








Neuro-Oncology
Vestibular schwannoma
May. 27, 2026
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author explains the clinical presentation, pathophysiology, prevention, diagnostic work-up, and management of labyrinthine infarction. Although a variety of conditions can cause labyrinthine ischemia, labyrinthine infarction most commonly occurs in the setting of thromboembolic disease of the anterior inferior cerebellar artery or the basilar artery, and almost all of these cases present with acute, prolonged vertigo and vestibular dysfunction of peripheral, central, or combined origin. Unlike labyrinthine dysfunction from a viral cause, the most common pattern of dysfunction with labyrinthine infarction includes a combined loss of auditory and vestibular function. Canal paresis associated with posterior circulation ischemic stroke, usually within the anterior inferior cerebellar artery territory, typically normalizes within 5 years.
|
• The clinical manifestations of ischemia of the inner ear can include acute vertigo, nausea and vomiting, imbalance, unilateral deafness, tinnitus, and canal paresis. | |
|
• A variety of conditions can cause labyrinthine ischemia, including thromboemboli of the posterior circulation, fat emboli, thromboangiitis obliterans, migrainous infarction, decompression illness, hyperlipidemia, macroglobulinemia, sickle cell disease, leukemia, polycythemia vera, and other causes of hypercoagulation or hyperviscosity. | |
|
• Most commonly, labyrinthine infarction occurs in the setting of thromboembolic disease of the anterior inferior cerebellar artery or the basilar artery. | |
|
• Unlike labyrinthine dysfunction from a viral cause, the most common pattern of dysfunction with labyrinthine infarction includes a combined loss of auditory and vestibular function. | |
|
• If neurologic symptoms are absent, it is more likely that viral labyrinthitis is the cause of acute audiovestibular symptoms, especially in the absence of abnormal findings on imaging. | |
|
• Although acute unilateral hearing loss and hypofunction of the vestibulo-ocular reflex typically indicate labyrinthine dysfunction, cerebellar findings should not be overlooked, including direction-changing positional nystagmus, which suggests dysfunction of the posterior cerebellar vermis. | |
|
• Small infarcts of the brainstem or cerebellum can produce vertigo without other localizing neurologic symptoms: roughly 1 in 10 patients with an isolated cerebellar infarction present with vertigo, nystagmus, and postural unsteadiness mimicking acute peripheral vestibular disorders. | |
|
• The blood supply to the inner ear flows through only one main blood vessel, the internal auditory artery (or labyrinthine artery), which typically originates from the anterior inferior cerebellar artery. |
A series of important experimental studies in animals in the 1950s established that (1) cochlear function is extremely sensitive to anoxia, and electrical activity deteriorates within 60 seconds of interruption of blood flow; (2) cochlear function may return to normal if blood flow is restored within 8 minutes of complete obstruction but not if blood flow is interrupted for more than 30 minutes; (3) permanent obstruction of either the inferior cochlear vein or the internal auditory artery produces rapid loss of function and histologic changes; (4) external hair cells and the ganglion cells of the cochlea are particularly vulnerable to arterial obstruction, whereas the vestibular end organs are relatively resistant; (5) venous obstruction produces early epithelial edema, followed by hemorrhage into the epithelium and perilymphatic and endolymphatic spaces, hair cell damage with secondary ganglion cell degeneration, and later fibrosis and ossification; (6) arterial obstruction produces more rapid and severe damage than venous obstruction; (7) arterial obstruction produces early histologic changes in hair cells within 30 minutes, followed in a few hours by extensive necrosis including the supporting cells without hemorrhage and ultimately severe fibrosis and ossification by 6 months; (8) several patterns of end-organ involvement were observed with arterial obstruction corresponding to different arterial distributions within the inner ear; and (9) patterns of end-organ damage with arterial obstruction included involvement of all cochlear and vestibular end organs, involvement of the cochlea, saccule, and the posterior canal ampulla, or involvement of the utricle, part of the saccule, and the anterior and horizontal canal ampullae, but without cochlear involvement (21; 52; 53; 54; 55; 98; 97).
• Labyrinthine ischemia typically occurs in conjunction with brainstem and cerebellar ischemia due to involvement of the anterior inferior cerebellar artery (AICA) or the vertebrobasilar system. | |
• The preponderance of AICA-associated labyrinthine infarcts occurs because the labyrinth is supplied by the internal auditory artery, which, in turn, derives from the AICA. | |
• Clinically, labyrinthine infarction has been diagnosed based on several different scenarios: (1) AICA-territory infarcts with associated audiovestibular defects consistent with labyrinthine involvement; (2) an isolated acute audiovestibular defect is later followed by an AICA-territory infarct; or (3) an isolated acute audiovestibular defect occurs in conjunction with embolic infarctions outside of the AICA territory. | |
• The clinical manifestations of ischemia of the inner ear can include acute vertigo, nausea and vomiting, imbalance, unilateral deafness, tinnitus, and canal paresis. | |
• Arterial occlusion affecting the inner ear may present in several ways, with predominant auditory dysfunction, predominant vestibular dysfunction, or both. |
Labyrinthine ischemia typically occurs in conjunction with brainstem and cerebellar ischemia because of involvement of the anterior inferior cerebellar artery (AICA) or the vertebrobasilar system. The preponderance of AICA-associated labyrinthine infarcts occurs because the labyrinth is supplied by the internal auditory artery, which, in turn, typically derives from the AICA. Less commonly, labyrinthine ischemia may occur in conjunction with cochlear ischemia in the absence of brainstem or cerebellar involvement, or it may occur in isolation, for example, because of cardioemboli (13; 45; 95; 78). The constellation of clinical manifestations depends on the extent and distribution of the ischemia.
