Etiology and pathogenesis
The intrinsic human circadian rhythm is typically longer than 24 hours, yet daily time cues allow for this reorientation of the clock to the surrounding environment. The loss of the ability of the time cues to influence the clock appears to be the major factor in non-24-hour sleep-wake rhythm disorder. Those time cues include bright light, activity, food, and social interaction. Some estimate that over half of blind individuals have non-24-hour sleep-wake disorder, with 50% to 80% complaining of sleep disturbances (31).
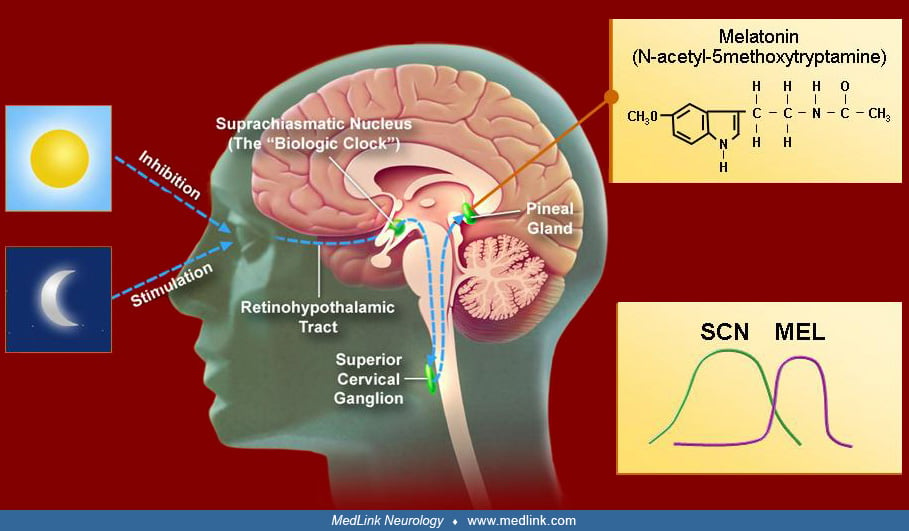
The connection of lack of sight to this circadian rhythm disorder is through a different pathway than the conventional pathway of vision. Light influences the retinal ganglion cell layer from which axons course along the optic nerve and leave the optic chiasm to innervate the suprachiasmatic nucleus. Interruption of these fibers, by either congenital or acquired blindness prevents information regarding light to be transmitted to the master circadian pacemaker and, thus, prevents light from contributing to the entrainment process. Thus, the endogenous non-24-hour rhythm is unmasked and demonstrated in the sleep-wake cycle. Individuals who are blind because of lesions posterior to the optic chiasm, such as cortical blindness, do not get the disorder. For many blind subjects who have a chiasmal or prechiasmal lesion, nonphotic (social, timed meals) cues may not be sufficient to synchronize the endogenous rhythm with the environmental.
For individuals who are sighted and have non-24-hour sleep-wake rhythm disorder, the pathology is less clear. Some of these individuals have a history of head trauma, suggesting a possible disruption of the retino-hypothalamic fibers, caused by damage to the suprachiasmatic nucleus or disrupted the secretion of melatonin. The etiology of non-24-hour sleep-wake disorder in sighted individuals is unknown, but it has been theorized to be due to prolongation of the endogenous circadian period, making it more difficult to entrain to a 24-hour day (27). In one case series, similar features of cases starting in adolescence raise the possibility of maturational changes to the inherent clocks’ responsiveness to time cues or abnormally long rhythms in which typical entrainment cues actually cause a prolongation of the rhythm (25; 26). In another case, a man underwent chemotherapy for Hodgkin lymphoma and developed a free running cycle of 25.27 hours, which did not respond to bright light and melatonin (11). Another possible contributing mechanism may be an impaired melanopsin-dependent phototransduction pathway. The melanopsin pathway does contribute to pupillary constriction to high intensity blue light. An indirect measure of this utilizes quantification of post-illumination pupil ability to sustain contraction. Abbott and colleagues showed that sighted individuals with non-24-hour sleep-wake rhythm disorder had a reduced response, indicating a possible reduction in the contribution the melanopsin pathway to entraining the circadian rhythm (02). This proposed mechanism of decreased light to the back of the eye is one hypothesis offered to explain the higher frequency of non-24-hour sleep-wake disorder in sighted older adults (20).
