
|
Selective serotonin reuptake inhibitors |
Citalopram |
Blocks the serotonin transporter (SERT), which increases the availability of serotonin in the synaptic cleft, enhancing serotonergic neurotransmission and improving mood and anxiety symptoms |
Most prescribed drugs for autism spectrum disorder, although their use for the reduction of core symptoms is not supported by research evidence (Reiersen et al 2011; 16) |
- Upset stomach | |
|
Anti-seizure |
Divalproex |
Modulate neurotransmitter systems, including GABA and glutamate, and influence calcium channel activity |
Available evidence of the therapeutic behavioral effects of anti-seizure medications is inconclusive but promising (Allard et al 2025; Jang et al 2025) |
- Dizziness | |
|
Stimulants |
Methylphenidate |
Non-competitive blocks the reuptake of dopamine or noradrenaline transporter and leads to the increase levels of dopamine and noradrenaline in the synapse |
Only one small study with extended-release methylphenidate found a significant benefit (22) |
- Insomnia | |
|
Noradrenergic reuptake inhibitor |
Atomoxetine |
A reuptake inhibitor for neurotransmitters norepinephrine and epinephrine by blocking the norepinephrine transporter |
Believed to help with hyperactivity, irritability, aggression, and repetitive behaviors (Harfterkamp et al 2014; 12) |
- Fatigue | |
|
Alpha adrenergic receptor agonists |
Guanfacine |
Mimics epinephrine to activate alpha receptors |
Believed to help with behavioral regulation, especially hyperactivity, impulsiveness, irritability, and sleep issues (06) |
- Fatigue | |
|
Hormone analog |
Melatonin |
A hormone secreted by the pineal gland in response to the circadian rhythms |
Considered a first-line treatment of sleeping problems refractory to behavioral interventions (Gagnon et al 2018) |
- Daytime drowsiness |
Strong research evidence supports it for treating sleeping problems association with autism spectrum disorder |
Cannabinoids. Various trials have been conducted with positive results but many methodological issues. A randomized, double-blind, placebo-controlled single-site trial reported improvements in disruptive behavior significantly higher than placebo in 49% of subjects (02). Parents have reported adverse side effects such as insomnia, restlessness, irritability, unexplained laughter, loss of appetite, fatigue, mood changes, and gastrointestinal symptoms. More research, especially on long-term outcomes, is still needed.
Melatonin. Across clinical trials in children with autism spectrum disorder, melatonin (particularly prolonged-release formulations) consistently improves sleep onset latency and increases total sleep time. Early small studies using immediate-release melatonin showed modest benefits, whereas larger randomized controlled trials of pediatric prolonged-release melatonin (PedPRM) demonstrated more robust improvements in sleep onset, sleep duration, and sleep continuity, with added gains in caregiver sleep and quality of life. Long-term open-label data suggest sustained benefits and generally mild adverse effects. Despite these positive findings, evidence remains limited by small samples, short trial durations, and a lack of long-term controlled studies. A systematic review noted that melatonin prescriptions in young children have increased by more than 500% over two decades, even though rigorous autism spectrum disorder-specific safety and efficacy data are still lacking (17).
Outcomes in children diagnosed with autism spectrum disorder are variable, and it is well known that autism spectrum disorder is a stable diagnosis with symptoms noted along the lifespan. There is no effective treatment that will cure the symptoms of autism spectrum disorder. All affected individuals show functional impairments ranging from mild to severe, with an equivalent level of needed support. Language and cognitive level are the most important factors affecting outcomes. With treatment, there may be improved social functioning, but it may never be of normal quality or quantity.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Taiwo T Ajumobi DO MS
Dr. Ajumobi of Goreyb Children's Hospital has no relevant financial relationships to disclose.
See ProfileSaidi Clemente MD
Dr. Clemente of Saint Peter's University Hospital has no relevant financial relationships to disclose.
See Profile
Bernard L Maria MD
Dr. Maria of Thomas Jefferson University has no relevant financial relationships to disclose.
See ProfileMedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125