Spectrum of labyrinthine infarction. Clinically, labyrinthine infarction has been diagnosed based on several different scenarios:
(1) AICA-territory infarcts with associated audiovestibular defects consistent with labyrinthine involvement. This is the most common scenario. Labyrinthine infarction is most often presumed when patients show a combined loss of hearing and peripheral vestibular function associated with brainstem or cerebellar infarctions in the AICA territory (67; 78). Labyrinthine artery occlusion (sudden deafness and vertigo in one ear) may also herald a basilar artery stroke because the labyrinthine artery bifurcates from the AICA (120).
(2) An isolated acute audiovestibular defect is later followed by an AICA-territory infarct. Isolated labyrinthine infarction or ischemia has been described as an initial presentation of AICA infarctions based on subsequent progression of an isolated acute audiovestibulopathy into a full AICA-territory infarction involving the brainstem and cerebellum (50; 67; 78).
(3) An isolated acute audiovestibular defect occurs in conjunction with embolic infarctions outside of the AICA territory. Rarely, sudden deafness with or without caloric canal paresis may occur in association with infarctions involving the cerebellum or brainstem but in a non-AICA vascular territory. The sudden deafness in these cases was attributed either to a dominant posterior inferior cerebellar artery supplying the labyrinth, to the relative ischemic vulnerability of the labyrinth (63), or to a separate embolism to the labyrinth, which was not visualized with available imaging techniques (78). When there is an evident cardiac or artery-to-artery source of emboli, and when the associated non-AICA-territory infarctions are consistent with embolic phenomena, then a separate embolism to the labyrinth is the most likely explanation for the acute audiovestibular defects (78).
The clinical manifestations of ischemia of the inner ear can include acute vertigo, nausea and vomiting, imbalance, unilateral deafness, tinnitus, and canal paresis (85; 82; 23; 29; 83; 84; 94; 51; 113; 44; 68; 67; 78).
Arterial occlusion affecting the inner ear may present in several ways, with predominant auditory dysfunction, predominant vestibular dysfunction, or both. Those patients with predominant auditory dysfunction may present with sudden deafness (23; 121; 73; 65; 63), sometimes accompanied by transient dizziness and intermittent tinnitus (23; 29; 73; 65). Those with predominant vestibular dysfunction present typically with vertigo, nausea and vomiting, imbalance, canal paresis without hearing loss (83; 47; 63), and occasionally with tinnitus (113) or subsequent positional vertigo (77). Finally, patients may present with combined deficits, including vertigo and deafness (23; 29; 83; 121; 51; 119; 73; 65; 12; 99). These patterns reflect different vascular territories or susceptibilities to ischemia.
With ischemia of a labyrinth, there is typically a depression of vestibular activity on that side with resulting ipsilateral deafness or tinnitus and nystagmus beating away from the affected side and with a tendency to past-point and fall toward the ischemic labyrinth with Romberg testing or tandem gait (60; 61). Rarely, transient ischemia may produce brief excitation of inner ear structures, resulting in ipsilateral tinnitus but horizontal-rotatory nystagmus beating toward the affected side (113). This is thought to result from transiently increased excitability of hair cells and neurons with the onset of ischemia, resulting in an increased firing rate (113). With more prolonged ischemia, however, the membrane depolarizes, and the axonal membrane becomes inexcitable, thus producing the typical manifestations of labyrinthine hypofunction.
Hyperviscosity syndromes. Ischemia may also occur with vascular obstruction in the venules and capillaries that drain the inner ear, as occurs most commonly with conditions that produce marked serum hyperviscosity. The “hyperviscosity syndrome” includes many diverse clinical manifestations, including headache, fatigue, vertigo, nystagmus, sudden or progressive hearing loss, visual disturbances, and mucosal hemorrhages (92; 05). Ophthalmoscopic findings include markedly distended and tortuous (“sausage-shaped”) retinal veins and retinal hemorrhages similar to the pattern seen in retinal vein occlusion.
Vertebrobasilar ischemia. Vertebrobasilar ischemia with occlusion of the vertebrobasilar junction can present with episodes of monosymptomatic vertigo, likely due to labyrinthine ischemia (26; 22; 25). Peripheral vestibular abnormalities are common among such patients on electronystagmographic testing and presumably also on videonystagmography (26). Similarly, vertigo is among the most common prodromal symptoms of basilar artery occlusion; a number of these cases have clinical or pathologic evidence of peripheral vestibular dysfunction (122; 57; 20; 35).