In another venue, Emens and colleagues reported three sighted individuals with non-24-hour sleep-wake rhythm disorder, in which one demonstrated in a prolonged time controlled environment using plasma and salivary assessment of dim light melatonin onset a normal circadian rhythm length (07). The other two individuals sleep-wake cycles responded to adjustment of the schedule. From this, Emens and colleagues concluded that for these three individuals that behavior and light exposure was the underlying driver of the progressive sleep-wake schedule. However, two of the individuals had depressed mood issues. The underlying driver for these patients' conditions is unclear and may represent the complex interaction of the sleep homeostatic process, the monoamine system relating to mood and the central circadian system (21). In a separate case report, a 14-year-old male developed non-24 sleep-wake disorder in association pediatric autoimmune neuropsychiatric disorder associated with streptococci infection that occurred prior to the onset of symptoms (09).
Review of circadian mechanisms. All living organisms possess an inherent circadian rhythm. This near 24-hour cycle modulates a variety of physiologic and behavioral processes, such as sleep-wake cycle, body temperature, mood, hormone secretion, and many others. The paired suprachiasmatic nuclei of the hypothalamus have been established as the “master clock” that sets the timing of the mammalian circadian system. The suprachiasmatic nuclei are composed of 10,000 anterior ventromedial hypothalamic neurons that maintain a self-sustaining daily rhythm. This cycle is achieved through a complex system of timed gene expression that creates an autoregulatory feedback loop. A variety of genes are involved in this cycle, including Clock, Per, Bmal1, and Cry. This complex cycle is vulnerable to changes in these genes or genes of proteins involved in regulation of these factors (23).
The biological clocks of normal humans of all ages have a natural endogenous circadian cycle of slightly more than 24 hours, generally about 24.2 hours. Therefore, the internal body clock must be adjusted on a daily basis to align with the 24-hour day, a process called entrainment. Entrainment involves using zeitgebers (German for “time givers”) to reset the internal clock slightly each day. Common zeitgebers include light, melatonin, food intake, social interaction, and exercise. Each of these factors can independently change the timing of the circadian pacemaker, thereby altering the time of all physiologic processes that are regulated on a circadian basis.
Light is the main zeitgeber for endogenous clocks in humans. The human circadian system is more sensitive to short-wave blue-green light than to long-wave red-spectrum light. The major afferent input to the SCN consists of a melanopsin-containing subset of photosensitive retinal ganglion cells whose axons synapse on SCN cells. This retinohypothalamic tract transmits nonvisual, light-dark information to the SCN, which is mediated through glutamate and pituitary cyclase-activating peptide. In addition to a direct pathway, retinal ganglion cells also project to the intergeniculate leaflet of the lateral geniculate body, which in turn projects to the SCN. Neuropeptide Y and GABA are the main neurotransmitters. Other time clues appear to influence the SCN through serotonergic input from the brainstem raphe nuclei.
Key to understanding the zeitgebers is that the response of the circadian rhythm depends on when the stimulus is delivered. For example, light delivered prior to the temperature nadir (typically 4:00 AM in normal phase individuals) will cause a delay in the body clock. Light delivered after the body temperature nadir will advance the clock. Thus, for light therapy to be appropriately used, understanding the true timing of the circadian rhythm is essential. The temperature nadir is typically 1.5 to 2 hours before the undisturbed natural wake up time. Therefore, if a person is naturally waking at 11 AM without an alarm, the temperature nadir would most likely be between 9:00 and 9:30 AM.
Similar to light, melatonin also has a time-dependent effect on the phase of the circadian rhythm. However, melatonin has the opposite effect of light, such that melatonin delivered in the evening causes a phase advance whereas morning use may cause a mild phase delay. The SCN exhibit dense melatonin receptors, probably establishing a feedback mechanism for the sleep-wake cycle. Melatonin and potentially other factors such as light help synchronize the multitude of endogenous rhythms in the brain and other organs. Synchronization of these endogenous rhythms is important to optimal body function. Isolated delay in an endogenous rhythm has been implicated in individuals with nocturnal eating syndrome, which appears to be a delay in the feeding rhythm. Although appearing benign, in this disorder the timing of food intake can impact insulin sensitivity and metabolism, as well as potentially lead to weight gain. Meals also appear helpful in aligning peripheral cocks, such as in the liver, to the new schedule.