Posterior inferior cerebellar artery (PICA) infarcts with mixed central and peripheral vestibular deficits. The spectrum of clinical presentation for PICA territory infarcts (lateral medullary syndrome or Wallenberg syndrome) includes a range of labyrinthine, brainstem, and cerebellar symptoms and signs, but isolated vertigo is possible and, indeed, fairly common (64). This syndrome is usually characterized by crossed sensory deficits affecting the face on the side of the infarct and affecting the trunk and extremities on the opposite side: specifically, there is a loss of pain and temperature sensation on the ipsilateral (ipsilesional) side of the face and the contralateral (contralesional) side of the body. Clinical symptoms and signs may include nystagmus, diplopia, skew deviation, facial pain, vertigo, dysphagia, dysarthria, dysphonia, ipsilesional hemiataxia, ipsilesional Horner syndrome, and possibly palatal myoclonus. Nystagmus and vertigo may result from involvement of the region of Deiters’ nucleus and other vestibular nuclei. Cases have been reported with mixed central and peripheral deficits following vertebral artery dissection and development of lateral medullary infarction and embolic internal auditory artery infarction (12). Findings on clinical examination in patients presenting with an acute vestibular syndrome include a normal bedside head impulse test, absence of acute hearing loss, variable spontaneous or gaze-evoked nystagmus, variable skew deviation, and variable (though usually severe) postural instability (11; 64; 48).
Anterior inferior cerebellar artery (AICA) infarcts with mixed central and peripheral vestibular deficits. The spectrum of clinical presentation for AICA territory infarcts also includes a range of labyrinthine, brainstem, and cerebellar symptoms and signs: ipsilateral Horner syndrome (rare), skew deviation (rare), pathological ocular torsion, nystagmus, ipsilateral facial numbness, ipsilateral facial paresis (possibly restricted to emotional facial paresis), vertigo, sudden ipsilateral hearing loss with or without tinnitus, dysarthria, vomiting, variable unsteadiness, ipsilateral truncal deviation, ipsilateral hemiataxia, and contralateral loss of pain and temperature sensation on the limbs and body (03; 94; 04; 32; 72; 70; 73; 65; 63; 67; 42; 88; 66; 112; 01; 46; 79; 64). Vertigo with hypoacusis occurs most commonly in anterior inferior cerebellar artery-territory infarctions that involve both the middle cerebellar peduncle and the inferior lateral pons (101). Hearing loss occurs in about two thirds of patients with anterior inferior cerebellar artery-territory infarcts (116). In some cases, the only neurologic sequela is isolated permanent ipsilateral hearing loss (88). Occasionally, isolated vertigo may occur as transient ischemic attacks preceding anterior inferior cerebellar artery-territory infarction or with partial anterior inferior cerebellar artery infarcts (03; 94; 64). It is difficult to establish labyrinthine infarction clinically in the setting of anterior inferior cerebellar artery territory infarction because central and peripheral signs are often mixed (112). Also, central lesions may uncommonly produce similar clinical manifestations of vertigo, nystagmus, hearing loss, canal paresis, and ataxia (103; 34; 33; 24; 64). In particular, vascular lesions at the root entry zone or involving the vestibular nuclei and portions of the cerebellum can present clinically as acute unilateral vestibulopathy, including with concomitant caloric canal paresis and an abnormal bedside head impulse test (28; 33; 24; 93; 11; 64; 110); this subtype of anterior inferior cerebellar artery stroke has been labeled AICAp with peripheral characteristics, which is indicated by a positive clinical head impulse test, as distinguished from AICAc with central characteristics, which is indicated by a negative clinical head impulse test (11).
Acute cochleovestibulopathy. An acute, persisting vestibular syndrome lasting more than 24 hours with ipsilateral sensorineural hearing loss suggests a vascular etiology (ie, labyrinthine infarction) rather than inflammatory disease (eg, labyrinthitis), especially in patients with cardiovascular risk factors (44; 67; 02; 16).
An acute isolated labyrinthine infarction may progress into brainstem or cerebellar stroke (50; 45), and in this way, labyrinthine infarction is comparable to amaurosis fugax or branch retinal artery occlusion.
HINTS and HINTS plus. An isolated labyrinthine infarction (without brainstem or cerebellar involvement) does not elicit a central "HINTS" examination result because it is a peripheral vestibulopathy, even if it carries a significant risk of posterior circulation stroke (16). The so-called “H.I.N.T.S.” or “HINTS” tripartite examination (ie, Head Impulse test, Nystagmus type, and Test-of-Skew) combines an assessment of the head impulse test (HIT), assessment of direction-changing horizontal nystagmus evoked by lateral gaze to the right and left, and assessment of vertical skew deviation by alternate cover testing (41; 10; 91; 90; 106; 105; 09; 118). The acronym mnemonic INFARCT—Impulse Negative (negative head impulse test); Fast phase Alternating (central pattern nystagmus); and Refixation during Cover Test (ie, skew deviation)—suggests a stroke or other central diagnosis (41). Typically, with labyrinthine infarction, the HINTS exam would not suggest a stroke or other central diagnosis: (1) the head impulse test will be abnormal with a visible refixation saccade with ipsilesional head impulses; (2) there will be a peripheral vestibular nystagmus characterized by unidirectional horizontal-torsional jerk nystagmus with a contralesional fast phase that intensifies with fixation removed; and (3) there will be no skew deviation evident with alternate cover testing. In the absence of other information, this HINTS result would generally be interpreted as suggesting a relatively benign peripheral vestibular condition, like vestibular neuritis. However, acute cochleovestibular loss is not always due to a viral or inflammatory inner ear condition; it may result from ischemia or infarction of the cochlea and labyrinth (40).
The updated form of the HINTS examination approach, the “H.I.N.T.S. plus” or “HINTS plus” quadripartite examination, addresses some of the limitations of HINTS. The HINTS plus examination is simply the HINTS examination plus an assessment of bedside hearing by finger rub (91; 90; 106). Most cases of labyrinthine infarction with both labyrinthine and cochlear involvement will be identified by the HINTS plus approach because, fortunately, the most common pattern of dysfunction with labyrinthine infarction is a combined loss of auditory and vestibular function (45).
Despite the numerous studies promoting HINTS or HINTS plus, the individual elements of the quartet of findings may be misleading at times. Patients with peripheral vestibulopathy may have a skew deviation, suggesting (wrongly) that the lesion is central. In fact, up to a quarter of individuals with an acute unilateral vestibulopathy have a skew deviation (27; 59), although such skew deviations with peripheral vestibular disorders are usually of small magnitude (39; 18) and may be evident only with a Maddox rod testing rather than with alternate cover testing (27). Consequently, some patients with labyrinthine infarction, including those with isolated labyrinthine infarction and those with a skew deviation, might not be separately identified with the HINTS plus approach (95). Furthermore, when used in isolation by emergency physicians, the HINTS examination has not been shown to be sufficiently accurate to rule out a stroke (including labyrinthine infarction) in those presenting with an acute vestibular syndrome (96).
The overall prognosis depends on the underlying etiology. In isolated labyrinthine infarction, vertigo, nystagmus, and autonomic manifestations resolve over days to weeks, but deafness and canal paresis typically remain (83; 43; 121; 36; 51). If no brainstem symptoms develop and brain imaging is normal, the risk of recurrence or subsequent stroke is rare (83; 51). Late effects can include benign paroxysmal positional vertigo, especially with infarction in the territory of the anterior vestibular artery (77). In this situation, ischemia of the utricle results in displacement of otoconia from the macula, which may then lodge in the still-functioning posterior semicircular duct, producing the symptoms of positioning nystagmus (62). Patients with labyrinthine ischemia due to vertebrobasilar insufficiency can have an overall good prognosis with anticoagulation or antiplatelet therapy (22). Rarely, surgical correction of a rotational vertebral artery syndrome is necessary (113). However, patients with labyrinthine infarction combined with brainstem or cerebellar infarcts have a worse prognosis (25), particularly if associated with occlusive disease of the basilar artery (20; 35).
Case 1. Labyrinthine infarction with combined audiovestibulopathy and pathologic confirmation at autopsy (51).
An 84-year-old woman developed acute vertigo with nausea and vomiting, followed by a brief syncopal spell as well as subsequent right-sided deafness, left-beating spontaneous nystagmus, and profound imbalance with a tendency to fall to the right (51). Electronystagmography showed absent caloric responses on the right. MRI of the brain and an echocardiogram were normal. The vertigo, nystagmus, and autonomic symptoms resolved over several days, although she continued to have profound right-sided hearing loss, poor balance, and nonspecific dizziness. She was treated with aspirin. Six years later, an audiogram showed profound sensorineural hearing loss on the right and age-appropriate mild sensorineural hearing loss on the left. The patient died of myocardial infarction 7 years after the onset of her symptoms. At autopsy, there was no evidence of brainstem or cerebellar infarction. Also, despite some atherosclerotic changes in the posterior circulation, the vertebrobasilar system, right anterior inferior cerebellar artery, and right internal auditory artery were patent. There were marked degenerative changes in the right cochlea, utricular macule, and cristae of the anterior and horizontal semicircular ducts and less severe changes in the crista of the posterior duct and the saccular macule. In the cochlea, there was complete destruction of the organ of Corti in the basal portion and loss of hair cells in the apex without evident fibrosis or ossification. In the vestibular labyrinth, the hair cells and underlying nerve fibers were destroyed in the anterior and horizontal duct cristae but were preserved in some areas of the posterior duct crista. There was mild fibrosis, but no ossification, of the vestibular labyrinth. Patchy degeneration was evident in the right vestibulocochlear nerve. Additionally, a marked loss of Scarpa ganglion cells with degenerative changes was found in the remaining cells. These findings demonstrated the residua of labyrinthine infarction, likely resulting from a transient period of decreased perfusion in the internal auditory artery.
Case 2. Labyrinthine infarction with combined audiovestibulopathy from cardiac septic emboli due to bacterial endocarditis (78).
A previously healthy 42-year-old woman with fever, headache, and pharyngitis for 3 days developed sudden bilateral visual loss and dysarthria and then became confused and agitated, requiring sedation. Examination showed tachycardia (142 beats/minute), fever (39.6°C), nuchal rigidity, and tender maculopapular rashes in both hands and feet consistent with Janeway lesions. Fundus examination showed multiple scattered retinal hemorrhages with a white center in both eyes, consistent with Roth spots. Hematologic assays showed leukocytosis (12,700/μL with 94% neutrophils), mild anemia (hemoglobin 9.6 g/dL; hematocrit 29.9%), and mild thrombocythemia (135,000/μL). CSF studies showed a marked neutrophilic pleocytosis (1,020/mm3 with 80% neutrophils), elevated RBC count (200/mm3), elevated CSF protein (166.0 mg/dL), and a normal CSF glucose but with a low CSF/serum glucose ratio (55 mg/dL with corresponding serum glucose 122 mg/dL, with a CSF/serum glucose ratio of 0.45, whereas the normal ratio is 0.6). Because of suspected bacterial meningitis, the patient was started on vancomycin (2.6 g per day) and ceftriaxone (4 g per day). Blood cultures later grew methicillin-resistant Staphylococcus aureus. Transthoracic echocardiography showed a hypermobile vegetation attached to the mitral valve, which precipitated mitral valve replacement 20 days after the onset of symptoms.
When the patient regained consciousness 1 day after her heart surgery, she complained of dizziness, hearing loss, and tinnitus in the right ear. Examination showed no spontaneous nystagmus with or without visual fixation, but horizontal head-shaking induced a left-beating nystagmus. Horizontal saccades and smooth pursuit were normal. She fell to the right when she attempted to stand or walk. The remainder of her neurologic examination was unrevealing. She had no weakness, sensory changes, or cerebellar dysfunction.
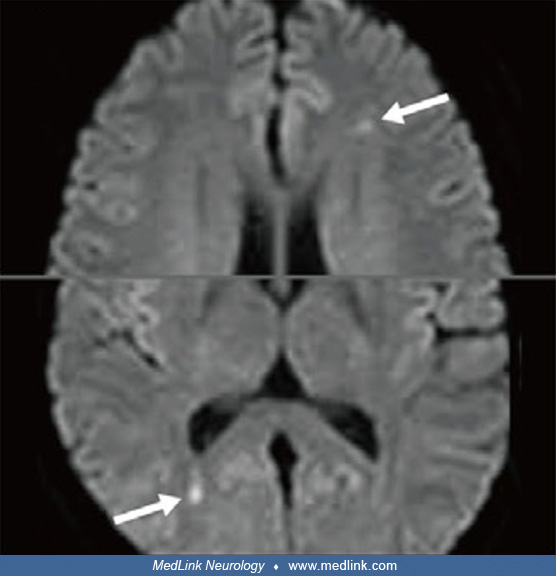
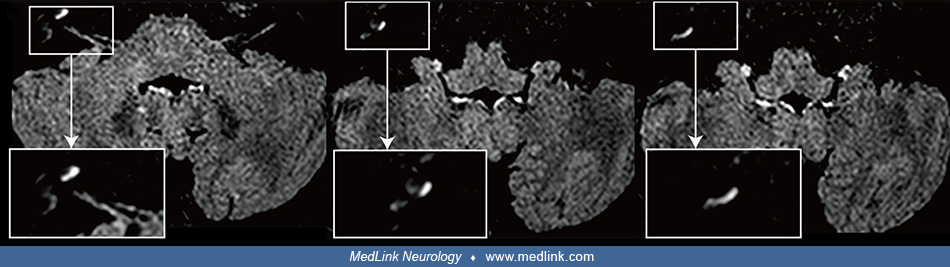
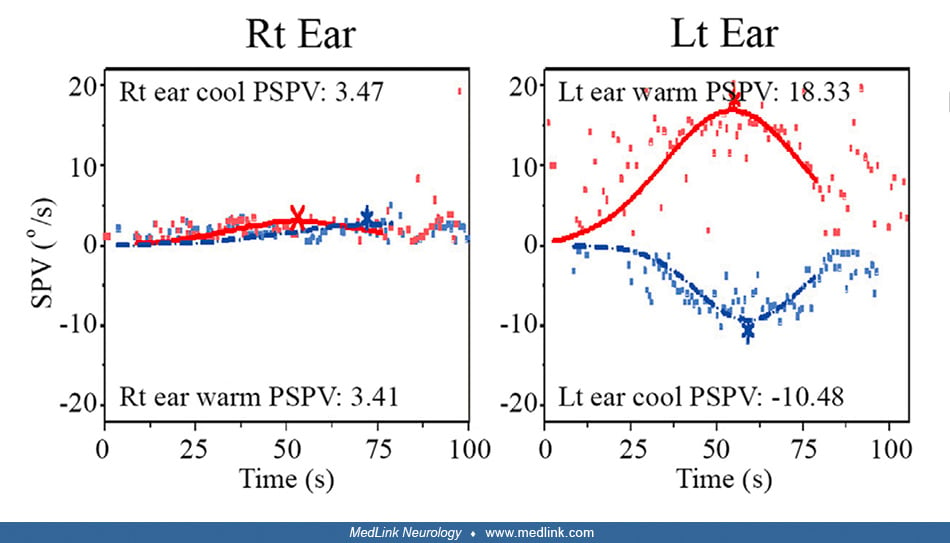
Video head-impulse tests were abnormal for the right horizontal and posterior canals. Bithermal caloric tests showed a right canal paresis of 81%. Pure-tone audiometry showed some residual hearing in the lower frequencies in the right ear, 250 to 500 Hz, but complete deafness at or above 1000 Hz in the right ear. Measurements of ocular torsion and subjective visual vertical were normal. Cervical and ocular vestibular-evoked myogenic potentials (VEMPs) showed no responses during right ear stimulation. Brain MRI with gadolinium showed contrast enhancement of the vestibule, cochlea, and semicircular canals on the right side as well as multiple scattered infarctions in the frontal and occipital lobes. MR angiography was normal.
Her clinical history, neuro-otologic and general neurologic examinations, and the results of diagnostic testing were consistent with multiple infarctions due to endocarditis with septic emboli from a cardiac vegetation.
Embolic labyrinthine infarction was diagnosed based on the occurrence of acute audiovestibular symptoms consistent with labyrinthine infarction in the presence of a cardiac source of embolism, no concurrent AICA infarction involving the brainstem or cerebellum, and concurrent embolic infarctions observed in the non-AICA territories.
She was discharged after 6 weeks of intravenous vancomycin and anticoagulation. She had minimal residual dizziness, but her hearing loss and tinnitus remained unchanged.
Case 3. Labyrinthine infarction with isolated vestibulopathy in a patient with a patent foramen ovale (78).
A 73-year-old man with a known patent foramen ovale developed acute vertigo with nausea and vomiting on his way to the bathroom on awakening. He denied associated aural fullness, tinnitus, hearing loss, or sensorimotor symptoms. The vertigo lasted into the afternoon with associated severe imbalance, but it subsided after symptomatic medication was administered at a local hospital for a presumed diagnosis of “vestibular neuritis.”
When evaluated at an otolaryngology unit at a tertiary medical center 6 days after symptom onset, he showed spontaneous nystagmus beating leftward and upward without fixation. Bedside head impulse tests were abnormal for the right horizontal canal. Rightward ocular torsion was observed on fundus photos. Measurements showed that the subjective visual vertical was significantly tilted to the right on both monocular and binocular viewing. Bithermal caloric tests showed complete right canal paralysis. Ocular VEMPs showed no responses during right ear stimulation, but findings of cervical VEMPs were symmetric. Audiometry was normal. Brain MRI disclosed a tiny acute infarction in the left parahippocampal gyrus (posterior cerebral artery territory). The findings of MR angiography were normal.
Pure-tone audiometry shows symmetric responses between the ears . There is evidence of bilateral symmetric sloping high-frequency sensorineural hearing loss. Lt = left; Rt = right; O= air conduction, unmasked, right ear; < =...
Embolic labyrinthine infarction was diagnosed based on the occurrence of acute audiovestibular symptoms consistent with labyrinthine infarction in the presence of a cardiac source of embolism, no concurrent AICA infarction involving the brainstem or cerebellum, and concurrent embolic infarctions observed in the non-AICA territories.
|
• Labyrinthine infarction results from ischemia localized to the peripheral labyrinth, although there may be concomitant infarction of the brainstem and cerebellum. | |
|
• The blood supply to the inner ear flows through only one main blood vessel, the internal auditory artery (or labyrinthine artery), which typically originates from the anterior inferior cerebellar artery. | |
|
• Venous drainage of the labyrinth is via the vein of the cochlear aqueduct for the cochlea and saccule. | |
|
• The anterior inferior cerebellar artery, a branch of the basilar artery, supplies the lateral pons, the middle cerebellar peduncle, the flocculus, the anterior part of the cerebellar lobules, and the inner ear. |
Labyrinthine infarction results from ischemia localized to the peripheral labyrinth, although there may be concomitant infarction of the brainstem and cerebellum. In addition, labyrinthine infarction may be incomplete, with partial sparing of the inferior vestibular labyrinth because of better collateral blood flow to this portion of the labyrinth (51). Sudden bilateral hearing impairment suggests vertebrobasilar occlusive disease (111; 35; 15; 72; 08).
The blood supply to the inner ear flows through only one main blood vessel, the internal auditory artery (or labyrinthine artery), which typically originates from the anterior inferior cerebellar artery (AICA), but sometimes originates directly from the vertebral or basilar artery and uncommonly from the posterior inferior cerebellar artery (PICA) (06; 80; 81; 30; 16; 117). The internal auditory artery divides into two main branches within the internal auditory canal: (1) the anterior vestibular artery and (2) the common cochlear artery (06; 81; 30). The anterior vestibular artery supplies the anterior superior vestibule, including the utricle with its macula, the superior part of the saccule, and the ampullae and cristae of the anterior and horizontal semicircular ducts (06; 81; 30). The common cochlear artery divides into the main cochlear artery and the vestibulocochlear artery, which together supply the cochlea (30). In addition, a posterior vestibular branch of the vestibulocochlear artery supplies the posterior vestibule, including the inferior saccule along with its macula, and the ampulla and crista of the posterior semicircular duct (06; 81; 30). The internal auditory artery and its branches are terminal or end arteries, so even transient ischemia can cause permanent inner ear damage (16). The organ of Corti is particularly sensitive to ischemia (107), especially at its apical region, so low-frequency hearing loss is common with inner ear ischemia (71). Inner ear ischemia should be suspected when unilateral posterior canal hypofunction occurs in combination with unilateral sensorineural hearing loss on the same side because both receptor organs are supplied by the common cochlear artery (vestibulocochlear artery) (99; 16).
Venous drainage of the labyrinth is via the vein of the cochlear aqueduct for the cochlea and saccule. The vein of the vestibular aqueduct is utilized by the utricle and semicircular canals (06; 81). The vein of the cochlear aqueduct empties into the bulb of the jugular vein, whereas the vein of the vestibular aqueduct drains into the superior petrosal sinus (06; 81). Labyrinthine ischemia attributed to impaired venous drainage most commonly results from hyperviscosity syndromes (87; 102; 92; 05; 104; 114). Increased blood viscosity produces obstruction in the labyrinthine venules and capillaries with decreased blood flow and inner ear ischemia as well as subsequent hemorrhage and, later, fibrosis and ossification (52; 53). Similar changes in the eye produce visual disturbances, markedly distended and tortuous (“sausage-shaped”) retinal veins, and retinal hemorrhages.
The anterior inferior cerebellar artery, a branch of the basilar artery, supplies the lateral pons, the middle cerebellar peduncle, the flocculus, the anterior part of the cerebellar lobules, and the inner ear (03). The course of the anterior inferior cerebellar artery is somewhat variable (109). In patients with anterior inferior cerebellar artery territory infarction, the most consistently involved areas were the lateral pons and the middle cerebellar peduncle (03; 101). Because of the sharp angulation of the anterior inferior cerebellar artery at its origin, it is rarely occluded by emboli (121); rather, most occlusions are due to either basilar artery plaques extending into the anterior inferior cerebellar artery or microatheroma of the anterior inferior cerebellar artery origin (04). Whether isolated or in combination with other symptoms and signs, vertigo can occur in anterior inferior cerebellar artery-distribution infarctions due to involvement of several central and peripheral sites, including the labyrinth, the eighth nerve, the vestibular nuclei, the vestibulocerebellum, or some combination of each. However, isolated vertigo from anterior inferior cerebellar artery-territory infarctions is rare (04). Labyrinthine infarction, in conjunction with anterior inferior cerebellar artery territory infarction, has been anticipated based on animal studies (55), supported by clinical studies (94), and reported on in histologic studies (32). The limited histopathologic data are controversial (31).
Damage to vestibular end organs during ischemia is mediated in part by glutamate (108) and reactive oxygen species (38). Morphological changes induced by glutamate cytotoxicity are evident in the bouton-type endings and the nerve chalices (formed by vestibular nerve branches that surround type I hair cells) by 30 minutes of ischemia in animal models (108).
The condition is uncommon but probably under-recognized. Most reports are individual case reports or small case series.
No specific information is available. Presumably, the risk factors are the same as for general stroke.
Most commonly, labyrinthine infarction occurs in the setting of thromboembolic disease of the anterior inferior cerebellar or the basilar artery (29; 32; 94; 04; 35; 51; 119; 113; 72; 70; 73; 65; 66; 110). As a result of such lesions, there is often mixed central and peripheral vestibular dysfunction, making recognition of the components difficult (69; 64). Without associated central nervous system signs, it may be difficult to recognize the ischemic basis of the clinical presentation. Indeed, if neurologic symptoms are absent, it is more likely that viral labyrinthitis is the cause of acute audiovestibular symptoms, especially in the absence of abnormal findings on imaging (70; 49). Nevertheless, labyrinthine infarction may cause acute unilateral peripheral vestibulopathy that mimics vestibular neuritis, and concomitant labyrinthine infarction should be suspected in patients with acute vestibular syndrome and acute infarction in the territory of the anterior inferior cerebellar artery (89). Other considerations may include inflammatory, viral, and other infectious and traumatic causes of labyrinthine dysfunction. Unlike labyrinthine dysfunction from a viral cause, the most common pattern of dysfunction with labyrinthine infarction includes a combined loss of auditory and vestibular function (68). Although acute unilateral hearing loss and hypofunction of the vestibulo-ocular reflex typically indicate labyrinthine dysfunction, cerebellar findings should not be overlooked, including direction-changing positional nystagmus, which suggests dysfunction of the posterior cerebellar vermis (110). Small infarcts of the brainstem or cerebellum can produce vertigo without other localizing neurologic symptoms: approximately 11% of the patients with an isolated cerebellar infarction present with vertigo, nystagmus, and postural unsteadiness mimicking acute peripheral vestibular disorders (69; 64; 76).
A variety of conditions can cause labyrinthine ischemia, including thromboemboli of the posterior circulation (17; 66; 73; 71; 47; 99), dissection of the vertebral artery (19), fat emboli (37), thromboangiitis obliterans (56), migrainous infarction (71); Susac syndrome (115; 14); decompression illness, particularly in the presence of a right-to-left cardiac shunt (58), hyperlipidemia (104), macroglobulinemia (102; 92), sickle cell disease (87; 05; 100), intravascular lymphomatosis (07), leukemia (05), polycythemia vera (05; 114), and other causes of hypercoagulation or hyperviscosity (37; 05).
|
• Diagnostic studies can include imaging of the brain and cerebral vessels, audiograms and brainstem auditory evoked potentials, electronystagmography or videonystagmography with bithermal caloric irrigation, and cervical vestibular-evoked myogenic potential studies. | |
|
• Audiovestibular tests do not readily distinguish ischemic and nonischemic causes of combined vertigo and sudden sensorineural hearing loss. | |
|
• Audiograms demonstrate sensorineural hearing loss that may be profound. | |
|
• Brain imaging is important to exclude brainstem or cerebellar lesions, but, unfortunately, current imaging techniques are inadequate to allow confident identification of isolated labyrinthine infarctions as a cause of acute audiovestibulopathy. | |
|
• In cases of clinically suspected labyrinthine ischemia resulting from hyperviscosity, the following blood studies can be considered: serum viscosity determination, complete blood count, syphilis serologies, sedimentation rate, serum protein, serum protein electrophoresis, and lipid studies. |
Diagnostic studies can include imaging of the brain and cerebral vessels, audiograms and brainstem auditory evoked potentials, electronystagmography or videonystagmography with bithermal caloric irrigation, and cervical vestibular-evoked myogenic potential studies. Audiovestibular tests do not readily distinguish ischemic and non-ischemic causes of combined vertigo and sudden sensorineural hearing loss (99).
Audiograms demonstrate sensorineural hearing loss that may be profound. Brainstem auditory evoked potentials may show an absence of wave 1 or all waveforms, but they may also show an absence of wave 1 with delay of waves 3 and 5 if there is also dysfunction in the retrocochlear eighth nerve and brainstem auditory nuclei and pathways (119).
Electronystagmography or videonystagmography with bithermal caloric testing demonstrates ipsilateral horizontal canal paresis. Canal paresis associated with posterior circulation ischemic stroke, usually within the territory of the anterior inferior cerebellar artery, typically normalizes within 5 years (74).
Brain imaging is important to exclude brainstem or cerebellar lesions and occasionally may be supportive of labyrinthine infarction, especially with delayed contrast (86); but unfortunately, current imaging techniques are inadequate to allow confident identification of isolated labyrinthine infarctions as a cause of acute audiovestibulopathy (13; 78; 16). In particular, MRI does not generally visualize the inner ear well enough to identify infarction. Conventional or MR angiography in cases of sudden bilateral deafness may demonstrate stenosis of the distal vertebral arteries and proximal basilar artery (72).
In cases of clinically suspected labyrinthine ischemia resulting from hyperviscosity, the following blood studies can be considered: serum viscosity determination, complete blood count, syphilis serologies, sedimentation rate, serum protein, serum protein electrophoresis, and lipid studies.
|
• Acute vertigo and concomitant nausea and vomiting can be suppressed with a variety of medications. | |
|
• Vestibular rehabilitation should be begun early. |
Management depends on the underlying etiology. Acute vertigo and concomitant nausea and vomiting can be suppressed with a variety of medications (60). Vestibular rehabilitation should be begun early (60). Anticoagulation can effectively stop attacks of episodic vertigo due to vertebrobasilar insufficiency; this treatment is particularly effective in patients with recurrent symptoms, despite antiplatelet therapy (22).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
May. 27, 2026
General Child Neurology
May. 12, 2026
Neuro-Ophthalmology & Neuro-Otology
Apr. 07, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 30, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 30, 2026
Neuromuscular Disorders
Mar. 02, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 02, 2026
Neuro-Ophthalmology & Neuro-Otology
Mar. 02, 2026